Embed Size (px)
Citation preview

American Journal of Medical Genetics 565247-251 (1995)
Prenatal Diagnosis and Fetopathological Findings in Five Fetuses With Trisomy 9
David Chitayat, Kathy Hodgkinson, Anthony Luke, Elizabeth Winsor, Toby Rose, and Dagmar Kalousek Prenatal Diagnosis Program (D.C., K.H., A.L., E. W., T.R.), Toronto Hospital‘s Division of Medical Genetics, The Hospital for Sick Children (D.C.), Department of Pathology (T.R.), The Women’s College Hospital, University of Toronto, Toronto, Ontario; and Department of Medical Genetics and Pathology (D.K.), British Columbia Children’s Hospital, Vancouver, British Columbia, Canada
~
Five male fetuses with trisomy 9 are dis- cussed. Three were detected prenatally and terminated, 1 aborted spontaneously, and the fifth delivered prematurely and died soon after. Multiple congenital abnormali- ties characteristic of trisomy 9 were de- tected in all 5 cases and are compared to those of previous reports. 0 1995 Wiley-Liss, Inc.
KEY WORDS: trisomy 9, prenatal diagno- sis, cystic hygroma, multiple congenital abnormalities, chromosome abnormalities, spontaneous abortion
INTRODUCTION Trisomy 9 syndrome comprises complete trisomy 9,
partial trisomy 9, and trisomy 9 mosaicism. These pre- sent similar phenotypes with the diversity of anomalies corresponding to the amount of extra chromosomal ma- terial present. Complete trisomy 9 is a rare chromo- some aneuploidy accounting for 2.7% of trisomic spon- taneous abortions [Lauritsen, 19821. Most trisomy 9 fetuses are thus spontaneously lost. Newborn infants with trisomy 9 probably represent the less severe cases and they may be mosaic. Clinical manifestations in- clude low birth weight, developmental delay, micro- cephaly, small palpebral fissures, bulbous nose, appar- ently low-set malformed ears, hypoplastic genitalia, and several cardiac, skeletal, and cerebral malforma- tions [Feingold and Atkins, 1973; Kurnick et al., 1974; Sutherland et al., 1976; Qazi et al., 1977; Mace et al., 1978; de Grouchy and Thurleau, 1984; Schinzel, 1984;
Received for publication September 7, 1993; revision received July 1, 1994.
