Embed Size (px)
Citation preview

PREDICTING THE AIRWAY CHANGES DURING THE
COURSE OF PREGNANCY, LABOUR AND AFTER
DELIVERY USING MALLAMPATI CLASSIFICATION
AMONG INDIAN WOMEN – A PROSPECTIVE
OBSERVATIONAL STUDY.
Dissertation submitted to the Tamil Nadu Dr.M.G.R Medical University in
partial fulfilment of the rules and regulations for MD Degree examination in
Anaesthesiology to be held in April 2017.
Dr. JAYAPRAKASH ARUNACHALAM
DEPARTMENT OF ANAESTHESIOLOGY,
PSG INSTITUTE OF MEDICAL SCIENCES AND RESEARCH,
COIMBATORE 641004.
TAMIL NADU, INDIA

CERTIFICATE

CERTIFICATE
This is to certify that Dr. JAYAPRAKASH ARUNACHALAM a post
graduate student (2014-2017) in the Department of Anaesthesiology, PSG
Institute of Medical Sciences & Research, Coimbatore has done this dissertation
titled "PREDICTING THE AIRWAY CHANGES DURING THE COURSE
OF PREGNANCY, LABOUR AND AFTER DELIVERY USING
MALLAMPATI CLASSIFICATION AMONG INDIAN WOMEN." under
the direct guidance and supervision of guide Prof. Dr.C.GANESAN in partial
fulfillment of the regulations laid down by the Tamilnadu Dr.M.G.R. Medical
University.
Prof. Dr. C. GANESAN MD,DNB, PDCCA Prof. Dr. RAMALINGAM MD
HEAD OF THE DEPARTMENT PRINCIPAL
DEPARTMENT OF ANAESTHESIOLOGY PSGIMS&R
PSGIMS&R

CERTIFICATE BY THE GUIDE
This is to certify that Dr. JAYAPRAKASH ARUNACHALAM a post
graduate student (2014-2017) in the Department of Anaesthesiology, PSG
Institute of Medical Sciences & Research, Coimbatore has done this dissertation
titled "PREDICTING THE AIRWAY CHANGES DURING THE COURSE
OF PREGNANCY, LABOUR AND AFTER DELIVERY USING
MALLAMPATI CLASSIFICATION AMONG INDIAN WOMEN." under
the direct guidance and supervision of guide Prof. Dr.C.GANESAN in partial
fulfillment of the regulations laid down by the Tamilnadu Dr.M.G.R. Medical
University.
Prof. Dr. C. GANESAN MD,DNB, PDCCA
HEAD OF THE DEPARTMENT
DEPARTMENT OF ANAESTHESIOLOGY
PSGIMS&R

DECLARATION

DECLARATION
I hereby declare that this dissertation entitled "PREDICTING THE
AIRWAY CHANGES DURING THE COURSE OF PREGNANCY,
LABOUR AND AFTER DELIVERY USING MALLAMPATI
CLASSIFICATION AMONG INDIAN WOMEN" was prepared by me under
the direct guidance and supervision of Prof. Dr. C. GANESAN, PSG Hospitals,
Coimbatore.
This dissertation is submitted to the Dr.M.G.R Medical university in
partial fulfillment of the university regulations for the award of MD degree in
Anaesthesiology, Examination to be held in April 2017.
PLACE: Coimbatore Dr. JAYAPRAKASH ARUNACHALAM
DATE:




ACKNOWLEDGEMENT

ACKNOWLEDGEMENTS
At the outset I am extremely indebted to the Department of
Anaesthesiology, PSGIMS&R, Coimbatore and the Institutional Human Ethics
Committee for permitting me to carry out this thesis.
I am fortunate enough to do research with the scholarly supervision of
Professor and Head of the department Dr.C.GANESAN. His words of
encouragement, academic discussions and valuable guidance have enabled me in
completing this thesis. But for his good sense and large hearted forbearance I
would not have completed it. His contribution is visible in the outcome of this
thesis. So I record my heartfelt gratitude and indebtedness to him.
I take this opportunity to express my gratitude to Professor Dr.SEETHA
PANICKER, Head of the Department of Obstetrics and Gynaecology and other
members for providing me all facilities to undertake this research work.
It is my privilege to express my thankfulness to my revered teachers and
my colleagues of my department for helping me at various stages to complete
this thesis.
Though it is like thanking myself, my heartfelt gratitude always goes to
my parents Dr. R. Arunachalam and Dr.P.Amirtha Rani Manimekalai and
memebers of my family who shape my life with utmost care and affection.

Last but not the least I am thankful to the patients who cooperated with
me in this study for survey and Dr .S. Preethi, Post graduate, Department of
Community Medicine, Yenopaya Medical College, Mangalore for her timely
statistical assistance.
Dr. JAYAPRAKASH ARUNACHALAM
LIST OF ABBREVATIONS
ASA : AMERICAN SOCIETY OF ANAESTHESIOLOGISTS
BMI : BODY MASS INDEX
Cms : CENTIMETRES
IV : INTRAVENOUS
IV 1 : INTRAVENOUS FLUIDS GIVEN DURING FIRST
STAGE OF LABOUR
MP : MALLAMPATI
MPC : MALLAMPATI CLASSIFICATION
MP I : MALLAMPATI CLASS AT FIRST TIME INTERVAL
MP II : MALLAMPATI CLASS AT SECOND TIME INTERVAL
MP III : MALLAMPATI CLASS AT THIRD TIME INTERVAL
MP IV : MALLAMPATI CLASS AT FOURTH TIME INTERVAL
TMD : THYROMENTAL DISTANCE
TMJ : TEMPOROMANDIBULAR JOINT
VC : VOCAL CORDS

INDEX
CONTENT PAGE NO.
1) INTRODUCTON 1
2) AIMS OF THE STUDY 3
3) OBJECTIVES OF THE STUDY 4
4) REVIEW OF LITERATURE 5
5) METHODOLOGY 42
6) RESULTS 46
7) DISSCUSSION 76
8) CONCLUSION 81
9) BIBLIOGRAPHY
10) ANNEXURE

INTRODUCTION

1
INTRODUCTION
Ability to predict a difficult airway aids in conducting anaesthesia safely
and effectively by keeping all the equipment and personnel ready. A difficulty in
airway management in patients is highly stressful for an anaesthetist and
especially in obstetrics patients it is even more catastrophic1-4
.
In obstetrical anaesthesia the risk associated with difficult airway leading
to failed tracheal intubation which finally causes anaesthesia related deaths are
high. It is said that obstetric patients carry 8 times more risk than normal
population for failed intubation5.
Difficult tracheal intubation during induction of general
anaesthesia for obstetric patients remains the major contributing factor to
anaesthesia related obstetric complications. A proper preoperative evaluation is
required to anticipate and be prepared for these situations. It is also very
important to have knowledge about the factors which are more associated with
these airway changes in obstetric patients so an anaesthesiologist can have all the
equipment ready before hand and handle the situation seamlessly thereby
improving the safety of pregnant patients5.
A variety of examinations and measures are used to predict difficult
airway including Mouth opening, range of neck movements, thyromental
distance, sternomental distance etc. Mallampati classification of airway with

2
Samsoon modification is a bedside test to asses difficulty of airway by looking at
the oropharyngeal structures.
This test is universally accepted and highly specific bedside test for
assessing airway difficulty. We have used this test in our study because of its
convenience to the patient and a very good tool to assess the airway difficulty.
Numbers of studies have proven that there are changes in airway during
pregnancy and labour. These changes are mostly soft tissue changes such as
airway oedema which can increase in pregnancy which can be examined using
Mallampati classification. Studies have also suggested that airway of pregnant
women change along the course of pregnancy and labour because of various
physiological changes such as weight gain, airway oedema etc.
However there are very few studies that has suggested about the
predicting factors causing these airway changes in pregnant women. There are
many factors such as fluids administered during labour, duration of labour which
plays an important role in changing difficulty in airway along the course of the
pregnancy and labour. There are very few studies that actually correlate with
these factors.
Keeping this in mind we evaluated the changes along the course of
pregnancy and labour and even predicting factors that are more likely to cause
these airway changes in pregnant women.

AIMS OF THE STUDY
3
AIMS OF THE STUDY
To study the incidence of changes in the airway during course of
pregnancy, labour and after delivery and to predict the factors that are influential
in causing these changes.

OBJECTIVES

4
OBJECTIVES OF THE STUDY
PRIMARY OBJECTIVE
To predict the factors causing airway changes during the course of
pregnancy, labour and delivery so that an anaesthesiologist can anticipate the
difficulty beforehand and provide safer anaesthesia.
SECONDARY OBJECTIVE
To conduct a study of this kind in Indian population as all previous
studies pertaining to this topic have been done only in western population.

REVIEW OF LITERATURE

5
REVIEW OF LITERATURE
An anaesthesiologist has many responsibilities, one of the most prime
responsibilities is to secure and maintain a patent airway. Failure in doing so can
result in catastrophic events or even death6. In a study conducted by Samsoon
GL et.al. which was a retrospective study of more than 15000 patients, it was
found out that every 1 out of 2230 in general surgical patients and every 1 out of
283 in obstetric patients had a failed intubation7. So it is noted that obstetric
patients are at 8 times more risk than general surgical population for a failed
intubation.
In the meta-analysis conducted by Shiga et al that included 35 studies
with 50,760 patients the incidence of difficult intubation was 5.8% for overall
population8.
CLINICAL PRACTICE PRINCIPLES OF TRACHEAL INTUBATION
There are four principles which help in preventing complications9
Maintaining oxygenation- this is the top priority. Preoxygenation should
be done and practised regularly before induction of anaesthesia. It is better to
prevent trauma and first attempt is always the best attempt.
Equipment for difficult airway should be kept ready if any difficulty is
suspected. Call for help as soon as possible if any difficulty in tracheal
intubation is encountered.

6
INDICATIONS FOR TRACHEAL INTUBATION10
:
SURGICAL AND ANAESTHETIC –
Providing general anaesthesia.
Requirement of neuromuscular blockade for surgical procedures such
as abdominal surgeries.
Surgeries in which airway is shared such as ENT surgeries.
Patients who are at high risk for aspiration of gastric contents such as
upper GI obstruction, sepsis, trauma.
Prolonged surgery.
Surgeries that impair gas exchange.
CRITICAL ILLNESS-
Poor or impaired respiratory function leading to hypoxia/hypercarbia
which does not respond to non-invasive ventilation.
Airway protection in patients who are unable to protect their airway such
as comatose patients.
Prevention of increase in ICP in TBI patients.

7
AIRWAY ANATOMY
An anaesthesiologist should be aware of the anatomy of airway as it helps
in securing the airway without any complications11
NOSE-
It has two parts which includes external nose and internal nasal cavity.
Cribriform plate forms the roof of nasal cavity. The lateral wall is formed by
three bony turbinates. Para nasal sinuses drain into the lateral wall. The
anaesthetic consideration is
1. Nose helps in humidification of air.
2. Nasal mucosal lining is very friable and highly vascular so nasal
decongestants prior to any procedure will help in decreasing the bleeding.
3. Cribriform plate damage can cause a communication between nasal
cavity and intracranial cavity which can lead to meningitis.
FIGURE 1- ANATOMY OF THE NOSE

8
ORAL CAVITY
Hard palate and soft palate forms roof of oral cavity
Floor of the oral cavity is made up of tongue which on either side is
bounded by teeth. The posterior part of the tongue is bounded by the lingual
tonsil. Importance to anaesthetist is that if the lingual tonsil is hypertrophied can
cause difficulty on working space.
FIGURE 2- ANATOMY OF THE ORAL CAVITY

9
PHARYNX-
It is a fibro muscular tube which extends from the skull base to the
cricoid cartilages. The upper part communicates with oral cavity and nose and
lower part communicates with the oesophagus and larynx. Anaesthetic
implications are that any blind attempt of intubation can cause trauma of
pharyngeal structures and can cause bleeding and any application of greater
force can cause sub mucosal passage of the tube.
FIGURE 3- ANATOMY OF PHARYNX
10
LARYNX-
Cartilaginous structure which extends from the epiglottis to the cricoid
cartilages. It consists of cartilages which are supported by the ligaments and
muscles.
Three paired cartilages are arytenoid, cuneiform and corniculate and three
unpaired are cricoid, thyroid and epiglottis.
The laryngeal inlet is surrounded by aryepiglottic folds, epiglottis,
posterior cartilage and inter arytenoid notches. The vocal cords are attached to
the vocal process of thyroid and arytenoid cartilages. Valleculae are space
between median and lateral glossoepiglottic folds.
Importance – while performing laryngoscopy the macintosh blade is
inserted and placed into valleculae where it tenses the epiglottic ligament and it
causes elevation of the larynx.

