Embed Size (px)
Citation preview

Pharmacoeconomics 2007; 25 (9): 783-792ORIGINAL RESEARCH ARTICLE 1170-7690/07/0009-0783/$44.95/0
© 2007 Adis Data Information BV. All rights reserved.
Preferences of CommunityPharmacists for Extended Rolesin Primary CareA Survey and Discrete Choice Experiment
Anthony Scott,1 Christine Bond,2 Jackie Inch2 and Aileen Grant2
1 Melbourne Institute of Applied Economic and Social Research, The University of Melbourne,Melbourne, Victoria, Australia
2 Department of General Practice and Primary Care, University of Aberdeen,Aberdeen, Scotland
Background: Major changes in the roles and responsibilities of pharmacistsAbstractacross the world are occurring. A new Scottish Community Pharmacy contractwas introduced in April 2006, following the introduction of a similar contract inEngland in 2005. This contract encourages greater involvement in medicinesmanagement and other clinical cognitive roles, whilst retaining a supply function.
Objective: To use a discrete choice experiment (DCE) to examine the strength ofpreference of community pharmacists for existing and potential new roles, prior tothe introduction of the new contract.
Study design: The DCE was a component of a larger questionnaire, whichassessed demography, workload, attitudes to, and satisfaction with, proposed newroles, and current levels of activity. Attributes and levels for the DCE were basedon the recent policy document for Scotland, The Right Medicine, and informedconsensus, respectively. Scenarios were organised into pairs, and pharmacistswere asked “Which job would you prefer?” The questionnaire was mailed to allpharmacists working in the community setting in Scotland (n = 1621), as identi-fied from a telephone survey. The questionnaire was totally anonymous, and tworeminders were sent.
Results: There was an overall response rate of 56.4% (914/1621). Communitypharmacists preferred to work in an extended pharmacy team, to have strongintegration with secondary care, and to provide a minor illness advice service. In2003, they would forgo an annual income of £3443, £2183 and £2798, respective-ly to achieve this. However, overall, the pharmacists preferred more income toless. Repeat dispensing, chronic disease management, offering health promotionservices, and the number of prescriptions dispensed per month were not signifi-cant predictors of job choice.
Conclusion: Community pharmacists placed the highest value on organisationalaspects of their work, and having a first contact primary care role. Although total

784 Scott et al.
income was important, there were indications that they would be prepared to forgoincome to attain their preferred job.
In many countries, community pharmacy is macists can advise GPs about cost-effective pre-based around the dispensing of prescribed pharma- scribing, and their patients on the optimal use ofceuticals and retail sales of non-prescription medicines. The Right Medicine suggests expandedpharmaceuticals and other products. However, in roles in chronic disease management, medicationmany developed countries, the emphasis in commu- review and repeat prescribing. Community pharma-nity pharmacy is moving away from the traditional cists are therefore regarded as a key element both indispensing role. Community pharmacists are play- managing pharmaceutical demand in primary careing an increased role in the provision of first contact and in promoting more cost-effective prescribing,primary care and health promotion, and in the provi- which may help slow the growth of NHS pharma-sion of expert advice to GPs and patients about the ceutical expenditure.cost effectiveness of pharmaceuticals. Many of these new proposed roles are based on
The UK is among those countries in which this innovative pilot schemes and evaluated interven-increased role is at an advanced stage of national tions providing evidence of benefit.[4] However,implementation and acceptance. Policy documents with the current fixed capacity workforce and skillwithin the UK have set out an ambitious programme mix, the possibility for changes to occur in the workof reform that includes fundamental changes to the patterns of community pharmacists is limited; thisway community pharmacies work.[1-3] This is being will be particularly problematic in remote and ruralsupported by a new NHS contract for community areas. It is necessary to alter the skill mix within thepharmacy in the UK, which is more clearly remuner- community pharmacy team and/or improve recruit-ating these new roles as part of the ‘core’ work of ment and retention[5] in order to address the currentcommunity pharmacists. In Scotland, a strategy doc- shortages. If dispensing is to remain the responsibil-ument entitled The Right Medicine[1] was published ity of community pharmacists, then an expansion inbefore the new contract was introduced. It outlined the community pharmacy workforce will be re-the framework for these new community pharmacy quired to deliver these new services. Policies toroles. The document included 59 actions relating to improve recruitment and retention depend on im-pharmacy, which were split into themes relating to proving the relative attractiveness of communitygovernment healthcare priorities for improving ac- pharmacy. To do this requires evidence on the rela-cess, helping patients make better use of their tive importance of different aspects of the communi-medicines, service re-design to improve health, and ty pharmacy role.partnership with staff. The work reported here was part of a larger study
