Embed Size (px)
Citation preview

Radiología. 2014;56(6):485---495
www.elsevier.es/rx
UPDATE IN RADIOLOGY
A practical introduction to the hemodynamic analysis
of the cardiovascular system with 4D Flow MRI�
J.A. Pineda Zapata a,∗, J.A. Delgado de Bedout a, S. Rascovsky Ramírez a,C. Bustamante a, S. Mesab, V.D. Calvo Betancur a
a Grupo de Investigación, Instituto de Alta Tecnologia Médica (IATM), Medellín, Antioquia, Colombiab Universidad CES, Medellín, Antioquia, Colombia
Received 15 November 2013; accepted 14 August 2014
KEYWORDS4D Flow;Cardiovascularmagnetic resonanceimaging;Phase contrastangiography;Hemodynamics;Blood flow
Abstract The 4D Flow MRI technique provides a three-dimensional representation of blood
flow over time, making it possible to evaluate the hemodynamics of the cardiovascular system
both qualitatively and quantitatively. In this article, we describe the application of the 4D Flow
technique in a 3 T scanner; in addition to the technical parameters, we discuss the advantages
and limitations of the technique and its possible clinical applications. We used 4D Flow MRI to
study different body areas (chest, abdomen, neck, and head) in 10 volunteers. We obtained
3D representations of the patterns of flow and quantitative hemodynamic measurements. The
technique makes it possible to evaluate the pattern of blood flow in large and midsize vessels
without the need for exogenous contrast agents.
© 2013 SERAM. Published by Elsevier España, S.L.U. All rights reserved.
PALABRAS CLAVE4D Flow;Resonanciamagnéticacardiovascular;Angiografía concontraste de fase;Hemodinámica;Flujo sanguíneo
Introducción práctica al análisis hemodinámico del sistema cardiovascular mediante
la técnica «4D Flow»
Resumen La técnica de resonancia magnética 4D Flow permite evaluar cualitativa y cuanti-
tativamente la hemodinámica del sistema cardiovascular representando en tres dimensiones
los patrones de flujo sanguíneo en el tiempo y cuantificando variables hemodinámicas. En este
trabajo describimos la técnica 4D Flow en un equipo de resonancia de 3 T y adicionalmente se
exponen, además de los parámetros técnicos, las ventajas, las limitaciones y las posibles apli-
caciones clínicas. Para esto estudiamos a diez voluntarios con la técnica 4D Flow en diferentes
áreas corporales (tórax, abdomen, cuello y cráneo) con la que obtuvimos representaciones
� Please cite this article as: Pineda Zapata JA, Delgado de Bedout JA, Rascovsky Ramírez S, Bustamante C, Mesa S, Calvo Betancur VD.Introducción práctica al análisis hemodinámico del sistema cardiovascular mediante la técnica «4D Flow». Radiología. 2014;56:485---495.
∗ Corresponding author.E-mail address: [email protected] (J.A. Pineda Zapata).
2173-5107/© 2013 SERAM. Published by Elsevier España, S.L.U. All rights reserved.
Documento descargado de http://www.elsevier.es el 02/08/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

486 J.A. Pineda Zapata et al.
tridimensionales de los patrones del flujo y medidas cuantitativas hemodinámicas. La técnica
permite evaluar los patrones de flujo sanguíneo en vasos grandes y medianos sin la necesidad
de contrastes exógenos.
© 2013 SERAM. Publicado por Elsevier España, S.L.U. Todos los derechos reservados.
Introduction
During the last years we have seen important innovationsin magnetic resonance images (MRI), especially in the fieldof cardiovascular imaging; this means that today not onlythe anatomical study but also the functional study of heartand vessels is possible. The very first maps of in vivo vascu-lar velocities were reported back in the early 1980s1 andsince then angioresonance sequences like phase contrastangiography (PCA)---consisting of 2D retrospective acquisi-tions with the cardiac cycle (2D cine PCA) are availablein most MRI equipments. This sequence is essential for thefunctional evaluation of the cardiovascular system and it canbe acquired during one apnea only.2
The time-resolved three-dimensional flow-sensitive MRIwith three-directional velocity encoding (4D Flow) modalityconsists of MRI acquired though a phase contrast angiographythat acquires blood flow data in three (3) spatial directions(3D) during the whole cardiac cycle3 for the qualitative andquantitative evaluation of vascular hemodynamics.4 In thiscase acquisition lasts more (5---20 min) and it is necessaryto synchronize it with breathing. With 4D Flow data we canboth see and analyze quantitatively blood flow patternsin heart and large vessels through 3D cine representa-tions during the whole cardiac cycle by means of pathlines,streamlines, vector graphics and 3D velocities. It also allowsus to perform hemodynamic measurements of mid, peakand minimum velocities, ejection volumes, vessel wall shearforces and pressure gradients.5 Given it is a 3D modalityamong the multiples advantages of 4D Flow the possibilityof quantifying the flow in any interesting views and vesselsby postprocessing images is included when the patient isno longer in the resonance equipment without the needfor any more sequences in other views as it happens withthe 2D cine PCA. Also 4D Flow is a modality that does notuse any ionizing radiation or contrast media.6,7 Its clinicalpotential is enormous because it allows us to perform theanatomic and hemodynamic evaluation of the patient’s ves-sels with cardiac or cardiovascular diseases like: congenitalheart diseases, heart failure, arteriovenous malformations,aneurysms, fistulas or stenoses in blood vessels, amongothers.
