Embed Size (px)
Citation preview

Middle East Fertility Society Journal (2012) 17, 275–282
Middle East Fertility Society
Middle East Fertility Society Journal
www.mefsjournal.orgwww.sciencedirect.com
ORIGINAL ARTICLE
Prediction of fetal anemia by middle cerebral artery Doppler
S. El. Shourbagy a,b,*, M. Elsakhawy a,c
a Fetal Medical Unit, King George Hospital, Barkely Lane, Goodmayes, Essex IG3 8YB, UKb Departments of Obstetric & Gynecology, Faculty of Medicine, Tanta University, Egyptc Departments of Diagnostic Radiology, Faculty of Medicine, Menoufiya University, Egypt
Received 11 March 2012; accepted 14 September 2012Available online 30 October 2012
*
Fa
E-
Pe
11
ht
KEYWORDS
Fetal anemia;
Doppler of peak systolic
velocity in MCA;
Cordocentesis;
Red cell antibodies
Corresponding author at: De
culty of Medicine, Tanta Un
mail address: shahyshorbagy
er review under responsibilit
Production an
10-5690 � 2012 Middle East
tp://dx.doi.org/10.1016/j.mef
partmen
iversity,
70@yaho
y of Mid
d hostin
Fertility
s.2012.09
Abstract Objectives: To assess the value of peak systolic velocity in the middle cerebral artery
(MCA) in prediction of fetal anemia as a non invasive method in non hydropic fetuses.
Methods: The study included 30 pregnant women with non hydropic fetuses and with known red
cell antibodies. Full ultrasound examination was done and peak velocity of systolic cerebral blood
flow in MCA was measured. If severe anemia was suspected, fetal blood sampling by cordocentesis
was performed.
Results: Thirty fetuses were examined, 22 were anemic and eight had a hemoglobin value within
a normal range. The mean MCA peak systolic velocity for fetus with the normal hemoglobin (Hb)
was 48.98 ± 13.94 while that for the anemic fetus was 64.79 ± 11.97 and P= 0.004.
Sensitivity of increased peak velocity of systolic blood flow in MCA for prediction of fetal anemia
was 90.5% and specificity was 78.6%.
Conclusion: Doppler of peak velocity of systolic blood flow in MCA can be reliable in predicting
anemia so delaying invasive methods until treatment (blood transfusion) is expected to be necessary.� 2012 Middle East Fertility Society. Production and hosting by Elsevier B.V. All rights reserved.
1. Introduction
Maternal alloimmunization occurs when a pregnant womanhas an immunologic response to a paternally derived red-cell
antigen that is foreign to the mother and inherited by the fetus.The antibodies may cross the placenta, bind to antigens pres-ent on the fetal erythrocytes, and cause hemolysis, hydrops
ts of Obstetric & Gynecology,
Egypt.
o.com (S. El. Shourbagy).
dle East Fertility Society.
g by Elsevier
Society. Production and hosting b
.003
fetalis, and fetal death (1). Women with rising red cell antibody
levels, with or without a history of a previously affected preg-nancy, are usually referred to fetal medicine units for special-ized managements (2). Survival rates can exceed 90 percent ifanemia is diagnosed and treated with intrauterine blood trans-
fusions (3).The most accurate test to assess the degree of fetal anemia,
and thus the need for transfusion, is the fetal hemoglobin (Hb)
measurement by fetal blood sampling (4). However, the stan-dard test to evaluate the need for fetal transfusion is serialamniocentesis for the determination of bilirubin levels in amni-
otic fluid. Hemolysis leads to the accumulation of bilirubin inamniotic fluid, so its level correlates with the severity of hemo-lysis. The bilirubin level is quantified by spectrophotometry
and expressed as the change in optical density at a wavelength
y Elsevier B.V. All rights reserved.

276 S. El. Shourbagy, M. Elsakhawy
of 450 nm (DOD450); the DOD450 values are then plotted on a
Liley chart to estimate the severity of anemia (5). Both proce-dures have a significant rise of causing miscarriage, prematurerupture of membrane, preterm delivery and increase antibodyconcentration (6).