The new roles for community pharmacists em- examining evidence-based options for the remuner-phasise their place as a key primary care and public ation of the new community pharmacy contract inhealth provider with specialist knowledge of the Scotland,[6] which included analysis of policy docu-effectiveness of pharmaceuticals. As a primary care mentation; focus groups and interviews; and nation-provider, a community pharmacist’s new role in- al community pharmacy and public surveys. Thecludes clinical monitoring, needle exchange, metha- aim of this work was to use a discrete choice exper-done supervision, emergency hormonal contracep- iement (DCE) to examine the strength of preferencetion, pharmacist prescribing, domiciliary visits, of community pharmacists for existing and newpharmaceutical care initiatives for older people and roles, as defined by a number of job characteristics.schemes for supporting carers. As specialists on the The DCE formed part of the national communityeffectiveness of pharmaceuticals, community phar- pharmacy survey in Scotland.[7]
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (9)

Pharmacists’ Preferences for Extended Roles 785
Methods bute and other attributes can be used to obtain wel-fare estimates of the respondents’ willingness topay/accept compensation to have more or less of aDiscrete Choice Experiments (DCEs)particular attribute. This is given as the ratio of the
DCEs are being used within health economics monetary and non-monetary regression coefficients.(and in environmental and transport economics) as a The implied trade-offs between job characteristicsmethod of establishing the relative strength of pref- are used to calculate the amount of income thaterence for goods and services.[8-10] The method is pharmacists would need to be compensated for (orgrounded in random utility theory, where a discrete need to give up) to provide more (or less) of thechoice is offered and respondents choose the option specific service. This is particularly relevant whenwith the highest utility. In the context of this study, it assessing the relative importance of attributes in ais pharmacists’ preferences over different job pack- common metric and in estimating the overall will-ages that are of interest. ingness to pay of a specific combination of attributes
Since this method is based on the empirical esti- making up the healthcare service. The ratio of coef-mation of a utility function, regression coefficients ficients can be interpreted as an implicit ‘price’ forrepresent the marginal utility of attributes, and the the service; the lack of accurate prices is a problem,ratios of coefficients represent their marginal rates as prices convey information about the strength ofof substitution. Pharmacists are assumed to be individuals’ preferences for these goods and ser-choosing a job in which to work. It is assumed that vices. Although some pharmacists already receivethe utility function (U) is defined over bundles of job payment for some new services, the low level ofcharacteristics (z), with each bundle representing a provision of some services suggests that the currentjob offer. The alternatives in the choice set are price does not reflect adequate compensation. Themutually exclusive, with z exogenous at the time the DCE derives prices that reflect more closely thechoice is made. The utility function is an indirect preferences of pharmacists for various aspects ofutility function, i.e. given the constraints on choice their job.and therefore the alternatives in the feasible choiceset, which bundle of job characteristics maximises Questionnaire Designutility. With two jobs, i and j, a pharmacist willchoose job j if (equation 1): Our survey was conducted in Scotland. There-
fore, we focused on aspects of The Right MedicineUj (z j, s) > Ui (zi, s)that outline new roles for community pharmacists in(Eq. 1)Scotland.[1] Job characteristics included in each sce-and if U* is positive, where (equation 2):nario were chosen on the basis of those aspects of
U* = (z j, s) – (z i, s) recent policy documents that were important to(Eq. 2) community pharmacists, according to information
i.e. the difference in utility between jobs i and j, with from focus groups and interviews. Interviews ands representing personal and socio-economic charac- focus groups addressed a range of perspectives asso-teristics of the pharmacist. Using random utility ciated with extended pharmacy roles and their con-theory, the indirect utility of each job is given by tractual implications. Thirteen interviews were heldequation 3: with a purposive sample of opinion leaders. Three
U ε εi = Vi + i and Uj = Vj + j focus groups were held in Edinburgh, Glasgow and(Eq. 3) Elgin and were attended by 25 community pharma-
where V = ƒ(z,s) and is the deterministic component cists. It was not possible to include all aspects of Theof utility, and ε is the random component. Right Medicine, since DCEs can only have a limited
Where a price or cost attribute is included in z, number of attributes. Realistic levels for each jobthe marginal rate of substitution between this attri- characteristic were assigned to each attribute (see
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (9)

