Embed Size (px)
Citation preview

Predicting inadequate spirometry technique and the use ofFEV1/FEV3 as an alternative to FEV1/FVC for patients with mildcognitive impairmentStephen Allen1, Pan Yeung2, Marek Janczewski3 and Nasir Siddique1
1 Department of Medicine, The Royal Bournemouth Hospital, Dorset, UK2 Department of Medicine, Princess Margaret Hospital, Hong Kong, China3 Poole Primary Care Trust, Dorset, UK
AbstractIntroduction and Objectives: Some patients cannot perform forced vital capacity(FVC). We conducted a study to answer three questions: Can the ability to performcomponents of spirometry be predicted by the Mini Mental State Examination(MMSE)? What proportion of subjects can perform forced expiratory volume in 3 s(FEV3) but not FVC? Does the forced expiratory volume in 1 s (FEV1)/FEV3 ratioconcord with FEV1/FVC ratio in patients with airflow obstruction?Methods: We conducted a prospective observational study of 267 patients with amean age of 79 years, including subjects with indicators of frailty. They performedspirometry and the MMSE. Spirometric recordings were compared to the Ameri-can Thoracic Society 1994 criteria.Results: FVC was achieved by 51% of patients. Inability to perform FVC waspredicted by an MMSE < 24 (specificity 94%, sensitivity of 51%). An FEV1/FEV3ratio < 80% matched a FEV1/FVC ratio < 70% (sensitivity 96%, specificity 97%).Twenty-five percent of subjects were able to reach FEV3 but not FVC; 14% of thatgroup had an MMSE < 24. Subjects with an MMSE < 20 were unable reliably toperform any spirometry.Conclusion: Patients with an MMSE < 24 are usually unable to reach FVC reliablywhen tested on a single occasion, but some can reach FEV3. Patients withMMSE < 20 cannot do spirometry. An FEV1/FEV3 ratio < 80% can be used to helpidentify patients with airflow obstruction if they are unable to perform full spirom-etry to FVC.
Please cite this paper as: Allen S, Yeung P, Janczewski M and Siddique N. Predictinginadequate spirometry technique and the use of FEV1/FEV3 as an alternative toFEV1/FVC for patients with mild cognitive impairment. The Clinical RespiratoryJournal 2008; 2: 208–213.
Introduction
Spirometry provides essential information for the accu-rate diagnosis and effective management of a number ofcommon respiratory disorders, particularly asthma andchronic obstructive pulmonary disease (COPD). Theimportance of spirometry in this context is reflected inthe recommendations for the wider use of spirometrythat are embedded in the British Thoracic Societyguidelines for the management of COPD, with empha-sis on the diagnostic potential for middle-aged and
elderly subjects (1). Diagnostic spirometry criteria forasthma, COPD and other conditions are predicated onabsolute volumes for forced expiratory volume in 1 s(FEV1) and forced vital capacity (FVC), and the FEV1/FVC ratio interpreted alongside biometric data, theclinical history, symptoms and physical signs. Elderlypeople, and some younger patients, often have difficul-ties performing spirometry (2–5). There are a numberof reasons for this, although the evidence indicates thatthe most important factors that have an adverse effecton performance are cognitive impairment, fatigue and
Key wordsairways obstruction – cognitive impairment –FEV1/FEV3 – spirometry – spirometrytechnique
CorrespondenceStephen C. Allen, MD, FRCP, Post Point A10,The Royal Bournemouth Hospital, Castle LaneEast, Bournemouth, BH7 7DW, UKTel: +44 1202 704539Fax: +44 1202 704542email: [email protected]
Received: 07 February 2008Revision received: 19 March 2008Accepted: 24 March 2008
DOI:10.1111/j.1752-699X.2008.00063.x
EthicsThis study was reviewed and approved by theDorset Research Ethics Committee and hasbeen performed according to the standardslaid down by the Declaration of Helsinki. Allparticipants gave informed consent prior tothe study
The Clinical Respiratory Journal ORIGINAL ARTICLE
208 The Clinical Respiratory Journal (2008) • ISSN 1752-6981© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd

dyspraxia (4); age is at most a weak independent pre-dictor (3), although the prevalence of cognitive impair-ment rises with age. As age, frailty and cognitiveimpairment increase, the clinical information availableto the clinician is often obscured by poor memory,comorbidities and age-related physiological changes, soit can be argued that reliable spirometry is of evengreater value as an objective measure of airflow obstruc-tion in frail elderly patients. It has been shown that olderpeople with good functional status, free-living in thecommunity, can usually perform adequate spirometryirrespective of age (6), whereas only a small proportionof frail elderly inpatients can meet agreed standards forreliable spirometry (4). It has also been found that manypatients in the frail category, or with mild to moderatecognitive impairment, can reliably perform the earlypart of spirometry, and failure to meet the standards forfull spirometry by those subjects was frequently causedby inability to sustain forced expiration or by disruptivecoughing