Embed Size (px)
Citation preview

Predictors of Rehospitalization after Total WeightRecovery in Adolescents with Anorexia Nervosa
Josefina Castro,* Araceli Gila, Josefa Puig, Sonia Rodriguez, and Josep Toro
Eating Disorders Unit, Department of Child and Adolescent Psychiatry and Psychology,Institute of Psychiatry and Psychology, Hospital Clinic Universitari of Barcelona,
IDIBAPS, Barcelona, Spain
Accepted 9 May 2003
Abstract: Objective: The current study analyzed the variables related to rehospitalizationafter total weight recovery in adolescents with anorexia nervosa. Method: One hundred andone patients first admitted for inpatient treatment, aged 11–19 years, were followed up for12 months after discharge. Results: Twenty-five subjects (24.8%) required readmission aftercomplete weight recovery and 76 (75.2%) did not. Duration of disorder, weight loss, bodymass index at first admission, and global body image distortion were similar in the twogroups. Patients needing readmission had a lower rate of weight gain (p < .001), a lowermean age (p ¼ .007), a higher mean score on the Eating Attitudes Test (EAT; p ¼ .009), and ahigher percentage of hips overestimation (p ¼ .049). In a stepwise logistic regressionanalysis, these three variables predicted readmission and correctly classified 77.6% ofpatients. Taken as discrete variables, age younger than 15 years old, EAT score above 55,and a rate of weight gain lower than 150 grams per day were associated with a higherpercentage of readmissions. Discussion: The variables most clearly related to readmissionwere young age, abnormal eating attitudes, and a low rate of weight gain. # 2004 by WileyPeriodicals, Inc. Int J Eat Disord 36: 22–30, 2004.
Key words: rehospitalization; anorexia nervosa; adolescents
INTRODUCTION
Anorexia nervosa is a complex disorder that usually needs long-term, intensive treat-ment (Strober, Freeman, & Morrell, 1997; Steinhausen, Seidel, & Winkler Metzke, 2000).Treatment programs differ widely and may be based on inpatient, day hospital, oroutpatient care. In many cases, the resources available are insufficient or the programsare too short (Striegel-Moore, Leslie, Petrill, Garvin, & Rosenheck, 2000). The mean stayof patients admitted to psychiatric wards in general hospitals for treatment of anorexia
*Correspondence to: Josefina Castro, M.D., Ph.D., Department of Child and Adolescent Psychiatry andPsychology, Institute of Psychiatry and Psychology, Hospital Clinic Universitari, Barcelona, Sabino de Arana,1, Barcelona 08028, Spain. E-mail: [email protected]
Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/eat.20009
# 2004 by Wiley Periodicals, Inc.

nervosa is longer compared with hospitalization for other psychiatric disorders (McKenzie& Joyce, 1992). Approximately 15 years ago, the average hospital stay was 140–150days. Currently, the average stay ranges from 24 days to 40 days (Howard, Evans,Quintero-Howard, Bowers, & Andersen, 1999; McKenzie & Joyce, 1992; Nozoe et al.,1995; Wiseman, Sunday, Klapper, Harris, & Harris, 2001). This reflects a general trend inthe duration of inpatient care for adolescent patients with psychiatric disorders (Pottick,McAlpine, & Andelman, 2000). During the adolesecent years, it is important not tointerrupt patients’ normal patterns of adjustment to school, family, and social life forlonger than necessary, but some authors have suggested that the excessive shortening ofstays may increase the rate of readmission (Wickizer, Lessler, & Travis, 1999). In anorexianervosa, weight recovery needs time. For biologic reasons, weight restoration must notbe done too fast and the patient’s psychological resistance to gaining weight should alsobe taken into account. The result of shorter hospital stays is that patients are dischargedbefore they reach minimum normal weight (Wiseman et al., 2001) and before theirpsychological treatment program is complete. Consequently, they continue to receivetreatment as outpatients (Howard et al., 1999; Wiseman et al., 2001).