Several non-invasive methods for the prediction of fetalanemia have been assessed, aiming to defer the use of invasivetesting until transfusion is necessary (2,7,10). The association
of increased blood flow velocity in the fetal middle cerebral ar-tery (MCA) with fetal anemia is the most promising of thesenon-invasive tests as has subsequently been reported (9,8). Fe-
tuses with anemia have a high cardiac output and decreasedblood viscosity, resulting in high blood-flow velocities thatcould be used in prediction of fetal anemia (11,12). Brennad
showed that in anemic fetus changes in cardiac output &blood-flow velocities are reflected by an increase in peak sys-tolic velocity in the middle cerebral artery (13).
The objective of the current study is to assess the value of
measuring peak systolic velocity in the middle cerebral artery(MCA) as a non invasive method in non hydropic fetusesfor prediction of fetal anemia due to maternal red-cell
alloimmunization.
2. Methods
2.1. Subjects’ studies
The study included 30 pregnant women with red cell antibodiesreferred for assessment and management. Patients were mainly
referred if there was an increase in antibody levels in the mater-nal serum, or if there was a previous obstetric history of an ane-mic fetus or neonate. Assessment consisted of ultrasoundexamination for fetal biometry, exclusion of any structural
abnormalities, liquor volume assessment, umbilical arteryDoppler blood flow studies and Doppler blood flow velocitystudies of the MCA. Hydrops was defined as fluid collection
in body cavities or skin edema, and hydropic fetuses were ex-cluded from the study. Cordocentesis was performed on 18 pa-tients at their first visit and for the remaining, follow- up was
arranged and those whose assessment was suggestive of wors-ening anemia underwent cordocentesis on the second visit.
2.2. Doppler studies
Doppler examination of the MCA was performed before cor-docentesis in all cases. An axial section of the brain, including
the thalami and the cavitas septi pellucidi, was obtained. Thecircle of Willis was visualized and the middle cerebral arteryof one side was examined close to its origin in the internal car-
otid artery. We have found that the systolic velocity decreaseswith distance from the point of origin of this vessel, so the anglebetween the ultrasound beam and the direction of blood flow
was kept as close as possible to 0 and in all cases not to exceed30�. The highest point of the wave from peak systolic velocity(PSV) was measured. Doppler images were recorded at a timewhen there was an absence of marked fetal body and respira-
tory movements, to avoid false elevation in PSV with fetal heartrate acceleration. At least three measurements were taken andthe highest one is accepted as the final value. The reference test
for the diagnosis of fetal anemia was measurement of peak sys-tolic velocity of the MCA more than 1.5 multiple of median
(MOM) using reference produced by Mari and his colleagues
(9). Practical approach is to convert actual values into MOMto account for changes in gestational age, internet based calcu-lator is available at www.perinatology.com.
2.3. Cordocentesis
Fetal blood sampling was performed by cordocentesis from the
umbilical vein at the placental cord insertion with blood readyfor fetal transfusion if necessary. Fetal blood was immediatelyexamined for the determination of the full blood count and, if
anemia was confirmed, intravascular transfusion wasperformed.
The reference test for the diagnosis of fetal anemia was
measurement of the hemoglobin level in umbilical-cord blood.Fetal anemia is defined as Hb less than 0.65 times the medianfor gestational age, with the use of the published referencerange (9).
2.4. Statistics
Statistical presentation and analysis of the present study wasconducted, using the mean by SPSS V.16.
Mean value �X: the sum of all observations divided by the
number of observations:
�X ¼P
x
n
Where R = sum & n= number of observations.
ROC-curve: Receiver Operating Characteristic curveanalysis
Sensitivity: Probability that the test results will be positive
when the disease is present (true positive rate, expressed as apercentage).
Specificity: Probability that the test results will be negativewhen the disease is present (true negative rate, expressed as a
percentage).
3. Results
This study included 30 pregnant women with alloimmuniza-tion and non-hydropic fetuses. Twenty three cases had RhD
antibodies. Other 5 cases were with Rh C antibodies and last2 cases were with anti E antibodies.
Medium gestational age was 29.27 ± 3.54 (range 24–
35 weeks). Medium maternal age was 31.1 ± 5.67 (range 22–44 years). All patients were multi gravid. Among the 30 fetusesat risk of anemia, 22 were anemic (Hb 8.07 ± 0.93) and 8 hadnormal Hb (Hb 10.08 ± 0.96).
Fetal blood was taken by cordocentesis for hemoglobinanalysis in 22 cases, 18 at first visit and four at second visit.In the other 8 cases the MCA Doppler was within normal
range (48.98 ± 13.94) and follow up antibodies titer remainsstable and hemoglobin was determined in fetal cord blood ob-tained at birth and show normal Hb or mild anemia.
