Embed Size (px)
Citation preview

w w w . e l s e v i e r . c o m / l o c a t e / p a i n
PAIN�
153 (2012) 2370–2379
Predictors for postpartum pelvic girdle pain in working women: TheMom@Work cohort study
Suzanne G.M. Stomp-van den Berg a,b,c, Ingrid J.M. Hendriksen a,c, David J. Bruinvels b,d, Jos W.R. Twisk e,f,Willem van Mechelen a,b,d, Mireille N.M. van Poppel a,b,⇑a Body@Work, Research Centre Physical Activity, Work and Health, TNO-VUmc, VU University Medical Centre, Amsterdam, The Netherlandsb Department of Public and Occupational Health, EMGO Institute, VU University Medical Centre, Amsterdam, The Netherlandsc TNO Quality of Life, Leiden, The Netherlandsd Research Centre for Insurance Medicine: A Collaboration Between AMC-UWV-VUmc, Amsterdam, The Netherlandse Department of Clinical Epidemiology and Biostatistics, VU University Medical Centre, Amsterdam, The Netherlandsf Department of Health Sciences, Vrije Universiteit, Amsterdam, The Netherlands
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
a r t i c l e i n f o a b s t r a c t
Article history:Received 27 December 2011Received in revised form 31 July 2012Accepted 3 August 2012
Keywords:PregnancyReturn to workPredictorsPelvic girdle painPostpartum
0304-3959/$36.00 � 2012 International Associationhttp://dx.doi.org/10.1016/j.pain.2012.08.003
⇑ Corresponding author. Address: Department of PuEMGO Institute for Health and Care Research, VU Under Boechorststraat 7, 1081 BT Amsterdam, The Neth
E-mail address: [email protected] (M.N.M
The objective of this study was to examine which factors during pregnancy and postpartum predict pelvicgirdle pain (PGP) at 12 weeks postpartum among working women. A total of 548 Dutch pregnant employ-ees were recruited in 15 companies, mainly health care, child care, and supermarkets. The definition ofPGP was any pain felt in the pelvic girdle region at 12 weeks postpartum. Participants received question-naires at 30 weeks of pregnancy and at 6 and 12 weeks postpartum with demographic, work-related,pregnancy-related, fatigue, psychosocial, PGP-related and delivery-related questions. Univariate andmultiple logistic regression analyses were performed. Almost half of the women experienced pain in theirpelvic girdle at 12 weeks postpartum. However, the level of pain and the degree of disability due to post-partum PGP was low. Pregnancy-related predictors for PGP at 12 weeks were history of low back pain,higher somatisation, more than 8 hours of sleep or rest per day, and uncomfortable postures at work.The pregnancy and postpartum-related predictors were: more disability at 6 weeks, having PGP at6 weeks, higher mean pain at 6 weeks, higher somatisation during pregnancy and at 6 weeks postpartum,higher birth weight of the baby, uncomfortable postures at work and number of days of bed rest. Based onthese results, it is concluded that extra attention should be given to women who experience PGP duringpregnancy to prevent serious PGP during late pregnancy and postpartum. More research is needed toconfirm the roles of hours of sleep, somatisation, and bed rest in relation to PGP.
� 2012 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
1. Introduction tively few women recover from PGP after 3 months postpartum
The majority of women intend to return to work after the birthof their first child [30], and in the Netherlands this is even 90% ofall working women [5]. However, many of these women experi-ence postpartum health problems that may hinder or delay returnto work. One of the most commonly occurring health problemsduring the postpartum period is pelvic girdle pain (PGP) [6].
Although the majority of women recover from PGP within3 months after delivery, about 33% to 38% women report to expe-rience PGP after this period [13,46]. Based only on prospectivestudies with objectively verified symptoms, Kanakaris et al. [19]reported a postpartum prevalence of between 16% and 25%. Rela-
for the Study of Pain. Published by
blic and Occupational Health,iversity Medical Centre, Vanerlands.. van Poppel).
[29]. Even though the majority (80%) of women with postpartumPGP experience only mild complaints, PGP causes serious problemsfor 8% of these women [27,52]. The exact pathology of PGP remainsunknown [52]. No distinction between low back pain and girdlepain was made in the majority of the literature, and there is no dif-ference in prognosis between PGP and low back pain [7].
Women with PGP may experience many problems in their dailyactivities [22]. Because of these problems with performing theirusual chores, women with PGP often have to report sick for work[22,43]. A retrospective Dutch study found that 29% of the workingwomen were on sick leave for 2 weeks or more, directly after theend of their maternity leave, which is between 10 and 12 weeksafter delivery in the Netherlands [6]. About 56% of this postpartumsick leave was caused by pelvic and/or back pain. Sick leave be-cause of back pain during pregnancy was found to be a risk factorfor postpartum PGP [2,26,26].
Elsevier B.V. All rights reserved.

S.G.M. Stomp-van den Berg et al. / PAIN�
153 (2012) 2370–2379 2371
Even though many etiologic and risk factors have been de-scribed [4,52], little is known about work-related factors that pre-dict postpartum PGP. Previously, strenuous work was found to be arisk factor for postpartum PGP [52], and more recently, fixed even-ing work, rotating shifts (without night shift), physically strenuouswork, and jobs with high psychosocial strain [17]. Job status, num-ber of working hours per week, working posture and carrying hea-vy burdens during work were not related to pelvic pain [17]. Otherearlier reported risk factors for postpartum PGP are pelvic painduring pregnancy [24], history of low back pain, a history of PGP,and younger maternal age [52].
It is important to identify predictors for postpartum PGP, be-cause professionals such as physicians, obstetricians, and mid-wives, and also employers, may use them to identify women atrisk for PGP and develop and implement preventive measures.These professionals can also give extra guidance aimed at the pre-vention of PGP during pregnancy or in the early postpartum periodto women at risk for developing postpartum PGP.
This article describes the results of a cohort study on postpar-tum PGP among working women, that is part of the Mom@Workstudy [42]. The aim was to establish which factors during preg-nancy and postpartum period predicted PGP at 12 weeks postpar-tum among working women.
2. Methods
2.1. Study design
The Mom@Work study on return to work after childbirth wassimultaneously designed as a randomised controlled trial (RCT)and cohort study. Detailed information about the design of theMom@Work study can be found elsewhere [42]. The Medical Eth-ics Committee of VU University Medical Centre, Amsterdam, theNetherlands, approved the study design, study protocol, and in-formed consent procedure.
