Embed Size (px)
Citation preview
http://neurology.thelancet.com Vol 5 October 2006 823
Articles
IntroductionEpilepsy, one of the most common neurological disorders, is characterised by recurrent unprovoked seizures and aff ects up to 50 million people worldwide. Around 80% of individuals with epilepsy live in resource-poor countries where the disorder is largely untreated.1
Mortality associated with a specifi c disease can be an indirect estimator of severity.2 Patients with epilepsy have an increased risk of premature death compared with the general population.3 However, the extent and nature of this risk has not been suffi ciently examined,4
especially in resource-poor countries where there is often a large treatment gap with many patients not being treated.1
Mortality associated with a specifi c disease is assessed with particular parameters: mortality rate, case fatality rate (CFR), proportional mortality rate (PMR), and standardised mortality ratio (SMR). In China, only a few studies have described mortality rates of epilepsy in the general population, providing a range of 3·0–7·9 per 100 000 people per year.5–7 The CFR estimated from national health statistics is 0·7% of in-patient cases.8 Studies of PMR or SMR in epilepsy have not been done.
From 2000–04, a WHO supported demonstration project, Epilepsy Management at Primary Health Level (EMPHL), was undertaken in rural China. The aim of the
project was to improve the identifi cation and management of people with convulsive forms of epilepsy in rural areas within the existing primary health-care system. Phenobarbital treatment was provided to 2455 people with epilepsy in a population of 3 185 000.9 The EMPHL protocol used strict follow-up and management procedures, and so it was possible for us to calculate PMRs and SMRs to assess mortality in people with epilepsy.
MethodsTarget populationThe detailed methods of the selection of the target population of participants with epilepsy were described in our previous report.9 Briefl y, the target population was people with epilepsy who were managed by the EMPHL demonstration project, which was undertaken under the auspices of the WHO, International League Against Epilepsy, and International Bureau for Epilepsy’s Global Campaign against Epilepsy in eight rural counties of six provinces in China with a population of 3 185 000 people. Neurologists used strict criteria to confi rm the diagnosis of convulsive seizures in all participants. Patients were older than 2 years with at least two convulsive seizures in the previous 12 months and were not taking standard antiepileptic treatment. Inclusion and exclusion criteria for the study are provided elsewhere.9
Premature mortality in people with epilepsy in rural China: a prospective studyDing Ding, Wenzhi Wang, Jianzhong Wu, Guangyu Ma, Xiuying Dai, Bin Yang, Taiping Wang, Chenglin Yuan, Zhen Hong, Hanneke M de Boer, Leonid Prilipko, Josemir W Sander
SummaryBackground In China, few studies have described annual mortality associated with epilepsy in a general population and these have provided a range of 3·0–7·9 deaths per 100 000 people. We calculated the case fatality rate (CFR), proportional mortality rate (PMR), and standardised mortality ratio (SMR) to assess mortality in people with epilepsy in rural China.
Methods The target population was people with epilepsy who participated in an assessment of epilepsy management at primary health level in rural China. Neurologists confi rmed the diagnosis using strict criteria in all participants who were then treated with phenobarbital. Demographic data and putative cause of death were recorded for each person whose death was reported. PMRs for each cause of death and SMRs were estimated on the basis of the 2004 Chinese population.
Findings Case fatality rate was 1·4% (35 deaths) among 2455 people with epilepsy. The age-adjusted PMRs for injury, stroke, neoplasm, myocardial infarction, and pneumonia were 30%, 30%, 15%, 6%, and 5%, respectively. The SMR was 3·9 (95% CI 3·8–3·9). Patients aged 15–29 years had higher mortality ratios than did those in other age-groups, with SMRs exceeding 23.
Interpretation Risk for premature death is three to four times higher in people with epilepsy than in the general Chinese population. Furthermore, the risk in young people with epilepsy in China is much higher than previously reported. Injury, stroke, myocardial infarction, and pneumonia are among the leading putative causes of death in patients with epilepsy in rural China.
