Embed Size (px)
Citation preview

Predictive Biomarkers in Lung Cancer Reinhard Buettner
www.lungcancergroup.de
Reinhard Büttner Institute for Pathology Univ at Cologne CIO Köln Bonn [email protected]

The outcome of lung cancer patients remained unchanged (and poor) between 1950-2000
Etzioni et al. 2003
5 ye
ar s
urvi
val %
IV III I-II stage
1950
-195
9
1970
-197
9 19
60-1
969
1980
-198
9 19
90-1
999
2-year OS < 15 %

? Biomarkers define specific clinical entities specific therapeutic vulnerabilities
Kloth M, Buettner R, Changing histopathological diagnostics by genome-based tumor classification. Gene 2014 (review).

Science Translational Medicine Oct 30th, 2013

Michels S, Buettner R, Wolf J (submitted from NGM-L):Overall survival of stage IV with ROS1-rearrangement (n=14) and comparison with other genetically defined stage IV subgroups (n=115). Shaw AT et al, NEJM Sept 2014: Crizotinib in ROS1-rearranged non-small cell lung cancer.
Oncogenic drivers are prognostic (p≤0.001)
ROS1
EML4-ALK
EGFR
FGFR1
KRAS

Michels S, Buettner R, Wolf J (submitted from NGM-L):Overall survival of stage IV with ROS1-rearrangement (n=14) and comparison with other genetically defined stage IV subgroups (n=115). Shaw AT, NEJM Sept 2014: Crizotinib in ROS1-rearranged non-small cell lung cancer.
Oncogenic drivers are prognostic (p≤0.001)
ROS1
EML4-ALK
EGFR
FGFR1
KRAS
Do we need biomarkers to predict therapeutic responses ?
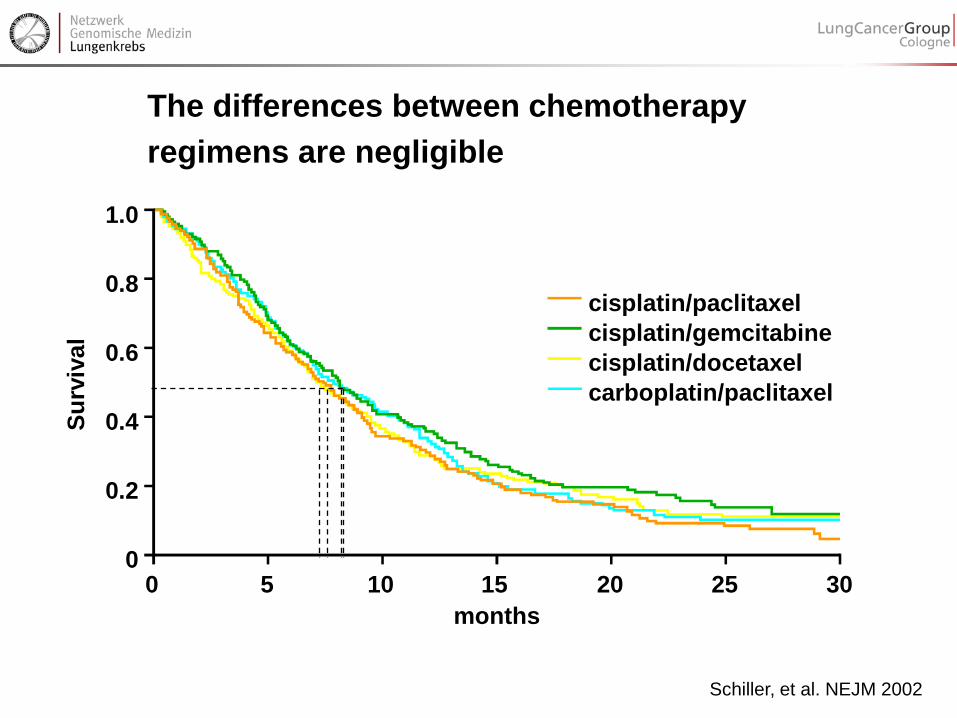
Schiller, et al. NEJM 2002
1.0
0.8
0.6
0.4
0.2
0 0 5 10 15 20 25 30
months
cisplatin/paclitaxel cisplatin/gemcitabine cisplatin/docetaxel carboplatin/paclitaxel
Surv
ival
The differences between chemotherapy regimens are negligible

In unselected patients targeted drugs will add only marginal benefits (if at all)
Shepherd, 2005
Bevacizumab + PC vs PC: SV + 2 m Erlotinib vs. Plac.: SV + 2 m Sandler, 2006
Do we hit the target ?
EGFR-TKI mono anti-VEGF mab + chemotherapy

Activating EGFR-mutations in about 12% of adenocarcinoma
Erlotinib in EGFR-mut. NSCLC: med. OS: 27 months
Rosell, NEJM 2009 EURTAC-study
Paradigm of personalized cancer therapy: EGFR-TKI treatment of EGFR-mutated lung cancer
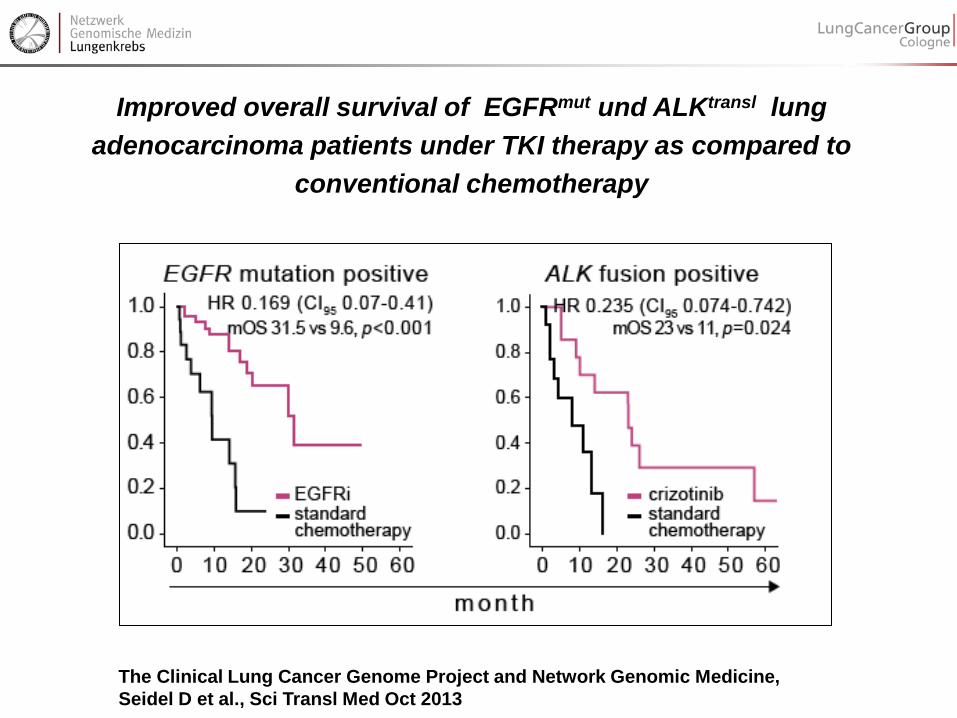
Improved overall survival of EGFRmut und ALKtransl lung adenocarcinoma patients under TKI therapy as compared to
conventional chemotherapy
The Clinical Lung Cancer Genome Project and Network Genomic Medicine, Seidel D et al., Sci Transl Med Oct 2013

