Embed Size (px)
Citation preview
ORIGINAL CONTRIBUTION aorta, thoracic, rupture; rupture, aortic, thoracic
Prediction of Traumatic Aortic Rupture From Plain Chest Film Findings Using Stepwise Logistic Regression
We reviewed initial chest radiographs of 21 patients with, and 26 without, aortic rupture, and examined the presence or absence of individual signs previously cited to be associated with aortic rupture. Using stepwise logistic regression, the three most significant signs associated with rupture were loss of aortic contour, tracheal deviation, and mediastinal-to-chest ratio. A for- mula calculating the probability of aortic rupture (P) using these three vari- ables was derived. Using a low cutoff point, this equation would approach I00% sensitivity in detecting aortic rupture while reducing the number of negative aortographs. The reliability of this equation and the optimal cutoff point must be determined in a prospective study before being used to make clinical decisions. [Huang P, Fong C, Rademaker A: Prediction of traumatic aortic rupture from plain chest film findings using stepwise logistic regres- sion. Ann Emerg Med December 1987;16:1330-1333.]
INTRODUCTION Rupture of the thoracic aorta in blunt chest trauma is frequently a lethal
disease for which early diagnosis is essential but difficult due to nonspecific clinical signs and symptoms.I, 2 Chest roentgenograms often raise suspicion after which the definitive test of aortography is done to confirm or rule out the diagnosis. While more than a dozen radiological signs have been associ- ated with aortic rupture, 3 there is still controversy as to what combination of presence or absence of these signs could best predict or rule out this diag- nosis. 4q2 Signs such as first and second rib fractures, pneumothorax, and pulmonary contusions have since been shown consistently to have no pre- dictive value.13,14 Accordingly, these signs were not included for analysis in our study. A reliable method to exclude rupture using the remaining signs from plain films while retaining 100% sensitivity would reduce the need for aortographs.
Our study was undertaken to generate a formula through stepwise logistic regression to determine the probability of aortic rupture given a combination of various plain chest radiograph signs previously cited 4-1~ to be associated with aortic rupture. While this formula needs to be shown to be valid and reliable in future prospective studies, a decision then may be made to set the most appropriate cutoff point in the probability curve for performing aor- tographs that would approach 100% sensitivity. This would still reduce the number of negative aortographs performed because of "positive" plain film findings.
MATERIALS AND METHODS The medical records and radiographs of inpatients of the four major Calga- Alberta, hospitals from 1980 to 1984 with an admission or discharge diag-
nosis of aortic rupture were reviewed. Included were Foothills, Calgary General, Holy Cross, and Rockyview hospitals. In addition, patients admit- ted to intensive care units wi th a diagnosis of mul t ip le t rauma or chest trauma and those who died in the emergency department with trau- matic arrests were included. Patients who underwent aortograms or had au- topsies to confirm or exclude aortic rupture were candidates in our study. Only the patients who had an initial chest radiograph available for examina- tion were included.
Using this method, 21 patients with aortic rupture and 26 without were
Paul Huang, MD, CCFP* Chen Fong, MD, FRCPCt Alfred Rademaker, PhD!~ Calgary, Alberta, Canada
From the Department of Emergency Medicine* and Radiology, t Foothills Hospital; and the Department of Community Health Sciences, University of Calgary,¢ Calgary, Alberta, Canada.
Received for publication March 23, 1987. Revision received August 10, 1987. Accepted for publication August 14, 1987.
Address for reprints: Paul Huang, MD, CCFP, Foothills Hospital, Department of Emergency Medicine, Room C231, 1403 29th Street, NW, Calgary, Alberta, Canada T2N 2T9.
16:12 December 1987 Annals of Emergency Medicine 1330/41

TRAUMATIC AORTIC RUPTURE Huang, Fong & Rademaker
TABLE 1. Frequency (%) of chest radiograph signs in patients with aortic rupture (n =21) and patients without (n =26)
Rupture No Rupture
Radiological Sign Present Absent Present Absent P Aortic Contour 100 0 31 69 < ,001"
Tracheal Deviation 57 43 27 73 .043*
Esophageal Deviation 48 52 27 73 .222
Left Mainstem Depression 38 62 42 58 1.000
Right Paratracheal Stripe Width 67 33 27 73 .009*
Pleural Cap 76 24 27 73 < .001"
Hemothorax 67 33 38 62 .080
*P < .05 using two-tailed Fisher exact test.
included in our study. All patients had aortograms performed. Init ial chest radiographs were portable supine ante- rior-posterior (AP) fi lms using stan- dard 100 cm focal-film distance, with 75 kilovolt peak and 2 to 3 mA. These films were reviewed independently in a blind examination by a radiologist and an emergency physician. Specific definitions of radiological signs corre- sponding to those of previous stud- ies3,7,8,1]A 2 were applied to reduce inter-observer variation.