Lancet Neurol 2006; 5: 823–27
Published Online August 17, 2006DOI:10.1016/S1474-4422(06)70528-2
See Refl ection and Reaction page 804
Department of Biostatistics and Epidemiology, Institute of Neurology, Fudan University, WHO Collaborating Centre for Research and Training in Neurosciences, Shanghai, China (D Ding MD, Z Hong MD); Department of Neuroepidemiology, Beijing Neurosurgical Institute, Beijing, China (W Wang MD, J Wu MD); Universal Love Hospital, Mudanjiang, Heilongjiang Province, China (G Ma MD); Ningxia Medical College, Ningxia Hui Autonomous Region, China (X Dai MD); Jiaozuo People’s Hospital, Henan Province, China (B Yang MD); Zezhou County Hospital, Shanxi Province, China (T Wang MD); Department of Neurology, Yangzhou Medical College, Jiangsu Province, China (C Yuan MD); ILAE/IBE/WHO Global Campaign Against Epilepsy, Stichting Epilepsie Instellingen Nederland (SEIN), WHO Collaborating Centre for Research, Training, and Treatment of Epilepsy, Heemstede, Netherlands (H M de Boer); Department of Mental Health and Substance Abuse, World Health Organization, Geneva, Switzerland (L Prilipko MD); and Department of Clinical and Experimental Epilepsy, UCL Institute of Neurology, London, UK (Prof J W Sander FRCP)
Correspondence to: Prof Ley Sander, Department of Clinical and Experimental Epilepsy, Institute of Neurology, Queen Square, London WC1N 3BG, UK [email protected]
Articles
ProceduresA team of neurologists trained local primary-care physicians in the diagnosis and management of epilepsy, the use of antiepileptic drugs, and the follow-up aspects of the study protocol. Patients were treated with phenobarbital monotherapy as the fi rst option. They visited the local clinic every 2 weeks for the fi rst 2 months and monthly thereafter for dose adjustments, assessment of adverse events, adherence checking, and to receive further supplies of medication. The study began recruitment in December, 2001, and follow-up continued until the end of June, 2004. Median duration of follow-up was 25 months (range 0–32).9
During follow-up, local primary-care physicians recorded demographic data and putative cause of death of any patient who died. Cause of death was attributed on clinical grounds and verbal autopsy.10 Specialists and the principal investigators in each study area gathered information about cause of death through interviews with relatives or local village physicians. Death certifi cates were also used for the confi rmation of the cause of death. We classifi ed the putative cause of death according to the International Classifi cation of Diseases, ninth revision. Sudden unexpected death in epilepsy (SUDEP) is defi ned as sudden unexpected death in an individual with epilepsy with or without evidence of a seizure, and excluding documented status epilepticus, where post-mortem examination does not reveal an anatomical or toxicological cause of death.11
The Institutional Ethics Committee of the Beijing Neurosurgical Institute scrutinised the EMPHL protocol and gave ethical approval for the study. All participants provided written consent to participate in the study; for children, consent was given by their guardians. All aspects of the study were monitored and supervised by an international steering committee.
Statistical analysisCFR was calculated as the number of deaths during follow-up divided by the number in the study cohort.2
PMR was calculated as the proportion of deaths due to a specifi c cause in the population under study.2 The major causes of death were based on the death classifi cation of the Bulletin of Health Statistics in China.8 We calculated the PMRs of major causes of death in people with epilepsy adjusted by the age structure of the Chinese population in 2004, and compared these with PMRs in the 2004 Chinese population. SMRs, the ratios of observed number of deaths in the target epilepsy population to those expected,2 were calculated on the basis of age-specifi c and sex-specifi c mortality rates in the Chinese population in 2004. Specifi c SMRs for sex, age-group, and cause of death were also calculated. All results are presented with 95% CIs. All mortality measurements were calculated within the follow-up time, with the median being 25 months in the current study.
Role of the funding sourceThe project from which the data were derived was approved and supported by the Chinese Ministry of Health and the WHO. The sponsors approved the protocol but were not directly involved in its design. The sponsors were represented on the steering committee and their representatives were involved in the drafting of the paper. JWS had full access to all the data in the study and had fi nal responsibility for the decision to submit for publication.
