Embed Size (px)
Citation preview


Pre-operative CHO Pre-operative CHO loading an integral loading an integral component of peri-component of peri-
operative careoperative care- Only the Beginning-- Only the Beginning-


Response to Surgery and Response to Surgery and FastingFasting
SurgerySurgery FastingFasting Endocrine responseEndocrine response
GlucagonGlucagon
InsulinInsulin Metabolic responseMetabolic response
Glycogen breakdownGlycogen breakdown
Protein breakdownProtein breakdown
LipolysisLipolysis Insulin resistanceInsulin resistance
Fasting further increases metabolic response to surgery
Insulin resistance is a useful metabolic marker

IL1bTNFaIL6
Immune cells activated
Cytokines produced
Muscle mobilised LBM
Appetite Reduced
Effects of Cytokines on Nutritional Status
Altered fuel mix
Gluconeogenisis
lipolysis
Fat mobilised
WEIGHT LOSS
SURGERYSURGERY

Traditional Traditional
FastingPatient involvement – passive

Traditional Post-opTraditional Post-op Opiate analgesia patient unable to sit up and Opiate analgesia patient unable to sit up and
take fluids for several hours (no fluid pre-take fluids for several hours (no fluid pre-op).op).Also contribute to ileus, N&V.Also contribute to ileus, N&V.
NBM ?3-5/7 NBM ?3-5/7 Further starvationFurther starvationImmobilisationImmobilisation
Patient expectations – Patient expectations – passive in their passive in their carecare
expect to be hospitalised 10/7expect to be hospitalised 10/7lengthy recoverylengthy recovery

Where Are We Where Are We NowNow

Multimodel Strategies to Multimodel Strategies to Improve Surgical OutcomeImprove Surgical Outcome
Dela
yed
Accele
rate
d
• Anxiety/Fear
• Organ dysfunction
• Hypothermia
• Nausea, vomiting, ileus, semi- starvation
• Hypoxemia
• Sleep disturbance
• Drains, NG tubes,catheters
• Patient info• Optimise nutrition
• Modify alcohol/smoking
• Neuraxial blockade
• Laprascopic surgery
• Normothermia
• Nausea and ileus prevention
• Early enteral feeding
• Undisturbed sleep
•Opiate sparing analgesia
Adapted Kehlet, 2000

Patterns of RecoveryPatterns of Recovery
Enhanced Recovery
Traditional Care
Rate
of
Retu
rn o
f F
un
ctio
n
Days Weeks
Adapted Luff,2003

Where are we now –Where are we now –
CHO loading has CHO loading has influenced traditional influenced traditional peri-operative care in peri-operative care in colorectal surgery colorectal surgery
- Fast track peri-operative - Fast track peri-operative care.care.

Fearon et al, 2005 Clin Nut24: 466-467

Insulin Resistance Insulin Resistance Following Elective Following Elective
SurgerySurgery Enhanced by fastingEnhanced by fasting
Symptoms similar to type 2 diabetesSymptoms similar to type 2 diabetes
Reduced by regional anaesthetic and Reduced by regional anaesthetic and minimally invasive techniquesminimally invasive techniques
Related to magnitude of surgery Related to magnitude of surgery
Can remain for about 3 weeksCan remain for about 3 weeks
Associated with length of stayAssociated with length of stay

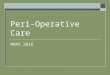
Insulin Resistance and Insulin Resistance and Length of StayLength of Stay
Thorell et al, Curr Opin Clin Nutr Metab Care 1999
Log length of stay (Days)
Pos
t-op
Ins
ulin
sen
sitiv
ity
(
% p
re-o
p)
1.41.21.00.80.60.40.2 0.0-0.20
20
40
60
80
100
R=0.53p<0.0001n=60

Preop CHO loading-Clinical Preop CHO loading-Clinical ResearchResearch
A pre-operative fast is not ideal to prepare a A pre-operative fast is not ideal to prepare a patient for surgical stress since:patient for surgical stress since: it is uncomfortableit is uncomfortable It contributes to an additional catabolic stress It contributes to an additional catabolic stress
and worsens recoveryand worsens recovery Hypothesis: Hypothesis:
The negative effects of pre-operative fasting can The negative effects of pre-operative fasting can be reduced by pre-operative carbohydrate loadingbe reduced by pre-operative carbohydrate loading Improve post-operative insulin sensitivityImprove post-operative insulin sensitivity Reduce post-operative insulin resistanceReduce post-operative insulin resistance Improve patient well being Improve patient well being Improve recovery and reduce length of stayImprove recovery and reduce length of stay

It has been demonstrated that CHO It has been demonstrated that CHO fluids provided 2-3 hours before fluids provided 2-3 hours before induction of anaesthesia induction of anaesthesia
- attenuate early - attenuate early postoperative postoperative metabolic metabolic stress.stress.
- improve insulin resistance.- improve insulin resistance.
- reduce recovery time.- reduce recovery time.
Preoperative oral Preoperative oral carbohydrate carbohydrate
administrationadministration

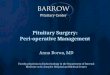
Fast Track vs Fast Track vs Traditional Traditional

Length of Hospital Stay in Length of Hospital Stay in Colorectal SurgeryColorectal Surgery
01
23
45
678
910
Days Stay
TraditionalEnhanced
Len
gth
of
Sta
y
n=48
n=33
**** p>0.01
Fearon and Luff, 2003

Fast Track vs Fast Track vs TraditionalTraditional
n=451 (Traditional n=333 (4 countries), Fast Track n=118 (Denmark))
Retrospective case note review.
Patients underwent laparotomy for colorectal resection.
No difference in morbidity or 30 day mortality between centres.
The median length of stay was 2days in Fast Track and 7-9 days in Traditional (p<0.05).
Readmission rate was 22% in Fast Track cf 2-16% Traditional (p<0.05).
Nygren et al, 2005 Clin Nutr. 24: 455-61

Early Oral Nutrition After Early Oral Nutrition After Elective Colorectal SurgeryElective Colorectal Surgery
Influence of balanced analgesia and Influence of balanced analgesia and enforced mobilisation.enforced mobilisation.
- Mobility significantly improved - Mobility significantly improved (5.5 (5.5 hrs/day vs 1.7 hrs/day).hrs/day vs 1.7 hrs/day).
- Nutritional intake greater.- Nutritional intake greater.
- No significant loss of body - No significant loss of body compositioncomposition
Henriksen et al, 2002 Nutrition18: 263-267

What role the What role the Dietitian ?Dietitian ?