786 Scott et al.
Table I. Attributes and levels for the discrete choice experiment
The pharmacy teamBasic: you and counter assistantsa
Extended: ‘basic’ plus medicines counter assistants and regular locumsComprehensive: ‘extended’ plus other pharmacists and technicians, and access to other health professionals
Medication reviewNoneIn GP surgeriesb
In the pharmacy
Change in annual income (the change in your own annual income, after tax and other costs)No change+10%+20%
Repeat dispensingc and chronic disease managementNoneSimple repeat dispensingRepeat dispensing plus chronic disease management
Change in the number of prescriptions dispensed per monthNo change–10%+10%
Integration and links with primary and secondary care (e.g. information technology, paper-based systems, access to patientrecords, good relationships)MinimalSome formal linksFully integrated
Minor illnessd and health promotion advice (including pharmacist prescribing for minor illness, and counselling on lifestyle,smoking, contraception, etc.)NoneMinor illness adviceMinor illness and health promotion advice
a ‘Counter assistants’ refers to ‘retail sales assistants’ who have no pharmacist-related duties.
b GP surgeries refers to a GP’s consulting rooms/offices.
c ‘Repeat dispensing’ is the dispensing of multiple prescriptions to a patient.
d ‘Minor illness’ is defined as minor health conditions that patients do not consider serious enough to require a visit to their GP.
table I). These were agreed by consensus within the The constant scenario did not represent any par-ticular combination of attribute levels (i.e. the ‘cur-research team, which included health economistsrent’ situation), although it was important that theand pharmacists with recent practice and strategicpairing satisfied the statistical properties of the de-management involvement.sign, discussed below. The pairs were then divided
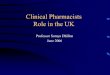
The scenarios were organised into pairs (see fig- across three versions of the questionnaire, as a highure 1 for an example). If all combinations of attri- number of choices may lead to respondent fatigue.bute levels had been used, it would have resulted in Each questionnaire therefore contained six pairs ofa full factorial design of 2187 possible scenarios. scenarios (i.e. so that the results did not depend onWe reduced this to a more manageable level of 18 the way the scenarios were paired).[11,12]
scenarios by using a fractional factorial experimen- The three statistical properties of orthogonality,tal design. These were then placed in pairs by having level balance and minimal overlap were examined.a constant scenario paired with every other scenario. Orthogonality was assessed by examining the corre-With the high number of attributes, this made the lations between attribute differences across all sce-choices easier to understand and also helped to narios. Level balance was assessed by checking themaintain the statistical properties of the design. frequencies of the levels of each attribute for all
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (9)

Pharmacists’ Preferences for Extended Roles 787
scenarios. Minimal overlap was assessed by deter- cies randomly selected from the list of all registeredmining the number of attribute differences that were premises in Scotland. The letter of invitation wasequal to zero. The design property of utility balance addressed to the pharmacy manager, and a secondwas not examined given that a priori the utility of letter and form were included to pass on to a secondeach scenario was not known. We tested the face pharmacist or locum working in the same premises.and content validity of the questionnaire in the pilot The decision to run two pilots resulted from a slowof the main questionnaire survey.[13] response to the first pilot, and a decision to reformat
the questionnaire. As a result of the pilot surveys,The questionnaire also included information onminor changes were made to the questionnaire torespondent demography (personal and pharmacy),facilitate completion and remove or clarify ques-workload and attitudes to and satisfaction with Thetions poorly answered.Right Medicine recommendations. It also included
respondents’ current involvement with, and work- The sample for the main mailing was identifiedload related to, the key new service areas. The by telephone calls made to all 1035 registered com-questionnaire was pre-piloted on six pharmacists, munity pharmacies in Scotland; the name of thetwo from each of the three focus groups. Two ver- pharmacist in charge was recorded, plus the namessions of the pilot questionnaire were tested in two of any other pharmacists working in those premisesseparate sub-samples from 50 community pharma- as ‘second’, part-time or locum pharmacists. During
Imagine that in the future you are looking for a new position and have been offered two jobs, A and B. You have negotiated terms and conditions.
