Embed Size (px)
Citation preview
PREGNANCY COMPLICATIONS Supplement
Symphysis pubis dysfunction: women’s experiences of care
By Vanda K Wellock and Margaret A Crichton
Epilepsy in pregnancyBy Sonji D Clarke
Acute fatty liver of pregnancyBy Katie Pateman, Patrick O’Brien
Tackling maternal obesity: suggestions for midwives
By Yana Richens
Caring for women with nausea and vomiting in pregnancy:
new approaches By Catherine McParlin, RH Graham and SC Robson
RESEARCH AND EDUCATION
Symphysis pubis dysfunction:women’s experiences of careBy Vanda K Wellock and Margaret A Crichton
Symphysis pubis dysfunction (SPD) is a distressing and painful condition that affects women during preg-nancy, labour and the early postpartum period. It is
defined as an abnormal stretching and instability of the pubic joint during pregnancy (Wellock, 2002), which often has an adverse effect on the sacro-iliac joints (Albert et al, 2002). This compromises women’s ability to carry out normal activi-ties of daily living, mainly due to pain.
Evidence has highlighted that women with SPD are dis-satisfied with the treatment they received from health care professionals (Hattersley, 2002; Akrigg, 2003; Whitby, 2003; Raheem, 2003). Some identified that the professionals had insufficient knowledge of the condition and were totally unsympathetic to their distress. Relatively little systematic research led to the investigation reported in this paper.
It is clear that the incidence of SPD varies considerably from 1:521 individuals to 1:20,000 (Boland, 1933; Perez, 1951; Lindsey et al, 1988) but these figures are not compa-rable since studies have taken place from the 1950s to 1990s, with different countries, varying cultures, health care systems and methods of data collection.
MethodologyIn order to achieve the aims of the research a qualitative methodology was employed, utilizing the phenomenological approach. This particular philosophical tradition was chosen in order to capture the ‘lived-in’ or ‘essence’ of the experience for each woman (Heidegger, 1975). The researchers favoured the Heideggerian approach to phenomenology since he did not favour ‘bracketing’ and stated that not using bracketing might be an advantage (Heidegger, 1962). Bracketing is to hold all preconceptions in abeyance, in order to reach the true essence of the phenomena and be faithful to the Husserlian concept of phenomenology (Koch, 1999). However this con-cept of not accepting bracketing concurs with other health care related research such as Taylor (1995). Taylor found that preconceptions about nursing practice would add to the body of knowledge rather than detract from it. The researchers in this study are midwives and by virtue of their experience would have certain preconceptions about normal midwifery which would aid understanding of the woman’s experiences. It could be argued that it has not biased the work, merely enhanced expression and helped the researchers understand what it feels like to ‘be in the world’ of women with SPD.
The descriptive rather than the interpretive method were chosen in order to capture exactly what the women said about the health care professionals.
Ethical approval was obtained from the Local Research Ethics Committee (LREC), the Research and Development Committee of the hospital and the University of Manchester Ethics Committee. Women were interviewed using a semi-structured interview schedule with open questions used throughout. The research question asked was:
‘What was your experience of the care offered by health care professionals throughout the experience of symphysis pubis dysfunction?’Three themes and several sub-themes were identified relat-
ing to women’s interactions with health care professionals.A detailed literature review, methodology and the theme of
pain can be found in Wellock and Crichton (2007).
SampleThe sample was purposive meaning that only women diag-nosed as having SPD were invited into the study (Holloway,
Vanda K Wellock is Family Nurse Supervisor, Kath Locke Centre, Hulme, Manchester and Margaret A Crichton is Lecturer in Midwifery & Nursing, School of Nursing, Midwifery and Social Work, University of ManchesterE-mail: [email protected]
AbstractThis paper explores the interaction between health care professionals and pregnant and newly delivered women, who have symphysis pubis dysfunction (SPD). The aim of this research was to identify women’s experiences of the care offered by health care professionals when they were diagnosed with SPD. Recent media coverage has suggested it is poor.A qualitative, phenomenological approach using semi-structured interviews was used so that women’s experiences with health care professionals could be told.The study was carried out in a large maternity hospital in the north-west of England. Twenty-eight women were interviewed at diagnosis of condition, 36 weeks gestation and 6 weeks postpartum.Three themes and four sub-themes were identified in the study relating to women’s interactions with their carers. Midwives, doctors and physiotherapists were the main carers highlighted. There were positive and negative comments in all cases. The sub-themes of pain, negative labelling, dismissive staff and feelings of dissatisfaction were expressed by most women.Women with SPD found that pain and the inability to perform the normal activities of daily living had a profound effect on them. Some women found that professionals lacked knowledge about how to manage their condition.
494 BRITISH JOURNAL OF MIDWIFERY, AUGUST 2007, VOL 15, NO 8

RESEARCH AND EDUCATION
1997). The women were referred by midwives or doctors to the physiotherapy department for clarification of diag-nosis. Twenty-eight women were recruited with no refusals or withdrawals. The interviews were carried out between March 2003 and February 2005. The women who agreed to participate were given an information sheet that outlined the study (The Gap Study) and a telephone number for the researchers so they could contact them if they had any questions. The researchers telephoned all interested women two days after diagnoses to arrange a time and date for interview. Written informed consent was obtained prior to each interview.
Data collectionData were collected using audio-taped in-depth interviews which took place in women’s homes. The interviews were scheduled at three designated points: initial diagnosis, 36 weeks gestation and 6 weeks post delivery.
The intention was to interview the women on three occasions. This was not always possible as many women were in hospital as a result of SPD and were unavailable for the 36th week interview. However three women were interviewed on all three occasions, seventeen twice and eight once. Eight women were seen only once because they had moved away from the area before the second and third observation points. This gave a total of 28 women inter-viewed at various points during the antenatal and postnatal periods, giving a pre- and post-view of the condition. The interviews lasted between 30 and 90 minutes, averaging at 60 minutes per woman. Numerical codes were assigned to each participant in order to maintain anonymity. Data on tapes was destroyed on completion of the study.
AnalysisThe interviews were transcribed verbatim. Analysis was informed by the phenomenological tradition using the Colaizzi method of analysis (Colaizzi, 1978). Colaizzi rec-ommends a ‘seven step’ approach.
An iterative approach identified emergent themes. These were explored in depth by the researchers.
ResultsThe theme discussed in this paper is women’s interaction with health care professionals. There were a range of positive and negative comments relating to each of the professionals mentioned. In-service training to midwives was delivered by the researchers to explain SPD, the symptoms and implica-tions for practice prior to the study. There was no formal policy at this time. Following training the midwives were required to refer any woman who complained of any of the symptoms of SPD to the physiotherapy department for confirmation of diagnosis and management.
Interaction with midwivesMany of the women commented that they had been well-supported by the midwives:
‘Midwives very supportive… usually they help you up and they get you off (the couch) which way you think best.’ (VM48)
‘They (midwives) all seemed really concerned…there wasn’t anything like, “don’t worry about it, it’s just general aches and pains”...I didn’t want to be a nuisance.’ (VM45)However, there were also some negative responses from
some of the women in relation to midwives appearing dis-missive. Some women tried to explain that the midwives did not have any interest in the symptoms:
‘I went to the midwife and she just poo poo’d me a little bit because she wasn’t my midwife from before...’ (VM44)Care in labour was mentioned by several of the women par-
ticularly in relation to the ‘pain-free’ gap between their knees. This is a tape measure assessment of the space between the knees, when abducted, that is pain free. Prior to any admission in labour, or with any other antenatal admission all women with SPD were advised by the physiotherapists to mention their condition to staff and further advised to measure the individual ‘pain-free’ gap between their knees in inches or centimetres when their knees were abducted. The women were also advised to remind husbands/partners to tell staff about this measurement so that when the women’s legs needed to be abducted, staff would know how far they could abduct, with-out causing difficulty and pain for the woman during vaginal examinations or when vaginal delivery occurred:
‘The midwife kept telling me to open my legs and my husband kept telling them, “no she can’t”, he was trying to keep my legs together and they were trying to pull them further apart’ (VM36)
‘I had to mention my SPD to them and to be honest, I didn’t feel they were taking an awful lot of notice… in half an hour I had a caesarean, so there’s not a lot of time to keep saying...oh by the way watch my leg.’ (VM1)
‘I had to tell them even though it was on my notes (SPD)… to be honest it didn’t feel like they were taking an awful lot of notice of it.’ (VM2)Several women with other medical conditions commented
that some midwives tended to view SPD as less of a priority in comparison to the other problem, however, the women were more used to their medical conditions and considered SPD to be a much bigger problem. Some of the conditions men-tioned in the study were hypertension, rhesus incompatibility and liver disorders. It appeared that midwives respond more effectively to conditions familiar to them but shy away from SPD. This was possibly due to lack of knowledge of the effects of the condition of SPD, lack of confidence or an inability to provide a treatment or a cure. One woman in the study felt that her hypertension was minor compared to her SPD, and thought that one condition could impact on the other. The following examples illustrate the women’s prioritization of the medical/obstetric conditions:
‘I think it (SPD) affects my hypertension and people don’t realise. I think when I’m in a lot of pain, I go (antenatal clinic) and my blood pressure is up and they go “oh, your BP is up etc”…I have a feeling it does go up when I’m in most pain.’ (VM19)
BRITISH JOURNAL OF MIDWIFERY, AUGUST 2007, VOL 15, NO 8 495
RESEARCH AND EDUCATION
‘…they (HCPs) are more concerned from the liver side than the SPD side...’ (VM 30)
‘...it’s more on the lines of…ehm…the rhesus antibodies side and it’s how you’re getting on with that…but it’s not affecting me and my SPD is…’ (VM32)
Interaction with doctorsGeneral Practitioners (GP) were not usually involved after confirmation of pregnancy. This was primarily because the women attended midwives or hospital antenatal clinics. Some women did need to see their GP during pregnancy because they had other concerns about themselves or their pregnancy. The women who approached their GPs with concern over SPD were met with mixed responses. It must be noted that the GPs had not had any briefing about the condition prior to the research. Some GPs did show support when approached:
‘Day by day it was getting worse, that is why the midwife at clinic told the doctor and he sent me to the physio’ (VM3)
‘GP very sympathetic, he said if you need a sick note, it’s no problem at all.’ (VM31)
‘I spoke to the GP, she referred me to the physio…it was SPD.’ (VM45)Most women however experienced negative responses
in relation to the pain experienced and the reason for that pain. The following example illustrates a doctors’ negative response to the woman’s pain:
‘I went to my GP and explained about the pain and she said, “if you’re in that much pain why don’t you go to Casualty?”... I was stuck inside all day… and I couldn’t move… and she said “are you getting depressed?” and I said, “well, I am depressed that you have dragged me all the way here”… the doctor was no good at all.’ (VM44)Such negative responses to their pain left women feeling
frustrated. As the pain increased women worried more, they made appointments with their GPs but several of them were told that the pain was normal in pregnancy and that they would have to put up with it until after delivery. However, the woman may not see it in the same way and may feel that the doctor did not understand their pain.
‘GP said that SPD was one of those things that will pass when you have had the baby … you just have to grin and bear it.’ (VM48)
‘He (GP] couldn’t understand what I meant … “no, no, no” he said and put it down that it was pain in my stomach… I read my notes and I thought I never mentioned pain in my stomach.’ (VM33)
‘I can’t find the words to express it [pain]… it hurts…I was taking a ridiculous amount of painkillers and that worried me...but they weren’t optional.’ (VM11)
‘The pain…it can be to a point where I don’t know what to do…you can’t even cry.’ (VM45)
Some of the women felt that a female GP would be more understanding and consequently decided to seek out a female GP in the hope of receiving more support.
In most cases this was actualised—they were better sup-ported, which is consistent with other research findings (Malterud, 1987).
‘Male GP thought it was part of pregnancy, the female GP was more sympathetic.’ (VM38) In comparison obstetricians were generally rated as being
more supportive and keen to refer the women to other pro-fessionals such as physiotherapists:
‘Whatever has happened in that hospital has been brilliant… they were keyed up to the fact that I had SPD.’ (VM13)There were a few cases where it appeared that hospi-
tal doctors did not understand the effects of SPD on the women. As a result confrontation occurred. One example expresses this well:
‘This doctor said, ‘‘other than SPD, are you coping?”… and something went inside me at the word coping and I was screaming at him… “if sitting on the kitchen floor at 3am with a knife in my hand thinking… if I put a cut in here, they will have to finish the job… and if that’s coping then I’m coping”… he had to go away and find someone to calm me down.’ (VM11)This woman was clearly very frustrated and distressed.
Some of the women in the Gap study felt that no one was lis-tening and no one really understood what they were experi-encing. So many women said in field notes that they wanted the researchers to publish the findings so that the health care professionals would know about the condition.
Interaction with physiotherapistsAll the women with symptoms of SPD were referred to the physiotherapy department. This is where the ‘pain’ was given a label and an explanation of the condition and management was given. As a result, many of the women felt that they had a name for the pain and were grateful to the physiotherapists. They reported positively in relation to the support they had received:
‘…think the world of (name of physio)…she gave advice…referred me to a pain clinic…and continues to be supportive’ (VM19)Unfortunately not everyone managed to get an appoint-
ment when they felt they most needed it. Many had to wait longer than two or three weeks and this had an effect on the way they viewed the service. Almost all the women com-plained to the researchers about the long wait. During this process many acknowledged that the department was busy but felt that the staff should have been able to improve the long waiting times:
‘…she said she could put me down for it (an appointment) …but there would be no point… by the time it came through…it would be too late…there is a long wait for appointments.’ (VM30)
‘…then I was referred to physio, which I thought I was never going to get…they said it would be about ten days to two weeks…I ‘phoned every day.’ (VM38)
496 BRITISH JOURNAL OF MIDWIFERY, AUGUST 2007, VOL 15, NO 8
RESEARCH AND EDUCATION
‘…it took a while to get the appointment…they said they were quite busy, so she got me a cancellation, but it was…let me see…about six weeks I think before I got the appointment’ (VM51)When the women finally got their appointments they were
under the impression that the condition would be remedied; many were disappointed:
‘…oh your referral…and you think they’ll do something but they can’t do anything…“if you’re not right in six weeks, contact your physio”…what they gonna do?’ (VM40)
‘…I mean the support I got from the physios was good but there is no knowing if there is nothing that anyone can do really…it’s quite…is very sort of...em…disheartening really.’ (VM39)Women with a history of SPD in previous pregnancy
(n=5) were already familiar with the system and knew how to make an appointment. In many cases they already knew the physiotherapist and made appointments with them directly:
‘…at 23 weeks I had a funny feeling…that came before the pain…the pelvic girdle felt higher on the left than the right…so I booked with the physio.’ (VM41)Not all the women were satisfied with the support they
received from the physiotherapy department, especially in terms of long term support:
‘The physio was probably testing my physical limits, well I was in agony for two weeks…she told me about wheelchairs and crutches and upset me…oh God I thought…that’s not me’ (VM44)
‘I have been following the physio’s instructions…but they are not helping, I have had a second referral because the pain has got worse since I last saw her.’ (VM45)The overall effect on the women in the Gap Study in rela-
tion to the care they received was one of disappointment. The women thought that the health care professionals would know about the condition and be able to help them. They found that this was not always the case.