The mean MCA peak systolic velocity for fetuses with nor-mal Hb was 48.98 ± 13.94 while that for anemic fetuses was64.79 ± 11.97 (P 6 0.004). The MOM of MCA for fetuses
with normal Hb was 1.22 ± 0.21 while that for anemic fetuseswas 1.62 ± 0.08 (P 6 0.001).
There were non significant correlations between fetal Hband maternal age with P = 0.19 (Fig. 1), while there were

50
1211109876Fetal Hb
Mat
erna
l age
yea
rs
r.0.270 p. 0.129
40
30
20
Figure 1 Correlation between fetal Hb and maternal age in fetuses at risk of anemia due to red-cell alloimmunization. Open rectangle
indicates fetuses with anemia & solid rectangle indicates fetuses with no or mild anemia.
7060504030
50
40
30
209080
MCA
Mat
erna
l age
yea
rs
r.0.756 p. 0.001
Figure 2 Correlation between fetal peak systolic velocity of MCA and maternal age in fetuses at risk of anemia due to red-cell
alloimmunization. Open rectangle indicates fetuses with anemia & solid rectangle indicates fetuses with no or mild anemia.
gestational age3634323028262422
1.0
.8
.6
.4
.2
0.0
r. -0.358 p. 0.028
MO
M o
f fet
al H
b
Figure 3 Correlation between MoM of fetal Hb and gestational age in fetuses at risk of anemia due to red-cell alloimmunization. Open
rectangle indicates fetuses with anemia & solid rectangle indicates fetuses with no or mild anemia.
Prediction of fetal anemia by middle cerebral artery Doppler 277

3634323028262422
90
80
70
60
50
40
30
gestational age
MC
A-P
SV
Figure 4 Correlation between MCA-PSV and gestational age in fetuses at risk of anemia due to red-cell alloimmunization. Open
rectangle indicates fetuses with anemia & solid rectangle indicates fetuses with no or mild anemia.
1.0.8.6.4.20.0
1.8
1.6
1.4
1.2
1.0
MOM of fetal Hb
r.-0.574 p. 0.003
MO
M o
f MC
A
Figure 5 Strong correlation between MoM of fetal Hb and MoM of MCA in fetuses at risk of anemia due to red-cell alloimmunization.
Open rectangle indicates fetuses with anemia & solid rectangle indicates fetuses with no or mild anemia.
822N= 30Non-anemic fetusesAnemic fetuses
2.0
1.8
1.6
1.4
1.2
1.0
.8
22
MO
M o
f MC
A
Figure 6 The distribution of MOM of MCA values in the anemic and non-anemic fetuses. Non anemic fetuses’ median 1.19, range 1.53,
maximum value 1.37, minimum value 1.03, anemic fetuses’ median 1.62, range1.53 maximum value 1.78, minimum value 1.52 .
278 S. El. Shourbagy, M. Elsakhawy

ROC Curve
1 - Specificity1.00.75.50.250.00
Sen
sitiv
ity
1.00
.75
.50
.25
0.00
ROC-curve: Characteristic curve analysis for sensitivity and specificity.
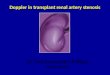
Figure 7 Normal Doppler imaging of the middle cerebral artery peak systolic velocity (46.8) at 32 weeks 4 days’ gestation in a multi
gravida 25 years with fetal Hb10.3.
Prediction of fetal anemia by middle cerebral artery Doppler 279
significant correlations between MCA and maternal age withP = 0.001 (Fig. 2).
On the other hand there was a strong negative correlationbetween gestational age and MOM of fetal Hb (correlationcoefficient r= �0.358, P 6 0.028) (Fig. 3). Also, there was a
significant correlation between gestational age and MCA (cor-relation coefficient r = �0.525, P 6 0.014) (Fig. 4).
The relation between the multiples of the median of thehemoglobin concentration and the multiples of the median
of peak systolic velocity was strong (correlation coefficientr= �0. 574, P 6 0.003 for MOM of PSV) (Fig. 5).
