Embed Size (px)
Citation preview

JAMDA 14 (2013) 761e767
JAMDA
journal homepage: www.jamda.com
Original Study
Predictors of Rehospitalization Among Elderly Patients Admittedto a Rehabilitation Hospital: The Role of Polypharmacy, Functional Status,and Length of Stay
Alessandro Morandi MD, MPH a,b,c,*, Giuseppe Bellelli MD b,d, Eduard E. Vasilevskis MD c,e,f,g,Renato Turco MD a,b, Fabio Guerini MD a,b, Tiziana Torpilliesi MD a,b, Salvatore Speciale MDb,Valeria Emiliani MD a, Simona Gentile MD a,b, John Schnelle PhD c,g,h, Marco Trabucchi MDb,i
aDepartment of Rehabilitation and Aged Care Hospital Ancelle, Cremona, ItalybGeriatric Research Group, Brescia, ItalycCenter for Quality Aging, Department of Medicine, Vanderbilt University, Nashville, TNdDepartment of Health Science, University of Milano-Bicocca and Geriatric Clinic, S. Gerardo Hospital, Monza, ItalyeDepartment of Medicine, Vanderbilt University, Nashville, TNfCenter for Health Services Research, Department of Medicine, Vanderbilt University, Nashville, TNgDivision of General Internal Medicine and Public Health, Department of Medicine, Vanderbilt University, Nashville, TNh Tennessee Valley Geriatric Research Education Clinical Center, Nashville, TNiUniversity of Tor Vergata, Rome, Italy
Keywords:Rehospitalizationelderlyin-hospital rehabilitation risk factors
The authors declare no conflicts of interest.E.E.V. is supported by the National Institutes of He
Veterans Affairs Geriatric Research, Education andfunding sources did not participate in the planning,pretation of data or in the decision to submit for publfull access to the data and were responsible for th
1525-8610/$ - see front matter Copyright � 2013 - Ahttp://dx.doi.org/10.1016/j.jamda.2013.03.013
a b s t r a c t
Objectives: Rehospitalizations for elderly patients are an increasing health care burden. Nonetheless, wehave limited information on unplanned rehospitalizations and the related risk factors in elderly patientsadmitted to in-hospital rehabilitation facilities after an acute hospitalization.Setting: In-hospital rehabilitation and aged care unit.Design: Retrospective cohort study.Participants: Elderly patients 65 years or older admitted to an in-hospital rehabilitation hospital after anacute hospitalization between January 2004 and June 2011.Measurements: The rate of 30-day unplanned rehospitalization to hospitals was recorded. Risk factors forunplanned rehospitalization were evaluated at rehabilitation admission: age, comorbidity, serumalbumin, number of drugs, decline in functional status, delirium, Mini Mental State Examination score,and length of stay in the acute hospital. A multivariable Cox proportional regression model was used toidentify the effect of these risk factors for time to event within the 30-day follow-up.Results: Among 2735 patients, with a median age of 80 years (interquartile range 74e85), 98 (4%) wererehospitalized within 30 days. Independent predictors of 30-day unplanned rehospitalization were theuse of 7 or more drugs (hazard ratio [HR], 3.94; 95% confidence interval, 1.62e9.54; P ¼ .002) anda significant decline in functional status (56 points or more at the Barthel Index) compared with themonth before hospital admission (HR 2.67, 95% CI: 1.35e5.27; P ¼ .005). Additionally, a length of stay inthe acute hospital of 13 days or more carried a twofold higher risk of rehospitalization (HR 2.67, 95% CI:1.39e5.10); P ¼ .003).Conclusions: The rate of unplanned rehospitalization was low in this study. Polypharmacy, a significantworsening of functional status compared with the month before acute hospital admission, and hospitallength of stay are important risk factors.
Copyright � 2013 - American Medical Directors Association, Inc.
alth (K23AG040157) and theClinical Center (GRECC). Thecollection, analysis, or inter-ication. The investigators hade study protocol, statistical
analysis plan, progress of the study, analysis, reporting of the study, and the deci-sion to publish.* Address correspondence to Alessandro Morandi, MD, MPH, Via Aselli 16, Cre-
mona 26100, Italy.E-mail address: [email protected] (A. Morandi).
merican Medical Directors Association, Inc.

