Embed Size (px)
Citation preview

Shorter communication
Preliminary tests of a cognitive model of generalizedanxiety disorder
Adrian Wells a, *, Karin Carter b
aUniversity of Manchester, Department of Clinical Psychology, Rawnsley Building, Manchester Royal In®rmary,
Manchester M13 9WL, UKbSalford NHS Trust, Manchester, UK
Received 17 July 1998
Abstract
Although worry is the central feature of Generalised Anxiety Disorder (GAD), little is known aboutthe factors that contribute to pathological or problematic worry. In a recent cognitive model of GAD,Wells, A. (1995) proposed that negative appraisal of worrying itself (meta-worry or type 2 worry) shouldbe distinguished from other types of worrying (type 1 worry). A central feature of this model is the ideathat individuals with GAD hold rigid positive beliefs about the usefulness of worrying as a copingstrategy. However, these individuals also hold negative beliefs and appraise worrying as uncontrollableand dangerous. This combination of cognitions and associated responses leads to an increased frequencyand generality of worrying, and thus to the pathological worry characteristic of GAD. This paperreports a preliminary test of the hypothesis that meta-worry contributes to problematic and pathologicalworrying, and this relationship is independent of the frequency of other types of worry. In testing forassociations between worry dimensions we controlled for overlaps with Trait anxiety, and thecontrollability of worrying. Results of a series of regression analyses support the hypothesis thatpathological worry is associated with meta-worry and this association is independent of Trait-anxietyand type 1 worry. The clinical implications of these data are brie¯y discussed. # 1999 ElsevierScience Ltd. All rights reserved.
Keywords: Generalised anxiety disorder; Worry; Meta-cognition; Cognitive model; Cognitive therapy
Behaviour Research and Therapy 37 (1999) 585±594
0005-7967/99/$ - see front matter # 1999 Elsevier Science Ltd. All rights reserved.PII: S0005-7967(98)00156-9
BEHAVIOURRESEARCH AND
THERAPY
PERGAMON
* Corresponding author. Tel.: +44-161-276-5399; Fax: +44-161-273-2135; E-mail: [email protected]
1. Introduction
Generalised Anxiety Disorder is a common and disabling condition that is di�cult to treat.The prevalence rate of GAD is approximately 3% in community samples increasing to 5%over life (DSM-IV, APA, 1994). The central feature of GAD is chronic worry (DSM-IIIR,APA, 1987). However, worry is not only a feature of GAD but contributes to other emotionaldisorders as well. A better understanding of worry is likely to inform our understanding ofother emotional disorders. For example, Wells and Matthews (1994) have advanced a cognitiveattentional model of emotional vulnerability in which perseverative self-relevant worry is acharacteristic processing style of distress-prone individuals. Potentially important distinctionshave been made between worry and other types of thought (Borkovec & Inz, 1990; Wells,1994a; Wells & Morrison, 1994) and worry has been shown to be associated with particularcognitive, physiological and a�ective experiences (Borkovec, 1994; Wells & Papageorgiou,1995).Although there have been recent advances in our understanding of the phenomenon of
worry, this has not been paralleled by advances in the conceptualisation of GAD. GADremains a di�cult anxiety disorder to treat. Only approximately 50% of patients improve withcognitive behaviour therapy and there is considerable variability in the degree of improvement(Butler, Cullington, Hibbert, Klimes, & Gelder, 1987; Borkovec & Costello, 1993, Durham &Allan, 1993). The e�ectiveness of treatment could be improved if treatment was based on aspeci®c cognitive model of the maintenance of GAD. Such a model should centre on thecognitive and behavioural factors which maintain chronic worry. Aside from improvingtreatment e�ectiveness, a speci®c model could have advantages of leading to re®nements in theassessment of the nature of worry in GAD. Recently, Wells (1995, 1997) has advanced aspeci®c cognitive model of GAD which emphasises the role of meta-cognition. The presentpaper reports a study designed to test a central prediction of this model.