For some new roles below, assume that you have been trained.In each of the 6 questions on the next page, you are asked to choose which job you prefer.
When answering the six questions on the next page:• assume all other characteristics are the same between jobs• answer all choices − assume that these are the only options available to you• there are no right or wrong answers• job A is the same for all six questions, and job B is different
The team in the pharmacy
Medication review
Change in annual income
Repeat dispensing and chronic disease management
Change in the number of scripts dispensed per month
Integration and links with primary and secondary care
Minor illness and health promotion
Extended
None
No change
Repeat dispensing plus chronic diseasemanagement
No change
Some formal links
Minor illness
Extended
In the GP's surgery
+20%
Simple repeatdispensing
No change
Fully integrated
Minor illness andhealth promotion
Q48. Which job would you prefer? Job A Job B
Tick one box only Prefer job A Prefer job B
Fig. 1. An example of a paired scenario used in the discrete choice experiment.
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (9)

788 Scott et al.
this phone call, the opportunity was taken to explain sating wage differentials suggests that, in a welland stress the importance of the project, and to functioning labour market, the wage rate (the priceencourage participation. The final questionnaire was of labour) incorporates the value of all the advan-mailed in mid-April 2003. The survey was anony- tages and disadvantages of work.[14] Undesirablemous, and responders were identified by the mailing jobs, or jobs located in geographical areas with poorof a separate identifiable reply-paid card, confirm- amenities, will require higher wages to attract anding they had completed and returned the question- retain workers. Relatively lower wages will be re-naire. Reminders, together with a further copy of the quired for more desirable jobs or those in morequestionnaire, were sent to non-responders after 4 desirable geographical areas. Workers in undesir-and 8 weeks. able jobs will need to be compensated to accept the
undesirable features; if not, they will take other jobsThe questionnaires were produced in an opticallyin a competitive labour market. Workers in morereadable format and respondent data were automati-desirable jobs will be willing to pay or forgo some ofcally coded and scanned into an ‘Eyes and Hands’their wage to have a desirable job or to work indatabase, then exported to SPSS version 11 fordesirable geographical area. The amount for whichWindows.they will need to be compensated or will be preparedto forgo is the compensating wage differential.Analysis
In the DCE, these compensating wage differen-A probit regression model was used to analyse tials were the trade-offs between each job character-
the data; the dependent variable was binary, whether istic and income, and were quantified by dividingthe respondent chose job A or job B. Explanatory each regression coefficient by the regression coeffi-variables were the differences between the levels of cient for income. This gave the equivalent amountseach job characteristic. Attributes with categorical of income that respondents were prepared to give uplevels were coded as dummy variables in the regres- or accept for a change in the level of another charac-sion analysis, relative to the level appearing in sce- teristic, and indicated the relative importance ofnario A. A random effects probit model was used to each job characteristic. Confidence intervals for theaccount for the potential correlation in responses ratio of these coefficients were calculated usingbetween the six choices completed by each respon- Fieller’s theorem. This is more appropriate thandent. This included the seven main job characteris- using a Taylor series expansion as it accounts for thetics. potential skewness of the sampling distribution of
The approach used for estimating the monetary the ratio estimator.[15]
value of each job characteristic followed exactly theResultssame methods used in DCEs that produce welfare
estimates (willingness to pay) from patients’ prefer-ences for attributes of healthcare services. This ap- Sample Characteristicsproach is based on estimating the marginal rate of
An overall response rate of 56.4% (914/1621)substitution between each characteristic and thewas achieved.[1] The sample was broadly representa-price of the good or service. What differs in thistive in terms of age, gender and health board area ofstudy is the definition of the price proxy. Our ‘cost’all community pharmacists in Scotland.[7]or ‘price’ attribute is defined as the change in annual
income, which is used as a proxy for wages; this The mean age of respondents was 39.9 yearsrepresents the ‘price’ of labour being supplied.[10] (range 21–84 years); 61.5% were women and 38.5%This has a strong theoretical justification in labour were men. Nearly 15% held a post-graduate qualifi-economics, just as the marginal rate of substitution cation. Self-employed pharmacists made up 32.7%has a strong theoretical justification in consumer of the respondents, 65.6% were employee pharma-theory. In labour economics, the theory of compen- cists and 1.7% were other types of pharmacists.