Address reprint requests to D. Chitayat, M.D., Prenatal Diag- nosis Program, Toronto Hospital, General Division, 200 Elizabeth Street, 6EN-323, Toronto, Ontario, Canada M5G 2C4.
0 1995 Wiley-Liss, Inc.
Smart et al., 1988; Diaz-Mares et al., 1990; Benacerraf et al., 1992; de Michelena et al., 1992; Louwen et al., 1992; Shere et al., 19921.
With advances in fetal ultrasound technology and more thorough pathological investigations of products of conception, information on fetuses with rare chromo- some abnormalities may be collected. Five cases are re- ported complete with autopsy findings, all with puta- tive complete trisomy 9.
CLINICAL REPORTS Case 1
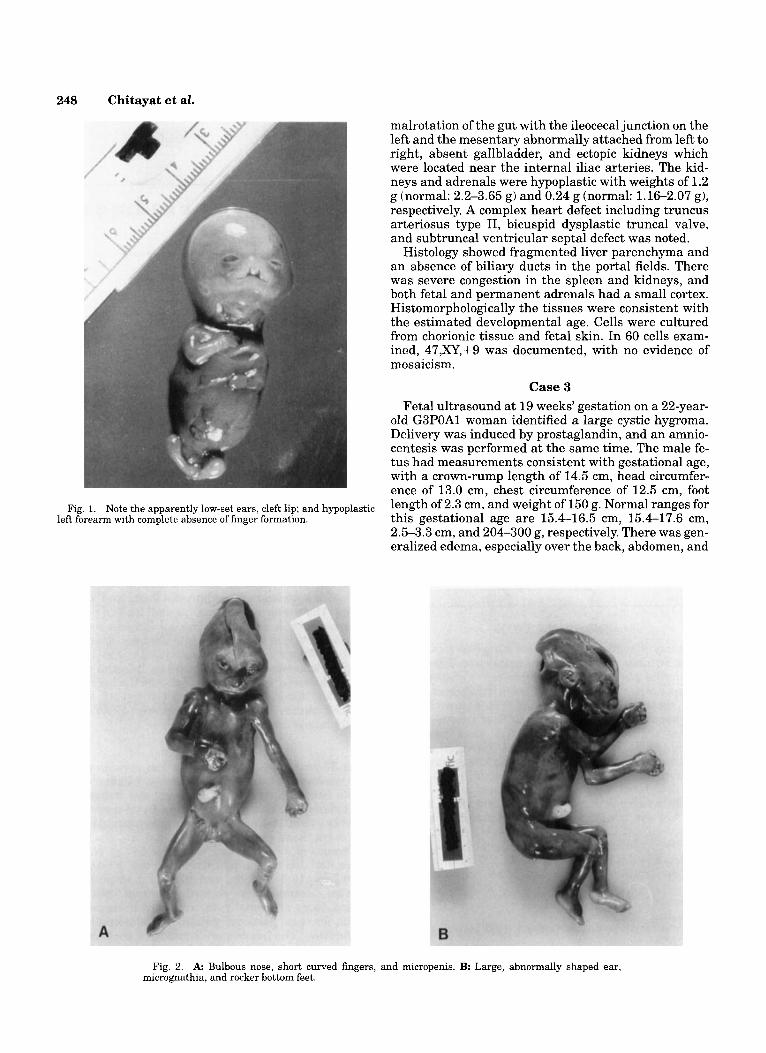
This fetus was spontaneously aborted at 14 weeks’ gestation by a 30-year-old G2P1 woman. At autopsy, a macerated male fetus of 8 weeks’ development was noted with a crown-rump length of 4.0 cm, and weight of 3.5 g. There was microcephaly, a cleft lip and palate, and apparently low-set ears. The left forearm was hy- poplastic and short with complete absence of fingers. The toes on the right foot were hypoplastic (Fig. 1). Ra- diological assessment was not possible. Internal exam- ination showed a ventricular septa1 defect, a horseshoe kidney, and abnormal lung lobation. Cytogenetic analy- sis of cell culture from the amnion showed 47,XY,+9 in 6 metaphases.
Case 2 The 37-year-old G2PlAO woman had amniocentesis
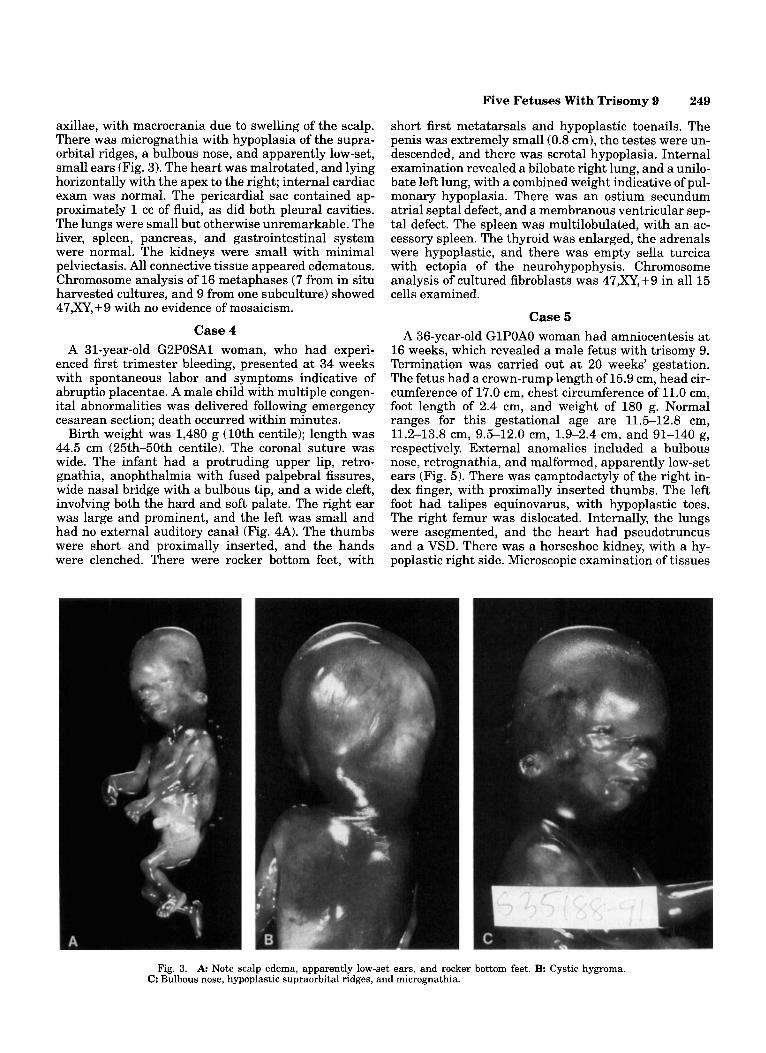
at 16 weeks for advanced maternal age, which showed a male fetus with trisomy 9. Delivery was induced by prostaglandin at 21 weeks’ gestation. Developmentally the fetus was of 16-week size with a crown-rump length of 14.0 cm, head circumference of 12.5 cm, chest cir- cumference of 11.5 cm, and weight of 277 g. Normal ranges for 19 weeks postovulation are 17-18 cm, 18-19.5 cm, 15.5-16.8 cm, and 365411 g, respectively. External examination showed bilateral microph- thalmia, large abnormal ears, a bulbous nose, microg- nathia, an open posterior palate, and abnormal gum proliferation. The hands were small with short curved fingers, and there were rocker bottom feet with short toes. The penis was extremely small (Fig. 2A,B). There were several internal anomalies; an annular pancreas,