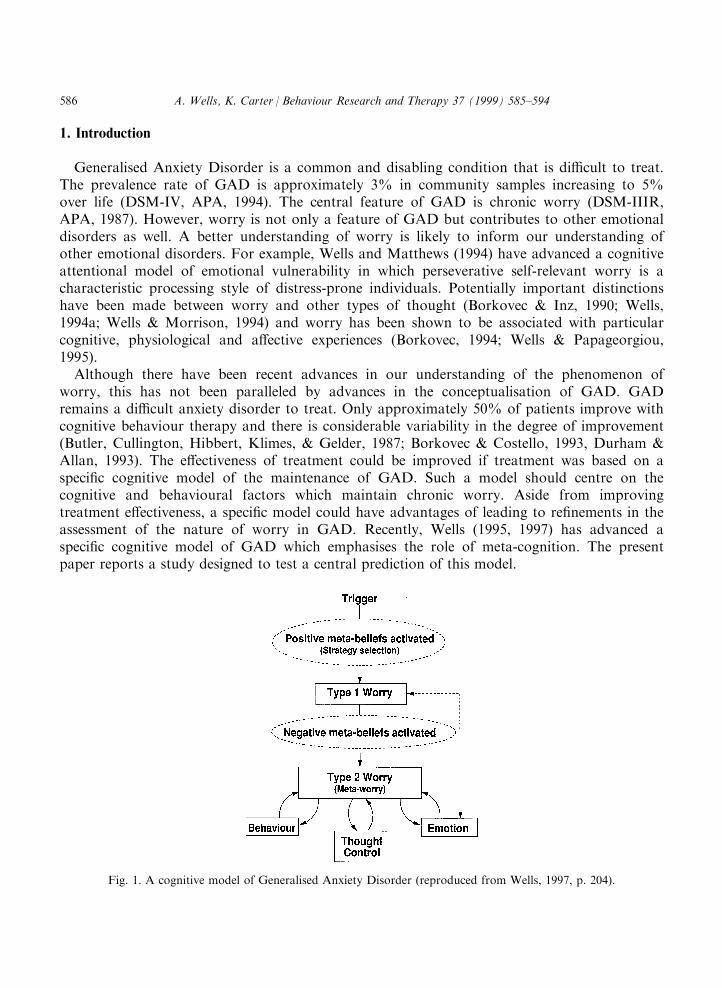
Fig. 1. A cognitive model of Generalised Anxiety Disorder (reproduced from Wells, 1997, p. 204).
A. Wells, K. Carter / Behaviour Research and Therapy 37 (1999) 585±594586
The central variables contributing to the development and maintenance of GAD in Wells'model, are depicted diagrammatically in Fig. 1.
Worry is a relatively normal cognitive process. However, in Wells' model, individuals withGAD are prone to execute worrying as a coping strategy in response to particular threatrelated triggers. These triggers are often intrusive negative thoughts e.g. after hearing a newsitem about a tra�c accident an individual may think ``what if my partner is involved in anaccident''. This trigger activates the individual's meta-cognitive beliefs and plans for coping.Individuals with GAD appear to have rigid positive beliefs about the advantages of usingworry as a coping strategy, and therefore select worrying as a means of generating a range ofcatastrophes and potential solutions. Type 1 worrying is thereby implemented. Type 1 worryingrefers to worrying about external events and noncognitive internal events such as physicalsymptoms. In the short-term, type 1 worrying may increase anxiety and associated cognitiveand somatic symptoms as depicted by the dotted arrow in Fig. 1. However, if worrying isexecuted over an extended time course, such that solutions to anticipated catastrophes arefound, then anxiety decreases. Individuals with GAD often use internal information such as a`feeling' that they will be able to cope in terminating worrying. The feedback route fromemotion back to type 1 worry shows that reductions in emotion following protracted worryingepisodes may reinforce the subsequent execution of type 1 worrying when future threatappraisals occur. In contrast, somatic symptoms of anxiety may be interpreted in a negativeway thus contributing to type 1 worries.
In this model GAD patients also develop negative beliefs about worrying. Once these beliefsare established, the individual with GAD is prone to develop negative appraisals of their ownworry activity. Such appraisals are known as type 2 worry or meta-worry. Type 2 worry isessentially worrying about worry. For example, the person with GAD may develop the beliefthat worrying could lead to a `mental breakdown' and this belief will give rise to negativeappraisal of the worry process once it is activated. Once type 2 worry is established, three setsof processes contribute to the generalised, distressing and uncontrollable worry characteristic ofGAD. These are depicted by the behaviour, thought control and emotion cells and the arrowslinking with them in Fig. 1.