A. Morandi et al. / JAMDA 14 (2013) 761e767762
Among high-income countries, older people (age 65 and older)make up a large (15%e20%) proportion of the population and manyrequire hospitalization for aging-related diseases.1 In theUnited States,almost one-fifth (24.8%) of the government-sponsored Medicarebeneficiariesdischarged fromahospitalwerehospitalizedagainwithin30 days of their index admission.2,3 Rehospitalizations for elderlypatients account for about $15 billion of Medicare expenses4 and anestimated £1.6 billion each year in the United Kingdom.5 A substantialnumber of older patients leaving the hospital receive postacute care(PAC) services in either skilled nursing facilities (SNF) (38% of thosewho receive services after a hospitalization in the United States) or ina hospital rehabilitation setting (9% of all patients in the United Stateswho receive services after a hospitalization).6 The rate of 30-day repeathospitalizations range from 23.5% in skilled nursing7 and 20% in theinpatient rehabilitation settings (P Gozalo and V Mor, Rates of 30-dayrehospitalization by PAC setting, unpublished data). Despite these highrates of hospital readmission, there are limited data about the riskfactors for readmission from either setting.
One study8 reported an 18% hospital readmission rate fora heterogeneous group of patients discharged to a SNF in the UnitedStates and also identified patients with congestive heart failure,urinary tract infection, renal failure, and respiratory diseases at thehighest risk for readmission. A second study9 found that a history ofa malignant solid tumor, a recent hospitalization involving gastro-intestinal diseases, and a low serum albumin level were associatedwith an increased risk for 30-day unplanned rehospitalization froman SNF.
There are no data reported on risk factors for readmission inpatients who receive PAC services in hospital rehabilitation settings.To fill this research gap, we examined a cohort of elderly Italianpatients admitted to an in-hospital rehabilitation setting after anacute hospitalization, given that in Italy about 58% of beds for PACservices after a hospitalization are in rehabilitation hospitalsettings.10 Our primary aim was to describe the rate of unplannedrehospitalization occurring within 30 days and to identify clinical riskfactors for rehospitalization, considering the importance of control-ling the phenomenon to avoid the stress to elderly frail patientsinduced by repeated hospital readmissions.
Methods
We performed a retrospective cohort study of patients older than65 years and consecutively admitted to an in-hospital rehabilitationsetting following an acute care hospitalization. The in-patient reha-bilitation setting was the “Ancelle della Carità” Hospital (Cremona,Italy). Patients were admitted to the Department of Rehabilitationand Aged Care (DRAC), a 90-bed unit staffed by full-time geriatricians,physiatrists, nurses, nurse aids, and physical, speech, and occupa-tional therapists.11 An on-site physician provided 24-hour medicalcoverage. We excluded patients who were admitted from noneacutecare settings, patients younger than 65 years, and those who diedduring the rehabilitation stay. The DRAC admits patients after anacute hospitalization for surgical procedures (hip fracture surgicalrepair; hip or knee arthroplasty; abdominal, cardiac, vascular, orthoracic surgery), stroke (recent or chronic), acute heart failure,chronic obstructive pulmonary diseases, Parkinson disease, or gaitand balance disorders.11 Patients are considered eligible for the DRACadmission if they are capable of performing a standard rehabilitativeprogram including 2 daily sessions per patient (40 minutes in themorning and 40 minutes in the afternoon) from Monday to Fridayand a single session (40 minutes in the morning) on Saturday. Specifictraining is then required according to the admission diagnosis. TheEthics Committee of Gerontological Sciences of the Geriatric ResearchGroup, Italy, approved the study protocol and the waiver of informedconsent.
Data Sources
All data were collected through existing administrative databases.
Risk Factors for 30-Day Unplanned Rehospitalization to HospitalAfter Admission to DRAC
Risk factors for unplanned rehospitalization were determineda priori according to previous research in acute hospital settings,12
clinical importance, and availability/completeness in the adminis-trative databases. In addition, we focused on factors readily availableat the time of admission to rehabilitation so as to provide clinicianswith variables useful to identify patients at higher risk ofhospitalization.
Demographic factors included age. Comorbidity was defined ac-cording to the Cumulative illness rating score (CIRS).13 CIRS is a co-morbidity index, assessing chronic medical illness burden whiletaking into account the severity of chronic diseases; the score for eachof the 14 conditions can range from 1 (absence of pathology) to 5(maximum level of severity of the disease). The CIRS severity index isthe average score of the first 13 items, whereas the Comorbidity Indextotal score represents the number of the 14 items with a score of 3 orhigher. Admission diagnoses to the in-hospital rehabilitation settingwere recorded. Additionally, we recorded the diagnoses related to there-admission in acute hospital and we categorized them by reviewingeach patient’s medical records.8 A surrogate measure of nutritionalstatus was measured with albumin levels at the time of DRACadmission. Functional status was assessed with the Barthel Index (BI)through patient and surrogate interview referring to the monthbefore the acute hospital admission,14,15 at rehabilitation admission,and discharge. We examined the change in BI (delta-BI), defined asthe BI before acute hospital admission minus the BI at rehabilitationadmission; cognitive assessments at DRAC admission included thepresence of delirium evaluated by expert geriatricians with theConfusion Assessment Method (CAM)16 and global cognitive perfor-mance with Mini Mental State Examination (MMSE).17 As per theCAM algorithm, delirium was considered as present if there was anacute onset or fluctuating course, inattention, and either disorganizedthinking or altered level of consciousness. Medication burden wasmeasured by the total number of drugs at DRAC admission. Finally,health care use was measured using length of stay (LOS) at the acutehospital measured in days.
