CORRESPONDENCE* All letters must be typed with double spacing
and signed by all authors.
* No letter should be more than 400 words.
* For letters on scientific subjects we normally reserve our
correspondence columnsfor those relating to issues discussed
recently (within six weeks) in the BMJ.
* We do not routinely acknowledge letters. Please send a stamped
addressedenvelope ifyou would like an acknowledgment.
* Because we receive many more letters than we can publish we
may shorten thosewe do print, particularly when we receive several
on the same subject.
Abortion rates still risingSIR,-A recent report from the Office
ofPopulationCensuses and Surveys' has been widely quoted inthe
press,2 3and was reported by Ms Luisa Dillner,4as indicating that
the abortion rate has tripled inthe past 20 years in England and
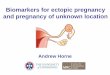
Wales. Detailedanalysis of these figures, however, shows
thatrequests for abortion have remained remarkablyconstant since
1972 (figure).The initial rapid rise from 3-5/1000 women aged
15-44 in 1968 (the first year when abortions werenotified) to a
level rate of 11 0/1000 in the 1970sprobably reflects the
increasing availability of legaltermination of pregnancy and
corresponds to adecrease in illegal abortion. Much of the
modestincrease since then (35%) can be explained bydemographic
changes rather than a profoundchange in women's requests for
abortion. Womenborn during the "baby boom" of 1960-5 reachedsexual
maturity during the 1980s, and hence alarger proportion of the
female population is at riskof unwanted pregnancy. The Office of
PopulationCensuses and Surveys calculated that becausethere has
been an increase in the proportion ofwomen aged between 16 and 29
(a group that has ahigher termination rate than older women)
withoutany change in the age specific termination rates thenumber
of terminations would have been expectedto increase by 14% between
1972 and 1989.The remaining increase is likely to be due mainly
to a gradual change in the attitudes of doctors,and particularly
gynaecologists, to therapeuticabortion in certain parts of the
country. In Scotlandthere were appreciable regional differences in
theabortion rate in 1972, with the rate in the westbeing half that
in the north and east. Though therates in the east and north have
remained fairlyconstant over the past 20 years (for example, thatin
Grampian), the rate in Greater Glasgow hasdoubled to reach the
national average. Thesedifferences probably reflect the influence
of two
X1 16 pEngland and14 / Wales(o)12 A ,c~~~~ c
E >rGlasgow (e)10 Grampiana(*)88d;/;96 so -'> W <
Scotand (o)
S6 *i
Z 21970 1974 1976 1980 1984 1988
Abortion rate among women aged 1544 in Grampianregion, Greater
Glasgow, Scotland, and England andWales, 1970-88*Figures for North
East Scotland Regional Hospital Board. tFiguresfor West ofScotland
Regional Hospital Board.
eminent senior gynaecologists. My father, SirDugald Baird, who
worked in Aberdeen, played animportant part in supporting the
change in theAbortion Law in 1967; Professor Ian Donald inGlasgow
was vehemently opposed to therapeuticabortion. Though religious and
social factors mayhave had some role, it seems unlikely that the
risein abortion rate in Glasgow is totally unrelated tothe retiral
of Professor Donald in 1976. Similarregional differences in
attitudes existed throughoutEngland and Wales, and hence the
increase in theabortion rate nationally probably reflects
thegradual levelling out of provision of abortionservices rather
than an increased resort to abortionas a means of controlling
fertility.A major factor determining the demand for
abortion is the provision of contraceptive services.The abortion
rate in Scotland (9-8/1000 womenin 1989) is lower than that in most
Europeancountries and less than one third that in the UnitedStates'
partly because contraception is widelyavailable to all sections of
the community from theNHS. Recent attempts by many health
authoritiesto limit the provision of "social" sterilisations andto
reduce budgets for family planning services maylead to a rise in
the incidence of unplanned andunwanted pregnancies. The consequent
increasein the demand for therapeutic abortion would bevery
undesirable at a personal level and would putincreasing strain on
medical services.
DAVID T BAIRDCentre for Reproductive Biology,Department ot
Obstetrics and Gynaccology,University of Edinburgh,Edinburgh EH3
9EW
I Office of lopulation Censuses and Surveys. 'I'rends in
abortion.In: Population trends 64. London: Government
StatisticalService, 1991:19-29.
