Embed Size (px)
Citation preview
1
Emergency Medicine
Prehospital Post Arrest CareAHA Strive to Revive 2017November 3, 2017
Jon Rittenberger, MD, MSDepartment of Emergency MedicineUniversity of Pittsburgh
Emergency Medicine
Disclosures - Rittenberger• Employers:
– University of Pittsburgh
– UPMC
• Grants:
– Mallincrodt, LLC (inhaled NO study)
– BrainCool, LLC (surface cooling device study)
– Laerdal Foundation (early EEG study)
– AHA Innovation Award (Rehabilitation after cardiac arrest)
– AHA Grant in Aid (Neurostimulants after cardiac arrest)
– NIH/NINDS (NETT and SIREN research consortia)
2
Emergency Medicine
Outline
• Preventing the ”Crump”
• Treating the etiology
• Resuscitate the Brain
Emergency Medicine
• 64M arrests on treadmill at YMCA
• Bystander calls 911, applies AED with shock *1
• ALS arrives to find asystolic
• Receives 3mg IV epinephrine, shock *2 with
ROSC
3
Emergency Medicine
Emergency Medicine
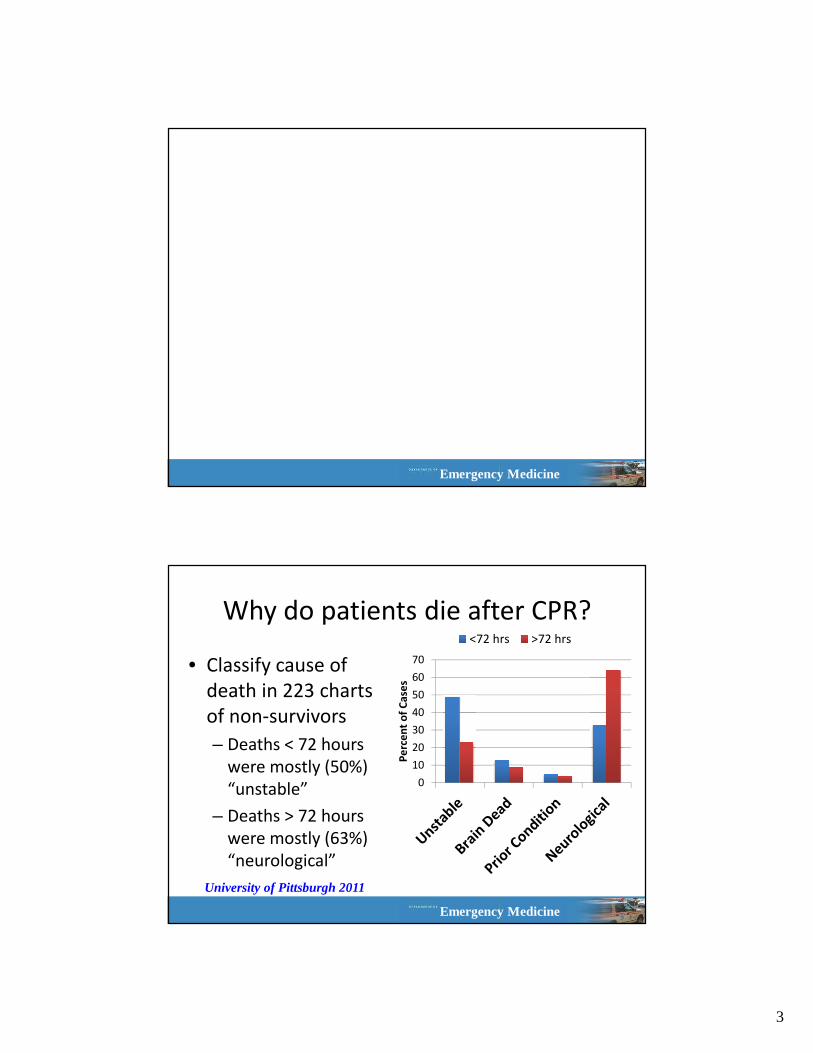
Why do patients die after CPR?
• Classify cause of
death in 223 charts
of non-survivors
– Deaths < 72 hours
were mostly (50%)
“unstable”
– Deaths > 72 hours
were mostly (63%)
“neurological”
0
10
20
30
40
50
60
70
Pe
rce
nt
of
Ca
ses
<72 hrs >72 hrs
University of Pittsburgh 2011
4
Emergency Medicine
The Crump!
Emergency Medicine
Goals?
