Embed Size (px)
Citation preview

42Published by Oxford University Press on behalf of the Gerontological Society of America 2015.
Special Issue: Veterans Aging: Research Article
Predicting Functional Decline and Recovery for Residents in Veterans Affairs Nursing HomesJanusz Wojtusiak, PhD,1 Cari R. Levy, MD, PhD,2 Allison E. Williams, ND, PhD, RN,*,3 and Farrokh Alemi, PhD1,4
1Department of Health Administration and Policy, George Mason University, Fairfax, Virginia. 2Department of Internal Medicine, Palliative Care, Veterans Affairs Medical Center Eastern Colorado Health Care System, Denver. 3Department of Research, Bay Pines Veterans Affairs Healthcare System, Bay Pines, Florida. 4Office of Chief of Staff, District of Columbia Veterans Affairs Medical Center, Washington, DC.
*Address correspondence to Allison E. Williams, ND, PhD, RN, Department of Research, Bay Pines Veterans Affairs Healthcare System, 10000 Bay Pines Boulevard, Mail Code 151, Bay Pines, FL 33744. E-mail: [email protected]
Received January 26, 2015; Accepted April 8, 2015
Decision Editor: Nicholas G. Castle, PhD
AbstractPurpose of the Study: This article describes methods and accuracy of predicting change in activities of daily living (ADLs) for nursing home patients following hospitalization.Design and Methods: Electronic Health Record data for 5,595 residents of Veterans Affairs’ (VAs’) Community Living Centers (CLCs) aged 70 years and older were analyzed within the VA Informatics and Computing Infrastructure. Data included diagnoses from 7,106 inpatient records, 21,318 functional status evaluations, and 69,140 inpatient diagnoses. The Barthel Index extracted from CLC’s Minimum Data Set was used to assess ADLs loss and recovery. Patients’ diagnoses on hospital admission, ADL status prior to hospitalization, age, and gender were used alone or in combination to predict ADL loss/gain following hospitalization. Area under the Receiver–Operator Curve (AUC) was used to report accuracy of predictions in short (14 days) and long-term (15–365 days) follow-up post-hospitalization.Results: Admissions fell into 7 distinct patterns of recovery and loss: early recovery 19%, delayed recovery 9%, delayed recovery after temporary decline 9%, early decline 29%, delayed decline 10%, delayed decline after temporary recovery 6%, and no change 18%. Models accurately predicted ADL’s 14-day post-hospitalization (AUC for bathing 0.917, bladder 0.842, bowels 0.875, dressing 0.871, eating 0.867, grooming 0.902, toileting 0.882, transfer 0.852, and walking deficits was 0.882). Accuracy declined but remained relatively high when predicting 14–365 days post-hospitalization (AUC ranging from 0.798 to 0.875).Implications: Predictive modeling may allow development of more personalized predictions of functional loss and recovery after hospitalization among nursing home patients.
Key Words: Activities of daily living, Community living centers, Hospitalization, Data analysis, Predictive modeling
IntroductionHospitalization is common among nursing home resi-dents (Department of Health and Human Services, Office of Disability, Aging and Long-Term Care Policy, 2011; Department of Health and Human Services, Office of the Inspector General, 2013) and is often associated with
functional decline (Ferguson-Pare et al., 2000; Gill, Allore, Gahbauer, & Murphy, 2010; Gill, Gahbauer, Han, & Allore, 2009a; Gill, Gahbauer, Han, & Allore, 2011; McCusker, Kakuma, & Abrahamowicz, 2002). Studies of community-dwelling elders conducted over the past 20 years estimate that 30%–60% of those hospitalized develop new activities
The Gerontologistcite as: Gerontologist, 2016, Vol. 56, No. 1, 42–51
doi:10.1093/geront/gnv065Advance Access publication July 16, 2015
Downloaded from https://academic.oup.com/gerontologist/article-abstract/56/1/42/2605210by gueston 16 April 2018

43
of daily living (ADL) dependencies (Gill, Allore, Gahbauer, & Murphy, 2010; Landefeld, 2003; Lamont, Sampson, Matthias, & Kane, 1983; Landefeld, Palmer, Kresevic, Fortinsky, & Kowal, 1995; Mahoney, 1999; McVey, Becker, Saltz, Feussner, & Cohen, 1989; Sager et al., 1996a; Sager et al., 1996b; Volpato et al., 2011; Wu, Sahadevan, & Ding, 2006). Furthermore, bed rest in the setting of illness is a strong predictor of transition from no disability to severe dis-ability (Gill, Allore, Gahbauer, & Han, 2014). Functional loss during hospitalization is also a predictor of mortality among elderly patients (Inouye et al., 1998; Sleiman et al., 2009). Models of functional trajectory following illness among per-sons discharged to nursing homes suggests that disability is heterogeneous, especially for those with organ failure (Gill, Gahbauer, Han, & Allore, 2010). In one study of 296 newly admitted nursing home residents, the majority (64%) had no ADL deficits in the month preceding hospitalization and only 32% ultimately returned home (Gill, Gahbauer, Han, & Allore, 2009b). Importantly, this study illustrates the impor-tance of assessing deficits in the weeks prior to hospitaliza-tion and, in the present analysis, the data analyzed attempt to account for changes that may occur in the weeks leading up to hospitalization by using functional assessments within 14 days of the index hospitalization.
Knowledge about functional status impacts decision mak-ing regarding health care. In one study, patients confronted with a possibility that they were unlikely to return to their baseline functional status were less likely to proceed with hos-pital treatment (Fried, Bradley, Towle, & Allore, 2002). For many patients, what matters is not whether they live longer but their quality of life in the coming months (McCarthy, Phillips, Zhong, Drews, & Lynn, 2000). Knowledge of post-hospitalization functional ability may inform care planning and expectations following hospitalization.
However, little is known about how functional sta-tus changes following hospitalization among residents of nursing homes. The current article describes patterns of functional loss and recovery among hospitalized, Veteran nursing home patients.