2 Fletcher D. Abortion rate has trebled in 20 years. Daily
Telegraph1991 June 19:4(col 1).
3 Hunit L. Abortions on the increase. Independent 1991
June19:4(col ).
4 Dillner L. Abortion rates still rising. BMJ
1991;302:1559-60.(29 June.)
5 Henshaw SK. Induced abortion: a world review. FamilyPlanning
Perspecti'ves 1990;22:76-89.
Vital statistics of birthsSIR,-The measurement of maternal
mortalityis important enough that a minor point in DrGeoffrey
Chamberlain's excellent paper' deservesmention. The denominator for
maternal mortalityin a given year is either the total number of
birthsor the number of live births during that year, notthe number
of maternities-the term maternities isambiguous. The World Health
Organisation'sdefinition states that "A 'maternal death' is
definedas the death of a woman while pregnant or within42 days of
termination of pregnancy, irrespectiveof the duration and the site
of the pregnancy,
from any cause related to or aggravated by thepregnancy or its
management, but not fromaccidental or incidental causes" and goes
on tosay that "the denominator used for calculatingmaternal
mortality should be specified as eitherthe number of live births or
the total number ofbirths (live births plus fetal deaths). Where
bothdenominators are available, a calculation should bepublished
for each."2To allow for an extension of the period during
which deaths can be related to pregnancy or itsoutcome, the 1989
international conference for thetenth revision of the International
Classification ofDiseases introduced the concept of late
maternaldeath: "A 'late maternal death' is defined as thedeath of a
woman from direct or indirect obstetriccauses more than 42 days but
less than one yearafter the termination of pregnancy."2
Similarly, the conference has introduced theconcept of
"pregnancy related death" to permitclassification of deaths of
women while pregnantor when recently delivered, even though
localfacilities may not allow the cause of death to beidentified as
"related to or aggravated by thepregnancy or its management." A
pregnancyrelated death is thus defined as "the death of awoman
while pregnant or within 42 days oftermination of pregnancy,
irrespective of the causeof death." It. is likely, for instance,
that somehomicides and suicides of pregnant or recentlypregnant
women fall into this category, andaccidents may also be considered
in this light,in so far as fatigue or reduced mobility in
advancedpregnancy affects ability to avoid or
surviveaccidents.'
A C P' L'HOURSM C THURIAUX
Division ot Epidemiological Surveillance andHealth Situation and
Trend AssessmentStrengthening of Epidemiological andStatistical
Services,
World Health Organisation,1211 Geneva,Switzcrland
I Chamberlain G. Vital statistics of births. BMJ
1991;303:178-81.(20 July.)
2 International conference for the tenth revision of the
InternationalClassification of I)iseases, Geneva, 26 September-2
October1989. Wttrld Health Statistics Quarterly 1990;43:204-45.
3 Fortney JA. Implications of the ICD-I( definitions related
todeath in pregnancy, childbirth or the puerpwrium. WorldHealth
Statistics Quarterly 1990;43:246-8.
Nursing: an intellectual activitySIR,-For doctors to comment on
matters con-cerning nursing risks touching a raw nerve-the"doctor's
handmaiden" nerve-but the forthrightviews of June Clark, a
professor of nursing,deserve discussion.' Doctors and nurses need
each
BMJ VOLUME 303 7 SEPTEMBER 1991 579
other. They learn from each other. And if theydon't work well
together it's the patient whosuffers. Both professions ought to be
matureenough to discuss the problems of the other fromtime to time
without coming to blows over it.Our goals are surely the same.
Those listed by
Professor Clark are the goals of all health workers,not just of
nurses. Certainly you can't be a gooddoctor if you don't consider
the whole patient, asleaders of the medical profession like Lister
andOsler emphasised 100 years ago.