11
FIGURE 4- ANATOMY OF LARYNX
FIGURE 5- ANATOMY OF VOCAL CORDS

12
TRACHEA
Cartilaginous structure which extends from the cricoid cartilages to the
carina. It consists of U shaped cartilaginous rings joined by trachealis muscle
and fibroelastic tissue.
FIGURE 6- ANATOMY OF TRACHEA

13
ANATOMICAL AND PHYSIOLOGICAL FACTORS12
The factors both anatomically and physiologically that take place in
pregnancy place the pregnant woman at a bigger risk than nonpregnant woman.
ANATOMICAL FACTORS12
-
Anatomical factors that place the pregnant woman at increased risks
include
1) Pregnancy-induced weight gain
2) Enlargements of breast
3) Respiratory system mucosal oedema
4) Pulmonary aspiration.
In supine position, the breasts fall back against the neck, which can
hinder both laryngoscopy and intubation.
Certain features that are present in the non-obstetric population include
total dentition, tiny mandible, restricted mouth opening, small neck, arched
palate can cause more difficulty in airway for anaesthesiologist. Several
disorders which have systemic involvement such as diabetes milletus which can
cause of glycosalation of ligaments, rheumatoid arthritis which can cause stiff
joints, sarcoidosis, and any swellings such as tumours involving the neck can
make it difficult to produce neck extension or even make it difficulty in opening
the mouth in the obstetric patient.

14
The diaphragm can be pushed above due to an increase due to enlarged
uterus at later stages in the pregnancy can cause anatomical difficulty. Moreover,
a hip wedge that is positioned incorrectly which can result in thoracic lift effect,
improperly applied cricoid pressure due to improper explanation by the
anaesthetist to the technician, lighter planes of anaesthesia due to reduced dosage
of neuromuscular blocking drugs and less opiods due to its effect on the foetus
which is common in obstetric anaesthesia during anaesthesia can also cause
difficulty in securing an airway in obstetric population. Proper education and
preparation can help us in reducing most of the adverse events associated with
difficult airway.
PHYSIOLOGICAL CHANGES12
-
Physiological changes associated with pregnancy are well known. These
physiological changes along with the anatomical changes which are already
discussed can cause severe consequences in difficult airway in obstetric
population.
Due to increase in foetal requirements a pregnant women has higher
oxygen demand and consumption to meet the foetal demands. Approximately
the oxygen consumption is 20% to 25% in pregnant women and this is achieved
by increase in respiratory rate and work of breathing. As the diaphragm is
pushed upwards in pregnancy the compliance of the chest wall is decreased
causing increase in airway pressure and basal atelectasis.

15
Due to these changes there is decrease in functional residual capacity
causing a fall in oxygen reserve which can lead to rapid desaturation during even
a small episode of apnoea can lead to hypoxic brain injury. However closing
capacity remains normal which can result in decrease of FRC/CC ratio and it
leads to closure of smaller airways than in patients with normal functional
residual capacity. When there is airway closure at normal tidal volume it will
increase in when patient is put in supine position and also the pulmonary shunt
fraction or the blood that is shunted from the pulmonary circulation which does
not take place in gas exchange increases and these patients are more prone for
hypoxemia.
Certain factors such as patients who are started on magnesium sulphate
therapy for severe pre eclampsia or for pre-term labour and patients who are on
narcotics for labour analgesia and patients with neuromuscular disorders such as
myasthenia gravis are more prone to have a profound decrease in minute
ventilation which can lead to hypoxemia or hypercapnia. This can manifest as
dangerous situations in clinical settings with patients more prone for very rapid
hypoxemia during induction of general anaesthesia.
To prevent these catastrophic events during induction of general
anaesthesia it is utmost importance to have a proper or patent airway that could
help us administering 100% oxygen to the patient. Positioning plays a major role
in oxygenating the patient before anaesthesia ,preferably a slightly head up
position helps in aligning three axis to help keep a patent airway and it helps in

16
increasing the functional residual capacity. Supine position in a pregnant woman
is dangerous as there is aortocaval compression causing decreased venous return
and that leads to hypotension by decreased cardiac output so it is better to keep a
slight left down tilt. This hypotension has been reported in 15-20% of the
patients.
Another dangerous complication in pregnant women is that they are at
increased risk for aspiration than the non-pregnant women are they are more
prone for aspiration of the contents in the stomach during induction of
anaesthesia. It occurs in almost 60% of the pregnant women at term . The reason
behind these affects are that they have increased amount of gastric acid secretion
which is also associated with decrease in pH of gastric acid along with laxity in
the sphincter action of gastroesophageal sphincter attributed to hormonal and
mechanical changes that occur in pregnancy.
The hormonal changes in the pregnancy include increased levels of
progesterone which decreases the gastric emptying and decreased pressure in the
lower oesophageal sphincter and placental gastrin hormone causes increase in
the gastric acid production and secretion. The changes become more prominent
such as to cause significant clinical effects only 12 weeks of pregnancy. The
gravid uterus attains a size to cause physical compression on stomach and it
causes to displace the stomach upwards causing pressure on the diaphragm and
also decreases the laxity of the gastroesophageal sphincter and causes more
chance of aspiration.

17
There are many other conditions in pregnancy that can cause increase in
gastric pressure such as twin gestation, lithotomy position and also
polyhydramnios. Fundal pressure applied during labour to push the foetus
downwards and help in delivery of the foetus cab increase the gastric pressure.
These are the reasons that place pregnant women at very high risk for aspiration
during general anaesthesia and it is recommended that all pregnant patients
coming for procedures that require general anaesthesia should receive anti
aspiration prophylaxis either pharmacologically or mechanically before
induction of general anaesthesia. Pharmacologically it is recommended to use
0.3 molar soidium citrate solution 25-30 ml which is non-particulate and should
be given at least 30 minutes prior to induction.
The main disadvantage associated with giving the sodium citrate is lesser
duration of action so it can‟t protect from the risk of aspiration during extubating
the patient post-surgery. To counter this problem associated with the sodium
citrate administration it is recommended to give an intravenous dosage of H2
receptor antagonist i.e. histamine receptor antagonist at least 45 minutes before
any manipulation of the airway. Cimetidine can cause severe hemodynamic
instability and can even lead to liver dysfunction so it is not being administered
anymore.
Ranitidine is the preferred drug of administration in these situations
because it is more safer and has no major hemodynamic disturbances and can
also be safely used in case of an emergency and another advantage of ranitidine

18
is that it has a duration of action of 4-6 hours so its action will help prevent
aspiration even during emergence from general anaesthesia. Proton pump
inhibitors are another class of drugs that can be used in decreasing gastric
secretions preoperatively. Omeprazole, a proton pump inhibitor is used
frequently and it takes at least 30-40 minutes to increase the pH of gastric
secretion. Metoclopramide is another agent used, it helps by prokinesis or by
increasing the motility of the gut to empty the gastric contents at a faster rate.
The main disadvantage is that is shown to cause extrapyramidal
symptoms in the mother and it can also the cross the placental barrier causing
neurobehavioral effects in the neonate as well. All these combination of drugs
discussed before are only useful and effective only if the patient has had a solid
diet recently before anaesthesia. Another method useful in these situations are
insertion of a nasogastric tube prior to induction and emptying out all the
contents and this method is useful if the pregnant woman is sedated in view of
labour analgesia. Although these methods have been carried out there is still a
risk of aspiration in pregnant population. Another method to decrease the risk of
aspiration in pregnant women is to apply cricoid pressure or Sellick‟s manoeuvre
during induction of anaesthesia.
In this method pressure applied on the cricoid cartilage compresses the
trachea downwards using the thumb and the middle finger and the aspiration is
reduced . Cricoid cartilage is preferred because it is a complete cartilaginous
structure and applying pressure on it can occlude the oesophagus preventing

19
aspiration of gastric contents properly. First the patient should be explained
about the cricoid pressure and cricoid pressure should be started at the beginning
of administration of induction agent, anaesthesiologist should ask for help of a
trained assistant and 15-20 newton of pressure should be applied on the cricoid
cartilage and the pressure should be sustained and only removed after
confirmation of position of the endotracheal tube by the anaesthesiologist.
Cricoid pressure application has been proved to reduce the incidence of
aspiration over the years and it has become a gold standard technique in
preventing aspiration in pregnant women or any patients with a full stomach
coming for general anaesthesia.
Another important factor in pregnancy that causes difficult airway in
pregnancy is that there is increase in total water composition of body leading to
fluid accumulation in mucosal membranes. The total body water composition in
pregnancy increases due to an increase in progesterone levels in the body and
also increased sodium and water retention due to over activity of the renin
aldosterone function in pregnancy.
The consequences of increased total body water can lead to fluid
accumulation in mucosal membranes causing oedema of the upper airway and
also larynx and vocal cords. This engorgement in addition to disorders such as
pre eclampsia, increased valasalva during strenuous labour and any respiratory
tract disorders can cause more oedema in airway in pregnant women causing
more difficult airway in pregnant women. Moreover, most of the patients receive

20
oxytocin during labour and an undesirable side effect of oxytocin is its
antidiuretic effect which leads to more fluid retention and causing fluid overload
and oedema which may result in decrease in working space of laryngoscopy
causing more chances of trauma and the friability of the mucosa in pregnancy
can lead to increased bleeding. Therefore, it is recommended to keep ready
smaller sized endotracheal tubes and agents which cause vasoconstriction of
mucosa with very little effect on uteroplacental vessels. Increase of tongue size
can make it problematic to draw back onto the mandibular space while
laryngoscopy. The weightiness increase that go with pregnancy is frequently 12
kg or more. Obesity has been told to extra increase risk of anaesthetic
complications in pregnant patients. An elevation in body mass index (BMI) has
been connected with an amplified risk of airway management complications
such as difficult intubation. [BMI is the weight in kilograms divided by height in
metres square. The ordinary BMI is 20-24.9; a BMI of 25-29.9 is overweight, a
BMI of 30-39.9 is obese, and a BMI more than 40 is morbidly obese. An
overweight patient weighs fewer than 20%-25% more than the expected IBW,
obese patient weigh up more than IBW (IDEAL BODY WEIGHT), and
morbidly obese patient weighs extra than twice of IBW. The breast increase that
escorts pregnancy is more prominent in the presence of disproportionate weight
gain. Intubation of these types of patients with engorged breasts is aided by the
use of a short or small handled laryngoscope and breast retraction. Good placing
of the patient aids intubation attempts and rises the likelihood of success.
Regional anaesthesia is also difficult to execute and extra-long needles should be

21
made available. Related variations in respiratory factors in adding to the
deviations due to pregnancy consist of, reduction in functional residual capacity,
total lung capacity and chest wall compliance. Additionally, there is increase in
the work of breathing because the contents in the abdominal cavity press against
the diaphragm and makes breathing difficult. Moreover, morbidly obese
pregnant women have a greater frequency of other obscuring medical conditions
such as diabetes mellitus and pregnancy induced hypertension.
Morbid obesity has been concerned as a causative factor in up to 75% of
anaesthesia associated maternal morbidity and mortality. Thus, assessment of
airway is of utmost importance. Measurement of oxygenation using oxygen
saturation in sitting and supine positions make available an early approach to
assess the grade of airway compromise and the possible for decline with more
decline in functional residual capacity. If general anaesthesia is “unavoidable”
and airway difficulty is expected, proper arranging of the patient with raised
shoulders by keeping folded towels under the occiput and place the head in
position like a sniffing position so that, the engorged breasts could be fallen off
from the neck providing more space for laryngoscopy. These tactics would
expose up the area that is lost in rolls of fat and allowing easy performance of
the laryngoscopy. In these kind of patients, the airway “gadgets” and substitute
methods of securing the airway become very important.
The bulk of pregnant women deliver without any need for airway and
ventilator support; nonetheless, when general anaesthesia is essential, the

22
changes both anatomically and physiologically that occur in pregnancy and
labour can add to difficulty with airway management thereby increasing the
threat of maternal morbidity and mortality. The commonest indication for
intubation of a pregnant patient is emergency caesarean delivery due to a
disturbing of falling foetal heart rate form. Other indications contain an
unsuccessful regional procedure preceding to a caesarean delivery, a high
blockade from a regional anaesthetic agent, systemic toxicity of local anaesthetic
agent, respiratory emergencies, and maternal cardiac asystole or arrest.