In this review we will describe the 4D Flow modality in ten(10) volunteers through a 3T MRI and we will be discussingthe advantages, limitations and possible clinical alterations.
Principles of the 2D cine PCA
The 2D cine PCA is an MRI modality synchronized with theelectrocardiogram (ECG) that delivers phase contrast images
velocity-sensitive. 2D cine PCA images are acquired in dif-ferent stages of the cardiac cycle (retrospective acquisition)and they can be seen dynamically. Their main goal is toevaluate hemodynamic parameters like flows, volumes, andvelocities.
Flow is quantified by measuring spin-echo transversemagnetization in two (2) different time frames after apply-ing one bipolar pulsed magnetic field gradient with a positive«lobule» followed by a negative one of the same magnitudebut different direction. The coding of blood velocity in anyspatial directions is based on the phase difference betweenthe moving spin transverse magentization vector and staticspins.8,9 This is possible due to the fact that the static spinsdo not accumulate phase difference because when theyexperience the positive gradient they rotate to a certainangle and when they experience the negative gradient theyrotate to the same angle but in a different direction. Thismeans that the net phase displacement is zero. However,moving spins accumulate phase difference due to the factthat the intensity experienced by the positive and negativegradients is not the same due to movement and change ofposition (Fig. 1). The phase difference angle is directly pro-portional to both the velocity and movement of the spins.10
It is important to highlight that the maximum veloc-ity detected is determined by the Velocity Encodingparameter---expressed in cm/s. Blood flow velocities beyondthis parameter are coded erroneously, so aliasing9 occurs.With the data acquired magnitude and phase images arebuilt (Fig. 2) through the complex difference and the phasedifference of the transverse magnetization vectors.11
4D Flow
The 2D cine PCA modality can be extended to the 3D spatialacquisition in an effort to code the blood flow in the three (3)directions of Cartesian coordinate system in different phasesof the cardiac cycle. Because we need three (3) directionsfor flow coding we need four (4) sequences---three (3) thatare sensitive to velocity and one (1) reference sequence thetotal acquisition time is longer than with 2D modality. Thismodality is known as 4D Flow since it is named after four (4)dimensions---three (3) spatial dimensions plus a 4th temporaldimension.
4D Flow images allow us to quantitatively evaluatethe regional and global dynamics of blood flow throughhemodynamic measurements like the average, maximumand minimum velocities, the average beat flow, regurgitantand progressive flows, ejection volumes and mathematicalapproximations to pressure gradients and shear forcesin the vessel walls. It also allows us to analyze quanti-tatively the temporal evolution of the complex patterns
Documento descargado de http://www.elsevier.es el 02/08/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Hemodynamic analysis of the cardiovascular system with 4D Flow MRI 487
Time 1 Time 2
Flow* *
Bipolar
gradient
Magnetic
field
Spin
mismatch
Static
spin
Static
spin
Moving
spin
Moving
spin
Figure 1 Velocity coding principle in 2D cine PCA images. In time 1 a positive gradient is applied resulting in a phase displacement
that is the same both for the static (circle without asterisk) and mobile spin (circle with asterisk). In time 2 a gradient of the same
magnitude but different opposed to the 1st one is applied. It is now that the mobile spin has been displaced from its original
position while perceiving a different gradient magnitude from the static spin. After the application of the bipolar gradient the
result is that static spin phase between time 1 and time 2 is zero; however, the mobile spin rotates different angles in two (2) times
and consequently accumulates a phase proportional to the velocity and distance gone by.
of blood flow through streamlines, pathlines, 3D velocitycharts, and vectors; representations that describe bloodtrajectory across the cardiovascular system.12---14
At the beginning this modality was known thanks to itscapacity to give qualitative information through the 3D rep-resentation of cardiovascular flow. However, recently with4D Flow some methods have been developed for the quan-titative analysis of blood flow. Also the new technologicaladvancements in both hardware and software allow us to
reduce the sequence time of acquisition and apply it in theclinical setting.13
Technique of acquisition
For the gathering of time-based volumetric data combinedwith velocity coding data in the three (3) spatial direc-tions we use k-space segmentation methods synchronized
Figure 2 2D cine PCA axial images at the level of the pulmonary artery bifurcation. (A) Magnitude image. Blood vessel anatomic
information. (B) Phase image. Blood velocity is coded through the intensity of pixels---bright color meaning flow coming out of the
image and dark color meaning flow coming in.