SBP>100mmHg
SpO
2>90
%
HR>0
5
Emergency Medicine
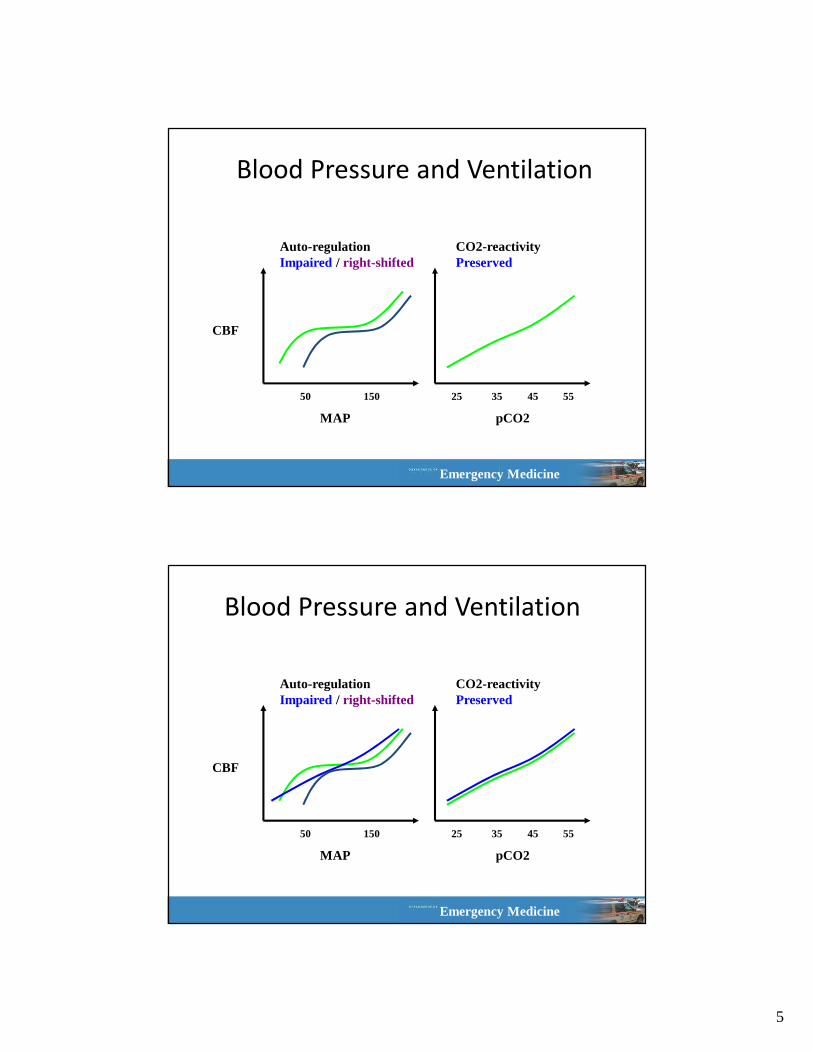
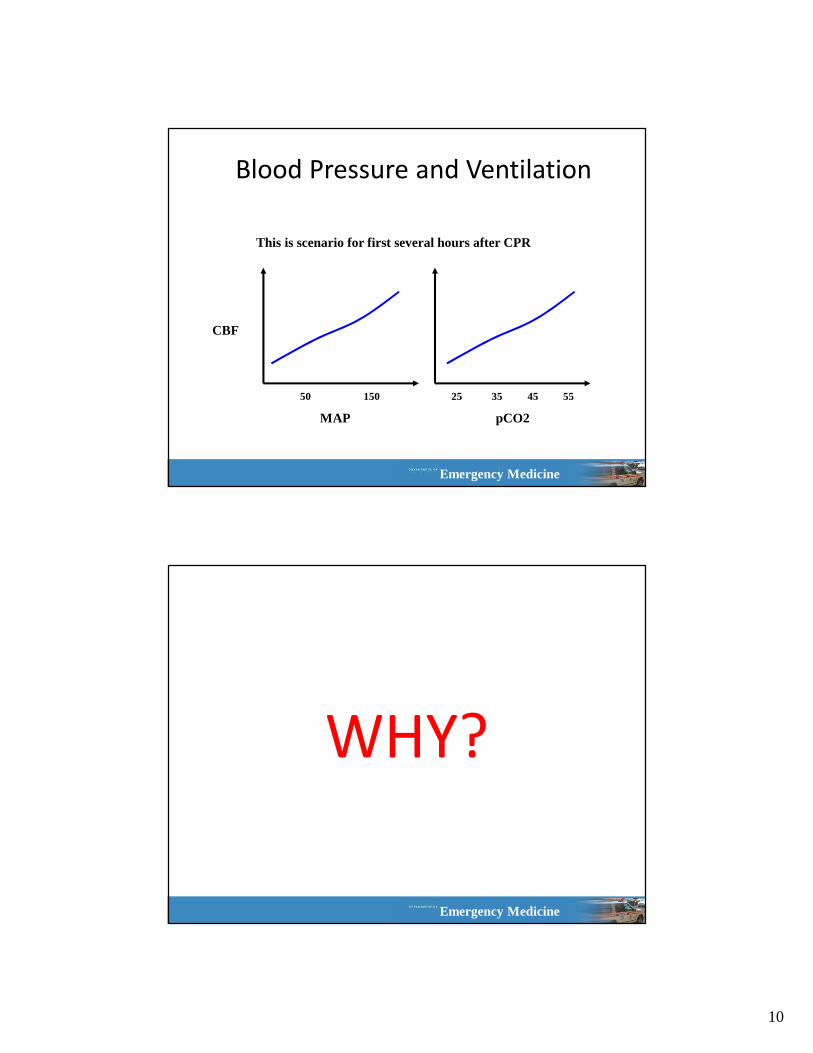
Blood Pressure and Ventilation
MAP
CBF
pCO2
50 150 25 35 45 55
Auto-regulationImpaired / right-shifted
CO2-reactivityPreserved
Emergency Medicine
Blood Pressure and Ventilation
MAP
CBF
pCO2
50 150 25 35 45 55
Auto-regulationImpaired / right-shifted
CO2-reactivityPreserved
6
Emergency Medicine
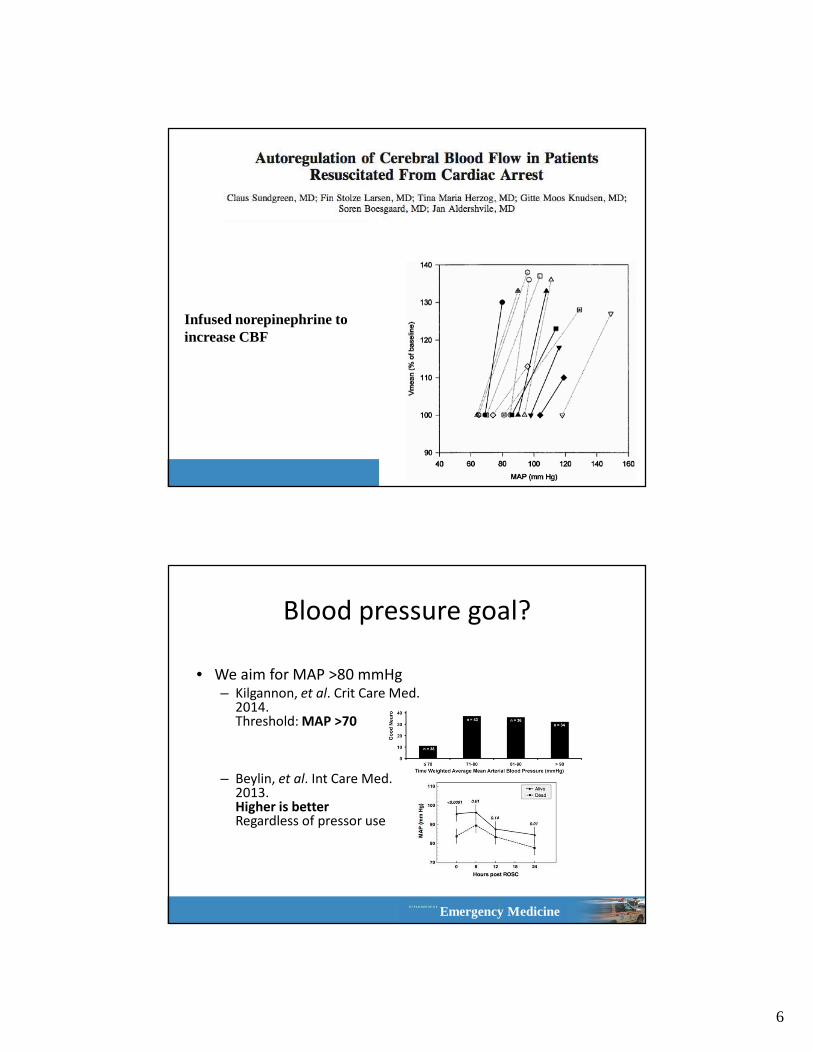
Infused norepinephrine to increase CBF
Emergency Medicine
Blood pressure goal?