Because the person with GAD negatively appraises worrying, behaviours are engaged whichare intended to avert the dangers of worrying. Often these are subtle behaviours such asavoidance of particular types of stimuli or situations that may trigger worrying, reassuranceseeking in an attempt to terminate worry episodes, and the use of distracting activities in orderto displace worry. These responses maintain type 2 worrying and negative belief. In particular,avoidance of situations reduces the available opportunities for discovering that type 2 worriesare inaccurate. Avoidance also maintains preoccupation with the triggering situations forworry. The termination of worrying through reassurance-seeking prevents the individual fromdiscovering that worrying is subject to voluntary control, and similar to avoidance, it removesthe opportunity to discover that severe and extended worrying is not catastrophic. The use ofdistraction also prevents the practise of alternative worry management strategies and preventsdiscon®rmation of belief in type 2 worries. For example, the nonoccurrence of catastropheassociated with worrying can be attributed to use of the distraction strategy rather than to thefact that catastrophe cannot occur.
A. Wells, K. Carter / Behaviour Research and Therapy 37 (1999) 585±594 587
The use and focus of direct thought control strategies is also important in the maintenanceof GAD. This is separated from behaviour in the model depicted in Fig. 1 since it requiresdetailed attention in formulating GAD cases. Because GAD patients hold positive beliefsabout worrying, often these individuals do not attempt to interrupt or discontinue the type 1worry process once it is activated since this would be equivalent to not coping. Thus, worryingmay be practised in a particular way that is intended to exploit the advantages of worryingwhilst avoiding the dangers. The dissonance between positive and negative worry beliefs isoften resolved in GAD by attempts to suppress intrusive thoughts that trigger the need toworry in the ®rst place. More speci®cally, rather than discontinuing the execution of the worryprocess, individuals with GAD tend to suppress thinking about worry triggers. For example,an individual who is currently prone to worry about a personal work situation will attempt notto think about work. However, if an intrusive thought about work arises the person with GADwill execute a worry routine in order to enhance con®dence in coping. Attempts to suppressthoughts (ie totally remove them from consciousness) is often problematic since it can lead to aresurgence of unwanted thoughts as demonstrated experimentally in thought suppressionstudies (e.g. Wegner, Schneider, Carter, & White, 1987). Moreover, the individual is targetingcontrol attempts at processes which are largely automated and may not be subject to highdegrees of control. In contrast, the execution of worry sequences is an executive activity that issubject to high degrees of control. In summary, the suppression of thoughts may lead to aresurgence of these thoughts thus reinforcing meta-worries concerning loss of control, andfailure to attempt interruptions of the worry sequence deprive the individual of controlexperiences that discon®rm meta-worries and negative beliefs concerning controllability.
Finally, when type 2 worries are activated (e.g. the person with GAD appraises his/herworrying as a sign of impending `mental breakdown') anxiety responses increase. Theseemotional symptoms may be interpreted as evidence supporting type 2 worry themes andnegative beliefs. When patients with GAD appraise their worry responses and associatedsymptoms as evidence of an immediate impending catastrophe, sudden increments in arousalconstituting panic attacks are the result. Moreover, the increase in anxiety symptoms thataccompany type 2 worry interfere with the individual attaining an internal state that normallysignals that it is safe to discontinue type 1 worrying. Thus, worrying is more likely to becomechronic and generalised as e�orts to achieve the sense that one can cope through the use oftype 1 worrying continue.
A central feature of the present model is the distinction between type 1 and type 2 worry.The model predicts that pathological worry characteristic of GAD should be correlated withboth types of worry. Furthermore, as type 2 worry is a central causal factor in the escalation,generalisation, and pathologising of worry, type 2 worry should predict pathological worryindependently of type 1 worry, but the converse should not apply.
Two separate dependent measures were used in the present study: the Penn-state worryquestionnaire (PSWQ: Meyer, Miller, Metzger, & Borkovec, 1990); and a measure of subjectiveproblem level associated with worrying. The PSWQ served as the principal measure ofpathological worry like that found in GAD. The measure has particular relevance to GADworries since it taps three central criteria of GAD worry: worry has to be chronic, excessive,and generalised.