Very few studies have analyzed the outcome of treatment programs, duration of stay,and readmission rates in adolescents with anorexia nervosa. Most of the data availableare from studies with adult patients. Kahn and Pike (2001) found that the anorexiasubtype and the length of illness were modestly predictive of treatment drop-out inadult patients. Some studies have found a high readmission rate (i.e., 25%–35%) amongadult patients with anorexia nervosa and an even higher rate (i.e., approximately 63%)among adolescent patients (Howard et al., 1999; McKenzie & Joyce, 1992; Wiseman et al.,2001). Shortened hospitalization and low weight at discharge have been reported toincrease the readmission rate (Howard et al., 1999; Wiseman et al., 2001). Other variablesthat have been related to readmission are young age, long duration of the disorder, lowbody mass index (BMI) at admission, and purgative symptomatology (Baran, Weltzin, &Kaye, 1995; Howard et al., 1999; McKenzie & Joyce, 1992; Ostuzzi, Didonna, & Micciolo,1999). Although few studies of large samples have analyzed variables related to read-mission, it seems likely that discharge below normal weight is one. Identifying the othervariables involved is less easy, especially among young adolescents with a relativelyshort duration of the disorder.
If we can determine which variables at first admission are related to repeated read-mission, we will be able to differentiate groups of patients at high risk of relapse and toadapt treatment decisions to their characteristics. Given the importance of total weightrecovery for a good outcome after discharge, the objective of the current study was toanalyze a range of variables at first admission to determine which ones are related toreadmission among adolescent patients after complete weight recovery is achieved.
METHOD
Subjects and Procedure
The group of patients comprised 101 adolescents aged 11–19 years old who met thediagnostic criteria for anorexia nervosa as described in the 4th ed. of the Diagnostic andStatistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994).All patients were first admitted consecutively from January 1999 to December 2000 to theEating Disorders Unit at the Hospital Clinic University of Barcelona. Study procedures
Rehospitalization in Anorexia Nervosa 23

were approved by the ethics committee of the institution. At admission, clinical character-istics were recorded and hormonal data were assessed. All samples were taken in themorning. Abnormal eating attitudes were evaluated with the Spanish version (Castro,Toro, Salamero, & Guimera, 1991) of the Eating Attitudes Test (EAT; Garner & Garfinkel,1979). Body image distortion was evaluated with the Subjective Body Dimensions Appar-atus (SBDA; Gila, Castro, Toro, & Salamero, 1998). The SBDA evaluates patients’ idea oftheir body dimensions. It is a body site estimation procedure that provides a simultaneousrepresentation of several body sites and, thus, gives a global silhouette. After 12 months offollow-up, patients who needed readmission were compared with patients who did notusing clinical and psychological parameters during first admission.
Treatment Program
Treatment is based on outpatient, day hospital, or inpatient care. Inpatient treatment isindicated when physical risk is high, psychopathology is intense, or collaboration in theoutpatient setting is poor. Treatment during admission is based on a multidisciplinaryapproach that combines biologic management, nutritional rehabilitation, a behavioral pro-gram to improve eating patterns and weight, individual and group cognitive treatment, andindividual and group parent counseling. During hospitalization, all patients receive initiallya complete diet of about 1,250 calories per day, which is increased progressively to 2,500calories per day. The minimum weight increase per week required during hospitalization is900 g, which is achieved through a behavioral treatment program. Providing this minimumis reached, patients can decide freely the amount of food intake and whether they wouldprefer a somewhat higher rate of weight gain. Many patients with positive attitudes toadmission and weight recovery have achieved increases of 2–2.5 kg per week. During thetreatment program, patients are allowed one or two admissions to achieve a normal BMI,which is estimated on the basis of normative Spanish data (Hernandez, Sanchez, &Sobradillo, 2000), for their age and sex. After the second discharge, nutritional recovery isalmost complete as patients’ BMI values are within the normal ranges. However, they needlong-term psychological follow-up as outpatients because the psychological improvementduring a short inpatient stay is insufficient. Many patients achieve total weight recovery butdo not maintain weight during outpatient treatment after discharge. Patients who fail tomaintain weight are readmitted within a few weeks. The decision to readmit is made by theclinician in charge of the patient according to a treatment program that is compulsory for allpatients. Even though the readmission rate is high, the goals are to avoid a long period oftime during which subjects are underweight and to prevent the physical sequelae of thedisorder among these young patients (Castro, Lazaro, Pons, Halperin, & Toro, 2001; Montet al., in press). Other criteria for readmission are the onset of binge eating or vomiting and aconflictive family relationship. The majority of these patients require intensive outpatienttreatment. Patients who succeed in maintaining weight and are clinically stable afterdischarge continue to receive cognitive-behavioral treatment as outpatients.