Design and MethodsUnder the Nursing Home Quality Initiative of Centers for Medicare & Medicaid Services (Department of Health and Human Services, Centers for Medicare & Medicaid Services, 2014), nursing homes are required to assess the functional capabilities of their residents by collecting a Minimum Data Set (MDS). The MDS contains quantified functional sta-tus measures that allow derivation of a functional status score. The scores found in MDS reflect observations within a 24–48 hr time frame (Department of Health and Human Services, Centers for Medicare & Medicaid Services, 2014). The evaluation is done at least every 90 days, with a change in condition, and includes evaluation within 14 days postdis-charge from hospital. MDS can be converted to the Barthel Index, for research purposes (Shah, Vanclay, & Cooper,
1989; Wade & Collin, 1988). The mapping used in this study is based on MDS questions G1, G2, and H2 as shown in Table 1. These questions capture information used in Barthel Index; however, the formulation of the actual questions and the scale anchors are somewhat different. For example, for the items “dressing” and “toilet use,” the MDS captures five levels of ability: independent, supervision, limited assis-tance, extensive assistance, total dependence, and activity not observed, In contrast the Barthel Index offers three levels for these items: independent, needs some help, and dependent. Furthermore, questions for items are specified for MDS data whereas in the Barthel Index categories are rated within the assessment level. For dressing, the MDS item is: “How resi-dent puts on, fashions, and takes of all items of street clothing, including donning/removing prosthesis.” In the Barthel Index, dressing is identified as the item with assessment levels speci-fied as dependent, needs help, but can do about half unaided, and independent (including buttons, zips, laces, etc.). Thus, the constructed measures we use cannot be considered com-pletely equivalent to Barthel Index. While the presented work focused on ADLs as defined by Barthel Index, there are other possible measures that can be extracted from MDS.
Source of Data
Inpatient records for patients in Veterans Affairs (VA) nursing homes, called Community Living Centers (CLC) were extracted from the Department of Veteran’s Affairs Corporate Data Warehouse and analyzed within the VA Informatics and Computing Infrastructure computing infra-structure. Electronic Health Record data for 324,435 resi-dents of VA’s CLCs were extracted. Data included diagnoses from 1,622,352 inpatient records and 1,901,354 functional status evaluations. Nursing home residents provide a unique population in which to study ADL loss associated with acute illness resulting in hospitalization. Basic ADLs are routinely documented for nursing home residents. These assessments provide an opportunity to measure changes prior to hospi-talization, in the weeks following hospital discharge, and in the months that follow readmission to the nursing home.
Inclusion Criteria
All patients were required to be at least 70 years old at time of index hospitalization. Patients were required to have Barthel Index evaluations within 14 days before hospitali-zation, 14 days after hospitalization, and at least one score between 14 days and 1 year after hospitalization. After applying the criteria, the data consisted of 7,106 inpatient records for 5,595 patients and 69,140 inpatient diagnoses.
Dependent Variables
The dependent variable in this study was change in func-tional status, as measured through Barthel Index. The aver-age Barthel Index prior to the hospitalization was 48.01
The Gerontologist, 2016, Vol. 56, No. 1
Downloaded from https://academic.oup.com/gerontologist/article-abstract/56/1/42/2605210by gueston 16 April 2018

44
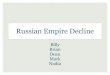
(standard deviation [SD] = 25.74), immediate post-hos-pitalization was 44.37 (SD = 26.19), and at least 14 days post-hospitalization was 44.02 (SD = 27.42). On average, the post-hospitalization evaluation was done 9 days after discharge, and follow-up evaluation was done 77 days after discharge. It can be observed in Figure 1 that on average functional decline occurs during the hospitalization or within 14 days of hospitalization, and in lesser degree at the follow-up visit. In addition to total Barthel Index Score, models for all nine considered Barthel Index items were constructed.
The dependent variables included the Barthel scores as well as seven possible changes in functional status post-hospi-talization: (a) early recovery, (b) delayed recovery, (c) delayed recovery after temporary decline, (d) early decline, (e) delayed decline, (f) delayed decline after temporary recovery, and (g) no change. These categories represent meaningful factorial combinations of improvement, decline, and no change.
Independent Variables
The independent variables included 296 independent vari-ables: age, gender, Barthel Index (overall and individual daily living function scores) pre-hospitalization, and 284 indica-tors of diagnoses during hospitalization as defined by Agency for Healthcare Research and Quality’s Clinical Classification Software (Department of Health and Human Services, Agency for Healthcare Research and Quality, 2012). Table 2 shows distributions of variables in predicting functional sta-tus. One can note that overall Barthel Index declines post-hospitalization by 3.642 (p < .01) points. While a minimally
clinically important difference has not been established for nursing home cohorts, the value for acute stroke cohorts is 1.85 points (Hsieh & Wang, 2007). For 33% of subjects functional decline occurred following hospitalization but for 19% functional scores following hospitalization were higher than those in the 14 days preceding hospitalization. Since some patients improve and others decline, it is important to build individualized models to predict overall change as well as change on specific Barthel items.
Method of Prediction
Predictive modeling to classify trajectories of functional loss as well as actual values of Barthel was done using Random Forest approach, which is a popular machine learning method (Breiman, 2001). It uses boosting and randomiza-tion to produce a large number of decision trees that describe data from different perspectives. The analysis was setup as a classification (dependent variables are discrete), rather than regression (dependent variables are numeric). On the data at hand, Random Forest has shown superior performance as compared to other well-known methods such as Naïve Bayes, Logistic Regression, or Support Vector Machines. Previously multiple researchers applied Random Forests to classification (i.e., Gu et al., 2015; Raju, Su, Patrician, Loan, & McCarthy, 2015) and regression problems (i.e., Li, Leung, Wong, & Ballester, 2014). We have performed a sensitivity analysis to confirm that parameters of the method do not significantly affect results, as well as tests with subsets of con-sidered variables to check issues related to multicolinearity.
Table 1. Barthel Index Items and Mapping From MDS Questionnaire
Item Levels Mapping from MDS
Feeding 0 = unable; 5 = needs help cutting; spreading butter, etc., or requires modified diet; 10 = independent
G1HA = 1,2 G1HA = 0
Bathing 0 = dependent; 5 = independent (or in shower) G2A = 0.1Grooming 0 = needs to help with personal care; 5 = independent face/hair/
teeth/shaving (implements provided)G1JA = 0,1
Dressing 0 = dependent; 5 = needs help but can do about half unaided; 10 = independent (including buttons, zips, laces, etc.)