2.2. Study population
Dutch pregnant employees could enter the Mom@Work cohortstudy between January 1, 2004, and March 31, 2006. Workers wereeligible if they were pregnant, worked for at least 12 hours per weekat 1 of the 15 participating companies, had the intention to return towork after maternity leave, were sufficiently fluent in the Dutch lan-guage, and gave written informed consent. Women were not eligibleif they met any of the following exclusion criteria: definitely notreturning to work after maternity leave, having experienced miscar-riage or delivery before 27 weeks, receiving a full disability benefit,or submitting an application for a full disability benefit.
2.3. Outcome measurements
The primary dependent variable, measured with a questionnaireat 12 weeks postpartum, was the presence of postpartum PGP. Inaccordance with the Maastricht PGP cohort study [3], participantswere asked whether they experienced pain in the lower back, but-tocks, the pubic symphysis, groin, or radiation into either or bothlegs during the past 6 weeks. Pain intensity for each location wasmeasured on an 11-point scale, where zero was defined as ‘‘no pain’’and 10 as ‘‘much pain’’. The mean pain score was calculated forall locations. Locations with zero pain were not included in thismean.
2.4. Predictors
A broad range of variables was measured with a postal ques-tionnaire at each measurement. The baseline measurement
consisted of two parts: a first part (T0) when the employee madeherself known as a participant between 6 weeks and 40 weeks oftheir pregnancy (mean, 25 weeks), and a second part at 30 weeksof pregnancy (T1). Participants received also a postal questionnaireat 6 weeks (T2) postpartum. An overview of all measurements andmore details about the used instruments are described in the de-sign paper about the Mom@Work study [42]. Based on the contentand timing of the variables, we grouped predictors in 10 clusters; 6clusters of predictors were measured during pregnancy and 4 clus-ters postpartum.
The following so called ‘pregnancy-related’ clusters of predic-tors were measured.
2.4.1. Demographic predictorsDemographic predictors measured included age, marital status,
pre-pregnancy body weight, body height, education, income, eth-nicity, smoking behaviour, and alcohol use during pregnancy.
2.4.2. Work-related predictorsWork-related predictors measured included profession, work-
ing hours per week, work overtime in hours per week, travel timein hours per week, work shifts, work sector, type of job (sitting,standing, physically active job), job satisfaction, relation withsupervisor and sick leave during pregnancy due to PGP. Also, sev-eral scales of the Job Content Questionnaire (JCQ) were used: skilldiscretion, social support, psychological job demands, decisionauthority, job insecurity, physical exertion, tempo and posture[20]. These subscales of the JCQ had Cronbach’s a coefficients be-tween 0.70 and 0.79 [20].
2.4.3. Pregnancy-relatedPregnancy-related predictors measured included sick leave dur-
ing previous pregnancies, time between pregnancies, twin preg-nancy, miscarriages, method of conception, rank of pregnancy,and child.
2.4.4. FatigueFatigue-related predictors measured included fatigue (11-point
scale and CIS; Checklist Individual Strength; Cronbach’s a of 0.93for fatigue and 0.85 for poor concentration) [48,49], hours of sleepor rest per day, and satisfaction about sleep.
2.4.5. Psychosocial predictorsPsychosocial predictors measured included coping style (Utr-
echt Coping List [UCL], Cronbach’s a between 0.64 and 0.82[16,41]]), daily difficulties (short version of the Everyday ProblemsChecklist [EPCL], test–retest correlation of 0.85 [31,50]), health andquality of life (36-Item Short Form Health Survey (SF-36; RAND-36,with Cronbach’s a coefficients between 0.71 and 0.92 and test–retest correlations of 0.58 to 0.82 [47,51]), social support (SocialSupport List [SSL], test–retest correlations for subscales rangingfrom 0.56 to 0.66 [11,32]), life events, distress, fear and somatisa-tion (Four Dimensional Symptom Questionnaire [4DSQ]; Cron-bach’s a for subscales from 0.67 to 0.81 [44]), and depression(Edinburgh Postnatal Depression Scale [EPDS]; Cronbach’s a of0.80 [10,35]).
2.4.6. PGP-related predictorsPGP-related predictors included history of back and/or pelvic
pain (no/yes), history of pregnancy-related back and/or pelvic pain(no/yes), disability (Roland-Morris Disability-24 questionnaire[RDQ]; test–retest correlation of 0.92 [12,37,39]), mean pain inten-sity of pain in the lower back, buttocks, pubic symphysis, groin, orradiation into either or both legs (11-point scale anchored by ‘‘0’’for ‘‘no pain’’ and ‘‘10’’ for ‘‘many pain’’) and PGP at 30 weeks preg-nancy (no/yes).

2372 S.G.M. Stomp-van den Berg et al. / PAIN�
153 (2012) 2370–2379
The following so-called ‘postpartum-related’ clusters of predic-tors were measured:
2.4.7. Delivery-related predictorsDelivery-related predictors included body weight gain during
pregnancy, mode and duration of delivery, place of birth, deliveryexperience (eleven-point scale anchored by ‘‘0’’ for ‘‘very easydelivery’’ and ‘‘10’’ for ‘‘very difficult delivery’’), rupture or episiot-omy during delivery, induced labour or extra stimulation duringdelivery, birth weight of infant in grams, breastfeeding, days ofcomplete bed rest after delivery, days in hospital after delivery,and days between delivery and the first time of stair walking.
All fatigue, psychosocial and PGP predictors were also measuredat 6 weeks postpartum with the same instruments as used at30 weeks pregnancy, except for coping and daily difficulties. Thelatter ones were measured only at 30 weeks pregnancy.
2.5. Statistical analysis
Two prediction models were created: 1 for pregnancy-relatedpredictors, and 1 for pregnancy- and postpartum-related predic-tors. Both models were created because health care providersshould be able to recognise predictors during pregnancy and dur-ing the postpartum period. Before developing the 2 predictionmodels, the linearity of the relationship with the outcome waschecked for all ordinal and continuous variables. The first stepfor each of the prediction models was an univariate logistic regres-sion analysis with each presumed predictor. To be sure not to ex-clude relevant factors in the multivariate analyses, variables withP < .20 were selected for the second step. In this second step, abackward selection procedure was used to obtain a final preg-nancy-related prediction model and a final pregnancy and postpar-tum prediction model by performing multiple logistic regressionanalysis. In both prediction models, only variables with P < .05were present. Prediction models were first created for each clusterof potential predictor variables (for example, all variables withP < .20 of the psycho-social cluster) and finally for predictor vari-ables of all clusters together.