248 Chitayat et af.
malrotation of the gut with the ileocecal junction on the left and the mesentary abnormally attached from left to right, absent gallbladder, and ectopic kidneys which were located near the internal iliac arteries. The kid- neys and adrenals were hypoplastic with weights of 1.2 g (normal: 2.2-3.65 g) and 0.24 g (normal: 1.16-2.07 g), respectively. A complex heart defect including truncus arteriosus type 11, bicuspid dysplastic truncal valve, and subtruncal ventricular septa1 defect was noted.
Histology showed fragmented liver parenchyma and an absence of biliary ducts in the portal fields. There was severe congestion in the spleen and kidneys, and both fetal and permanent adrenals had a small cortex. Histomorphologically the tissues were consistent with the estimated developmental age. Cells were cultured from chorionic tissue and fetal skin. In 60 cells exam- ined, 47,XY,+9 was documented, with no evidence of mosaicism.
Case 3 Fetal ultrasound at 19 weeks’ gestation on a 22-year-
old G3POA1 woman identified a large cystic hygroma. Delivery was induced by prostaglandin, and an amnio- centesis was performed at the same time. The male fe- tus had measurements consistent with gestational age, with a crown-rump length of 14.5 cm, head circumfer- ence of 13.0 cm, chest circumference of 12.5 cm, foot
this gestational age are 15.4-16.5 cm, 15.4-17.6 cm, 2.5-3.3 cm, and 204-300 g, respectively. There was gen- eralized edema, especially over the back, abdomen, and
Fig. 1. Note the apparently low-set ears, cleft lip; and hypoplastic length Of 2-3 cm, and weight Of 150 g. ranges for left forearm with complete absence of finger formation.
Fig. 2. A Bulbous nose, short curved fingers, and micropenis. B: Large, abnormally shaped ear, micrognathia, and rocker bottom feet.
Five Fetuses With Trisomy 9 249
short first metatarsals and hypoplastic toenails. The penis was extremely small (0.8 cm), the testes were un- descended, and there was scrota1 hypoplasia. Internal examination revealed a bilobate right lung, and a unilo- bate left lung, with a combined weight indicative of pul- monary hypoplasia. There was an ostium secundum atrial septa1 defect, and a membranous ventricular sep- tal defect. The spleen was multilobulated, with an ac- cessory spleen. The thyroid was enlarged, the adrenals were hypoplastic, and there was empty sella turcica with ectopia of the neurohypophysis. Chromosome analysis of cultured fibroblasts was 47,XY,+9 in all 15 cells examined.