G1GA = 2 G1GA = 0,1
Bowels 0 = incontinent (or neewds to be given enemas); 5 = occasional accident; 10 = continent
H1A = 2 H1A = 0,1
Bladder 0 = incontinent, or catheterized and unable to manage alone; 5 = occasional accident; 10 = continent
H1B = 1,2 H1B = 0
Toilet use 0 = dependent; 5 = needs some help, but can do something alone; 10 = independent (on and off, dressing, wiping)
G1IA = 2 G1IA = 0,1
Transfers (bed to chair and back)
0 = unable, no sitting balance; 5 = major help (one or two people, physical), can sit; 10 = minor help (verbal or physical); 15 = independent
G1BA = 3 G1BA = 2 G1BA = 0,1
Mobility (on level surfaces)
0 = immobile or <50 yards; 5 = wheelchair independent, including corners, >50 yards; 10 = walks with help of one person (verbal or physical) >50 yards; 15 = independent (but may use any aid; for example, stick) >50 yards
G1DA = 3,4 and G5B = 1 G1DA = 1,2 G1DA = 0
Stairs 0 = unable; 5 = needs help (verbal, physical, carrying aid); 10 = independent
Not applicable to CLC residents and not used in this study.
Note: CLC = Community Living Center; MDS = Minimum Data Set.
The Gerontologist, 2016, Vol. 56, No. 1
Downloaded from https://academic.oup.com/gerontologist/article-abstract/56/1/42/2605210by gueston 16 April 2018

45
Technical details of these tests and comparisons are not pre-sented here as they are outside of main focus of the work. These results are available by writing to the first author.
Data preprocessing was done using Microsoft SQL Server, statistical analysis was done using R 3.1.0, and predictive mod-eling was done using Weka 3.6 (Witten & Frank, 2005). The software was available in the VA’s Informatics and Computing infrastructure. Tenfold cross-validation was used to ensure validity. The results of predictions are reported using the Area Under Receiver–Operator Curve (AUC; also known as C-statistic). AUC is a standard method of comparing predic-tion models combining precision and recall on a continuous scale. The maximum value of AUC is 1 and 0.5 corresponds to AUC for a random prediction. The advantage of AUC is that it does not require using fixed thresholds as other methods.
ResultsTable 3 illustrates average trajectories for changes in functional status. The percent of admissions that fell into the seven dis-tinct patterns of recovery were as follows: early recovery 19%,
delayed recovery 9%, delayed recovery after temporary decline 9%, early decline 29%, delayed decline 10%, delayed decline after temporary recovery 6%, and no change 18%. Table 3 also reports average numbers of days at follow up evalua-tion. Most patients (45%) declined in functional status and a minority (37%) regained their baseline functional status.
Application of the Random Forest method resulted in a set of prediction models that detect change in total Barthel Index score and individual scores for Barthel Items, as well as predicting the actual values of Barthel Items. The aver-age AUC for predicting the change is 0.751, with the val-ues ranging 0.681 for predicting change in eating (eating is the only item with AUC below 0.7) to 0.832 for predicting change in bathing. Table 4 shows AUC in predicting change in functional status based on previous status and inpatient diagnoses for the Barthel Index and its individual items.
When predicting the actual values of Barthel Index items postdischarge the average AUC is 0.877, however when predict-ing only functional independence versus any degree of depend-ence Barthel Index items, the average AUC is 0.9 and range from 0.884 (eating) to 0.918 (dressing). Tables 5 shows AUC
Table 2. Means and Standard Deviations for Dependent Variables (N = 7,106)
Pre-hospitalization, mean (standard deviation)
Post-hospitalization, mean (standard deviation)
p value pre-post
Follow-up, mean (standard deviation)
p value post-follow
Age 71.35 (6.1)Female 5.33%Score 48.014 (25.736) 44.372 (26.189) <.01 44.02 (27.419) .08Feeding 7.212 (3.427) 6.842 (3.602) <.01 6.677 (3.749) <.01Bathing 0.972 (1.979) 0.857 (1.884) <.01 0.899 (1.92) .02Grooming 1.713 (2.373) 1.53 (2.304) <.01 1.575 (2.323) .04Dressing 4.41 (4.011) 3.987 (3.989) <.01 3.974 (4.082) .72Bowels 7.112 (4.158) 6.601 (4.364) <.01 6.319 (4.449) <.01Bladder 7.562 (3.831) 7.381 (3.948) <.01 7.293 (3.999) .02Toilet use 4.546 (4.242) 4.028 (4.202) <.01 4.038 (4.286) .01Transfers 9.674 (5.196) 8.898 (5.376) <.01 8.91 (5.608) .01Mobility 4.812 (6.167) 4.248 (6.010) <.01 4.334 (6.052) .13
Figure 1. Average scores on Barthel Index items, pre-hospitalization, post-hospitalization, and in follow-up evaluation. Note that the total score is divided by 10 to visually scale with individual items.
The Gerontologist, 2016, Vol. 56, No. 1
Downloaded from https://academic.oup.com/gerontologist/article-abstract/56/1/42/2605210by gueston 16 April 2018

46
for predicting individual Barthel scores 14 days postdischarge and during follow-up period (15–365 days postdischarge).
Because the constructed models consist of 100 decision trees based on over 200 variables, it is not possible to include them explicitly in this publication. The complete models cre-ated in this research are available at http://www.mli.gmu.edu/adl-prediction. The files included in this archive can be used in Weka 3.6 software. Details of the models as well as results of testing are also available through the corresponding author. The size of the models also makes it impractical or impossi-ble to apply them “manually,” without appropriate software. Thus, the presented models are intended to be implemented as a decision support tool linked to an electronic health record, from which all the needed data can be automatically extracted and final results presented to clinicians.
DiscussionSeveral investigators have examined loss of ADL post-hospitalization (Covinsky et al., 2003; Covinsky, Justice,
Rosenthal, Palmer, & Landefeld, 1997; Givens, Jones, & Inouye, 2009; Mahoney 1999; Murray et al., 1993; Pedone et al., 2005) and risk factors for such losses (Huyse et al., 2001; Inouye et al., 1993; Lang 2007; Li et al., 2005; McCusker et al., 1999; Sager et al., 1996a; Sager et al., 1996b; Volpato et al., 2007; Wu et al., 2000). This article extends these analyses by predicting which ADL deficits are expected to decline in an individual patient.
On average, ADL function declined significantly for the overall Barthel Index score and for all nine ADL categories in the immediate post-hospitalization assessment. On aver-age, scores did not improve at the subsequent assessment. While slight improvement in some of the individual ADL domain scores was observed, none of the scores returned to baseline. On average, some (but not all) residents lose func-tional abilities post-hospitalization. Therefore, it is critical to accurately identify patients who will decline and distinguish them from those who will recover some or all function.