unknown
KRAS
EGFR
ALK BRAF PIK3CA
HER2 MET RET ROS
unknown
FGFR1amp
PTENmut
PTENloss
PIK3CAmut
KRASmut DDR2mut
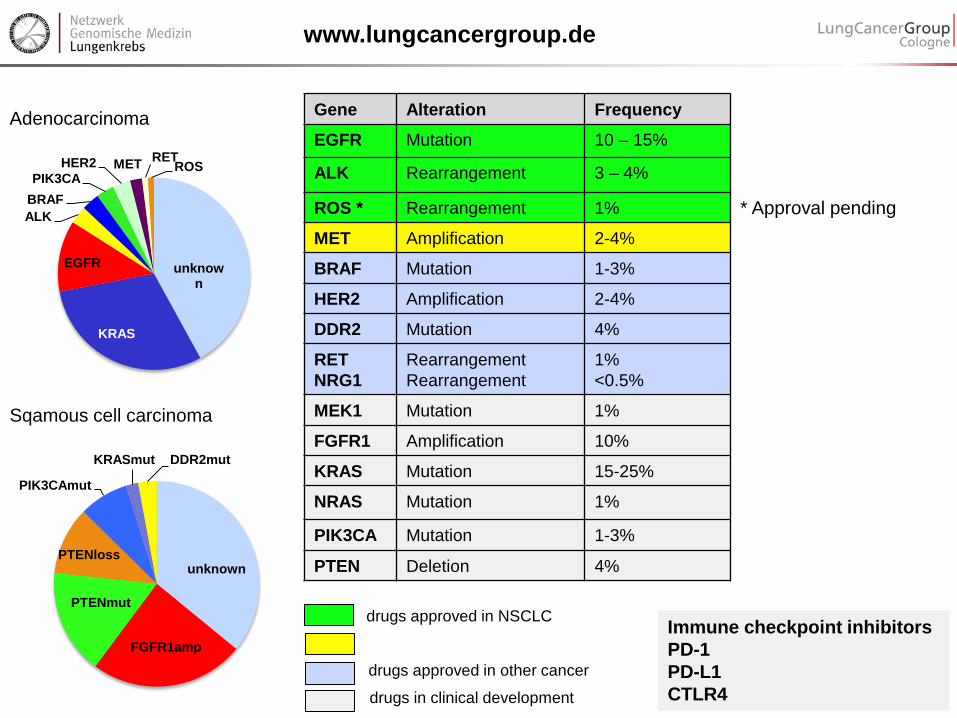
Adenocarcinoma
Sqamous cell carcinoma
LCGC personalized trial portfolio
www.lungcancergroup.de
Gene Alteration Frequency
EGFR Mutation 10 – 15%
ALK Rearrangement 3 – 4%
ROS * Rearrangement 1%
MET Amplification 2-4%
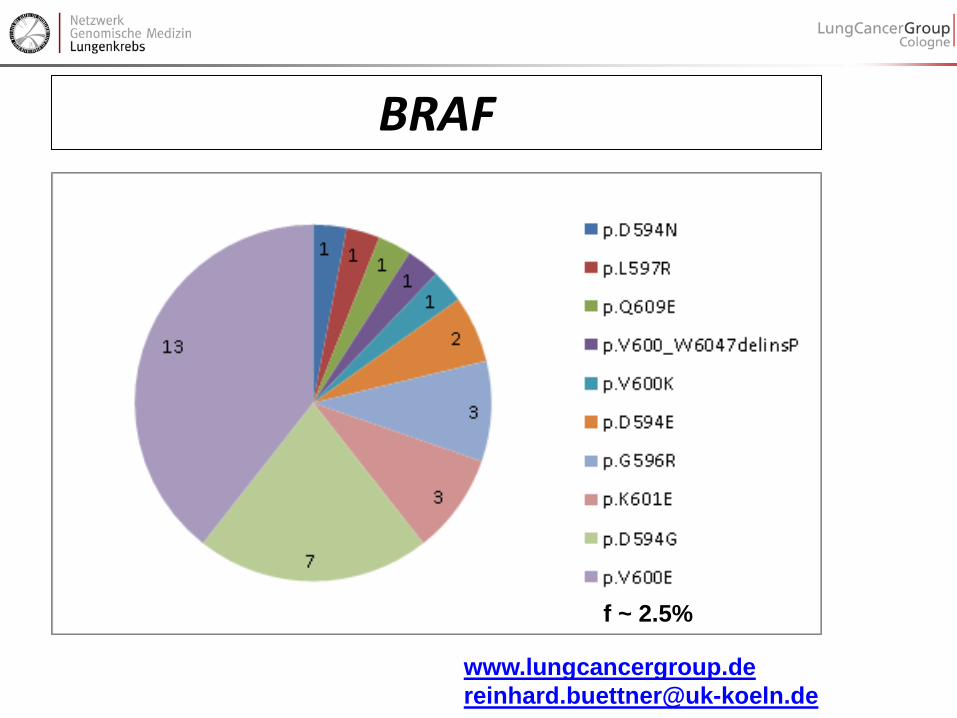
BRAF Mutation 1-3%
HER2 Amplification 2-4%
DDR2 Mutation 4%
RET Rearrangement 1%
MEK1 Mutation 1%
FGFR1 Amplification 10%
KRAS Mutation 15-25%
NRAS Mutation 1%
PIK3CA Mutation 1-3%
PTEN Deletion 4%
drugs approved in NSCLC
drugs approved in other cancer
drugs in clinical development
Immune checkpoint inhibitors PD-1 PD-L1 CTLR4
* Approval pending