Statistical Analysis
Means of continuous variables in the two groups were compared using Student’s t test.The chi-square or Fisher’s exact test was used to compare percentages of discrete vari-ables. Logistic regression analysis was performed using forward stepwise selection andthe likelihood ratio test to obtain the model that best predicted readmission after totalweight recovery. The level of statistical significance was p < .05. Statistical analysis wasperformed using the SPSS package (Norusis, 1993).
24 Castro et al.

RESULTS
General Characteristics
Ten (9.9%) patients were male. Eighty patients (79.2%) had restrictive-type anorexianervosa and 21 (20.8%) had purging-type anorexia nervosa. Twenty-five (24.8%) patientsreceived psychopharmacologic treatment during admission with selective serotoninreuptake inhibitors. Table 1 shows the general characteristics of patients, hormonaldeterminations, weight recovery, and the results of the EAT and SBDA.
Readmission Rate after Weight Recovery
Twenty-five (24.8%) patients required readmission after total weight recovery, whereas76 (75.2%) did not. Readmission was due to a failure to maintain weight after discharge.Patients who were not readmitted succeeded in maintaining the complete weight recov-ery achieved during admission and were clinically stable after 12 months.
Comparison between Patients who Required Readmission after WeightRecovery and Those who did not
Table 2 shows the percentages of purging-type anorexia nervosa patients, males, andpatients receiving psychopharmacologic treatment who required readmission after totalweight recovery and those who did not. There were no statistically significant differencesbetween patients who were readmitted and those who were not.
A comparison of the various continuous variables studied for readmitted and non-readmitted patients is shown in Table 3. The variables that presented higher statisticallysignificant differences in the two groups were age, rate of weight gain, and abnormaleating attitudes. Hips overestimation also determined significant differences, but to alesser extent.
Table 1. Characteristics of the patients (N ¼ 101)
Characteristics M (SD)
Age at first admission (years) 15 (1.8)Duration of disorder (months) until first admission 14.9 (10.3)Duration of amenorrhea (months)a 8.9 (6.7)Weight loss (%) until first admission 22.3 (6.8)Body mass index at first admission 15.9 (1.3)Total weight increase during first admission (kg) 6.3 (2.4)Rate of weight increase during first admission (g/day) 257.5 (144.8)Days of stay during first admission (days) 31.2 (17.3)
Hormonal determinationsInsulin-like growth factor 273.7 (162)Triiodothyronin (T3) .65 (.5)Estradiol in female patients .21.1 (20.8)Testosterone in male patients 256.9 (242.7)
Eating attitudes and body image perceptionEating Attitudes Test 44.7 (25.6)Global body image overestimation in female patients (%)b 37.4 (19.8)Hips overestimation (%) in female patientsb 52.8 (26.9)
aOnly girls with secondary amenorrhea (N ¼ 76).bKnown for 75 of the 91 patients.
Rehospitalization in Anorexia Nervosa 25

Logistic Regression Analysis for Prediction of Readmission after Total Weight Recovery
The variables that showed statistically significant differences between patients whowere readmitted and patients who were not (age, a rate of weight recovery, and EATscore) were included in the logistic regression analysis using forward stepwise selection.Hips overestimation was not included because it was not known for all patients. Thethree variables entered in the analysis were selected as independent predictors of read-mission (rate of weight recovery: b ¼ �.008, SE ¼ .003, p ¼ .009; age: b ¼ �.360, SE ¼ .149,p ¼ .016; EAT: b ¼ .026, SE ¼ .011, p ¼ .020). With these three variables at first admission,77.6% of the patients were correctly classified as needing readmission after weightrecovery. The �2 log likelihood was 88.1 (�2 ¼ 23.2; p < .001).