23
INCIDENCE-
Difficult intubation has been reported in 0.45 to 5.7 percentage of
intubations in pregnant women. Although a similar proportion of the general
surgical population (5.8 percentage) has difficult intubation13
, the concerns of
difficult intubation can be bigger in the pregnant population.
Failed intubation is much less common than difficult intubation, but it
occurs much more frequently in obstetric patients than in surgical patients.
Several observational studies of obstetric patients have reported failed intubation
rates of 0.26 to 0.4 percent. In contrast, in a retrospective study of 13,380
surgical patients, only 0.045 percent had failed intubation8.
STUDIES-
An identical case record study, a prospective observational study was
done in 2005-06 in 12 maternity clinics dealing with around 49 500 deliveries a
year14
.
Records were acquired from 1095 women who underwent general
anaesthesia for caesarean section, out of which 47% were classified as category I
and 18% classified as category IV. Tracheal intubation was scheduled in all the
cases with 97% undergoing rapid-sequence induction. Grading was done using
Cormack-lehane system and 3.6% had grade III and 0.6% had grade IV
laryngoscopic view. Almost 3.3% patients had a difficult intubation. Four failed
intubations among which laryngeal mask airway was used in 3 cases. In 94% of

24
cases posted electively and 64% of cases posted as an emergency. Eight cases
(1.2%) had regurgitation and one case c of aspiration (0.1%) was found out. No
cases had airway-related morbidity and mortality.
Samsoon GL et al7. conducted a study retrospectively in which patients
had previous history of failed intubation. In the same patient he found out that
there is a relationship between the degree of difficulty and the anatomy of the
oropharynx. Obstetric patients were studied initially but the study was also
extended to patients from various surgeries to increase the amount of cases
investigated. Over a 3-year period the incidence of failed intubation in obstetric
patients were 7of 1980 cases and 6 of 13,380 patients in surgical patients. So any
screening assessment which can add to our ability to foresee difficulty in
intubation must be received, as failure to intubate can in practice lead to fatality.
Kodali BS et al15
. piloted two studies to estimate airway changes during
labour. The Samsoon and Young modification of Mallampati airway class was
used in the first study. Photographs were taken at the onset and at the end of
labour. Class 4 airways were not included from initial participation. In the
second study, acoustic reflectometry was used to measure the upper airway
volumes at the onset and at the end of labour. Oral cavity volume, pharyngeal
cavity volume were calculated using acoustic reflectometry software15
.
Study I showed, the increase in airway class increased from before labour
to after labour with a significance (P<0.001). 33% patients had one grade
increase and 3 patients had 2 grades increase after labour.8 patients had class IV

25
at the end of labour and 30 patients had airway class III or class IV. Study 2,
significant decreases in oral cavity volume (P<0.05) and pharyngeal cavity
volume (P<0.05). No association was detected between airway changes during
labour and duration of sages of labour, or fluids administered during each stage
of labour in both studies. They concluded that airways can undergo change
during the process of labour. Hence, a careful airway assessment is important
just before giving anaesthesia during labour rather than gaining this information
from prelabour information.
EurRespir J et al16
. directed a study to determine whether there was upper
airway narrowing associated with pregnancy. 100 patients in the3rd trimester of
pregnancy were enrolled and 50 patients have agreed to be studied again 3
months post-delivery. 100 non pregnant patients were recruited. Acoustic
reflection was used to measure upper airway dimensions. Snoring was less
common in non-pregnant than pregnant women and pregnant women had
significantly smaller upper airway volumes than nonpregnant women at the
when seated, and smaller pharyngeal volumes in the seated, supine and lateral
position compared with the nonpregnant women. Pregnant females had lesser
pharyngeal volume compared with post labour in the seated, supine and lateral
position. In conclusion, this study confirmed increased changes and showed that
upper airways become narrower during the last trimester of pregnancy.
Another study by Izci B et al17
. Pregnant patients with pre-eclampsia
showed increased upper airway narrowing while sleeping. The study was done to

26
compare upper airway measurements in pregnant and nonpregnant women and
in pregnant women with pre-eclampsia. 50 women in the last trimester and 37
women suffering from pre-eclampsia were enrolled from the antenatal clinic and
compared with 50 nonpregnant women. Acoustic reflection was used to
measure dimensions of upper airway. Analysis was made using Student-
Newman-Keuls tests.
Snoring : 14% in non-pregnant women
: 28% in pregnant women
: 75% in pre-eclamptic women.
When in sitting, pregnant women had differences in upper airways than in
nonpregnant women, but no difference when in supine position. Study revealed
that women with pre-eclampsia have increased upper airway narrowing in both
sitting and supine position. These changes could add to the upper airway
narrowing episodes while sleeping in patients with pre-eclampsia, which can
further cause hypertension.
A study by Rocke DA et al18
. which emphasised on factors predicting
difficult airway in pregnancy showed that the capability to foresee these kind of
cases preoperatively would be of great importance. 1,500 patients undergoing
emergency and elective caesarean section under general anaesthesia underwent
preoperative airway assessment and risk factors for predicting difficult

27
intubation was recorded. Airway assessment was done using a modified
Mallampati score. Potential risk factors noted down were
1. Obesity as per BMI
2. Short neck using thyromental distance
3. Missing, protruding maxillary incisors
4. Receding mandible
5. Facial oedema and also swollen tongue.
Following induction of anaesthesia, the view seen during laryngoscopy
and difficulty in intubation were noted. Significant correlation between the view
of oropharyngeal structures and the view at laryngoscopy and difficulty in
intubation was present. Univariate analysis demonstrated a significant
association between difficult intubation and
1) Short Neck
2) Obesity
3) Missing Maxillary Incisors
4) Protruding Maxillary Incisors
5) Single Maxillary Incisor
6) Receding Mandible .
Both facial oedema (P = 0.414) and swollen tongue (P = 0.141) were not
found to be linked with difficult intubation. Multivariable analysis removed both
obesity and missing maxillary incisors as potential risk factors. Obesity was
eliminated from the study because of its very strong association with occurrence

28
of short neck. The probability of facing a difficult intubation from various
different combinations of mentioned above risk factors were determined18
.
A retrospective study by Djabatey EA et al19
. was performed of all
obstetric cases receiving general anaesthesia at hospital to find the incidence of
both difficult and failed intubation over a 8 year period. 3430 rapid sequence
general anaesthesia were given during this period and taken for study. 23
patients had difficult intubation. None of the patients had failed intubation.3
cases required awake fibreoptic intubation.
There are three keys for making a proper management of airway , which
are
1) Anticipation of difficulty by routine preoperative assessment,
2) Adequate preparation of the patient and also keeping the equipment
ready,
3) A very detailed plan of action should any complications arise.
The condition of both the foetus and the emergency of the interventional
procedure should be taken into account while dealing with obstetric patients. The
management of a difficult airway differs on whether it is predicted before or
after intubation. There is robust agreement among experts and doctors from all
over the world in airway management that definite strategies lead to better and
improved outcome. Patients in the obstetrics unit should have been assessed
airway preoperatively and also over different periods. On doing this we can be
prepared and preparation is very important to avoid catastrophe associated with

29
airway problems in obstetrics, particularly in those patients who are at risk for
caesarean delivery19
.
Evaluation of obstetrics should be done and they should include a record
of previous anaesthesia techniques used. The assessment allows the
establishment of wellbeing and rapport between the anaesthesiologist and patient
and this will be helpful when patients come for invasive procedures such as
awake intubation.
If any anatomical features that indicate there would be difficult intubation
via conventional means such as very large breasts, large tongue, difficulty in
neck flexion and massive jaw may also indicate difficult mask ventilation. If
there is any doubt about the ability to sustain airway patency then alternative
methods such as regional anaesthesia, local anaesthesia and awake intubation.

30
ASSESSMENT OF AIRWAY10
-
Identification and documentation of difficult airway before intervention is
gold standard of clinical management10
. The revolutionary article of Cass and
colleagues almost 50 years ago stresses this point. It is the first and primary step
in preparing for patient management and care. Selection of devices to aid the
airway, techniques to be done, and procedures to be done are all important on
airway evaluation. It is difficult to investigate difficult airway events all over the
world because these events occur very infrequently and a large group of
population must be studied. Numerous factors must be taken into account as
there are variety of factors that can influence airway anatomy and patients
entered into each study must be divided into several and various groups. Each
group must contain a very large number of patients. There are many other
additional problems such as expertise of the intubator. Different skill levels
among several operators present another variable into recognizing difficult and
failed intubations. In an ideal world, laryngoscopy should be performed by a
limited number of anaesthesiologists. Factors that must be organized include10
1) Type of laryngoscope as there are many different sizes,
2) The laryngoscope blade either macintosh, mc coys and millers,
3) The intubating position (sniffing position),
4) Degree of muscle relaxation,
5) The presence of a qualified trained assistant.

31
Other techniques apart from bedside evaluation to assess airway include
radiographs of the neck and other imaging techniques such as CT scans have
been supported to predict difficult intubation more accurately but these are too
costly. Newer techniques such as acoustic reflectometry are of very dubious
dependability. More specific and non-invasive measurements like bubble
inclinometer and goniometer can give us accurate measurements but these
methods have never made it to clinical practice.
SNIFFING POSITION10
-
The airway consists of 3 visual axes. They are long axis of the mouth,
axis of oropharynx and axis of larynx. In the normal neutral position of the head,
three axes form both acute and obtuse angles. To bring all these three axes into
proper alignment, McGill advised the “sniffing the morning air” position. The
true and proper sniffing position has two major components that are flexion of
cervical vertebrae and extension of atlanto-occipital joint. Cervical flexion helps
in approximating the laryngeal and pharyngeal axes. Atlanto-occipital extension
helps in bringing the oral axis into a proper and better alignment with the other
two laryngeal and pharyngeal axes. 35 degrees is the normal atlanto occipital
extension. Laryngeal opening becomes easy to visualise with optimal alignment
of these three airway axes. A reduction in gap between atlas and occiput along
with very prominent c1 spinous process can be difficult to perform
laryngoscopy. Inability to undertake the sniffing position is a very good

32
predictor of difficult intubation. Problems that can prevent the sniffing position
are
1) Cervical Vertebrae Arthritis
2) Ankylosing Spondylitis of Cervical Vertebrae
3) Cervical Vertebrae Fractures
4) Cervical Disc Protrusion
5) Atlantoaxial Subluxation
6) Cervical Vertebrae Fusion and
7) Application of Cervical Collar.
Obese patients have posterior neck pad of fat that hinder extension of
atlanto-occipital joint.
FIGURE 7 A) Normal position FIGURE 7 B) Sniffing position

33
MOUTH OPENING10
-
This is very important as it determines the amount of available space that
is present for manipulating laryngoscopes as well as endotracheal tubes20
. A
restricted mouth opening cannot accommodate both. Mouth opening depends on
the mobility of the temporomandibular joint (TMJ), which can function in 2
ways.
1) 1)Hinge like motion and
2) Gliding motion also known as translation.
The hinge like motion helps in pivoting the mandible over the maxilla.
Measuring the interincisor distance is a test to identify adequacy of mouth
opening. An interincisor distance of more than 3 cm offers adequate space for
intubation. This approximately correlates to two finger breadths. Factors which
interfere with mouth opening are
1) Masseter muscle spasm
2) TMJ dysfunction
FIGURE 8 – MEASURING INTER INCISOR GAP

34
DENTITION-
There is a high risk of damage to the teeth while instrumentation of
airway21
. There are several problems that can occur from any dental injury.
Teeth may be dislodged or broken. The main issue with broken teeth is that it
can migrate into the trachea and into the lung and cause obstruction of the lung
segment which can result in pneumonia. Any teeth that can be pulled easily with
fingers should be removed to be safe. During laryngoscopy, proper efforts
should be made to evade inserting pressure on maxillary incisors. In doing this,
laryngoscopes are placed into improper positions causing poor vision of glottis.
FIGURE 9- DENTITION

35
TONGUE-
Tongue occupies the space present in the mouth and also oropharynx.
The base of the tongue is in close proximity to the glottis. During laryngoscopy,
the base of tongue tends to fall posteriorly thus obstructing the view of the
glottis. The tongue should be displaced from its base anteriorly so that the glottis
structures can be visualised properly. The tongue is displaced with a
laryngoscope, to which Macintosh or Miller blades are attached. These
laryngoscopes help in pushing the tongue anteriorly. A large tongue fits very
poorly into mandibular space. Always a large tongue (macroglossia) is a very
good predictor of difficult intubation.
FIGURE 10- ANATOMY OF TONGUE

36
MALLAMPATI CLASSIFICATION23
-
Knowing the consequences of tongue size for effective laryngoscopy,
Mallampati SR22
predicted a system in 1985 to predict difficulty in
laryngoscopy. There is difficult laryngoscopy when not even the slightest part of
vocal cords are visualised. Mallampati along with Samsoon rationalised that a
bigger and larger tongue could be easily identified upon inspection of the mouth
opened. Both the classification systems analyse and relate the tongue size to that
of the oropharyngeal structures visualised. As discussed earlier a normal size
tongue can allow proper visualization of oropharyngeal structures. When the
tongue size increases, some oropharyngeal structures are unseen from view.
Therefore, both the investigators suggested systems that reasoned for this
premise.
Application of both Mallampati and Samsoon classification system is
very easy and is painless to the patient as it is non-invasive. “The patient is
seated in the neutral position. The mouth is opened as wide as possible and the
tongue is protruded as far as possible. Phonation is discouraged because it raises
the soft palate and allows visualization of additional structures. The observer
looks for specified anatomic landmarks. They are the fauces, pillars, uvula, and
soft palate”. The Mallampati classification system employs 3 groups and the
Samsoon classification system utilises 4 groups.