EGFR ALK ROS1 Resistance
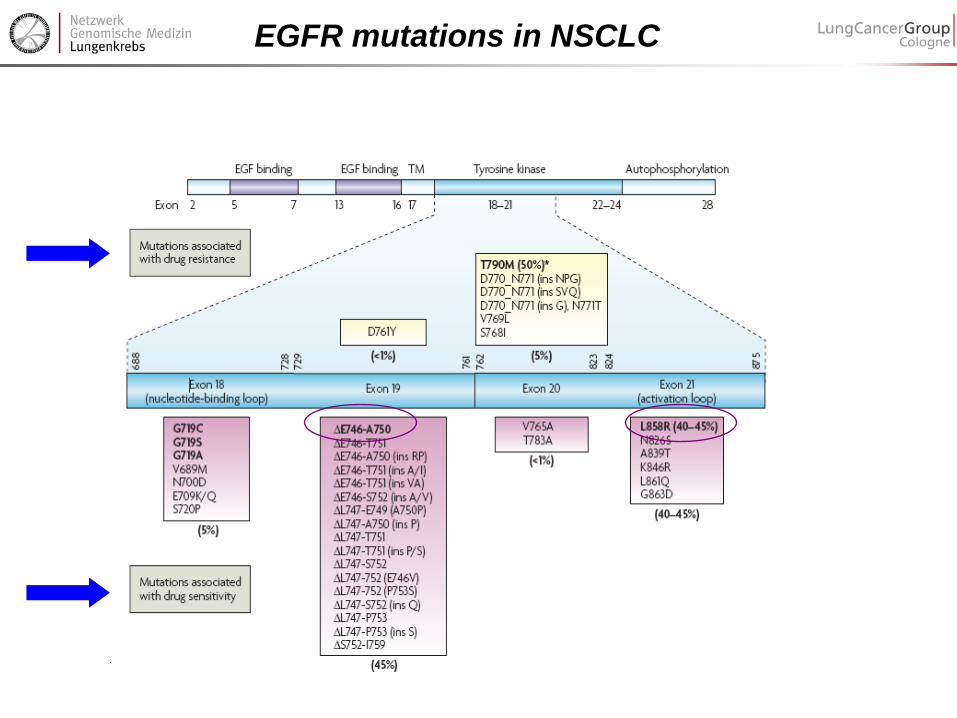
EGFR mutations in NSCLC
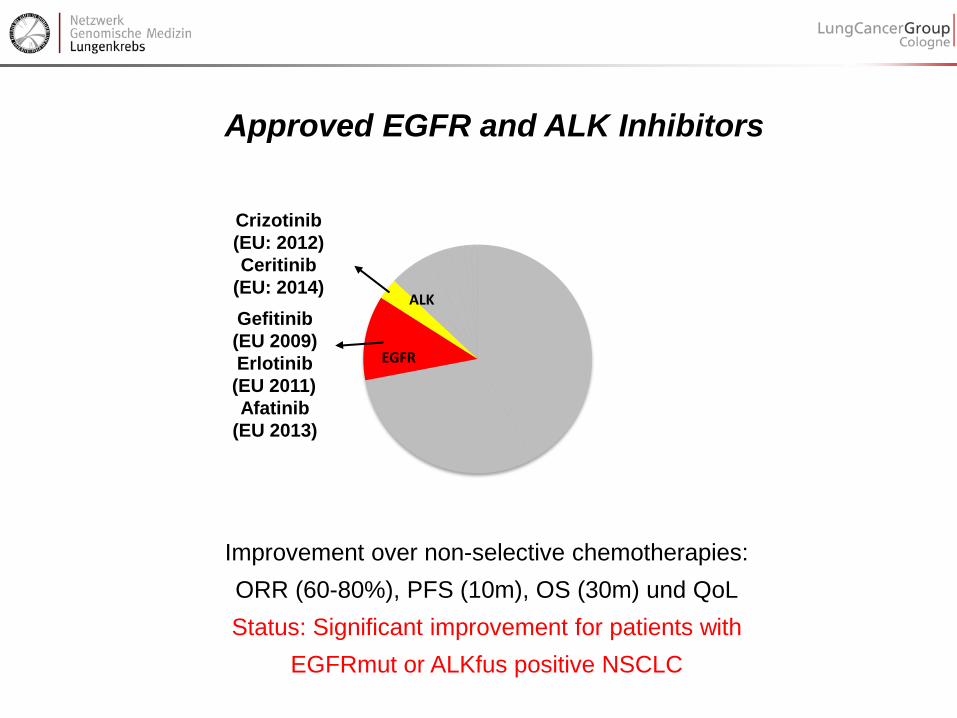
Approved EGFR and ALK Inhibitors
EGFR
ALK
Crizotinib (EU: 2012) Ceritinib
(EU: 2014) Gefitinib (EU 2009) Erlotinib (EU 2011) Afatinib
(EU 2013)
Improvement over non-selective chemotherapies: ORR (60-80%), PFS (10m), OS (30m) und QoL Status: Significant improvement for patients with
EGFRmut or ALKfus positive NSCLC

Molecular testing prior to first-line therapy recommended by International Guidelines
• Test for activating EGFR-mutations and ALK-fusions in all non-resectable cases of NSCLC
• Test all non-pure squamous • Test squamous in never smokers
Lindeman et al. J Thorac Oncol. 2013;8:823-859 // NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non–Small Cell Lung Cancer V.2.2013 // Peters et al. Ann Oncol. 2012;23 Suppl 7:vii56-64.

ALK-fus positive NSCLC (f=4%): Fast-track development and Approval of Crizotinib Phase I/II (~150 patients)
Soda, Nature 2007
Bang, ASCO 2010, Kwak NEJM 2010 FDA-approval: 2011 EMEA-appoval: 2012
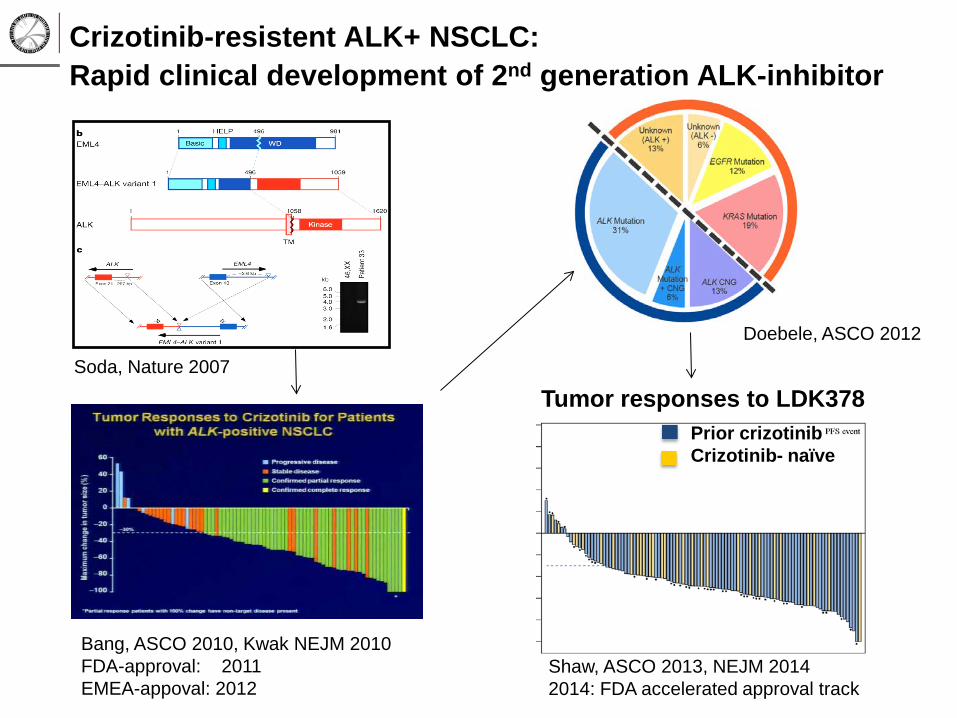
Crizotinib-resistent ALK+ NSCLC: Rapid clinical development of 2nd generation ALK-inhibitor
Shaw, ASCO 2013, NEJM 2014 2014: FDA accelerated approval track
Doebele, ASCO 2012
Soda, Nature 2007
Bang, ASCO 2010, Kwak NEJM 2010 FDA-approval: 2011 EMEA-appoval: 2012
Prior crizotinib Crizotinib- naïve
Tumor responses to LDK378