in the later phase of the forced expiratorymanoeuvre (4). This raises the possibility that usefuldiagnostic information could be gleaned from the ratiobetween the FEV1 and forced expiratory volume in 3 s(FEV3) or 6 s (FEV6). Attempts to utilise the FEV1/FEV6 ratio as a substitute for the FEV1/FVC ratio havebeen explored by some researchers (7–13),but it is likelythat such an approach will be hampered in frail elderlygroups for the same reasons as FEV1/FVC becauseFEV6 is temporally and volumetrically close to FVC.These limitations should be less apparent for FEV3.Therefore, to explore this alternative further, we con-ducted a study to determine the proportion of oldersubjects able to perform FEV1, FEV3 and FEV6 incomparison with full spirometry to FVC, and tocompare those performances with the Mini MentalState Examination (MMSE), a general test of cognitionand praxis (14). We also set out to explore the potentialof the FEV1/FEV3 ratio to detect airflow obstruction bycomparing it with the FEV1/FVC ratio in those subjectsable to perform FVC.
Materials and methods
Subjects
We conducted a prospective observational study of 267patients with a mean age of 79 years (range 50–101). Toinclude a wide spread of subjects of differing func-tional and cognitive status, we included 120 function-ally independent outpatients and inpatients (mean age74 years, 81 female), 80 inpatients undergoing rehabili-tation (mean age 82 years, 59 female), all of whom hadat least one indicator of frailty (recurrent falls, cogni-
tive impairment, incontinence, dependence on othersto complete personal activities of daily living, inabilityto walk unaided) and 67 residents in community resi-dential care (mean age 86 years, 47 female) with at leastone of the indicators of frailty listed above. All requiredspirometry as part of their work up for suspectedobstructive airways disease. They were included inorder of presentation within each group, so were aquasi-random sample. We included subjects from theage of 50 years because clinical experience indicatedthat the proportion of patients with impairment ofcognition begins to rise at around that age. However,all but 13 of the recruited subjects were above the ageof 60 years.
Inclusion and exclusion criteria
The inclusion criteria were age 50 years or more,requiring spirometry for diagnostic or follow-up pur-poses, willing to attempt to perform spirometry and tocomplete the MMSE, willing to give written consentfor the data collected to be used for research and lack ofexclusion criteria.
The exclusion criteria were severe dementia (a pre-vious or current MMSE < 11), terminal illness, relapseof asthma or COPD not yet stable, an acute confu-sional state, dyspraxia demonstrated on neurologicalexamination, severe communication difficulties, visionor hearing too poor to perform the tests and contrain-dications to spirometry, such as recent pneumothoraxor eye surgery. We excluded people with severe demen-tia for two reasons; first, pilot studies showed that theywere almost never able to perform any part of spirom-etry reliably, and second, ethical opinion was thatpatients with severe dementia would not be able to giveinformed consent for this study.
Spirometry
Spirometry was performed by experienced and fullytrained staff using a Microlabs™ (Cardinal Health,Dublin, OH, USA) 3000 portable spirometer (commu-nity residential home and rehabilitation groups) orVitalograph™ (Maids Moretan, Buckinghamshire,UK) compact spirometer (functionally independentgroup). Both instruments were calibrated before thestudy began and a calibration check was performedaround the midpoint of the data collection. Thefactory-loaded spirometry software was used withoutmodification. Although two different spirometers wereused, thus introducing a potential source of error, thecalibration checks confirmed volume and flow differ-ences of less than 1%. Very few of the subjects had
Allen et al. Predicting inadequate spirometry technique
209The Clinical Respiratory Journal (2008) • ISSN 1752-6981© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd

previous experience of spirometry, so the staff usedexplanation, demonstration and practice to preparethem for an attempt. All then made at least threeattempts, and up to eight attempts were encouraged forpatients having difficulties achieving acceptablevolume–time curves, if they were willing to keep tryingto produce two acceptable and reproducible curvesaccording to the ATS94 criteria (15). The time betweenattempts was about 1–2 min. Real time visual displayof the spirogram was used during the procedure tohelp the subjects to complete spirometry as accuratelyas possible. Accurate spirometry was achieved if thesubject performed at least three acceptable attempts(no artefacts, satisfactory start, at least 6 s durationand/or 1 s final plateau), two of which were reproduc-ible (less than 200 mL difference between the curves atFVC and FEV1) in accordance with the ATS94 criteria(15). The data were recorded both electronically and asprinted graphs for subsequent analysis.