To evaluate the predictive performance of the models calibra-tion and discrimination was studied. Calibration of the modelswas assessed by plotting the predicted probabilities of poor out-come of PGP against the observed frequencies. For this, womenwere grouped into deciles according to their predicted probability.The prevalence of the outcome measure within each decile equalsthe observed frequency. Discrimination was studied by calculatingthe area under the ROC-curve, which illustrates the ability of themodels to discriminate between women with and women withoutPGP at subsequent cut-off points along the range of the predictedprobabilities. An area under the curve (AUC) of 0.5 indicates no dis-crimination above chance, whereas an AUC of 1.0 indicates perfectdiscrimination. All analysis were performed in SPSS 14.0.
3. Results
3.1. Study population
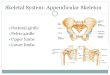
A total of 1219 female employees responded after invitation bytheir company. About half of the women declined to participate(n = 573), and after screening the inclusion and exclusion criteria,a total of 598 women participated in the Mom@Work cohort study.In all, 548 women, who completed the questions about PGP at all 3measurement moments (T1, T2 and T3), were included in the dataanalysis. The flowchart of the cohort is presented in Fig. 1.
Table 1 shows the baseline characteristics of the Mom@Workpopulation for the total population and women with and without
PGP at 12 weeks postpartum. The mean age was 32 years (SD4.0), the majority of the women had a high education and the meanworking hours per week was 29 hours (SD 8.4). Half of the womenwere pregnant with their first child.
The prevalence of PGP was 73% at 30 weeks pregnancy, 48% be-tween 0 and 6 weeks postpartum and 43% between 6 and 12 weekspostpartum. About 62 (25%) of the 234 women who had PGP at12 weeks postpartum had no PGP between 0 and 6 weeks afterdelivery. Although, more women had a mean pain score of 6 orhigher during pregnancy than during the postpartum period (Ta-ble 2), the median pain intensity remained stable throughout allmeasurement moments: 4.3 at 30 weeks pregnancy and 6 weekspostpartum, and 4.5 at 12 weeks postpartum.
3.2. Predictive factors
Table 3 presents the significant pregnancy variables in the uni-variate logistic regression analysis and the multiple cluster logisticregression analysis for the pregnancy prediction model and thepregnancy–postpartum prediction model. Variables that had noassociation with PGP in the univariate logistic regression analysis(P > .20) are not presented.
Table 4 shows the results of the 2 final models. In the pregnancymodel, from the variables measured at 30 weeks pregnancy, his-tory of low back pain in the past (including pregnancy-relatedand postpartum PGP), higher somatisation, more than 8 hours ofsleep or rest a day and uncomfortable postures at work were pre-dictors for PGP at 12 weeks postpartum.
In the final model including both pregnancy and postpartumvariables, the following factors were predictors for PGP at 12 weekspostpartum: more disability at 6 weeks postpartum, higher meanpain at 6 weeks postpartum, having PGP at 6 weeks postpartum,higher birth weight of the baby, higher somatisation during preg-nancy and at 6 weeks postpartum, and uncomfortable postures atwork. Also, number of days with complete bed rest was a predictivefactor. One to 2 days, and especially 3 to 4 days of bed rest decreasedthe risk of PGP compared to no days of bed rest after delivery.
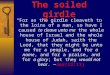
Fig. 2 shows the calibration of the 2 overall prediction models.The predicted and observed probabilities for both prediction mod-els were close to the 45� line, demonstrating good calibration ofthe prediction by both models. The areas under the curve (AUC)for the pregnancy prediction model and pregnancy–postpartumprediction model were 0.73 (CI 0.68–0.77) and 0.84 (CI 0.80–0.87), respectively.
4. Discussion
In this article, we describe the results of a cohort study on pre-dictive factors for PGP at 12 weeks postpartum among workingwomen. About 43% of the women experienced any pain in theirpelvic girdle after delivery. The pain was relatively mild at12 weeks postpartum, and 15% of the women had a mean painscore of 6 or higher. Several predictors for PGP at 12 weeks post-partum were found, some of them were already known to be re-lated to PGP, such as history of low back pain in the past,uncomfortable postures at work, and more disability [52]. How-ever, more somatisation, more hours of sleep or rest, and no daysof bed rest after delivery were also found to be related to an in-creased risk of PGP, and those are new findings.
Two previous Dutch studies reported high rates of sick leavecaused by postpartum PGP [6,40]. The initial intention of the pres-ent study was, therefore, to examine which factors during preg-nancy and postpartum period predicted sick leave due to PGP at12 weeks postpartum among working women. However, only 4women of the whole cohort claimed to be on sick leave after

Invited for participation (n=1800-2500)
Responded to invitation (n=1219)
Entered cohort (n=598)
Excluded (n=621) • Refused to participate (n=573) • Did not meet inclusion criteria (n=25 ) • Response too late (n=23) EN
RO
LLM
ENT
FOLL
OW
-UP T0 n=598
T1 30 weeks pr n=580 complete data n=598 n=12 loss to follow-up
n=6 missing Reasons for loss to follow-up: - problems with questionnaire (n=3) - early delivery (n=3) - no reason mentioned (n=3) - other reason (n=3)
T2 6 weeks pp n=574 complete data n=586 n=9 loss to follow-up n=3 missing
Reasons for loss to follow-up: - problems with questionnaire (n=3) - child had problems (n=2) - child died (n=1) - early delivery (n=2) - no reason mentioned (n=1)
T3 12 weeks pp n=563 complete data n=577 n=7 loss to follow-up n=7 missing
Reasons for loss to follow-up: - problems with questionnaire (n=1) - child had problems (n=1) - no time (n=2) - no reason mentioned (n=2) - other reason (n=1)
Fig. 1. Flow chart of the Mom@Work cohort.
S.G.M. Stomp-van den Berg et al. / PAIN�
153 (2012) 2370–2379 2373
maternity leave, which is 10–12 weeks after delivery in The Neth-erlands, due to problems with their back or pelvis. Further exami-nation showed a low level of disability: a mean score of 4.9 on amaximum of 17. Therefore, it was not possible to study factors pre-dicting sick leave due to PGP. Internationally, postpartum sickleave due to PGP has not often been described as a problem, prob-ably because of the differences in the length of maternity leave andparental leave postpartum in the different countries. In this study,many women increased the length of their leave by taking addi-tional vacation and/or parental leave, although it might have beenpossible that they did have serious PGP.