Mediast inal wid th (M) was mea- sured objectively at the level of the aortic arch. This was recorded to with- in 0.5 cm. The chest width (C) also was measured at this level. Corre- sponding mediastinal to chest (M:C) ratio was obtained by dividing the me- diastinal width by chest width. The chest width and M:C ratio were the only signs wi th numer i ca l values. There was agreement to wi th in 0.5 cm of these width measurements be- tween the observers.
The presence of the following signs was considered for aortic rupture: loss of the aortic knob contour, tracheal or esophageal deviation at level of T-4, right paratracheal stripe widening of more than 1 cm, depression of left m a i n s t e m bronchus beyond 40 de- grees from horizontal, apical pleural cap(s), and hemothorax.
Inter-observer variation was mini- mal, with an average of three changes per sign for the 47 patients. The radi- ologist's opinion was accepted as the correct one in these instances.
Each sign was correlated with the presence of aortic rupture and statis- tical significance (P < .05) was deter- mined using either an unpaired t test
TABLE 2. Mediastinal width (cm) and mediastinal-to-chest width ratio of patients with aortic rupture (n=21) and without rupture (n=26)
Mediastinal Width Mean Range Standard Deviation
With Rupture 9.7* 8,0-11.5 1.05
No Rupture 8.1 5.0-11.0 1.30
Mediastinal to Chest Ratio With Rupture 0.38* 0.33-0.49 0.043
No Rupture 0.32 0.23-0.43 0.048
*P < .001 comparing rupture to no rupture using unpaired t test.
or a two-tai led Fisher exact test. 15 Multivariate analysis of signs as pre- dictors of aortic rupture was done by stepwise logistic regression analysis.i6 Variables were entered into the equa- tion if P < .05.
RESULTS There was an average of five posi-
tive findings for patients with aortic rupture. The percentages of the indi- vidual findings in patients with and w i t h o u t aor t ic ruptures are l isted (Table 1).
Significant findings separating the two groups inc luded loss of aort ic knob contour , t r achea l devia t ion , widening of right paratracheal stripe width, and presence of pleural cap. Not significant were left ma ins t em bronchus depression, esophageal de- viation, and hemothorax.
The mean mediastinal width of pa- t ients wi th aortic ruptures was 9.7 cm, with a range of 8 to 11.5 cm (Table 2). This was statistically wider than in pa t i en t s w i t h o u t rup tures , whose mean width was 8 cm, with a range of 5 to 11 cm (P < .001}. The correspond-
ing M:C ratios were also significantly different: 0.38 (range, 0.33 to 0.49) in patients with ruptures compared with 0.32 (range, 0.23 to 0.43) in patients without ruptures (P < .001).
Using stepwise logistic regression, the formula derived for the probability of aortic rupture (P) was: P = 1 / {1 + exp[ 46.4 - 9.5 ACONT - 1.48 TD - 109 MCRATIO]}, where ACONT = - 1 if aortic contour is preserved, + 1 if lost; TD = - 1 if tracheal position is n o r m a l , +1 if d e v i a t e d ; and MCRATIO = mediastinal/chest ratio measured at the level of the aortic arch.
The statistical significance of these three variables was of such magnitude tha t add i t ion of o the r factors , al- though significant individually, did not improve the predictive value of the function.