37
FIGURE-11 MALLAMPATI CLASSIFICATION
“ORIGINAL MALLAMPATI TEST23
–
Grade 1 : Faucial pillars, soft palate, and uvula could be visualized
Grade 2 : Faucial pillars and soft palate could be visualized, but
uvula was masked by base of the tongue.
Grade 3 : Only soft palate could be visualized”
“MODIFIED MALLAMPATI TEST 24–
Class 1- : Soft palate, fauces, uvula, pillars seen
Class 2 : Soft palate, fauces, uvula seen
Class 3 : Soft palate, base of uvula seen
Class 4 : Soft palate not visible at all
Class 0 : Ability to see any part of the epiglottis on mouth”

38
A retrospective study was conducted by Samsoon and Young24
and they
concluded that the Mallampati test can be used to monitor the population to
detect those patients who are at more risk for difficult airway. Patients with class
III and IV are at risk of difficult airway. Classes I and II were not associated
with any serious problems. “Since we began the study, we have been so
impressed by the positive correlation between the classification and the ease. or
otherwise, of intubation, that in our obstetric department we most vigorously
encourage early use of regional analgesia in those classified as grades III and
IV, in the hope that general anaesthesia may be avoided”.
A meta-analysis was conducted by Shiga T et al8. of various bed side
screening tests to properly predict difficult intubation, Thirty-five studies
(50,760 patients) were selected. The overall incidence of difficult intubation was
5.8%. Screening tests included the
1. Mallampati classification,
2. Sternomental distance,
3. Thyromental distance. Each and every test yielded very poor to moderate
sensitivity (20-62%) and moderate to fair specificity (82-97%).
A combination of both Mallampati classification and thyromental
distance was found to be more useful in identifying patients for difficult airway.
When used alone the screening tests that are being used carries poor
discriminative power for prediction of difficult airway. This is the limitation of
bedside tests to be used as methods for predicting difficult airway.

39
A meta-analysis was conducted by Lee etal25
. comparing both Mallampati
and modified Mallampati classification and established their specificity and
sensitivity. The Mallampati test was used properly to correctly predict the
incidence of difficult tracheal intubation in 5 studies registering12,351 patients.
The popularity of difficult intubation ranged from 5% to 13%. In the study it
was found that Mallampati classification had low sensitivities (0.35 to 0.67) and
differing specificities (0.64 to 1.04).

40
The other tests for assessing airway bed side are –
THYROMENTAL DISTANCE–
The patient is asked to extend his head atatlanto-occipital joint26
. The
structures to be identified are mentum of mandible and thyroid cartilage in
front of the neck. “Adam's apple” (thyroid notch) serves as a very good
landmark for the thyroid cartilage as it is very superficial it can be easily
identified. The distance between the two landmarks the thyroid cartilage and
mentum is measured in three ways.
1. A set of spacers can be used
2. A pocket ruler can be used
3. Observer's or even patient‟s own fingers can be used.
The normal distance between mentum and thyroid cartilage is 6.5 cm. A
distance greater than 6 cm is indicative of easy intubation. A distance of 6 cm
or less is predictive of difficult intubation.
FIGURE 12- THE ARROWED LINE SHOWING THE MENTUM AND
THE THYROID CARTILAGE IS THE THYROMENTAL DISTANCE.

41
UPPER LIP BITE TEST27
-
The modified temporomandibular test is the upper lip bite test. The
upper lip bite test is implemented by requesting the patient to move the
incisors as high as possible on the upper lip. The exercise is like to biting the
lip. If the teeth gets above or touches the vermilion border then it is easy to
predict that there is adequate space for laryngoscopy. If the teeth cannot touch
the vermilion border then it is considered as difficult intubation as there is not
much space for laryngoscopy.
FIGURE 13- A & B SHOW THAT THE VERMILION BORDER CAN BE
TOUCHED AND IT IS A PREDICTOR FOR EASY LARYNGOSCOPY.
C&D SHOW THAT THE VERMILION BORDER CANNOT BE
TOUCHED AND THAT THERE WILL NOT BE ENOUGH SPACE FOR
LARYNGOSCOPY.

METHODOLOGY

42
METHODOLOGY
This study commenced after obtaining clearance from Institutional
Human Ethics committee (IHEC) for a study period of 10 months starting from
August 2015.
Pregnant women at 32-34 weeks of gestation coming to the Outpatient
department for antenatal check-up were approached and included in this study
after explaining them about the study thoroughly and obtaining informed and
written consent.
INCLUSION CRITERIA:
1. Above 21 years
2. Indian population
EXCLUSION CRITERIA:
1. Below 21 years
2. Non-Indian population.
3. Patients who deny consent.
4. Patients with eclampsia.

43
The investigators involved in this were
1) Principal investigator : Also the observer 1 and the postgraduate involved
in this study who was responsible for explaining and obtaining written
consent, evaluation of measurements over the time periods, compilation
of study data and statistical analysis of the study.
2) Co-investigator: Guide of the study involved in studying previous
literature and also statistical analysis of the study.
STUDY DESIGN:
Observational prospective study.
SAMPLE SIZE CALCULATION:
Formula used to calculate is:
n=(z∝^2 PQ)/L^2
Where n is sample size, zα= 95% confidence interval
1.96 standard deviation
P= Population prevalence during previous studies= 37%.
Q= [100-P].
L= Allowable error (20%).
n=(〖1.96〗^2 x37x[100-37])/〖[20/100 x37]〗^2
n = 164.
Sample size of my study is 164.

44
MEASUREMENTS:
The following measurements were taken
1) Height – was measured in centimetres (cms) with the subject standing
on a flat surface with the head, shoulders and heels touching the wall.
2) Weight – was measured in kilograms (kgs) with the subject standing
on a analogue weighing machine without any support.
3) BMI was calculated in using quartet‟s index.
4) Weight gain during pregnancy was recorded from the history.
STUDY :
Each patient‟s contact information was obtained for follow up at various
time intervals. The study consists of primary investigator observing the
Mallampati classification in the subjects at four time intervals over the course of
pregnancy and labour.
TIME INTERVALS :
1st Time interval: Between 32-34 weeks of gestation where patients are
recruited from the Outpatient department.
2nd
Time interval: At the time of admission for safe confinement usually
at 40 weeks of gestation.
3rd
Time interval: 2-4 hours after delivery of the baby.
4th
Time interval: 48-72 hours after delivery.

45
DATA OBTAINED:
1) Amount of intravenous fluids administered during each single stage
of labour.
2) Duration of each single stage of labour.
Mallampati scores recorded at each time interval were stored and studied.
The change in the scores were studied and were compared to factors such as
duration of labour, BMI, Weight gain during pregnancy and amount of
intravenous fluids administered during labour.

RESULTS

46
RESULTS
All statistical analysis were done using SPSS version 20.0 Mean,
standard deviation and P value were computed for all data. Wilcoxon signed
rank test was performed to find the association between multiple variables.
Wilcoxon signed rank test30
:
Was preferred over paired T-test because the multiple variables were not
distributed equally. It is an analysis or a hypothetical statistical analysis
which is non-parametric which can be used in conditions such as when two
related samples or a single sample with repeated measurements that can help
us in assessing whether the mean ranks of the population can differ. It is also
a paired difference test. It can be used when the population cannot be
predicted or assumed properly and also as an substitute to the paired
Student's t-test.Assumptions are:
1. Data come from the same group of population and are paired.
2. Pair is selected independently and randomised.
3. An ordinal scale is used to measure the data obtained.

47
TABLE 1: DISTRIBUTION OF STUDY POPULATION IN DIFFERENT
AGE GROUPS
Frequency
in the study
Percentage Valid
Percentage
Cumulative
Percentage
<30yrs 146 89.0 89.0 89.0
>30yrs 18 11.0 11.0 100.0
Total no. 164 100.0 100.0
FIGURE 1: DISTRIBUTION OF STUDY POPULATION IN DIFFERENT
AGE GROUPS
A total of 164 pregnant women were included in the study and about 89%
of them were below 30 years of age and remaining 11% were between 30-35
years of age.
48
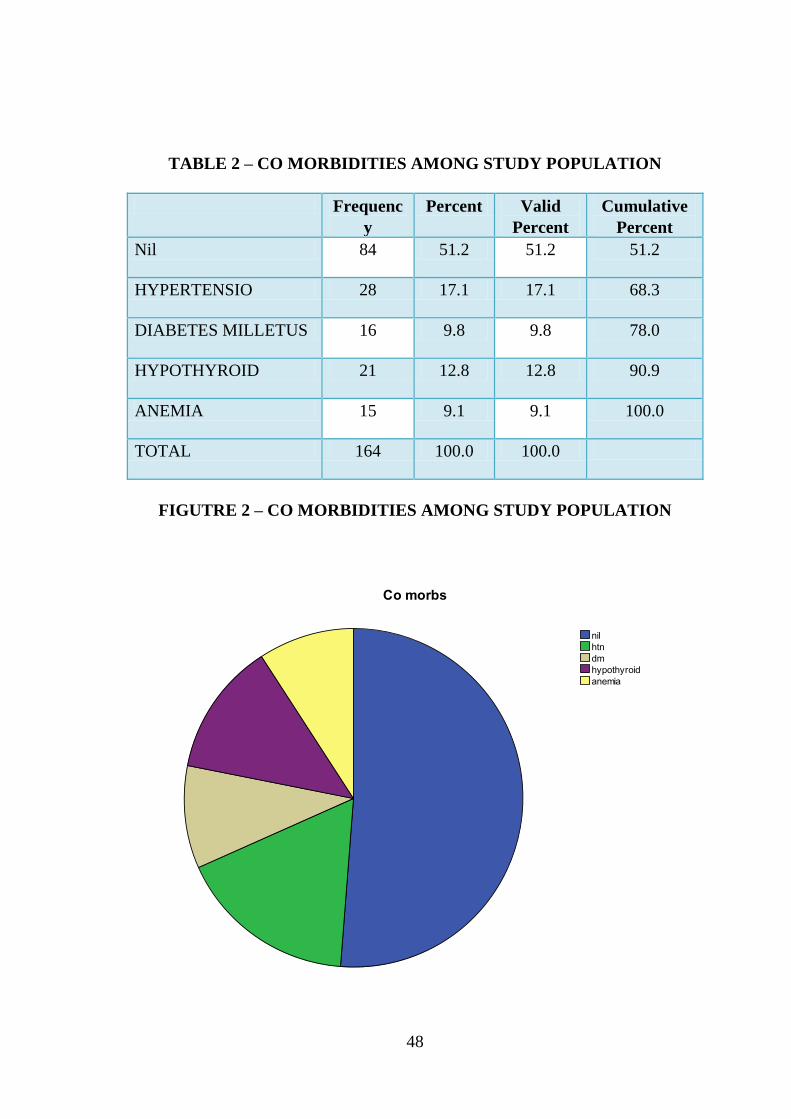
TABLE 2 – CO MORBIDITIES AMONG STUDY POPULATION
Frequenc
y
Percent Valid
Percent
Cumulative
Percent
Nil 84 51.2 51.2 51.2
HYPERTENSIO 28 17.1 17.1 68.3
DIABETES MILLETUS 16 9.8 9.8 78.0
HYPOTHYROID 21 12.8 12.8 90.9
ANEMIA 15 9.1 9.1 100.0
TOTAL 164 100.0 100.0
FIGUTRE 2 – CO MORBIDITIES AMONG STUDY POPULATION

49
TABLE 3 – WEIGHT GAIN AMONG STUDY POPULATION
Frequency Percent Valid Percent Cumulative
Percent
<15 121 73.8 73.8 73.8
>15 43 26.2 26.2 100.0
Total 164 100.0 100.0
FIGURE 3 – WEIGHT GAIN AMONG STUDY POPULATION

50
TABLE 4- DURATION OF FIRST STAGE OF LABOUR
Frequency Percent Valid Percent
Cumulative
Percent
<15hrs 21 12.8 12.8 12.8
15-20hrs 111 67.7 67.7 80.5
>20hrs 32 19.5 19.5 100.0
Total 164 100.0 100.0
FIGURE 4- DURATION OF FIRST STAGE OF LABOUR

51
TABLE 5- DURATION OF SECOND STAGE OF LABOUR
Frequency Percent Valid Percent Cumulative
Percent
Valid
<1hr 81 49.4 49.4 49.4
>1hr 83 50.6 50.6 100.0
Total 164 100.0 100.0
FIGURE 5- DURATION OF SECOND STAGE OF LABOUR