Case 5 A 36-year-old GlPOAO woman had amniocentesis a t
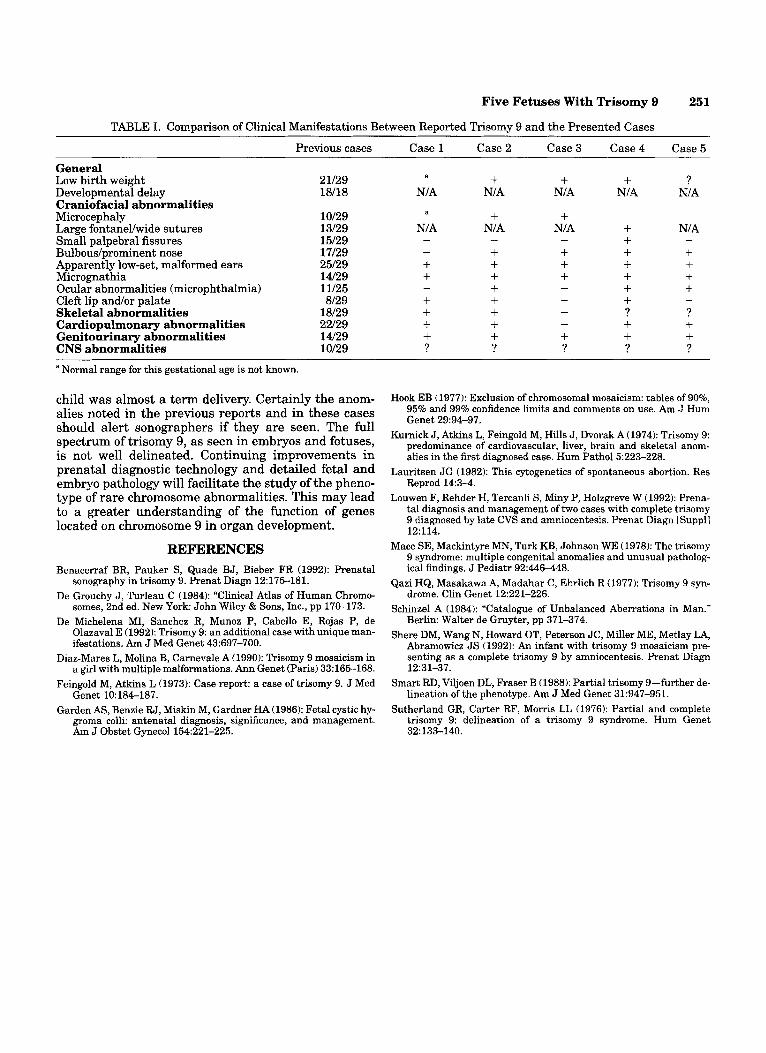
16 weeks, which revealed a male fetus with trisomy 9. Termination was carried out at 20 weeks’ gestation. The fetus had a crown-rump length of 15.9 cm, head cir- cumference of 17.0 cm, chest circumference of 11.0 cm, foot length of 2.4 cm, and weight of 180 g. Normal ranges for this gestational age are 11.5-12.8 cm, 11.2-13.8 cm, 9.5-12.0 cm, 1.9-2.4 cm, and 91-140 g, respectively. External anomalies included a bulbous nose, retrognathia, and malformed, apparently low-set ears (Fig. 5). There was camptodactyly of the right in- dex finger, with proximally inserted thumbs. The left foot had talipes equinovarus, with hypoplastic toes. The right femur was dislocated. Internally, the lungs were asegmented, and the heart had pseudotruncus and a VSD. There was a horseshoe kidney, with a hy- poplastic right side. Microscopic examination of tissues
axillae, with macrocrania due to swelling of the scalp. There was micrognathia with hypoplasia of the supra- orbital ridges, a bulbous nose, and apparently low-set, small ears (Fig. 3). The heart was malrotated, and lying horizontally with the apex to the right; internal cardiac exam was normal. The pericardial sac contained ap- proximately 1 cc of fluid, as did both pleural cavities. The lungs were small but otherwise unremarkable. The liver, spleen, pancreas, and gastrointestinal system were normal. The kidneys were small with minimal pelviectasis. All connective tissue appeared edematous. Chromosome analysis of 16 metaphases (7 from in situ harvested cultures, and 9 from one subculture) showed 47,XY,+9 with no evidence of mosaicism.
Case 4 A 31-year-old G2POSAl woman, who had experi-
enced first trimester bleeding, presented at 34 weeks with spontaneous labor and symptoms indicative of abruptio placentae. A male child with multiple congen- ital abnormalities was delivered following emergency cesarean section; death occurred within minutes.