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (9)

Pharmacists’ Preferences for Extended Roles 789
Most respondents (40.8%) worked for large multi- to undertake medication review in GP surgeriesples (>31 stores), 25.7% worked in small chains (p = 0.007), and would need to be compensated(2–10 stores) and 23.1% worked in independent £728 to do so.single outlets. The remaining 2.1% were in health Repeat dispensing and chronic disease manage-centres or worked as locums. Organisations classed ment were not statistically significant predictors ofas medium chains (11–30 stores) employed 8.3% of job choice. Repeat dispensing plus chronic diseasethe sample. Almost 52% of pharmacists described management was preferred to no repeat dispensing,themselves as managers and 18.6% as owners. The and simple repeat dispensing was preferred to repeatmajority of the sample (62.1%) reported a personal dispensing plus chronic disease management.net income in 2003 of £20 000–39 999 and 21.3% Strong integration and links with primary andreported a personal income of £10 000–19 999 (183 secondary care was preferred to minimal integrationrespondents did not answer this question). and links. Pharmacists would be prepared to forgo
£2183 of additional income to work in a pharmacyDCE Results with some integration compared with minimal, and
would be prepared to forgo £1372 of additionalThe three statistical properties of the experimen- income to work in a pharmacy that was fully inte-
tal design (orthogonality, level balance and minimal grated compared with a pharmacy with only someoverlap) were all satisfied. Correlations between integration.attributes were all <0.1 and not statistically signifi- Community pharmacists preferred to provide mi-cant. The design ensured that attribute levels ap- nor illness services compared with no minor illnesspeared with equal frequency. In terms of minimal or health promotion advice. They would be preparedoverlap, an attribute difference is defined as the to forgo £2798 of additional income to work in alevel of the first attribute in Job B minus the level of pharmacy that provides minor illness advice. How-the first attribute in Job A. In total, there were seven ever, providing health promotion advice was notattribute differences in each of the 18 discrete significantly related to job choice. Pharmacists pre-choices, giving 126 attribute differences. Of these, ferred to provide only minor illness advice.only six were equal to zero. This was the minimum The pharmacists significantly preferred more in-number of zeroes given the choice of the constant come to less. The number of prescriptions dispensedscenario (scenario A). per month was not a significant predictor of job
The results from the DCE are shown in table II. choice. This can be explained by the fact that theMonetary values are presented in terms of net pay- number of prescriptions would be valued for theirments in 2003 per year. Pharmacists preferred an ex- effect on income, but since we have controlled fortended pharmacy team to a basic team (p < 0.001); income, the number of scripts is not significant bythey would be willing to forgo an increase in net itself. The negative sign indicates that pharmacistsincome of £3443 to work in a pharmacy with an prefer fewer scripts per month; this may have beenextended team. This was the most important job interpreted as an indicator of workload.characteristic with the largest monetary value. Phar-macists preferred an extended team to a comprehen- Discussionsive team, although this was not statistically signifi-cant and therefore did not influence job choice The results from this study show that community(p = 0.94). pharmacists seem to place the highest value on
The pharmacists preferred to undertake medica- organisational aspects of work, such as having antion review in the pharmacy premises compared extended pharmacy team and integration with pri-with not doing a medication review, although this mary and secondary care, rather than on the includedwas not a statistically significant factor influencing services from The Right Medicine. Stronger linksjob choice (p = 0.15). Pharmacists would prefer not with the NHS may be expressing a preference to be
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (9)