• We aim for MAP >80 mmHg– Kilgannon, et al. Crit Care Med.
2014.Threshold: MAP >70
– Beylin, et al. Int Care Med. 2013. Higher is betterRegardless of pressor use
7
Emergency Medicine
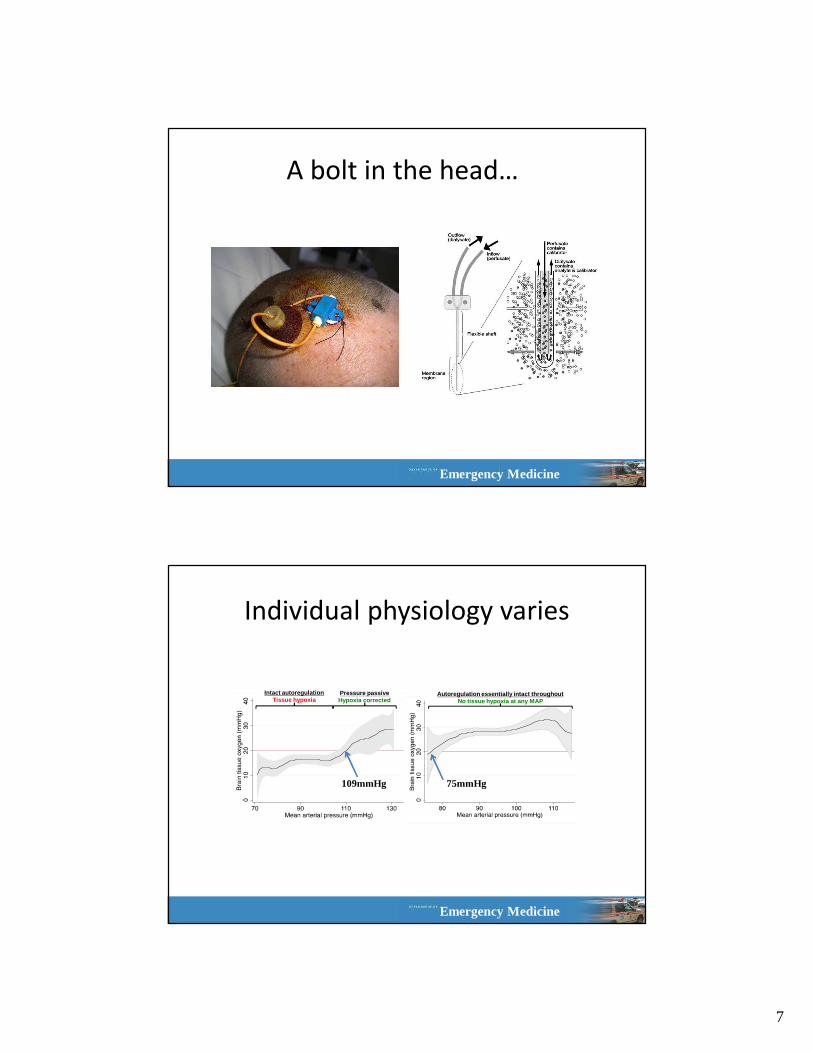
A bolt in the head…
Emergency Medicine
Individual physiology varies
Intact autoregulationTissue hypoxia
Pressure passiveHypoxia corrected
Autoregulation essentially intact throughoutNo tissue hypoxia at any MAP
109mmHg 75mmHg
8
Emergency Medicine
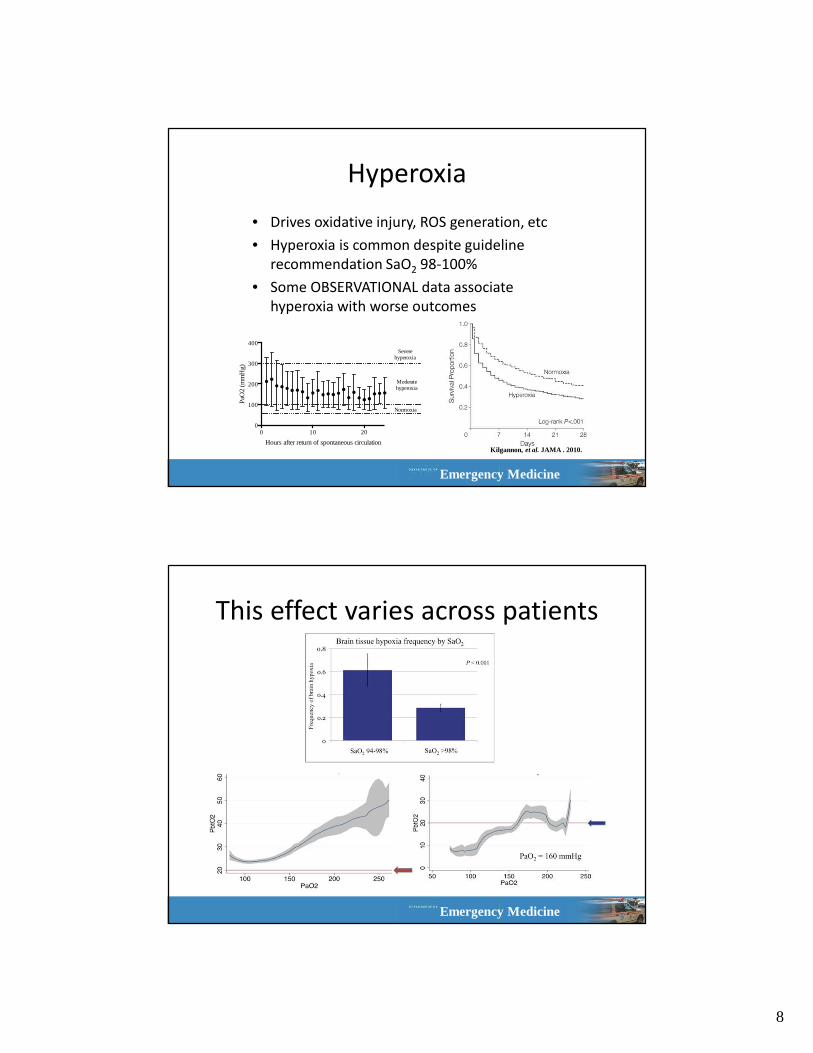
Hyperoxia
• Drives oxidative injury, ROS generation, etc
• Hyperoxia is common despite guideline
recommendation SaO2 98-100%
• Some OBSERVATIONAL data associate
hyperoxia with worse outcomes
0 10 200
100
200