Pre Surgery Pre Surgery DischargeDischarge
Weight
BMI
Anthropometry (TSF/AMC)
800mls placebo/CHOD
2-3hours pre-surgery
400mls placebo/CHOD
Weight
BMI
Anthropometry(TSF/AMC)
LOS
New Approach to Pre-op New Approach to Pre-op Management (n=65)Management (n=65)

Preoperative vs Preoperative vs Discharge BMIDischarge BMI
19
20
21
22
23
24
25
26
Pre-op Discharge
BM
I (k
g/m
)
Placebo
CHOD
2

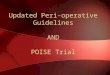
Anthropometry changesAnthropometry changes
-1.6
-1.4
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0
un
it c
han
ge
Placebo
CHOD*
*p<0.05
AMC TSF


Preoperative oral Preoperative oral carbohydrate carbohydrate
administration administration
The provision of utilisable energy can The provision of utilisable energy can minimise the loss of lean body mass.minimise the loss of lean body mass.
What remains to be elucidated is What remains to be elucidated is whether:whether:
This attenuation of lean body mass This attenuation of lean body mass can improve sustainable can improve sustainable improvement of functionimprovement of function

Dietitians taking this Dietitians taking this Forward ?Forward ?
Henriksen Henriksen et al et al (2002) provided 200ml (2002) provided 200ml ONS to intervention group 1day pre-op ONS to intervention group 1day pre-op and 7 days post-op. Assumption made and 7 days post-op. Assumption made that patients compliant.that patients compliant.
Alluded to other factors that may have Alluded to other factors that may have improved intakeimproved intake
- patient involvement- patient involvement
- early mobilisation- early mobilisation

Nutrition as Component Nutrition as Component ERER
As with pharmacological As with pharmacological interventions this nutritional interventions this nutritional approach relies strongly on patient approach relies strongly on patient compliance however the compliance however the commitment from patients to adhere commitment from patients to adhere to prescribed nutritional regimens is to prescribed nutritional regimens is poor (Bruce poor (Bruce et al, et al, 2003; Akner and 2003; Akner and Cederholm, 2001; Lawson Cederholm, 2001; Lawson et al, et al, 2000)2000). .

Appropriately Involve Appropriately Involve PatientPatient
Where do we Start ?Where do we Start ? Patient’s perception of dietetic Patient’s perception of dietetic
consultation.consultation. How does the patient value nutrition as a How does the patient value nutrition as a
component of their nutritional care?component of their nutritional care? Determine the patient’s knowledge and Determine the patient’s knowledge and
understanding of key nutritional understanding of key nutritional concepts.concepts.
Explicitly identify what contribution the Explicitly identify what contribution the patient can make to their nutritional care. patient can make to their nutritional care.

Patient Perception of Dietetic Patient Perception of Dietetic ConsultationConsultation
Rate nutrition as factor in recovery Rate nutrition as factor in recovery (VAS) and justify.(VAS) and justify.
What advice given and asked in their What advice given and asked in their view advice acceptableview advice acceptable
Did patient feel able to contribute to Did patient feel able to contribute to dietary targets set ? How could dietary targets set ? How could patient involvement be improved?patient involvement be improved?
Out-patient review mode and media Out-patient review mode and media of consultation.of consultation.

Do Patients Understand Key Do Patients Understand Key Nutritional Concepts?Nutritional Concepts?
Health literacy importance element Health literacy importance element in achieving compliance.in achieving compliance.
Use body map as tool to allow Use body map as tool to allow patient to patient’s understanding of patient to patient’s understanding of the relationship between the relationship between pathophysiology/recovery.pathophysiology/recovery.
Non- threatening multiple choice Non- threatening multiple choice questions and ask for justification questions and ask for justification for their selection.for their selection.

Where are we GoingWhere are we Going Examine the use of multimodal Examine the use of multimodal
accelerated recovery programme in accelerated recovery programme in elderly elderly #NOF patients.#NOF patients.
- pre-op carbohydrate loading.- pre-op carbohydrate loading.- anaesthesia and pain control.- anaesthesia and pain control.- training programme.- training programme.- nutrition.- nutrition.- active patient involvement.- active patient involvement.- monitor in the rehabilitation phase - monitor in the rehabilitation phase
of care.of care.


TeamTeam
DietitiansDietitians- Emma Kehoe, Project Lead.- Emma Kehoe, Project Lead.- Jackie Bird, Patient Involvement.- Jackie Bird, Patient Involvement.
Clinicians – Dr Alan Davidson, Dr Eric Clinicians – Dr Alan Davidson, Dr Eric GardinerGardiner
Physiologist – Dr Isobel Davidson.Physiologist – Dr Isobel Davidson.Physiotherapist – Dr Sarah Mitchell.Physiotherapist – Dr Sarah Mitchell.OT – Claire Ritchie.OT – Claire Ritchie.Cosultant – Christine Russell Cosultant – Christine Russell