In accordance with previous studies [28,38], the univariateanalysis in this study confirmed that higher pain and more disabil-ity at 30 weeks pregnancy and at 6 weeks postpartum are predic-tors for PGP at 12 weeks postpartum. It seems that having PGP6 weeks earlier with a higher pain and more disability is an impor-tant predictor for PGP 12 weeks postpartum. In the pregnancymodel, previous low back pain (including previous PGP) was astrong predictive factor for PGP postpartum, which is comparableto the findings of other studies [1,3,25,52]. It should be noted, how-ever, that about 25% of the women with PGP at 12 weeks postpar-tum did not have pain at 6 weeks postpartum. Perhaps their painwas not pregnancy related, but ‘normal’ back or pelvic pain.
In the present study, higher somatisation during pregnancy andat 6 weeks postpartum predicts PGP at 12 weeks postpartum.Somatisation is a condition in which people feel unexplained so-matic symptoms, such as headache, stomach-ache, heart beating,shortness of breath, nausea, etc. When these somatic symptomsare mild and do not occur frequently, they represent a ‘normal’bodily stress reaction. However, many and disruptive symptomsrepresent psychiatric illness [9,21]. Somatisation is also a predictorfor chronic low back pain [34] and irritable bowel syndrome [18],but has not been previously reported as a predictor of PGP. Oneexplanation might be that women who have PGP probably havea higher awareness of their bodily sensations [8]. Alternatively,women who have mental problems might somatise and reportPGP as a result.
All the variables related to sleep, rest, and fatigue were relatedto PGP in the univariate analyses, and only 9 hours or more sleep/rest a day was a predictor in the pregnancy model. It can be rea-soned that women who are fatigued will sleep and rest more perday, making this variable an easily assessed proxy for fatigue dur-ing pregnancy.
Surprisingly, bed rest after delivery was related to PGP. Three to4 days of bed rest decreased the risk of PGP at 12 weeks postpar-tum. Also, 1 to 2 days of bed rest was better than no days of bed

Table 1Baseline characteristics of the Mom@Work population.
Variable Totalpopulation
Womenwithout PGP
Womenwith PGP
n % n % n %
Maternal age (y)<2626–35>35
27418103
(4.9)(76.3)(18.8)
1624157
(5.1)(76.8)(18.2)
1117746
(4.7)(75.6)(19.7)
Parity123P4
2681747630
(48.9)(31.8)(13.9)(5.4)
151994618
(48.1)(31.5)(14.6(5.7)
117753012
(50.0)(32.1)(12.8)(5.1)
Marital statusMarriedLiving togetherAlone/divorced
36217115
(66.1)(31.2)(2.7)
1991078
(63.4)(34.1)(2.5)
163647
(69.7)(27.4)(3.0)
Highest education levelLowMediumHigh
46181320
(8.4)(33.1)(58.5)
23102189
(7.3)(32.5)(60.2)
2379131
(9.8)(33.8)(56.0)
Working hours per week12–19 hours20–35 hoursP36 hours
85303160
(15.5)(55.3)(29.2)
4417397
(14.0(55.1)(30.9)
4113063
(17.5)(55.6)(26.9)
Work sectorHealth careDay careSupermarketElse
361759121
(65.9)(13.7)(16.6)(3.8)
206445014
(65.6)(14.0)(15.9)(4.5)
15531417
(66.2)(13.2)(17.5)(3.0)
Type of workMainly sittingStanding or standing/sittingPhysical active or heavy work
183137228
(33.4)(25.0)(41.6)
11481119
(36.3)(25.8)(37.9)
6956109
(29.5)(23.9)(46.6)
BMI<18.518.5–2525–30>30
2036212936
(3.7)(66.2)(23.6)(6.6)
142166816
(4.5)(68.8)(21.7)(5.1)
61466120
(2.6)(62.4)(26.1)(8.5)
BMI = body mass index (body weight/height2).
2374 S.G.M. Stomp-van den Berg et al. / PAIN�
153 (2012) 2370–2379
rest. This is, to our knowledge, the first study that reports this re-sult. One small Dutch study found that early mobilisation, meaningwalking within 3 hours after the delivery, seemed to protectagainst PGP 6 weeks postpartum [23]. These results cannot becompared with our study findings, as mobilisation at such an earlytime after delivery was not assessed. There is no clear explanationwhy 3 to 4 days of bed rest would reduce PGP. It could be that wo-men who already have serious health problems stay in bed formore than 3 to 4 days, or that 3 to 4 days is the optimum rest per-iod for the body to recover from delivery. Women who take a shortperiod of bed rest (shorter then 3 days), might recover slower thenwomen who take a period of bed rest for 3 to 4 days. This findingneeds further examination.
In a review, weak evidence was found for heavier foetal weightas a risk factor for pregnancy-related PGP, but no evidence was
Table 2Pain variables.
Variable 30 Weeks pregnancy
n %
PGP 386 73.0Median pain, including 0 2.8Median pain, excluding 0 4.3Pain P 6 155 28.3
PGP = pelvic girdle pain.
found for postpartum PGP [52]. However, in our study we foundthat the odds for PGP is 1.001 higher for each gram increase inbirth weight. A higher birth weight might mean a higher mechan-ical pressure in the pelvic region during pregnancy and delivery,resulting in more PGP.
Even though many work-related variables were univariate re-lated to PGP, the only work-related predictor for postpartum PGPin the 2 models was uncomfortable postures during pregnancy,which may be part of strenuous work. Strenuous work was foundby many studies as a risk factor [17,26,52] and uncomfortable pos-tures by 1 study [15].
The strength of the Mom@Work study is that it is a prospectivecohort study with a relatively large sample of working women inwhich a wide variety of variables have been measured, with a focuson work-related factors. Women were recruited from a variety ofcompanies, resulting in a wide range of jobs and working condi-tions. Another strength is that variables measured during preg-nancy and at 6 weeks after delivery are used together in 1analysis to predict postpartum PGP.
One of the weaknesses of the study is that it is not representa-tive for the general Dutch female employees, who are in theirreproductive phase. The women of this study were mainly workingin health care, children’s day care, and supermarkets, had a higheducation and worked more hours per week than the average fe-male worker in the Netherlands [36]. About one-fourth to one-third of the eligible women participated in the study. Therefore,it is possible that a selective population participated in the study.As mentioned earlier, due to different definitions, comparison ofthe prevalence of PGP between studies is difficult. In the reviewby Wu, a wide range in prevalence of PGP was found, ranging from0.3% to 67%, with an average of 25%. Our rates of PGP were compa-rable to the prevalence of PGP in recent studies in the Netherlands[3], Sweden [25], and Australia [45].