A. Wells, K. Carter / Behaviour Research and Therapy 37 (1999) 585±594588
Proneness to type 1 and type 2 worries were measured with the Anxious Thoughts Inventory(AnTI: Wells, 1994b). This instrument has a meta-worry subscale assessing meta-cognitionssimilar to those implicated in the model. In particular, it measures worry about thoughts, andprocess dimensions of uncontrollability and repetitiveness of thinking.In order to test our principal hypothesis, that meta-worry contributes to pathological/
problematic worry, multiple regression analyses were run to test this against the simplestalternative: that pathological/problematic worry is caused by type 1 rather than type 2 worry.If the correlation between problem level/pathological worry and type 2 worries is dependent ontype 1 worry, the model is weak. However, if type 2 worry is an independent and strongerpredictor than type 1 worry, when all of the predictors are entered in the equation, the modelis upheld. In summary, type 2 worry should be associated with pathological worry/problemlevel independently of the inclusion of type 1 worry in the equation. To provide a conservativetest of this hypothesis we controlled for nonspeci®c e�ects that may be associated with generalanxiety proneness (trait-anxiety). We also ran tests controlling for other dimensions of worry.We controlled for the uncontrollability of worry in predicting pathological worry scores, andfor uncontrollability and the dimensions assessed by the PSWQ in predicting problem level. Ifthese other dimensions predict pathological, and problematic worry, but meta-worry does not,support for the model is weak. Although appraisals of uncontrollability represent onedimension of meta-worry in Wells' (Wells, 1995, 1997) model, stronger support for the modelwould be achieved if meta-worry predicted problematic worry independently of thesedimensions. If meta-worry is associated with pathological worry independently ofcontrollability then we can be more con®dent that the relationship is not a consequence ofdiminished control but is a consequence of appraisals.
2. Method
2.1. Subjects
One-hundred and forty subjects participated in the study. The subjects were studentsattending undergraduate and postgraduate university courses. The mean age of subjects was29.79 years (S.D. 8.70). One-hundred and six of the subjects were women and 34 were men.
2.2. Measures
2.2.1. Dependent variablesIn order to test hypotheses concerning the relative contribution of type 1 and type 2 worries
to pathological worry, the Penn-State Worry Questionnaire (PSWQ: Meyer et al., 1990), wasused as a dependent measure of pathological GAD-type worry. The PSWQ is a 16 itemmeasure of proneness to chronic, excessive and general worry. It has good psychometricproperties (a 0.97), and distinguishes patients with GAD from other anxiety disorders (Brown,Antony, & Barlow, 1993).A visual analogue (VAS) measure was constructed as a means of assessing the individual
problem level associated with worrying. This measure consisted of the item: ``How much is
A. Wells, K. Carter / Behaviour Research and Therapy 37 (1999) 585±594 589
worry a problem for you?'' and responses were requested on a scale with two anchor pointsranging from: 0 = ``not at all''; to 100 = ``very much so, could not be more''.
2.2.2. Independent variablesType 1 and type 2 worry proneness was assessed with the Anxious Thoughts Inventory
(AnTI: Wells, 1994b). The AnTI consists of 22 items assessing social and health (type 1) worryon separate subscales, and meta-worry (type 2) worry on a third subscale. The subscalescorrelate with other anxiety measures, and the a reliabilities range from 0.75 to 0.84. Whilst thecontent of situational worries is highly variable, and this diversity was re¯ected in the selectionof the initial items for the AnTI, only three categories reliably emerged from repeated analyses.It appears that most worries are reliably categorizeable in terms of these three basicdimensions.Subjects were also administered the Spielberger trait anxiety subscale (Spielberger, Gorsuch,
Lushene, Vagg, & Jacobs, 1983), a 20 item measure of anxiety proneness. The subscale has ana of 0.90 in college students.The controllability of worry was assessed by a VAS rating: ``How much control do you have
over your worries?'' using the following extreme anchor points: 0 for ``no control'' to 100 for``total control''.
2.3. Procedure
All subjects volunteered to participate after they had been introduced to the aims of thestudy. Subjects were informed that the study was intended to explore the characteristics ofworry. Each subject received a questionnaire battery with a cover page consisting of thefollowing orienting instructions: ``Most people worry from time to time. We are interested in®nding out some of the characteristics of people's worries and their attitudes towardsworrying''. The cover sheet also emphasised the anonymity of responses.
3. Results
The distribution of scores on the AnTI subscales were skewed, and so these data weresubject to log transformation prior to further analysis. Initially we computed simple (Pearson)correlations between predictor variables, and the dependent measures. All predictor variableswere signi®cantly correlated with the PSWQ and VAS rating of problem level. Thecorrelations, means and 95% con®dence limits for these variables are presented in Table 1.Consistent with our hypotheses both type 1 and type 2 worry were signi®cantly and
positively correlated with pathological worry and problem level. Type 2 worry accounted for48% of the variance in PSWQ score, and 40% of the variance in problem level. Type 1 worriesaccounted for 11±36% of the variance in PSWQ and 13±24% in problem level.Multiple regressions were run using forced entry to test for the independent contribution of
type 1 and type 2 worries to the dependent variables. Before proceeding we examined theintercorrelations between predictors to check for multi-collinearity, which was not a problem.