The percentage of patients who experienced recov-ery was consistent with a frail population at high risk
Table 3. Change of ADLs After Hospitalization in 7,106 Admissions of 5,595 Patients
Early Recovery
1328 (19%) admissions 1236 (22%) patients 63(SD=80) days until follow-up evaluation od ADLs
Delayed Recovery 618 (9%) admissions 564 (10%) patients 92(SD=98) days until follow-up evaluation od ADLs
Delayed Recovery after Temporary Decline
623 (9%) admissions 583 (10%) patients 83(SD=91) days until follow-up evaluation od ADLs
No change 1285 (18%) admissions 1074 (19%) patients 58 (SD=71) days until follow-up evaluation of ADLs
Early Decline 2096 (29%) admissions 1861 (33%) patients 74 (SD=85) days until follow-up evaluation of ADLs
Delayed Decline 726 (10%) admissions 638 (11%) patients 106 (SD=100) days until follow-up evaluation of ADLs
Delayed Decline after Temporary Recovery
457 (6%) admissions 424 (8%) patients 112 (SD=105) days until follow-up evaluation of ADLs
SD=Standard Deviation
Note: ADL = activities of daily living.
The Gerontologist, 2016, Vol. 56, No. 1
Downloaded from https://academic.oup.com/gerontologist/article-abstract/56/1/42/2605210by gueston 16 April 2018

47
of functional decline. We found that approximately half of nursing home residents remained stable, recovered to baseline or improved while prior investigations of pre-dominately community-dwelling elders have estimated recovery among two-thirds of the elders hospitalized (Covinsky et al., 2003; Hirsch, Sommers, Olsen, Mullen, & Winograd, 1990; Sleiman et al., 2009). In our sample, immediate decline occurred for 38% of admissions, which is comparable to patients considered at intermediate or high risk of functional decline in other studies (Sager et al., 1996b).
The term “iatrogenic disability” has been coined to describe avoidable dependence which often occurs during the course of care and has been defined as the cumulative effect of three components, (a) the patient’s baseline level of frailty, (b) the severity of the illness leading to hospitalization, and (c) hospital structure and care processes. Efforts to prevent iatro-genic disability have involved risk assessment tools, consul-tation teams, single and multi-domain interventions (Lafont, Gerard, Voisin, Pahor, & Vellas, 2011), but these interventions have had only modest success. A criticism of these interven-tions has been that they do not address prevention of decline. In response, recent research focuses on increasing ambulation which does not occur for the majority of hospitalized older adults (Callen, Mahoney, Grieves, Wells, & Enloe, 2004) through the use of restorative or “function-focused care.”
Hospital-based interventions to reduce functional decline such as the Family-Centered, Function-Focused Care (Fam-FFC) Intervention include function-focused care that includes environmental assessment and modification, staff education, individual and family education and partnership in care plan-ning with follow-up after hospitalization (Boltz, Resnick, Capezuti, Shuluk, & Secic, 2012; Boltz, Resnick, Chippendale, & Galvin, 2014; Resnick et al., 2011). Acute Care for Elder Units are another approach to minimize decline and compli-cations during hospitalization and key components include early rehabilitation and function-focused interventions (Counsell et al., 2000; Fox et al., 2013). Mobility has been a primary focus of many other function focused care interven-tions during hospitalization (Ostir et al., 2012; Ostir et al., 2013). Evidence indicates that those exposed to function focused care experience less severe and shorter episodes of delirium, improved sleep, decreased agitation and improved walking performance compared to controls (Boltz et al., 2014; Ostir et al., 2012; Ostir et al., 2013). A summary of these interventions concludes that identifying baseline func-tion and means to maintaining function are essential in sup-porting functional stability and preventing complications associated with hospitalization. One of the aims of this inves-tigation was to assess the accuracy of models predicting loss of specific ADL to both provide specificity to comprehensive programs such as the Fam-FFC intervention to aid in bedside
Table 4. Accuracy (Area Under Curve) for Predicting Change in Barthel Index Items
Bathing Bladder Bowels Dressing Eating Grooming Toilet Transfers Mobility Average
Early decline 0.942 0.672 0.750 0.808 0.710 0.891 0.820 0.729 0.879 0.800Delayed decline 0.916 0.660 0.693 0.760 0.645 0.857 0.769 0.671 0.845 0.757Delay decline after temporary recovery
0.729 0.813 0.813 0.643 0.713 0.734 0.664 0.722 0.599 0.714
No change 0.830 0.740 0.740 0.725 0.663 0.757 0.754 0.696 0.782 0.743Delay recovery after temporary decline
0.899 0.632 0.665 0.718 0.570 0.806 0.745 0.653 0.788 0.720
Delayed recovery 0.715 0.869 0.848 0.711 0.820 0.788 0.739 0.770 0.692 0.772Early recovery 0.768 0.882 0.868 0.734 0.820 0.782 0.765 0.768 0.689 0.786Average 0.832 0.741 0.746 0.735 0.681 0.774 0.760 0.709 0.780 0.751
Table 5. Accuracy of Models for Predicting Values of Barthel Index Items
Score Bathing Bladder Bowels Dressing Eating Grooming Toilet Transfers Mobility
14 days postdischarge
0 0.917 0.868 0.898 0.885 0.886 0.902 0.896 0.881 0.8875 0.917 0.783 0.782 0.817 0.835 0.902 0.82 0.827 0.784
10 0.848 0.886 0.918 0.884 0.915 0.794 0.84215 0.904 0.916Average 0.917 0.842 0.875 0.871 0.867 0.902 0.882 0.852 0.882
15–365 days postdischarge
0 0.875 0.827 0.85 0.847 0.832 0.855 0.851 0.826 0.8345 0.875 0.732 0.73 0.762 0.78 0.855 0.758 0.766 0.65
10 0.805 0.848 0.866 0.84 0.861 0.728 0.77715 0.843 0.866Average 0.875 0.798 0.832 0.827 0.819 0.855 0.833 0.795 0.827
Note: Values indicating prediction of functional independence are marked in bold.
The Gerontologist, 2016, Vol. 56, No. 1
Downloaded from https://academic.oup.com/gerontologist/article-abstract/56/1/42/2605210by gueston 16 April 2018

48
care planning and broadening discussion of function focused care beyond mobility to other functional deficits.
The results of this analysis suggest that for patients admitted from nursing homes, functional status data can be used to predict with a moderate degree of accuracy, the specific ADL(s) that are likely to decline during hospitaliza-tion. Such data could be used to tailor programs in the hos-pital not only to rehabilitate those who experience decline, but also to prevent iatrogenic disability before it occurs.