Another limitation of this study was that a broad definition ofPGP was used that was not confirmed by physical examination.As discussed earlier, it is not easy to define the complaints womenfeel in their back and pelvis during pregnancy and the postpartumperiod. This makes it difficult to compare the results with otherstudies. Furthermore, some previously reported predictors of PGPrequiring clinical examination [14,38] were not included in ourstudy, and could therefore not be confirmed.
The results of this study may be a starting point for developinginterventions to prevent PGP postpartum. Most efforts should beaimed at preventing PGP during pregnancy becoming a serioushealth problem during late pregnancy and postpartum. Duringpregnancy, health care providers, and employers should pay atten-tion to women who experience PGP and who had back and/or pel-vic pain complaints in the past, who perform strenuous work orhave jobs with uncomfortable postures, who have many or severesomatic symptoms, who are (severely) fatigued, and sleep or restmore than 8 hours per day. Those women may benefit from ergo-nomic adjustments or working shorter dayshifts. According to aCochrane review [33], promising interventions for PGP duringpregnancy are water gymnastics and acupuncture. After delivery,
6 Weeks postpartum 12 Weeks postpartum
n % n %
257 47.6 234 42.71.8 04.3 4.591 16.6 80 14.6

Table 3Univariate and multiple cluster associations with Pelvic girdle pain (PGP) at 12 weeks postpartum for the two prediction models.
Univariate, P < .20 Multiple cluster, P < .05 pregnancy prediction model Multiple cluster p < 0.05 Pregnancy and postpartum prediction model
n % OR 95% CI P OR 95% CI P OR 95% CI P
PGP factors30 Weeks of pregnancy
History of back/pelvic pain, yes (no*) 142 26.8% 2.75 (1.85–4.09) .00 2.14 (1.41–3.24) <.01 1.65 (1.03–2.64) .04History pregnancy-related back/pelvic pain, yes (no*) 40 7.5% 3.96 (1.93–8.10) .00PGP at 30 weeks of pregnancy, yes (no*) 386 73.0% 2.17 (1.44–3.27) .00Disability (RDQ, 0–24); mean (SD) 6.2 (5.9) 1.09 (1.06–1.13) .00 1.08 (1.04–1.11) <.01Pain (0–10); mean (SD) 3.7 (2.5) 1.18 (1.10–1.27) .00
6 Weeks postpartumPGP at 6 weeks postpartum, yes (no*) 215 39.8% 7.73 (5.24–11.41) .00 2.43 (1.42–4.15) <.01Disability (RDQ, 0–24); mean (SD) 1.5 (3.4) 1.61 (1.42–1.82) .00 1.23 (1.09–1.39) <.01Pain (0–10); mean (SD) 2.1 (2.7) 1.36 (1.36–1.59) .00 1.19 (1.08–1.32) <.01
Psychosocial factors30 Weeks of pregnancy
Life events, yes (no*) 156 29.4% 1.44 (0.99–2.12) .06Passive reaction approach (UCL, 7–28) P11 (<11*) 300 58.3% 1.53 (1.07–2.19) .02Number of daily stressors (EPCL, 0–48) P10 (<10*) 298 56.1% 1.40 (0.99–1.99) .06Role limitations-physical (SF-36, 0–100); P50 (<50*) 281 52.9% 0.57 (0.40–0.81) .00Role limitations-emotional (SF-36, 0–100); 100 (0*) 449 94.1% 0.52 (0.24–1.13) .10Social functioning (SF-36, 0–100); mean (SD) 74.5 (19.8) 0.98 (0.97–0.99) .00 0.99 (0.98–1.00) .03Health (SF-36, 0–100); mean (SD) 77.3 (14.5) 0.98 (0.97–0.99) .00Distress (4DSQ, 0–32); mean (SD) 7.4 (5.5) 1.08 (1.04–1.11) .00Somatisation (4DSQ, 0–32); mean (SD) 7.2 (4.7) 1.15 (1.10–1.20) .00 1.16 (1.10–1.22) <.01 1.10 (1.05–1.16) <.01Depression (EPDS, 0–30); mean (SD) 5.6 (4.0) 1.04 (1.00–1.09) .07 0.94 (0.88–1.00) .04
6 Weeks postpartumSocial support spouse (SSL, 1–5); mean (SD) 3.9 (0.7) 0.74 (0.57–0.96) .02Health (SF-36, 0–100); mean (SD) 79.5 (14.9) 0.98 (0.97–0.99) .00Distress (4DSQ, 0–32); mean (SD) 5.2 (5.1) 1.06 (1.02–1.09) .00Fear (4DSQ, 0–24); mean (SD) 0.6 (1.5) 1.12 (0.99–1.26) .07Somatisation (4DSQ, 0–32); mean (SD) 4.7 (3.9) 1.22 (1.16–1.29) .00 1.17 (1.09-1.25) <.01
Fatigue factors30 Weeks of pregnancy
Self-reported fatigueLittle fatigue*
Mild fatigueSevere fatigue
161189172
30.8%36.2%33.0%
1.001.402.89
(0.90–2.17)(1.47–3.57)
.00
.13
.00Sleep /rest per day (1–24 hours) P9 (<9*) 321 60.3% 1.84 (1.29–2.64) .00 1.71 (1.17–2.50) .01 1.67 (1.13–2.47) .01Satisfaction about sleepEnough sleep*
I would like to sleep lessI would like to sleep more
20482242
38.6%15.5%45.8%
1.001.641.39
(0.98–2.75)(0.95–2.03)
.11
.06
.09Fatigue (CIS, 0–140); P76 (<76*) 243 47.1% 2.19 (1.53–3.13) <.01 2.00 (1.39–2.89) <.01 2.11 (1.45–3.09) <.01
6 Weeks postpartumSelf-reported fatigue
Little fatigue*
Mild fatigueSevere fatigue
192162183
38.8%30.2%34.1%
1.001.321.97
(0.86–2.03)(1.30–2.98)
.01
.21<.01
Satisfaction about sleepEnough sleep*
I would like to sleep lessI would like to sleep more
11016410
20.5%3.0%76.5%
1.002.341.50
(0.81–6.77)(0.97–2.32)
.11
.12
.70
(continued on next page)
S.G.M
.Stomp-van
denBerg
etal./PA
IN�
153(2012)
2370–2379
2375

Table 3 (continued)
Univariate, P < .20 Multiple cluster, P < .05 pregnancy prediction model Multiple cluster p < 0.05 Pregnancy and postpartum prediction model