Percentage of Readmission in Relation to Significant Variables
To determine the relation between the most significant variables and readmission, weassessed the percentage of readmitted subjects above and below a cutoff point estab-lished for each variable. The better cutoff points were established by analyzing the rate ofweight gain (150 g per day), age (15 years), and an EAT score of 55. Figure 1 shows thepercentages of patients with these characteristics in the two groups. There was a sig-nificantly greater proportion of readmitted patients younger than 15 years old (N ¼ 20[80%]) compared with patients who were not readmitted (N ¼ 37 [48.7%]; �2 ¼ 7.5; df ¼ 1;
Table 2. Differences between patients requiring readmission after weightrecovery (N ¼ 25) and patients who did not (N ¼ 76)
Characteristics No Readmission (%) Readmission (%) pa
Purging type 13 (17.1) 8 (32.9) .154Male patients 9 (11.8) 1 (4) .444Psychopharmacologic treatment 18 (23.7) 7 (28) .791
aFisher’s exact test (two sided).
Table 3. Differences in characteristics during first admission between patients who neededreadmission after weight recovery (N ¼ 25) and patients who did not (N ¼ 76)
No Readmission Readmission
Characteristics M (SD) M (SD) ta p
Age (years) 15.3 (1.8) 14.2 (1.3) 2.8 .007Duration of disorder (months) 15.6 (10.8) 12.8 (8.1) 1.6 .250Duration of amenorrhea (months)b 9.5 (10.8) 7.3 (5.3) 1.7 .210Loss of weight (%) 21.8 (6.8) 23.6 (6.7) �1.1 .272Body mass index at admission 15.8 (1.3) 16.1 (1.2) �.8 .352Total weight gain (kg) 6.4 (2.5) 5.8 (1.9) 1.2 .243Rate of weight gain (g/day) 280.8 (154) 186.4 (76) 4.0 <.001Days of hospitalization 29.7 (17.5) 35.4 (16.2) �1.4 .161
Eating attitudes and body imageEating Attitudes Test 40.8 (25.8) 56.1 (21.5) �2.6 .009Global body image overestimation (%)c 35.6 (20.5) 41.7 (18.0) �1.2 .234Hips overestimation (%) female patientsc 48.9 (25.9) 62.3 (27.3) �2.0 .049
aStudent’s t test, two-tailed.bOnly girls with secondary amenorrhea (N ¼ 76).cKnown for 75 of the 91 female patients.
26 Castro et al.
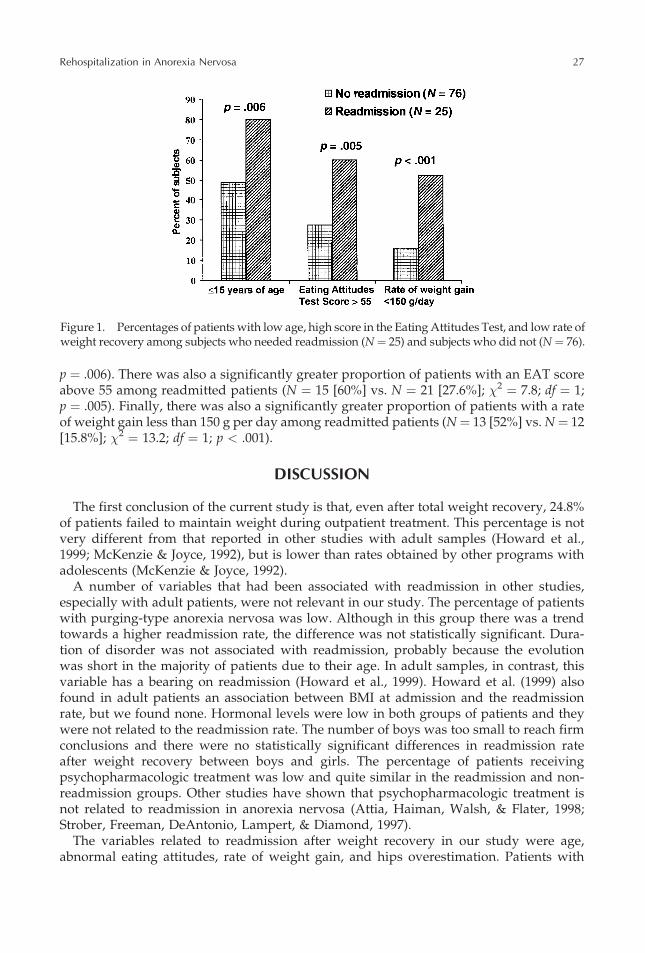
p ¼ .006). There was also a significantly greater proportion of patients with an EAT scoreabove 55 among readmitted patients (N ¼ 15 [60%] vs. N ¼ 21 [27.6%]; �2 ¼ 7.8; df ¼ 1;p ¼ .005). Finally, there was also a significantly greater proportion of patients with a rateof weight gain less than 150 g per day among readmitted patients (N¼ 13 [52%] vs. N¼ 12[15.8%]; �2 ¼ 13.2; df ¼ 1; p < .001).