A primary tenant of care in nursing homes is to ensure that a resident’s condition does not decline unless it is medically unavoidable. Yet, adults in nursing homes with severe cogni-tive impairment participate in less than 1 minute of moderate physical activity daily and expend on average only 24.65 kcals in a 24 hour period. Even for persons in long-term care facili-ties for care focused on rehabilitation, patients receive rehabil-itation for only 1 to 2 hours of their day and remain inactive for the majority of the day (Resnick & Galik, 2015; Munin et al., 2010). Function focused care in nursing homes appears to provide benefit, but a key recommendation to improve the fidelity of these interventions was to provide more practical assessments of the capabilities of older adults to establish function focused care goals and interactions specific to their current or anticipated deficits (Resnick, Galik, & Boltz, 2013).
A distinct advantage of this analysis was the availability of functional status measurement within 2 weeks prior to hos-pitalization. Palleschi et al. (2014) found that 42% of geriat-ric patients experienced functional decline prior to hospital admission and preadmission functional status was a strong indicator of post-hospitalization disability. Measurement of functional status only at the time of admission to and dis-charge from the hospital omits a potentially important phase of the illness and debility that may contribute to predictive modeling (Mudge, O’Rourke, & Denaro, 2010; Palleschi et al., 2011). We also found pre-hospitalization functional status to be predictive of disability at the time of discharge and the combination of previous functional status and comorbidities present at hospitalization refined the models.
Modeling Implications
It is possible to predict with a reasonable accuracy which of the seven considered trajectories of functional status change is to be expected. Models created by Random Forest method can be used either to predict the one most probable trajectory of change, or to rank multiple trajectories, depending on spe-cific needs. While the selected Random Forest method is accu-rate in making predictions, its downside is that it cannot be easily interpreted by clinicians and constitutes a “black box” type of model (every model developed in the study consists of 100 decision trees, each with nine levels). Our intention is that these models may be implemented within an Electronic Health Record (EHR) system, as a decision support tool.
This article reports the benchmarks for loss of various ADL functions post-hospitalization. These benchmarks could be used in evaluation of interventions designed to prevent
ADL decline. This work provides a platform for understand-ing posthospital trajectories among nursing home residents and can be used to understand what diseases, therapies, and care approaches serve as modifiers of these trajectories.
In models developed in this article, the accuracy of pre-dictions depended on the specific ADL. In predicting ability to bathe, dress, groom, transfer, walk, and toilet the models were more accurate (AUC > 0.9) than in predicting bladder continence, bowel continence, and eating independently (AUC < 0.9). It was also more accurate to predict func-tional ability immediately postdischarge than in a longer term follow-up (AUC 0.877 vs. 0.851, p < .01).
Policy Implications
Our data indicate that on average functional status contin-ues to decline following discharge from the hospital. Thus, while the patient symptoms may be stable, functional sta-tus stability may not yet be achieved. Implications postdis-charge would thus underscore those functional items upon which to focus in the next setting of care.
Replication of this analysis within health care systems designed to avoid hospitalization by reimbursing providers for intensive management within the nursing home such as Optum, formerly the EverCare program, will provide essential information regarding the relative importance of hospitaliza-tion in the setting of acute illness. Evaluations of the Optum model indicate that hospitalization rates are lower, quality of care is similar and cost savings are realized but functional evaluations are not available (Kane, Flood, Bershadsky & Keckhafer 2004; Kane, Homyak, Bershadsky, Flood & Zhang 2004; Kane, Keckhafer, Flood, Bershadsky and Siadaty 2003).
Limitations
There are several limitations of the presented work. The work focuses on veterans aged 70 years and older, who resided in VA’s Community Living Centers and generalization to other populations is not possible. Due to strict inclusion criteria that required residents to have three MDS evaluations, the cohort only included approximately 6,000, as compared to 300,000 CLC residents with available data. In the presented study only MDS data elements related to Barthel Index were used. Higher prediction accuracy may be achieved when additional data elements (e.g., measures of cognitive status) are included in the models. Additionally, studies of MDS data have indi-cated variation in assessments across clinical settings, and consequent measurement error (Dellefield, 2007). Deriving Barthel Index scores from MDS data introduces this error into the analysis and may systematically impact findings.
This article provides evidence that functional decline and recovery can be predicted with relatively high accuracy fol-lowing hospitalization of VA nursing home residents. This information has the potential for use in optimizing health ser-vice delivery and care planning. For example, predictive mod-eling could be used to stratify residents according to their risk
The Gerontologist, 2016, Vol. 56, No. 1
Downloaded from https://academic.oup.com/gerontologist/article-abstract/56/1/42/2605210by gueston 16 April 2018

49
of developing new deficits and allow for testing of programs aimed at preventing the onset of new ADL deficits. Moreover, individualized predictions on the most likely trajectories of change can be used to design personalized post-hospitaliza-tion care plans and test interventions designed to improve outcomes following hospitalization of nursing home residents.
FundingThis material is the result of work supported with resources and the use of facilities at the Bay Pines VA Healthcare System. It is part of a quality improvement project evaluating the Medical Foster Home program supported by appropriation #3620160 from the VA Office of Geriatrics and Extended Care.
AcknowledgmentsThe authors thank members of VA’s Medical Foster Home evalua-tion team (Arthur R. Williams, Bryce Sutton, Etienne Pracht, Lisa Argyros, Phan Giang, Jacqueline Higginbottom, Bruce A. Citron, and James Blankenship) for their collaboration in this research. The authors also thank anonymous reviewers who provided detailed comments that helped improve the presented work and sparked fur-ther discussion on methodological issues. The contents of this article do not represent the views of the Department of Veterans Affairs or the United States Government.
ReferencesBoltz, M., Resnick, B., Capezuti, E., Shuluk, J., & Secic, M. (2012).