n % OR 95% CI P OR 95% CI P OR 95% CI P
Fatigue (CIS, 0–140); P76 (<76*) 184 36.0% 1.56 (1.08–2.24) .02
Pregnancy and delivery factors30 Weeks of pregnancy
Prepregnancy BMINormal weight*
UnderweightOverweightObese
3622012936
66.2%3.7%23.6%6.6%
1.000.631.331.85
(0.24–1.69)(0.89–1.99)(0.93–3.69)
.13
.36
.17
.08Miscarriages in past, yes (no*) 52 9.7% 0.67 (0.37–1.23) .20Place of giving birth; hospital (home*) 370 67.6% 1.30 (0.91–1.89) .15Delivery >18 hours, yes (no*) 49 10.4% 1.76 (0.97–3.19) .06Delivery with pressure, yes (no*) 44 8.0% 1.67 (0.90–3.11) .10Extra-stimulated delivery, yes (no*) 97 17.7% 1.70 (1.10–2.65) .02Bed rest after delivery
0 days*
1–2 days3–4 daysP5 days
2629089102
48.3%16.6%16.4%18.8%
1.000.690.581.53
(0.42–1.14)(0.35–0.96)(0.97–2.43)
.01
.15
.04
.07
1.000.580.431.78
(0.32–1.05)(0.24–0.77)(1.04–3.03)
<.01.07<.01.04
Weight of baby (per gram); mean (SD) 3531 (571) 1.00 (1.00–1.00) <.01 1.00 (1.00–1.00) <.01
Work factors30 Weeks of pregnancy
Type of workMainly sitting*
Standing or standing/sittingPhysically active or heavy work
183137228
33.4%25.0%41.6%
1.001.141.51
(0.73–1.80)(1.02–2.25)
.11
.57
.04Job insecurity (JCQ, 3–10) >4 (64*) 95 17.7% 1.65 (1.06–2.58) .03Co-worker support (JCQ, 4–16); P12 (<12*) 481 89.1% 0.59 (0.34–1.01) .05Uncomfortable posture(JCQ, 2–8); mean (SD) 3.91 (1.05) 1.42 (1.19–1.69) .00 1.42 (1.17–1.713) <0.01Physical exertion (JCQ, 3–12); mean (SD) 6.64 (2.07) 1.10 (1.01–1.20) .02Consulted physician, yes (no*) 42 7.7% 0.65 (0.33–1.26) .20Sick leave due to back/pelvic problems, yes (no*) 77 14.6% 2.28 (1.39–3.73) .00 2.21 (1.26–3.87) 0.01Irregular work with weekend shifts, yes (no*) 153 28.1% 1.29 (0.89–1.88) .19Adjusted job, yes (no*) 246 46.5% 1.72 (1.21–2.44) .00Income <30.000 Euros per year, yes (no*) 103 20.9% 1.71 (1.10–2.64) .02
OR = odds ratio, CI = confidence interval; 30wP = 30 weeks of pregnancy; 6wPP = 6 weeks postpartum; RDQ = Roland-Morris Disability Questionnaire; 4DSQ = Four Dimensional Symptom Questionnaire; EPCL = Everyday ProblemsChecklist; UCL = Utrecht Coping List; EPDS = Edinburgh Postnatal Depression Scale; CIS = Checklist Individual Strength; BMI = body mass index, SF-36 = 36-Item Short Form Health Survey; JCQ = Job Content Questionnaire.* Reference category.
2376S.G
.M.Stom
p-vanden
Berget
al./PAIN
�153
(2012)2370–
2379

Table 4Overall prediction models for pregnancy-related factors only and for pregnancy- and postpartum-related factors combined.
Overall pregnancy prediction model Women without PGP Women with PGP OR 95% CI P
30 Weeks of pregnancyHistory of back/pelvic pain (%)
YesNo
18%82%
38%62%
2.391
(1.54–3.72) <.01
Somatisation (4DSQ, 0–32), mean (SD) 6.0 (4.0) 8.8 (5.1) 1.12 (1.07–1.18) <.01
Hours of sleep/rest a day (%)P9<9
46%54%
31%69%
1.711
(1.14–2.56) .01
Uncomfortable posture (JCQ, 2–8); mean (SD) 3.8 (1.0) 4.1 (1.1) 1.35 (1.11–1.64) <.01
Overall pregnancy and postpartum prediction model
30 Weeks of pregnancyDisability (RDQ, 0–24); mean (SD) 0.3 (1.7) 3.2 (4.2) 1.19 (1.05–1.35) .01Pain (0–10); mean (SD) 1.1 (2.0) 3.5 (2.8) 1.16 (1.04–1.31) .01Somatisation (4DSQ, 0–,32); mean (SD) 6.0 (4.0) 8.8 (5.1) 1.07 (1.01–1.13) .02Uncomfortable posture (JCQ, 2–8); mean (SD) 3.8 (1.0) 4.1 (1.1) 1.31 (1.04–1.65) .02
6 Weeks postpartumPGP at 6 weeks postpartum (%)
YesNo*
20%80%
66%34%
2.561
(1.42–4.61) <.01
Bed rest after delivery (%)0 days*
1–2 days3–4 days
47%19%20%
50%14%12%
10.510.25
(0.26–0.99)(0.13–0.52)
<.01.05<.010
Overall pregnancy prediction modelP5 days 15% 24% 0.78 (0.42–1.40) .38Weight of baby (grams); mean (SD) 3441 (557) 3649 (569) 1.001 (1.00–1.00) .01Somatisation (4DSQ, 0–32); mean (SD) 3.5 (3.1) 6.2 (4.3) 1.08 (1.00–1.16) .04
OR = odds ratio; CI = confidence interval, RDQ = Roland-Morris Disability Questionnaire; 4DSQ = Four Dimensional Symptom Questionnaire; EPDS = Edinburgh PostnatalDepression Scale; CIS = Checklist Individual Strength; SF-36 = 36-Item Short Form Health Survey; JCQ = Job Content Questionnaire.* Reference category.
pregnancy
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
observed probability
pred
icte
d pr
obab
ility
postpartum
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
observed probability
pred
icte
d pr
obab
ility
A B
Fig. 2. The calibration of the two overall prediction models. Observed versus expected plot for (A) the pregnancy prediction model, and (B) the pregnancy–postpartumprediction model.
S.G.M. Stomp-van den Berg et al. / PAIN�
153 (2012) 2370–2379 2377
PGP at 6 weeks postpartum with higher pain and more disability,and many or severe somatic symptoms may be markers for healthcare providers and employers to reduce the work load or changework time when those women return to work.