52
TABLE 6- DISTRIBUTION OF INTRAVENOUS FLUIDS IN FIRST
STAGE OF LABOUR
Frequency Percent Valid Percent Cumulative
Percent
<500ml 6 3.7 3.7 3.7
500-1000ml 138 84.1 84.1 87.8
>1000ml 20 12.2 12.2 100.0
Total 164 100.0 100.0
FIGURE 6- DISTRIBUTION OF INTRAVENOUS FLUIDS IN FIRST
STAGE OF LABOUR

53
TABLE 7 – DISTRIBUTION OF SECOND STAGE OF LBOR IN
SECOND STAGE OF LABOUR
Frequency Percent Valid Percent Cumulative
Percent
<50ml 1 .6 .6 .6
50-100ml 67 40.9 40.9 41.5
>100ml 96 58.5 58.5 100.0
Total 164 100.0 100.0
FIGURE 7 – DISTRIBUTION OF SECOND STAGE OF LBOR IN
SECOND STAGE OF LABOUR

54
TABLE 8 – BMI DISTRIBUTION AMONG SUBJECTS
Frequency Percent Valid Percent Cumulative
Percent
18.5-24.9 9 5.5 5.5 5.5
25.0-29.99 104 63.4 63.4 68.9
30.0-34.99 50 30.5 30.5 99.4
35.0-39.99 1 .6 .6 100.0
Total 164 100.0 100.0
FIGURE 8 – BMI DISTRIBUTION AMONG SUBJECTS

55
TABLE 9 – DISTRIBUTION OF GRAVIDA AMONG SUBJECTS
Frequency Percent Valid Percent Cumulative
Percent
0 1 .6 .6 .6
1 99 60.4 60.4 61.0
2 39 23.8 23.8 84.8
3 17 10.4 10.4 95.1
4 6 3.7 3.7 98.8
5 1 .6 .6 99.4
6 1 .6 .6 100.0
Total 164 100.0 100.0
FIGURE 9 – DISTRIBUTION OF GRAVIDA AMONG SUBJECTS

56
TABLE 10- DISTRIBUTION OF MALLAMPPATI CLASS 1 AMONG
TIME INTERVALS
MP I
Frequency Percent Valid Percent Cumulative
Percent
1 3 1.8 1.8 1.8
2 95 57.9 57.9 59.8
3 61 37.2 37.2 97.0
4 5 3.0 3.0 100.0
Total 164 100.0 100.0
FIGURE 10- DISTRIBUTION OF MALLAMPPATI CLASS 1 AMONG
TIME INTERVALS

57
TABLE 11- DISTRIBUTION OF MALLAMPPATI CLASS II AMONG
TIME INTERVALS
MP II
Frequency Percent Valid Percent Cumulative
Percent
1 1 .6 .6 .6
2 32 19.5 19.5 20.1
3 77 47.0 47.0 67.1
4 54 32.9 32.9 100.0
Total 164 100.0 100.0
FIGURE 11 - DISTRIBUTION OF MALLAMPPATI CLASS II AMONG
TIME INTERVALS

58
TABLE 12- DISTRIBUTION OF MALLAMPPATI CLASS III AMONG
TIME INTERVALS
MP III
Frequency Percent Valid Percent Cumulative Percent
1 1 .6 .6 .6
2 35 21.3 21.3 22.0
3 79 48.2 48.2 70.1
4 49 29.9 29.9 100.0
Total 164 100.0 100.0
FIGURE 12- DISTRIBUTION OF MALLAMPPATI CLASS III AMONG
TIME INTERVALS

59
TABLE 13- DISTRIBUTION OF MALLAMPPATI CLASS IV
AMONG TIME INTERVALS
MP IV
Frequency Percent Valid Percent Cumulative
Percent
1 2 1.2 1.2 1.2
2 50 30.5 30.5 31.7
3 92 56.1 56.1 87.8
4 20 12.2 12.2 100.0
Total 164 100.0 100.0
FIGURE 13- DISTRIBUTION OF MALLAMPPATI CLASS IV AMONG
TIME INTERVALS

60
DESCRIPTIVE STATISTICS
N Mean Std. Deviation
MP I 164 2.41 .585
MP II 164 3.12 .733
MP III 164 3.07 .731
MP IV 164 2.79 .660
This table shows the mean values of all Mallampati classes, MP I is on an
average 2.41, MP II on an average is 3.12, MP III on an average is 3.07 and MP
IV on an average is 2.79.

61
WILCOXON SIGNED RANKS TEST
Test Statisticsc
MP II -
MP I
MP III -
MP I
MP IV -
MP I
MP III -
MP II
MP IV -
MP III
MP IV
- MP II
Z -9.641a -9.312
a -7.750
a -2.000
b -6.374
b -7.086
b
Asymp. Sig.
(2-tailed) .000 .000 .000 .046 .000 .000
Based on the above non-parametric test , P <0.001 is significant.
Assosciation is found out between different classes using p value.
There is significant difference between MPI-II (z-9.641, P=<0.001)
There is no significant difference between MP II-III (z -2.000, P=<0.001)
, so this signifies that the Mallampati which was recorded at second time interval
and third interval does not differ much , Mallampati at safe confinement and
Mallampati at 2-4 hours after labour.

62
COMPARISION OF MALLAMPATI CLASS AT II AND IV TIME
INTERVALS WITH THE DURATION OF FIRST STAGE OF LABOUR
Ranks
N Mean Rank Sum of
Ranks
MP II – first stage
duration
Negative Ranks 3a 39.50 118.50
Positive Ranks 123b 64.09 7882.50
Ties 38c
Total 164
MP IV – first stage
duration
Negative Ranks 9d 39.50 355.50
Positive Ranks 98e 55.33 5422.50
Ties 57f
Total 164
a. MP II < first stage duration
b. MP II > first stage duration
c. MP II = first stage duration
d. MP IV < first stage duration
e. MP IV > first stage duration
f. MP IV = first stage duration

63
Test Statisticsb
MP II – first stage
duration
MP IV – first stage
duration
Z -9.793a -8.300
a
Asymp. Sig. (2-tailed) .000 .000
a. Based on negative ranks.
b. Wilcoxon Signed Ranks Test
This shows the significance of change in Malllampati class from 2nd
time
interval to the 4th
time interval with respect to duration of first stage of
LABOUR as both the P values are 0.000.

64
COMPARISION OF MALLAMPATI CLASS AT II AND IV TIME
INTERVALS WITH DURATION OF SECOND STAGE OF LABOUR
AND AMOUNT OF INTRAVENOUS FLUIDS ADMINESTERED
DURING SECOND STAGE OF LABOUR.
Descriptive Statistics
N Mean Std. Deviation Minimum Maximum
Second stage duration 164 1.51 .501 1 2
Second stage iv 164 2.58 .507 1 3
MP II 164 3.12 .733 1 4
MP IV 164 2.79 .660 1 4
Wilcoxon Signed Ranks Test
Ranks
N Mean Rank Sum of Ranks
MP II – second stage
duration
Negative Ranks 0a .00 .00
Positive Ranks 150b 75.50 11325.00
Ties 14c
Total 164
MP IV – second stage
iv
Negative Ranks 23d 34.61 796.00
Positive Ranks 51e 38.80 1979.00
Ties 90f
Total 164

65
a. MP II < second stage duration
b. MP II > second stage duration
c. MP II = second stage duration
d. MP IV < second stage iv
e. MP IV > second stage iv
f. MP IV = second stage iv
Test Statisticsb
MP II – second stage
duration
MP IV – second
stage iv
Z -10.847a -3.490
a
Asymp. Sig. (2-tailed) .000 .000
Exact Sig. (2-tailed) .000 .000
Exact Sig. (1-tailed) .000 .000
Point Probability .000 .000
a. Based on negative ranks.
b. Wilcoxon Signed Ranks Test
This shows the significance of Mallampati class at 2nd
time interval and
amount of intravenous fluids administered during second stage of LABOUR.

66
COMPARISION OF MALLAMPATI CLASS AT III AND IV TIME
INTERVALS WITH RESPECT TO AMOUNT OF INTRAVENOUS
FLUIDS ADMINESTERED DURING FIRST STAGE OF LABOUR
Ranks
N Mean Rank Sum of Ranks
MP III – first stage
iv
Negative Ranks 1a 45.00 45.00
Positive Ranks 125b 63.65 7956.00
Ties 38c
Total 164
MP IV – first stage
iv
Negative Ranks 4d 45.50 182.00
Positive Ranks 103e 54.33 5596.00
Ties 57f
Total 164
a. MP III < first stage iv
b. MP III > first stage iv
c. MP III = first stage iv
d. MP IV < first stage iv
e. MP IV > first stage iv
f. MP IV = first stage iv

67
Test Statisticsb
MP III – first stage iv MP IV – first stage iv
Z -10.111a -9.113
a
Asymp. Sig. (2-tailed) .000 .000
a. Based on negative ranks.
b. Wilcoxon Signed Ranks Test
This shows that there is significance P values 0.000 of change in
Mallampati class at III and IV time intervals with respect to amount of
intravenous fluids administered during first stage of LABOUR.

68
COMPARISION OF MALLAMPATI CLASS AT III AND IV TIME
INTERVALS WITH RESPECT TO AMOUNT OF FLUIDS
ADMINISTERED DURING SECOND STAGE OF LABOUR
Ranks
N Mean Rank Sum of Ranks
MP III – second
stage iv
Negative Ranks 12a 34.00 408.00
Positive Ranks 74b 45.04 3333.00
Ties 78c
Total 164
MP IV – second
stage iv
Negative Ranks 23d 34.61 796.00
Positive Ranks 51e 38.80 1979.00
Ties 90f
Total 164
a. MP III < second stage iv
b. MP III > second stage iv
c. MP III = second stage iv
d. MP IV < second stage iv
e. MP IV > second stage iv
f. MP IV = second stage iv

69
Test Statistics
MP III – second
stage iv
MP IV – second stage
iv
Z -6.709 -3.490
Asymp. Sig. (2-tailed) .000 .000
a. Based on negative ranks.
This shows that there is significance P values 0.000 with increase in
Mallampati class at III and IV time intervals with respect to amount of
intravenous fluids administered during second stage of LABOUR.

70
COMPARISION OF MALLAMPATI CLASS AT I AND II TIME
INTERVALS WITH RELATION TO WEIGHT GAIN DURING
PREGNANCY
Ranks
N Mean Rank Sum of Ranks
MP I – Weight
gain
Negative Ranks 0a .00 .00
Positive Ranks 147b 74.00 10878.00
Ties 17c
Total 164
MP II – Weight
gain
Negative Ranks 0d .00 .00
Positive Ranks 163e 82.00 13366.00
Ties 1f
Total 164
a. MP I <Wt gain
b. MP I >Wt gain
c. MP I = Wt gain
d. MP II <Wt gain
e. MP II >Wt gain
f. MP II = Wtgainnew

71
Test Statisticsb
MP I - Wtgainnew MP II - Wtgainnew
Z -11.073a -11.473
a
Asymp. Sig. (2-tailed) .000 .000
a. Based on negative ranks.
b. Wilcoxon Signed Ranks Test
This shows that there is significance P values 0.000 in increasing
Mallampati class at 1st and 2
nd time intervals.