Recording the MMSE
The MMSE was performed before the spirometry by aseparate observer. The MMSE is a test of global cogni-tive function that is used widely in clinical medicine. Ascore of <24/30 is normally considered to indicate cog-nitive impairment (14), and that threshold has beenfound to predict inability to perform spirometry infrail inpatients (4).
Analysis of the spirometry
A separate observer analysed the spirometry by takinginto account the visual and electronic data within thecontext of the ATS94 criteria (this was the guidelineavailable at the time the study was designed and ethi-cally approved), initially to ascertain whether the crite-ria were met for full spirometry to FVC, then todetermine whether the criteria were met in terms ofacceptability at FEV1, FEV3 and FEV6. Printed curvesof the‘best blow’were then used to check FEV1 and FVCand to measure FEV3 and FEV6. For the purposes of
this study, the ‘best blow’ for full spirometry used theATS94 definition of the largest sum of FEV1 and FVC.For FEV3 and FEV6, this definition was modified to thelargest sum of FEV1 and FEV3 or FEV6, respectively.
Analysis of the MMSE
As well as recording the overall MMSE score, the inter-secting pentagon (IP) drawing component of theMMSE was analysed separately, using the guideline forscoring it as part of the MMSE. To do the IP correctly,a subject must understand the instruction, then planand perform a copy of the printed diagram with apencil; these stages are sequentially similar to thoseneeded to perform a task such as spirometry. The IPwas considered to be adequate (IP+) if it consisted oftwo shapes, each with five sides and five angles and hadtwo angles overlapping. Those not meeting that defi-nition were scored IP-.
Statistical analysis
Categorical data were tested using Yates’ chi-squaredtest and the correlation coefficient was calculated withSpearman’s formula.
Results
Of the total subjects, 137/267 (51%) met the ATS94criteria for full spirometry, and it can be seen in Table 1that those with an MMSE < 24 or IP- were signifi-cantly less likely to meet the criteria. In the functionallyindependent group, 12/120 had an MMSE < 24, com-pared with 33/80 rehabilitation patients and 29/67community residential patients. Furthermore, nosubject with an MMSE below 20 was able to dospirometry. There were no such patients in the func-tionally independent group, 11 in the rehabilitationgroup and 14 in the community residential group.Ability to do full spirometry was observed in 88/120(73%) of the functionally independent subjects and in49/147 (33%) of the frail patients (P < 0.001). There
Table 1. Comparison of Mini Mental State Examination (MMSE) and intersectingpentagon drawing (IP) results of subjects able to meet the ATS94 criteria for fullspirometry with subjects not able to meet the criteria
Met ATS94 criteriafor full spirometry
Did not meet ATS94criteria for full spirometry P
MMSE < 24 8 66 <0.0001MMSE > 23 129 64IP– 4 71 <0.0001IP+ 133 59
Predicting inadequate spirometry technique Allen et al.
210 The Clinical Respiratory Journal (2008) • ISSN 1752-6981© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd

was no significant difference between the two frailgroups; full spirometry being achieved by 25/80 (31%)of the rehabilitation patients and 24/67 (36%) of thecommunity residential patients. There was no appar-ent difference in spirometry performance betweenmen and women that was independent of cognitivescores, and numbers were not sufficient to perform areliable multivariate analysis in this domain. The pro-portion of subjects unable to perform full spirometrywas higher in patients over the age of 75 years (56%compared to 41( of those < 75 years); the differencecould again be explained by the higher prevalence of anMMSE < 24 in the older group. Visual analysis of theprinted spirometry recordings for artefacts showedthat subjects with an MMSE < 24 and/or IP- usuallyfailed to meet the full ATS94 criteria because of lack ofsustained expiratory effort or had an overtly dyspraxictechnique (such as intermittent blowing or alternatingsucking and blowing), whereas cognitively intact sub-jects who did not fulfil the criteria did so mainlybecause of disruptive coughing, usually in the later partof the manoeuvre (slight coughing was accepted if thesubject was able to continue to FVC), or fatigue, asmanifested by progressively falling recorded volumesor shorter duration of forced expiration with succes-sive attempts. For example, two of the 13 subjectsunder the age of 60 years were unable to complete fullspirometry because of severe coughing. The predictive
values of an MMSE < 24 or IP- in identifying subjectswho are unlikely to perform adequate spirometry areshown in Table 2.