A. Wells, K. Carter / Behaviour Research and Therapy 37 (1999) 585±594590
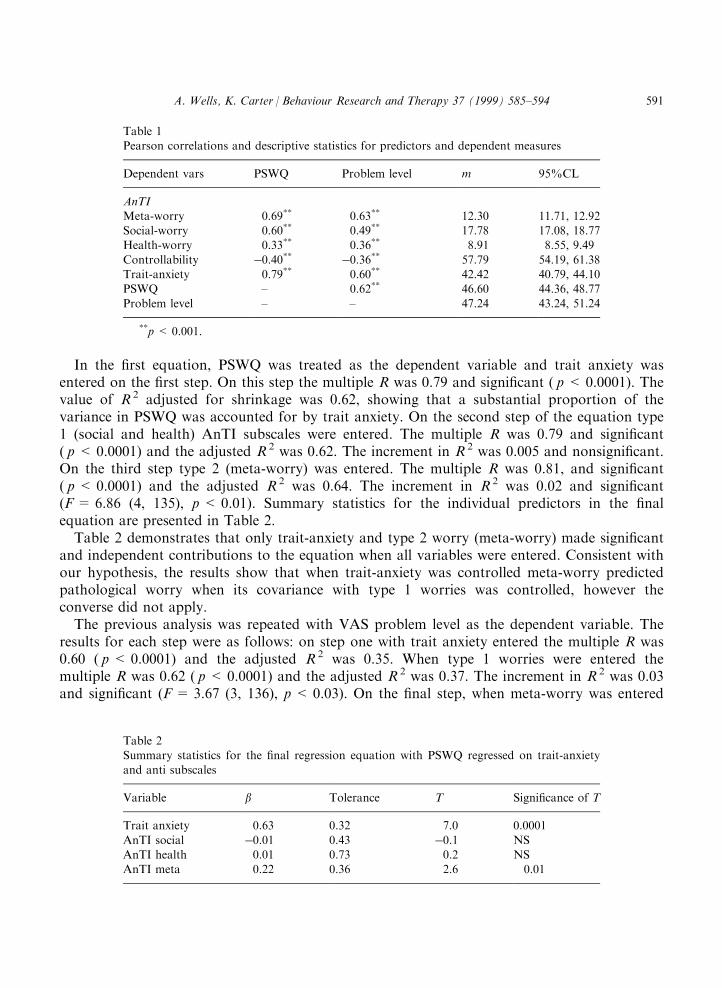
In the ®rst equation, PSWQ was treated as the dependent variable and trait anxiety wasentered on the ®rst step. On this step the multiple R was 0.79 and signi®cant ( p < 0.0001). Thevalue of R 2 adjusted for shrinkage was 0.62, showing that a substantial proportion of thevariance in PSWQ was accounted for by trait anxiety. On the second step of the equation type1 (social and health) AnTI subscales were entered. The multiple R was 0.79 and signi®cant( p < 0.0001) and the adjusted R 2 was 0.62. The increment in R 2 was 0.005 and nonsigni®cant.On the third step type 2 (meta-worry) was entered. The multiple R was 0.81, and signi®cant( p < 0.0001) and the adjusted R 2 was 0.64. The increment in R 2 was 0.02 and signi®cant(F= 6.86 (4, 135), p < 0.01). Summary statistics for the individual predictors in the ®nalequation are presented in Table 2.Table 2 demonstrates that only trait-anxiety and type 2 worry (meta-worry) made signi®cant
and independent contributions to the equation when all variables were entered. Consistent withour hypothesis, the results show that when trait-anxiety was controlled meta-worry predictedpathological worry when its covariance with type 1 worries was controlled, however theconverse did not apply.The previous analysis was repeated with VAS problem level as the dependent variable. The
results for each step were as follows: on step one with trait anxiety entered the multiple R was0.60 ( p < 0.0001) and the adjusted R 2 was 0.35. When type 1 worries were entered themultiple R was 0.62 ( p < 0.0001) and the adjusted R 2 was 0.37. The increment in R 2 was 0.03and signi®cant (F= 3.67 (3, 136), p< 0.03). On the ®nal step, when meta-worry was entered
Table 1Pearson correlations and descriptive statistics for predictors and dependent measures
Dependent vars PSWQ Problem level m 95%CL
AnTIMeta-worry 0.69** 0.63** 12.30 11.71, 12.92Social-worry 0.60** 0.49** 17.78 17.08, 18.77Health-worry 0.33** 0.36** 8.91 8.55, 9.49
Controllability ÿ0.40** ÿ0.36** 57.79 54.19, 61.38Trait-anxiety 0.79** 0.60** 42.42 40.79, 44.10PSWQ ± 0.62** 46.60 44.36, 48.77