36 years old female Turkish patient June 2010: pneumonectomy of a sarcoma with pleural involvement July 2011: relapse, diagnosis of IMFT with ALKfus+ Aug 2011: crizotinib with excellent remission May 2014: relapse of tumor growth, multiple new thoracic wall nodules, gate-keeper mutation c3806G>C p.1269A ceritinib with excellent remission
IMFT under crizotinib (n=3)

ALK-amplification after crizotinib resistance

JTO, March 2014

July2013-June2014 ALK-FiSH+ IHC+ Pre-tested by FiSH 42 34 (81%) Pre-tested by IHC n=174 0 2 (98.7 %) July2013-June2014 ROS1-FiSH+ IHC+ (D4D6) Pre-tested by FiSH 20 11 (55 %)
FiSH/IHC discordance data from NGM
ALK-Harmonization Trial (D3F5 Optiview) von Laffert M, JTO, 2014

ASCO June 2012: Crizotinib highly effective in ROS1fus+ AdCA Shaw et al.,ASCO 2012 #7508
Aug. 2012: ROS1-FISH in NGM established, Bos Lung Cancer 2012
Sept. 2012: Crizotinib – Start Sept 2012 complete remission until today. EUCROSS-trial PI Wolf J, Pathol Buettner R
ROS1 a new oncogenic driver
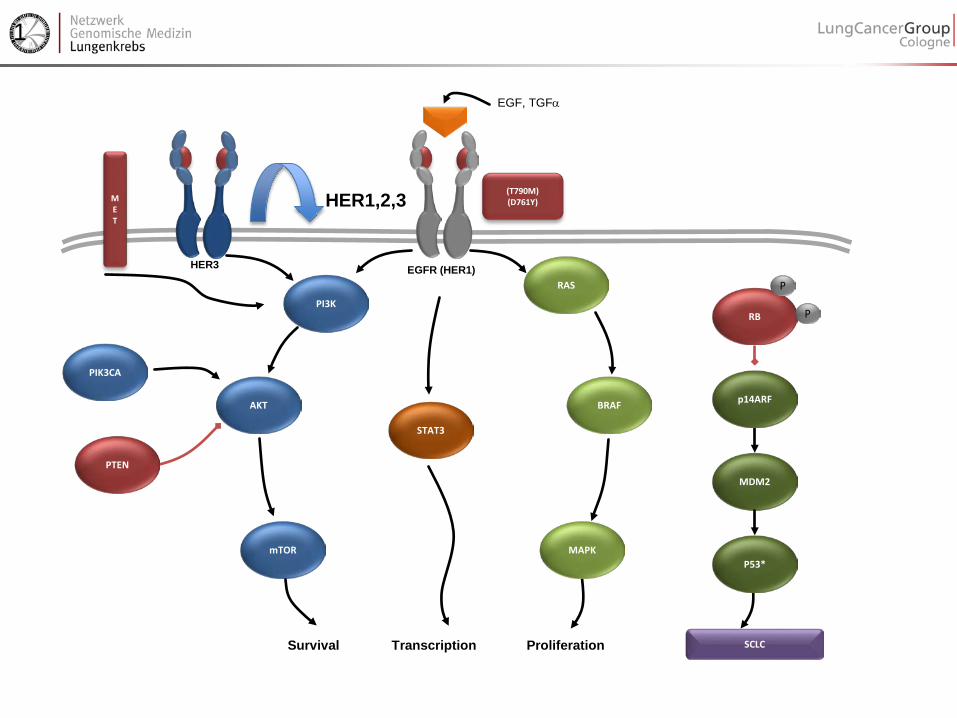
Resistance in EGFR mut + lung cancer
• Resistance emerges in almost all patients • T790M mutation accounts for app. 50% • MET amplification (app 10-20%) • Pi3-kinase activation • EMT • SCLC transformation
AKT
mTOR
PIK3CA
RAS
MAPK
BRAF
PI3K
EGFR (HER1)
Survival
HER3
(T790M) (D761Y)
EGF, TGFα
STAT3
RB
P
P
MDM2
P53*
SCLC
p14ARF
Transcription Proliferation
PTEN
M E T
1
HER1,2,3

AKT
mTOR
PIK3CA
RAS
MAPK
BRAF
PI3K EGFR (HER1)
Survival
HER3
(T790M) (D761Y)
EGF, TGFα
STAT3
RB P
P
MDM2
P53*
SCLC
p14ARF
Transcription Proliferation
PTEN
M E T
1
MET wt
MET amp
Cancer Treatment Comm., 2013
Understanding Mechanisms of Resistance