790 Scott et al.
Table II. Results of the discrete choice experiment
Explanatory variable Regression coefficient Monetary value of job characteristics(t ratio) [£, 2003 values] (95% CI)a,b
Basic pharmacy team –0.557 (–11.21)* –3443 (–6912, 27)(compared with an extended team)
Comprehensive pharmacy team –0.030 (–0.56) –177 (–677, 323)(compared with an extended team)
Medication review in GP surgeries –0.118 (–2.44)* –728 (–1567, 111)(compared with no medication review)
Medication review in pharmacy premises 0.060 (1.00) 381 (–262, 1024)(compared with no medication review)
Percentage change in annual income 0.061 (18.55)*
No repeat dispensing –0.0008 (–0.02) –10 (–423, 403)(compared with repeat dispensing and chronic disease management)
Simple repeat dispensing 0.047 (0.84) 294 (–269, 857)(compared with repeat dispensing and chronic disease management)
Percentage change in the number of prescriptions –0.002 (–0.8) –0.02 (–0.06, 0.02) per 1%dispensed per month increase in the number of
prescriptions per month
Minimal formal integration with primary and secondary care –0.355 (–6.06)* –2183 (–4425, 58)(compared with some integration)
Fully integrated with primary and secondary care 0.221 (4.17)* 1372 (–74, 2189)(compared with some integration)
No minor illness or health promotion advice –0.456 (–6.19)* –2798 (–5644, –47)(compared with minor illness advice only)
Minor illness and health promotion advice –0.077 (–1.29) –465 (–930, 0.30)(compared with minor illness advice only)
Constant 0.015 (0.19)
Rho (SE)c 0.191 (9.30)*
Log-likelihood –3128
Model Chi-square (12df) 617*
Number of individuals 881
Number of observations 5202
a Calculated using Fieller’s theorem (see Briggs and Gray[15]).
b Figures converted from percentages (i.e. unit of measurement of income variable) to £ using self-reported average net income(£37 727).
c This is a measure of the extent to which the six choices per respondent were correlated; this accounts for such correlation whencalculating standard errors.
Df = degrees of freedom; SE = standard error; * p < 0.001.
more integrated with primary and secondary care. itations included the slight over representation ofMinor illness advice is also highly valued, perhaps ‘middle aged’ (40–49 years) and under representa-reflecting a preference for a stronger first contact tion of ‘older’ (>60 years) pharmacists, and theprimary care role. For those job characteristics that unknown generalisability of the findings beyondwere statistically significant, the monetary values Scotland to the UK and wider.suggest a set of implicit prices that can be inter- Given a priori expectations, the results of thepreted as the amount of remuneration for each job study are plausible and support the theoretical valid-characteristic. ity of the technique; DCEs have generally been
The study had several strengths and limitations, shown to be reliable and valid, although this doesmost of which related to the survey. These have depend on the context.[9] However, the choicesbeen fully detailed in a previous publication.[7] Lim- presented to the pharmacists were hypothetical, and
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (9)

Pharmacists’ Preferences for Extended Roles 791
further research needs to compare these results with suggested in The Right Medicine is unlikely to occurresults based on actual behaviour. Nevertheless, the unless accompanied by organisational reform.hypothetical nature of the exercise has its advan-tages over using actual data, as the researcher has Acknowledgementscomplete control over the experimental design andthis ensures statistical robustness. This study was funded by the Scottish Pharmaceutical
General Council (SPGC) Research Trust. The research wasThe identification and inclusion of most attrib-conducted whilst Anthony Scott was at the Health Economicsutes was motivated by policies and ways of workingResearch Unit (HERN). HERN is funded by the Chief Scien-for pharmacists that do not yet exist; attributes are tists Office of the Scottish Executive Health Department. The
usually included based on what is already known to authors thank Verity Watson for assistance with the design ofbe important to respondents. Therefore, it is perhaps the experiment and two anonymous referees for helpful com-
ments. The views in this paper are those of the authors and notnot surprising that some variables were not statisti-the SPGC or the Scottish Executive. Christine Bond hascally significant.received two separate unrestricted research grants from the
Two studies have suggested that monetary values SPGC. The authors have no other conflicts of interest tofrom DCEs are sensitive to the range of monetary declare.attributes included in the choices.[16,17] There is alsosome debate in the literature about the appropriate
Referencesestimation of willingness to pay using DCEs.[18-21]1. Scottish Executive. The right medicine: a strategy for pharma-
However, this only seems relevant where the aggre- ceutical care in Scotland. Edinburgh: Scottish Executive, 20012. Department of Health. Pharmacy in the future: a vision forgate willingness to pay for a specific bundle of
pharmacy in the new NHS. London: Department of Health,attributes (aggregate expected compensating varia- 2000tion) is of interest, or where a change in an attribute 3. Welsh Assembly Government. Remedies for success: a strategy
for pharmacy in Wales. Cardiff: Welsh Assembly Govern-is likely to alter the probability of choosing anment, 2002
alternative. These issues were less relevant to this 4. Bond CM, Laing A, McKee L, et al. Evolution and change incommunity pharmacy. Aberdeen: Community Pharmacy Re-paper, which was focussed on marginal willingnesssearch Consortium, 2003to pay for individual attributes and where a discrete
5. Hassell K. Contemporary workforce patterns and historicalchange in an attribute was unlikely to alter the trends: the pharmacy labour market over the last forty years.