Problem level ± ± 47.24 43.24, 51.24
**p < 0.001.
Table 2Summary statistics for the ®nal regression equation with PSWQ regressed on trait-anxietyand anti subscales
Variable b Tolerance T Signi®cance of T
Trait anxiety 0.63 0.32 7.0 0.0001
AnTI social ÿ0.01 0.43 ÿ0.1 NSAnTI health 0.01 0.73 0.2 NSAnTI meta 0.22 0.36 2.6 0.01
A. Wells, K. Carter / Behaviour Research and Therapy 37 (1999) 585±594 591
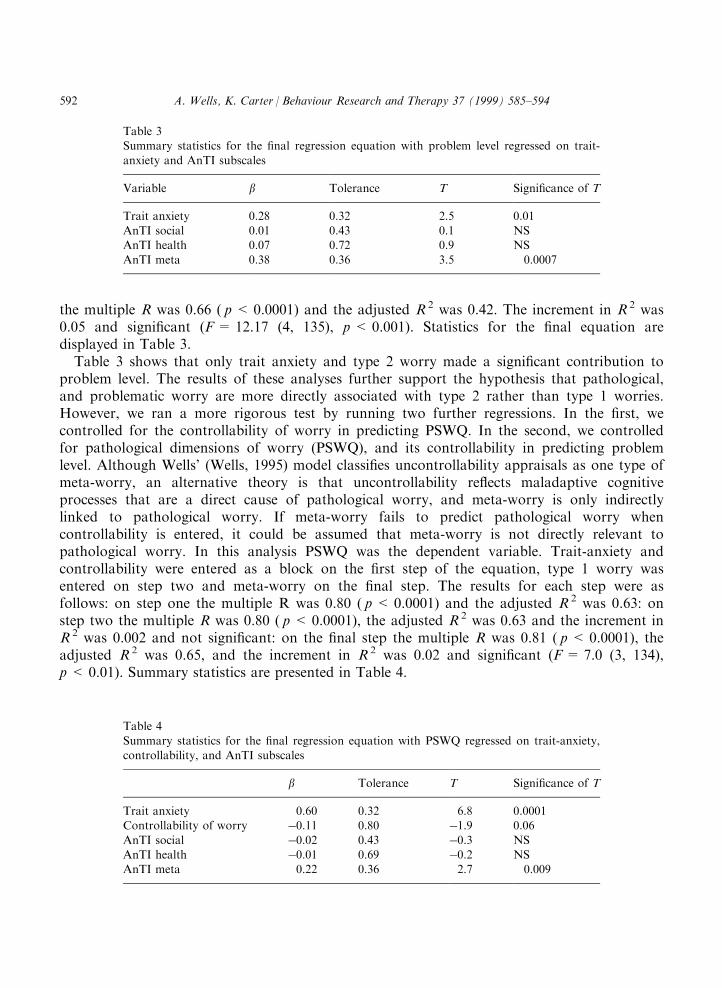
the multiple R was 0.66 ( p < 0.0001) and the adjusted R 2 was 0.42. The increment in R 2 was0.05 and signi®cant (F= 12.17 (4, 135), p < 0.001). Statistics for the ®nal equation aredisplayed in Table 3.Table 3 shows that only trait anxiety and type 2 worry made a signi®cant contribution to
problem level. The results of these analyses further support the hypothesis that pathological,and problematic worry are more directly associated with type 2 rather than type 1 worries.However, we ran a more rigorous test by running two further regressions. In the ®rst, wecontrolled for the controllability of worry in predicting PSWQ. In the second, we controlledfor pathological dimensions of worry (PSWQ), and its controllability in predicting problemlevel. Although Wells' (Wells, 1995) model classi®es uncontrollability appraisals as one type ofmeta-worry, an alternative theory is that uncontrollability re¯ects maladaptive cognitiveprocesses that are a direct cause of pathological worry, and meta-worry is only indirectlylinked to pathological worry. If meta-worry fails to predict pathological worry whencontrollability is entered, it could be assumed that meta-worry is not directly relevant topathological worry. In this analysis PSWQ was the dependent variable. Trait-anxiety andcontrollability were entered as a block on the ®rst step of the equation, type 1 worry wasentered on step two and meta-worry on the ®nal step. The results for each step were asfollows: on step one the multiple R was 0.80 ( p < 0.0001) and the adjusted R 2 was 0.63: onstep two the multiple R was 0.80 ( p < 0.0001), the adjusted R 2 was 0.63 and the increment inR 2 was 0.002 and not signi®cant: on the ®nal step the multiple R was 0.81 ( p < 0.0001), theadjusted R 2 was 0.65, and the increment in R 2 was 0.02 and signi®cant (F= 7.0 (3, 134),p < 0.01). Summary statistics are presented in Table 4.