DiscussionThe method chosen for this research was descriptive phe-nomenology. On reflection this was the ideal method that enabled the researchers to share with the women their expe-riences of care during pregnancy. The researchers decided to produce the actual accounts of the women so that health care professionals could see for themselves the impact this condition has on the pregnant women.
Pregnant women with SPD were shocked by the pain they experienced, it was so unexpected. Many arranged to see their health care professional and hoped they would find out what was happening to them and receive a label for what was wrong. This suggests an expectation that health care professionals will identify their pain and alleviate it. The relevance to midwives is that they have a responsibility to provide care/support to women throughout the course of childbirth (NMC, 2004).
The women in this study did not feel that their expecta-tions were met. Some felt that the midwives and doctors
were ignorant of the condition, dismissive of the pain and disinterested in what they had to say. Negativity was expressed by some health care professionals and mislabelling with other conditions occurred. Peters et al (1998) found that frustration occurred in women when a satisfactory explanation could not be given by the doctor. The concept of ‘labelling’ a condition or explaining a cause has been researched (Asbring and Narvanen, 2004). Often when a condition cannot be explained or understood as having an organic cause the doctor–patient relationship is in jeopardy (Chew-Graham and May, 1999). This latter aspect was also very apparent in the Asbring and Navanen (2004) study when they researched the power strategies between patients and doctors. In the Chew-Graham study there was a strong desire to show that they were ‘genuine’ sufferers and not ‘psychological cases’ (Chew-Graham and May, 1999:48). Asbring and Narvanen (2002) also found this was true in their work on chronic fatigue syndrome and fibromyalgia, conditions that have caused a degree of stigma prior to research and media coverage. This concept of having and explaining a ‘real pain’ was true of the women in the Gap study. The women needed an explanation for their pain and required a diagnosis so that they could confirm they had a problem. This feeling is particularly common in people with chronic illness; it is important to know what is wrong and to gain control over it (Malterud, 1993; Jerret, 1996; Peters et al, 1998; Asbring and Narvanen, 2004). Not only did they worry for themselves, they were pregnant and worried about their unborn child.
Requesting a change of carer represents an effort to gain the support required and in itself signifies dissatisfaction with the service received. Asbring and Narvanen (2004) call this behaviour ‘exiting’. This process is a way of trying to reduce dissatisfaction and take back control.
The lack of understanding displayed by some GPs frus-trated several women. They felt that the doctor was not really listening and some came away from the surgery feeling upset. Asbring and Narvanen (2004) point out that these women need to have their concerns taken seriously. When symptoms are ignored or inaccurately diagnosed, this may demonstrate lack of interest or lack of knowledge on the part of the doctor. One woman articulated that her doctor had put it down to a ‘mental thing’ caused by her pregnancy, which was a feeling echoed in other studies (Chew-Graham, 1999; Asbring and Navanen, 2002; 2004).
Asbring and Narvanen (2004) also found that in most cases confrontation surfaced because of sheer frustration and dissatisfaction.
The women felt that there was an over identification with pre-existing conditions such as hypertension. In the case of hypertension the women often had no obvious symptoms of the pre-existing condition, however, they felt that if it became worse it was because the SPD impacted on it and caused the problems. This was clearly demonstrated in the women’s narratives. However one could argue that the women may not have understood the importance of the existing condition.
The paucity of studies into SPD means that it is quite difficult to predict the care midwives could give to women.
BRITISH JOURNAL OF MIDWIFERY, AUGUST 2007, VOL 15, NO 8 497

RESEARCH AND EDUCATION
However midwives’ responsibility and sphere of practice is quite clearly outlined in Rule 6 of the NMC Midwives Rules and Standards and includes psychological support and advice (NMC, 2004). The findings of this study concur with the findings of Shepherd (2005). She found that some health care professionals were not very knowledgeable or sympathetic about women with SPD. Comparisons can however be made with other conditions that cause pelvic pain. Savidge et al (1998) found that the ways in which professionals related to women with pelvic pain was impor-tant. She found that it was important that women had the opportunity to describe their pain and its effect on their daily lives. Many of the women in the Gap study expressed the same feelings and some used the interview as an oppor-tunity to express their experience of pain.
This evidences that women with SPD need an opportu-nity to tell their stories. Some women felt that informing the researchers of their experiences was a catharsis in itself. If the health care professionals could be informed about the condition, it might be better managed. This was mentioned during several interviews and recorded in field notes. The fact that no formal complaints were made is in-keeping with results from a previous study on the experiences of care and how it is perceived by participants and family members (Atree, 2001).
The doctors approached by the women had not received in-service training but in most cases it was offered. They were informed that the study was taking place and that information was available if required. The women felt that some doctors lacked concern since they suggested that pain during pregnancy was normal. This trivialised their pain. The women needed a label for their pain and some valida-tion for what they were experiencing. The level of frustra-tion this aroused could often spill over and cause concern. The difficulties experienced by the women when trying to find a diagnosis for their pain and inability to mobilise has been demonstrated in a study by Peters et al (1998). In the Gap study it could have been interpreted that the doctor was rejecting the symptoms presented by the woman because other aspects of the pregnancy were considered more impor-tant than the pain of SPD (Salmon et al, 1999).
The women were pleased to be referred to the physi-otherapists because they felt something was being done. Unfortunately waiting times for appointments were often lengthy. When the appointment finally came, diagno-sis brought some relief. Some were disappointed since the treatment was not as successful as the women had expected or hoped it would be. In response to the docu-ment, ‘Choice, Responsiveness and Equity’ (Department of Health, 2003) a publication produced by the Chartered Society of Physiotherapists (CSP) (2003) re-iterated the professional status of physiotherapists and made recom-mendations for future practice. Among the suggestions for change that would be particularly useful for women with SPD was ‘self-referral’ to physiotherapy. This would ensure that women with problems would be able to access the specialist services of obstetric physiotherapists. The benefits are that women with suspected SPD could be assessed and managed at their antenatal appointments (Haynes, 2003).
In the hospital where the Gap Study took place, the referral system was reviewed and changed to try and meet the needs of women.
Like other health care professionals, physiotherapists have a duty of care, which was highlighted in a recently published document (Stenner, 2005). Physiotherapists must ensure that any intervention used is only to benefit the patient. In SPD this is difficult because protocols for man-agement are scarce but have been produced since the Gap Study finished.
The women freely gave their opinions to the research-ers. In fact the researchers felt that some could not wait to ‘tell all’ because someone was listening to them at last. There appeared to be total honesty and a very real wish to express how the condition impacted on their lives. Emotion displayed had a profound effect on the researchers as they became more aware of the extent of the situation.
In conclusion, more research into causation of SPD is required to find better methods of managing the condition. The most important aspect must be that all health care professionals are made aware of the condition and the effect that it can have on the lives of pregnant women. There can be no doubt that labelling the condition does help since this can validate the pain. What is evident is that some health care professionals need to be more accepting, sensitive and empathic to the needs of women with SPD. BJM
AcknowledgementsThe authors would like to thank the women who participated in this study for their patience and their time. The author’s would also like to thank Dr Margaret Chesney for her support and help in the writing of the article.
Akrigg L (2003) Having triplets left me crippled. Woman 23rd June: 53Albert HB, Godskesen M, Westergaard JG (2002) Incidence of Four Syndromes of Pregnancy-Related Pelvic Joint Pain. Spine 27(24): 2831–4Asbring P, Narvanen AL (2002) Women’s Experiences of Stigma in Relation toChronic Fatigue Syndrome & Fibromyalgia. Qualitative Health Research 12(2): 148–60Asbring P, Narvanen AL (2004) Patient Power & Control; A Study of Women with Uncertain Illness Trajectories. Qualitative Health Research 14(2): 226–40Atree M (2001) Patients and relatives experiences and perspectives of “Good” & “Not so good quality” care. Journal of Advanced Nursing 33(4): 456–66Boland BF (1933) Separation Of Symphysis Pubis. A report on ten cases occurring during delivery. New England Journal of Medicine 208(8): 431–8Chartered Society of Physiotherapists (CPS) (2003) Response to the Department of Health’s Consultation Paper. www.csp.org.uk/mediagovern-ment/government/westminsterandwhitehall/cspdocu (Accessed 26/04/07)Chew-Graham C, May C (1999) Chronic low back pain in General Practice: the challenge of the consultation. Family Practice 16(1): 46–9Colaizzi PF (1978) Psychological Research as the Phenomenologist Views it. In: Valle R, King M eds. Existential Phenomenological Alternatives for Psychology. Oxford University Press, OxfordDepartment of Health (2003) Choice, responsiveness and equity in the NHS & social care: a national consultation. HMSO, LondonHattersley L (2002) My body felt as if it was splitting in two. London Guardian 30th May: Health PageHaynes R (2003) Response to the Department of Health’s Consultation Paper: Choice, Responsiveness & Equity. Chartered Society of Physiotherapists, LondonHeidegger M (1975) The Basic problems of Phenomenology. Indiana University Press. USA. www.marxists.org/reference/subject/philosophy/works/ge/heidegge.htm (Accessed 07/06/2007)Heidegger M (1962) Being and Time. (Translated by Macquarrie J &
498 BRITISH JOURNAL OF MIDWIFERY, AUGUST 2007, VOL 15, NO 8

RESEARCH AND EDUCATION
Robinson E) Basil Blackwell Ltd, OxfordHolloway I. (1997) Basic concepts for qualitative research. Blackwell Science: Oxford.Jerret MD, Costello EA (1996) Gaining Control: Parent’s experiences of accommodating children’s asthma. Clinical Nursing Research 5(3): 294–308Koch T (1999) An interpretive research process: revisiting phenomenological and hermeneutical approaches. Nurse Researcher 6(3): 20–34Lindsey RW ,Leggon RE, WrightDJ, Nolasco MD.(1988) Separation of the symphysis pubis in association with childbearing. Journal of Bone Joint Surg Am. 70(2): 289-92 Malterud K (1987) Illness and disease in female patients.1. Pitfalls and Inadequacies of Primary Health Care. Scandinavian Journal of Primary Health Care 5(4): 205–9Malterud K (1993) Strategies for Empowering Women’s Voices in the Medical Culture. Health Care for Women International 14(4): 365–73Nursing & Midwifery Council (2004) Midwives Rules and Standards. NMC, LondonPerez ML (1951) Tratado de Obstetrica. edn 6. Lopez and Etchegoyen, Buenos Aries: 619–21Peters S, Stanley I, Rose M, Salmon P (1998) Patient’s with medically unexplained symptoms: sources of patient’s authority and implications for demands on medical care. Social Science and Medicine 46(4-5): 559–65Raheem D (2003) Pelvic joint dysfunction – a midwives story. The Practising Midwife 6(4): 17–19Salmon P, Peters S, Stanley I (1999) Patient’s perceptions of medical explana-tions for somatisation disorders: qualitative analysis. BMJ 318(7180): 372–6Savidge CJ, Slade P, Stewart P (1998) Women’s Perspectives of their Experiences of Chronic Pelvic Pain and Medical Care. Journal of Health Psychology 3(1): 103–16Shepherd J (2005) Symphysis pubis dysfunction: a hidden cause of morbidity. 13(5): 301–7
Stenner R (2005) Back pain – opportunity or threat? Physiotherapy 91(1): 62–3Taylor B (1995) Interpreting phenomenology for nursing research. Nurse Researcher 3(2): 66–79Wellock VK (2002) The ever widening gap-symphysis pubis dysfunction. British Journal of Midwifery 10(6): 348–53WellockVK, Crichton MA (2007) Understanding pregnant women’s experi-ences of symphysis pubis dysfunction: the effect of pain. Evidence Based Midwifery 5(2): 40–6Whitby P (2003) The agony of pelvic joint dysfunction. The Practising Midwife 6(4): 14–16
Key Pointsn SPD is a distressing and painful condition and women have
highlighted dissatisfaction with the care and support from health care professionals.
n Lack of knowledge by health care professionals can result in women feeling that dismissive staff did not understand the depth of their pain and suffering.
n More research is required in order to explore better methods of managing pain.
n Health care professionals need to be more knowledgeable, accepting, sensitive and empathic to the women’s very special needs.
BRITISH JOURNAL OF MIDWIFERY, AUGUST 2005, VOL 15, NO 8 499
Epilepsy in pregnancy
By Sonji D Clarke
Epilepsy affects 1 in 200 women of childbear-ing age and is therefore the most commonly encountered neurological condition in preg-
nancy. The importance of the condition for midwives and obstetricians lies, however, not in the fact that it is common, but that it is a recognized cause of maternal mortality as discussed by De Swiet in the report ‘Why Mothers Die’, (2004) and associated with significant perinatal morbidity. It is for these reasons that it is best managed with pre-conceptual counsel-ling and during pregnancy, using a multidisciplinary team approach, to achieve the best outcomes for both mother and baby.
What is epilepsy?Epilepsy is a condition characterized by seizure activ-ity. It may be classified in many different ways, but the following is a classification based on clinical pattern (Clarke, 2002):n Generalized: Bilateral abnormal electrical activity in the
brain, producing abnormal movement and impaired consciousness
n Absence seizuresn Myoclonic seizuresn Tonic clonic (grand-mal) seizuresn Tonic seizuresn Akinetic seizuresn Partial: Localized seizures owing to activity in a
small number of neurones in one brain hemisphere. Otherwise known as ‘focal’ seizures
n Simple partial seizures (without loss of consciousness (LOC))
n Complex partial seizures (with LOC)n Partial seizures evolving to generalized tonic clonic
seizuresn Unclassifiable: Seizures which do not fit into the above
categories.The most well known types of epilepsy are the tonic
clonic seizures, ‘petit mal’ and temporal lobe seizures with aura.
DiagnosisMore than 60% of diagnosed epilepsy is idiopathic. In the other 30–40% of people with a diagnosis of epi-lepsy, a number of underlying causes may be found:n Cerebrovascular diseasen Cerebral mass lesionsn Alcohol withdrawaln Previous cerebral trauman Antiphospholipid syndrome (Nelson-Piercy, 2006).
There is a hereditary component to epilepsy, as evi-denced by the fact that epilepsy can be found in the first degree relatives of 30% of people with epilepsy. There are also more than 200 genetic disorders that class epilepsy as one of the constellation of symptoms (Clarke, 2002).