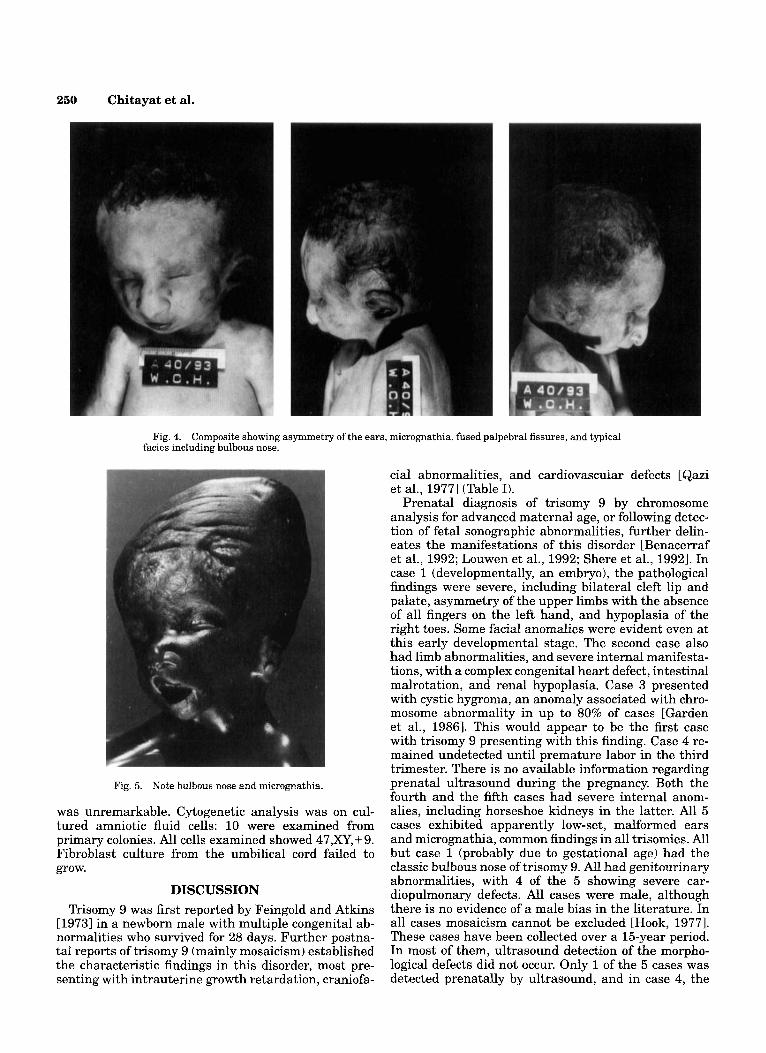
Birth weight was 1,480 g (10th centile); length was 44.5 cm (25th-50th centile). The coronal suture was wide. The infant had a protruding upper lip, retro- gnathia, anophthalmia with fused palpebral fissures, wide nasal bridge with a bulbous tip, and a wide cleft, involving both the hard and soft palate. The right ear was large and prominent, and the left was small and had no external auditory canal (Fig. 4A). The thumbs were short and proximally inserted, and the hands were clenched. There were rocker bottom feet, with
Fig. 3. A Note scalp edema, apparently low-set ears, and rocker bottom feet. B Cystic hygroma. C: Bulbous nose, hypoplastic supraorbital ridges, and micrognathia.
250 Chitayat et al.
Fig. 4. Composite showing asymmetry of the ears, micrognathia, fused palpebral fissures, and typical facies including bulbous nose.
Fig. 5. Note bulbous nose and micrognathia.
was unremarkable. Cytogenetic analysis was on cul- tured amniotic fluid cells: 10 were examined from primary colonies. All cells examined showed 47,XY, + 9. Fibroblast culture from the umbilical cord failed to grow.
DISCUSSION Trisomy 9 was first reported by Feingold and Atkins
[19731 in a newborn male with multiple congenital ab- normalities who survived for 28 days. Further postna- tal reports of trisomy 9 (mainly mosaicism) established the characteristic findings in this disorder, most pre- senting with intrauterine growth retardation, craniofa-
cia1 abnormalities, and cardiovascular defects [Qazi et al., 19771 (Table I).