Table 3Summary statistics for the ®nal regression equation with problem level regressed on trait-
anxiety and AnTI subscales
Variable b Tolerance T Signi®cance of T
Trait anxiety 0.28 0.32 2.5 0.01AnTI social 0.01 0.43 0.1 NSAnTI health 0.07 0.72 0.9 NS
AnTI meta 0.38 0.36 3.5 0.0007
Table 4
Summary statistics for the ®nal regression equation with PSWQ regressed on trait-anxiety,controllability, and AnTI subscales
b Tolerance T Signi®cance of T
Trait anxiety 0.60 0.32 6.8 0.0001Controllability of worry ÿ0.11 0.80 ÿ1.9 0.06
AnTI social ÿ0.02 0.43 ÿ0.3 NSAnTI health ÿ0.01 0.69 ÿ0.2 NSAnTI meta 0.22 0.36 2.7 0.009
A. Wells, K. Carter / Behaviour Research and Therapy 37 (1999) 585±594592

The results of this regression further support the hypothesised contribution of meta-worry topathological worry experiences. Only trait-anxiety and meta-worry made signi®cantindependent contributions to PSWQ scores when all variables were entered.Finally, we ran another regression with problem level regressed on Trait anxiety,
controllability, PSWQ, and the AnTI subscales. On step one, Trait anxiety, controllability andPSWQ were entered. The statistics for this step were as follows: the multiple R was 0.65( p < 0.0001) and the adjusted R 2 was 0.42. On step two, social and health (type 1) worrieswere entered. The multiple R was 0.67 ( p < 0.0001), the adjusted R 2 was 0.43, and theincrement in R 2 was 0.02 and not signi®cant. On the ®nal step meta-worry was entered and themultiple R was 0.69 ( p < 0.0001), the adjusted R 2 was 0.46, and the increment in R 2 was 0.03and signi®cant (F= 8.36 (6, 133), p < 0.005). Statistics for the ®nal regression are presented inTable 5.The summary data in Table 5 show that only meta-worry and PSWQ made independent
contributions to problem level.
4. Discussion
The results of this study support the hypothesis that pathological, and problematic worry isdirectly associated with type 2 (meta-worry) rather than type 1 worry. Even under rigorousconditions in which covariances with trait-anxiety and controllability were statisticallycontrolled, meta-worry was positively associated with pathological worry. In the ®nalregression analysis we controlled for pathological worry dimensions in predicting the degree towhich worry was a problem for the individual. By entering PSWQ as a predictor we partialledout the variance accounted for by the frequency and chronicity of worry. In this equationmeta-worry remained a signi®cant predictor of problem level. PSWQ was also independentlyand signi®cantly associated with problem level in this equation. This incidental ®nding isconsistent with Wells' cognitive model of GAD. The model proposes that worry becomesproblematic partially because it is consistently and frequently used as a coping strategy. Theemergence of meta-worry and the PSWQ as independent predictors of problem worry may be amarker for the tension that exists between negative and positive beliefs about worry.