Fig. 6 demonstrates the distribution of MOM of MCA val-ues in the anemic and non-anemic fetuses, showing the median,
range and maximum–minimum values for each group.Sensitivity of increased PSV of MCA to predict fetal ane-
mia in cases alloimmunized with red cell antibodies was
90.5% and specificity was 78.6% (ROC Curve).Doppler imaging of the middle cerebral artery, peak sys-
tolic velocity shows a normal level in the non anemic fetus(where MCA was 46.8 at 32 weeks 4 days’ gestation in multi
gravida 25 years with fetal Hb 10.3) and was very high in casesof fetal anemia (where MCA was 68.8 at 30 weeks 6 days’

Figure 8 High Doppler imaging of the middle cerebral artery peak systolic velocity (68.5) in anemic fetus with fetal Hb 7.5 at 30 weeks
6 days’ gestation of a multi gravida 29 years.
Figure 9 High Doppler imaging of the middle cerebral artery peak systolic velocity (74.0) in anemic fetus with fetal Hb 8.5 at 32 weeks
3 days’ gestation in a multi gravida 44 years.
280 S. El. Shourbagy, M. Elsakhawy

Prediction of fetal anemia by middle cerebral artery Doppler 281
gestation in multi gravida 29 years with fetal Hb 7.5 & MCA
was 79.2 at 32 weeks 3 days’ gestation in multi gravida 44 yearswith fetal Hb 8.5) (Figs. 7–9).
4. Discussion
Doppler velocimetry of the middle cerebral artery (MCA) hasplayed a major role in the fetal medicine for the last 23 years,
both in intrauterine growth-restricted (IUGR) and anemic fe-tuses. Its utility in the diagnosis and management of cases offetal anemia was initially demonstrated in the cases of red cell
alloimmunization and later extended to other types of anemia(16,15).
Data of the present findings confirm that MCA peak sys-
tolic velocity compared with hemoglobin levels at either fetalblood sampling, or cord sampling at delivery if antenatal inter-vention had not been indicated is significantly increased in the
cases of fetal anemia owing to red cell antibodies. The mostlikely physiological explanation for this is that anemia is asso-ciated with both increased cardiac output, due to the hyperdy-namic circulation, and a reduction in blood viscosity, both
leading to increased blood flow velocity.The association between increased MCA blood flow veloc-
ity and fetal anemia has been previously demonstrated using
peak systolic velocity (9,10,17). The use of published, generallyagreed, reference range was preferred for this study.
The peak systolic velocity in the middle cerebral artery de-
creases when the fetal hematocrit rises (20). These findingsindicate that there is a reciprocal relation between the hemo-globin concentration and hematocrit values and the velocityof cerebral blood flow (18). We found that the risk of anemia
was high in fetuses with a peak systolic velocity of 1.50 timesthe median or higher. Such findings support the previous workof Moise who found that an elevated peak MCA velocity of
>1.5 multiples of the median is useful in the timing of theinitial intrauterine transfusion (IUT) in the red cell-alloimmu-nized pregnancies (19). Fetuses with values below 1.50 either
did not have anemia nor had only mild anemia. The fact thatthis test does not predict mild anemia well is not clinicallyimportant, because no intervention is indicated in fetuses with
mild anemia, as defined in our study, whereas those withmoderate or severe anemia should undergo cordocentesisand may need transfusion as had been previously reportedby (1).
Although cordocentesis allows direct measurement of fetalhemoglobin, it is associated with infection, bleeding, fetal bra-dycardia, premature rupture of the membranes and pregnancy
loss (21). However, amniocentesis is less invasive than cordo-centesis but the reliability of measurements of bilirubin inamniotic fluid before 27 weeks of gestation is questionable.
Yet for both procedures there are no data concerning optimalaccuracy (22,23). Opekes and his colleagues showed throughcomparing Doppler ultrasonography versus amniocentesis
that measurements of the peak velocity of systolic blood flowin MCA can safely replace invasive testing managements ofRh-alloimmunized pregnancies (24).
Therefore, the use of measurements of peak systolic velocity
as described here would be beneficial and decrease the numberof fetuses subjected to cordocentesis and amniocentesis. Thesefindings coincided with the work of Alshimmiri and his
colleagues who have shown that fetal MCA-PSV weakly
correlates with the degree of fetal anemia in groups with or
without previous intrauterine transfusion; however, velocitythreshold levels were sensitive enough to predict most fetuseswith moderate to severe anemia (25).