A diagnosis of epilepsy will usually predate pregnancy, but if epilepsy is diagnosed in pregnancy, then the history given can be invaluable for establishing the diagnosis. It is preferable to have a witness because the person fitting would not be conscious and a witness can give an accu-rate description. Investigations to confirm the diagnosis should include:n Renal profile and serum uraten Calcium and liver function testsn Full blood count, clotting screen and blood film n Serum glucose levelsn Blood pressure and urinalysis n Electroencephalogram (EEG) and/or sleep studyn Computerized tomography (CT) scan/magnetic reso-
nance imaging (MRI).
Dr Sonji D Clarke is Consultant Obstetrician and Gynaecologist, Women’s Health, 10th Floor, North Wing, St Thomas’ Hospital, Lambeth Palace Road, London E-mail: [email protected]
AbstractEpilepsy affects 1 in 200 women of childbearing age and is a cause of maternal death. For the fetus and neonate, epilepsy is associated with a significant risk of major and minor congenital anomalies, related to the use of anti-convulsant medication. Recent guidance published by the National Institute for Clinical Excellence and recommendations from the CEMACH reports into maternal deaths and perinatal mortality, have clearly recommended the need for multi-disciplinary team management of these women during pregnancy and the need for pre-conceptual care and advice. There is a clear opportunity to reduce the risks to both mother and fetus if we embed these in our practice. The teratogenic potential of anti-convulsants is discussed, and the most recent recommendations for contraception for women with epilepsy, which apply to women pre-pregnancy and post delivery.
CLINICAL
740 BRITISH JOURNAL OF MIDWIFERY, DECEMBER 2007, VOL 15, NO 12

Differential diagnoses in pregnancyn Eclampsia (in women >20 weeks pregnant)n Cerebral vein thrombosisn Cerebrovascular accident (stroke/subarachnoid haem-
orrhage)n Gestational epilepsy (seizures in pregnancy only)n Pseudo-epilepsy (can be present with true epilepsy)n Rare infections (tuberculoma, toxoplasmosis, encepha-
litis)Fitting can be associated with biochemical derange-
ment, for example:n Hypoglycaemian Hyponatraemian hypocalcaemia n Drug or alcohol withdrawal.
Pre-conception counsellingThe National Institute for Health and Clinical Excellence (NICE) guidelines on epilepsy (2004) gave firm rec-ommendations regarding pre-conception counselling:. ‘Information (on epilepsy, its risks and management) should be given in advance of sexual activity or preg-nancy’. The Confidential Enquiry into Maternal and Child Health (CEMACH) recommendations in ‘Why Women Die 2000-2002’ (CEMACH, 2004) further stated that women with pregnancies complicated by medical conditions, like epilepsy, should have a multidisciplinary care pathway for optimized care. This should include an interested physician, neurologist or obstetric physician, together with an interested obstetrician and midwife or midwifery team.
In an ideal world, a woman with epilepsy would be referred to a multidisciplinary pre-conception clinic where the issues are clearly discussed, including the possibility of sudden unexplained death in epilepsy (SUDEP), as recommended by CEMACH and NICE (De Swiet, 2004; NICE, 2004). The issues can be divided into:n Contraceptionn Anti-epileptic drugs and the fetus/neonate/infantn Pregnancyn After-birth.
ContraceptionOur hope is that women will prepare for pregnancy and for women with epilepsy, this may mean using contracep-tion until medication is optimized. Advice should include taking folic acid 5 mg, once daily, at least 3 months before pregnancy and throughout the pregnancy once conception has taken place, because of the increased risk with some medications of neural tube defects. Contraception which is not recommended for women taking enzyme inducing drugs (Table 1) includes:n Progesterone only pilln Progesterone implant (implanon)n Emergency contraception may be given, but should be
given as a double first dose of levonogestrel (1.5 mg) followed by a single pill 12 hours later (750 mg)
(O’Brien and Gilmour-White, 2006). Previously it had been suggested that the administra-
tion interval between Depot medroxyprogesterone acetate (Depo- Provera) injections should be shortened from 12 weeks to 10 weeks, but the latest recommendations say this is not necessary (O’Brien and Gilmour-White, 2006). This differs from the guidelines published by NICE (2004) so they will need to be updated to reflect this. Furthermore, the Mirena intra-uterine system has not shown to be significantly affected by anti-epileptic drugs (AEDs) and can be recommended as effective contracep-tion (Bounds and Guillebaud, 2002).
The efficacy of the combined oral contraceptive pill (COCP) is also compromised in women taking AEDs, which are enzyme inducers. It is important, therefore, to advise women choosing the COCP to double the dose and/or tricycle (use the pill for three months and then have a pill-free interval) the COCP for best protection. Alternatively, women may be advised to have a shorter ‘pill-free’ interval of four days rather than seven (O’Brien and Gilmour-White, 2006; Harden and Leppik, 2006). Conversely, the effectiveness of lamotrigine in women taking the COCP is reduced, requiring an increase in the dose and checking of blood levels. Women should be advised to use a condom until the lamotrigine level is known to be in the therapeutic range.
While this information is important for planning preg-nancy at an appropriate time, it is also very important for women postpartum and who may be breastfeeding. Most progesterone only preparations (POPs) should not be recommended for contraception and alternative methods sought, although double-dose cerazette may be useful in this context (O’Brien and Gilmour-White, 2006; Harden and Leppik, 2006).
Anti-epileptic drugs (AEDs)One of the aims of pre-conception counselling is to keep women informed about the risks of AEDs to both mother and baby. They must be aware of the need to take pre-conceptual folic acid at a dose of 5 mg, once daily for 3 months, preferably before conception and throughout pregnancy, as they may be at higher risk of folate deficient anaemia (Nelson-Piercy, 2006). Women taking enzyme inducing drugs (Table 1) are advised to take vitamin K (10–20 mg once daily) from 36 weeks onwards, to prevent haemorrhagic disease of the new-born. Women should aim to optimize anticonvulsant therapy prior to pregnancy to achieve the best outcome
Phenytoin
Carbamazepine
Oxcarbazepine
Phenobarbitone
Primodone Not commonly used in women of child-bearing age
Topiramate Significant at drug levels >200 mg/day
Table 1. Enzyme inducing anti-epileptic drugs
CLINICAL
BRITISH JOURNAL OF MIDWIFERY, DECEMBER 2007, VOL 15, N0 12 741
for mother and child. The term ‘optimize’ is different for each individual, however:n Avoid polypharmacy: Aim for one drug to control
seizures as polypharmacy increases the risk of major and minor congenital anomalies (Morrow, 2006)
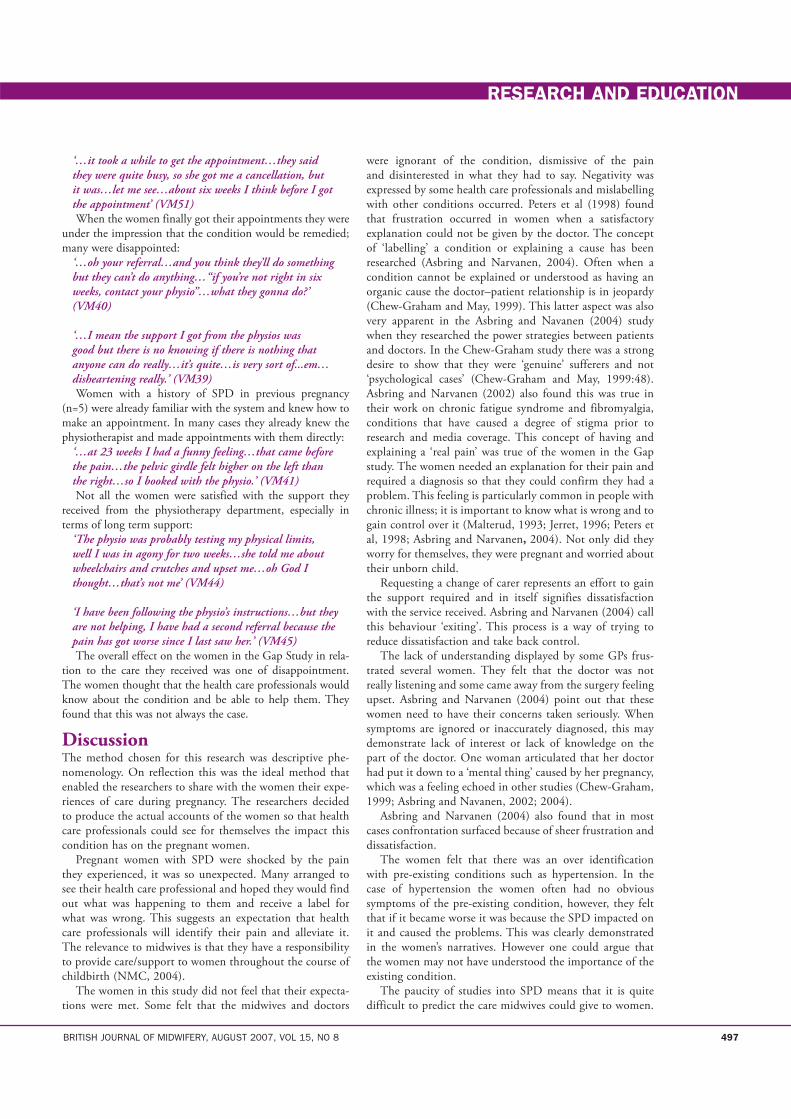
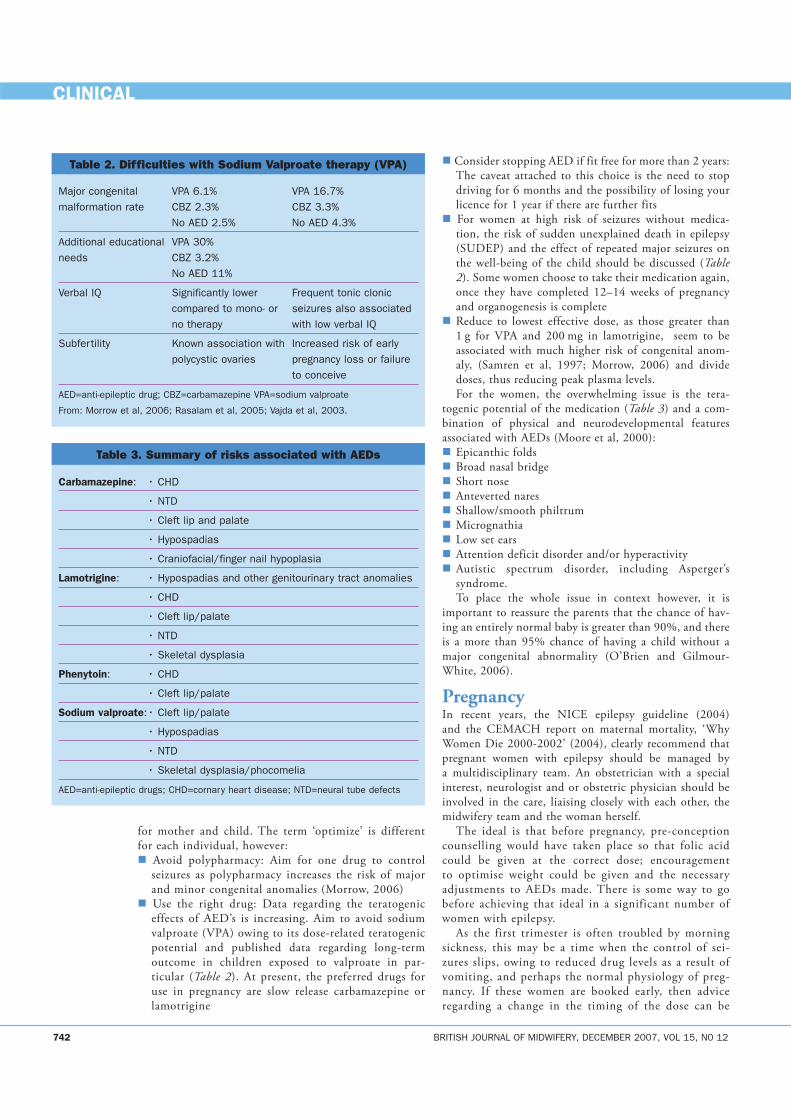
n Use the right drug: Data regarding the teratogenic effects of AED’s is increasing. Aim to avoid sodium valproate (VPA) owing to its dose-related teratogenic potential and published data regarding long-term outcome in children exposed to valproate in par-ticular (Table 2). At present, the preferred drugs for use in pregnancy are slow release carbamazepine or lamotrigine
n Consider stopping AED if fit free for more than 2 years: The caveat attached to this choice is the need to stop driving for 6 months and the possibility of losing your licence for 1 year if there are further fits
n For women at high risk of seizures without medica-tion, the risk of sudden unexplained death in epilepsy (SUDEP) and the effect of repeated major seizures on the well-being of the child should be discussed (Table 2). Some women choose to take their medication again, once they have completed 12–14 weeks of pregnancy and organogenesis is complete
n Reduce to lowest effective dose, as those greater than 1 g for VPA and 200 mg in lamotrigine, seem to be associated with much higher risk of congenital anom-aly, (Samren et al, 1997; Morrow, 2006) and divide doses, thus reducing peak plasma levels.For the women, the overwhelming issue is the tera-
togenic potential of the medication (Table 3) and a com-bination of physical and neurodevelopmental features associated with AEDs (Moore et al, 2000):n Epicanthic foldsn Broad nasal bridgen Short nosen Anteverted naresn Shallow/smooth philtrumn Micrognathian Low set earsn Attention deficit disorder and/or hyperactivityn Autistic spectrum disorder, including Asperger’s
syndrome.To place the whole issue in context however, it is
important to reassure the parents that the chance of hav-ing an entirely normal baby is greater than 90%, and there is a more than 95% chance of having a child without a major congenital abnormality (O’Brien and Gilmour-White, 2006).
PregnancyIn recent years, the NICE epilepsy guideline (2004) and the CEMACH report on maternal mortality, ‘Why Women Die 2000-2002’ (2004), clearly recommend that pregnant women with epilepsy should be managed by a multidisciplinary team. An obstetrician with a special interest, neurologist and or obstetric physician should be involved in the care, liaising closely with each other, the midwifery team and the woman herself.
The ideal is that before pregnancy, pre-conception counselling would have taken place so that folic acid could be given at the correct dose; encouragement to optimise weight could be given and the necessary adjustments to AEDs made. There is some way to go before achieving that ideal in a significant number of women with epilepsy.