300
400
Hours after return of spontaneous circulation
PaO
2 (m
mH
g)
Severe hyperoxia
Moderate hyperoxia
Normoxia
Kilgannon, et al. JAMA . 2010.
Emergency Medicine
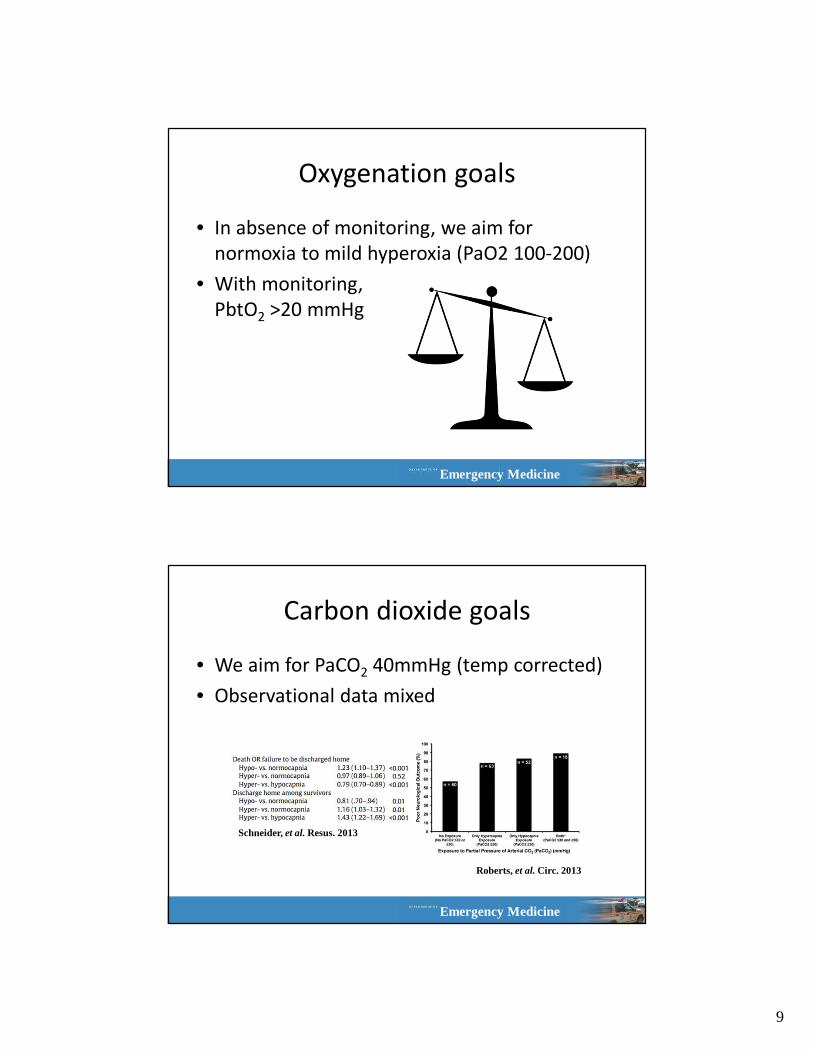
This effect varies across patients
9
Emergency Medicine
Oxygenation goals
• In absence of monitoring, we aim for
normoxia to mild hyperoxia (PaO2 100-200)
• With monitoring,
PbtO2 >20 mmHg
Emergency Medicine
Carbon dioxide goals
• We aim for PaCO2 40mmHg (temp corrected)
• Observational data mixed
Roberts, et al. Circ. 2013
Schneider, et al. Resus. 2013
10
Emergency Medicine
Blood Pressure and Ventilation
MAP
CBF
pCO2
50 150 25 35 45 55
This is scenario for first several hours after CPR
Emergency Medicine
WHY?