Outcome Definition
Rehospitalization was defined as every unplanned readmission tothe hospital occurring within 30 days after admission to the DRAC. Ifa patient was rehospitalized more than once, each episode wascounted as a separate hospitalization.
Statistical Analysis
Demographics and clinical variables were summarized usingmedian and interquartile range (IQR) for continuous variables orproportions for categorical variables. For descriptive purposes, theadmission diagnoses to the in-hospital rehabilitation and the read-mission diagnoses were reported. A multivariable Cox proportionalregression model was used to identify the effect of the previouslymentioned risk factors on the time to unplanned rehospitalizationwithin the 30-day follow-up. Patient data were censored at time tohospital readmission. All the risk factorswerefirst entered in themodelas continuous variables, except for delirium at DRAC admission. Thevariables found to be statistically associated with a higher risk ofhospital readmission (P < .05) were then categorized in tertiles, ac-cording to their distribution, to provide clinicians with actionable

A. Morandi et al. / JAMDA 14 (2013) 761e767 763
thresholds that could be applied in daily practice. Because there is noformal definition of polypharmacy, we chose the tertiles cutoff for thenumber of medications, which produced results similar to a previouspublication.18 A test for trend showed an increased risk of hospitali-zation across 3 different risk factors: total number of drugs (P ¼ .000),thedelta-BI (P¼ .002), and theLOS in the acutehospital (P¼ .000). A testfor proportional hazard assumptionwas also performed (c2 6.92, df 12;P¼ .8625), which showed that there was no evidence to contradict theproportionality of hazard assumption. Kaplan-Meier analyses and log-rank testwere also used to assess the effect of these risk factors on timeto hospital re-admission. All statistical analyses were performed usingSTATA version 11 (http://www.stata.com/stata11/) (Stata Corp, CollegeStation, TX).
Results
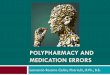
Between January 2004 and June 2011, a total of 6383 patientswere admitted to the DRAC. Of these, 3648 were excluded: 896 weretransferred from other rehabilitation settings, 2144 were admittedfrom home or SNFs, 512 were younger than 65 years, and 96 diedduring the DRAC stay. The remaining cohorts of 2735 patients aredescribed in Table 1. The cohort had a median age of 80 years andmost (71%) were women. The main overall admission diagnoses tothe DRAC were orthopedic (44%), followed by neurologic (16%),respiratory (17%), and cardiologic (10%). The rate of 30-day unplannedrehospitalization was 4% (n ¼ 98). In Figure 1 are shown the maincauses of readmission to the acute hospital wards. About half of thepatients who were admitted to the DRAC with a musculoskeletal(46%), cardiovascular (64%), or respiratory (46%) diagnosis werereadmitted with the same diagnosis (online Appendix 1).
Table 1Clinical Characteristics and Demographics of a Population of Elderly PatientsAdmitted to a Department of Rehabilitation and Aged Care
Variable* n ¼ 2735
Age, y 80 (74e85)Female, n (%) 1.975 (71)Barthel Index prehospital admissiony 94 (78e100)Barthel Index at rehabilitation admission 44 (26e62)Barthel Index at rehabilitation discharge 82 (57e94)Delta Barthel Indexz 40 (24e56)Cumulative illness rating score severity indexx 1.62 (1.46e1.84)No. of drugs at rehabilitation admission 5 (4e7)Albumin at rehabilitation admission, mg/dL 3.1 (2.8e3.3)Delirium at rehabilitation admission, n (%) 500 (18)Mini Mental State Examination at rehabilitationadmission
23 (17e27)
Admission diagnoses to the in-hospital rehabilitationsetting, n (%)Orthopedic 1204 (44)Neurologic 422 (16)Respiratory 457 (17)Cardiologic 281 (10)Gait disturbances 255 (9)Other 116 (4)
Length of stay acute hospital 8 (6e13)Length of stay rehabilitation setting 24 (20e34)Rehospitalization within 30 days, n (%) 98 (4)
*Median and interquartile range, unless otherwise noted.yBarthel Index a month before the index admission to the acute hospital evalu-
ated through surrogate interview.zDelta Barthel Index was calculated as the difference of Barthel Index prehospital
admission (ie, Barthel index a month before the index acute hospital admission) andthe Barthel Index at rehabilitation admission.
xCumulative illness rating score (CIRS) is a screening tool for comorbidity,assessing the chronic medical illness burden while taking into account the severityof chronic diseases; the score for each of the 14 items can range from 1 (absence ofpathology) to 5 (maximum level of severity of the disease). The CIRS severity indexis the result of the average score of the first 13 items.