Pharm J 2002; 269 (7213): 291-6choice probabilities. A further issue is that some6. Bond C, Scott A, Inch J, et al. Examining alternatives for thestudies have suggested that respondents may not remuneration of community pharmacy: report to Scottish Phar-
maceutical General Council Research Trust. Aberdeen: Uni-‘trade-off’ attributes but use more simple decisionversity of Aberdeen, 2003heuristics.[22,23] These are important topics of ongo-
7. Inch J, Bond C, Lee A, et al. Scottish community pharmacists’ing research. The monetary values in this study current involvement in and attitudes towards ‘extended ser-
vice’ provision: a national survey. Int J Pharm Pract 2005; 13:should therefore be interpreted with these issues in289-301mind. 8. Ryan M, Farrar S. Eliciting preferences for health care usingconjoint analysis. BMJ 2000; 320: 1530-3
9. Ryan M, Gerard K. Using discrete choice experiments in healtheconomics: moving forward. In: Scott A, Maynard A, Elli-Conclusionott R. Advances in health economics. Wiley: Chichester, 2002
10. Scott A. Eliciting GPs’ preferences for pecuniary and non-pecuniary job characteristics. J Health Econ 2001: 20; 329-47Organisational issues seem more important to
11. Zwerina K, Huber J, Kuhfeld W. A general method for con-community pharmacists than the specific aspects of structing efficient choice designs. Durham (NC): Duke Uni-versity, 1996The Right Medicine included in the DCE. This result
12. Carlsson F, Martinsson P. Design techniques for stated prefer-is corroborated by the findings from the focusence methods in health economics. Health Econ 2003; 12:
groups.[13] Effective medication review and chronic 281-9413. Inch J, Bond C, Lee A, et al. Scottish Community Pharmacists’disease management cannot take place without
current involvement in and attitudes towards ’extended ser-strong links with the NHS or without an extended vice’ provision: a national survey. Int J Pharm Pract 2005; 13:team. The growth of specific service developments 289-301
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (9)

792 Scott et al.
14. Rosen S. The theory of equalising differences. In: Ashenfelter 20. Ryan M. Deriving welfare measures in discrete choice experi-O, Layard R, editors. Handbook of labour economics. Vol I. ments: a comment to Lancsar and Savage (1). Health Econ LettAmsterdam: North Holland, 1986: 641-92 2004; 13: 909-12
15. Briggs AH, Gray AM. Handling uncertainty when performing 21. Santos Silva JMC. Deriving welfare measures in discrete choiceeconomic evaluations of health care interventions. Health experiments: a comment to Lancsar and Savage (2). HealthTechnol Assess 1999; 3 (2): 1-134 Econ Lett 2004; 13: 913-8
16. Ratcliffe J. The use of conjoint analysis to elicit willingness to 22. Scott A. Identifying and analysing dominant preferences inpay: proceed with caution? Int J Technol Assess Health Care discrete choice experiments: an application in health care.2000; 16: 270-90 J Econom Psyc 2002; 23: 383-98
17. Skjoldborg US, Gyrd-Hansen D. Conjoint analysis: the cost23. Lloyd AJ. Threats to the estimation of benefit: are preferencevariable. An Achilles’ heel? Health Econ 2003; 12: 479-92
elicitation methods accurate? Health Econ 2003; 12: 393-40218. Lancsar E, Savage E. Deriving welfare measures from discretechoice experiments: inconsistency between current methodsand random utility and welfare theory. Health Econ Lett 2004; Correspondence: Professor Anthony Scott, Melbourne Insti-13: 901-7
tute of Applied Economic and Social Research, The Univer-19. Lancsar E, Savage E. Deriving welfare measures from discretesity of Melbourne, VIC 3010, Australia.choice experiments: a response to Ryan and Santos Silva.
Health Econ Lett 2004; 13: 919-24 E-mail: [email protected]
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (9)