4.1. Conclusions
Several predictors for PGP at 12 weeks postpartum were found.Almost half of the women experienced any pain in their pelvic gir-dle after delivery. However, the level of pain and the degree of dis-
ability were low, and there was hardly any postpartum sick leavedue to PGP. More attention should be given to women who expe-rience PGP during pregnancy so as to prevent serious PGP duringlate pregnancy and postpartum. More research is needed to con-firm the role of sleep, and somatisation during pregnancy andbed rest after delivery in relation to PGP.
Conflict of interest statement
None of the authors has declared a conflict of interest.

2378 S.G.M. Stomp-van den Berg et al. / PAIN�
153 (2012) 2370–2379
Acknowledgements
We thank the participants and companies who joined the study,as well as the research assistants Marije Olsthoorn-Ooms, MSc;Karin Johnson; Giel Pool, MD; Monique Heemskerk, MSc and Lydater Hofstede, PT, and data entry assistants for their contribution tothe study. We thank also Ingrid Riphagen for researching the liter-ature. The study is funded by Body@Work, Research Centre Physi-cal Activity, Work and Health, TNO-VUmc, Van der Boechorststraat7, 1081 BT Amsterdam, The Netherlands, and is performed at theEMGO Institute, The Netherlands.
References
[1] Albert HB, Godskesen M, Korsholm L, Westergaard JG. Risk factors indeveloping pregnancy-related pelvic girdle pain. Acta Obstet Gynecol Scand2006;85:539–44.
[2] Ansara D, Cohen MM, Gallop R, Kung R, Schei B. Predictors of women’s physicalhealth problems after childbirth. J Psychosom Obstet Gynecol2005;26:115–25.
[3] Bastiaanssen JM, de Bie RA, Bastiaenen CH, Heuts A, Kroese ME, Essed GG, vanden Brandt PA. Etiology and prognosis of pregnancy-related pelvic girdle pain;design of a longitudinal study. BMC Public Health 2005;5:1. http://dx.doi.org/10.1186/1471-2458-5-1.
[4] Bastiaanssen JM, de Bie RA, Bastiaenen CHG, Essed GGM, van den Brandt PA. Ahistorical perspective on pregnancy-related low back and/or pelvic girdle pain.Eur J Obstet Gynecol Reprod Biol 2005;120:3–14.
[5] Beckers I. Nine out of ten women keep working after childbirth [In Dutch:Negen van de 10 vrouwen blijven werken na geboorte kind]. Available at:<http://www.cbs.nl/nl-NL/menu/themas/dossiers/vrouwen-en-mannen/publicaties/artikelen/archief/2004/2004-1605-wm.htm>; 2004. (accessed05.09.12).
[6] van Beukering MDM. Work during pregnancy and postpartum period:Research on sick leave [In Dutch: Werken tijdens zwangerschap en periodepost-partum: onderzoek naar ziekteverzuim]. TBV 2002;10:2–7.
[7] Brynhildsen J, Hansson A, Persson A, Hammar M. Follow-up of patients withlow back pain during pregnancy. Obstet Gynecol 1998;91:182–6.
[8] Burton C. Beyond somatisation: a review of the understanding and treatmentof medically unexplained physical symptoms (MUPS). Br J Gen Pract2003;53:231–9.
[9] Clarke DM, Smith GC. Somatisation. What is it? Aust Fam Physician2000;29:109–13.
[10] Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression.Development of the 10-item Edinburgh Postnatal Depression Scale. Br JPsychiatry 1987;150:782–6.
[11] Daalen G, Sanders K, Willemson TM. Sources of social support as predictors ofhealth, psychological well-being and life satisfaction among Dutch male andfemale dual-earners. Women Health 2005;41:43–62.
[12] Gommans IHB, Koes BW, van Tulder MW. Validity and responsiveness of theDutch Roland Disability Questionnaire [In Dutch: Validiteit en responsiviteitNederlandstalige Roland Disability Questionnaire]. Nederlands Tijdschrift voorFysiotherapie 1997;107:28–33.
[13] Gutke A, Lundberg M, Ostgaard HC, Oberg B. Impact of postpartumlumbopelvic pain on disability, pain intensity, health-related quality of life,activity level, kinesiophobia, and depressive symptoms. Eur Spine J2011;20:440–8.
[14] Gutke A, Ostgaard HC, Oberg B. Predicting persistent pregnancy-related lowback pain. Spine [Phila Pa 1976] 2008;33:386–93.
[15] Heiberg Endresen E. Pelvic pain and low back pain in pregnant women – anepidemiological study. Scand J Rheumatol 1995;24:135–41.
[16] Huizink AC, Robles de Medina PG, Mulder EJH, Visser GHA, Buitelaar JK. Copingin normal pregnancy. Ann Behav Med 2002;24:132–40.
[17] Juhl M, Andersen PK, Olsen J, Andersen AMN. Psychosocial and physical workenvironment and risk of pelvic pain in pregnancy. A study within the Danishnational birth cohort. J Epidemiol Community Health 2005;59:580–5.
[18] Jung HK, Halder S, McNally M, Locke III GR, Schleck CD, Zinsmeister AR, TalleyNJ. Overlap of gastro-oesophageal reflux disease and irritable bowelsyndrome: prevalence and risk factors in the general population. AlimentPharmacol Ther 2007;26:453–61.
[19] Kanakaris NK, Roberts CS, Giannoudis PV. Pregnancy-related pelvic girdlepain: an update. BMC Med 2011;9:15. http://dx.doi.org/10.1186/1741-7015-9-15.
[20] Karasek R, Brisson C, Kawakami N, Houtman ILD, Bongers PM, Amick B. The JobContent Questionnaire (JCQ): an instrument for internationally comparativeassessments in psychosocial job characteristics. J Occup Health Psychol1998;3:322–55.
[21] Katon W, Lin E, Von KM, Russo J, Lipscomb P, Bush T. Somatization: a spectrumof severity. Am J Psychiatry 1991;148:34–40.
[22] Larsen EC, Wilken-Jensen C, Hansen A, Jensen DV, Johansen S, Minck H,Wormslev M, Davidsen M, Hansen TM. Symptom-giving pelvic girdle
relaxation in pregnancy. I. Prevalence and risk factors. Acta Obstet GynecolScand 1999;78:105–10.
[23] Lemstra-Luckerhof GF, Kuyvenhoven MM, Chavannes AW. Early mobilisationafter delivery and pelvic pain 6 weeks postpartum. Huisarts Wet2001;44:287–9.
[24] Mogren IM. BMI, pain and hyper-mobility are determinants of long-termoutcome for women with low back pain and pelvic pain during pregnancy. EurSpine J 2006;15:1093–102.