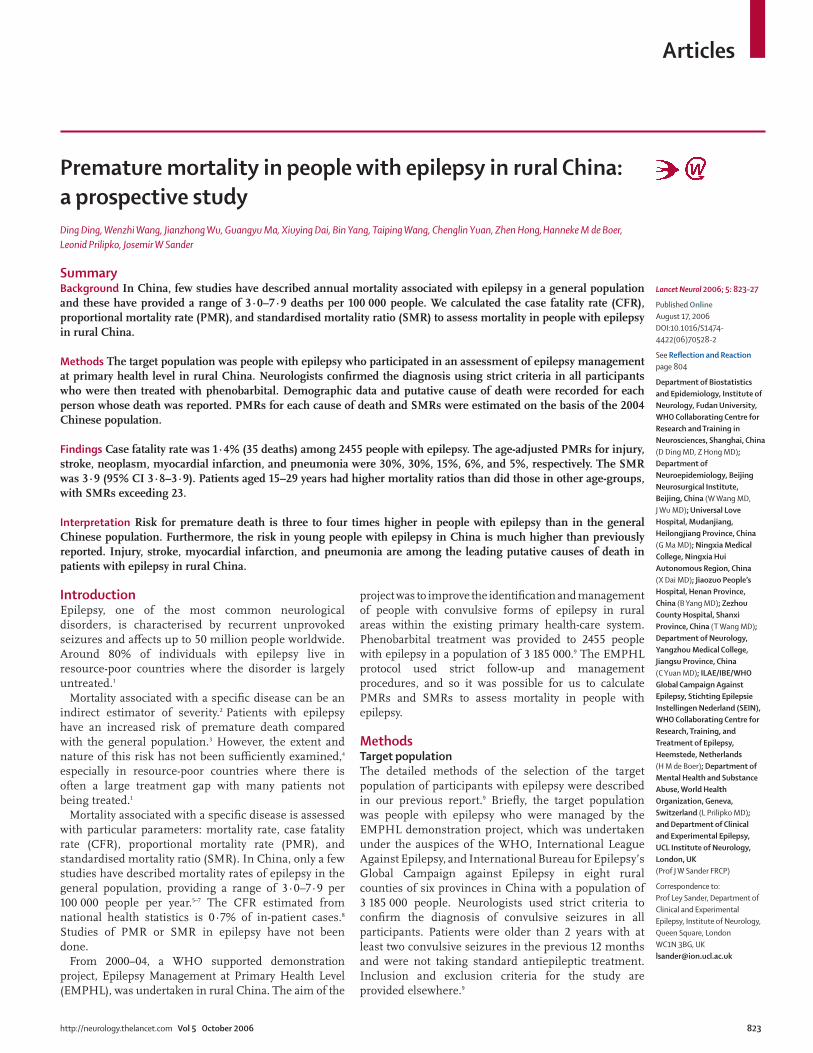
ResultsThere were 35 deaths among 2455 people with epilepsy during follow-up. Therefore, the CFR was 1·4% in this treated cohort. The table shows demographic details, seizure frequency, and duration of follow-up for participants enrolled in the phenobarbital trial and in those who died.
The main cause of death was accidental or as a result of injury (self-infl icted or otherwise); 13 (37%) patients died of drowning (n=6), suicide (n=4), poisoning (n=2), or a road traffi c accident (n=1). In 11 (31%) patients, death was attributed to haemorrhagic or ischaemic stroke, whereas in two (6%), death was attributed to pneumonia. The age-adjusted PMRs for injury (30%), stroke (30%), pneumonia (5%), and myocardial infarction (6%) were higher for the trial participants than for the 2004 Chinese population (8%, 19%, 2%, and 3%, respectively).8 The adjusted PMR for neoplasm (15%) was lower in the study population
Figure number
Author
Editor
Created by
XXXXXXXX
XXXXXXXX
XXXXXXXX
Helen
€$£¥∆Ωµ∏π∑Ωαβχδεγηκλμτ†‡§¶√+−±×÷≈<>≤≥
0
10
20
30
40
Injury Stroke Neoplasm Pneumonia Myocardial infarction
PMR
(%)
People with epilepsyChinese population 2004
Figure 1: Age-adjusted cause-specifi c PMRs in people with epilepsy compared with the general Chinese population, 2004
All patients enrolled Those enrolled who died
Number of people with epilepsy 2455 35
Number of men (%) 1381 (56) 22 (63)
Mean age, years (SD) 33 (21) 45 (19)
Mean onset age, years (SD) 17 (14) 30 (23)
Median baseline convulsive seizure frequency, per year (IQR)
10 (4–24) 12 (6–24)
Median follow-up time, months (IQR) 25 (15–30) 11 (7–22)
Table: Characteristics of patients enrolled in the phenobarbital trial
824 http://neurology.thelancet.com Vol 5 October 2006
Articles
http://neurology.thelancet.com Vol 5 October 2006 825
than in the general population (fi gure 1). In one patient (3%), death was attributed to SUDEP after a negative post-mortem examination. In three patients (9%), the cause of death was not attributed because of lack of information.