− SCF binding site − 5 IgG domains
2 tyrosine kinase domains
• Structure of a tyrosine kinase (c-KIT)
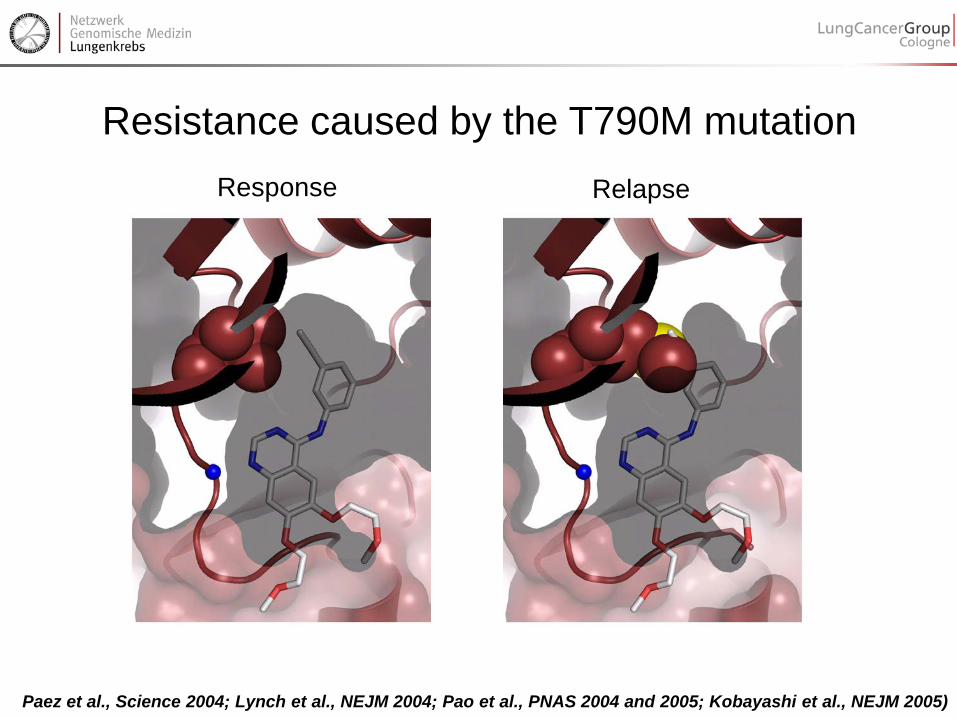
Resistance caused by the T790M mutation Relapse Response
Paez et al., Science 2004; Lynch et al., NEJM 2004; Pao et al., PNAS 2004 and 2005; Kobayashi et al., NEJM 2005)

Overcoming resistance by structure-based compound design
Zhou et al., Nature 2009

Clinical efficacy of next-gen EGFR inhibitors
CO-1686
AZD9291

Precision medicine: erlotinib-crizotinib Kombination
SD SD
Molecular findings EGFR L858R High-level MET amplification EGFR T790M

Conclusions
• All non-resectable cases of NSCLC should be tested for EGFR, ALK, ROS, except Squamous Cell Carcinomas in smokers
• Most frequent and actionable EGFR mutations are in exons 19 and 21, few others in exon 18
• FISH is the current standard for detection of ALK or ROS1 gene fusions
• Every tumor relapsing after therapy with TKI should undergo rebiopsy and analysis for resistance mechanisms
• The most frequent actionable resistance mechanisms of EGFRmut-positive adenocarcinomas to TKIs are T790M gatekeeper mutations and Met-amplifications

DDR2 mutations occur in a higher frequency in Adeno compared to
SCC revealed by NGS
Andreas Scheel Institute of Pathology, Cologne Margarethe Odenthal Claudia Vollbrecht Sabine Merkelbach-Bruse Jana Fassunke Michaela Ihle Helen Künstlinger Carina Heydt Theresa Buhl Ursula Rommerscheidt-Fuss Alexandra Florin Frank Ueckeroth Michael Kloth Michal R Schweiger Martin Sos Peter Nürnberg Cologne Center for Genomics (Cologne) Janine Altmüller Kerstin Becker Christian Becker Roman Thomas Institute of Genomics (Cologne) Martin Peifer Thomas Henkel Targos (Kaseel) Katrin Stamm Jürgen Wolf Center for Integrated Oncology Cologne/ Bonn Lung Cancer Group Cologne


Novel Biomarkers in Lung Cancer Reinhard Buettner
www.lungcancergroup.de
Reinhard Büttner Institute for Pathology Univ at Cologne CIO Köln Bonn [email protected]
unknown
KRAS
EGFR
ALK BRAF PIK3CA
HER2 MET RET ROS
unknown
FGFR1amp
PTENmut
PTENloss
PIK3CAmut
KRASmut DDR2mut
Adenocarcinoma
Sqamous cell carcinoma
www.lungcancergroup.de
Gene Alteration Frequency
EGFR Mutation 10 – 15%
ALK Rearrangement 3 – 4%
ROS * Rearrangement 1%
MET Amplification 2-4%
BRAF Mutation 1-3%
HER2 Amplification 2-4%
DDR2 Mutation 4%
RET NRG1
Rearrangement Rearrangement
1% <0.5%
MEK1 Mutation 1%
FGFR1 Amplification 10%
KRAS Mutation 15-25%
NRAS Mutation 1%
PIK3CA Mutation 1-3%
PTEN Deletion 4%
drugs approved in NSCLC
drugs approved in other cancer
drugs in clinical development
Immune checkpoint inhibitors PD-1 PD-L1 CTLR4
* Approval pending

FGFR1 amplification Sqamous cell cancer (SqCC) of the lung (f=12%)
Genomic disovery Preclinical validation
Weiss et al., Sci Transl Med 2010 Schildhaus HU et al,
Mod Pathol, 2012
FISH-diagnostics
Clinical evaluation
Chromosome 8p geography
Malchers et al. Cancer Discovery 2013
Understanding response on the molecular level FIM trial BGJ398 in
FGFR1-ampl. SQLC Nogova, #8034 ASCO 2014
ORR: 15,4%

Cologne patient at 100mg BGJ398:
day 28
baseline
baseline
day 56
AACR2012, LBA, J. Wolf et al. ASCO#7022, L. Nogova et al. 2014
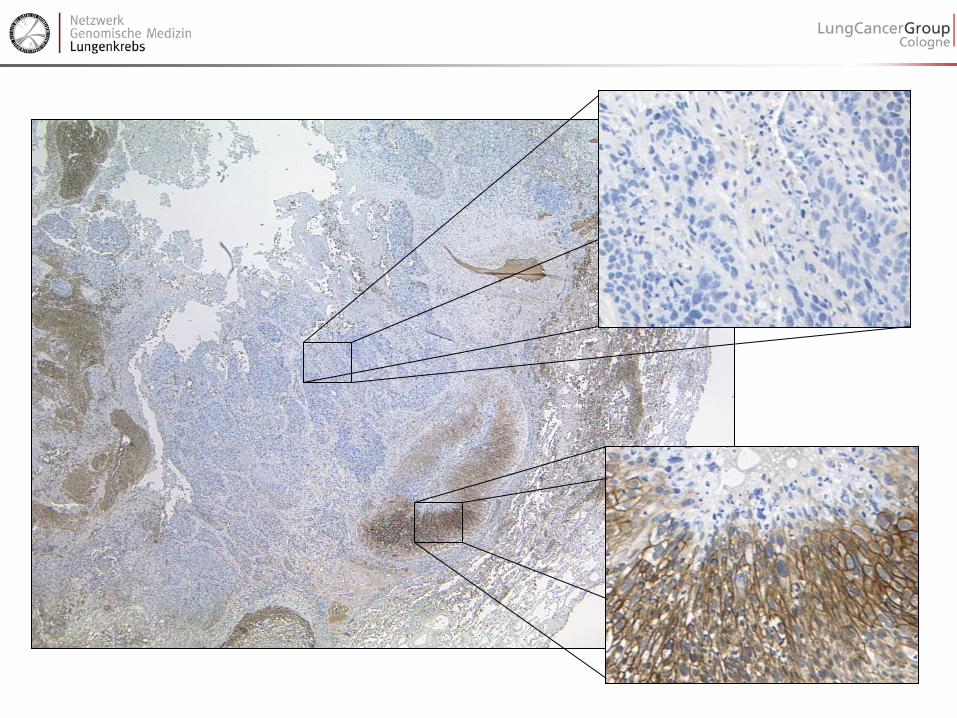
Emerging topics: FGFR FISH in lung cancer pFGFR1 expression by ICH FGFR1-3 lesions in tumors other than lung cancer
Reinhard Büttner Institute for Pathology UoC & CIO Köln