As the first trimester is often troubled by morning sickness, this may be a time when the control of sei-zures slips, owing to reduced drug levels as a result of vomiting, and perhaps the normal physiology of preg-nancy. If these women are booked early, then advice regarding a change in the timing of the dose can be
Major congenital VPA 6.1% VPA 16.7%malformation rate CBZ 2.3% CBZ 3.3% No AED 2.5% No AED 4.3%
Additional educational VPA 30%needs CBZ 3.2% No AED 11%
Verbal IQ Significantly lower Frequent tonic clonic compared to mono- or seizures also associated no therapy with low verbal IQ
Subfertility Known association with Increased risk of early polycystic ovaries pregnancy loss or failure to conceive
AED=anti-epileptic drug; CBZ=carbamazepine VPA=sodium valproate
From: Morrow et al, 2006; Rasalam et al, 2005; Vajda et al, 2003.
Table 2. Difficulties with Sodium Valproate therapy (VPA)
Carbamazepine: • CHD
• NTD
• Cleft lip and palate
• Hypospadias
• Craniofacial/finger nail hypoplasia
Lamotrigine: • Hypospadias and other genitourinary tract anomalies
• CHD
• Cleft lip/palate
• NTD
• Skeletal dysplasia
Phenytoin: • CHD
• Cleft lip/palate
Sodium valproate: • Cleft lip/palate
• Hypospadias
• NTD
• Skeletal dysplasia/phocomelia
AED=anti-epileptic drugs; CHD=cornary heart disease; NTD=neural tube defects
Table 3. Summary of risks associated with AEDs
742 BRITISH JOURNAL OF MIDWIFERY, DECEMBER 2007, VOL 15, N0 12
CLINICAL

given and blood tests for therapeutic levels taken. The relevant scans can also be booked:n Nuchal translucency scann Fetal cardiology scann 20-week anomaly scan
Serial growth scans should not be necessary as growth restriction is not a feature in this group of women.
The partner and other family members should be taught about the use of the recovery position, should a major fit occur, and general instruction about keeping the door of the bathroom or toilet unlocked should be given. Showers rather than baths should be encouraged and if a bath is taken, shallow water should be used. A plan for prescribing vitamin K (phytomenodione) 10–20 mg daily, from 36 weeks until delivery, should be written in the notes of women taking enzyme inducing drugs (Table 1).
Labour is the most likely time to experience seizures (1–2%), with a further 1–2%, experiencing seizures in the following 24 hours (Nelson-Piercy, 2006). This is related to hyperventilation, dehydration, fatigue and reduced drug absorption from a slowed gastrointestinal motility time during labour.
A plan for labour may be written that involves the fol-lowing factors:n Epilepsy medication should be taken as normal during
labourn Woman should be accompanied throughout labour and
not left alone for 24 hours afterwardsn Seizures are usually self-limiting and may be managed
by attending to the woman’s safety and placing her in the recovery position with appropriate support
n Prolonged (>10 minutes) seizures can be curtailed using lorazepam 4 mg intravenous, diazemuls or rectal diazepam at a dose of 10–20 mg. Oxygen should also be administered by mask at this time
n Continuous electronic fetal monitoring should also be carried out, should a seizure occur.
n For women that have had previous seizures during labour, rectal carbamazepine or intravenous phenytoin or valproate may be administered to achieve adequate blood levels and reduce the risk of intrapartum sei-zures.It is expected that most women with epilepsy will
achieve a normal vaginal delivery and a caesarean should only take place for the normal obstetric indications.
Women who have epilepsy diagnosed for the first time in pregnancy should be prescribed lamotrigine or carbamazepine, because of the lower anomaly potential and the minimal effects on infant neurodevelopment. Certain types of epilepsy are best managed using sodium valproate, but the risks and benefits would need to be carefully discussed, depending on the gestation.
After the birthWomen with epilepsy should not be left unattended fol-lowing delivery. If the midwife is required to leave the room, a birthing partner should be advised to stay with the mother and shown the emergency bell for help, or a colleague asked to relieve her. The parents should be
encouraged to consent to the neonate being given vitamin K (phytomenodione), 1 mg intramuscularly, because of the risk of haemorrhagic disease of the newborn. Women with epilepsy should also be encouraged to breastfeed as the level of AEDs in breast milk is low (3–5% of the neonatal therapeutic dose), when compared to the levels, the neonate would have received while in utero (Nelson-Piercy, 2006). Lamotrigine does cross to the breast milk in significant amounts (30–50% of the dose), and breast milk allows careful weaning, reducing the risk of with-drawal symptoms (phenobarbitone).
For women whose medication was increased during pregnancy, careful reduction of the dose over some weeks should take place, apart from lamotrigine, which should be reduced quickly, i.e. within the first few days postpar-tum.
If the mother finds that feeding is not establishing well, because the baby is prone to sleepiness, she may be advised to feed the baby before taking her AED, thereby further reducing the effective dose the baby receives through the breast milk.
Practical advice to mothers following discharge should include:n Changing babies on the floor rather than on a high
surface n Bathing the baby in shallow water, or with someone
else presentn They should be discouraged from sleeping with the
baby in bed.
ConclusionsAppropriate contraception should be recommended and ideally discussed during the pregnancy. This allows the parents time to read and digest the information before a choice is made. The recent information regarding the combined oral contraceptive pill and its effect on breast milk has been modified to allow the combined pill in breastfeeding women, because most pills prescribed have a low oestrogen dose. This does not apply to women with epilepsy who are taking enzyme inducing drugs, and the combined pill also has an effect on the effective dose for lamotrigine, leading to a requirement for the dose to be increased. Depot progestogen and the Mirena intrauterine system may be promoted, because neither is affected by
CLINICAL
BRITISH JOURNAL OF MIDWIFERY, DECEMBER 2007, VOL 15, N0 12 743
Women with epilepsy should not be left unattended following delivery. If the midwife is required to leave the room, a bir thing par tner should be advised to stay with the mother and shown the emergency bell for help...
‘
’

the anticonvulsants and they do not affect breastfeeding.Awareness of the risks related to pregnancy and pre-
pregnancy counselling have the potential to make an enormous difference to the outcomes for both mother and infant. As health professionals, we should be aiming to develop this further, with the hope of seeing a significant reduction in congenital anomalies and neurodevelopmen-tal problems into childhood, as well as maternal harm. BJM
Bounds W, Guillebaud J (2002) Observational series on women using the contraceptive Mirena concurrently with anti-epileptic and other enzyme inducing drugs. J Fam Plann Reprod Health Care 28(2): 78–80Clarke C (2002) Neurological disease. In: Kumar P, Clarke M, eds. Clinical Medicine. Saunders, Edinburgh: 1123–224De Swiet M (2004) Other indirect deaths in: Confidential Enquiry into Maternal and Child Health, Why Mothers Die 2000-2002. RCOG Press, London: 183–96Harden CL, Leppik I (2006) Optimizing therapy of seizures in women who use oral contraceptives. Neurology 67(12 supp 4): s56–s58Moore SJ, Turnpenny P, Quinn A et al (2000) A clinical study of 57 children with fetal anticonvulsant syndromes. Journal of Medical Genetics 37(7): 489–98Morrow J, Russel A, Guthrie E et al (2006) Malformation risks of antiepileptic drugs in pregnancy: a prospective study from the UK Epilepsy and Pregnancy Register. Journal of Neurology, Neurosurgery and Psychiatry 77: 193–8National Institute for Health and Clinical Excellence (2004) Information for women with epilepsy. In: The diagnosis and management of the epilepsies in adults and children in primary and secondary care.
BRITISH JOURNAL OF MIDWIFERY, DECEMBER 2007, VOL 15, N0 12 745
CLINICAL
www.nice.org.uk/CG020fullguideline (accessed 7 November 2007)Nelson-Piercy C (2006) Neurological problems. In: Handbook of Obstetric Medicine 3rd edn Informa Healthcare Oxon: 169–95O’Brien MD, Gilmour-White SK (2005) Management of epilepsy in women. Postgraduate Medical Journal 81: 278–85O’Brien MD, Guillebaud J (2006) Critical Review: Contraception for Women with Epilepsy. Epilepsia 47(9): 1419–22Rasalam AD, Hailey H, Williams J et al (2005) Characteristics of fetal anticonvulsant syndrome associated autistic disorder. Developmental Medicine and Child Neurology 47(8): 551–6 Samren EB, Van Dujn CM, Hiilesmaa VK et al (1997) Maternal use of antiepileptic drugs in pregnancy and the risk of congenital malforma-tions. Epilepsia 38: 981–90Vajda FJ, O’Brien TJ, Hitchcock A, Graham J, Lander C (2003) The Australian registry of anti-epileptic drugs in pregnancy: Experience after 30 months. J Clinical Neuroscience 10(5): 543–9
Key Pointsn Pre-conception counselling is a very important part of the
management of women with epilepsy.n Careful attention to correct contraceptive prescribing, should
take place for women with epilepsy.n Polypharmacy should be avoided for women contemplating
pregnancyn Women with epilepsy should be managed by a multidisciplinary
team during pregnancy. n Alternatives to sodium valproate should be used where
possible to avoid its effects on the embryo, fetus, neonate and child.
Acute fatty liver of pregnancy
By Katie Pateman, Patrick O’Brien
Acute fatty liver of pregnancy (AFLP) is a rare condi-tion affecting women primarily in the third trimester of pregnancy, complicating 1 in 7 000 to 1 in 15 000
pregnancies (Nelson-Piercy, 2006). AFLP is potentially life-threatening to both mother and fetus; the maternal mortality rate is 18% and perinatal mortality 23% (Mjahed, 2006). The fetal outcome is poorer than maternal outcome (Knight, 2008).
Clinical featuresThis condition typically presents at around thirty weeks’ gestation (Ko, 2006) with generalized malaise, progressive nausea and vomiting (Nelson-Piercy, 2006; Knight, 2008). Abdominal pain (epigastric or right upper quadrant from the damaged liver) or jaundice can develop, occasionally with ascites. Proteinuria and hypertension are often present suggesting the possibility of pre-eclampsia (PE). AFLP must also be distinguished from HELLP syndrome (haemolysis, elevated liver enzymes and low platelets).
Disseminated intravascular coagulation (DIC) can com-plicate the condition and may be the presenting feature postpartum when it can cause excessive bleeding. Transient diabetes insipidus (DI) is sometimes associated with AFLP; liver cell damage impairs the degradation of vasopressinase (the enzyme responsible for the breakdown of anti-diuretic hormone), leading to the symptoms of DI: polydipsia and polyuria, i.e. great thirst associated with passing large volumes of very dilute urine (Kennedy, 1994). There is often renal impairment and the woman may go on to develop fulminant liver failure and hepatic encephalopathy, which may lead to confusion, coma and even death. There have been reports of women developing acute and chronic pancreatitis second-
ary to AFLP (Apiratpracha, 2008) but no documented case studies of AFLP affecting cranial nerves. Table 2 assists with the differential diagnosis of HELLP syndrome and AFLP (Nelson-Piercy, 2006).
PathogenesisAFLP may be considered a variant of pre-eclampsia in which the liver is predominantly affected. Liver histology shows fatty infiltration of liver cells (hepatocytes), particularly in the central zone, but with little or no inflammation or necrosis. (Nelson-Piercy, 2006).
Women carrying twins appear to be at increased risk of developing AFLP (Knight, 2006) and there also seems to be an association with some disorders of fat metabolism. Women whose fetus is homozygous for long-chain 3-hydroxyacyl-CoA dehydrogenase (LCHAD) are at increased risk of developing AFLP or HELLP syndrome (Ko, 2006; Nelson-Piercy, 2006). LCHAD is a disorder of fatty acid oxidation in the mito-chondria that can result in severe metabolic and neurological problems in the infant. The unmetabolised long-chain fatty acids enter the maternal circulation from the fetus, leading to an accumulation of these fatty acids in the liver. However, in many women with AFLP, no such metabolic disorder will be found.
Primigravid women and women with multiple pregnancies are more at risk of AFLP; in addition there is a suggestion that the risk of AFLP is inversely proportional to BMI (Knight, 2008).
DiagnosisLiver function tests are abnormal with a marked increase in the transaminases (ALT, AST)—the levels will often be in the hundreds or even thousands, compared with a normal value of less than 30. Clotting function can also be abnormal, with prolongation of the prothrombin time. However normal platelet count and function help to distinguish AFLP from pre-eclampsia and HELLP syndrome.
Another distinguishing feature is profound hypoglycaemia and hyperuricaemia which are common in AFLP, but not usu-ally found in women with PE or HELLP syndrome.
A liver biopsy will show micorovesicular steatosis (fatty liver) (Ko, 2006) however liver biopsy is not usually performed for the diagnosis of AFLP, as the procedure itself carries risks especially in the presence of coagulopathy. The diagnosis cannot be made with certainty with ultrasound, though sometimes fat deposition in the liver may be seen. CT or MRI scan may also suggest fatty infiltration but again cannot make the diagnosis with certainty. Table 1 summarises suggested criteria for diagnosis trialled in a recent prospective national study (Knight, 2008).
Katie Pateman is Specialist Trainee Registrar year 1; Patrick O’Brien is Consultant Obstetrician at Elizabeth Garrett Anderson Institute for Women’s Health University College London HospitalsEmail: [email protected]
AbstractAcute fatty liver of pregnancy (AFLP) is a rare condition affecting women primarily in the third trimester of pregnancy. It is potentially life-threatening to both mother and fetus. This article discusses the clinical features, how to diagnose the condition and how to manage it.
CLINICAL
242 BRITISH JOURNAL OF MIDWIFERY, APRIL 2008, VOL 16, NO 4
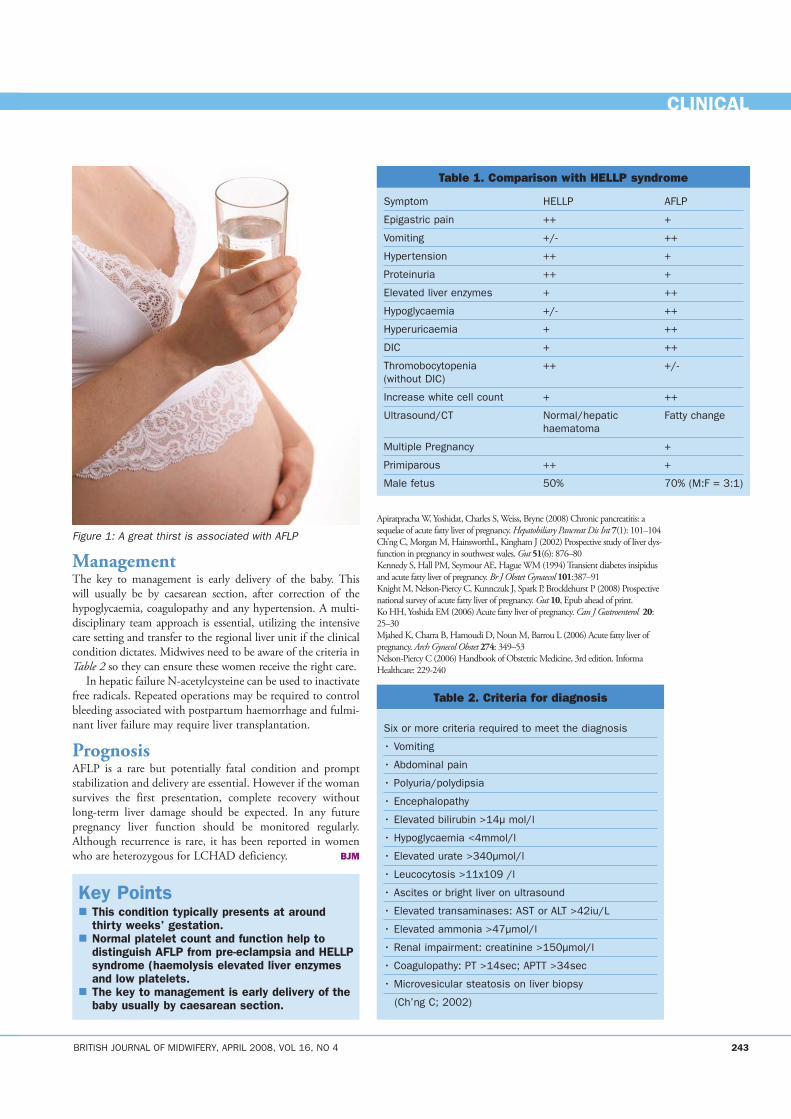
ManagementThe key to management is early delivery of the baby. This will usually be by caesarean section, after correction of the hypoglycaemia, coagulopathy and any hypertension. A multi-disciplinary team approach is essential, utilizing the intensive care setting and transfer to the regional liver unit if the clinical condition dictates. Midwives need to be aware of the criteria in Table 2 so they can ensure these women receive the right care.