[25] Mogren IM, Pohjanen AI. Low back pain and pelvic pain during pregnancy:prevalence and risk factors. Spine 2005;30:983–91.
[26] Ostgaard HC, Andersson GB. Postpartum low-back pain. Spine 1992;17:53–5.[27] Ostgaard HC, Andersson GB, Karlsson K. Prevalence of back pain in pregnancy.
Spine 1991;16:549–52.[28] Ostgaard HC, Roos-Hansson E, Zetherstrom G. Regression of back and posterior
pelvic pain after pregnancy. Spine 1996;21:2777–80.[29] Ostgaard HC, Zetherstrom G, Roos-Hansson E. Back pain in relation to
pregnancy: a 6-year follow-up. Spine 1997;22:2945–50.[30] Overturf Johnson J, Downs B. Maternity leave and employment patterns:
1961–2000. Current population report, vol. 14. Washington, DC: US CensusBureau; 2003. p. 70–103.
[31] Paarlberg KM, Vingerhoets AJJM, Passchier J, Heinen AGJJ, Dekker GA,van Geijn HP. Psychosocial factors as predictors of maternal well-beingand pregnancy-related complaints. J Psychosom Obstet Gynaecol1996;17:93–102.
[32] Parasuraman S, Greenhause J, Skromme Granrose C. Role Stressors socialsupport and well-being among two-career couples. J Organ Behav1992;13:339–56.
[33] Pennick VE, Young G. Interventions for preventing and treating pelvic and backpain in pregnancy. Cochrane Database Syst Rev 2007:CD001139. http://dx.doi.org/10.1002/14651858.CD001139.pub2.
[34] Pincus T, Burton AK, Vogel S, Field AP. A systematic review of psychologicalfactors as predictors of chronicity/disability in prospective cohorts of low backpain. Spine 2002;27:E109–20.
[35] Pop VJ, Komproe IH, Son MJv. Characteristics of the Edinburgh postnataldepression scale in the Netherlands. Br J Psychiatry 1992;26:105–10.
[36] Portegijs W, Hermans B, Lalta V. Emancipatiemonitor, vol. SCP-publicatie, ISSN1568–1262; 2006/22. Den Haag: Sociaal en Cultureel Planbureau [Voorburgetc.]: Centraal Bureau voor de Statistiek; 2006.
[37] Riddle DL, Stratford PW. Roland-Morris scale reliability. Physiotherapy2002;82:512–5.
[38] Robinson HS, Mengshoel AM, Veierod MB, Vollestad N. Pelvic girdle pain:potential risk factors in pregnancy in relation to disability and pain intensitythree months postpartum. Man Ther 2010;15:522–8.
[39] Roland M, Morris R. A study of the natural history of back pain. Part I.Development of a reliable and sensitive measure of disability in low back pain.Spine 1983;8:141–4.
[40] Rost C, Jacqueline J, Kaiser A, Verhagen A, Koes B. Prognosis of women withpelvic pain during pregnancy: a long-term follow-up study. Acta ObstetGynecol Scand 2006;85:771–7.
[41] Schreurs PJG, Willige Gvd, Brosschot JF, Tellegen B, Graus GMH. TheUtrecht Coping List: coping with problems and incidents; revised manual [InDutch: De Utrechtse Coping Lijst: UCL. Omgaan met problemen engebeurtenissen; herziene handleiding]. Lisse, The Netherlands: Swets &Zeitlinger; 1993.
[42] Stomp-van den Berg SG, van Poppel MN, Hendriksen IJ, Bruinvels DJ, Uegaki K,de Bruijne MC, van Mechelen W. Improving return-to-work after childbirth:design of the Mom@Work study, a randomised controlled trial and cohortstudy. BMC Public Health 2007;7:43. http://dx.doi.org/10.1186/1471-2458-7-43.
[43] Sydsjo A, Alexanderson K, Dastserri M, Sydsjo G. Gender differences in sickleave related to back pain diagnoses: influence of pregnancy. Spine2003;28:385–9.
[44] Terluin B, van Marwijk HW, Ader HJ, de Vet HC, Penninx BW, Hermens ML, VanBoeijen CA, van Balkom AJ, van der Klink JJ, Stalman WA. The Four-Dimensional Symptom Questionnaire (4DSQ): a validation study of amultidimensional self-report questionnaire to assess distress, depression,anxiety and somatization. BMC Psychiatry 2006;6:34. http://dx.doi.org/10.1186/1471-244X-6-34.
[45] Thompson JF, Roberts CL, Currie M, Ellwood DA. Prevalence and persistence ofhealth problems after childbirth: associations with parity and method of birth.Birth 2002;29:83–94.
[46] Van De Pol G, Van Brummen HJ, Bruinse HW, Heintz APM, Van Der Vaart CH.Pregnancy-related pelvic girdle pain in the Netherlands. Acta Obstet GynecolScand 2007;86:416–22.
[47] Van der Zee KI, Sanderman R, Heyink J. Psychometric characteristics of theMOS 36-item Short Form Health Survey (SF-36) in a Dutch Population [InDutch: De psychometrische kwaliteiten van de MOS 36-item Short FormHealth Survey (SF-36) in een Nederlandse populatie]. Tijdschrift voor SocialeGezondheidszorg 1993;4:183–91.
[48] Vercoulen JHMM, Alberts M, Bleijenberg G. Short tools: the ChecklistIndividual Strength (CIS) [In Dutch: Kort instrumenteel: De checklistindividual strength (CIS)]. Gedragstherapie 1999;32:131–6.
[49] Vercoulen JHMM, Swanink CMA, Fennis JFM, Galama JMD, Meer JWMvd,Bleijenberg G. Dimensional assessment of chronic fatigue syndrome. JPsychosom Res 1994;38:383–92.

S.G.M. Stomp-van den Berg et al. / PAIN�
153 (2012) 2370–2379 2379
[50] Vingerhoets AJJM, Tilburg MAL. Everyday Problems Checklist (EPCL) [In Dutch:Alledaagse Problemen Lijst (APL)]. Lisse, The Netherlands: Swets & Zeitlinger;1994.
[51] Ware JE, Sherbourne CD. The RAND-36 Short-form Health Status Survey: I.Conceptual framework and item selection. Med Care 1992;30:473–81.
[52] Wu WH, Meijer OG, Uegaki K, Mens JMA, Van Dieen JH, Wuisman PIJM,Ostgaard HC. Pregnancy-related pelvic girdle pain (PPP). I: Terminology,clinical presentation, and prevalence. Eur Spine J 2004;13:575–89.