11
Emergency Medicine
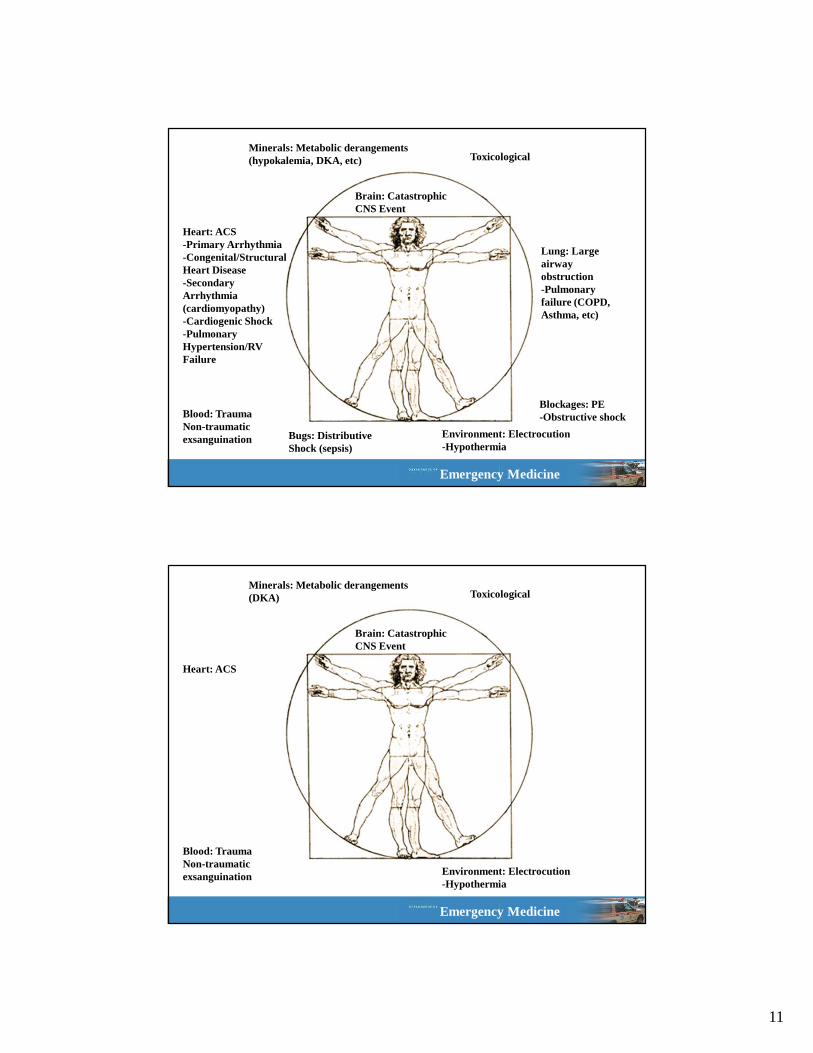
Brain: Catastrophic CNS Event
Heart: ACS-Primary Arrhythmia-Congenital/Structural Heart Disease-Secondary Arrhythmia (cardiomyopathy)-Cardiogenic Shock-Pulmonary Hypertension/RV Failure
Lung: Large airway obstruction-Pulmonary failure (COPD, Asthma, etc)
Blood: TraumaNon-traumatic exsanguination
Blockages: PE-Obstructive shock
Minerals: Metabolic derangements (hypokalemia, DKA, etc)
Bugs: Distributive Shock (sepsis)
Toxicological
Environment: Electrocution-Hypothermia
Emergency Medicine
Brain: Catastrophic CNS Event
Heart: ACS
Blood: TraumaNon-traumatic exsanguination
Minerals: Metabolic derangements (DKA) Toxicological
Environment: Electrocution-Hypothermia
12
Emergency Medicine
Emergency Medicine
• Stenting or coronary bypass surgery (CABG) followed
CATH
– 34/42 (81%) STEMI
– 30/54 (55%) nonSTEMI cases.
• Intraaortic Balloon Pump (IABP) was used
– 16/42 (38%) STEMI
– 18/54 (33%) nonSTEMI cases.
• LV assist device (LVAD), or transplantation for
– 4/42 (9.5%) STEMI
– 10/54 (19%) nonSTEMI cases.
13
Emergency Medicine
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Early
CATH
Delayed
+ No
CATH
Early
CATH
Delayed
+ No
CATH
Early
CATH
Delayed
+ No
CATH
Early
CATH
Delayed
+ No
CATH
Early
CATH
Delayed
+ No
CATH
All Type I Type II Type III Type IV
Mo
rta
lity
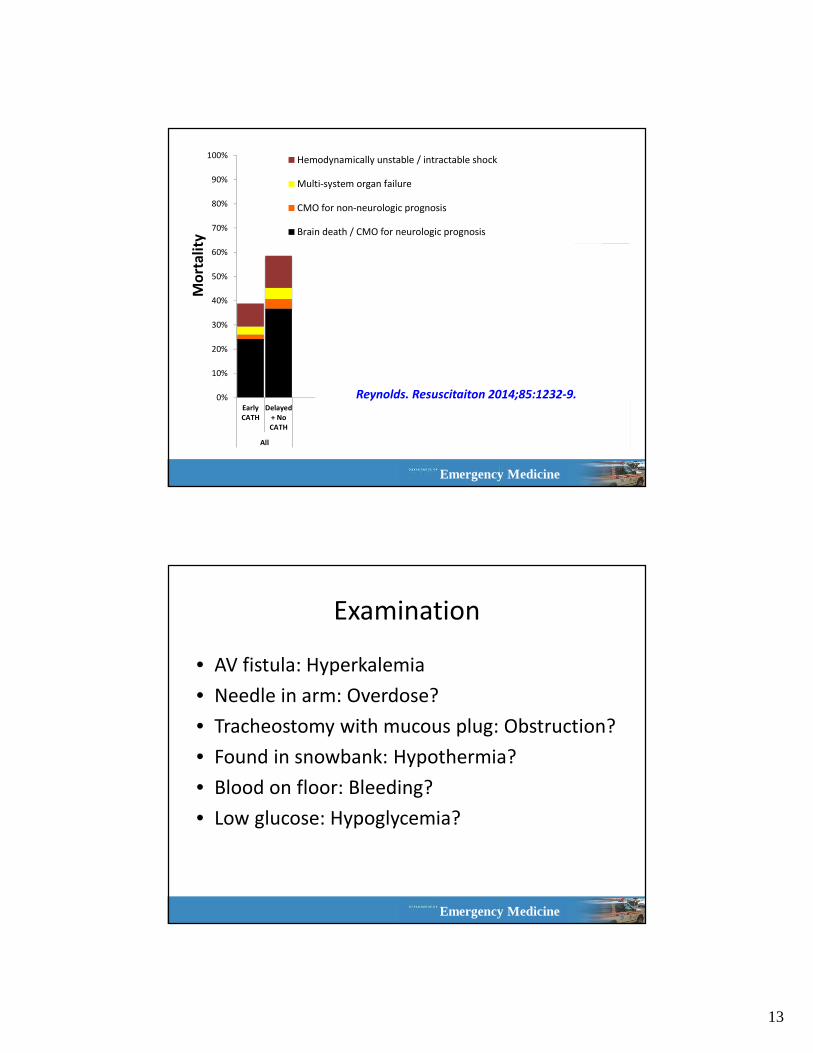
Hemodynamically unstable / intractable shock
Multi-system organ failure
CMO for non-neurologic prognosis
Brain death / CMO for neurologic prognosis
Reynolds. Resuscitaiton 2014;85:1232-9.