72
COMPARISION OF MALLAMPATI CLASS AT I AND II TIME
INTERVALS WITH RESPECT TO GRAVIDA OF THE PATIENT
Ranks
N Mean Rank Sum of Ranks
MP I –
Gravida
Negative Ranks 20a 53.43 1068.50
Positive Ranks 108b 66.55 7187.50
Ties 36c
Total 164
MP II –
Gravida
Negative Ranks 10d 44.75 447.50
Positive Ranks 138e 76.66 10578.50
Ties 16f
Total 164
a. MP I <Gravida
b. MP I >Gravida
c. MP I = Gravida
d. MP II <Gravida
e. MP II >Gravida
f. MP II = Gravida
73
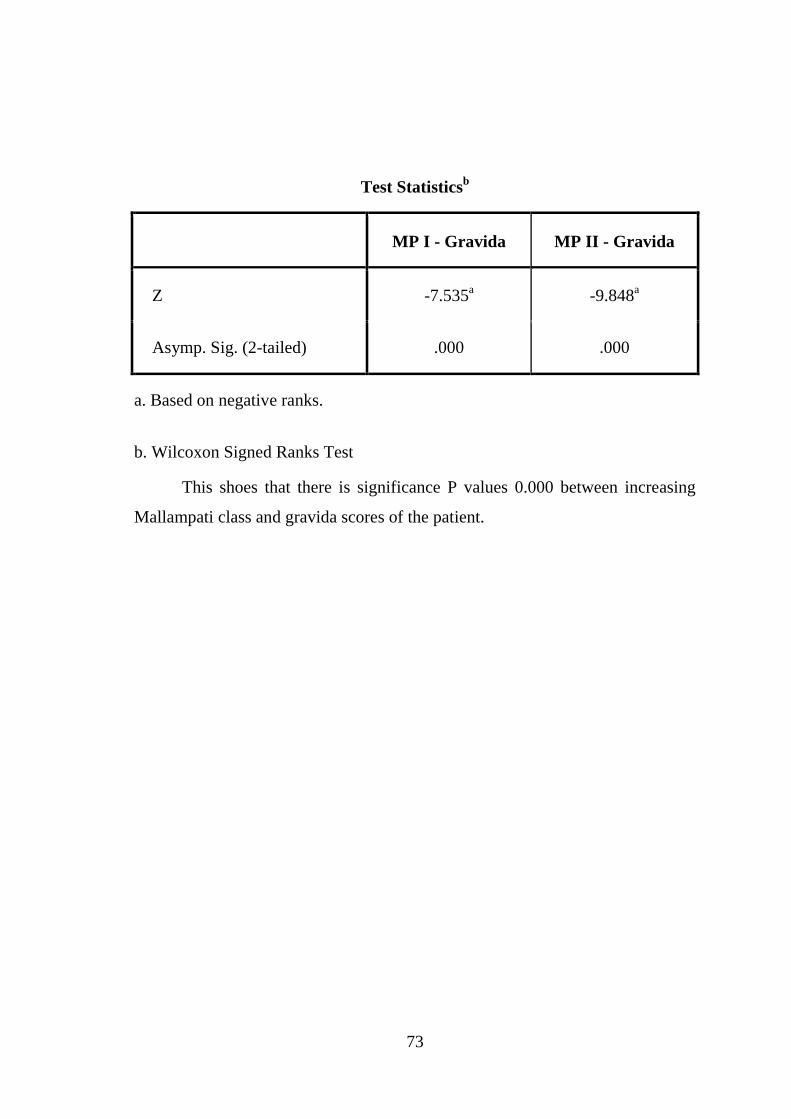
Test Statisticsb
MP I - Gravida MP II - Gravida
Z -7.535a -9.848
a
Asymp. Sig. (2-tailed) .000 .000
a. Based on negative ranks.
b. Wilcoxon Signed Ranks Test
This shoes that there is significance P values 0.000 between increasing
Mallampati class and gravida scores of the patient.

74
COMPARISION OF MALLAMPATI CLASS AT I AND II TIME
INTERVALS IN RESPECT TO BODY MASS INDEX OF THE
PATIENTS
Ranks
N Mean Rank Sum of Ranks
MP I – BMI
Negative Ranks 119a 60.59 7210.00
Positive Ranks 1b 50.00 50.00
Ties 44c
Total 164
MP II – BMI
Negative Ranks 42d 31.74 1333.00
Positive Ranks 20e 31.00 620.00
Ties 102f
Total 164
a. MP I < BMI
b. MP I > BMI
c. MP I = BMI
d. MP II < BMI
e. MP II > BMI
f. MP II = BMI

75
Test Statisticsb
MP I - BMI MP II – BMI
Z -10.110a -2.853
a
Asymp. Sig. (2-tailed) .000 .004
a. Based on positive ranks.
b. Wilcoxon Signed Ranks Test
This shows that there is significance P values 0.000 between increasing
Mallampati class at I and II time intervals in relation to BMI.

DISCUSSION

76
DISCUSSION
Safe conduct of anaesthesia and maintenance of is an important goal for
an anaesthesiologist. Obvious airway abnormalities initiate a chain of
communications that help in getting valuable assistance; however unrecognized
difficult airway may lead to serious consequences. Several clinical tests over
many years have been suggested for recognizing patients who may have difficult
airway preoperatively but unfortunately there is still no specific test that can
accurately predict a difficult airway. As discussed before difficult intubation
remains the most important and prevalent condition to cause anaesthesia related
morbidity and mortality in obstetric population. So it remains of top priority for
an anaesthesiologist to tackle this problem.
There have been many studies which has discussed about airway
changes in pregnancy and many of the studies have shown that airway changes
in pregnancy are very much prevalent and found that airway gets more difficult
as the pregnancy progresses. But only a few studies have been conducted to
predict the factors causing these changes in airway in pregnancy. So our study
was aimed to study as to predict the factors causing these changes. Predicting
these factors can help an anaesthesiologist in anticipating difficult intubation
beforehand and be prepared for the challenge.
Previous studies conducted were from western countries and a study of
this kind has not been conducted in Indian population. According to Indian
literature airway changes during pregnancy was not a major factor in obstetrics

77
because it was believed that airway changes does not occur much in pregnancy
due to high incidence of malnutrition and less weight gain during pregnancy. But
nowadays as obesity is becoming more prevalent and improvement of nutritional
status among Indian women because of education and awareness has shown
more incidence of pregnancy related disorders becoming a major concern. This
increased prevalence in obesity and weight gain in recent times have led
increased changes in airway over the course of pregnancy , so Indian population
also are more prone for difficult intubation airway related morbidity and
mortality in obstetrics. No studies have been conducted to suggest this in Indian
population. Our Study shows that almost in 64% of pregnant women airway has
changed from either Mallampati 1or 2 to Mallampati 3or 4 in Indian population.
This shows the changing trend in Indian population.
The even more important part is to find or predict the factors causing
these changes . No study of such has been done in Indian population. Our study
aims at predicting the factors causing these changes in airway in Indian
population.
Our study has been done at PSG institute of Medical sciences and
research, Coimbatore, Tamil nadu, India by recruiting patients coming to the
outpatient department of obstetrics. Study was done as discussed in the
methodology.
In a study conducted by Pilkington and colleagues28
where they examined
the Mallampati class in pregnant women at two different time intervals. The time

78
intervals were at 12 weeks of gestation and 38 weeks of gestation. They found
out that there was significant increase in Mallampati class at 38 weeks of
gestation. There was34% increase of class IV at 38 weeks of gestation. They
emphasized a relationship between airway change and body weight gain during
pregnancy. “We observed a increase in patient‟s Mallampati class that was
significant (P< 0.001) and we also found that increase in body weight was
predictive for airway changes”. The average body weight gain in their study was
11 kg but it was 14.3 kg in our study. Consequently, it is possible that there is
increase in Mallampati class connected to increased gain in body weight can
occur before 33 weeks of gestational period.
Studies comparing BMI and increase in Mallampati during pregnanacy
are not found. In our study we compared BMI of the patients with changing
Mallampati scores in pregnancy and found out that average BMI was 26.5 and
there was a significant (P>0.001) association between increase in BMI and
increase in Mallampati during pregnancy.
In a study, Kodali and colleagues15
reported that there was significant
change in Mallampati class during pregnancy and labour and also found that
there is 1.7 times elevation in the Mallampati classes III and IV in the post-
partum in compared to pre-labour evaluation. From the findings we have
analysed in our study there were similar results accounting for almost 64%
increase in Mallampati scores evaluated pre and post labour. Agreeable with the
findings of Kodali and colleagues' findings, we succeeded in identifying the

79
factors that can be predicted to cause increase in Mallampati class. This can be
attributed to the airway oedema that can be caused by fluid accumulation and
increased straining or Valsalva efforts. We concluded that two important factors
such as volume of fluids administered intravenously during first stage of labour
and durations of both first stage of labour and second stage of labour might be
very potential factors that can cause airway changes in pregnant women.
So in our study we have decided to measure and the amount of
intravenous fluids being administered during first and second stage of labour.
We have found out that the amount of fluid being administered during first stage
of labour that there was significant ( P<0.001) increase in Mallampati from class
1or 2 to 3or 4 .
It is hypothesized that prolonged valsalva efforts during labour causing
fluid accumulation of fluid causing oedema of upper airway leading to difficult
airway in pregnant women. So we have decided to calculate the duration of the
first stage and second stage of labour. In our study we have found out that the
average first stage of labour duration was 16.2 hours and there was significant
(P<0.001) change in Mallampati scores. The average second stage of labour
duration was around 45 minutes and found out that there was no significant
(P>0.001) association with changes in the Mallampati scores. This may be
attributed to the fact that majority of the valsalva are done in first stage of labour
to help in delivery of foetus, whereas in second stage of labour the number of
valsalva done are reduced as the foetus is delivered.

80
Finally, we even evaluated whether or not the Mallampati class changes
that were present immediately after labour reversed after 48-72 hours after
delivery of foetus and also whether or not we can predict the second stage of
labour duration and the amount of intravenous fluids given during labour can be
predictive. Our results showed significant trend that there is increase of
Mallampati class in pregnant women who had Mallampati class III or IV
throughout labour, but these changes did not get fully reversed even after 48
hours post-labour in patients who had reached Mallampati class IV. We suggest
that according to our study we could identify factors such as amount of
intravenous fluids administered during first stage of labour and duration of first
stage of labour were the predictive factors that anticipated the presence of
increase in Mallampati class at 48 hours after delivery of the foetus.
In a study conducted by M.BOUTTONETT 29
published in the British
Journal of Anaesthesia in 2005 they have found that majority of the pregnant
women have undergone airway changes but they were not able to predict the
factors associated with airway changes as the couldn‟t find any significant
changes with amount of intravenous fluids administered and duration of labour.
In our study we have found that there is significant association between airway
changes and factors such as weight gain , BMI, fluids administered during first
stage of labour and also duration of first stage of labour.

CONCLUSION

81
CONCLUSION
This is a observational prospective study which consists of 164 subjects
who were examined over their period of pregnancy and labour at four different
time intervals. The Mallampati class was studied over these periods and also the
predicting factors such as weight gain during pregnancy, body mass index,
duration of first and second stage of labour and amount of intravenous fluids
administered during first and second stage of labour were noted.
Statistical analysis was done by Wilson‟s signed rank test which is a
nonparametric test used as there are many variables to be studied.
We conclude that in our study the change in Mallampati class of the first
interval i.e.; at 32-34 weeks compared to change in Mallampati class at third
interval i.e.; at 4-6 hours after delivery of the baby is present in 64% of the study
population.
On evaluating the different factors causing these changes we have found
that there is a strong association between the BMI of the patient and the change
in Mallampati score as patients over BMI of 25 were significant ( P <0.001) with
respect to Mallampati score. We conclude that BMI over 25 is a predictive factor
of increasing Mallampati class during the course of pregnancy and labour.
We found that weight gain over 15 kilograms during pregnancy has
significant ( P< 0.001) association with increasing trend of Mallampati class
over course of pregnancy an labour.

82
We also found that duration of first stage of labour carries a higher
significance (P <0.001) in increasing the Mallampati score which is attributed to
increased number of valsalva manoeuvres causing airway oedema. However the
duration of second stage of labour did not have a significance (P > 0.001) with
increasing in Mallampati score which may be due to less straining and decreased
duration.
Intravenous fluids given during the first stage of labour also had a
significance (P <0.001) in increasing Mallampati class during the course of
labour.
We conclude our study by postulating that there is definitive increase of
Mallampati class during the course of pregnancy and labour and factors that can
used to predict these changes are weight gain during pregnancy, Body mass
index (BMI), duration of first stage of labour and intravenous fluids
administered during first stage of labour.
Any pregnant woman coming for anaesthesia should be properly
examined and all the mentioned factors should be noted and taken into
consideration by an anaesthesiologist and be prepared for a difficult airway
situation.