Functional decline in hospitalized older adults: Can nurs-ing make a difference? Geriatric Nursing, 33(4), 272–279. doi:10.1016/j.gerinurse.2012.01.008
Boltz, M., Resnick, B., Chippendale, T., & Galvin, J. (2014). Testing a family-centered intervention to promote functional and cognitive recovery in hospitalized older adults. Journal of the American Geriatrics Society, 62(12), 2398–2407. doi:10.1111/jgs.13139
Breiman, L. (2001). Random forests. Machine Learning, 45(1), 5–32.Callen, B. L., Mahoney, J. E., Grieves, C. B., Wells, T. J., & Enloe,
M. (2004). Frequency of hallway ambulation by hospitalized older adults on medical units of an academic hospital. Geriatric Nursing, 25(4), 212–217. doi:10.1016/j.gerinurse.2004.06.016
Counsell, S. R., Holder, C. M., Liebenauer, L. L., Palmer, R. M., Fortinsky, R. H., Kresevic, D. M.,…Landefeld, C. S. (2000). Effects of a multicomponent intervention on functional out-comes and process of care in hospitalized older patients: A randomized controlled trial of Acute Care for Elders (ACE) in a community hospital. Journal of the American Geriatrics Society, 48(12), 1572–1581. doi:10.1111/j.1532-5415.2000.tb03866.x
Covinsky, K. E., Justice, A. C., Rosenthal, G. E., Palmer, R. M., & Landefeld, C. S. (1997). Measuring prognosis and case mix in hospitalized elders. The importance of functional sta-tus. Journal of General Internal Medicine, 12(4), 203–208. doi:10.1046/j.1525-1497.1997.012004203.x
Covinsky, K. E., Palmer, R. M., Fortinsky, R. H., Counsell, S. R., Stewart, A. L., Kresevic, D.,…Landefeld, C. S. (2003). Loss of independence in activities of daily living in older adults hospi-talized with medical illnesses: Increased vulnerability with age.
Journal of the American Geriatrics Society, 51(4), 451–458. doi:10.1046/j.1532-5415.2003.51152.x
Dellefield, M. E. (2007). Implementation of the resident assessment instrument/minimum data set in the nursing home as organi-zation: Implications for quality improvement in RN clinical assessment. Geriatric Nursing, 28(6), 377–386. doi:10.1016/j.gerinurse.2007.03.002
Department of Health and Human Services, Agency for Healthcare Research and Quality. (2012). HCUP CCS Fact Sheet. Healthcare Cost and Utilization Project (HCUP). Retrieved from http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccsfactsheet.jsp
Department of Health and Human Services, Centers for Medicare & Medicaid Services. (2014). Nursing Home Quality Initiative. Retrieved from http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/NursingHomeQualityInits/index.html?redirect=/nursinghomequalityinits/
Department of Health and Human Services, Office of Disability, Aging and Long-Term Care Policy. (2011). Hospitalizations of Nursing Home Residents: Background and Options. Retrieved from http://aspe.hhs.gov/daltcp/reports/2011/NHResHosp.pdf
Department of Health and Human Services, Office of the Inspector General. (2013). Medicare Nursing Home Resident Hospitalization Rater Merit Additional Monitoring. Retrieved from http://oig.hhs.gov/oei/reports/oei-06-11-00040.pdf
Ferguson-Pare, M., Bourret, E., Bernick, L., Buchanan, D., Cabico, L., King, B., & Rivera, T. M. (2000). Best practices in the care of elderly persons in hospital. Hospital Quarterly, 3(4), 30–37. doi:10.12927/hcq..16541
Fox, M. T., Sidani, S., Persaud, M., Tregunno, D., Maimets, I., Brooks, D., & O’Brien, K. (2013). Acute care for elders compo-nents of acute geriatric unit care: Systematic descriptive review. Journal of the American Geriatrics Society, 61(6), 939–946. doi:10.1111/jgs.12282
Fried, T. R., Bradley, E. H., Towle, V. R., & Allore, H. (2002). Understanding the treatment preferences of seriously ill patients. New England Journal of Medicine, 346(14), 1061–1066. doi:10.1056/NEJMsa012528
Gill, T. M., Allore, H. G., Gahbauer, E. A., & Han, L. (2014). Establishing a hierarchy for the two components of restricted activity. Journal of Gerontology: Series A, Biological Sciences and Medical Sciences. doi:10.1093/gerona/glu203
Gill, T. M., Allore, H. G., Gahbauer, E. A., & Murphy, T. E. (2010). Change in disability after hospitalization or restricted activity in older persons. JAMA, 304(17), 1919–1928. doi:10.1001/jama.2010.1568
Gill, T. M., Gahbauer, E. A., Han, L., & Allore, H. G. (2009a). Factors associated with recovery of prehospital function among older persons admitted to a nursing home with disability after an acute hospitalization. Journal of Gerontology: Series A, Biological Sciences and Medical Sciences, 64A(12), 1296–1303. doi:10.1093/gerona/glp115
Gill, T. M., Gahbauer, E. A., Han, L., & Allore, H. G. (2009b). Functional trajectories in older persons admitted to a nursing home with disabil-ity after an acute hospitalization. Journal of the American Geriatrics Society, 57(2), 195–201. doi:10.1111/j.1532-5415.2008.02107.x
Gill, T. M., Gahbauer, E. A., Han, L., & Allore, H. G. (2010). Trajectories of disability in the last year of life. The New England Journal of Medicine, 362(13), 1173–1180. doi:10.1056/NEJMoa0909087
The Gerontologist, 2016, Vol. 56, No. 1
Downloaded from https://academic.oup.com/gerontologist/article-abstract/56/1/42/2605210by gueston 16 April 2018

50