When the current data were sub- stituted into this equation, the predic- tive probability for rupture obtained for the r u p t u r e and n o n - r u p t u r e groups fell into two distinct distribu- tions. All but one of the patients with aortic rupture had P > .66. The re-
42/1331 Annals of Emergency Medicine 16:12 December 1987
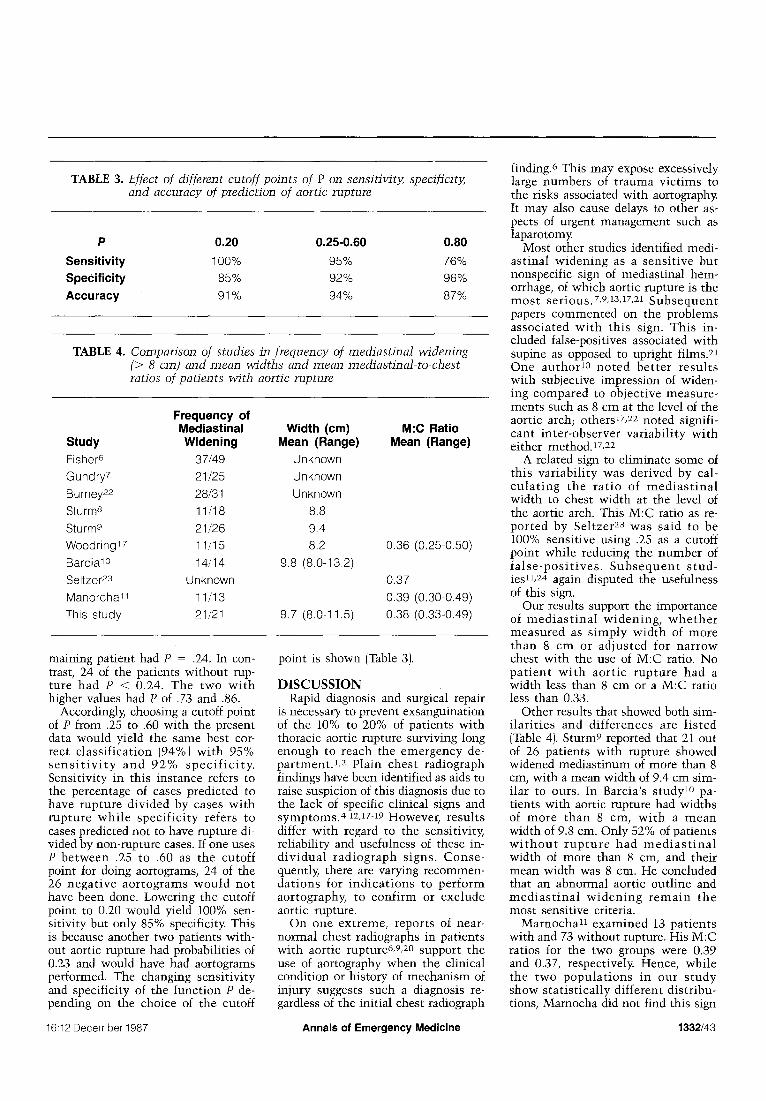
TABLE 3. Effect of ch'fferent cutoff points of P on sensitivity, specificity, and accuracy of prediction of aortic rupture
P 0.20 0.25-0.60 0.80
Sensitivity 100% 95% 76% Specificity 85% 92% 96% AcCuracy 91% 94% 87%
TABLE 4. Comparison of studies in frequency of mediastinal widening (> 8 cm) and mean widths and mean mediastinal-to-chest ratios of patients with aortic rupture
Frequency of Mediastinal Width (cm) M:C Ratio
Study Widening Mean (Range) Mean (Range) Fisher 6 37/49 Unknown
Gundry 7 21/25 Unknown
Burney 22 28/31 Unknown
Sturm 8 11/18 8.8
Sturm e 21/26 9.4
Woodringl 7 1 I/15 8.2 0.36 (0.25-0.50)
Barcia 10 14/14 9.8 (8.0-13.2)
Seltzer 23 Unknown 0.37
Manorcha~ 1 11/13 0.39 (0.30-0.49)
This study 21/21 9.7 (8.0-11.5) 0,38 (0.33-0.49)
maining pat ient had P = .24, In con- trast, 24 of the patients wi thout rup- ture had P < 0.24. The two w i t h higher values had P of .73 and .86.