BIBLIOGRAPHY
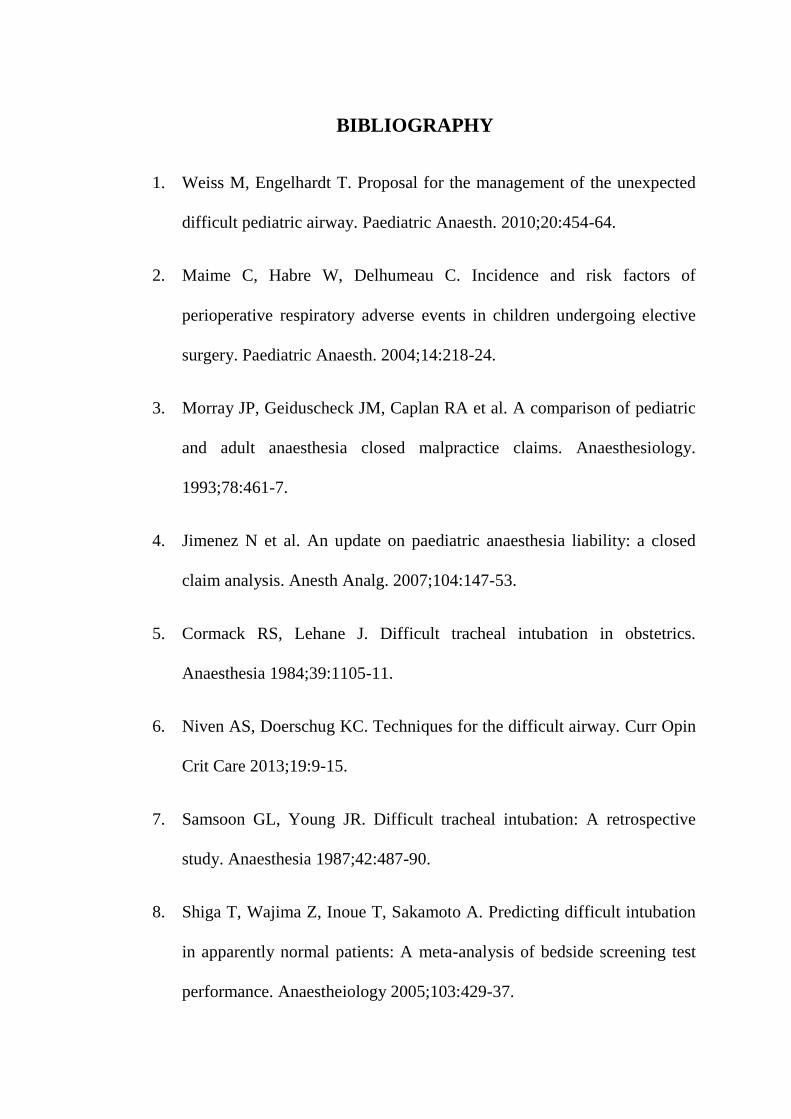
BIBLIOGRAPHY
1. Weiss M, Engelhardt T. Proposal for the management of the unexpected
difficult pediatric airway. Paediatric Anaesth. 2010;20:454-64.
2. Maime C, Habre W, Delhumeau C. Incidence and risk factors of
perioperative respiratory adverse events in children undergoing elective
surgery. Paediatric Anaesth. 2004;14:218-24.
3. Morray JP, Geiduscheck JM, Caplan RA et al. A comparison of pediatric
and adult anaesthesia closed malpractice claims. Anaesthesiology.
1993;78:461-7.
4. Jimenez N et al. An update on paediatric anaesthesia liability: a closed
claim analysis. Anesth Analg. 2007;104:147-53.
5. Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics.
Anaesthesia 1984;39:1105-11.
6. Niven AS, Doerschug KC. Techniques for the difficult airway. Curr Opin
Crit Care 2013;19:9-15.
7. Samsoon GL, Young JR. Difficult tracheal intubation: A retrospective
study. Anaesthesia 1987;42:487-90.
8. Shiga T, Wajima Z, Inoue T, Sakamoto A. Predicting difficult intubation
in apparently normal patients: A meta-analysis of bedside screening test
performance. Anaestheiology 2005;103:429-37.

9. Miller textbook of Anaesthesia 7th
edition; chapter 50. Page 1586.
10. Benumof‟s Airway management 2nd
edition- 2008.
11. Miller textbook of Anaesthesia 7th
edition; chapter 50. Page 1574.
12. Munnur, Uma MD; de Boisblanc, Ben MD; Suresh, Maya S. MD. Critical
Care Medicine:October 2005 - Volume 33 - Issue 10 - pp S259-S268.
13. Crosby ET, Cooper RM, Douglas MJ, Doyle DJ, Hung OR, Labrecque P
et al. The unanticipated difficult airway with recommendations for
management. Can J Aneasth 1998;45:757-76.
14. Rahman K, Jenkins JG. Failed tracheal intubation in obstetrics: no more
frequent but still managed badly. Anaesthesia 2005; 60:168.
15. Kodali BS, Chandrasekhar S, Bulich LN, et al. Airway changes during
labor and delivery. Anesthesiology 2008; 108:357.
16. Ezri, T., Medalion, B., Weisenberg, M. et al. Can J Anaesth (2003) 50:
179. doi:10.1007/BF03017853.
17. Izci B, Riha RL, Martin SE, et al. The upper airway in pregnancy and pre-
eclampsia. Am J Respir Crit Care Med 2003; 167:137.
18. Rocke DA, Murray WB, Rout CC, Gouws E. Relative risk analysis of
factors associated with difficult intubation in obstetric anesthesia.
Anesthesiology 1992; 77:67.

19. Djabatey EA, Barclay PM. Difficult and failed intubation in 3430
obstetric general anaesthetics. Anaesthesia 2009; 64:1168.
20. Sunanda Gupta, Rajesh Sharma KR, Dimpel Jain. Airway assessment:
predictors of difficult airway; Indian J. Anaesth. 2005; 49(4):257-262.
21. Oven H, Waddell Smith I. Dental trauma associated with anaesthesia.
Anaesthes intensie care 28:133-145,2000.
22. S. Rao Mallampati MD, Stephen P, Gatt MD, Laverne D. A Clinical sign
to predict difficult tracheal intubation: a prospective study: pdf p 429-
434:2002.
23. Mallampati SR. Clinical sign to predict difficult tracheal intubation
(hypothesis). Can Anaesth Soc J 1983; 30: 316-7.
24. Difficult tracheal intubation: a retrospective study. Samsoon and Young:
Anaesthesia 1987 May(5), 487-90.
25. Lee A, Fan L T, Gin T. A systematic review of accuracy of Mallampati
test to predict difficult airway: Anae anal 102:1867-1878,2006.
26. P A Baker, JMD Thomson: Thyromental distance measurement- finger
don‟t rule: Anaesthesia, vol 64, issue 8, page 878-882 Aug 2009.
27. Leopold H, J.Eberhart; Reliability and validity of upper lip bite test
compared with Mallampati classification to predict difficult
laryngoscopy: a prospective evaluation: Anaes Analg 2005:101:284-9.
28. Pilkington S, Carli F, Dakin MJ, et al. Increase in Mallampati score
during pregnancy. Br J Anaesth 1995; 74:638.
29. Boutonnet M, Faitot V, Katz A, et al. Mallampati class changes during
pregnancy, labour, and after delivery: can these be predicted? Br J
Anaesth 2010; 104:67.
30. Lowry, Richard. "Concepts & Applications of Inferential Statistics".
Retrieved 24 March 2011.

ANNEXURES

ANNEXURES
CONFIDENTIALITY FORM
From,
Dr.JAYAPRAKASH ARUNACHALAM,
POST GRADUATE,
DEPARTMENT OF ANAESTHESIOLOGY,
PSGIMS&R,
COIMBATORE.
TO WHOMSOEVER IT MAY CONCERN
I, Dr.JAYAPRAKASH ARUNACHALAM, am undertaking a study titled
‟ PREDICTING THE AIRWAY CHANGES DURING THE COURSE OF
PREGNANCY, LABOUR AND AFT ER DELIVERY USING
MALLAMPATI CLASSIFICATION AMONG INDIAN WOMEN.‟
I hereby assure that the data taken will be used only for the approved
study and the subject information and subject identity will not be revealed to
anybody under any circumstances.
Thanking you,
Yours sincerely,
Signature of PI Signature of Co-investigator/s:
Date:

Application form for requesting Waiver of Written Informed Consent/
waiver of consent
(To be filled by PI)
1. Proposal Number :
2. Principal Investigator‟s name:
3. Department:
4. Title of project:
5. Names of co-investigators:
6. Request for waiver of informed consent:
Please check the reason(s) for requesting waiver
1. Research involves „not more than minimal risk‟
2. There is no direct contact between the researcher and participant
3. Emergency situations
4. Any other (please specify)
I hereby assure that the rights of the participants will not be violated.
Undertaking: I hereby declare that contents of the soft and hard copies of this
document submitted to the IHEC are the same.
Principal Investigator‟s signature with date:

CONSENT FORMS IN TAMIL


DATA COLLECTION PROFORMA
NAME :
AGE :
OCCUPATION :
ADDRESS AND CONTACT INFO :
OBSTETRIC SCORE :
HEIGHT :
WEIGHT :
BMI :
LMP AND EDD :
GAIN IN BODY WEIGHT DURING PREGNANCY:
CO-MORBID ILLNESS :
MALLAMPATI AT 1ST
TIME INTERVAL:
MALLAMPATI AT 2ND
TIME INTERVAL:
MALLAMPATI AT 3RD
TIME INTERVAL:
MALLAMPATI AT 4TH
TIME INTERVAL:
DURATION OF 1ST
STAGE OF LABOUR:
DURATION OF 2ND
STAGE OF LABOUR:
AMOUNT OF INTRAVENOUS FLUIDS GIVEN IN 1ST
STAGE OF
LABOUR :
AMOUNT OF INTRAVENOUS FLUIDS GIVEN IN 2ND
STAGE OF
LABOUR :


MASTER CHART

MASTER CHART
S No. Age Weight Height BMI Wt gain Gravida Para Live Abortion MP I MP II MP III MP IV 1st stage 2nd stage IV 1st IV 2nd Co morbs
1 29 85 170 29.4 18 2 1 0 1 3 4 4 3 20 2 620 130
2 26 62 150 27.6 11 1 0 0 0 3 3 3 3 21 2 500 180
3 29 64 153 27.3 17 2 1 0 1 2 3 3 2 18 1 380 100 1
4 31 70 162 26.7 13 1 0 0 0 2 2 2 2 21 1.45 800 190
5 29 72 158 28.8 16 3 1 1 2 2 4 4 3 15 1 620 280 3
6 22 80 165 29.4 13 1 0 0 0 2 3 3 2 18 1.3 500 250
7 28 72 152 31.2 17 1 0 0 0 2 4 4 3 20 2 760 400
8 24 66 151 28.9 12 2 0 0 1 2 3 3 3 21 2 780 120
9 26 78 163 29.4 15 1 0 0 0 1 3 3 2 23 2.3 1000 250 4
10 22 68 160 26.6 12 1 0 0 0 2 3 3 1 20 1.3 750 180
11 26 68 160 26.6 15 1 0 0 0 2 3 3 2 22 1.45 650 170
12 28 63 149 28.4 12 1 0 0 0 2 2 2 2 19 2 800 125
13 23 78 168 27.6 11 2 1 1 0 2 2 2 2 16 1 700 300
14 25 73 162 27.8 16 1 0 0 0 2 4 4 3 21 2.3 720 200 3
15 25 60 153 25.6 15 2 0 0 1 2 4 4 3 18 1 500 100
16 25 68 158 27.2 11 4 1 1 2 2 3 3 3 14 1 450 75
17 29 72 152 31.2 13 2 1 1 0 2 3 3 2 15 1 600 125 2
18 27 68 162 25.9 14 1 0 0 0 2 3 3 3 19 2 800 150
19 27 76 164 28.3 13 2 0 0 1 3 3 3 3 16 1.3 550 200 1
20 25 77 159 30.5 16 1 0 0 0 3 4 4 4 18 1 600 150 1
21 22 65 154 27.4 16 1 0 0 0 2 4 4 3 22 2 780 120 2
22 23 79 165 29 17 2 1 1 0 2 4 3 3 21 1 650 120 1
23 25 78 165 28.7 15 1 0 0 0 3 3 3 3 20 2 800 130 4
24 23 67 159 26.5 16 1 0 0 0 3 4 3 3 18 1.3 650 110
25 32 68 165 25 13 2 1 0 1 2 4 3 3 16 1.2 750 130 2

26 22 75 163 28.2 16 1 0 0 0 2 3 3 3 19 2 860 140
27 22 65 163 24.5 12 1 0 0 0 2 2 2 2 17 1.2 600 100
28 25 78 163 29.4 16 2 0 0 1 3 4 3 3 18 2 550 120 1
29 27 69 154 29.1 11 1 0 0 0 3 3 3 3 17 2 600 110
30 23 77 167 27.6 14 1 0 0 0 2 4 4 3 18 2 700 110 2
31 26 66 171 22.6 10 1 0 0 0 1 2 2 2 16 1 570 80
32 27 65 165 23.9 14 1 0 0 0 2 2 2 2 18 2 650 100
33 26 87 167 31.2 18 1 0 0 0 3 4 4 4 17 1 880 120 1
34 26 76 164 28.3 16 1 0 0 0 2 3 3 2 20 2 670 170
35 34 82 174 27.1 15 1 0 0 0 3 3 3 3 22 2 860 120
36 29 65 154 27.4 14 2 1 1 0 2 3 3 3 16 1 670 110 3
37 26 68 164 25.3 11 3 2 1 1 3 4 3 3 17 1 560 80
38 22 76 165 27.9 16 1 0 0 0 2 3 3 3 21 2 800 120
39 23 76 156 31.2 18 1 0 0 0 3 4 4 4 22 1 780 120 1
40 26 58 153 24.8 9 3 2 1 1 2 2 2 2 15 1.2 520 75 4
41 29 75 148 34.2 15 2 1 0 1 3 4 4 3 18 2 680 80 1
42 22 80 154 33.7 16 1 0 0 0 4 4 4 4 16 2.3 890 90 3
43 29 67 165 24.6 10 3 1 1 1 2 3 3 3 17 2 660 100
44 23 75 153 32 14 2 0 0 1 2 3 3 2 17 1.3 880 80 1
45 22 64 160 22.1 11 1 0 0 0 2 2 2 2 19 1.5 760 90
46 26 77 168 27.3 14 1 0 0 0 2 3 4 3 18 2 1100 120
47 29 66 155 27.5 10 3 2 2 0 2 3 3 3 13 1 600 75 4
48 22 67 160 26.2 13 1 0 0 0 2 3 3 2 19 2 850 80
49 25 76 156 31.2 16 1 0 0 0 3 4 4 4 20 2 1200 150
50 26 80 167 28.7 14 1 0 0 0 3 4 4 3 23 1.45 1000 150 1
51 22 76 153 32.5 15 1 0 0 0 2 3 3 3 19 2 900 120
52 33 75 163 26.3 10 1 0 0 0 2 3 3 3 21 1.45 1000 120 2
53 29 68 150 30.2 16 1 0 0 0 3 4 4 3 20 1.3 900 100 3