In hepatic failure N-acetylcysteine can be used to inactivate free radicals. Repeated operations may be required to control bleeding associated with postpartum haemorrhage and fulmi-nant liver failure may require liver transplantation.
PrognosisAFLP is a rare but potentially fatal condition and prompt stabilization and delivery are essential. However if the woman survives the first presentation, complete recovery without long-term liver damage should be expected. In any future pregnancy liver function should be monitored regularly. Although recurrence is rare, it has been reported in women who are heterozygous for LCHAD deficiency. BJM
Apiratpracha W, Yoshidat, Charles S, Weiss, Bryne (2008) Chronic pancreatitis: a sequelae of acute fatty liver of pregnancy. Hepatobiliary Pancreat Dis Int 7(1): 101–104Ch’ng C, Morgan M, HainsworthL, Kingham J (2002) Prospective study of liver dys-function in pregnancy in southwest wales. Gut 51(6): 876–80Kennedy S, Hall PM, Seymour AE, Hague WM (1994) Transient diabetes insipidus and acute fatty liver of pregnancy. Br J Obstet Gynaecol 101:387–91Knight M, Nelson-Piercy C, Kunnczuk J, Spark P, Brocklehurst P (2008) Prospective national survey of acute fatty liver of pregnancy. Gut 10, Epub ahead of print.Ko HH, Yoshida EM (2006) Acute fatty liver of pregnancy. Can J Gastroenterol 20: 25–30Mjahed K, Charra B, Hamoudi D, Noun M, Barrou L (2006) Acute fatty liver of pregnancy. Arch Gynecol Obstet 274: 349–53Nelson-Piercy C (2006) Handbook of Obstetric Medicine, 3rd edition. Informa Healthcare: 229-240
Key Points� This condition typically presents at around
thirty weeks’ gestation.� Normal platelet count and function help to
distinguish AFLP from pre-eclampsia and HELLP syndrome (haemolysis elevated liver enzymes and low platelets.
� The key to management is early delivery of the baby usually by caesarean section.
Symptom HELLP AFLP
Epigastric pain ++ +
Vomiting +/- ++
Hypertension ++ +
Proteinuria ++ +
Elevated liver enzymes + ++
Hypoglycaemia +/- ++
Hyperuricaemia + ++
DIC + ++
Thromobocytopenia ++ +/-(without DIC)
Increase white cell count + ++
Ultrasound/CT Normal/hepatic Fatty change haematoma
Multiple Pregnancy +
Primiparous ++ +
Male fetus 50% 70% (M:F = 3:1)
Table 1. Comparison with HELLP syndrome
Six or more criteria required to meet the diagnosis
• Vomiting
• Abdominal pain
• Polyuria/polydipsia
• Encephalopathy
• Elevated bilirubin >14μ mol/l
• Hypoglycaemia <4mmol/l
• Elevated urate >340μmol/l
• Leucocytosis >11x109 /l
• Ascites or bright liver on ultrasound
• Elevated transaminases: AST or ALT >42iu/L
• Elevated ammonia >47μmol/l
• Renal impairment: creatinine >150μmol/l
• Coagulopathy: PT >14sec; APTT >34sec
• Microvesicular steatosis on liver biopsy
(Ch’ng C; 2002)
Table 2. Criteria for diagnosis
CLINICAL
BRITISH JOURNAL OF MIDWIFERY, APRIL 2008, VOL 16, NO 4 243
Figure 1: A great thirst is associated with AFLP
Tackling maternal obesity: suggestions for midwives By Yana Richens
The headlines in the newspapers following the latest publication of the Saving Mothers Lives (Confidential Enquiry into Maternal and Child
Health, 2007a) were of no surprise to midwives: ‘Obesity is biggest threat to women during pregnancy.’ (Hope, 2007) Midwives have been aware of, and dealing with, the
problems associated with obesity during pregnancy for sev-eral years, so, what has changed? The fact is that due to the current obesity epidemic an increasing number of women are becoming pregnant.
Currently obesity in the UK is rising at an alarming rate. In 1980, eight per cent of women in England were classi-fied as obese, compared tosix per cent of men. By 1998 the prevalence of obesity had nearly trebled to 21% of women and 17% of men (National Audit Office, 2001). Current figures suggest around 25% of women are classified as obese (Department of Health (DH), 2005). This figure is estimated to increase to 60% of men and 50% of women by 2050, and obesity-related diseases will cost an extra £45.5 billion per year (Butland et al, 2007). It is estimated that 1.2 million more women will be obese in 2010 than in 2003 (Zanninoto et al, 2006).The current estimated human cost of this epidemic is 18 million sick days a year, 30 000 deaths a year resulting in 40 000 lost years in working life (National Audit Office, 2001).
The problem is so serious that the government has published national guidance on the care and manage-ment of the obese adult, however, this does not extend to pregnant women (DH, 2007a). Yet the guidance and the stepped approach could be easily utilized in midwifery practice along with the guidance on ‘Raising the Issue of
weight with adults’ (DH, 2007b).The standard measure for determining obesity is the
classification adopted by the World Health Organization (WHO, 1997) shown in Table 1.
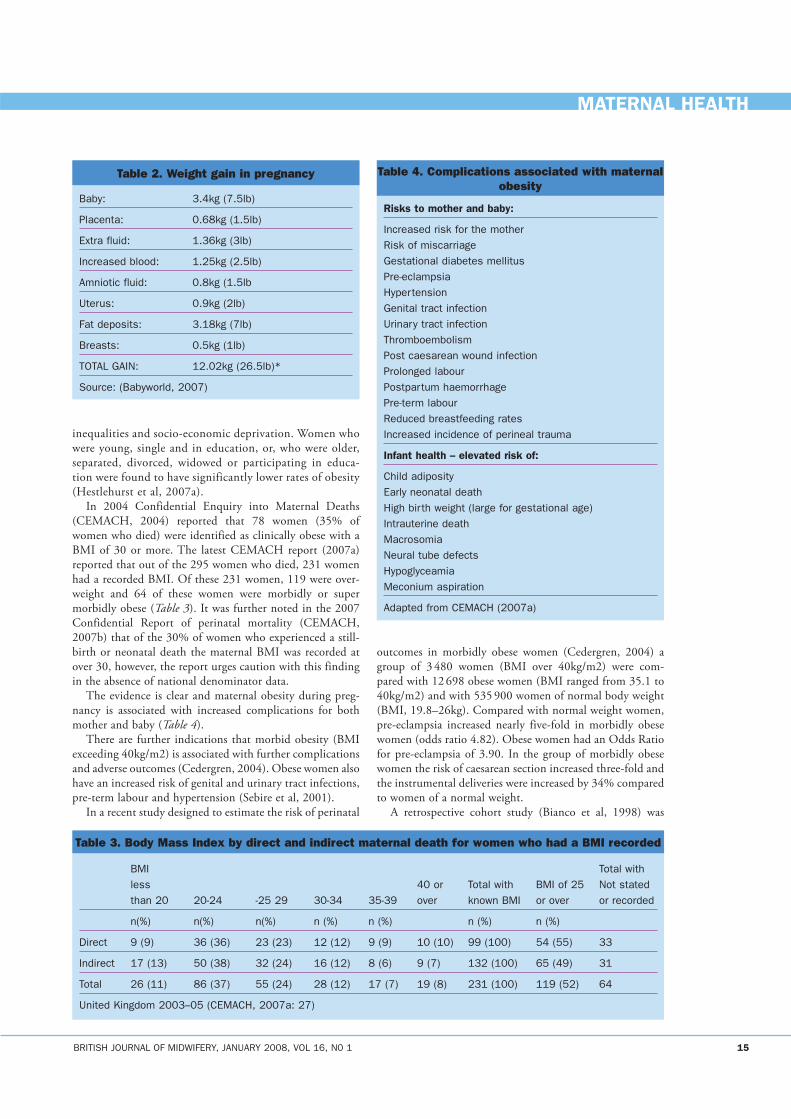
Body Mass Index (BMI) is the most common method of measuring obesity. BMI is calculated by dividing body weight (kilograms) by height (metres) squared. Although BMI is useful on a population scale, it has limitations on an individual level; BMI does not account for body fat distribution. More recently it has been recommended that the treatment of obesity needs to focus more on abdominal fat and not BMI (Despres et al, 2001). The ethnicity of the individual also needs to be considered as individuals from a South Asian background are considered overweight when BMI is greater than 23 kg/m². All pregnant women should have their BMI calculated and recorded at booking. Table 2 shows roughly where the weight gain is attributed during pregnancy for a healthy woman of average height. Therefore it is essential that a woman is weighed as early as possible in a pregnancy.
Obesity which is evident prior to pregnancy is often due to an accumulation of excess body fat caused by the number of calories consumed exceeding the number of calories which are being utilized by the individual. However this should be discussed at booking and any other underlying factors considered.
It is clear that obesity is the greatest public health challenge facing health care professionals and it is in eve-ryone’s best interest to turn this around. Obesity has been linked to inequalities in health and it is likely to effect the poorer members in our society than social class one where 14% of all men and women are obese compared to 28% of women and 19% of men in social class five (DH, 2005). This is supported by recent research undertaken by (Hestlehurst et al, 2007a) which stated that the risk factors determining maternal obesity included health
Yana Richens is Consultant Midwife at Elizabeth Garrett Anderson & Obstetric Hospital, University College London Hospitals NHS Trust, LondonEmail: [email protected]
AbstractMaternal obesity is the largest future challenge facing maternity services. Currently there is no national guideline on how midwives should care for this group of women. Those involved with the care of women must start to address this issue. This article highlights some of the complications and risks to mothers and babies and provides suggestions for care based on the current evidence.
14 BRITISH JOURNAL OF MIDWIFERY, JANUARY 2008, VOL 16, N0 1
MATERNAL HEALTH
Classification BMI (kg/m2)
Normal Range 18.5–24.9
Overweight 25–29.9
Obese I 30–34.9
Obese II 35–39.9
Obese IIIMorbidly obese greater or equal to 40
Table 1. Body Mass Index (BMI)
inequalities and socio-economic deprivation. Women who were young, single and in education, or, who were older, separated, divorced, widowed or participating in educa-tion were found to have significantly lower rates of obesity (Hestlehurst et al, 2007a).
In 2004 Confidential Enquiry into Maternal Deaths (CEMACH, 2004) reported that 78 women (35% of women who died) were identified as clinically obese with a BMI of 30 or more. The latest CEMACH report (2007a) reported that out of the 295 women who died, 231 women had a recorded BMI. Of these 231 women, 119 were over-weight and 64 of these women were morbidly or super morbidly obese (Table 3). It was further noted in the 2007 Confidential Report of perinatal mortality (CEMACH, 2007b) that of the 30% of women who experienced a still-birth or neonatal death the maternal BMI was recorded at over 30, however, the report urges caution with this finding in the absence of national denominator data.
The evidence is clear and maternal obesity during preg-nancy is associated with increased complications for both mother and baby (Table 4).
There are further indications that morbid obesity (BMI exceeding 40kg/m2) is associated with further complications and adverse outcomes (Cedergren, 2004). Obese women also have an increased risk of genital and urinary tract infections, pre-term labour and hypertension (Sebire et al, 2001).
In a recent study designed to estimate the risk of perinatal
outcomes in morbidly obese women (Cedergren, 2004) a group of 3 480 women (BMI over 40kg/m2) were com-pared with 12 698 obese women (BMI ranged from 35.1 to 40kg/m2) and with 535 900 women of normal body weight (BMI, 19.8–26kg). Compared with normal weight women, pre-eclampsia increased nearly five-fold in morbidly obese women (odds ratio 4.82). Obese women had an Odds Ratio for pre-eclampsia of 3.90. In the group of morbidly obese women the risk of caesarean section increased three-fold and the instrumental deliveries were increased by 34% compared to women of a normal weight.
A retrospective cohort study (Bianco et al, 1998) was
BRITISH JOURNAL OF MIDWIFERY, JANUARY 2008, VOL 16, N0 1 15
MATERNAL HEALTH
Baby: 3.4kg (7.5lb)
Placenta: 0.68kg (1.5lb)
Extra fluid: 1.36kg (3lb)
Increased blood: 1.25kg (2.5lb)
Amniotic fluid: 0.8kg (1.5lb
Uterus: 0.9kg (2lb)
Fat deposits: 3.18kg (7lb)
Breasts: 0.5kg (1lb)
TOTAL GAIN: 12.02kg (26.5lb)*
Source: (Babyworld, 2007)
Table 2. Weight gain in pregnancy
BMI Total with less 40 or Total with BMI of 25 Not stated than 20 20-24 -25 29 30-34 35-39 over known BMI or over or recorded
n(%) n(%) n(%) n (%) n (%) n (%) n (%)
Direct 9 (9) 36 (36) 23 (23) 12 (12) 9 (9) 10 (10) 99 (100) 54 (55) 33
Indirect 17 (13) 50 (38) 32 (24) 16 (12) 8 (6) 9 (7) 132 (100) 65 (49) 31
Total 26 (11) 86 (37) 55 (24) 28 (12) 17 (7) 19 (8) 231 (100) 119 (52) 64
United Kingdom 2003–05 (CEMACH, 2007a: 27)
Table 3. Body Mass Index by direct and indirect maternal death for women who had a BMI recorded
Risks to mother and baby:
Increased risk for the motherRisk of miscarriageGestational diabetes mellitusPre-eclampsiaHypertensionGenital tract infectionUrinary tract infectionThromboembolismPost caesarean wound infectionProlonged labourPostpartum haemorrhagePre-term labourReduced breastfeeding ratesIncreased incidence of perineal trauma
Infant health – elevated risk of:
Child adiposityEarly neonatal deathHigh birth weight (large for gestational age)Intrauterine deathMacrosomiaNeural tube defectsHypoglyceamiaMeconium aspiration
Adapted from CEMACH (2007a)
Table 4. Complications associated with maternal obesity
undertaken comparing a sample 613 morbidly obese women with 11 313 non-obese women who were delivered of a singleton live birth. In this study morbidly obese women were more likely to experience pregnancy complications including diabetes, hypertension, pre-eclampsia, as well as being more likely to experience fetal distress, meconium and to have a caesarean section. Weight gains of more that 25lb were strongly associated with birth of a large for gestational age neonate (P<.01); however, poor weight gain did not appear to increase the risk of delivery of a low birth weight baby (Bianco et al, 1998).