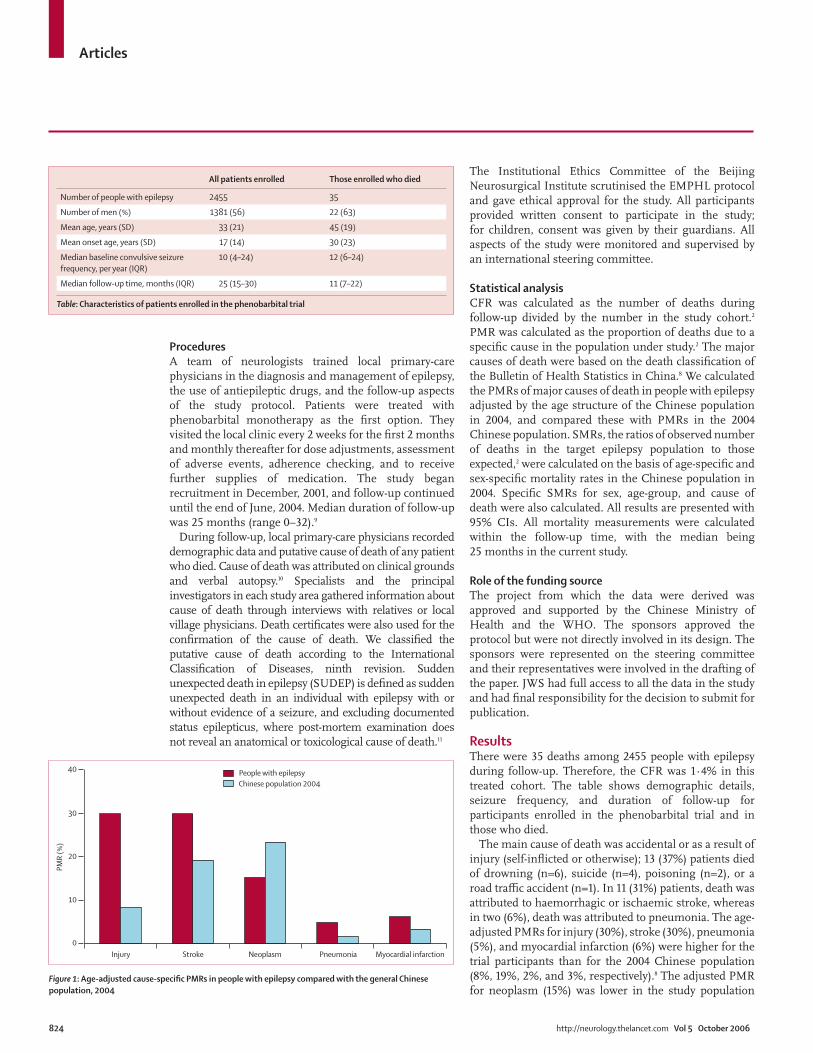
The SMR for people with epilepsy was 3·9 (95% CI 3·8–3·9) and was higher in women (4·1; 3·9–4·4) than in men (3·5; 3·4–3·6). Figure 2 shows that in patients aged at least 15 years, and with the exception of those aged 70–74 years, the SMR was raised. SMRs were especially high in patients ages 15–19 years (23·3; 15·9–43·9), 20–24 years (40·2; 32·4–52·8), and 25–29 years (33·3; 28·0–41·1). The SMRs for patients aged 30–49 years were in the range 2·3–8·1, and for people with epilepsy aged older than 49 years the SMRs were lower than for the 30–49 year age-group (fi gure 2). Cause-specifi c SMRs of the epilepsy population were calculated for: pneumonia (21·3; 14·5–40·0), injury (12·2; 11·4–13·0), myocardial infarction (10·7; 5·6–95·3), stroke (7·0; 6·5–7·6), and neoplasm (1·6; 1·5–1·8). Suicide (3·8; 3·2–4·6) and drowning (5·6; 4·7–6·5) were the major causes of death in those classifi ed as dying of injury.