Documento descargado de http://www.elsevier.es el 02/08/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

488 J.A. Pineda Zapata et al.
TECG
Bipolar gradient
in the x-axis
Bipolar gradient
in the y-axis
Bipolar gradient
in the z-axis
Reference Flow coding
in x
Flow coding
in y
Flow coding
in zKy
KxKz
Nsec
Magnitude image Phase images
Figure 3 Image acquisition scheme through the 4D Flow MRI modality. For each phase (�t) of the cardiac cycle (synchronized
with the ECG signal) four (4) different sets of 3D data are collected---one (1) reference set of data and three (3) sets of data to code
flow. After data acquisition the phase image reconstruction is performed with the existing phase difference between the reference
data and the phase codification data for every direction. The magnitude image is reconstructed through a complex difference. This
figure from left to right shows both the magnitude image and velocity images in the x-, y-, z-axes, respectively.
with the ECG signal---for a total description the reader canuse the quote.15 The Cartesian segmentation method usesthe k-space with its three (3) perpendicular axes (kx, ky,kz) and divides it into a 3D matrix (Nx, Ny, Nz). Then dur-ing each beat of the heart it acquires a set of single-cutk-space lines (Nseg) for all phases of the cardiac cycle.4,16 IfNy represents the lines all across the phase image (ky-axis)and Nz represents the cuts (kz-axis) the acquisition of thewhole 3D volume will last for a certain number of beats equalto NyNz/Nseg and a time equal to Tadq = (NyNz/Nseg)TECG,where Tadq is the duration of all acquisition and TECG isthe duration of a single beat. For every line of k-spacefour (4) different data need to be gathered: one referenceacquisition and three (3) velocity codifications resultingfrom the application of bipolar gradients in the x, y, z
directions.4,16 After the gathering of data the 3D imagesare reconstructed---including one (1) anatomic or magni-tude image and three (3) phase images representing bloodvelocity in the three (3) axes of the coordinate system(Fig. 3).
Image acquisition
We studied 10 volunteers (9 healthy ones and one with atransplanted kidney) using a Philips Ingenia 3T kit (PhilipsHealthcare, Eindhoven, The Netherlands) with 4D Flowin some of the following body areas: chest, abdomen, neckand skull. Acquisition parameters can be seen in Table 1. Weproceeding with free breathing, electrocardiographic syn-chronization and a chest, head, or neck cardiac coil basedon the examination area. Also in certain volunteers 2D cinePCA with parameters of temporal resolution similar to thoseof 4D Flow were acquired.
Image processing
Obtained data were extracted in RAR-REC format andpostprocessing was performed using the GTFlow software(Gyrotools LLC, Zurich, Switzerland) that allowed us to esti-mate each point, blood velocity in the three (3) spatial
Documento descargado de http://www.elsevier.es el 02/08/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Hemodynamic analysis of the cardiovascular system with 4D Flow MRI 489
Table 1 Acquisition parameters for the 4D Flow modality based on the area of study.
Thorax Abdomen Neck and skull
Field of view (mm) 350 × 350 × 120 350 × 350 × 120 270 × 270 × 70
Voxel size (mm) 2.5 × 2.5 × 5 2.5 × 2.5 × 5 1.5 × 1.5 × 1.5
Images 48---56 40---50 40---60
RT (ms)/ET (ms) 4/2.1 4/2.1 4/2.1
Venc (cm/s) 200---150 100 110---160
SENSE (factor) 2 2 2
Angle of inclination (◦) 6 6 6
Phases 16 20 16
ET, echo time; RT, repetition time; Venc, velocity encoding.
directions and in all phases of cardiac cycle. Postprocessis detailed in the three (3) simplified steps shown in Fig. 4.
Additionally the following hemodynamic variables wereestimated in different vessels: ejected volume, averagevelocity, maximum and minimum velocity17 by picking out2D regions of interest from one (1) automatic edge detectionalgorithm.
Methods of representation
4D Flow data are commonly viewed as streamlines, path-lines, vector charts and 3D meshes that allow us to represent3D blood flow patters in time.18 In Fig. 5 the differentkinds of 3D representation that can be obtained through thismodality can be seen.
1. Streamlines. Streamlines are curves that connectelements (particles) of a fluid in space with the charac-teristic that the curve is tangential to the velocity vectorof several particles in a given time. This is why stream-lines give us a general view of the flow pattern describedby a fluid element in the cardiac cycle.19
2. Pathlines. Pathlines indicate the trajectory followed byone particle of fluid. This representation can be regardedas the pathway followed by one fluid element within theflow at a given time. Pathlines are used to analyzethe temporal evolution of blood flow patterns during the
cardiac cycle. They can be coded with colors represent-ing flow velocity too.20
3. Vector charts and meshes. For every particle vectorscharts associate one vector with the magnitude anddirection of flow velocity at that point so that for everypoint the evolution of the flow velocity pattern canbe observed through time. You can also draw regionsof interest in any vessels in order to analyze the behav-ior of blood flow through any of the aforementionedmethods. You can also build 3D meshes to get profileinformation of blood flow velocity on one vessel or regionif interest.