Compared to normal weight women there is evidence that maternal obesity is also associated with fetal anomalies, particularly spina bifida, omphalocele, and heart defects (Watkins et al, 2003). Ehrenberg and colleagues (2004) found that women who were obese prior to pregnancy were more likely to have a baby that was large for gestational age. Kristensen and colleagues (2005) identified that maternal obesity resulted in unfavourable perinatal outcomes, includ-ing a two-fold increase in stillbirths and neonatal death, when compared to birth outcomes in women of normal bodyweight.
As we can see studies demonstrate that compared to normal weight women, those who were overweight or obese had significantly higher rates of gestational diabetes, pre-eclampsia, eclampsia and caesarean birth (Barau et al, 2006; Bianco, 1998). Stotland and colleagues (2004) found that excessive weight gain in pregnancy is an independent risk factor for caesarean birth and estimated that a significant number of caesarean sections could be avoided each year if women’s weight did not exceed that recommended by the Institute of Medicine (IOM, 1990).
16 BRITISH JOURNAL OF MIDWIFERY, JANUARY 2008, VOL 16, N0 1
MATERNAL HEALTH
Height for weight Recommendedcategory Kg BMI range weight kg
Underweight women <19.8 12.5 – 18.0
Normal weight 19.8 -26.0 11.5 – 16.0
Overweight women BMI 26.1 29.9 7.0 – 11.5
Obese women BMI > 29.9 At least 6.0
Based on the IOM adapted by Jevitt (2005)
Table 5. Recommended weight gain in pregnancy
Morbidly obese women (BMI >40) have risks for compli-cations that are significantly greater. Bianco and colleagues (1998) found that morbidly obese women (BMI >35) were at greater risk of prolonged labour, gestational diabetes, pre-eclampsia, placental abruption, surgical birth, postpartum endometritis, wound dehiscence and prolonged postpartum hospital stays than the non-obese women (BMI 19–27) (Cedergren, 2004; Sebrie et al, 2001).
There is also an added cost and resource implication, which as been recently highlighted by Hestlehurst and col-leagues (2007b). Issues identified by the study related to managing the care of obese women in pregnancy safely and the resources and costs needed to achieve this, as specialist equipment is required.
Currently there is no national advice for midwives on what to recommend to women who have a significantly raised BMI although there are calls for a national guideline (CEMACH, 2007a). The Royal College of Obstetricians and Gynaecologists provide advice for the clinical manage-
istockphoto.com

ment of women during pregnancy for obstetricians. Current advice given by the American Institute of Medicine (IOM, 1990) has produced guidance on how much weight women should gain during pregnancy (Table 5).
Current advice based on the available evidence recom-mends that women with a BMI over 30kg/m2 are booked under the care of a consultant and they have their baby in a consultant unit. Options for birth and reasons why consult-ant care is recommended must be discussed honestly and sensitively with the woman and her partner at booking. It may be possible after consultation with the obstetrican and discussion with the woman that, if she has no further co-morbidities, for example gestational diabetes or hyper-tension, she can remain in high risk midwifery-led care, although this will need to be carefully managed, and the woman referred immediately should there be any problems identified.
Boxes 1, 2 and 3 comprise a proposed outline for mid-wives on how to plan care for women with a BMI over 30. It is not exhaustive and provides suggestions for practice based on available evidence.
The way forwardIt has been suggested that pregnancy is not a time to lose weight. This is the advice that many women are given by their families and it is what they are likely to find on the internet. However, given the evidence surely the antena-tal booking is the ideal time to discuss with women who have been identified as obese/morbidly obese their diet and the effects that obesity can cause during pregnancy, in much the same way smoking is discussed. Recent stud-ies suggest that providing an intervention programme to support women to lose weight during pregnancy can have beneficial and longer lasting effects leading to postpartum weight loss, even though they did not effect delivery or neonatal outcome (Claesson et al, 2007; O’Toole et al, 2003; Jevitt, 2005).
Olafsdottir and colleagues (2006) identified that women with a BMI of 25–29.9 kg/m2 before pregnancy were most likely to gain excessive weight and be categorized as obese after pregnancy. This could significantly lead to a complica-tions in any further pregnancy. Villamor and Cnattingius (2006) identified that a weight gain of 3 BMI units after pregnancy was significantly associated with the risk of still-birth deliveries in subsequent pregnancies.
The fact is that it was estimated in the last confiden-
tial enquiry to be at least 360 existing children and 160 live newborn babies who lost their mother and we know that of these, 119 of the women were classified as obese (CEMACH, 2007a). We also know that of around 30% of babies who were stillborn or who had a neonatal death their mothers had a BMI greater than 30 (CEMACH, 2007b). Although caution is urged as there is no national denomina-tor data available.
As midwives we must prepare ourselves for this epi-demic and we must endeavour to help women who want to lose weight and dispel the myth that this cannot be achieved safely during pregnancy. We need to provide practical advice and support and stop beating around the bush. This problem will not go away and if we are serious at providing the best care for our women we must start addressing and tackling the problems at the root. This can be achieved by talking to pregnant women about their own weight and the impact that this will have on the future of their children, as we know that obese parents often have obese children.
At our local unit we are starting a new clinic led by myself and supported by the lead obstetrician. This clinic is for any woman who have BMIs over 30. The plan is to provide one to one support and care alongside the com-munity midwives, if the woman has one, as many women
BRITISH JOURNAL OF MIDWIFERY, JANUARY 2008, VOL 16, N0 1 17
MATERNAL HEALTH
Box 1. Antenatal management of women with a BMI over 30
� Book women as early as possible for consultant care where possible continuity of care by the same midwife
� Pre-existing medical problems to have appropriate and timely referral
� Discuss weight openly (women are aware that they are obese), provide advice on healthy eating and sug-gest a food diary so that you can read this at the next antenatal visit. Identify how much help and support the woman has helping to lose weight sensibly and refer to a dietician if help is required.
� Women with severe obesity (BMI >35 kg/m²) plus one additional risk factor for hypertensive disease should be prescribed aspirin 75 mg/day from 12 weeks.
� Advise folic acid 5mg per day� Discuss problems associated with obesity and preg-
nancy to both the woman and the baby� Schedule of antenatal care to reflect risk; use ultra-
sound to detect fetal heart when necessary, and give fetal movement chart from 28 weeks’ gestation (this is due to the fact that some women do not feel more than ten movements from 24 weeks)
� Weigh every visit and record, using the same scales� Delivery to take place in a consultant unit� Plan of care to be documented. Consultant appoint-
ments at 16, 28 and 36 weeks� Anaesthetic assessment� To see physiotherapist� Serial scans to assess fetal growth (difficult to assess
clinically).
As midwives we must ... endeavour to help women who want to lose weight and dispel the myth that this cannot be achieved safely during pregnancy.
‘’
wishing to have their baby at the hospital live outside the catchment area and do not have access to a community
midwife. The consultant obstetrician will see them at least twice during their pregnancy and we have a designed a pathway of care for women. This is likely to change and develop as the evidence base around the subject grows and national guidelines are produced. BJM
Babyworld (2007) Pregnancy kilo counting. http://www.babyworld.co.uk/information/pregnancy/kilo_counting.asp (Accessed 14 December)Barau G, Ribukkard P-Y Hulsey T.C, Dedecker F, Laffite A Gerardin P Kauffman E (2006)Linear association beteen maternal pre-pregnancy body mass index and rikd of caesarean secion in term deliveries. British Journal of Obstetrics and Gynaecology 113: 1173–7Bianco AT, Smilen SW, Davis Y, Lopez S, Lapinski R, Lockwood CJ (1998) Pregnancy outcome and weight gain recommendations for mor-bidly obese women. Obstet Gynecol 91: 97–102Butland B, Jebb S, Kopelman P, McPherson K, Thomas S, Mardell J, Parry V (2007) Foresight Tackling Obesity: Future Choices Project Report http://www.foresight.gov.uk/Obesity/obesity_final/17.pdfCedergren M (2004) Maternal morbid obesity and the risk of adverse pregnancy outcome. Obstet Gynecol 103: 219–24Claesson I, Sydsjo G, Brynhildsen J, Cedergren M, Jeppsson A, Nystrom F, Sydsjo A, Josefsson A (2007) Weight gain restriction for obese preg-nant women: a case-control intervention study DO1: British Journal of Obstetrics and Gynaecology 10.111/j.1471-0528.2007.01531.x. Confidential Enquiry into Maternal and Child Health (2004) Why moth-ers die 2000- 2002) RCOG, LondonConfidential Enquiry into Maternal and Child Health (2007a) Saving Mothers’ Lives Reviewing maternal deaths to make motherhood safer 2003-2005 CEMACH Chiltern CourtCEMACH (2007b) Perinatal mortality 2005 England Wales and Northern Ireland CEMACH Chiltern CourtDepartment of Health (2005) Delivering Choosing Health Making healthier choices easier. Londonhttp://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4105355Department of Health (2007a) Obese Adult Care pathway http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4134408Department of Health (2007b) Raising the issue of weight http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4134408Despres JP, Lemieux I, Prud’homme D (2001) Treatment of obesity: need to focus on high risk abdominally obese patients. British Medical Journal 322: 716–20Ehrenberg HM, Mercer BM & Catalano PM (2004) The influence of obesity and diabetes on the prevalence of macrosomia. American Journal of Obstetrics and Gynecology 191: 964–8Heslehurst N, Ells L, Simpson H, Batterham A, Wilkinson J, Summerbell C (2007a) Trends in maternal obesity incidence rates, demographic pre-dictors, and health inequalities in 36 821 women over a 15-year period. BJOG 114: 187–94Heslehurst N, Lang R, Rankin J, Wilkinson J, Summerbell CD (2007b) Obesity in pregnancy: a study of the impact of maternal obesity on NHS maternity services. BJOG 114: 334–42Hope J (2007) Daily Mail Tues 4 December 2007Institute of Medicine (1990) Subcommittee on Nutritional Status and Weight Gain During Pregnancy Nutrition during pregnancy Institute of Medicine Washington DC National Academy PressJevitt C (2005) Integrating obesity prevention into prenatal care Presentation of finding at the International Conference for Midwifery. Brisbane, AustraliaNational Audit Office (2001) Tackling Obesity in England. The Stationery Office, LondonKristensen J, Vestergaard M, Wisborg K, Kesmodel U & Secher NJ (2005) Pre-pregnancy weight and the risk of stillbirth and neonatal death. British Journal of Obstetrics & Gynaecology 112: 403–8Olafsdottir AS, Skuladottir GV, Thorsdottir I, Hauksson A, Steingrimsdottir L (2006) Maternal diet in early and late pregnancy in relation to weight gain. International Journal of Obesity 30(3): 492–9O’Toole ML, Sawicki ML Artal R (2003) Structured diet and physical
18 BRITISH JOURNAL OF MIDWIFERY, JANUARY 2008, VOL 16, N0 1
MATERNAL HEALTH
Box 2. Intrapartum management of women with a BMI over 30
� On admission inform consultant obstetrician/SPR and anaesthetist
� To be cared for by a senior midwife during active labour� Check presentation of baby; if in doubt undertake an
ultrasound, be aware of possible shoulder dystocia and PPH following delivery
� Large gauge Venflon to be sited; blood taken for FBC and Group and Save
� Ensure correct large size blood pressure cuff is used, and record maternal pulse
� Clear fluids only and ranitidine six-hourly � Epidural catheter to be sited early� Assessment of pressure areas using Waterlow or other
appropriate scoring system; check pressure areas every two hours
� Apply antiembolic stockings, ensure that the correct size is used
� Fetal monitoring by external transducer where possible, fetal scalp electrode to be applied if unable to record fetal heart (check HIV and hepatitis status first)
� Manual handling risk assessment to be undertaken; ensure correct equipment used
� If an emergency caesarean section is required two obstetricians should be present
� Inform paediatrician� Post-delivery be aware of possible postpartum haemor-
rage.� Ensure adequate analgesia is provided� Maintain skin integrity; observe and document pres-
sure areas� Encourage skin-to-skin of baby and support with
breastfeeding� Observations to include respirations and pulse oxime-
try� Encourage deep breathing and refer to physiotherapist
Box 3. Postnatal care for women with a BMI over 30
� Early mobilization� Adequate fluids� Wound must be assessed and observed daily for signs
of wound dehiscence; women advised to lift abdomen where needed and ensure wound is kept dry
� Involution of the uterus may difficult to palpate; be vigi-lant for signs of secondary postpartum haemorrhage, this may be due to large placental site or infection. Observe and record lochia taking note of the odour
� Thromboprophylaxis prophylactic low molecular weight heparin (even after vaginal delivery). May need to use higher dose than normal – adjust according to weight
� Broad spectrum antibiotics
activity prevent postpartum weight retention. Journal of womens health 12: 991–8Stotland N, Hopkins L, Caughey A (2004) Gestational Weight gain during macrosomia and risk of caesarean birth in nondiabetic nulli-paras. Obtet Gynecol 104(4): 1667–77Sebire NJ, Jolly M, Harris JP, Wadsworth J, Joffe M, Beard RW, Regan L, Robinson S (2001) Maternal obesity and pregnancy outcome: a study of 287 213 pregnancies in London. International Journal of Obesity 25: 1175–82World Health Organisation (1997) Consultation on Obesity Preventing and managing the global epidemic. Report on WHO ConsultationVillamor E, Cnattingius S (2006) Interpregnancy weight change and risk of adverse pregnancy outcomes: a population-based study. The Lancet 368: 1164–70Watkins M, Ramussen S, Honein M, Botto Moore C (2003) Maternal Obesity and risk for birth defect. Pediatrics 111(5): 1152–8Zanninoto P, Wardle H, Samakakis E, Mindell J, Head J (2006)
MATERNAL HEALTH
BRITISH JOURNAL OF MIDWIFERY, JANUARY 2008, VOL 16, N0 1 19
Key Points��Obesity in pregnancy is a growing problem and
presents severe risks to both mother and baby.��Currently there is no national guidance for
midwives on how to care for this increasing number of women.