DISCUSSION
The first conclusion of the current study is that, even after total weight recovery, 24.8%of patients failed to maintain weight during outpatient treatment. This percentage is notvery different from that reported in other studies with adult samples (Howard et al.,1999; McKenzie & Joyce, 1992), but is lower than rates obtained by other programs withadolescents (McKenzie & Joyce, 1992).
A number of variables that had been associated with readmission in other studies,especially with adult patients, were not relevant in our study. The percentage of patientswith purging-type anorexia nervosa was low. Although in this group there was a trendtowards a higher readmission rate, the difference was not statistically significant. Dura-tion of disorder was not associated with readmission, probably because the evolutionwas short in the majority of patients due to their age. In adult samples, in contrast, thisvariable has a bearing on readmission (Howard et al., 1999). Howard et al. (1999) alsofound in adult patients an association between BMI at admission and the readmissionrate, but we found none. Hormonal levels were low in both groups of patients and theywere not related to the readmission rate. The number of boys was too small to reach firmconclusions and there were no statistically significant differences in readmission rateafter weight recovery between boys and girls. The percentage of patients receivingpsychopharmacologic treatment was low and quite similar in the readmission and non-readmission groups. Other studies have shown that psychopharmacologic treatment isnot related to readmission in anorexia nervosa (Attia, Haiman, Walsh, & Flater, 1998;Strober, Freeman, DeAntonio, Lampert, & Diamond, 1997).
The variables related to readmission after weight recovery in our study were age,abnormal eating attitudes, rate of weight gain, and hips overestimation. Patients with
Figure 1. Percentages of patients with low age, high score in the Eating Attitudes Test, and low rate ofweight recovery among subjects who needed readmission (N¼ 25) and subjects who did not (N¼ 76).
Rehospitalization in Anorexia Nervosa 27

younger age, especially patients younger than 15 years old, had a higher readmissionrate, in agreement with one other study in adolescents (McKenzie & Joyce, 1992). It canbe speculated that cognitive therapy is less likely to succeed in very young patients andthat they will need more time and greater treatment resources. Follow-up studies withadolescent patients obtain higher recovery rates in the long run than studies with adultpopulations (Strober, Freeman, & Morrell, 1997), but this is probably because the treat-ment programs are intensive and long term, especially in younger subjects. The othervariables that are associated with the readmission rate are the degrees of severity of thepsychological factors of the disorder. Global body image distortion did not differbetween the two groups of patients but hips overestimation was greater in the read-mission group. The level of significance was lower than for other variables, in part due tothe fact that we did not have these data for all patients. A higher score on the EATreflected more abnormal eating attitudes and was also related to readmission. Gainingweight is to a large extent a question of personal disposition. Therefore, patients with alower rate of weight increase are less likely to accept weight recovery. In these patients,the disorder is probably more severe. Some authors have pointed out that a rapid weightincrease leads to a higher readmission rate if the weight recovery was not to some extentvoluntary (Lay, Jennen-Steinmetz, Reinghard, & Schmidt, 2002), but this was not the casein the current study. Using age, EAT score, and rate of weight gain at first admission, itwas possible to differentiate to a substantial degree between patients who would requirereadmission after weight recovery and those who would not. The significant variables forprediction of readmission seem to be related more to the severity of the psychologicaldisorder than to the level of biologic abnormalities.