Artifacts and difficulties
Phase contrast images are susceptible to errors inducedby eddy currents and other heterogeneities of the mag-netic field21 that have a tendency to increase as thestudied region moves away from the magnetic isocen-ter. Aliasing can occur since the velocity encoding (Venc)sampling is lower than blood velocity. It is important tocorrect data when these artifacts show up in order toguarantee the vision and quantification of flow.4,7,9 To pre-vent these artifacts from happening due to aliasing theuse of one 2D cine PCA sequence is recommended andbased on the estimated peak blood velocity the pick-ing of the most adequate value for Venc in the 4D Flow
Figure 4 4D Flow image postprocessing. Firstly the vascular structures in the magnitude image were segmented by choosing an
appropriate intensity threshold and secondly a 3D isosurface was created based on the maximum velocity data included in the
segmentation. Finally the vessel isosurface was used to generate a certain number of seeds (particles) inside the isosurface that
were used to estimate the streamlines, the pathlines and the 3D vector charts and meshes.
Documento descargado de http://www.elsevier.es el 02/08/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

490 J.A. Pineda Zapata et al.
A B
DC
Velocity (cm/s)
100.0
83.3
66.7
50.0
33.3
16.7
0.0
Velocity (cm/s)
100.0
83.3
66.7
50.0
33.3
16.7
0.0
Velocity (cm/s)
100.0
83.3
66.7
50.0
33.3
16.7
0.0
Velocity (cm/s)
100.0
83.3
66.7
50.0
33.3
16.7
0.0
Figure 5 3D view methods of the aorta. 4D Flow images. (A) The streamlines give a 3D perspective of the movement of blood
at the vascular structures. (B) The pathlines give us information on the trajectory, velocity, direction, and evolution of blood flow
patters in every phase of cardiac cycle. (C) Vector charts show the magnitude of velocity and direction for every particle inside the
flow in a 2D view. At the image both the aorta and pulmonary trunk are shown. (D) Representation of the profile of blood velocity
in the ascending and descending aorta through two (2) 3D meshes.
acquisition always bearing in mind that a high Venc elim-inates artifacts due to aliasing but it also limits the lowvelocity-flow sensitivity.22,23 When it comes to artifactscaused by respiratory motion there are several compen-sation modalities by using sensors (navigators) capable ofdetecting the patient’s respiration through the diaphrag-matic motion while synchronizing such respiration with 4DFlow acquisition.4,7,24,25
The main setback of 4D Flow is the duration of 4DFlow acquisition sequences---time especially increases whenmore spatial and temporal resolution is needed or sim-ply when the acquired volume is increased. To solve thisproblem there are speed-up methods including parallelimages, sampling strategies exploring the correlations in thespace---time domain and radial acquisitions of k-space.26---28
These modalities can produce overlapping artifacts orreduce the temporal resolution of images. Some of thesestrategies are currently under investigations and valida-tion.
The difficulty of clinically applying 4D Flow is dueto both the time of sequence acquisition and itscomplexity. However, both scientific investigation and theinterest of the industry on MRIs predict a bright future forthis modality.
Applications of the 4D Flow modality
The 4D Flow modality allows us to assess blood flowboth quantitatively and qualitatively in any vessels ofinterest and without any means of contrast. It allowsus to assess the heart large vessels, its ventricles andvalves in systole and diastole in one acquisition only. Alsothanks to 3D acquisition it allows us to select withinthe acquired volume 2D views through any angles. Simi-larly and based on the area of interest abdominal, neck,and skull vessels can be assessed among other vascularstructures.29---31
Documento descargado de http://www.elsevier.es el 02/08/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Hemodynamic analysis of the cardiovascular system with 4D Flow MRI 491
A B C
Velocity (cm/s)
100.0
80.0
60.0
40.0
20.0
0.0
Velocity (cm/s)
100.0
80.0
60.0
40.0
20.0
0.0
Velocity (cm/s)
98.0
81.7
65.3
49.0
32.7
0.0
16.3
528.00 ms
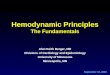
Figure 6 4D Flow images in large vessels and heart. (A) Segmentation of aorta and representation of blood flow through pathlines.
(B) View of blood trajectory in the aortic arch and the pulmonary artery in one healthy volunteer. (C) Heart ventricular filling in
diastole.
To better illustrate the capacity of quantitative analysisthis modality has the videos that can be seen in files 4D Flow
1 and 4D Flow 2.