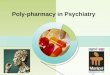
In the multivariable Cox regression models, 3 clinical variableswere independent predictors of time to unplanned readmission: thetotal number of drugs, the delta-BI, and the LOS in the acute hospital(Table 2). For these variables, there was an increasing risk as the doseof exposure increased. Patients taking 7 or more drugs on admissionto the DRAC had about a 4 times higher risk of being rehospitalized(hazard ratio [HR] 3.94; 95% confidence interval [CI] 1.62e9.54;P ¼ .002), whereas those taking 4 to 6 drugs had nonsignificant risk ofrehospitalization (HR 1.59; 95% CI 0.64e3.94; P ¼ .315) (Figure 2A).However, the test for trend across categories was statistically signif-icant, indicating that the greater number of medications, the greaterthe likelihood of readmission. Similarly, those who had the highestdecline in functional status (ie, delta-BI >56) from prehospital toDRAC admissions had almost a 3 times higher risk of being re-hospitalized (HR 2.67, 95% CI 1.35e5.27; P ¼ .005), whereas thosewith a delta-BI between 25 and 56 did not have an increased risk ofrehospitalization (HR 1.48, 95% CI 0.79e2.75; P ¼ .216) (Figure 2B). Asfor the number of medications, the test for trend across BI categorieswas statistically significant, indicating the greater functional decline,the greater the likelihood of readmission. Finally, patients who hada LOS in the acute hospital longer than 13 days had a more thantwofold higher risk of being readmitted to the hospital (HR 2.67, 95%CI 1.39e5.10; P ¼ .003), whereas those with a LOS between 7 and 13days (HR 1.74, 95% CI 0.93e3.25; P ¼ .080) were not at increased riskof rehospitalization (Figure 2C). Once again, the test for trend acrossLOS categories was statistically significant, indicating the longer theLOS, the greater the likelihood of readmission.
Discussion
In a large cohort of elderly patients admitted to an in-hospitalrehabilitation unit, we found a low rate of 4% unplanned re-hospitalization. Most of the patients who were admitted to the DRACwith musculoskeletal, cardiovascular, or respiratory diagnoses werereadmitted to the acute hospital with the same diagnosis. Among thesmall but important number of readmitted patients, we found thatusing 7 or more drugs, having a significant decline in functionalperformance (ie, delta-BI �56 points) in the 30 days before DRACadmission, and having a length of acute hospital stay longer or equalto 13 days were independent predictors of 30-day rehospitalization.These 3 risk factors are readily accessible at the bedside and offera potentially simple method to screen for patient risk. Although thedata are promising, their role in the prevention of unplanned read-mission to hospital needs to be further investigated, evaluatingprograms to improve transitions of care across different settings.
The topic of short-term unplanned readmissions after dischargefrom a health care facility has received increasing attention. Indeed,most of the investigations have studied readmissions among patientsleaving the hospital for home,12,19e21 and 3 studies reported read-missions from the SNFs.8,9,22 This is the first study, to the best of ourknowledge, to report rehospitalization and risk factor data from in-hospital PAC rehabilitation facilities.
It is of interest that the readmission rate found in our study iscomparable with 30-day readmission data for people dischargedhome from European acute hospitals19,20,23 and considerably lowerthan 30-day readmission rates reported for American patients dis-charged to all settings.7,8
There are a variety of potential explanations of these findings. Thefirst relies on the differences in the acute hospital LOS between Italyand the United States. Indeed, the average LOS in the United States is5 days,24 whereas in Italy the overall median acute hospital LOS isabout 8 days, similar to other European countries.24 Because previousstudies have shown that the shorter the LOS in acute hospital wards,the greater the likelihood of being discharged with unresolved

Fig. 1. Admission and readmission diagnoses. The y-axis describes the admission diagnoses to the Department of Rehabilitation and Aged Care for the 112 patients whowere readmitted. On the x-axis are reported the main readmission diagnoses. We selected the 3 most frequent admission diagnoses. Additional data are available in theonline Appendix 1.
A. Morandi et al. / JAMDA 14 (2013) 761e767764
medical issues,25e28 it could be hypothesized that patients trans-ferred from acute hospitals to the PAC rehabilitation settings are morefrequently clinically unstable in the United States than in the Italiancounterpart.