Accordingly, choosing a cutoff point of P from .25 to .60 wi th the present data would yield the same best cor- rect c lass i f i ca t ion (94%) w i t h 95% s e n s i t i v i t y a n d 92% s p e c i f i c i t y . Sensi t ivi ty in this ins tance refers to the percentage of cases predicted to have rup tu re d iv ided by cases w i th r u p t u r e w h i l e s p e c i f i c i t y refers to cases predicted not to have rupture di- vided by non-rupture cases. If one uses P be tween .25 to .60 as the cutoff point for doing aortograms, 24 of the 26 n e g a t i v e a o r t o g r a m s w o u l d n o t have been done. Lowering the cutoff point to 0.20 would yield 100% sen- si t ivity but only 85% specificity. This is because another two patients with- out aortic rupture had probabili t ies of 0.23 and would have had aortograms performed. The changing sens i t iv i ty and specif ici ty of the funct ion P de- pending on the choice of the cutoff
point is shown (Table 3).
D I S C U S S I O N Rapid diagnosis and surgical repair
is necessary to prevent exsanguination of the 10% to 20% of pat ients wi th thoracic aortic rupture surviving long enough to reach the emergency de- pa r tmen t . I , 2 P la in ches t rad iograph findings have been identified as aids to raise suspicion of this diagnosis due to the lack of specific clinical signs and symptoms.4q2,17-19 However, resu l t s differ wi th regard to the sensitivity, reliabil i ty and usefulness of these in- d i v i d u a l r a d i o g r a p h s igns. Conse - quently, there are varying recommen- da t i ons for i n d i c a t i o n s to p e r f o r m aortography, to conf i rm or exc lude aortic rupture.
On one ex t reme, repor ts of near- normal chest radiographs in pat ients wi th aort ic rupture6,9, 2o support the use of aortography when the clinical condit ion or his tory of mechanism of injury suggests such a diagnosis re- gardless of the ini t ial chest radiograph
finding. 6 This may expose excessively large numbers of t r auma v ic t ims to the risks associated with aortography. It may also cause delays to other as- pects of urgent management such as laparotomy.
Most other studies identified medi- as t ina l w i d e n i n g as a sens i t ive but nonspecific sign of mediast inal hem- orrhage, of which aortic rupture is the m o s t s e r ious . 7,9,13,17,21 S u b s e q u e n t papers c o m m e n t e d on the problems assoc ia ted w i t h th is sign. Th is in- cluded false-positives associated with supine as opposed to upright films. 21 One a u t h o r Io n o t e d b e t t e r r e su l t s wi th subjective impression of widen- ing compared to objec t ive measure - ments such as 8 cm at the level of the aort ic arch; others17, 2z noted signifi- cant in te r -observer va r i ab i l i t y w i t h either method. lh 22
A related sign to e l iminate some of th is va r i ab i l i t y was der ived by cal- c u l a t i n g the r a t i o of m e d i a s t i n a l width to chest width at the level of the aortic arch. This M:C ratio as re- po r t ed by Se l t ze r 23 was said to be 100% sensit ive using .25 as a cutoff point whi le reducing the number of f a l s e - p o s i t i v e s . S u b s e q u e n t s t u d - ies11, 24 again disputed the usefulness of this s i g n .
Our results support the importance of m e d i a s t i n a l w i d e n i n g , w h e t h e r measu red as s i m p l y w i d t h of more t han 8 c m or a d j u s t e d for n a r r o w chest wi th the use of M:C ratio. No p a t i e n t w i t h ao r t i c r u p t u r e had a width less than 8 cm or a M:C ratio less than 0.33.
Other results that showed both sim- i l a r i t i e s and d i f fe rences are l i s t ed (Table 4). Sturm 9 reported that 21 out of 26 pat ients wi th rupture showed widened medias t inum of more than 8 cm, wi th a mean width of 9.4 cm sim- i lar to ours. In Barcia 's s tudy 10 pa- t ients wi th aortic rupture had widths of m o r e t h a n 8 cm, w i t h a m e a n width of 9.8 cm. Only 52% of patients w i t h o u t r u p t u r e h a d m e d i a s t i n a l width of more than 8 cm, and their mean width was 8 cm. He concluded that an abnormal aort ic out l ine and m e d i a s t i n a l w i d e n i n g r e m a i n the most sensitive criteria.