1. Aorta and heart (Fig. 6). One of the various potentialclinical applications of 4D Flow is the study of flow inthe ascending aorta. Hope et al.31 evaluated one sub-group of patients with bivalve aortas and found withinthis group an eccentric abnormal blood flow associatedwith major shear forces in the vessel walls as well asa greater risk of aneurysms. Consequently the risk ofaneurysm in patients with bivalve aorta can be strati-fied by quantifying the shear forces obtained through 4DFlow, which allows more objectivity both in the diagnosisand possible interventions in the ascending aorta of thesepatients. Also possibly though 4D Flow we will be able toquantify both the abnormal flow and the hemodynamicload; define the risk of vascular diseases like aneurysmsor dissections before developing symptoms.31
The 4D Flow modality will possibly be useful in numer-ous clinical situations associated with congenital thoraciccardiovascular anomalies like persistent arterial ductus,conotruncal anomalies like the Fallot tetralogy, par-tial or total anomalous pulmonary venous returns andin patients with left-to-right shunting. Also with thismodality we can identify patients at risk of pulmonaryhypertension and further development of Eisenmengesyndrome.32 Similarly the MRI is the postoperative chosenmodality since it allows us to assess both anatomic andfunctionally the cardiac cavities and the integrity andfunctionality of surgical corrections like interatrial baf-fles, outflow septostomies and Fontan conduits, amongothers. This is why 4D Flow images have a greater clin-ical value because they give us information of bothintra and extra cardiac blood flow patterns in thesesituations.17,33
2. Abdomen.The Doppler ultrasound has been the lessinvasive modality for the study of blood flows and thequantification of hemodynamic parameters in the venacava, the portal system and vascular diseases (Fig. 7).However, it can be greatly affected by factors suchas obesity, intestinal air or edema. This is why the
MR-angiography is more and more important---because itdoes an excellent anatomical evaluation. Markl et al.4
published their results showing the potentiality of the4D Flow modality both for the quantification and charac-terization of blood flow of the different intra-abdominalvascular structures and in some pathological situationslike portal hypertension.34
In patients with renal transplant the MRIs can be veryuseful because they give us important information likeperfusion defects, tumors, post-transplant proliferativeconditions and collections, among others. Through the4D Flow modality we will be able to evaluate the size,orientation and relation to other abdominal organs andintegrity of the intra-renal vascular structures. It is alsopossible to evaluate the anastomoses of the renal arteryto the iliac artery and of the renal vein to the iliac veinwhile watching and quantifying blood flow through theseanastomoses (Fig. 7).4
3. Carotid and cerebral arteries. The digital subtractionangiography is the chosen method to evaluate neck andintra-cranial arteries but it is also an invasive methodrequiring iodinated contrast media. Thus techniqueslike CT-angiography (with iodinated contrast too though)and MR-angiography are more and more important forthe study of carotid and cerebral arteries. The carotidDoppler is a very valuable low cost-tool thanks to itsgreat accuracy for the study of carotid bifurcationsyet, it is limited to small fields, it depends on theoperator and is sensitive to a poor acoustic window.The 4D Flow modality has all the characteristics of theaforementioned methods while giving us anatomic andhemodynamic information (Fig. 8). It allows us to assessthe vascular structures of the neck and the distributionof the carotid walls shear forces, find carotid stenosesand quantify blood velocity in the common carotidartery and the carotid bifurcation.35 It is also useful toevaluate and quantify both flow and velocity patternsin aneurysms and intra- and extra-cranial arteriovenousmalformations.36---38 Studies performed in 7 T ultra-highmagnetic field resonance imaging devices have shownthat smaller caliber-vessels can adequately be assessed(e.g. the posterior cerebral artery) and their pulsatility
Documento descargado de http://www.elsevier.es el 02/08/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

492 J.A. Pineda Zapata et al.
Velocity (cm/s)
100.0
80.0
60.0
40.0
20.0
0.0
Velocity (cm/s)
100.0
80.0
60.0
40.0
20.0
0.0
Velocity (cm/s)
100.0
80.0
60.0
40.0
20.0
0.0
292.40 ms
Velocity (cm/s)
100.0
80.0
60.0
40.0
20.0
0.0
A CB
D E F
Figure 7 4D Flow images in abdominal vessels and in one patient with a renal transplant. (A) Healthy volunteer. Abdominal
aorta, main efferent branches and main intra-abdominal venous structures. (B) Detail from the origin of the celiac trunk, the
superior mesenteric artery and the portal vein. (C) Saggital image with anatomic reference of the abdominal aorta and some of
its main branches. (D) Patients with a renal transplant. Coronal view where 3D streamlines of the vascular structures irrigating the
transplanted kidney can be seen. (E) Detail of the arterial (caudal vessel) and venous flow (celiac vessel) and blood velocity coded
based on a scale of colors. (F) Pathlines of former case.
A B C
Velocity (cm/s)
6.7
40.0
20.0
0.0
13.3
26.7
33.3
Velocity (cm/s)
6.7
40.0
20.0
0.0
13.3
26.7
33.3
Velocity (cm/s)
100.0
40.0
0.0
20.0
60.0
80.0
Figure 8 Blood flow patterns at the main cerebral arteries and neck. (A) 4D Flow of the carotid and vertebrobasilar system of one
healthy volunteer performed in 3T. Color patterns are coded according to velocity. (B) View through pathlines at the bifurcation of
the right carotid and vertebral arteries. (C) Velocity patterns at the right carotid vertebral arteries showing greater peak velocity
in the carotid artery. Note the parabolic profiles so characteristic of laminar flow in both arteries.