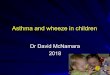
Of the 137 subjects able to perform full spirometry,53 had an FEV1/FVC ratio of less than 70% and weretherefore considered to have spirometric evidence ofairflow obstruction. The remaining 84 had an FEV1/FVC ratio of more than 69.9% and therefore did nothave spirometric support for the diagnosis of airflowobstruction. It can be seen in Table 3 that a high degreeof concordance was found between an FEV1/FVC ratioof less than 70% and an FEV1/FEV3 ratio of less than80%. Furthermore, there was a strong correlation(r = 0.959) between the two indices in patients withand without apparent obstruction (Fig. 1). An FEV1/FEV3 ratio of less than 80% was matched by an FEV1/FVC ratio of less than 70% with a high degree of
Table 2. Sensitivity, specificity, positive predictive value (PPV)and negative predictive value (NPV)(%) of an MMSE of <24 orIP- in predicting the inability of subjects to reach the ATS94criteria for full spirometry
Sensitivity Specificity PPV NPV
MMSE < 24 51 94 89 67IP- 54 97 94 69
MMSE, Mini Mental State Examination; IP, intersecting pentagon.
Table 3. Concordance between an FEV1/FVC ratio of <70% (the standard for com-parison) and an FEV1/FEV3 ratio of <80% in the diagnosis of airflow obstruction
ObstructedFEV1/FVC < 70%
Not obstructedFEV1/FVC > 69.9% P
FEV1/FVC and FEV1/FEV3concord (n)
50 82
Subjects meeting FEV1/FVCdefinition only (n)
3 2
Concordance (%) 94 98 <0.0001*
*Yates’ chi-squared test.FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; FEV3, forced expiratory volume in3 s.
0
20
40
60
80
100
120
0 20 40 60 80 100
FEV1/FVC (%)
FE
V1/
FE
V3
(%)
Figure 1. Graph showing the correlation between FEV1/FEV3and FEV1/FVC in patients able to perform full spirometry.N = 137 r = 0.959 P < 0.0001. The lines emphasise the cut-offfor FEV1/FVC = 70% (vertical) and FEV1/FEV3 = 80% (horizon-tal). Assuming an FEV1/FVC < 70% represents airways obstruc-tion, very few patients lie in the false positive (bottom right) andfalse negative (top left) rectangles.
Allen et al. Predicting inadequate spirometry technique
211The Clinical Respiratory Journal (2008) • ISSN 1752-6981© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd

specificity and sensitivity (Table 4). Similarly, an FEV1/FEV3 ratio of 80% or more was strongly associatedwith an FEV1/FVC ratio of 70% or more (Fig. 1).
Sixty-six subjects (25% of the total sample) were ableto perform acceptable and reproducible curves forFEV1 and FEV3 but not FVC. Nine of the 66 had anMMSE < 24 and 7 were IP-; none had an MMSE < 20.Only three of the subjects unable to record an accept-able FVC could perform an acceptable FEV6. On visualanalysis, the reasons for an unsatisfactory FEV6 werethe same as those for FVC. No further analysis wasmade of the FEV6 data. Sixty-four subjects (24% of thesample) were unable to perform any spirometry.
Discussion
This study showed that most functionally independ-ent older people could perform full spirometry unlessthey had cognitive impairment. The capable propor-tion was lower than that found in some previouscommunity-based studies (6), probably because unlikethose studies, our independent-living sample includeda large number of patients over the age of 75 years, inwhom subtle impairments of cognition, executivefunction and praxis were likely to be more prevalent(16). We also showed that patients falling in the frailcategory were often not able to do spirometry, usuallyas a result of cognitive impairment or fatigue. AnMMSE < 24 or IP- were predictive of a poor outcomefrom attempted spirometry. These findings generallyconfirm and reinforce previous observations that anMMSE score of less than 24 predicts inability to dospirometry with a useful degree of specificity but isrelatively insensitive and has limited negative predic-tive value. The same caveats apply to the use of IP- (4).