Gill, T. M., Gahbauer, E. A., Han, L., & Allore, H. G. (2011). The relationship between intervening hospitalizations and transi-tions between frailty states. Journal of Gerontology: Series A, Biological Sciences and Medical Sciences, 66A(11), 1238–1243. doi:10.1093/gerona/glr142
Givens, J. L., Jones, R. N., & Inouye, S. K. (2009). The overlap syn-drome of depression and delirium in older hospitalized patients. Journal of the American Geriatrics Society, 57(8), 1347–1353. doi:10.1111/j.1532-5415.2009.02342.x
Gu, W., Vieira, A. R., Hoekstra, R. M., Griffin, P. M., & Cole, D. (2015). Use of random forest to estimate population attribut-able fractions from a case-control study of Salmonella enterica serotype Enteritidis infections. Epidemiology and Infection, 1–9. doi:10.1017/S095026881500014X
Hirsch, C. H., Sommers, L., Olsen, A., Mullen, L., & Winograd, C. H. (1990). The natural history of functional morbidity in hospital-ized older patients. Journal of the American Geriatrics Society, 38(12), 1296–1303. doi:10.1111/j.1532-5415.1990.tb03451.x
Hsieh, Y. W., & Wang, C. H. (2007). Establishing the minimally clinically important difference of the Barthel Index in stroke patients.” Neurorehabilitation and Neural Repair, 21(3), 233–238. doi:10.1177/1545968306294729
Huyse, F. J., de Jonge, P., Slaets, J. P., Herzog, T., Lobo, A., Lyons, J. S.,…Rigatelli, M. (2001). COMPRI—an instrument to detect patients with complex care needs: Results from a European study. Psychosomatics, 42(3), 222–228. doi:10.1176/appi.psy.42.3.222
Inouye, S. K., Peduzzi, P. N., Robison, J. T., Hughes, J. S., Horwitz, R. I., & Concato, J. (1998). Importance of functional measures in predicting mortality among older hospitalized patients. Journal of the American Medical Association, 279(15), 1187–1193. doi:10.1001/jama.279.15.1187
Inouye, S. K., Wagner, D. R., Acampora, D., Horwitz, R. I., Cooney, L. M. Jr., Hurst, L. D., & Tinetti, M. E. (1993). A predictive index for functional decline in hospitalized elderly medical patients. Journal of General Internal Medicine, 8(12), 645–652. doi:10.1007/bf02598279
Kane, R. L., Flood, S., Bershadsky, B., & Keckhafer, G. (2004). Effect of an innovative medicare managed care program on the quality of care for nursing home residents. The Gerontologist, 44(1), 95–103. doi:10.1093/geront/44.1.95
Kane, R. L., Homyak, P., Bershadsky, B., Flood, S., & Zhang, H. (2004). Patterns of utilization for the Minnesota senior health options program. Journal of the American Geriatrics Society, 52(12), 2039–2044. doi:10.1111/j.1532-5415.2004.52558.x
Kane, R. L., Keckhafer, G., Flood, S., Bershadsky, B., & Siadaty, M. S. (2003). The effect of Evercare on hospital use. Journal of the American Geriatrics Society, 51(10), 1427–1434. doi:10.1046/j.1532-5415.2003.51461.x
Lafont, C., Gerard, S., Voisin, T., Pahor, M., & Vellas, B. (2011). Reducing “iatrogenic disability” in the hospitalized frail elderly. The Journal of Nutrition, Health & Aging, 15(8), 645–660. doi:10.1007/s12603-011-0335-7
Lamont, C. T., Sampson, S., Matthias, R., & Kane, R. (1983). The outcome of hospitalization for acute illness in the elderly. Journal of the American Geriatrics Society, 31(5), 282–288. doi:10.1111/j.1532-5415.1983.tb04872.x
Landefeld, C. S. (2003). Improving health care for older per-sons. Annals of Internal Medicine, 139(5_Part_2), 421–424. doi:10.7326/0003-4819-139-5_Part_2-200309021-00008
Landefeld, C. S., Palmer, R. M., Kresevic, D. M., Fortinsky, R. H., & Kowal, J. (1995). A randomized trial of care in a hospital medi-cal unit especially designed to improve the functional outcomes of acutely ill older patients. New England Journal of Medicine, 332(20), 1338–1344. doi:10.1056/NEJM199505183322006
Lang, P. O., Meyer, N., Heitz, D., Dramé, M., Jovenin, N., Ankri, J.,…Blanchard, F. (2007). Loss of independence in Katz’s ADL ability in connection with an acute hospitalization: Early clinical mark-ers in French older people. European Journal of Epidemiology, 22(9), 621–630. doi:10.1007/s10654-007-9150-1
Li, A. K., Covinsky, K. E., Sands, L. P., Fortinsky, R. H., Counsell, S. R., & Landefeld, C. S. (2005). Reports of financial disability predict functional decline and death in older patients discharged from the hospital. Journal of General Internal Medicine, 20(2), 168–174. doi:10.1111/j.1525-1497.2005.30315.x
Li, H., Leung, K. S., Wong, M. H., & Ballester, P. J. (2014). Substituting random forest for multiple linear regression improves binding affinity prediction of scoring functions: Cyscore as a case study. BMC Bioinformatics, 15(1), 291. doi:10.1186/1471-2105-15-291
Mahoney, J. E. (1999). Gender differences in hallway ambulation by older adults hospitalized for medical illness. WMJ: official publication of the State Medical Society of Wisconsin, 98(8), 40–43.
McCarthy, E. P., Phillips, R. S., Zhong, Z., Drews, R. E., & Lynn, J. (2000). Dying with cancer: Patients’ function, symp-toms, and care preferences as death approaches. Journal of the American Geriatrics Society, 48(5 Suppl.), S110–S121. doi:10.1111/j.1532-5415.2000.tb03120.x
McCusker, J., Bellavance, F., Cardin, S., Trépanier, S., Verdon, J., & Ardman, O. (1999). Detection of older people at increased risk of adverse health outcomes after an emergency visit: The ISAR screening tool. Journal of the American Geriatrics Society, 47(10), 1229–1237.