Documento descargado de http://www.elsevier.es el 02/08/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Hemodynamic analysis of the cardiovascular system with 4D Flow MRI 493
A
B
C70.0
60.0
50.0
40.0
30.0
20.0
10.0
0.0
–10.0
0 100 200 300 400 500 600 700 800 900
Time (ms)
70.0
60.0
50.0
40.0
30.0
20.0
10.0
0.0
–10.0
0 100 200 300 400 500 600 700 800 900
Time (ms)
Avera
ge v
elo
city (
cm
/s)
Avera
ge v
elo
city (
cm
/s)
cm/s
50
40
30
20
10
1 3 5 7 9 11 13 15
1 3 5 7 9 11 13 15
50
40
30
20
10
Vavg XYZ
Vavg XYZ
cm/s
Velocity (cm/s)
100.0
80.0
60.0
40.0
20.0
0.0
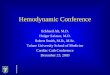
Figure 9 4D Flow and 2D PCA. (A) Quantification of the average velocity of flow in the ascending aorta through the 2D cine PCA
modality. To the left we can see flow direction for every vessel and to the right the chart of velocity values in the cardiac cycle.
(B) The same quantification was performed with 4D Flow. Note the similarity of values of the average velocity of blood measured
through 2D cine PCA and 4D Flow modalities (B). (C) Selection of the ascending aorta and the pulmonary artery in one single 4D
Flow study. The charts of average velocity of aorta (up) and pulmonary artery blood (down) are shown here as well. In charts A and
B y-axis is blood velocity (cm/s) while x-axis is time (s). However, in chart C x-axis represents the cardiac cycle divided into sixteen
(16) different phases.
index be measured which can be applied in processeslike trigeminal neuralgia.39
4D Flow and 2D cine PCA
Today 2D cine PCA is widely used for the study of blood flowin cardiovascular MRIs. However, its main setback is thatis uses 2D cut views that need to be selected during theexamination and require a highly skilled operator managingthe resonance equipment. In contrast in the 4D Flow modal-ity the whole heart is 3D volume-studied, so the planningof the sequence is greatly simplified without contributionfrom the operator (Fig. 9). However, the greater advantageof the 4D Flow modality lies in its capacity to perform mul-tiplanar image analyses in the postprocessing since it allowsthe quantification of blood flow in any arbitrary views andangles without the need for acquiring new images. Otherthan measuring flow and velocity it also allows us to esti-mate hemodynamic biomarkers such as shear stress in theblood vessel walls, pressure gradients and pulse wave veloc-ity without the use of any venous contrast media.40,41
Some studies have confirmed that the 4D Flow mea-surements of flow and velocity strongly correlate to thatof 2D cine PCA.42,43 On the other hand these modalitieshave a tendency to underestimate 20---25% of the maximumvelocity or average systolic peak observed through Dopplerultrasound.35 However, we need to understand that in theMRIs velocity is always averaged since both multiple car-diac beats and a greater voxel size are needed to be ableto obtain 3D images which in turn translates into a lowertemporal and spatial resolution than that of Doppler ultra-sound. When the resolution of the 4D Flow sequence is veryhigh only those voxels displaying the fastest velocity willshow values more proximal to that of Doppler ultrasound.
Conclusion
In this review the 4D Flow modality is shown to be valid,non-invasive and allowing us to perform quantitative andqualitative analyses of blood flow in large and medium-size vessels without the need for exogenous contrasts. Thismodality has a great clinical potential since it gives uscomplete morphologic and anatomical information on thecardiovascular system by estimating hemodynamic biomark-ers and visualizing blood flow patterns.
Conflict of interests
The authors reported no conflicts of interests.
Ethical responsibilities
Protection of people and animals. Authors confirm that noexperiments have been performed on human beings or ani-mals.
Data confidentiality. Authors confirm that the protocols oftheir centers have been followed on matters concerning thepublishing of data from patients. They also confirm that allpatients included in this study have been given enough infor-mation and handed over their written informed consent fortheir participation in this study.
Right to privacy and informed consent. Authors confirmthat in this report there are no personal data of patients.
Documento descargado de http://www.elsevier.es el 02/08/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

494 J.A. Pineda Zapata et al.
Authors/collaborators
1. Manager of the integrity of the study: JAPZ, JADB, SRR.2. Original idea of the study: JAPZ, JADB, SRR.3. Study design: JAPZ, VDCB, CBA, SMV.4. Data mining: JAPZ, CBA.5. Data analysis and interpretation: JAPZ, VDCB, CBA, SMV.6. Statistical analysis: VDCB.7. Reference search: CBA, SMV.8. Writing: JAPZ, VDCB, SMV, CBA, JADB, SRR.9. Manuscript critical review with intellectually relevant
contributions: JADB, SRR.10. Final version approval: JAPZ, VDCB, SMV, CBA, JADB,
SRR.
Appendix A. Supplementary data
Supplementary data associated with this article can befound, in the online version, at http://dx.doi.org/10.1016/j.rxeng.2014.08.001.
References
1. O’Donnell M. NMR blood flow imaging using multiecho, phasecontrast sequences. Med Phys. 1985;12:59---64.
2. Bolen MA, Setser RM, Gabriel RS, Renapurkar RD, Tandon Y,Lieber ML, et al. Effect of protocol choice on phase contrastcardiac magnetic resonance flow measurement in the ascend-ing aorta: breath-hold and non-breath-hold. Int J CardiovascImaging. 2013;29:113---20.
3. Wheaton AJ, Miyazaki M. Non-contrast enhanced MRangiography: physical principles. J Magn Reson Imaging.2012;36:286---304.