Marnocha 11 e x a m i n e d 13 pa t i en t s wi th and 73 wi thout rupture. His M:C ratios for the two groups were 0.39 and 0.37, respectively. Hence, whi le the two p o p u l a t i o n s in our s t u d y show s t a t i s t i c a l l y di f ferent d i s t r ibu- tions, Mamocha did not find this sign
16:12 December 1987 Annals of Emergency Medicine 1332/43

TRAUMATIC AORTIC RUPTURE Huang, Fong & Rademaker
useful in his study. Woodring 17 exam- ined 15 patients with and 20 without rupture. The former group had a mean medias t inal wid th of 8.2 cm and a mean M:C ratio of 0.36. Patients with non-rupture had values of 7.3 cm and 0.33, correspondingly. Accordingly , these two values were not included in his conc lus ions of use fu l signs. In Sefczek's series, 12 nine of ten patients wi th aort ic rupture had M : C rat io greater than 0.25. Gundry 19 reported a sensitivity of 89% and 82% for medi- ast inal widen ing and loss of aor t ic contour, respectively, in the 149 cases he examined; 16 had aortic rupture.
In an e x t e n s i v e r e v i e w of radio- graphic manifestations of mediastinal hemorrhage from blunt chest trauma, Woodring3 stated the variation in fre- quency and re l iab i l i ty of the o ther signs. These include abnormalities of aortic contour, aor topulmonary win- dow opacification, depression of left main bronchus, tracheal deviation to the right, displacement of nasogastric tube to the right, apical pleural cap, widening of paraspinal lines, widening of p a r a t r a c h e a l s t r ipe , h e m o p n e u - mothorax, and associated chest wall injuries.
Previous studies4-12,17-z4 focused on two separate issues. One was the abil- ity of individual plain radiograph find- ings to identify aortic rupture (sen- sitivity). The other was to reduce the number of negative aortographs due to fa lse-posi t ive ches t radiograph find- ings. Given the lack of sensitivity and specificity of individual signs, com- binations of signs that could exclude aortic rupture were examined in some of these studies.
Varying conclusions were made by authors of such studies. Barcia lo con- cluded that the possibili ty of aortic rupture was exceedingly small if the chest radiograph is normal. In addi- tion to the already stated importance of mediastinal widening and abnormal aortic outline, other useful signs to identify aortic rupture were displaced right paraspinous stripes and opacifi- cation of the aor topulmonary space. However, both of these signs are diffi- cult to assess accurately. Not as useful were d e p r e s s i o n of t he m a i n s t e m bronchus and tracheal deviation. Mar- nocha 11 concluded that the presence of normal visual izat ion of the aortic knob contour and lack of tracheal or esophageal dev ia t ion exclude aor t ic rupture. Other helpful signs for aortic
rupture inc luded depress ion of left m a i n s t e m bronchus and lef t apical cap. Woodring, 17 however, was unable to identify any combination of signs that would exclude the diagnosis with 100% certainty. His op t imum rule de- clares a pat ient to be normal if the aortic contour is normal wi th no me- diast inal widening, apical cap, r ight p a r a t r a c h e a l s t r i p e w i d e n i n g , or nasogastric tube deviation. This still yielded a false-negative rate of 3%.
G i v e n th is l ack of c o n c e n s u s in conclusions, at tempts to quantify the p r o b a b i l i t y of a o r t i c r u p t u r e are useful. Based on our data in this study, the m a j o r i t y of the n e g a t i v e aor- tographs wou ld have been avoided. While this formula would not affect current ind ica t ions for aor tography until validation based on prospective data is achieved, it may at that t ime permit the determination of a cutoff po in t for undergoing aortographs to reduce the n u m b e r of nega t ive aor- tographs whi l e re ta in ing 100% sen- sitivity.
C O N C L U S I O N In this retrospective analysis of pa-
t ients wi th and wi thou t aortic rup- ture, increased med ias t ina l - to -ches t width, loss of aortic contour, and tra- cheal deviation were found to be over- w h e l m i n g l y s ign i f i can t f ind ings of aortic rupture. A formula derived from s t e p w i s e l o g i s t i c r e g r e s s i o n u s ing these variables yielded probabilities of aortic rupture that dear ly delineated the two populations of patients with and wi thout aortic rupture. After test- ing wi th prospective data for valida- tion, choosing a suitably low cutoff point of the probability obtained from this equation can reduce the number of unnecessary aortographs whi le fa- cilitating maximal sensitivity.