��This article suggests guidance for midwives when caring for this group of women.
��Obesity is the largest health issue facing women today. It is estimated that 1.2 million more women will be obese in 2010 than 2003.
Forecasting obesity to 2010 [accessed December 1st 2007] commis-sioned by Department of Healthhttp://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsStatistics/DH_4138630
istockphoto.com
RESEARCH AND EDUCATION
Caring for women with nausea and vomiting in pregnancy: new approachesBy Catherine McParlin, RH Graham and SC Robson
Nausea and vomiting (NVP) is one of the most fre-quently occurring symptoms of pregnancy; nausea affects 80–85% of all pregnant women, while the
associated complaint of vomiting affects approximately 52% (Whitehead et al, 1992). Commonly referred to as ‘morning sickness’, women can be affected at any time of day or night with the severity of symptoms varying dramatically between individuals.
While mild cases are often thought to be a normal physi-ological symptom of pregnancy and usually self-limiting, more severe cases of intractable vomiting are referred to as hyperemesis gravidarum (HG). The point at which nausea and vomiting in pregnancy becomes HG is unclear, with HG reported to affect 0.3–2% of pregnant women (Eliakim et al, 2000) and being associated with fluid and electrolyte distur-bances, nutritional deficiency and a weight loss greater than 5% of pre-pregnancy weight. If untreated the condition can
lead to neurological, liver and renal abnormalities and even maternal death. There is no evidence that NVP and HG are teratogenic (Klebanoff and Mills, 1986) and observational studies suggests a reduced risk of spontaneous abortion, (OR 0.36, 95% CI 0.32–0.42) (Weigel and Weigel, 1989). Data regarding perinatal mortality are conflicting and severe HG involving poor maternal weight gain during pregnancy has been associated with lower birth weights and more infants who are born small for gestational age (Bailit, 2005; Dodds et al, 2006, Weigel and Weigel, 1989). HG therefore results in increased health care use, hospitalization, time lost from work and a reduced quality of life for sufferers. Midwives and doctors often feel helpless, unable to provide a cure and with limited medical interventions that often are inadequate in alleviating symptoms.
For women, severe NVP can be extremely debilitating. They are often bedridden, unable to move for fear that they will be overwhelmed by the uncontrollable urge to vomit (Jakeway, 2001). It can affect interactions with family, friends, partner and offspring as well as the ability to fulfil paid and domestic work. Mazzotta and Magee (2000) found that women suffering from severe NVP lost an average of 206 hours from paid work due to the condition. Apart from the debilitating physical symptoms, women have reported feeling isolated, depressed and lonely, adding to the pressure, anxiety and stress resulting from their symptoms. NVP is often mis-understood by family, employers and health care professionals and consequently women are often treated unsympathetically (Soltani and Taylor, 2003). Frustration at being unable to complete everyday tasks, fulfil roles, low self-efficacy and concern over their unborn baby add to women’s psychological morbidity; up to 60% of women with HG have been reported to develop secondary depression (Davis, 2004).
Pathophysiology and the role of psychological and sociocultrual factorsIt has been hypothesized that NVP may provide an evolu-tionary protective response; the mother vomits to remove potentially toxic or teratogenic chemicals from her body or avoids strong smelling and irritating substances which could be potentially harmful to the fetus (Sherman and Flaxman, 2002; Swallow et al, 2005; Verberg et al, 2005). Popular pathophysiological theories include increased human cho-rionic gonadotrophin, thyroid function and adrenocorticot-riphic hormone production, mineral and vitamin B6 deficien-cies and helicobacter pylori infection (Verberg et al, 2005).
Catherine McParlin is Research Midwife, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, Dr RH Graham is Lecturer in Sociology, Newcastle University, Newcastle upon Tyne; Professor SC Robson is Professor of Fetal Medicine, Newcastle University, Newcastle upon TyneE-mail: [email protected]
AbstractNausea and vomiting in pregnancy (NVP) is a frequently occurring but often debilitating condition. The more severe form, hyperemesis gravidarum (HG) results in increased health care use and a reduced quality of life for sufferers.Management is inconsistent and results in multiple admissions and poor experience of the health care system. Women feel isolated, depressed and lonely and are often treated unsympathetically.Assessment of the severity of symptoms alongside alternative approaches which take into account the interaction between social, psychological and biological events should be considered. A combination of traditional and alternative remedies may be of benefit while ongoing information, advice, social, psychological and emotional support results in increased knowledge, reassurance and confidence which hopefully empowers and encourages women to carry out health promoting activities. This can be carried out in person or via telephone which is an economical and convenient option. Ultimately this should result in improved care and quality of life for sufferers.
280 BRITISH JOURNAL OF MIDWIFERY, MAY 2008, VOL 16, NO 5
RESEARCH AND EDUCATION
The relationship between aetiology, psychological ill health and poor coping mechanisms is controversial. During the 1960s and 1970s it was commonly believed that HG was psychologically mediated, the act of vomiting was a way of unconsciously purging oneself of an unwanted pregnancy; Fairwalter (1968) suggested that up to 80% of HG cases were of psychiatric origin. Associations with hysteria, neuro-sis, rejection of femininity, sexual dysfunction, immaturity, resentment, ambivalence towards pregnancy and motherhood and strong maternal mother dependence became popular (Deuchar, 1995; Iancu et al, 1994; Verberg et al, 2005). HG has also been described as a conversion disorder, in which psychological trauma is translated into physical symptoms, a conditioned or anticipatory response, a psychosomatic symp-tom and a ‘hysterical defence against unconscious wishes’ (Buckwalter and Simpson, 2002: s210). The fact that hyp-nosis, imagery and psychotherapy have been reported to be successful in some circumstances adds weight to the argument that there may be a psychological component. It has been proposed that the condition is an ‘interaction of biological, psychological and sociocultural factors’, and the ‘physiological changes associated with pregnancy interact with a woman’s psychological state and cultural values.’ (Buckwalter and Simpson, 2002).
ManagementThere is no cure for NVP and so care focuses on alleviation of symptoms, prevention of serious morbidity and implementa-tion of strategies to help women cope with the condition. Current treatment approaches in the hospital setting include keeping sufferers nil by mouth, rehydration using intravenous fluids and prescribing anti-emetics. Gradually oral fluids and simple foods are introduced and once women are ‘tolerating’ diet they are discharged home, often with a prescription for anti-emetics.
Unfortunately, once at home women frequently slip back into the vicious cycle of being unable to eat or drink due to nausea and when they do, the vomiting re-starts, often result-ing in dehydration and readmission.
Despite reassurances many women feel guilty about tak-ing prescribed medication during pregnancy or wish to try alternative, non-medicalized approaches to symptom management. Ginger and acupressure are two alternative therapies that have the most promising results from clinical trials, however, neither are routinely used in hospitals in the UK. Fresh root or pharmaceutical ginger preparations have been shown to have beneficial effects on nausea and vomit-ing symptoms without increasing the rates of congenital malformations, miscarriage or caesarean section (National Collaborative Centre for Women’s and Children’s Health, 2003; Portnoi et al, 2003; Vutyabanich et al, 2001; Jewell and young, 2003) The value of acupressure is less clear; some trials have demonstrated improvements in nausea alone or both nausea and vomiting with stimulation of, or pressure on acupuncture point pericardium 6 (Carlsson et al, 2000; Acupuncture Research Resource Centre, 2004; Strong, 2001; Jewell and Young, 2003). Although some studies involving acupuncture apparently show treatment benefits (Carlsson et al, 2000; Strong, 2001) it is impossible to draw conclusions
about the effectiveness of the therapy due to the wide vari-ability in the types of acupuncture and methodological design of the studies.
Even if alternative therapies are tried and lifestyle changes made there comes a point for some women when symptoms become overwhelming and hospitalization is seen as a relief, a way of escaping the demands of everyday life and handing over responsibility to health care professionals (Agren and Berg, 2006). However the care received is often very different from what they anticipate. Aside from improving their symp-toms, women want support, understanding and compassion. In reality there is an emphasis on practical interventions and while women admitted to hospital usually have their physical needs addressed midwives on a busy antenatal ward rarely have the time to look after psychological and emotional needs or provide information and guidance about the condition (Soltani and Taylor, 2003). As a result women can feel unsup-ported, have negative interpersonal interactions with health care providers and feel dissatisfied with their care (Munch and Schmitz, 2006; Soltani and Taylor, 2003) In extreme cases women have been known to feel so wretched they request ter-mination of pregnancy (Jewell, 2003; Mazzotta and Magee, 2000), while others avoid a subsequent pregnancy for fear of a reoccurrence of the condition (Jakeway, 2001).
Non-medical management optionsAlternative management strategies could improve women’s experience of this debilitating condition. Moving away from the traditional medical model of health care may be help-ful. One of the problems with the biomedical model is the assumption that every illness has an objective and identifiable primary biological cause. Behavioural factors are not seen as causal factors, and so these are not assessed during diagnosis and management. The focus on biological causes appears to disregard the social and psychological aspects of illness events. In contrast, the biopsychosocial model incorporates all three factors as important determinants of health and ill-ness, encouraging medical diagnosis to take into account the interaction of all three when recommendations for treatment are made. Nausea and vomiting in pregnancy and HG are no exception to this (Stroebe, 2000).
Key intervention areasDrawing on the biopsychosocial model there are several ways in which care could be developed to improve the experiences of women with NVP/HG.
(a) Provision of information and advice Women suffering from NVP need individualized and appro-priate care, support and advice, both in the community and hospital setting. On first contact midwives need to ascertain what prior knowledge women may have about NVP, what self help measures have been tried, and to impart advice and information. A listening, sympathetic ear at this stage may be enough to give women the reassurance and confidence they need to stay at home and try new approaches to self help, or go to the GP for oral anti-emetics. Topics that should be covered by midwives are shown in Table 1.
Information that gives women knowledge as well as reas-
BRITISH JOURNAL OF MIDWIFERY, MAY 2008, VOL 16, NO 5 281

RESEARCH AND EDUCATION
surance may also serve to empower them, aid compliance with the advice they are given and encourage health pro-moting activities. For example, in NVP this could include persevering with lifestyle changes, taking regular anti-emetics, trying different foods or eating patterns and possibly alterna-tive therapies.
This advice could be added to an information leaflet and given to women either in the community or on discharge from hospital.
(b) Assessment of severity Not all women suffering from NVP need to be admitted to hospital; for women suffering from mild to moderate NVP unnecessary hospital admission may be disadvantageous, inconvenient and an unpleasant experience. However, it is sometimes difficult to make a decision about a woman’s con-dition over the telephone (Koren et al, 2005; 2002). Koren and colleagues (2002; 2005) devised a simple three question scale specifically for pregnant women, the ‘Pregnancy Unique Quantification of Emesis and Vomiting’ score, (PUQE score.) The questionnaire has been validated for use in early pregnancy, takes two minutes to complete and also contains a fourth question about general wellbeing.
The first three questions relate to the three physical symp-toms experienced by women, i.e. nausea, vomiting and retch-ing, and for how long, or how many times in the last 12 hours they have experienced each (Box 1).
Question 1 is relatively subjective and open to interpreta-tion, as it draws on women’s self-defined experience of feel-ing ‘nauseated or sick to your stomach’. Questions 2 and 3 involve the quantification of more objective events, vomiting and retching. Together these three questions provide a total score out of 15 points. It is perhaps not suitable for use as an absolute measure of the woman’s physical condition but it could be used as a guide.
There is an additional fourth question that provides the woman’s self defined evaluation of how debilitating her symptoms are in daily life. These brief questions collect two different types of data: objective medical signs of ill health (questions 2 and 3) and subjective experiences of symptoms (questions 1 and 4) (Malterud, 1999). The possible utility of comparing the results of the two question types has not been studied.
The dominance of the biomedical model in healthcare often results in a tendency to view objectively measured signs of disease as more important or more valid, than subjectively defined experiences of symptoms (Whitty et al, 2004). High scores on subjective symptoms but low scores on physi-cal symptoms or signs may be interpreted as an ‘abnormal’ response on the part of the individual (Kirmayer and Looper, 2006; Rietveld and Brosschot, 1999). Subjective experiences and social aspects of illness behaviour have attracted atten-tion in the social science community (Salmon et al, 1996). In health care research, subjective symptoms may be particularly valued in areas where there is a lack of objectively defined signs, such as drug addiction and mental health.
In relation to assessing women with NVP/HG a discrep-ancy between scores on objective signs and subjective experi-ences of impact could have clinical utility, particularly in cases where it is not clear whether hospital admission would be beneficial. Women react in different ways depending on variables such as personality, beliefs, attitudes, knowledge and personal circumstances. The comparison of the two types of data provides a perspective on how the individual woman is coping with the condition. For example, a woman may score highly on physical events (questions 2 and 3) but the data from questions 1 and 4 may suggest that the impact of regular vomiting is minimal and out patient management is reasonable. Alternatively, a woman may score low on physi-cal events, but the data from questions 1 and 4 may suggest these symptoms are having a dramatic impact on wellbeing and hospitalization may provide the support and reassurance needed to improve the woman’s ability to cope.
Midwives could therefore use the comparison of these two types of information as a clinical tool to quickly and effectively assess the condition of the woman and facili-tate decisions about hospital admission and the level of additional support required after discharge, especially in borderline cases.
(c) Ongoing social support Coping with a new pregnancy places additional emotional
282 BRITISH JOURNAL OF MIDWIFERY, MAY 2008, VOL 16, NO 5
� Incidence and description of NVP/HG
� Possible causes
� Effect on the fetus
� Duration of symptoms
� Treatment options
� Symptom management following discharge (if admit-ted to hospital)
� Contact numbers for further advice, concerns or if readmission required
� Addresses of helpful websites and support groups
Table 1. Suggested topics to be discussed with women
� Rest as much as you can; get some help if you can.� Small, frequent snacks, high carbohydrate and low fat protein foods e.g. cereal, pasta, rice potatoes, lean meat, eggs and fish. Avoid strong flavours and smells.� Don’t drink and eat at same time, leave a gap of 30 minutes.� If you can’t tolerate hot food try cold and vice versa.� Have a snack before going to bed and try to eat before getting up in the morning e.g. plain biscuits/crackers. Get out of bed slowly and don’t make any sudden movements.� Try travel sickness wristbands, available from chemists.� Take ginger – biscuits, tea, root, stem, capsules, ginger beer.� Try Lucozade, Sprite, 7-Up, Coke (not diet versions), and also ice pops/lollies which help to give fluid and sugar slowly.