McCusker, J., Kakuma, R., & Abrahamowicz, M. (2002). Predictors of functional decline in hospitalized elderly patients: A system-atic review. Journal of Gerontology: Series A, Biological Sciences and Medical Sciences, 57A(9), M569–M577. doi:10.1093/gerona/57.9.M569
McVey, L. J., Becker, P. M., Saltz, C. C., Feussner, J. R., & Cohen, H. J. (1989). Effect of a geriatric consultation team on func-tional status of elderly hospitalized patients. A randomized, con-trolled clinical trial. Annals of Internal Medicine, 110(1), 79–84. doi:10.7326/0003-4819-110-1-79
Mudge, A. M., O’Rourke, P., & Denaro, C. P. (2010). Timing and risk factors for functional changes associated with medical hos-pitalization in older patients. Journal of Gerontology: Series A, Biological Sciences and Medical Sciences, 65A(8), 866–872. doi:10.1093/gerona/glq069
Munin, M. C., Putman, K., Hsieh, C. H., Smout, R. J., Tian, W., DeJong, G., & Horn, S. D. (2010). Analysis of rehabilitation activities within skilled nursing and inpatient rehabilitation facilities after hip replacement for acute hip fracture. American Journal of Physical Medicine and Rehabilitation, 89, 530–540. doi:10.1097/PHM.0b013e3181e29f54
Murray, A. M., Levkoff, S. E., Wetle, T. T., Beckett, L., Cleary, P. D., Schor, J. D.,…Evans, D. A. (1993). Acute delirium and functional decline in the hospitalized elderly patient. Journal of Gerontology, 48(5), M181–M186. doi:10.1093/geronj/48.5.M181
The Gerontologist, 2016, Vol. 56, No. 1
Downloaded from https://academic.oup.com/gerontologist/article-abstract/56/1/42/2605210by gueston 16 April 2018

51
Ostir, G. V., Berges, I. M., Kuo, Y. F., Goodwin, J. S., Fisher, S. R., & Guralnik, J. M. (2013). Mobility activity and its value as a prognostic indicator of survival in hospitalized older adults. Journal of the American Geriatrics Society, 61(4), 551–557. doi:10.1111/jgs.12170
Ostir, G. V., Berges, I., Kuo, Y. F., Goodwin, J. S., Ottenbacher, K. J., & Guralnik, J. M. (2012). Assessing gait speed in acutely ill older patients admitted to an acute care for elders hospital unit. Archives of Internal Medicine, 172(4), 353–358. doi:10.1001/archinternmed.2011.1615
Palleschi, L., De Alfieri, W., Salani, B., Fimognari, F. L., Marsilii, A., Pierantozzi, A.,…Zuccaro, S. M. (2011). Functional recov-ery of elderly patients hospitalized in geriatric and general medicine units. The PROgetto DImissioni in GEriatria Study. Journal of the American Geriatrics Society, 59(2), 193–199. doi:10.1111/j.1532-5415.2010.03239.x
Palleschi, L., Fimognari, F. L., Pierantozzi, A., Salani, B., Marsilii, A., Zuccaro, S. M.,…De Alfieri, W. (2014). Acute functional decline before hospitalization in older patients. Geriatrics & Gerontology International, 14(4), 769–777. doi:10.1111/ggi.12160
Pedone, C., Ercolani, S., Catani, M., Maggio, D., Ruggiero, C., Quartesan, R.,…; GIFA Study Group. (2005). Elderly patients with cognitive impairment have a high risk for functional decline during hospitalization: The GIFA Study. Journal of Gerontology: Series A, Biological Sciences and Medical Sciences, 60(12), 1576–1580. doi:10.1093/gerona/60.12.1576
Raju, D., Su, X., Patrician, P. A., Loan, L. A., & McCarthy, M. S. (2015). Exploring factors associated with pressure ulcers: A data mining approach. International Journal of Nursing Studies, 52(1), 102–111. doi:10.1016/j.ijnurstu.2014.08.002
Resnick, B., & Galik, E. (2015). Impact of care settings on resi-dents’ functional and psychosocial status. International Journal of Older People Nursing. doi:10.1111/opn.12086.
Resnick, B., Galik, E., & Boltz, M. (2013). Function focused care approaches: Literature review of progress and future possibili-ties. Journal of the American Medical Directors Association, 14(5), 313–318. doi:10.1016/j.jamda.2012.10.019
Resnick, B., Galik, E., Enders, H., Sobol, K., Hammersla, M., Dustin, I.,…Trotman, S. (2011). Pilot testing of func-tion-focused care for acute care intervention. Journal of Nursing Care Quality, 26(2), 169–177. doi:10.1097/NCQ.0b013e3181eefd94
Sager, M. A., Franke, T., Inouye, S. K., Landefeld, C. S., Morgan, T. M., Rudberg, M. A.,…Winograd, C. H. (1996a). Functional outcomes of acute medical illness and hospitalization in older
persons. Archives of Internal Medicine, 156(6), 645–652. doi:10.1001/archinte.1996.00440060067008
Sager, M. A., Rudberg, M. A., Jalaluddin, M., Franke, T., Inouye, S. K., Landefeld, C. S.,…Winograd, C. H. (1996b). Hospital admission risk profile (HARP): Identifying older patients at risk for functional decline following acute medical illness and hos-pitalization. Journal of the American Geriatrics Society, 44(3), 251–257. doi:10.1111/j.1532-5415.1996.tb00910.x
Shah, S., Vanclay, F., & Cooper, B. (1989). Improving the sensitivity of the Barthel Index for stroke rehabilita-tion. Journal of Clinical Epidemiology, 42(8), 703–709. doi:10.1016/0895-4356(89)90065-6
Sleiman, I., Rozzini, R., Barbisoni, P., Morandi, A., Ricci, A., Giordano, A., & Trabucchi, M. (2009). Functional trajec-tories during hospitalization: A prognostic sign for elderly patients. Journal of Gerontology: Series A, Biological Sciences and Medical Sciences, 64A(6), 659–663. doi:10.1093/gerona/glp015
Volpato, S., Cavalieri, M., Sioulis, F., Guerra, G., Maraldi, C., Zuliani, G.,…Guralnik, J. M. (2011). Predictive value of the Short Physical Performance Battery following hospitalization in older patients. Journal of Gerontology: Series A, Biological Sciences and Medical Sciences, 66A(1), 89–96. doi:10.1093/gerona/glq167
Volpato, S., Onder, G., Cavalieri, M., Guerra, G., Sioulis, F., Maraldi, C.,…; Italian Group of Pharmacoepidemiology in the Elderly Study (GIFA). (2007). Characteristics of nondisabled older patients devel-oping new disability associated with medical illnesses and hospi-talization. Journal of General Internal Medicine, 22(5), 668–674. doi:10.1007/s11606-007-0152-1
Wade, D. T., & Collin, C. (1988). The Barthel ADL Index: A stand-ard measure of physical disability? Disability & Rehabilitation, 10(2), 64–67. doi:10.3109/09638288809164105
Witten, I. H., & Frank, E. (2005).Data mining: Practical machine learning tools and techniques, (Morgan Kaufmann Series in Data Management Systems) (2nd ed.). San Francisco: Morgan Kaufmann Publishers Inc.
Wu, H. Y., Sahadevan, S., & Ding, Y. Y. (2006). Factors associated with functional decline of hospitalised older persons following discharge from an acute geriatric unit. Annals of the Academy of Medicine, Singapore, 35(1), 17–23.
Wu, A. W., Yasui, Y., Alzola, C., Galanos, A. N., Tsevat, J., Phillips, R. S.,…Lynn, J. (2000). Predicting functional status outcomes in hospitalized patients aged 80 years and older. Journal of the American Geriatrics Society, 48(5 Suppl.), S6–15.
The Gerontologist, 2016, Vol. 56, No. 1
Downloaded from https://academic.oup.com/gerontologist/article-abstract/56/1/42/2605210by gueston 16 April 2018