R E F E R E N C E S 1. Greendyke RM: Traumatic rupture of the aorta -- special reference to automobile acci- dents. JAMA 1966;195:I19-122. 2. Parmley LF, Mattingly TW, Manion WC, et ah Nonpenetrating traumatic injury of the aor- ta. Circulation 1958;17:1086-1101. 3. Woodring JH, Dillon ML: Radiographic man- ifestations of mediastinal hemorrhage from blunt chest trauma. Ann Thorac Surg 1984;37: I71-178. 4. Wales LR, Morishima MS, Reay D, et ah Nasogastric tube displacement in acute trau- matic rupture of the thoracic aorta: A postmor- tem study. AIR 1982;138:821-823. 5. Simeone JF, Minagi H, Putman CE: Traumat- ic disruption of the thoracic aorta: Significance of the left apical extrapleural cap. Radiology
1975;117:265-268.
6. Fisher RG, Hadlock F, Ben-menachem Y: Laceration of the thoracic aorta and brachioce- phalic arteries by blunt trauma. Radiol Clin North Am 1981;19:91-98.
7. Gundry SR, Williams 8, Burney RE, et ah In- dications for aortography after blunt chest trau- ma: A reassessment of the radiographic findings associated with traumatic rapture of the aorta. Invest Radiol 1983;18:230-237.
8. Sturm JT, Marsh DG, Bodily KC: Ruptured thoracic aorta: Evolving concepts. Surgery 1979;85:363-367.
9. Sturm JT, Olson FR, Cicero JJ: Chest roent- genographic findings in 26 patients with trau- matic rupture of the thoracic aorta. Ann Emerg Med 1983;12:598-600.
10. Barcia TC, Livoni JP: Indications for an- giography in blunt thoracic trauma. Radiology 1983~147:15-19.
11. Mamocha KE, Maglinte DD, Woods J, et ah Blunt chest trauma and suspected aortic rup- ture: Reliability of chest radiograph findings. Ann Emerg Med 1985;14:644-649.
12. Sefczek DM, Sefczek RJ, Deeb ZL: Radio- graphic signs of acute traumatic rupture of the thoracic aorta. A JR 1983; 141:1259-1262.
13. Kirshner R, Seltzer S, D'Orsi C, et ah Upper rib fractures and mediastinal widening: Indica- tions for aortography. Ann Thor~c Surg 1983; 35:450-455.
14. Woodring JH, Fried AM, Hatfield DR, et al: Fractures of first and second ribs: Predictive value for arterial and bronchial injury. AJR 1982; 138:211-215.
15. Fleiss JL: Statistical Methods for Rates and Proportions, ed 2. New York, Wiley, 1981, p 25.
16. Kleinbaum DG, Kupper LL, Morgenstern H: Epidemiologic research: Principles and Quan- tifative Research. Belmont, California, Lifetime Learning Publications, 1978, p 421-446.
17. Woodring JH, Loh FK, Kryscio RJ: Medi- astinal hemorrhage: An evaluation of radio- graphic manifestations. Radiology 1984; 151: 15-21.
18. Woodring JH, Pulmano CM, Stevens RK: The right paratracheal stripe in blunt chest trauma. Radiology 1982;143:605-608.
19. Gundry SR, Burney RE, MacKenzie JR, et ah Assessment of mediastinal widening associated with traumatic rupture of the aorta. J Trauma 1983;23:293-299.
20. Shaikh KA, Schwab CW, Camishion RC: Aortic rupture in blunt trauma. Am Surg 1986;52:47-48.
21. Schwab CW, Lawson RBJ, Lind JF, et ah Aor- tic injury: Comparison of supine and upright portable chest films to evaluate the widened mediastinum. Ann Emerg Med 1984; 13:896-899.
22. Burney RE, Gundry SR, Mackenzie JR, et al: Chest roentgenograms in diagnosis of traumatic rupture of the aorta. Chest 1984;85:605-609.
23. Seltzer SE, D'Orsi C, Kirshner R, et al: Traumatic aortic rupture: Plain radiographic findings.A JR 1981;137:1011-1014.
24. Marnocha KE, Maglinte DD, Woods J, et al: Mediastinal-width/chest width ratio in blunt chest trauma: A reappraisal. AJR 1983;142: 275-277.
44/1333 Annals of Emergency Medicine 16:12 December 1987