Secondly, I fear that many doctors will not behappy with either
of the suggested "two ways oflooking at nursing." Those who are
said to look atnursing in the first way (which is described asthe
more prevalent of the two perspectives) areaccused of believing
that nurses do not require anunderstanding of why a task is
necessary, how itworks, or what its effects will be. But
surelynobody thinks this. Anyone with a grain of sensewants each
member of a team to have as muchunderstanding as possible ofwhat is
being done fora patient. Why else should nurses have lecturesfrom
specialists explaining the thinking behinddifferent surgical and
medical treatments?As regards Professor Clark's second way of
looking at nursing, everyone will agree with muchof what she
says and with the progress towards aneven better trained,
understanding, and skilfulnursing profession. But it seems to me
that toachieve what she would apparently like to see forall nurses
(examining and history taking, thoughtprocesses identical with
those used in medicine,sophisticated cognitive and social skills,
and so on)would mean that every nurse would have to gothrough a
course of training very similar to that atmedical schools.We have
all known nurses who, had they chosen
to do so, could have sailed through medical schoolwith flying
colours. But there are many others-equally excellent and with
equally good skill andjudgment in many circumstances-who would
bethe first to agree that they could never compete orcope at this
intellectual level and wouldn't want to.It doesn't help patients or
anyone else to pretendotherwise. To be blunt, what is at stake
here, itseems to me, is the credibility of those leaders ofthe
nursing profession who brush reality under thecarpet and talk as if
all nurses were broadly thesame in this respect.
THURSTAN B BREWINBray,Berkshire SL6 2BQ
1 Clark J. Nursing: an intellectual activity. BMJ
1991;303:376-7.(17 August.)
SIR,-IS Professor June Clark suggesting that,though the thought
processes in nursing areidentical with those in medicine, nursing
alonefocuses on the "human response" and the "unique-ness of the
individual"?'
Perhaps she has a vision of care provided bya multidisciplinary
team led by nurses, withpsychologists providing counselling or
behaviouralmanagement for problems that the nurse doesnot have time
for and doctors available to signprescriptions and undertake manual
tasks such aspinning femurs and performing tracheostomies.When I
become helpless, whether from illness,
advancing years, or sheer rage, I hope that there willbe someone
in this multidisciplinary team to soothemy fevered brow and, more
importantly, to keepmeclean and dry, thus avoiding the bedsores
that seemso common.
S BRANDONUniversity of Leicester School of Medicine,Leicester
Royal Infirmary,PO Box 65,Leicester LE2 7LX
1 Clark J. Nursing: an intellectual activity. BMJ
1991;303:376-7.(17 August.)
SIR,-Professor June Clarke's editorial on nursinginterested me
as I am a qualified nurse as well as aqualified doctor. When I
decided on a career innursing I had only two 0 levels. Fortunately,
Ipassed the entrance exam and spent eight happyyears as a nurse. My
training was intense andstimulating and had a strong element of
discipline.I changed my profession not because I didn't
enjoynursing but because I was searching for a differentsort of
challenge.
I am saddened by the standards of nursing caretoday. Nurses no
longer have time to sit andprovide that all important emotional
support.They say that they are understaffed, but perhapsthey are
too busy writing care plans and evaluatingthe care that they have
been too busy to provide.
I agree that nursing requires a good intellect, butraising the
entry requirement means that some realnurses are excluded. After
all, had I applied 10years later to become a nurse I would not have
beenaccepted with my two meagre 0 levels. I believethat standards
are falling partly because of thisleaning towards academia. It is
difficult to see howa degree in nursing produces better nurses
whenthey spend more time in a classroom than atthe bedside. Of
course good clinical research isneeded, but not at the expense of
good nurseson the wards, where practical skills are vital.
If nurses want to be "clinical specialists" whydon't they change
professions like I did? Believeme, the grass is not greener on the
other side.
SALLY-ANN HAYWARDLondon NW6 3HP
I Clark J. Nursing: an intellectual activity. BMJ
1991;303:376-7.(17 Augist.)
SIR,-As I read Professor June Clark's editorial onrecognising
nursing's intellectual component' Ithought of the women who, on
several occasions,have promoted my "physical and mental
comfort,healing, and recovery" and wondered what theywould have
made of it. They would probably haveasked, "What on earth is she on
about?"
Years ago I watched a district nurse restore mybadly burnt 80
year old grandfather throughconvalescence to renewed self
confidence. A"considerable intellectual and emotional chal-lenge"?