4. Markl M, Frydrychowicz A, Kozerke S, Hope M, Wieben O. 4Dflow MRI. J Magn Reson Imaging. 2012;36:1015---36.
5. Isoda H, Ohkura Y, Kosugi T, Hirano M, Alley MT, Bammer R,et al. Comparison of hemodynamics of intracranial aneurysmsbetween MR fluid dynamics using 3D cine phase-contrast MRIand MR-based computational fluid dynamics. Neuroradiology.2010;52:913---20.
6. Valverde I, Simpson J, Schaeffter T, Beerbaum P. 4Dphase-contrast flow cardiovascular magnetic resonance: com-prehensive quantification and visualization of flow dynamics inatrial septal defect and partial anomalous pulmonary venousreturn. Pediatr Cardiol. 2010;31:1244---8.
7. Markl M, Kilner PJ, Ebbers T. Comprehensive 4D velocity map-ping of the heart and great vessels by cardiovascular magneticresonance. J Cardiovasc Magn Reson. 2011;13:7.
8. Srichai MB, Lim RP, Wong S, Lee VS. Cardiovascular applica-tions of phase-contrast MRI. AJR Am J Roentgenol. 2009;192:662---75.
9. Lotz J, Meier C, Leppert A, Galanski M. Cardiovascular flowmeasurement with phase-contrast MR imaging: basic facts andimplementation. Radiographics. 2002;22:651---71.
10. Firmin D. Blood flow velocity assessment. In: Manning WJ, Pen-nell DJ, editors. Cardiovascular magnetic resonance. 2nd ed.Philadelphia, PA: Saunders; 2010. p. 91---9.
11. Bernstein MA. Angiographic pulse sequences. In: Bernstein MA,King KF, Zhou XJ, editors. Handbook of MRI pulse sequences.Burlington: Academic Press; 2004. p. 648---701.
12. Markl M, Chan FP, Alley MT, Wedding KL, Draney MT, ElkinsCJ, et al. Time-resolved three-dimensional phase-contrast MRI.J Magn Reson Imaging. 2003;17:499---506.
13. Ebbers T. Flow imaging: cardiac applications of 3D cine phase-contrast MRI. Curr Cardiovasc Imaging Rep. 2011;4:127---33.
14. Sigfridsson A, Petersson S, Carlhäll CJ, Ebbers T. Four-dimensional flow MRI using spiral acquisition. Magn Reson Med.2012;68:1065---73.
15. Moratal-Pérez D, Martí-Bonmatí L, Brummer ME, Millet-Roig J,Castells F. Surcando el espacio-k para mejorar la imagen porresonancia magnética. Radiología. 2004;46:133---50.
16. Walker PG, Cranney GB, Scheidegger MB, Waseleski G, PohostGM, Yoganathan AP. Semiautomated method for noise reduc-tion and background phase error correction in MR phase velocitydata. J Magn Reson Imaging. 1993;3:521---30.
17. Bächler P, Pinochet N, Sotelo J, Crelier G, Irarrazaval P, TejosC, et al. Assessment of normal flow patterns in the pulmonarycirculation by using 4D magnetic resonance velocity mapping.Magn Reson Imaging. 2013;31:178---88.
18. Som SK, Biswas G. Kinematics of fluido. Introduction to fluidmechanics and fluid machines. 2nd ed. New Delhi: Tata McGraw-Hill; 2007. p. 78---107.
19. Napel S, Lee DH, Frayne R, Rutt BK. Visualizingthree-dimensional flow with simulated streamlinesand three-dimensional phase-contrast MR imaging. J MagnReson Imaging. 1992;2:143---53.
20. Wigström L, Ebbers T, Fyrenius A, Karlsson M, Engvall J,Wranne B, et al. Particle trace visualization of intracardiac flowusing time-resolved 3D phase contrast MRI. Magn Reson Med.1999;41:793---9.
21. Lorenz R, Bock J, Snyder J, Korvink JG, Jung BA, Markl M. Influ-ence of eddy current, Maxwell and gradient field corrections on3D flow visualization of 3D CINE PC-MRI data. Magn Reson Med.2014;72:33---40.
22. Stadlbauer A, van der Riet W, Crelier G, Salomonowitz E. Accel-erated time-resolved three-dimensional MR velocity mapping ofblood flow patterns in the aorta using SENSE and k-t BLAST. EurJ Radiol. 2010;75:e15---21.
23. Pinochet N, Bãchler P, Tejos C, Crelier G, Parra R, Allendes JM,et al. 4D FLOW: una nueva herramienta de diagnóstico paracardiopatías congénitas. Rev Chil Radiol. 2011;17:134---40.
24. Uribe S, Beerbaum P, Sørensen TS, Rasmusson A, Razavi R, Scha-effter T. Four-dimensional (4D) flow of the whole heart andgreat vessels using real-time respiratory self-gating. Magn ResonMed. 2009;62:984---92.
25. Markl M, Bammer R, Alley MT, Elkins CJ, Draney MT, Barnett A,et al. Generalized reconstruction of phase contrast MRI: analysisand correction of the effect of gradient field distortions. MagnReson Med. 2003;50:791---801.