We found that a clinically useful percentage of peopleunable to do full spirometry could reliably reach FEV3.This raises the opportunity to consider the diagnosticutility of FEV1/FEV3 as supporting evidence of airflowobstruction in such patients.Our data indicated a broadagreement between a FEV1/FEV3 ratio < 80% andFEV1/FVC in the received obstructive range (<70%)
(17) in patients with a clinical working diagnosis ofobstructive airways disease. Of course, there are someprovisos. First, while the sample was large enough toindicate the potential to use FEV1/FEV3 in a clinicalcontext, it was not large enough to establish definitivediagnostic thresholds for the ratio. Second, it has beencontended that spirometric ratios are too simplistic anindex to use for diagnostic purposes (18), particularlyin patients with borderline readings. This is particularlythe case in old age because the lung compliance changesthat occur with normal aging reduce the FEV1/FVCratio, and hence are likely to similarly reduce the FEV1/FEV3 ratio, and might lead to over-diagnosis of mildairflow obstruction. This would need to be taken intoaccount when interpreting FEV1/FEV3, as it would befor FEV1/FVC. However, this should not be seen as amajor obstacle to the use of FEV1/FEV3, providing theindex is used carefully. Furthermore, in the same waythat discriminating power of FEV1/FVC is improved bytaking the fifth percentile as evidence of airflowobstruction rather than <70%, a fifth percentile cut-offcould be generated for FEV1/FEV3.
Nevertheless, our study points to a useful wayforward for clinicians dealing with patients who areunable, for one reason or another, to perform spirom-etry to FVC yet need objective evidence of airflowobstruction for diagnostic purposes or to track theresponse to treatment. Our data suggest that an FEV1/FEV3 ratio of less than 80% is likely to indicate thepresence of airflow obstruction. These findings are inkeeping with those of Ioachimescu (11) who derivedan estimated FVC from FEV3 using a predictive equa-tion generated from a sample of adult subjects of allages, and used the derived FVC to calculate a surrogatefor FEV1/FVC. However, our study indicates that itmight be more appropriate to establish normal andindicative ranges for FEV1/FEV3 ratio rather thanderive FVC from FEV3. A larger study is required to tryto establish a range of FEV1/FEV3 ratio and fifth per-centile cut-off values that could be used, along withother information, to support a diagnosis of, forexample, COPD or asthma. Such further work will alsoneed to include a large sample of healthy individualsacross the full adult age range. Establishing firm rangesand indicative thresholds would be particularly usefulfor patients who are unable to sustain the later part ofthe forced expiratory manoeuvre because of cough orfatigue, and some with mild to moderate cognitiveimpairment. The alternatives to spirometry eitherrequire as much or more patient cooperation (wholebody plethysmography), are expensive and not widelyunderstood (forced oscillation) or of uncertain validityin COPD (interrupter). Such alternatives are also not
Table 4. Sensitivity, specificity, positive predictive value (PPV)and negative predictive value (NPV)(%) of an FEV1/FEV3 ratio of<80% in predicting an FEV1/FVC ratio of <70% (n = 53)
Sensitivity Specificity PPV NPV
FEV1/FEV3 < 80%predictsFEV1/FVC < 70%
96 97 94 97
FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; FEV3,forced expiratory volume in 3 s.
Predicting inadequate spirometry technique Allen et al.
212 The Clinical Respiratory Journal (2008) • ISSN 1752-6981© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd

as portable, so are of less use in primary care or for frailpatients who prefer not to travel to a hospital. FEV1alone can be useful if it is normal, although a low FEV1alone does not differentiate obstructive and restrictivedefects. It can also be argued that slow vital capacity(SVC) can be used to derive FEV1/FVC in these cir-cumstances; however, we found in a pilot study thatpatients with cognitive impairment were rarely able tocomplete an SVC if they could not do forced spirom-etry. Therefore, we contend that a fresh appraisal of 3 sspirometry should be undertaken to accommodate therise in the number of patients unable to perform FVCas the population ages and cognitively impaired peoplebecome more prevalent.
Acknowledgements
There are no conflicts of interest and no commercialconnections. There was no funding, although PanYeung was a research fellow in the United Kingdom,supported by a grant from the Princess MargaretHospital, Hong Kong.