Table 2. General self help advice for women

RESEARCH AND EDUCATION
and physical demands on all women and social support is likely to be very beneficial to health at this time (Baker et al, 1997). Social support is a multi-faceted concept that has been difficult to define and measure. It has been described as ‘information from others that one is loved and cared for, esteemed and valued and part of a network of communica-tion and mutual obligation’ (Cobb, 1976: 300). All defini-tions imply some type of positive interaction or helpful behaviour provided to a person in need of support (Hupcey, 1998). The positive effects of social support on health and wellbeing have been extensively researched over recent dec-ades. Evidence suggests that there is an association between social support and physical and mental wellbeing and that somehow social support acts as a buffer against the high stress levels which have been shown to impact negatively on maternal and fetal outcomes (Mulder, 2002). This ‘buffer-ing’ effect is thought to provide a sense of belonging, reas-surance of worth and facilitate access to advice and services (Bullock et al, 2002).
Social support can be conceptualized as a diversity of natural helping behaviours which individuals actually receive (McLeod et al, 2006). It can be considered in terms of structural measures which assess the quantity and quality of social relationships or functional measures. These can be further divided into emotional, instrumental, informational and appraisal support, all of which theoretically should be provided by midwives as part of their role. There is also some evidence to indicate that social support has a positive associa-tion with behaviours that promote health, such as compliance with taking medication (Stroebe, 2000).
The quality of social relations is linked to the extent to which individuals perceive they are supported. In contrast the quantity of social contacts is a reflection of an individual’s social network and can have a positive or negative influence on health status (Baker et al, 1997). Therefore even if women suffering from NVP appear to have extensive family contacts it is still essential for midwives to asses their needs and give appropriate care and support.
Many social psychologists believe that a positive and stable self-esteem is important for individual wellbeing. Social relationships and groups help promote self-esteem as does emotional support, which also has a positive effect on psychological wellbeing and reduces women’s vulnerabil-ity to depression (Baker, 1997). This may involve simply expressing concern about general health and personal feel-ings and taking the time to discuss these feelings (McLeod, 2006). The evidence regarding the effectiveness of social support suggests that a method of offering ongoing, cost-effective, support may be beneficial for the mental and physical wellbeing of women suffering from NVP, and for reducing the economic burden associated with recurrent readmissions.
The clinic or hospital is unlikely to be the best place to give ongoing support; women may feel physically unable to make extra visits to hospital and additionally communi-cation between staff and women is frequently affected by time constraints or feelings of intimidation or discomfort within the surroundings. Non-verbal cues may also be an issue, for example, socio-economic status may potentially
become a barrier between middle class professionals and women with more deprived socio-economic backgrounds. It is therefore important that health care providers look for alternative ways to decrease or remove existing or potential barriers and provide support which is acceptable to women.
Telephones are an under-utilized resource in healthcare; they are accessible as most people have a landline or mobile. They are quick, convenient, immediate and flex-ible. Telephones have been used to give support to patients in other areas of medicine, for example, cancer sufferers and children and adults with chronic illness. In a study by Bullock and colleagues (2002), 20 pregnant American women were
BRITISH JOURNAL OF MIDWIFERY, MAY 2008, VOL 16, NO 5 283
Box 1. Pregnancy Unique Quantification of Emesis and Vomiting Score (PUQE)
(Please circle one answer for each question) Score
1) In the last 12 hours, for how long have you felt nauseated or sick to your stomach?
Not at all 1
1 hour or less 2
2-3 hours 3
4-6 hours 4
More than 6 hours 5
2) In the last 12 hours, have you vomited or thrown up?
7 or more times 5
5 to 6 4
3 to 4 3
1 to 2 2
I did not throw up 1
3) In the last 12 hours, how many times have you had retching or dry heaves without bringing anything up?
No time 1
1 to 2 2
3 to 4 3
5 to 6 4
7 or more 5
..../15
On a scale of 1–6 how would you rate your nausea and/or vomiting today, if 1 is acceptable and 6 is extremely debilitating? (Please circle)
1 2 3 4 5 6
(Koren et al, 2002)
PUQE Score Symptoms Recommendations for care
< or = 6 Mild Discharge to out patient management from GP and community midwife
7–11 Moderate Consider admission depending on woman’s preferences
> 12 Severe Recommend admission
Table 3. Suggested management options

RESEARCH AND EDUCATION
offered social support via a weekly telephone call. Overall the calls were seen as very acceptable by the women; they were not intrusive and in many cases were preferred to con-tact face to face with health care providers because of their informality. Using the telephone allowed for better rapport with the women as many of the barriers to successful com-munication already mentioned were eliminated. Women felt more comfortable in their own surrounding and therefore more in control of the conversation. This suggests that the telephone is potentially an efficient and cost-effective method of providing ongoing social support to women suffering from severe NVP in a private and non-stigmatizing way once they have been discharged from hospital. Women would have the opportunity to ask questions, relay fears or anxieties and at the same time be reassured and have advice and information reinforced.
By giving ongoing encouragement and support it may be possible to help empower women to be able to cope and carry on at home, whereas if discharged without sup-port they are likely to feel vulnerable, isolated and alone and may not have the strength or motivation to persevere with self help strategies, reverting back to old habits or not complying with medication. Such calls should therefore be considered as a viable option for supporting women with NVP/HG and their merits tested and validated by rand-omized controlled trials.
The major obstacle in providing such a service is that calls
may be hindered due to dialect and language barriers and an effective way to overcome these would have to be found.
Conclusions and recommendationsSevere NVP/HG can have a dramatic effect on the physical and mental health of women and results in a marked reduc-tion in their quality of life. The aetiology remains unknown and as such the most appropriate care and treatment remains unproven.
As a result many women have multiple admissions and a poor experience within the health care system. Appropriate assessment of the severity of symptoms would ensure that only women requiring medical care received it, hence reduc-ing the number of hospital attendances. At the same time women are likely to need psychological and social support and may benefit from the integration of alternative therapies with traditional medicine. By engaging effectively with women and giving information, advice and listening to concerns, either face to face or via the telephone, midwives can offer reassurance and increase knowledge, confidence, self-esteem and coping skills. This could enable and empower women to manage their symptoms more effectively, giving them the strength and resolve to persevere and try new approaches to alleviate symptoms. Initially extra resources may be needed to enable midwives to offer this support. However, the eco-nomic rewards gained due to fewer hospital attendances and admissions are more than likely to outweigh the costs. This
284 BRITISH JOURNAL OF MIDWIFERY, MAY 2008, VOL 16, NO 5

RESEARCH AND EDUCATION
evidence highlights the need to view psychological and social support with similar importance to the physical treatment of conditions such as NVP/HG, and emphasises the require-ment for good quality intervention studies in this area. BJM
Acupuncture Research Resource Centre (2004) Nausea and vomiting in pregnancy, evidence for the effectiveness of Acupuncture. Agren A, Berg M (2006) Tactile massage and severe nausea and vomiting during pregnancy – women’s experiences. Scandinavian Journal of Caring Sciences 20(2): 169–76Bailit JL (2005) Hyperemesis gravidarium: Epidemiologic findings from a large cohort. American Journal of Obstetrics and Gynecology 193(3): 811–4Baker D, Taylor H, the Alspac Survey Team (1997) The Relationship Between Condition Specific Morbidity, social Support and Maternal Deprivation in Pregnancy and Early Motherhood. Social Science & Medicine 45(9): 1325–36Buckwalter JG, Simpson SW (2002) Psychological factors in the etiol-ogy and treatment of severe nausea and vomiting in pregnancy. American Journal of Obstetrics and Gynecology 186(5): S210–S214Bullock LF, Browning C, Geden E (2002) Telephone Social Support for low-income pregnant women. Journal of Obstetrics, Gynaecology and neona-tal nursing 31(6): 658–64Carlsson CPO, Axemo P, Bodin A, Carstensen H, Ehrenroth B, Madegard-Lind I, Navander C (2000) Manual acupuncture reduces hyperemesis gravi-darum: A placebo-controlled, randomized, single-blind, crossover study. Journal of Pain and Symptom Management 20(4): 273–9Cobb S (1976) Social support as a moderator of life stress.Psychosomatic Medicine 38: 300–13Davis M (2004) Nausea and vomiting of pregnancy - An evidence-based review. Journal of Perinatal & Neonatal Nursing 18(4): 312–28Deuchar N (1995) Nausea and Vomiting in Pregnancy - a Review of the Problem with Particular Regard to Psychological and Social Aspects. British Journal of Obstetrics and Gynaecology 102(1): 6–8Dodds L, Fell DB, Joseph KS, Allen VM, Butler B (2006) Outcomes of pregnancies complicated by hyperemesis gravidarum. Obstetrics and Gynecology 107(2): 285–92Eliakim R, Abulafia O, Sherer DM (2000) Hyperemesis gravidarum: A cur-rent review. American Journal of Perinatology 17(4): 207–18Fairweather D (1968) Nausea and vomiting in pregnancy. American Journal of Obstetrics and Gynaecology 102:135–75Hupcey JH (1998) clarifying the social support theory-research linkage. Journal of Advanced Nursing 27: 1231–41Iancu I, Kotler M, Spivak B, Radwan M, Weizman A (1994) Psychiatric Aspects of Hyperemesis Gravidarum. Psychotherapy and Psychosomatics 61(3-4): 143–9Jakeway J (2001) Hyperemesis Gravidarum Not just mornign sickness! The Practising Midwife 4(10): 14–5Jewell D, Young G (2003) Interventions for nausea and vomiting in early pregnancy (Cochrane Review). The Cochrane Library, (3)Kirmayer L, Looper K (2006) Abnormal illness behaviour: physiologi-cal, psychological and social dimensions of coping with distress. Current Opinion in Psychiatry 19(1): 54–60Klebanoff MA, Mills JL (1986) Is vomiting during pregnancy teratogenic? British Medical Journal 292: 724–6Koren G, Piwko C, Ahn E, Boskovic R, Maltepe C, Einarson A, Navioz Y, Ungar WJ (2005) Validation studies of the Pregnacny Unique-Quantification of Emesis (PUQE) scores. Journal of Obstetrics and Gynaecology 25(3): 241–44Koren G, Boskovic R, Hard M, Maltepe C, Navioz Y, Einearson A (2002) Mortherisk-PUQE (pregnancy-unique quantification of emesis and nausea) scoring system for nausea and vomiting of pregnancy. American Journal of Obstetrics and Gynecology 186(5): S228–231Malterud K (1999) The (gendered) construction of diagnosis interpreta-tion of medical signs in women patients Theoretical Medicine and Bioethics 20(3): 275–86Mazzotta P, Magee LA (2000) A risk-benefit assessment of pharmacological and nonpharmacological treatments for nausea and vomiting of pregnancy. Drugs 59(4): 781–800McLeod A, Baker D, Black M (2006) Investigating the nature of formal social support provision for young mothers in a city in the North West of England. Health and Socail Care in the Community 14(6): 453–64
Mulder EJ, Robles de Medina PG, Huizink AC, Van den Bergh BR, Buitelaar JK, Visser GH (2002) Prenatal Maternal Stress: effects on preg-nancy and the (unborn) child. Early Human Development 70: 3–14Munch S, Schmitz MF (2006) Hyperemesis gravidarum and patient satis-faction: A path model of patients’ perceptions of the patient-physician rela-tionship. Journal of Psychosomatic Obstetrics and Gynecology 27(1): 49–57National Collaborative Centre for Women’s and Children’s Health (2003) Antenatal Care, Routine care for the healthy pregnant woman Portnoi G, Chng L-A, Karimi-Tabesh L, Kore G, Tan MP, Einarson A (2003) Prospective comparative study of the safely and effectiveness of ginger for the treatment of nausea and vomiting in pregnancy. American Journal of Obstetrics and Gynecology 189(5): 1374–7Rietveld S, Brosschot J (1999) Current persectives on symptom perception in asthma: a biomedical and psychological review. International Journal of Behvioral Medicine 6(2): 120–34Salmon P, Woloshynowych M, Valori R (1996) The measurement of beliefs about physical symptoms in English general prectice patients. Social Science & Medicine 42(11): 1561–7Sherman PW, Flaxman SM (2002) Nausea and vomiting of pregnancy in an evolutionary perspective. American Journal of Obstetrics and Gynecology 186(5): S190–S197Soltani H, Taylor FM (2003) Changing attitudes and perceptions to hyper-emesis gravidarum. Midwives 6(12): 520–5Stroebe W (2000) Social Psychology and Health. Buckingham. Open University Press, PhiladelphiaStrong TH (2001) Alternative therapies of morning sickness. Clinical Obstetrics and Gynecology 44(4): 653–60Swallow BL, Lindow SW, Aye M, Masson EA, Alasalvar C, Quantick P, Hanna J (2005) Smell perception during early pregnancy: no evidence of an adaptive mechanism. Bjog-an International Journal of Obstetrics and Gynaecology 112(1): 57–62Verberg MFG, Gillott DJ, Al-Fardan N, Grudzinskas JG (2005) Hyperemesis gravidarum, a literature revie. Human Reproduction Update 11(5): 527–39Vutyabanich T, Kraisarin T, Ruangsri R-A (2001) Ginger for Nausea and Vomiting in Pregnancy: Randomised, double-Masked, Placebo-Controlled Trial. The American college of Obstetricians and Gynecologists 97(4): 577–582Weigel RM, Weigel MM (1989) Nausea and vomiting of early pregnancy and pregnancy outcome. A meta-analytical review. British Journal of Obstetrics and Gynaecology 96: 1312–8Whitehead SA, Andrews PL, Chamberlain GV (1992) Characterisation of nausea and vomiting in early pregnancy: a survey of 1000 women. Journal of Obstetrics and Gyneacology 12: 364–9Whitty P, Browne S, Clarke M, McTigue O, Waddington, Kinsella T, Larkin C, O’Callaghan E (2004) Systematic comparison of subjective and objective measures of quality of life ant 4-year follow-up subsequent to a first episode of psychosis. Journal of Nervous and Mental Disease 192(12): 805–9
Key Points� Nausea and vomiting in pregnancy is a frequently occurring,
often debilitating condition that has a substantial impact on women’s quality of life and health care resources.
� Sufferers often feel isolated, depressed and lonely, are treated unsympathetically and have a poor experience of the health care system.
� Management is inconsistent and often not evidence based. The need for alternative non-pharmacological management approaches has been identified as a research priority.
� Appropriate assessment of severity, the use of alternative as well as traditional therapies and approaches which take into account social, psychological and biological factors are likely to be of benefit.
� Use of a telephone helpline which is staffed be midwives may be one method of providing additional social, psychological and emotional support required by women.
BRITISH JOURNAL OF MIDWIFERY, MAY 2008, VOL 16, NO 5 285