Emergency Medicine
Examination
• AV fistula: Hyperkalemia
• Needle in arm: Overdose?
• Tracheostomy with mucous plug: Obstruction?
• Found in snowbank: Hypothermia?
• Blood on floor: Bleeding?
• Low glucose: Hypoglycemia?
14
Emergency Medicine
Emergency Medicine
“Primum Non Nocere”
15
Emergency Medicine
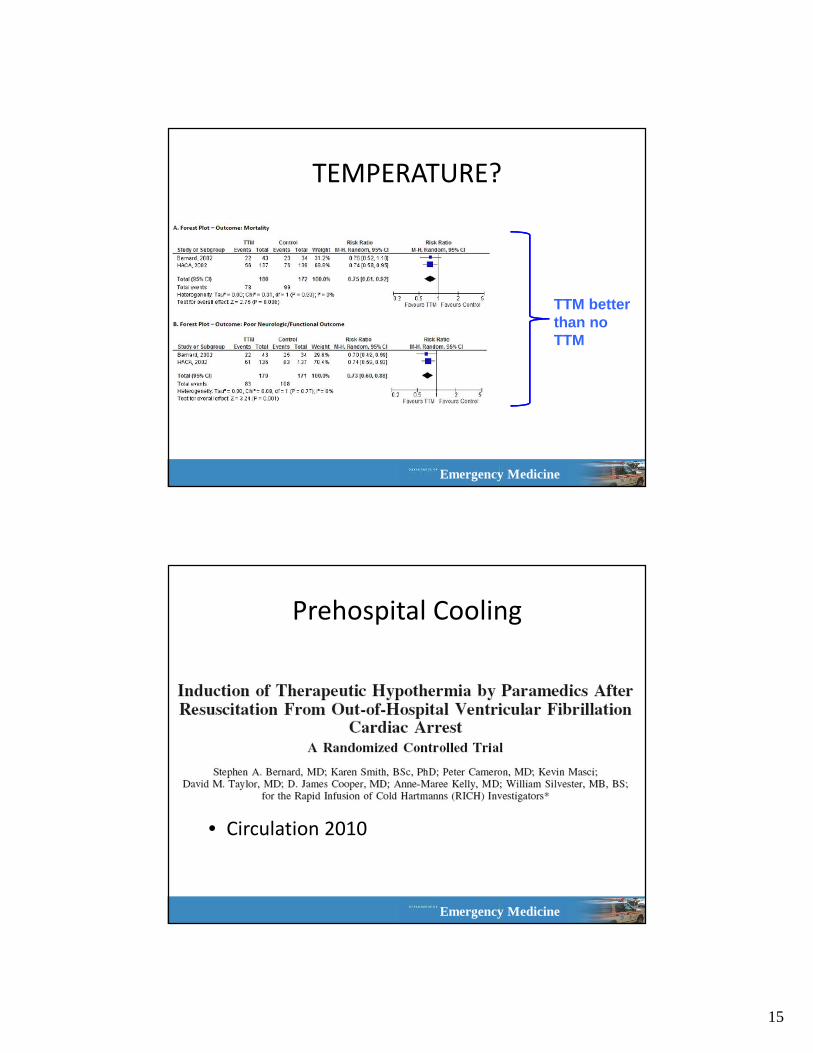
TTM better than no TTM
TEMPERATURE?