An additional explanation relies on the difference in the LOS ofin-hospital rehabilitation between the United States and Italy.Indeed, previous studies29,30 have shown that not only the median
Table 2Risk Factors for Time to Unplanned Readmission to the Hospital Within 30 DaysFollowing Admission to the DRAC*
Variable HazardRatio
95% ConfidenceInterval
P Value
Age 1.00 0.96e1.03 .93CIRS severity index1.46 to 1.84 0.98 0.45e1.89 .838�1.85 1.50 0.69e3.28 .300Albumin, mg/dL 0.64 0.38e1.05 .082
No. of drugs at DRAC admission<4 drugs Ref.4 to 6 drugs 1.59 0.64e3.94 .315�7 drugs 3.94 1.62e9.54 .002
Delta Barthel Index at rehabilitationadmissiony
�24 Ref25e56 1.48 0.79e2.75 .216>56 2.67 1.35e5.27 .005Delirium at DRAC admission 0.77 0.40e1.46 .421MMSE score at DRAC admission 0.97 0.94e1.01 .128
Length of stay in the acute hospital�6 days Ref.7e13 days 1.74 0.93e3.25 .080>13 days 2.67 1.39e5.10 .003
CIRS, Cumulative illness rating score; DRAC, Department of Rehabilitation and AgedCare; MMSE, Mini Mental State Examination.
*A multivariable Cox proportional regression model was used to identify theeffect of risk factors evaluated at the time of DRAC admission on the time tounplanned readmission to the acute hospital within a 30-day follow-up. All the riskfactors were first entered in the model as continuous variables, except for deliriumat DRAC admission. The variables found to be statistically associated with a higherrisk of hospital readmission (P < .05) were then categorized in tertiles, according totheir distribution, to provide clinicians with actionable thresholds that could beapplied in daily practice.
yDelta Barthel Index was calculated as the difference of Barthel Index pread-mission (ie, Barthel index a month before the index acute hospital admission) andthe Barthel Index at rehabilitation admission.
LOS in the American rehabilitation wards fell from 1994 to 2001from 20 to 12 days (exactly the half of median value in our popu-lation), but also that this trend30 was associated with an increasedrate of hospital readmissions in the same period. Therefore, it mightbe hypothesized that the longer the LOS in the PAC, the lower therisk of being rehospitalized. A plausible explanation of this findingmay be that with longer hospital stays, physicians have more timeto manage clinical instability when it develops during the rehabil-itation processes.
Third, in the United States, the in-hospital rehabilitation settingsare mainly staffed with physiatrists, whereas our institution is mainlystaffed with geriatricians with the support of physiatrists. Given theadvanced age of our population, it might be that a geriatric multidi-mensional approach provides better care for a frail population withbetter outcomes, as proven in other settings.31 Indeed, it is interestingto observe that although 18% of our population had delirium onadmission to our DRAC, only 2% of the patients were still delirious atthe time of discharge. The prevalence of delirium at discharge islower than previous investigations32,33 in which about 50% of elderlypatients who had delirium on admission to PAC still had delirium 1month later,32,33 indirectly suggesting a tight clinical surveillance inour setting to prevent and manage conditions possibly related toclinical instability.
Our finding that the longer the LOS in acute hospital, the greaterrisk of hospital readmissions might find an explanation in theconcept of “posthospital syndrome.”34 Patients with a longer LOSare more likely to develop new active medical issues and physicaldisabilities, suggesting an underlying condition of frailty. Thesepatients should receive a strict clinical surveillance to avoid furthercomplications. In line with this assumption, it has been shown byDharmarajan et al3 that the 30-day readmission diagnoses in frailelderly patients is often attributable to causes involving multiplephysiological systems and not only to the conditions related to theinitial acute hospitalization. Therefore, as suggested by Ouslanderet al,8 patients who are admitted to a rehabilitation setting shouldbe monitored not only for the primary hospital diagnosis, but alsofor other active medical problems that may lead to rehospitaliza-tions. It is important to underline that our readmission rate was lowand that the readmission diagnoses were, in about half of the cases,the same as the hospital admission diagnoses. These data indirectlysuggest that the multidimensional geriatric approach in our insti-tution led to an effective clinical management of the frail patients.

0.00
0.05
0.10
0.15
0.20
Prob
abilit
y of
reho
spita
lizat
ion
0 10 20 30Days
Drugs<4 Drugs 4-6Drugs >=7
Rehospitalization within 30 daysA
Log rank 0.0001
0.00
0.05
0.10
0.15
Prob
abilit
y of
reho
spita
lizat
ion
0 10 20 30Days
DeltaBI <=24 DeltaBI 25-56DeltaBI >56
Rehospitalization within 30 daysB
Log rank 0.003
0.00
0.05
0.10
0.15
0.20
Prob
abilit
y of
reho
spita
lizat
ion
0 10 20 30Days
LOS_H<=6 LOS_H 7-13 LOS_H>13
Rehospitalization within 30 daysC
Log rank 0.001
Fig. 2. Probability of unplanned readmission to the acute hospital according to (A) number of drugs (Drugs) evaluated on the Department of Rehabilitation and Aged Care (DRAC)admission; (B) length of stay in the acute hospital setting (LOS_H); (C) changes in functional status as detected with the delta-BI (Barthel index score prehospital admission minusBarthel index score at DRAC admission).