Our findings coincided with the work of previous research-
ers who demonstrated that MCA-PSV measurement is essen-tial in the diagnosis, evaluation, and management of thecases of fetal anemia (26,27). The use of this modality lessens
the need for invasive procedures. Also, Kenneth and Moiseshowed that the peak systolic velocity of the MCA was effec-tive in the detection of fetal anemia in a variety of pathologic
states (28). They showed that addition of this noninvasivemethod to detect the anemic fetus has enabled the maternal-fe-tal specialist to intervene earlier in the course of such diseases
as hemolytic disease of the fetus/newborn infant and fetal par-vovirus infection. Although the middle cerebral artery peaksystolic velocity Doppler has limited diagnostic accuracy, it re-mains the gold standard for noninvasive screening of fetal ane-
mia (29).Our results were compared with hemoglobin levels at either
fetal blood sampling in 22 cases, or cord sampling at delivery
in 8 cases where antenatal intervention had not been indicated.MCA-PSV had a sensitivity of 90.5% and a specificity of78.6% for the detection of severe anemia. Brennand showed
by comparing hemoglobin levels in 165 fetuses at either fetalblood sampling, or cord sampling at delivery that the sensitiv-ity and accuracy of the middle cerebral artery Doppler (sensi-tivity of 88%, specificity of 82%) were substantially greater
than amniocentesis (sensitivity of 76%, specificity of 77%)for the detection of anemia (13).
Hydropic fetuses were excluded from this study. This is be-
cause we wished to assess how effective the measurement ofMCA Doppler velocity is at predicting fetal anemia in border-line cases, in which the decision to sample the fetal blood is not
clear.In conclusion, measurements of the peak velocity of blood
flow in the middle cerebral artery in fetuses at risk for anemia
due to maternal red cell alloimmunization provide an accurate
and noninvasive means of determining the degree of anemia.Clearly, the widespread use in future of MCA Doppler assess-ment to detect fetal anemia in other fetal diseases is on the near
horizon. However, no non-invasive test is 100% accurate in allcases, and so the assessment of patients with red cell antibodiesshould be comprehensive and include all possible relevant
information, including obstetric history and rate of changeof antibody levels.
References
(1) Bowman JM. Haemolytic disease (Erythroblastsis fetalis). In:
Creasy RK, Rensnik R, editors. Maternal-fetal medicine 4th.
Philadelphia: W.B. Saunders; 1999. p. 736–67.
(2) Oepkes D, Brand R, Vandenbussche FP, Meerman RH, Kanhai
HUH. The use of ultrasonography and Doppler in the prediction
of fetal haemolytic anaemia: a multivariate analysis. Br J Obstet
Gynaecol 1994;101:680–4.
(3) van Kamp IL, Klum FJCM, Bakkum RSI. The severity of
immune fetal hydrops is predictive for fetal outcome after
intrauterine treatment. Am J Obstet Gynaecol 2001;185:668–73.
(4) Soothill PW. Fetal blood sampling before labor. In: James DK,
Steer PJ, Weiner CP, Gonik B, editors. High risk pregnancy,
management options. London: WB Saunders; 1999. p. 225–33.

282 S. El. Shourbagy, M. Elsakhawy
(5) Nicolaides KH, Rodeck CH, Mibashan RS, Kemp JR. Have
Liley charts outlived their usefulness? Am J Obstet Gynaecol
1986;155:680–4.
(6) Weiner CP, Okamura K. Diagnostic fetal blood sampling-
technique related losses. Fetal Diagn Ther 1996;11(3):169–75.
(7) Hadley AG, Wilkes A, Goodrick J, Penman DW, Lucas G. The
ability of the chemiluminescence test to predict clinical outcome
and the necessity for amniocenteses in pregnancies at risk of
haemolylic disease of the newborn. Br J Obstet Gynecol 1998;105:
231–4.
(8) Delle Chiaie L, Buck G, Grab D, Terinde R. Prediction of fetal
anemia with Doppler measurement of the middle cerebral artery
peak systolic velocity in pregnancies complicated by maternal
blood group alloimmunization or parvovirus B19 infection.
Ultrasound Obstet Gynecol 2001;18(3):232–6.
(9) Mari G, Deter RL, Carpenter RL. Noninvasive diagnosis by
Doppler ultrasonography of fetal anemia due to maternal red-cell
alloimmunization. N Eng J Med 2000;342:9–14.