The most important limitation of this study is that only some of the variables that maybe related to readmission are analyzed. Therefore, the predictors described in the currentstudy may not detect all patients at risk of readmission. It is highly possible that read-mission may be influenced, in part, by depressive or obsessive symptomatology or bypersonality characteristics. Moreover, certain studies have stressed the importance offamily relationships and parental rearing practices for readmission and outcome inadolescent patients, but these variables are not analyzed in the current study (Castro,Toro, & Cruz, 2000; North, Gowers, & Byram, 1997). Disturbance of body image, at leastof some parts of the body, seems to have an influence on readmission. However, becausesome of our data were missing, we were unable to quantify it. The number of males andpurging-type patients was low, which made it impossible to establish whether the rate ofreadmissions was different in these groups of patients. Finally, the EAT was adminis-tered at the beginning of the inpatient treatment and it is likely that the score would havechanged somewhat during admission. The EAT score just before discharge would prob-ably be even more relevant to readmission.
Clinical Implications
There seems to be a need to change the standard admission treatment program incertain patients who present a higher risk of readmission after weight recovery. Veryyoung adolescent patients (i.e., those younger than 15) with a high EAT score and a lowrate of weight recovery during admission probably need a longer hospitalization, aperiod of weight maintenance before discharge, and frequent therapeutic sessions inthe day hospital or outpatient treatment afterwards. All these variables are relatedmore to the severity of the psychological disorder than to the severity of biologicabnormalities. In all probability, there are other measures of psychological impairment
28 Castro et al.
in anorexia nervosa that could also be taken as predictors of readmission. Some of thevariables identified in adult samples, such as BMI at admission or duration of disorder,do not seem to indicate greater risk of readmission in adolescents. Future studies arenecessary to identify other variables that are relevant to the readmission rate in this agegroup. This would help to make treatment programs more flexible and adaptable to theneeds of different groups of patients and, therefore, to provide more effective care.
REFERENCES
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.).Washington, DC: Author.
Attia, E., Haiman, C., Walsh, B.T., & Flater, S.R. (1998). Does fluoxetine augment the inpatient treatment ofanorexia nervosa? American Journal of Psychiatry, 155, 548–551.
Baran, S.A., Weltzin, T.E., & Kaye, W.H. (1995). Low discharge weight and outcome in anorexia nervosa.American Journal of Psychiatry, 152, 1070–1072.
Castro, J., Lazaro, L., Pons, F., Halperin, I., & Toro, J. (2001). Adolescent anorexia nervosa: The catch-up effect inbone mineral density after recovery. Journal of the American Academy of Child and Adolescent Psychiatry,40, 1215–1221.
Castro, J., Toro, J., & Cruz, M. (2000). Quality of rearing practices as predictor of short-term outcome inadolescent anorexia nervosa. Psychological Medicine, 30, 61–67.
Castro, J., Toro, J., Salamero, M., & Guimera, E. (1991). The Eating Attitudes Test: Validation of the Spanishversion. Evaluacion Psicologica/Pshychological Assessment, 7, 175–190.
Garner, D.M., & Garfinkel, P.E. (1979). The Eating Attitudes Test: An index of the symptoms of anorexianervosa. Psychological Medicine, 9, 1–7.
Gila, A., Castro, J., Toro, J., & Salamero, M. (1998). Subjective body-image dimensions in normal and anorexicadolescents. British Journal of Medical Psychology, 71, 175–184.
Hernandez, M., Sanchez, E., & Sobradillo, B. (2000). Curvas y tablas de crecimiento [growth tables]. InJ. Argente, A. Carrascosa, R. Gracia, & F. Rodrıguez-Hierro (Eds.), Tratado de Endocrinologıa pediatrica y de laadolescencia [Child and Adolescent Endocrinology]. Second edition. Barcelona-Doyma, S.A. pp 1441–1500.
Howard, W.T., Evans, K.K., Quintero-Howard, C.V., Bowers, W.A., & Andersen, A.E. (1999). Predictors ofsuccess or failure of transition to day hospital treatment for inpatients with anorexia nervosa. AmericanJournal of Psychiatry, 156, 1697–1702.