54 23 55 142 27.3 8 1 0 0 0 2 3 2 2 21 2 800 75 1
55 23 58 152 25.1 10 1 0 0 0 2 2 2 2 20 1.3 850 100
56 31 65 152 28.1 12 1 0 0 0 2 3 4 3 17 1 900 100
57 23 78 169 27.3 14 1 0 0 0 2 4 4 2 19 2 800 75 3
58 23 67 149 30.2 13 1 0 0 0 3 4 3 3 20 2 1000 90
59 22 89 168 31.5 17 1 0 0 0 4 4 4 4 17 1.5 800 80 3
60 26 65 153 27.8 11 1 0 0 0 2 3 3 3 19 2 1000 100
61 22 77 160 30.1 13 2 1 1 0 2 3 3 3 16 1 800 90
62 35 85 166 30.8 16 3 0 0 2 3 4 4 3 13 1 1000 100 1
63 25 77 145 36.6 16 3 1 1 0 3 4 4 4 17 2 800 100 3
64 31 67 162 25.5 11 4 1 2 1 3 3 3 3 18 1 900 150 2
65 27 66 151 28.9 14 1 0 0 0 2 2 2 2 22 2 900 125 2
66 28 78 171 26.7 10 1 0 0 0 2 3 2 2 22 1 1000 100
67 27 66 156 27.1 14 1 0 0 0 2 3 3 3 21 2 1200 150 2
68 23 67 166 24.3 12 1 0 0 0 2 2 2 2 20 1 1000 125
69 31 56 142 27.8 11 2 1 0 1 2 3 4 3 17 1 780 100 1
70 28 67 177 27.5 13 1 0 0 0 1 1 1 1 18 1 740 60
71 24 88 165 32.3 19 1 0 0 0 3 4 4 4 19 2 560 80 1
72 31 59 142 29.3 10 2 1 1 0 2 3 3 2 17 1 800 90
73 26 66 148 30.1 16 1 0 0 0 2 3 3 3 21 2 800 120 1
74 27 65 156 26.7 15 2 1 1 0 2 2 2 2 17 1 890 60
75 23 79 160 30.9 16 2 0 0 1 2 3 2 3 18 1 900 75
76 29 66 150 29.3 12 1 0 0 0 2 3 3 3 16 2 750 150 3
77 28 65 175 21.2 14 1 0 0 0 2 2 2 2 19 2 800 75
78 32 78 160 30.5 16 4 2 1 1 3 4 4 3 18 1 900 100 1
79 25 77 170 26.6 12 3 1 1 1 2 3 3 2 16 1 1100 125 2
80 24 55 143 26.9 12 2 1 1 1 2 3 3 3 18 1 1000 80 1
81 30 67 160 26.2 12 1 0 0 0 2 2 2 2 18 1 900 100

82 25 78 156 32.1 16 1 0 0 0 3 4 4 3 21 2 1100 200 1
83 24 68 166 24.8 11 1 0 0 0 2 2 2 2 19 2 850 200
84 23 67 154 28.3 13 1 0 0 0 2 3 3 3 20 1 990 120
85 25 60 149 27 10 1 0 0 0 2 2 2 2 18 1 700 120
86 24 78 160 30.5 15 1 0 0 0 2 3 3 2 17 2 800 110
87 29 90 162 34.3 14 2 1 1 0 3 4 4 4 16 1 1200 175 3
88 27 76 165 27.9 13 6 1 1 4 3 3 3 3 12 0.45 800 120 4
89 28 88 166 31.9 15 1 0 0 0 3 4 4 3 19 2 1200 110 1
90 23 56 149 25.2 9 3 1 1 1 2 2 2 2 15 1 650 75 4
91 24 75 160 29.3 16 1 0 0 0 2 4 3 3 21 2 850 120 2
92 29 65 159 25.7 10 1 0 0 0 2 2 2 2 18 1.3 800 120
93 23 72 158 28.8 13 1 0 0 0 2 3 3 2 22 1 990 125
94 22 59 150 26.2 14 1 0 0 0 3 3 3 3 16 2 700 150
95 28 67 159 26.5 12 1 0 0 0 3 3 3 3 19 1 900 80
96 26 80 160 31.2 18 2 0 0 1 3 4 4 3 22 1 1000 150 3
97 24 89 156 26.6 17 1 0 0 0 3 4 4 4 20 2 1200 200 2
98 27 59 148 26.9 10 2 1 1 0 2 2 2 2 18 1 600 75
99 33 65 145 30.9 14 1 0 0 0 2 3 3 3 17 2 800 1.2
100 27 67 160 26.2 11 2 1 1 0 3 3 3 3 15 1 800 100 4
101 26 77 167 27.6 15 4 1 1 2 3 3 3 3 16 0.45 900 80
102 25 79 160 30.9 13 2 1 1 0 2 3 3 3 18 1 1000 150 2
103 25 55 141 27.7 11 2 0 0 1 2 3 3 2 18 1 750 110
104 24 66 156 27.1 13 1 0 0 0 2 2 2 2 18 1 900 100
105 24 76 168 26.9 12 1 0 0 0 2 2 2 2 19 1 800 120
106 30 88 165 32.3 14 5 2 2 2 3 4 4 4 12 0.3 920 80 3
107 32 66 152 28.6 15 2 1 1 0 2 3 3 3 17 1 1000 100 1
108 25 66 159 26.1 11 1 0 0 0 2 2 2 2 19 1 800 90 4
109 24 87 167 31.2 15 1 0 0 0 3 4 4 3 21 2 1250 230 3

110 26 67 162 25.5 10 1 0 0 0 2 2 2 2 17 1 770 80
111 29 76 150 33.8 14 2 1 1 0 2 3 3 3 16 0.45 800 140
112 25 67 154 28.3 13 2 1 1 0 2 3 3 3 17 1 900 110
113 25 95 167 34.1 18 1 0 0 0 4 4 4 4 21 2 1300 200 3
114 28 75 156 30.8 16 1 0 0 0 3 3 3 3 20 1 750 110
115 25 66 145 31.4 12 2 1 1 0 2 3 3 3 18 1 900 120 4
116 28 65 156 26.7 14 1 0 0 0 3 3 3 3 18 2 900 100
117 28 66 154 27.8 10 2 1 1 0 2 2 2 2 15 0.45 740 110
118 32 56 143 27.4 12 1 0 0 0 2 3 3 3 19 2 600 100
119 25 70 162 26.7 14 3 0 0 2 3 4 4 3 15 1 780 120 1
120 23 65 152 28.1 16 1 0 0 0 2 3 3 2 18 2 1100 170
121 29 78 166 28.3 13 2 0 0 1 3 3 3 3 14 0.45 800 100
122 29 59 142 29.3 14 1 0 0 0 3 4 4 4 17 1 900 100 1
123 25 67 156 27.5 11 1 0 0 0 3 3 3 3 19 1 750 125
124 30 89 165 32.7 16 1 0 0 0 2 4 3 3 21 1 900 130 1
125 22 65 155 27.1 10 1 0 0 0 3 3 3 3 17 2 700 100
126 24 67 153 28.7 12 3 1 1 1 3 3 3 3 14 1 650 100
127 25 77 159 30.5 15 3 0 0 2 2 4 3 3 17 1 850 120 2
128 27 78 167 28 10 1 0 0 0 4 4 4 4 16 2 800 120 4
129 27 66 145 31.4 14 2 0 0 1 2 3 3 3 19 1 900 100
130 25 87 165 32 18 1 0 0 0 3 4 4 3 18 2 1100 120 3
131 30 76 156 31.2 13 2 0 0 1 2 3 3 3 17 1.3 870 110 1
132 29 68 157 27.8 13 1 0 0 0 2 2 2 2 19 1 750 100
133 29 77 160 30.1 15 1 0
0 3 4 4 3 22 2 1200 130 2
134 23 66 143 32.3 16 2 1 1 0 3 4 4 4 16 1.45 800 120 3
135 25 77 165 28.3 15 1 0 0 0 3 3 3 3 18 1 850 120
136 23 65 142 32.2 12 3 1 1 1 2 3 3 2 14 0.45 600 80
137 30 65 160 25.4 12 3 1 1 1 2 2 2 2 15 0.3 500 75

138 24 71 163 26.7 11 1 0 0 0 3 3 3 3 17 1 1000 120
139 26 76 159 30.1 16 1 0 0 0 3 4 4 3 23 2 1200 150
140 34 67 148 30.6 16 2 1 1 0 3 4 4 4 16 1 800 120 1
141 22 60 149 27 12 1 0 0 0 2 2 2 2 20 2 1000 120 3
142 22 78 158 31.2 18 1 0 0 0 3 4 4 3 22 1 1300 180 3
143 25 67 153 28.6 14 0 0 0 0 2 3 3 3 20 2 1200 150 4
144 26 70 164 26 13 1 0 0 0 3 3 3 3 18 2 700 230
145 27 61 152 26.4 9 4 2 2 1 2 2 2 2 13 1 650 75 4
146 22 90 168 31.9 16 1 0 0 0 3 4 4 4 18 2 1000 120 3
147 24 63 142 31.2 14 1 0 0 0 2 3 4 3 19 1 1200 100
148 24 67 159 26.5 11 2 0 0 1 2 2 2 2 17 0.45 650 100
149 29 59 148 26.9 10 3 1 1 1 2 3 3 3 15 0.45 800 120
150 25 80 160 31.2 16 1 0 0 0 4 4 4 4 20 1 1200 75 1
151 29 65 158 26 10 1 0 0 0 3 3 3 3 21 2 1000 120 3
152 29 67 154 28.3 13 3 1 1 1 2 3 3 3 14 1 750 100 4
153 33 78 160 30.5 14 1 0 0 0 3 4 4 3 18 1 900 100 1
154 22 70 162 26.7 12 1 0 0 0 2 2 2 2 18 1 800 100 4
155 27 78 165 28.7 10 1 0 0 0 3 3 3 3 21 1 1000 110
156 33 78 159 30.9 17 4 2 1 1 3 4 4 3 14 0.3 600 60 4
157 28 68 154 28.7 15 2 1 1 0 2 3 3 3 16 1 700 120
158 31 67 159 26.5 13 1 0 0 0 3 3 3 3 18 2 1000 120 2
159 28 58 149 26.1 11 3 1 1 1 2 2 2 2 15 1 800 75
160 25 79 168 28 14 1 0 0 0 3 4 4 4 22 2 1400 150 2
161 28 66 156 27.1 13 2 1 1 0 2 2 2 2 16 1.3 770 100
162 28 87 165 32 16 2 1 1 0 3 4 4 4 18 1 800 120 1
163 31 68 158 27.2 13 1 0 0 0 3 3 3 3 19 2 780 120
164 25 89 160 34.8 20 1 0 0 0 3 4 4 3 22 2 1200 200 3

KEY TO MASTER CHART
BMI : Body mass index
Wt gain : Weight gain during pregnancy in kilograms
MP I : Mallampati class recorded at 1st time interval
MP II : Mallampati class recorded at 2nd
time interval
MP III : Mallapati class recorded at 3rd
time interval
MP IV : Mallampati class recorded at 4th
time interval
1st stage : Duration of first stage of labour in hours
2nd
stage : Duration of second stage of labour in hours
IV 1st : Amount of intravenous fluids given during 1
st stage of
labour in millilitres
IV 2nd
: Amount of intravenous fluids given during 2nd
stage of
labour in millilitres
Co-morbidities
1- Pregnancy induced hypertensive disorders
2- Gestational Diabetes milletus
3- Hypothyroidism
4- Anaemia.