DiscussionOur fi ndings suggest that injury, stroke, myocardial infarction, and pneumonia are among the leading putative causes of death in people with epilepsy in rural China. Risk of premature death was three to four times greater in people with epilepsy than in the general Chinese population. Additionally, this risk was much higher in young people than previously reported from mortality studies outside China.3,4,12,13
The issue of severity is of paramount concern in studies of mortality in epilepsy.2 Previous population-based studies undertaken in China obtained data to calculate mortality rates only.5–7 The mortality rate alone, however, is not suffi cient to measure the relative risk of death due to epilepsy and to ascertain severity accurately. We used CFR, PMR, and SMR to assess the risk of premature mortality of people with epilepsy in the Chinese population. The CFR of epilepsy estimates the average risk of dying and increases with duration of follow-up. The CFR of epilepsy in mainland China was previously only available from national health statistics, with an estimate of 0·7% in patients during hospitalisation.8 The current study shows a CFR of 1·4% during a median of 25 months of follow-up. A study of a Chinese population in Taiwan found a CFR of 0·9% in people with epilepsy attending a university epilepsy clinic for an average of 4·7 years,14 whereas another Taiwanese study obtained an overall CFR of 12% during a 10 year follow-up of people with epilepsy in an outpatient clinic.15
Cause-specifi c PMR and SMR in people with epilepsy have been studied in some developed countries. The wide range of rates in these studies can be partly explained by the diff erent lengths of follow-up. Neoplasms (PMR 12–35%; SMR 1·5–4·8), pneumonia (5–25%; 4·2–10·3), heart disease (8–19%; 1·1–2·5), cerebrovascular disease (5–17%; 1·8–5·3), and injuries (3–7%; 2·4–4·7) have been shown to be the main causes of death in epilepsy populations.15 Studies in Taiwan and Ecuador showed higher PMRs for SUDEP (14%) than rates calculated from data for developed countries (11%).14,16 Our study shows that the main causes of death were similar to those reported in previous studies in epilepsy populations;
0
10
20
30
40
50
60
SMR
0–4 5–9 10–14 15–19 20–24 25–29 30–34 35–39 40–44 45–49 50–54 55–59 60–64 65–69 70–74 75–79 80–84 ≥85
Age (years)
Figure 2: Age-specifi c SMRs of epilepsy in the study population in rural China, adjusted for the Chinese population, 2004Bars represent 95% CIs.

Articles
826 http://neurology.thelancet.com Vol 5 October 2006
however, the PMRs and SMRs of injury, stroke, myocardial infarction, and pneumonia were higher than previously reported. This fi nding could imply a higher risk of death from these causes in a Chinese rural population with epilepsy.
The overall SMR in the current study population of 3·9 (95% CI 3·8–3·9) was just within the range (1·6–4·1) reported from studies in developed countries.17 The SMR was lower than those reported from prospective studies in developing countries; however, two of these studies, one in Martinique (SMR 4·3) and the other in Ecuador (SMR 6·3), were hospital-based, whereas the study in Vasai (India) was a 10 year community follow-up study with an SMR of 7·8.16 Like most previous studies, we showed an inverse relation between SMR and age. The SMRs in young people aged 15–29 years, however, were much higher than those previously reported. The SMR in the 2–24 year age-group in the current study (22·8) is higher than that of a study in Rochester (0–24 year age-group: SMR 8·5, 95% CI 5·4–12·9).12 The Warsaw study reported an SMR of 3·5 in the 0–29 year age-group,13 whereas our study showed a much higher SMR of 26·7 for this age-group. The SMR in the current study of 10·1 for the 2–49 year age-group is higher than that of a study in the UK (0–49 year age-group: SMR 7·6, 95% CI 4·2–12·5).4 The high SMR in young adults with epilepsy is a refl ection of both the low mortality in the reference population and high mortality in epilepsy patients.18 Our fi ndings suggest that epilepsy could pose a potential threat to young people with the disorder in rural areas of China.