FGFR1 amplification (Cologne Score) Count 60 tumor cells (= 3 high power fields HPF à 20) High level: • FGFR1 / CEN8 ratio ≥ 2.0 • FGFR1 copy number (signals per tumor cell nucleus) ≥ 6 • percentage of tumor cells containing ≥ 15 FGFR1 signals or large clusters is ≥ 10% Low level: • percentage of tumor cells containing ≥ 5 FGFR1 signals is ≥ 50% Schildhaus HU et al, Mod Pathol 2012;25:1473-1480
Cytovision kit FGFR1(green)/cen8(red)

+ -
+ 38 11
- 5 14
pFGFR1
FGFR1amp.
p = 0.00014
n=68
FGFR1 – expression: amplification correlates with pFGFR1 staining
kindly provided by LC Heukamp

FGFR1-IHC (FISH pos-CS high)
p-FGFR1 (Abnova)
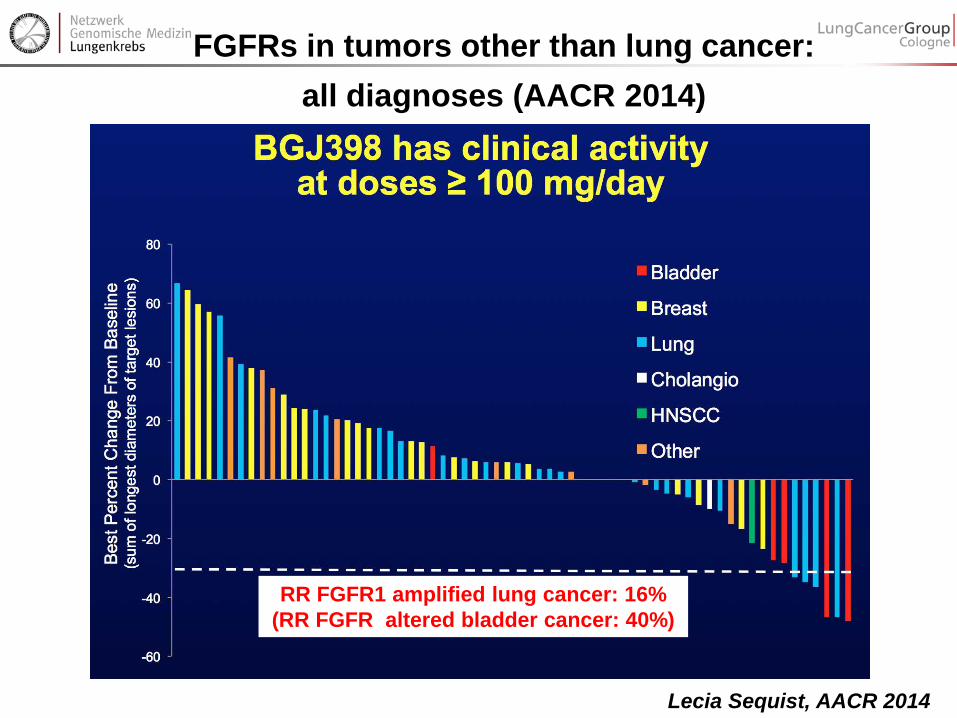
FGFRs in tumors other than lung cancer: all diagnoses (AACR 2014)
Lecia Sequist, AACR 2014
RR FGFR1 amplified lung cancer: 16% (RR FGFR altered bladder cancer: 40%)
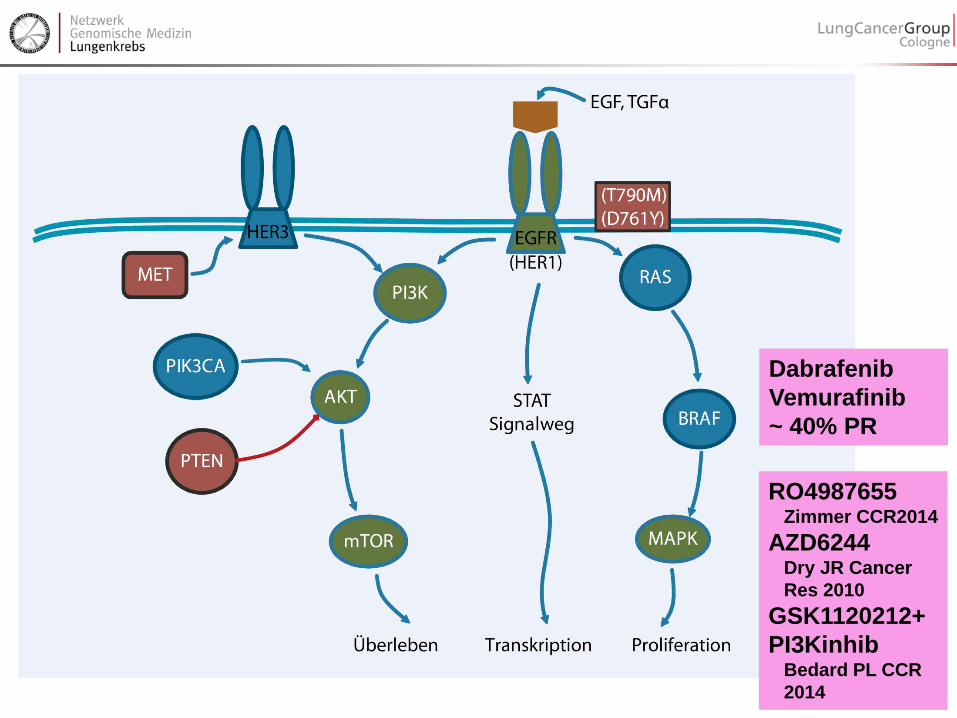
Dabrafenib Vemurafinib ~ 40% PR
RO4987655 Zimmer CCR2014 AZD6244 Dry JR Cancer Res 2010 GSK1120212+PI3Kinhib Bedard PL CCR 2014
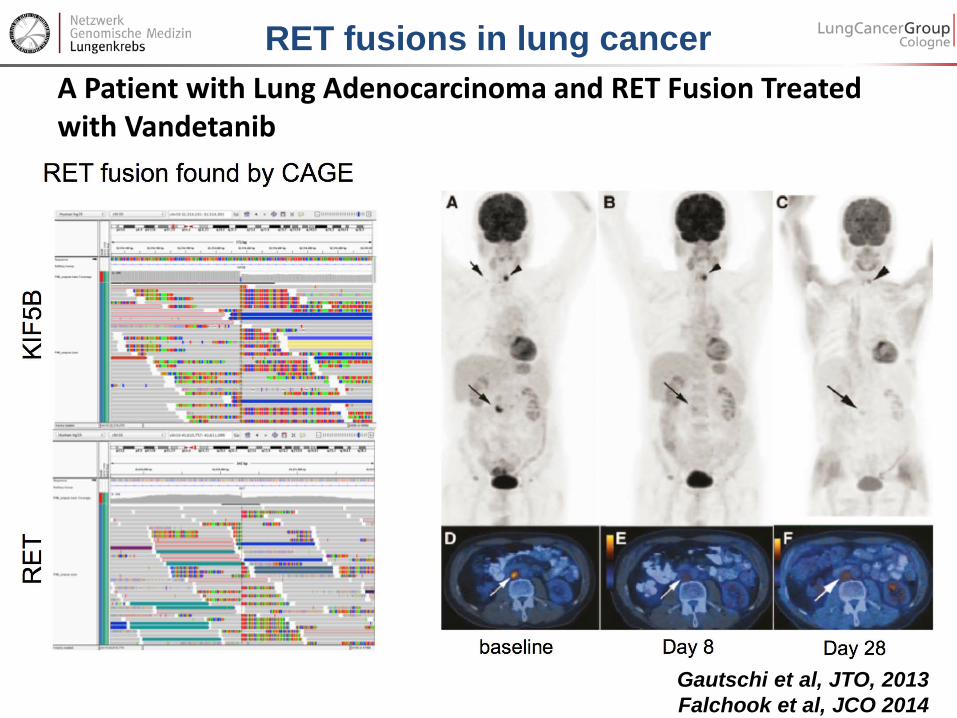
A Patient with Lung Adenocarcinoma and RET Fusion Treated with Vandetanib
Gautschi et al, JTO, 2013 Falchook et al, JCO 2014
RET fusions in lung cancer
• Mouse model: Saito M, Carcinogenesis 2014 • Falchook GS, JCO 2014 • Mukhopadhyay S, JTO 2014
• Vandetanib • Carbozantinib • Alectinib