She would have been mystified. She wassimply doing her job and
doing it superbly; and shewas not exceptional.The intellectual
component has always been
present, and recognised. But we didn't call it that.We called it
basic intelligence and common sense.To talk now of "coherent and
holistic care" and"extant definitions of quality care" is to use
theworst kind of academic jargon. Sadly, this is not anisolated
example-the whole article reeks of it.
I feel a sense of outrage on behalf of the womenwho nursed me,
some of whom became valuedfriends of the family. If I was a young
womanconsidering nursing today I would be frightened offby this
article. I am afraid that many will be.
KATHLEEN NORCROSSBirmingham B29 7JA
1 Clark J. Nursing: an intellectual activity. BMJ
1991;303:376-7.(17 August.)
HIV transmission duringsurgerySIR,-We should like to clarify
certain issuesraised by Dr A G Bird and colleagues.' Theseremarks
concern the case of the HIV infectedgynaecologist who agreed that
the 1000 patients hehad operated on should be contacted.
Letters were sent to patients in the three districts.They were
offered initial counselling by telephonehelpline and then
encouraged to attend for furthercounselling and discussion at
convenient centres.Alternative arrangements for counselling were
alsocatered for, including home visits for those unableto take time
off work or with transport difficulties,and an option of attending
their own generalpractitioner instead of the organised
counsellingsessions. The general practitioners had beenadvised
separately about the nature of the incident.No patients were
discouraged from having a
test, and the genitourinary clinics were used onlyfor
counselling and testing within one district,where other facilities
were not readily available.That many patients chose to have a test
aftercounselling was in part related to their level ofanxiety on
receipt of the letter. The role of thecounsellors was to offer
impartial information andnot to persuade or dissuade patients from
having atest.The Association of British Insurers, by recom-
mending a waiver note for patients taking the test,may have only
confused its prevailing message. InApril 1991 a "statement of
practice" was producedby the association, reiterating that a
negative HIVtest in the absence of lifestyle risk factors would
notjeopardise insurance premiums on any occasion. Awaiver notice
was therefore not strictly necessary,but the machinery to produce
this had in any casebeen put into operation well before the
eventsbecame public.Whereas it may be claimed that the exercise
illustrated could have been used to provide evengreater
epidemiological information, there is noevidence from the
evaluation of work carried outlocally in the health authorities of
any "collectivedenial" hindering epidemiological assessment.Indeed,
our objectives included acknowledgmentof the potential risk
(however small), sympatheticand confidential management of the
individualsconcerned, and delivery of unbiased and
correctinformation to the public.The success of the exercise cannot
be judged by
the level ofHIV testing achieved, but rather by thedissipation
of anxiety and uncertainty of all thoseinvolved.
S C CRAWSHAWR J WEST
West Suffolk Health Authority,Bury St Edmunds,Suffolk IP33 I
YJ
1 Bird AG, Gore SM, Leigh-Brown AJ, Carter DC. Escape
fromcollective denial: HIV transniission during surgery.
BMJ1991;303:351-2. (10 August.)
Guidelines for doctors with HIVinfectionSIR, -In
DrMichaelMorris'seditorialonAmericanlegislation on AIDS' the tired
old guidelines fromthe General Medical Council are repeated
yetagain: "It is unethical for physicians who know orbelieve
themselves to be infected with HIV toput patients at risk by
failing to seek appropriatecounselling or act upon it when
given."
This will not do. AIDS may eventually kill theunfortunate
surgeon who is HIV positive, but ifhe abandons his livelihood
poverty, loneliness,depression, and debt will kill him sooner.
Hisfamily surely have enough to cope with withoutlosing their house
and facing a mountain of debt.
If those eminent people who formulate suchguidelines truly
believe them then we must paythose whose counselling leads them to
give up theirprofession the full rate for the job they are
leaving.When the Ministry of Agriculture, Fisheries, andFood
destroys livestock to control an outbreak offoot and mouth disease
it pays the full market ratefor the animals it destroys, otherwise
the farmerswould not always cooperate. If we really want to
580 BMJ VOLUME 303 7 SEPTEMBER 1991