The study population was selected from six provinces in rural China, in which a signifi cant number of patients had not been treated with standard antiepileptic treatment, as reported in our previous studies.9,19,20 The treatment gap was mostly in those with low socio-economic status. Therefore, the relatively increased risk of premature mortality in our study population could be partly associated with poverty.
Our study included patients who had never been treated or had not been treated with standard antiepileptic treatment at the time of enrolment,9 which presumably represents a population with limited access to medical care in China. The reported treatment gap in epilepsy is high (47–77%) in rural China;19,20 nevertheless, the target population in our study might not be completely representative of the epilepsy population in China for medical attention. Thus, the mortality assessment reported might be underestimated because of the good effi cacy of the standard treatment during follow-up.
This pragmatic study did not diff erentiate between primary and secondary generalised seizures and did not recruit people with other seizure types who did not have convulsive seizures. Hence mortality rates were not calculated for other seizure types. Previous studies have reported SMRs of 1·5–2·1 for people with partial seizures
and of 4·1 for those with myoclonic seizures.12,21,22 Thus, our results might overestimate epilepsy mortality in view of the relative rarity of people with myoclonic seizures. Even with this potential overestimate of mortality, the SMR reported here is still lower than that of study populations in developing countries, which included all types of epilepsy.16
Our study is a prevalent mortality study and therefore might not be comparable with previous studies of incident epilepsy. Because the highest mortality rates in incident cohorts are in the fi rst few years after diagnosis,23 mortality rates in cohorts of people with prevalent epilepsy tend to be lower than those of incident cohorts. Despite the lower mortality rate expected, we found higher mortality rates than those reported in other incident cohorts.
Attribution of the cause of death is diffi cult in developed countries with facilities for post-mortem examination;24 in resource-poor countries where post-mortem exam-inations are the exception, the cause of death might be less accurate. For instance, only three of the people who died in this study had post-mortem examinations and, therefore, most of the attribution of cause of death is putative. This study recorded only one SUDEP case (after autopsy); some of the deaths attributed to myocardial infarction or stroke could in fact have been due to SUDEP, which is not well recognised in China.
Death is frequently not reported in China, and therefore the study may have missed some deaths in the population followed up. During the whole study, 91 people were lost to follow-up and 471 people withdrew from the study; some of these people might have died.9 Thus the fi gures calculated should be seen as minimum estimates of mortality risk.
In conclusion, there is an increased risk of premature mortality in people with epilepsy in rural China, especially among the young. The increase in mortality in young adults is higher than seen in developed countries. People in this study were receiving overall eff ective treatment; whether mortality would have been further increased if they had remained untreated is unclear.ContributorsThis work was conceptualised by JWS, WW, JW, and DD. All the authors approved the protocol. All authors apart from DD and ZH were members of the steering committee of the project. Data collection was done by GM, XD, BY, TW, and CY. The analysis was undertaken by DD, ZH, and JWS. DD, WW, JW, and JWS prepared the fi rst draft. All authors contributed to and approved the fi nal version. HdB, LP, and JWS organised the funding. JWS is the guarantor of the paper.
Confl icts of interestJWS has received honoraria, consultancy fees, grants, and travel grants from various pharmaceutical companies including Novartis, Pfi zer, UCB, Eisai, Schwarz Pharma, Janssen-Cilag, Sanofi -Aventis, and GSK. The National Society for Epilepsy endows his current position. He has been a member of the Management Committee of the International League Against Epilepsy and the Executive Committee of the International Bureau for Epilepsy. He is currently a Council member of the British chapter of the International League Against Epilepsy and of Epilepsy Action. The other authors have no confl icts of interest.

Articles
http://neurology.thelancet.com Vol 5 October 2006 827
AcknowledgmentsWe thank all the participants of the EMPHL demonstration project for their help and cooperation. We also wish to thank our colleagues in the study groups in the diff erent provinces of China for their help and support. The Ministry of Health in China and the WHO Regional Offi ce, to whom we are most grateful, supported this study.
References1 Scott RA, Lhatoo SD, Sander JW. The treatment of epilepsy in
developing countries: where do we go from here? Bull World Health Organ 2001; 79: 344–51.
2 Logroscino G, Hesdorff er DC. Methodologic issues in studies of mortality following epilepsy: measures, types of studies, sources of cases, cohort eff ects, and competing risks. Epilepsia 2005; 46 (suppl 11): 3–7.