A. Morandi et al. / JAMDA 14 (2013) 761e767 765
The avoidance of hospital readmission and the management of the“posthospital syndrome” in the rehabilitation setting is not only animportant marker of the quality of care but it should be on the topof the list of clinicians’ priorities to avoid further stress to thepatients and their families.
In addition to the increased LOS, we found polypharmacy anddecline in functional status as risk factors for rehospitalization. Thesefindings support previous research from acute hospitalsettings.20,35e37 Polypharmacy and inappropriate medicationprescription are frequent issues in elderly patients and they intensifywith increasing age and acute hospitalization.38e40 Between 50% and85% of elderly patients are discharged with potentially or actuallyinappropriate medications after an acute hospital stay.40,41 Inappro-priate medication prescription is associated with greater risk ofadverse events, such as confusion and falls, as well as increasedhealth care costs, hospitalization, cognitive impairment, andmortality.42e45 The association between polypharmacy and re-hospitalization might be the expression of the interaction of severaldrugs and their related adverse reaction,18 although we are unable tosupport this hypothesis with the data included in our investigation.Additionally, certain offending medications might further explain theadverse association between polypharmacy and rehospitalization. Forinstance, elderly patients are frequently prescribed proton pumpinhibitors for stress ulcer prophylaxis during the acute hospital stay.46
Most of the patients are then discharged on these drugs, potentially
exposing the patients to a higher risk of pneumonia and Clostridiumdifficile infection.47,48 In our investigation, we did not gather thisgranular information, but future investigation should further explorethe association between polypharmacy and rehospitalization toexplain the underling mechanisms, which should then be target offuture interventions.
Finally, the acute decline of functional status also provides clini-cians with key information on the patients’ global incapacity to reactto a stressful condition as an expression of a baseline frailty.49 Theassociation between functional decline during an acute illness is notjust a marker for rehospitalization, but can be used at the bedside alsoto estimate long-term prognosis.11,50,51
Our study includes a number of notable strengths. It is the first toevaluate the rate of unplanned readmissions to the hospital, and therelated risk factors, in a large population of elderly patients admittedto an in-hospital rehabilitation setting. In addition, our study containsfunctional and cognitive data obtained from a multidimensionalevaluation carried out by expert geriatricians. Findings from thisstudy might represent a basis for national and regional healthsystems to stimulate benchmarking policies across postacute andrehabilitative centers and to implement reimbursement strategies inrelation to rehospitalization rates.
Limitations of our study must be considered as well. First, this wasa retrospective cohort study carried out in a single center, thuspotentially limiting generalizability. In addition, although we

A. Morandi et al. / JAMDA 14 (2013) 761e767766
examined the total number of medications, we have not addressedwhether medication discrepancies, which often occur after thetransition from hospital to the setting of discharge,52 are a risk factorfor rehospitalization. Additionally, we were unable to collect infor-mation on specific types of drugs (eg, antipsychotics, sedatives,hypnotics). There are additional risk factors we have not accountedfor (eg, social determinants of health, such as health literacy, socio-economic status, caregiver support) that may explain lower rates ofreadmission and be important predictors of readmission. Last, theinclusion of admission diagnoses as possible confounding factorsshould also be included in future studies.
This study provides new important information on the epidemi-ology of unplanned rehospitalization of elderly patients admitted toan in-hospital rehabilitation setting after an acute hospitalization.Furthermore, it identifies 3 risk factors of unplanned 30-day re-hospitalization, which are easily accessible at the bedside and shouldbe used as a simple predictive model for clinicians at the time ofadmission to in-hospital rehabilitation.
Acknowledgments
We acknowledge Dr. Sara Morghen and Dr. Elena Lucchi for theirsupport in data collection.
We also would like to acknowledge Kelly H.S. Wright MA,Department of Medicine (General Internal Medicine and PublicHealth), Center for Health Services Research, Vanderbilt University,Nashville, TN, for her administrative and editorial assistance in thepreparation of this manuscript.
Supplementary Data
Supplementary data related to this article can be found online athttp://dx.doi.org/10.1016/j.jamda.2013.03.013.
References
1. World Health Organization. Regional Office for Europe’s Health EvidenceNetwork (HEN): Do current discharge arrangements from inpatient hospitalcare for the elderly reduce readmission rates, the length of inpatient stay ormortality, or improve health status?. 2005.
2. Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in theMedicare fee-for-service program. N Engl J Med 2009;360:1418e1428.
3. Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day read-missions after hospitalization for heart failure, acute myocardial infarction, orpneumonia. JAMA 2013;309:355e363.
4. Commission MPA. Report to the Congress: Promoting Greater Efficiency inMedicare. Washington, DC: Medicare Payment Advisory Commission; 2007.
5. Robinson P. Hospital readmissions and the 30 day threshold. London: CHKS.Available at: http://www.chks.co.uk/assets/files/Hospital_readmissions_and_the_30_day_threshold_final.pdf; 2010. Accessed November 12, 2012.
6. MedPAC. Report to the Congress: Medicare Payment Policy. Washington, DC:Medicare Payment Advisory Commission; 2011.
7. Mor V, Intrator O, Feng Z, Grabowski DC. The revolving door of rehospitaliza-tion from skilled nursing facilities. Health Aff 2010;29:57e64.
8. Ouslander JG, Diaz S, Hain D, Tappen R. Frequency and diagnoses associatedwith 7- and 30-day readmission of skilled nursing facility patients toa nonteaching community hospital. J Am Med Dir Assoc 2011;12:195e203.
9. Dombrowski W, Yoos JL, Neufeld R, Tarshish CY. Factors predicting rehospi-talization of elderly patients in a postacute skilled nursing facility rehabilitationprogram. Arch Phys Med Rehabil 2012;93:1808e1813.
10. Boldrini M, Di Cesare M, Pennazza F. Rapporto “Riabilitazione 2003”: Ministerodella Salute. Rome: Dipartimento della Qualità. Direzione Generale del SistemaInformativo, 2003.
11. Bellelli G, Magnifico F, Trabucchi M. Outcomes at 12 months in a population ofelderly patients discharged from a rehabilitation unit. J Am Med Dir Assoc2008;9:55e64.
12. Kansagara D, Englander H, Salanitro A, et al. Risk prediction models for hospitalreadmission: A systematic review. JAMA 2011;306:1688e1698.
13. Parmelee PA, Thuras PD, Katz IR, Lawton MP. Validation of the CumulativeIllness Rating Scale in a geriatric residential population. J Am Geriatr Soc 1995;43:130e137.
14. Mahoney Fi BD. Functional evaluation: The Barthel index. Md State Med J 1965;14:61e65.
15. Lawton MP, Brody EM. Assessment of older people: Self-maintaining andinstrumental activities of daily living. Gerontologist 1969;9:179e186.
16. Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: The confusionassessment method. A new method for detection of delirium. Ann Intern Med1990;113:941e948.
17. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical methodfor grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189e198.
18. Onder G, Petrovic M, Tangiisuran B, et al. Development and validation ofa score to assess risk of adverse drug reactions among in-hospital patients 65years or older: The GerontoNet ADR risk score. Arch Intern Med 2010;170:1142e1148.
19. Bisharat N, Handler C, Schwartz N. Readmissions to medical wards: Analysisof demographic and socio-medical factors. Eur J Intern Med 2012;23:457e460.
20. Zamir D, Zamir M, Reitblat T, et al. Readmissions to hospital within 30 days ofdischarge from the internal medicine wards in southern Israel. Eur J Intern Med2006;17:20e23.
21. Bianco A, Mole A, Nobile CG, et al. Hospital readmission prevalence andanalysis of those potentially avoidable in southern Italy. PloS One 2012;7:e48263.
22. Marcantonio ER, Kiely DK, Simon SE, et al. Outcomes of older peopleadmitted to postacute facilities with delirium. J Am Geriatr Soc 2005;53:963e969.
23. Guerini F, Frisoni GB, Morghen S, et al. Clinical instability as a predictor ofnegative outcomes among elderly patients admitted to a rehabilitation ward.J Am Med Dir Assoc 2010;11:443e448.
24. OECD. Health at a Glance 2011: OECD Indicators. 2011.25. Halm EA, Fine MJ, Kapoor WN, et al. Instability on hospital discharge and the
risk of adverse outcomes in patients with pneumonia. Arch Intern Med 2002;162:1278e1284.
26. Halm EA, Magaziner J, Hannan EL, et al. Frequency and impact of active clinicalissues and new impairments on hospital discharge in patients with hip frac-ture. Arch Intern Med 2003;163:108e113.
27. Metersky ML, Tate JP, Fine MJ, et al. Temporal trends in outcomes of olderpatients with pneumonia. Arch Intern Med 2000;160:3385e3391.
28. Qian X, Russell LB, Valiyeva E, Miller JE. ’Quicker and sicker’ under Medicare’sprospective payment system for hospitals: New evidence on an old issue froma natioanl longitudinal survey. Bull Econ Res 2011;63:3307e3378.
29. Ottenbacher KJ, Smith PM, Illig SB, et al. Trends in length of stay, living setting,functional outcome, and mortality following medical rehabilitation. JAMA2004;292:1687e1695.