Table 5Summary statistics for the ®nal regression equation with problem level regressed on trait-
anxiety, PSWQ, worry controllability and AnTI subscales
Variable b Tolerance T Signi®cance of T
Trait anxiety 0.08 0.24 0.6 NSPSWQ 0.30 0.34 2.8 0.006Controllability of worry ÿ0.08 0.78 ÿ1.1 NS
AnTI social 0.01 0.43 0.1 NSAnTI health 0.05 0.69 0.7 NSAnTI meta 0.31 0.34 2.9 0.005
A. Wells, K. Carter / Behaviour Research and Therapy 37 (1999) 585±594 593

The data suggests that modi®cation of meta-worry should be undertaken in the treatment ofpathological worry states such as GAD. This type of cognitive therapy has been described indetail elsewhere (Wells, 1995, 1997), and consists of a range of strategies for challenging beliefsin meta-worry and negative meta-beliefs. However, the model and treatment also emphasise theneed to restructure maladaptive positive beliefs about worry and explore with patientsalternative cognitive and behavioural strategies for appraising and dealing with threat. Furthertests of the cognitive model of GAD are required. In particular, future tests should usere®nements in the measurement of meta-worry and meta-beliefs (e.g. Cartwright-Hatton &Wells, 1997) and examine these dimensions in GAD patients.
References
American Psychiatric Association (1987). Diagnostic and Statistical Manual of mental disorders (3rd ed. revised). Washington, DC:
APA.
American Psychiatric Association (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: APA.
Borkovec, T. D. (1994). The nature, functions, and origins of worry. In G. C. L Davey & F. Tallis (Eds.). Worrying: perspective on
theory, assessment and treatment (pp. 5±33). Chichester, UK: Wiley.
Borkovec, T. D., & Costello, E. (1993). E�cacy of applied relaxation and cognitive-behavior therapy in the treatment of generalized
anxiety disorder. Journal of Consulting and Clinical Psychology, 61, 611±619.
Borkovec, T. D., & Inz, J. (1990). The nature of worry in generalized anxiety disorder: a predominance of thought activity. Behaviour
Research and Therapy, 28, 153±158.
Brown, T. A., Antony, M. M., & Barlow, D. (1993). Psychometric properties of the Penn State Worry Questionnaire in a clinical
anxiety disorders sample. Behaviour Research and Therapy, 30, 33±37.
Butler, G., Cullington, A., Hibbert, G., Klimes, I., & Gelder, M. (1987). Anxiety management for persistent generalised anxiety. British
Journal of Psychiatry, 151, 535±542.
Cartwright-Hatton, S., & Wells, A. (1997). Beliefs about worry and intrusions: the Meta-Cognitions Questionnaire and its correlates.
Journal of Anxiety Disorders, 11, 279±296.
Durham, R. C., & Allan, T. (1993). Psychological treatment of generalized anxiety disorder: a review of the clinical signi®cance of
results in outcome studies since 1980. British Journal of Psychiatry, 163, 19±26.
Meyer, T. J., Miller, M. L., Metzger, R. L., & Borkovec, T. D. (1990). Development and validation of the Penn State Worry
Questionnaire. Behaviour Research and Therapy, 28, 487±495.
Spielberger, C. D., Gorsuch, R. I., Lushene, R., Vagg, P. R., & Jacobs, G. A. (1983). Manual for the State-Trait Anxiety Inventory
STAI (form Y2). Palo Alto, CA: Consulting Psychologists Press.
Wegner, D. M., Schneider, D. J., Carter, S. R., & White, T. L. (1987). Paradoxical e�ects of thought suppression. Journal of
Personality and Social Psychology, 53, 5±13.
Wells, A. (1994a). Attention and the control of worry. In G. C. L. Davey & F. Tallis (Eds.), Worrying: perspectives on theory, assess-
ment and treatment. (pp. 91±114). Chichester UK: Wiley.
Wells, A. (1994b). A multi-dimensional measure of worry: development and preliminary validation of the Anxious Thoughts
Inventory. Anxiety, Stress and Coping, 6, 289±299.
Wells, A. (1995). Meta-cognition and worry: a cognitive model of generalized anxiety disorder. Behavioural and cognitive
Psychotherapy, 23, 301±320.
Wells, A. (1997). Cognitive therapy of anxiety disorders: a practise manual and conceptual guide. Chichester, UK: Wiley.
Wells, A. & Matthews, G. (1994). Attention and emotion: a clinical perspective. Hove, UK: Erlbaum.
Wells, A., & Morrison, A. P. (1994). Qualitative dimensions of normal worry and normal obsessions: a comparative study. Behaviour
Research and Therapy, 32, 867±870.
Wells, A., & Papageorgiou, C. (1995). Worry and the incubation of intrusive images following stress. Behaviour Research and Therapy,
33, 579±583.
A. Wells, K. Carter / Behaviour Research and Therapy 37 (1999) 585±594594