26. Thunberg P, Karlsson M, Wigström L. Accuracy and reproducibil-ity in phase contrast imaging using SENSE. Magn Reson Med.2003;50:1061---8.
27. Baltes C, Kozerke S, Hansen MS, Pruessmann KP, Tsao J, BoesigerP. Accelerating cine phase-contrast flow measurements using k-tBLAST and k-t SENSE. Magn Reson Med. 2005;54:1430---8.
28. Pedersen H, Kozerke S, Ringgaard S, Nehrke K, Kim WY. k-t PCA:temporally constrained k-t BLAST reconstruction using principalcomponent analysis. Magn Reson Med. 2009;62:706---16.
29. Lorenz R, Bock J, Barker AJ, von Knobelsdorff-BrenkenhoffF, Wallis W, Korvink JG, et al. 4D flow magnetic resonanceimaging in bicuspid aortic valve disease demonstrates altereddistribution of aortic blood flow helicity. Magn Reson Med.2014;71:1542---53.
30. Frydrychowicz A, Markl M, Hirtler D, Harloff A, SchlensakC, Geiger J, et al. Aortic hemodynamics in patients withand without repair of aortic coarctation: in vivo analysis by4D flow-sensitive magnetic resonance imaging. Invest Radiol.2011;46:317---25.
31. Hope MD, Hope TA, Crook SE, Ordovas KG, Urbania TH, AlleyMT, et al. 4D flow CMR in assessment of valve-related ascendingaortic disease. JACC Cardiovasc Imaging. 2011;4:781---7.
Documento descargado de http://www.elsevier.es el 02/08/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Hemodynamic analysis of the cardiovascular system with 4D Flow MRI 495
32. Reiter U, Reiter G, Kovacs G, Stalder AF, Gulsun MA, GreiserA, et al. Evaluation of elevated mean pulmonary arterialpressure based on magnetic resonance 4D velocity mapping:comparison of visualization techniques. PLOS ONE. 2013;8:e82212.
33. Geiger J, Hirtler D, Bürk J, Stiller B, Arnold R, Jung B, et al. Post-operative pulmonary and aortic 3D haemodynamics in patientsafter repair of transposition of the great arteries. Eur Radiol.2014;24:200---8.
34. Roldán-Alzate A, Frydrychowicz A, Niespodzany E, Landgraf BR,Johnson KM, Wieben O, et al. In vivo validation of 4D flow MRIfor assessing the hemodynamics of portal hypertension. J MagnReson Imaging. 2013;37:1100---8.
35. Harloff A, Zech T, Wegent F, Strecker C, Weiller C, Markl M.Comparison of blood flow velocity quantification by 4D flow MRimaging with ultrasound at the carotid bifurcation. AJNR Am JNeuroradiol. 2013;34:1407---13.
36. Ansari SA, Schnell S, Carroll T, Vakil P, Hurley MC, WuC, et al. Intracranial 4D Flow MRI: Toward individualizedassessment of arteriovenous malformation hemodynamics andtreatment-induced changes. AJNR Am J Neuroradiol. 2013;34:1922---8.
37. Hope MD, Purcell DD, Hope TA, von Morze C, Vigneron DB, AlleyMT, et al. Complete intracranial arterial and venous blood flowevaluation with 4D flow MR imaging. AJNR Am J Neuroradiol.2009;30:362---6.
38. Frydrychowicz A, Francois CJ, Turski PA. Four-dimensional phasecontrast magnetic resonance angiography: potential clinicalapplications. Eur J Radiol. 2011;80:24---35.
39. Schmitter S, Jagadeesan BD, Grande AW, Sein J, Ugurbil K, Vande Moortele P. 4D flow measurements in the superior cerebellarartery at 7 Tesla: feasibility and potential for applications inpatients with trigeminal neuralgia. J Cardiovasc Magn Reson.2013;15 Suppl. 1:W21.
40. Harloff A, Nussbaumer A, Bauer S, Stalder AF, Frydrychowicz A,Weiller C, et al. In vivo assessment of wallshear stress in theatherosclerotic aorta using flow-sensitive 4D MRI. Magn ResonMed. 2010;63:1529---36.
41. Wentland AL, Wieben O, Francois CJ, Boncyk C, Munoz delRio A, Johnson KM, et al. Aortic pulse wave velocity measure-ments with under sampled 4D flow-sensitive MRI: comparisonwith 2D and algorithm determination. J Magn Reson Imaging.2013;37:853---9.
42. Hsiao A, Alley MT, Massaband P, Herfkens RJ, Chan FP,Vasanawala SS. Improved cardiovascular flow quantificationwith time-resolved volumetric phase-contrast MRI. PediatrRadiol. 2011;41:711---20.
43. Brix L, Ringgaard S, Rasmusson A, Sørensen TS, Kim WY.Three dimensional three component whole heart cardiovascu-lar magnetic resonance velocity mapping: comparison of flowmeasurements from 3D and 2D acquisitions. J Cardiovasc MagnReson. 2009;11:3.
Documento descargado de http://www.elsevier.es el 02/08/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.