Emergency Medicine
Prehospital Cooling
• Circulation 2010
16
Emergency Medicine
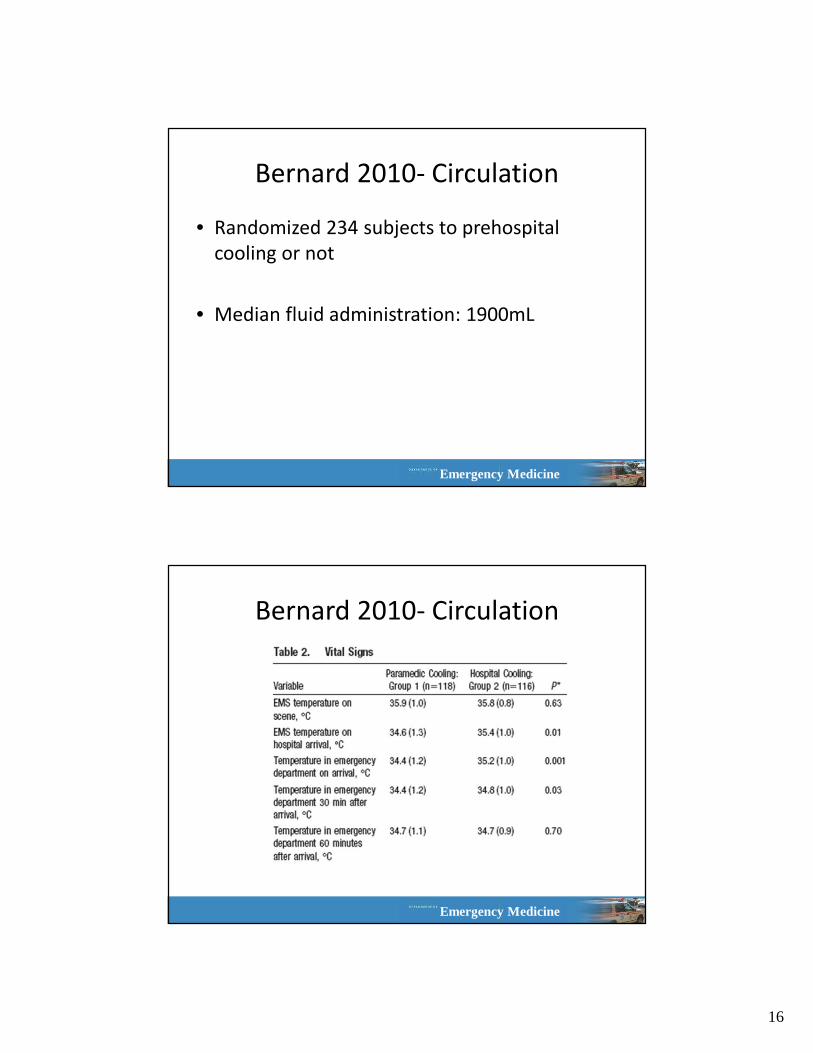
Bernard 2010- Circulation
• Randomized 234 subjects to prehospital
cooling or not
• Median fluid administration: 1900mL
Emergency Medicine
Bernard 2010- Circulation
17
Emergency Medicine
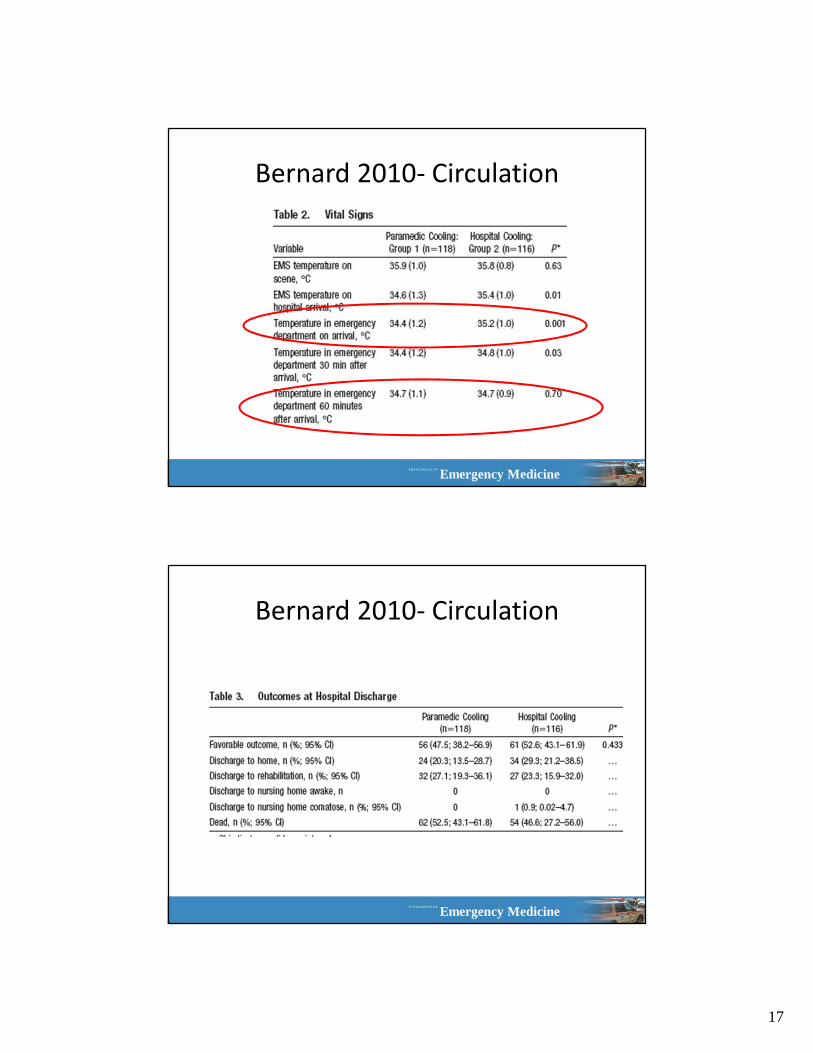
Bernard 2010- Circulation
Emergency Medicine
Bernard 2010- Circulation
18
Emergency Medicine
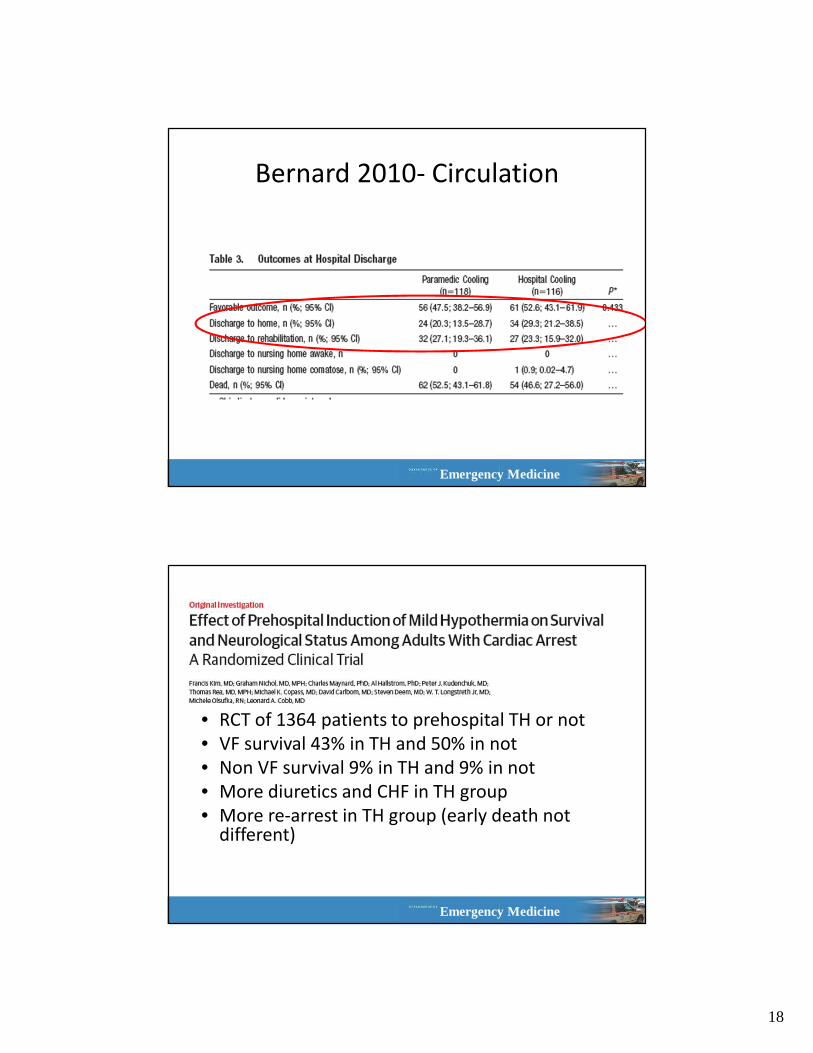
Bernard 2010- Circulation
Emergency Medicine
• RCT of 1364 patients to prehospital TH or not
• VF survival 43% in TH and 50% in not
• Non VF survival 9% in TH and 9% in not
• More diuretics and CHF in TH group
• More re-arrest in TH group (early death not different)
19
Emergency Medicine
Emergency Medicine
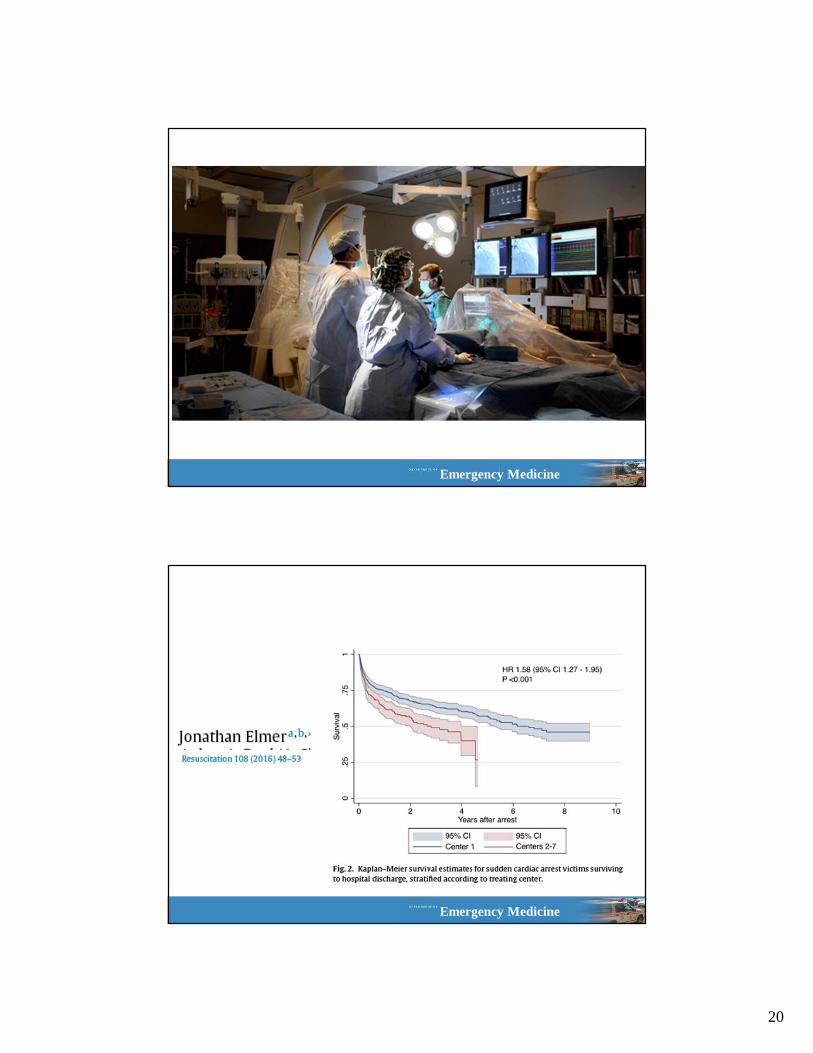
20
Emergency Medicine
Emergency Medicine
21
Emergency Medicine
What is our Cardiac Arrest Center?
• Comprehensive post
arrest care
– Early aggressive
resuscitation
– Temperature management
– Coronary revascularization
– Prognostication
– Secondary prevention
– Rehabilitation
– Teach CPR to survivors and
their families
• Feedback to providers
and referring physicians
• Referral to survivor
support groups
• Research infrastructure
to generate new
knowledge
• System-wide quality
control and
improvement
• Survivor celebrations
Emergency Medicine
Take Home
• First, prevent the re-arrest
– Optimize organ oxygenation/perfusion
• Start working on the etiology
– Fix what you can (i.e. bleeding, hypoglycemia,
popsickles)
• Make sure they go to the right place
22
Emergency Medicine
Thanks for your time!


























![Prehospital induced hypothermia post cardiac arrest jun 2010[1]](https://img.pdfslide.net/doc/110x75/554b6148b4c905e9388b5417/prehospital-induced-hypothermia-post-cardiac-arrest-jun-20101.jpg)