3 Gaitatzis A, Sander JW. The mortality of epilepsy revisited. Epileptic Disord 2004; 6: 3–13.
4 Cockerell OC, Johnson AL, Sander JW, Hart YM, Goodridge DM, Shorvon SD. Mortality from epilepsy: results from a prospective population based study. Lancet 1994; 344: 918–21.
5 Li SC, Wang WZ, Fang XH, et al. Epidemiologic study of central nerve system diseases in rural China. Chin J Neurosurg 1989; 5: 2–6.
6 Department of Psychiatry, Sichuan Medical School. Investigative report on the incidence of epilepsy in a population of 420,000 in Sichuan. Chin J Nerv Ment Dis 1981; 14: 135–38.
7 Li SC, Schoenberg BS, Wang CC, Cheng XM, Zhou SS, Bolis CL. Epidemiology of epilepsy in urban areas of the People’s Republic of China. Epilepsia 1985; 26: 391–94.
8 Chinese Ministry of Health. Bulletin of Health Statistics in China 2005. Beijing: China Xiehe Medical University Press, 2005.
9 Wang WZ, Wu JZ, Ma GY, et al. Effi cacy assessment of phenobarbital in epilepsy: a large community-based intervention trial in rural China. Lancet Neurol 2006; 5: 46–52.
10 Aspray TJ. The use of verbal autopsy in attributing cause of death from epilepsy. Epilepsia 2005; 46 (suppl 11): 15–17.
11 Lhatoo SD, Sander JW. Cause-specifi c mortality in epilepsy. Epilepsia 2005; 46 (suppl 11): 36–39.
12 Hauser WA, Annegers J, Elveback L. Mortality in patients with epilepsy. Epilepsia 1980; 21: 399–412.
13 Zielinski JJ. Epilepsy and mortality rate and cause of death. Epilepsia 1974; 15: 191–201.
14 Tsai JJ. Mortality of epilepsy from national vital statistics and University Epilepsy Clinic in Taiwan. Epilepsia 2005; 46 (suppl 11): 8–10.
15 Chen RC, Chang YC, Chen TH, Wu HM, Liou HH. Mortality in adult patients with epilepsy in Taiwan. Epileptic Disord 2005; 7: 213–19.
16 Carpio A, Bharucha NE, Jallon P, et al. Mortality of epilepsy in developing countries. Epilepsia 2005; 46 (suppl 11): 28–32.
17 Forsgren L, Hauser WA, Olafsson E, Sander JW, Sillanpaa M, Tomson T. Mortality of epilepsy in developed countries: a review. Epilepsia 2005; 46 (suppl 11): 18–27.
18 Brorson LO, Wranne L. Long-term prognosis in childhood epilepsy: survival and seizure prognosis. Epilepsia 1987; 28: 324–30.
19 Wang WZ, Wu JZ, Wang DS, et al. The prevalence and treatment gap in epilepsy in China—an ILAE/IBE/WHO study. Neurology 2003; 60: 1544–45.
20 Ding D, Lu GY, Huang MS, et al. A sampled epidemiological survey of epilepsy in Shanghai rural area. Chin J Neurosci 2004; 12: 122–24.
21 Olafsson E, Hauser WA, Gudmundsson G. Long-term survival of people with unprovoked seizures: a population-based study. Epilepsia 1998; 39: 89–92.
22 Lindsten H, NystromL, Forsgren L. Mortality in an adult cohort with newly diagnosed unprovoked epileptic seizure: a population-based study. Epilepsia 2000; 41: 1469–73.
23 Jallon P. Mortality in patients with epilepsy. Curr Opin Neurol 2004; 17: 141–46.
24 Bell GS, Gaitatzis A, Johnson AL, Sander JW. Predictive value of death certifi cation in the case ascertainment of epilepsy. J Neurol Neurosurg Psychiatry 2004; 75: 1756–58.




![Systematic review: isocaloric ketogenic dietary regimes ... · Hopkins University successfully treated a child with intractable epilepsy [6, 7]. Retrospective and prospective studies](https://img.pdfslide.net/doc/110x75/5bb7bce109d3f2d32a8d7448/systematic-review-isocaloric-ketogenic-dietary-regimes-hopkins-university.jpg)