Fernandez-Cuesta Cancer Discov 2014, Nakaoku , ClCR 2014
CD74-NRG1 fusions in mucinous lung adenocarcinoma
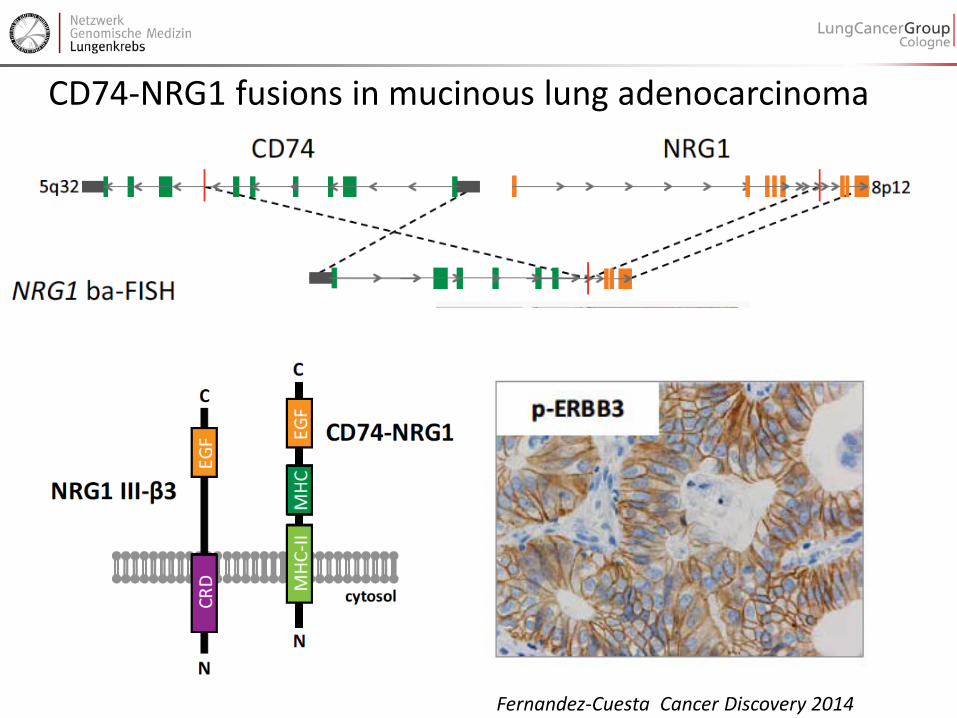
CD74-NRG1 fusions in mucinous lung adenocarcinoma
Fernandez-Cuesta Cancer Discovery 2014
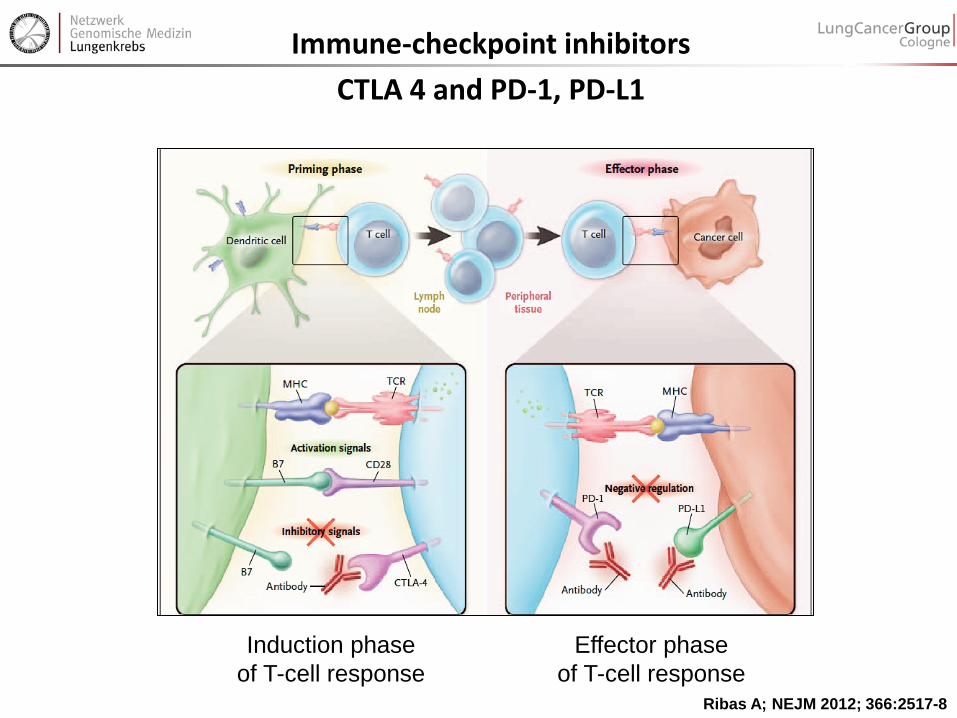
Ribas A; NEJM 2012; 366:2517-8
Immune-checkpoint inhibitors CTLA 4 and PD-1, PD-L1
Induction phase of T-cell response
Effector phase of T-cell response