(10) Teixeira IMA, Duncan K, Letsky E, Fisk NM. Middle cerebral
artery peak systolic velocity in the prediction of fetal anemia.
Ultrasound Obstet Gynaecol 2000;I5:305–8.
(11) Duker D, Oepkes D, Seaward G, Windrim R, Ryan G.
Noninvasive tests to predict fetal anemia: a study comparing
Doppler and ultrasound parameter. Am J Obstet Gynaecol 2003;
188:1310–4.
(12) Segata M, Mari G. Fetal anemia: new technologies. Curr Opin
Obstet Gynaecol 2004;16:153–8.
(13) Brennand J. Middle cerebral artery Doppler. AJUM
2009;12(4):35–9.
(15) Schenone MH, Mari G. The MCA Doppler and its role in the
evaluation of fetal anemia and fetal growth restriction. Clin
Perinatol 2011;38(1):83–102.
(16) Hanif F, Drennan K, Mari G. Variables that affect the middle
cerebral artery peak systolic velocity in fetuses with anemia and
intrauterine growth restriction. Am J Perinatol 2007;24(8):501–5.
(17) Ahmed B, Ghaffari Z, Ismail RS, Saleh N. Non-invasive
diagnosis of fetal anemia due to maternal red-cell alloimmuniza-
tion. Saudi Med J 2005;26(2):256–9.
(18) Mandic V, Mikovic Z, Filimonovic D, Dukic M, Vasiljevic M,
Bogavac M. Noninvasive diagnosis of fetal anemia in Rh-alloim-
munized pregnancies by color Doppler. Med Pregl 2005;58(5–6):
275–8.
(19) Moise Jr KJ. The usefulness of middle cerebral artery Doppler
assessment in the treatment of the fetus at risk for anemia. Am J
Obstet Gynecol 2008;198(2):161.e1–4.
(20) Mari G, Rahman F, Olofsson P, Ozcan T, Copel JA. Increase
fetal hematocrit decreases middle cerebral artery peak systolic
velocity in pregnancies complicated by rhesus alloimmunization. J
Matern Fetal Med 1997;6:206–8.
(21) Ghidini A, Sepulveda W, Lockwood CJ, Romero R. Complica-
tion of fetal blood sampling. Am J Obstet Gynaecol 1993;168:
1339–44.
(22) Rahman F, Detti L, Ozcan T, Khan R, Manohar S, Mari G. Can
a single measurement of amniotic fluid delta optical density be
safely used in the clinical management of rhesus-alloimmunized
pregnancies before 27 weeks gestation? Acta Obstet Gynecol Scan
1998;77:804–7.
(23) Bullock R, Martin WL, Coomarasamy A, Kilby MD. Prediction
of fetal anemia in pregnancies with red -cell isoimmunization
comparison of middle cerebral artery peak systolic velocity and
amniotic fluid DOD450. Ultrasound Obstet Gynaecol 2005;25:
331–4.
(24) Oepkes D, Seaward G, Vandenbussche FP, Windrim R, Beyene J,
Kanhai HUH. Doppler ultrasonography versus amniocentesis to
predict of fetal anaemia. N Eng J Med 2006;355:156–64.
(25) Alshimmiri MM, Hamoud MS, Al-Saleh EA, Mujaibel KY, Al-
Harmi JA, Thalib L. Prediction of fetal anemia by middle cerebral
artery peak systolic velocity in pregnancies complicated by rhesus
isoimmunization. J Perinatol 2003;23:536–40.
(26) Imbar T, Lev-Sagie A, Cohen S, Yanai N, Yagel S. Diagnosis,
surveillance, and treatment of the anemic fetus using middle
cerebral artery peak systolic velocity measurement. Prenat Diagn
2006;26(1):45–51.
(27) Lubusky M, Prochazka M, Santavy J, Mıckova I, Kantor L.
Actual management of pregnancies at risk for fetal anemia. Ceska
Gynekol 2006;71(4):272–80 [Article in Czech].
(28) Kenneth J, Moise Jr. The usefulness of middle cerebral artery
Doppler assessment in the treatment of the fetus at risk for
anemia. Am J Obstet Gynecol 2008;198:161.e1–4.
(29) Pretlove SJ, Fox CE, Khan KS, Kilby MD. Noninvasive methods
of detecting fetal anaemia: a systematic review and meta-analysis.
BJOG 2009;116(12):1558–67.