Kahn, C., & Pike, K.M. (2001). In search of predictors of dropout from inpatient treatment for anorexia nervosa.International Journal of Eating Disorders, 30, 237–244.
Lay, B., Jennen-Steinmetz, C., Reinghard, I., & Schmidt, M.H. (2002). Characteristics of inpatient weight gain inadolescent anorexia nervosa: Relation to speed of relapse and re-admission. European Eating DisordersReview, 10, 22–40.
McKenzie, J.M., & Joyce, P.R. (1992). Hospitalization for anorexia nervosa. International Journal of EatingDisorders, 11, 235–241.
Mont, L., Castro, J., Herreros, B., Pare, C., Azqueta, M., Magrina, J., Puig, J., Toro, J., & Brugada, J. (in press).Reversibility of cardiac abnormalities in adolescents with anorexia nervosa after weight recovery. Journal ofthe American Academy of Child and Adolescent Psychiatry.
North, C., Gowers, S., & Byram, V. (1997). Family functioning and life events in the outcome of adolescentanorexia nervosa. British Journal of Psychiatry, 171, 545–549.
Norusis, M.J. (1993). SPSS for windows base system. User’s guide (Release 6.0) [computer software]. Chicago:SPSS.
Nozoe, S., Soejima, Y., Yoshioka, M., Naruo, T., Masuda, A., Nagai, N., & Tanaka, H. (1995). Clinical features ofpatients with anorexia nervosa: Assessment of factors influencing the duration of inpatient treatment.Journal of Psychosomatic Research, 39, 271–281.
Ostuzzi, R., Didonna, F., & Micciolo, R. (1999). One-year weight follow-up in anorexia nervosa after inpatientpsycho-nutritional rehabilitative treatment. Eating and Weight Disorders, 4, 194–197.
Pottick, K.J., McAlpine, D.D., & Andelman, R.B. (2000). Changing patterns of psychiatric inpatient care forchildren and adolescents in general hospitals, 1988–1995. American Journal of Psychiatry, 157, 1267–1273.
Steinhausen, H.C., Seidel, R., & Winkler Metzke, C. (2000). Evaluation of treatment and intermediate and long-term outcome of adolescent eating disorders. Psychological Medicine, 30, 1089–1098.
Striegel-Moore, R.H., Leslie, D., Petrill, S.A., Garvin, V., & Rosenheck, R.A. (2000). One-year use and cost ofinpatient and outpatient services among female and male patients with an eating disorder: Evidence from anational database of health insurance claims. International Journal of Eating Disorders, 27, 381–389.
Strober, M., Freeman, R., DeAntonio, M., Lampert, C., & Diamond, J. (1997). Does adjunctive fluoxetineinfluence the post-hospital course of restrictor-type anorexia nervosa? A 24-month prospective, longitudinalfollow-up and comparison with historical controls. Psychopharmacological Bulletin, 33, 425–431.
Rehospitalization in Anorexia Nervosa 29

Strober, M., Freeman, R., & Morrell, W. (1997). The long term course of anorexia nervosa in adolescents: Survivalanalysis of recovery, relapse and outcome predictors over 10–15 years in a prospective study. InternationalJournal of Eating Disorders, 22, 339–360.
Wickizer, T.M., Lessler, D., & Travis, K.M. (1999). Effects of health care cost-containment programs on patternsof care and readmissions among children and adolescents. American Journal of Public Health, 89, 1353–1358.
Wiseman, C.V., Sunday, S.R., Klapper, F., Harris, W.A., & Halmi, K.A. (2001). Changing patterns of hospitaliza-tion in eating disorder patients. International Journal of Eating Disorders, 30, 69–74.
30 Castro et al.






![[PPT]Anorexia Nervosa - Mr Sitar's Website - homemrsitarswebsite.wikispaces.com/file/view/Anorexia Nervosa... · Web viewWhat is the definition to this illness? Anorexia nervosa is](https://img.pdfslide.net/doc/110x75/5af162f57f8b9ad0618f592d/pptanorexia-nervosa-mr-sitars-website-nervosaweb-viewwhat-is-the-definition.jpg)