“PD-1 pathway–targeting agents” in clinical development
McDermott DF et al; Cancer Medicine 2013; doi: 10.1002/cam4.106
/Astra-Zeneca

Nivolumab (anti-PD1) phase I trial: frequent and partly long lasting responses
65 / 306 pts with CR/PR: • 30 of 65 (46%) responses
evident at first tumour evaluation (8 weeks)
• 42 of 65 (65%) pts with
responses >1 year • 35 of 65 (54%) responses
ongoing at time of data analysis • Responses persisted off-drug
Maximum treatment duration
NSCLC
MEL
RCC
Topalian, et al. Clin Oncol 2013;31(suppl): abstr 3002

Responses after initial progression with anti-PD1 therapy immune associated pattern of response
Topalian SL et al; N Engl J Med 2012; 366:2443-54
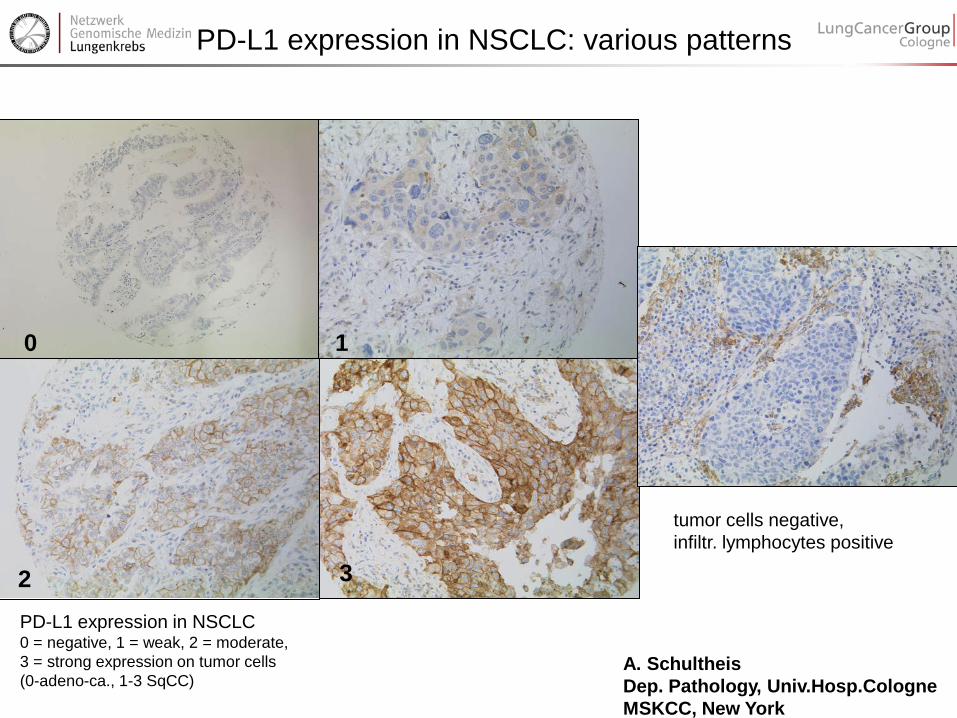
0 1
2 3
tumor cells negative, infiltr. lymphocytes positive
PD-L1 expression in NSCLC: various patterns
PD-L1 expression in NSCLC 0 = negative, 1 = weak, 2 = moderate, 3 = strong expression on tumor cells (0-adeno-ca., 1-3 SqCC)
A. Schultheis Dep. Pathology, Univ.Hosp.Cologne MSKCC, New York
The challenge: multiple tests on limited patient material Low tumor cell contect in the background of normal tissues
Molecular Diagnostics

EGFR-Diagnostics

Enrichment

NGS - Datenauswertung


Meyerson M, Gabriel S, Getz G. Nat Rev Genet. 2010 “ Advances in understanding cancer genomes through second-generation sequencing”
Genome alterations detectable by NGS

Molecular Staging IAP Case 2
Diagnosis: Two tumors of an invasive pulmonary adenocarcinoma of the lung in S2 and S9 as well as an AIS in S9. Initial TNM: cT4, cN1, cM0 EGFR TKI Therapy option? Separate primary tumors due to field cancerization or metastasis?

S2: KRAS: c.34G>T p.G12C; TP53: c.215C>G p.P72R
S9: KRAS: c.35G>T p.G12V; TP53: c.215C>G p.P72R;
S9 AIS: KRAS: c.34G>A p.G12S; TP53: c.215C>G p.P72R; TP53: c.818G>T p.R273L

Genes particularly useful for clonal analysis of multiple (solid) tumors TP53 KRAS, NRAS BRAF PI3K PTEN Mitochondrial Genome* * Adam AC, Faudou V, Paschen SA, Adam OM, Kahl P, Drebber U, Fischer HP, Büttner R. J Pathol. 2012 Nov;228(3):333-40.

Surveillance of solid tumors by liquid biopsies

Genomic Information adds to ….. Classification entity defining Prediction of Response to Therapy rational therapies vs empirical therapies Prognosis of Clinical Course no therapy – early therapy – targeted therapy multiplexing larger genes (BRCA1/2) Tumour Diagnostics, Staging mets versus multiple primary - CUP Surveillance, Relapse, Resistance managing cancer as a chronic disease

DDR2 mutations occur in a higher frequency in Adeno compared to
SCC revealed by NGS
Andreas Scheel Institute of Pathology, Cologne Margarethe Odenthal Claudia Vollbrecht Sabine Merkelbach-Bruse Jana Fassunke Michaela Ihle Helen Künstlinger Carina Heydt Theresa Buhl Ursula Rommerscheidt-Fuss Alexandra Florin Frank Ueckeroth Michael Kloth Michal R Schweiger Martin Sos Peter Nürnberg Cologne Center for Genomics (Cologne) Janine Altmüller Kerstin Becker Christian Becker Roman Thomas Institute of Genomics (Cologne) Martin Peifer Thomas Henkel Targos (Kaseel) Katrin Stamm Jürgen Wolf Center for Integrated Oncology Cologne/ Bonn Lung Cancer Group Cologne