References
1. British Thoracic Society. British Thoracic Societyguidelines on the management of chronic obstructivepulmonary disease. Thorax. 1997;53(Suppl V): S1–28.
2. Bellia V, Pistelli R, Catalano F, Antonelli-Incalzi R, GrassiV, Melillo G. Quality control of spirometry in the elderly.The S.A.R.A. study. Am J Respir Crit Care Med. 2000;161:1094–100.
3. Pezzoli L, Giardini G, Consonni S, Dallera I, Bilotta C,Ferrario G, Sandrini M, Annoni G, Vergani C. Quality ofspirometric performance in older people. Age Ageing.2003;32: 43–6.
4. Allen SC, Yeung P. Inability to draw intersectingpentagons as a predictor of unsatisfactory spirometrytechnique in elderly hospital inpatients. Age Ageing.2006;35: 304–16.
5. Sherman CB, Kern D, Richardson ER, Hubert M, FogelBS. Cognitive function and spirometry in the elderly. AmRev Respir Dis. 1993;148: 123–6.
6. Lehmann S, Vollset SE, Nygaard HA, Gulsvik A. Factorsdetermining performance of bronchodilator reversibilitytests in middle-aged and elderly. Respir Med. 2004;98:1071–9.
7. Vandervoorde J, Verbanck S, Schuermans D, Kartounian J,Vincken W. Obstructive and restrictive spirometricpatterns: fixed cut-offs for FEV1/FEV6 and FEV6. EurRespir J. 2006;27: 378–83.
8. Gleeson S, Mitchell B, Pasquarella C, Reardon E, FalsoneJ, Berman L. Comparison of FEV6 and FVC for thedetection of airway obstruction in a community hospitalpulmonary function laboratory. Respir Med. 2006;100:1397–401.
9. Bellia V, Sorino C, Catalano F, Augugliaro G, ScichiloneN, Pistelli R, Pedone C, Antonelli-Incalzi R. Validation ofFEV6 in the elderly: correlates of performance andrepeatability. Thorax. 2008;63: 60–6.
10. Melbye H, Medbe A, Crockett A. The FEV1/FEV6 ratio isa good substitute for the FEV1/FVC ration in the elderly.Prim Care Respir J. 2006;15: 294–8.
11. Ioachimescu OC, Venkateshiah SB, Kavuru MS, McCarthyK, Stoller JK. Estimating FVC from FEV2 and FEV3:assessment of a surrogate spirometric parameter. Chest.2005;128: 1274–81.
12. Swanney MP, Jensen RL, Crichton DA, Beckert LE,Cardno LA, Crapo RO. FEV6 is an acceptable surrogatefor FVC in the spirometric diagnosis of airwayobstruction and restriction. Am J Respir Crit Care Med.2000;162: 917–9.
13. Vandervoorde J, Verbanck S, Schuermans D, Kartounian J,Vincken W. FEV1/FEV6 and FEV6 as an alternative forFEV1/FVC and FVC in the spirometric detection ofairway obstruction and restriction. Chest. 2005;127:1560–4.
14. Folstein FM, Folstein SE, McHugh PR. Mini-mental state:a practical method for grading the cognitive state ofpatients for the clinician. J Psychiatr Res. 1975;12: 189–98.
15. American Thoracic Society. Standardization of spirometry– 1994 update. Am J Respir Crit Care Med. 1995;152:1107–36.
16. Grigsby J, Kaye K, Shetterly SM. Prevalence of disorders ofexecutive cognitive functioning among the elderly:findings of the San Luis valley health and aging study.Neuroepidemiology. 2002;21: 213–20.
17. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS.Global strategy for the diagnosis, management, andprevention of chronic obstructive pulmonary disease.NHLBI/WHO Global Initiative for Chronic ObstructiveLung Disease (GOLD) Workshop summary. Am J RespirCrit Care Med. 2001;163: 1256–76.
18. Hansen JE, Sun XG, Wasserman K. Spirometric criteriafor airway obstruction: use percentage of FEV1/FVC ratiobelow the fifth percentile, not <70%. Chest. 2007;131:
349–55.
Allen et al. Predicting inadequate spirometry technique
213The Clinical Respiratory Journal (2008) • ISSN 1752-6981© 2008 The Authors. Journal compilation © 2008 Blackwell Publishing Ltd