30. Ottenbacher KJ, Smith PM, Illig SB, et al. Length of stay and hospital read-mission for persons with disabilities. Am J Public Health 2000;90:1920e1923.
31. Ellis G, Whitehead MA, O’Neill D, et al. Comprehensive geriatric assessment forolder adults admitted to hospital. Cochrane Database Syst Rev2011;(7):CD006211.
32. Kiely DK, Bergmann MA, Jones RN, et al. Characteristics associated withdelirium persistence among newly admitted post-acute facility patients.J Gerontol A Biol Sci Med Sci 2004;59:344e349.
33. Marcantonio ER, Simon SE, Bergmann MA, et al. Delirium symptoms in post-acute care: Prevalent, persistent, and associated with poor functionalrecovery. J Am Geriatr Soc 2003;51:4e9.
34. Krumholz HM. Post-hospital syndromedan acquired, transient condition ofgeneralized risk. N Engl J Med 2013;368:100e102.
35. Philbin EF, DiSalvo TG. Prediction of hospital readmission for heart failure:Development of a simple risk score based on administrative data. J Am CollCardiol 1999;33:1560e1566.
36. van Walraven C, Dhalla IA, Bell C, et al. Derivation and validation of an index topredict early death or unplanned readmission after discharge from hospital tothe community. CMAJ 2010;182:551e557.
37. Hasan O, Meltzer DO, Shaykevich SA, et al. Hospital readmission ingeneral medicine patients: A prediction model. J Gen Intern Med 2010;25:211e219.
38. Corsonello A, Pedone C, Corica F, Incalzi RA. Polypharmacy in elderly patientsat discharge from the acute care hospital. Ther Clin Risk Manag 2007;3:197e203.
39. Burgess CL, Holman CD, Satti AG. Adverse drug reactions in older Australians,1981e2002. Med J Aust 2005;182:267e270.
40. Morandi A, Vasilevskis EE, Pandharipande PP, et al. Inappropriate medicationsin elderly ICU survivors: Where to intervene? Arch Intern Med 2011;171:1032e1034.
41. Onder G, Landi F, Cesari M, et al. Inappropriate medication use among hospi-talized older adults in Italy: Results from the Italian Group of Pharmacoepi-demiology in the Elderly. Eur J Clin Pharmacol 2003;59:157e162.
42. Wright RM, Roumani YF, Boudreau R, et al. Effect of central nervous systemmedication use on decline in cognition in community-dwelling older adults:Findings from the Health, Aging and Body Composition Study. J Am Geriatr Soc2009;57:243e250.
43. Fick DM, Mion LC, Beers MH, J LW. Health outcomes associated with poten-tially inappropriate medication use in older adults. Res Nurs Health 2008;31:42e51.
44. Hanlon JT, Schmader KE, Samsa GP, et al. A method for assessing drug therapyappropriateness. J Clin Epidemiol 1992;45:1045e1051.

A. Morandi et al. / JAMDA 14 (2013) 761e767 767
45. Lau DT, Kasper JD, Potter DE, et al. Hospitalization and death associated withpotentially inappropriate medication prescriptions among elderly nursinghome residents. Arch Intern Med 2005;165:68e74.
46. Hajjar ER, Hanlon JT, Sloane RJ, et al. Unnecessary drug use in frail older peopleat hospital discharge. J Am Geriatr Soc 2005;53:1518e1523.
47. Giuliano C, Wilhelm SM, Kale-Pradhan PB. Are proton pump inhibitors asso-ciated with the development of community-acquired pneumonia? A meta-analysis. Expert Rev Clin Pharmacol 2012;5:337e344.
48. Kwok CS, Arthur AK, Anibueze CI, et al. Risk of Clostridium difficile infectionwith acid suppressing drugs and antibiotics: Meta-analysis. Am J Gastroenterol2012;107:1011e1019.
49. Sleiman I, Rozzini R, Barbisoni P, et al. Functional trajectories during hospi-talization: A prognostic sign for elderly patients. J Gerontol A Biol Sci Med Sci2009;64:659e663.
50. Inouye SK, Peduzzi PN, Robison JT, et al. Importance of functional measures inpredicting mortality among older hospitalized patients. JAMA 1998;279:1187e1193.
51. Bellelli G, Noale M, Guerini F, et al. A prognostic model predicting recovery ofwalking independenceofelderlypatientsafterhip-fracture surgery.Anexperimentin a rehabilitation unit in Northern Italy. Osteoporos Int 2012;23:2189e2200.
52. Coleman EA, Smith JD, Raha D, Min SJ. Posthospital medication discrepancies:Prevalence and contributing factors. Arch Intern Med 2005;165:1842e1847.