Prenatal diagnosis of triaomy 9 by chromosome analysis for advanced maternal age, or following detec- tion of fetal sonographic abnormalities, further delin- eates the manifestations of this disorder [Benacerraf et al., 1992; Louwen et al., 1992; Shere et al., 19921. In case 1 (developmentally, an embryo), the pathological findings were severe, including bilateral cleft lip and palate, asymmetry of the upper limbs with the absence of all fingers on the left hand, and hypoplasia of the right toes. Some facial anomalies were evident even at this early developmental stage. The second case also had limb abnormalities, and severe internal manifesta- tions, with a complex congenital heart defect, intestinal malrotation, and renal hypoplasia. Case 3 presented with cystic hygroma, an anomaly associated with chro- mosome abnormality in up to 80% of cases [Garden et al., 19861. This would appear to be the first case with trisomy 9 presenting with this finding. Case 4 re- mained undetected until premature labor in the third trimester. There is no available information regarding prenatal ultrasound during the pregnancy. Both the fourth and the fifth cases had severe internal anom- alies, including horseshoe kidneys in the latter. All 5 cases exhibited apparently low-set, malformed ears and micrognathia, common findings in all trisomies. All but case 1 (probably due to gestational age) had the classic bulbous nose of trisomy 9. All had genitourinary abnormalities, with 4 of the 5 showing severe car- diopulmonary defects. All cases were male, although there is no evidence of a male bias in the literature. In all cases mosaicism cannot be excluded [Hook, 19771. These cases have been collected over a 15-year period. In most of them, ultrasound detection of the morpho- logical defects did not occur. Only 1 of the 5 cases was detected prenatally by ultrasound, and in case 4, the
Five Fetuses With Trisomy 9
TABLE I. Comparison of Clinical Manifestations Between Reported Trisomy 9 and the Presented Cases
251
General Low birth weight Developmental delay Craniofacial abnormalities Microcep haly Large fontanellwide sutures Small palpebral fissures Bulbous/prominent nose Apparently low-set, malformed ears Micrognathia Ocular abnormalities (microphthalmia) Cleft lip and/or palate Skeletal abnormalities Cardiopulmonary abnormalities Genitourinary abnormalities CNS abnormalities
Previous cases
21/29 18/18
10129 13/29 15/29 17/29 25/29 14/29 11/25 8/29
18/29 22/29 14/29 10/29
Case 3 Case 2 ~ _ _ _ _ _ ~
Case3 Case4 Case5
a
N/A a
N/A - -
+ + + + + +
-
?
+ N/A
+ N/A
+ + + + + + + + ?
-
+ + ? N/A N/A NIA
+ N/A
+ + +
-
+ ?
+ + + + + + + + + ?
?
N/A
+ + + +
-
-
? + + ?
a Normal range for this gestational age is not known.
child was almost a term delivery. Certainly the anom- alies noted in the previous reports and in these cases should alert sonographers if they are seen. The full spectrum of trisomy 9, as seen in embryos and fetuses, is not well delineated. Continuing improvements in prenatal diagnostic technology and detailed fetal and embryo pathology will facilitate the study of the pheno- type of rare chromosome abnormalities. This may lead to a greater understanding of the function of genes located on chromosome 9 in organ development.
REFERENCES Benacerraf BR, Pauker S, Quade BJ, Bieber FR (1992): Prenatal
sonography in trisomy 9. Prenat Diagn 12:175-181. De Grouchy J , Turleau C (1984): “Clinical Atlas of Human Chromo-
somes, 2nd ed. New York John Wiley & Sons, Inc., pp 170-173. De Michelena MI, Sanchez R, Munoz P, Cabello E, Rojas P, de
Olazaval E (1992): Trisomy 9: an additional case with unique man- ifestations. Am J Med Genet 43597-700.
Diaz-Mares L, Molina B, Carnevale A (1990): Trisomy 9 mosaicism in a girl with multiple malformations. Ann Genet (Paris) 33:165-168.
Feingold M, Atkins L (1973): Case report: a case of trisomy 9. J Med Genet 10:184-187.
Garden AS, Benzie RJ, Miskin M, Gardner HA (1986): Fetal cystic hy- groma colli: antenatal diagnosis, significance, and management. Am J Obstet Gynecol 154:221-225.
Hook EB (1977): Exclusion of chromosomal mosaicism: tables of 90%, 95% and 99% confidence limits and comments on use. Am J Hum Genet 29:94-97.
Kurnick J , Atkins L, Feingold M, Hills J , Dvorak A (1974): Trisomy 9: predominance of cardiovascular, liver, brain and skeletal anom- alies in the first diagnosed case. Hum Pathol5223-228.
Lauritsen JG (1982): This cytogenetics of spontaneous abortion. Res Reprod 14:3-4.
Louwen F, Rehder H, Tercanli S, Miny P, Holzgreve W (1992): Prena- tal diagnosis and management of two cases with complete trisomy 9 diagnosed by late CVS and amniocentesis. Prenat Diagn [Suppll 12:114.
Mace SE, Mackintyre MN, Turk KB, Johnson WE (1978): The trisomy 9 syndrome: multiple congenital anomalies and unusual patholog- ical findings. J Pediatr 92:446-448.
Qazi HQ, Masakawa A, Madahar C, Ehrlich R (1977): Trisomy 9 syn- drome. Clin Genet 12:221-226.
Schinzel A (1984): “Catalogue of Unbalanced Aberrations in Man.” Berlin: Walter de Gruyter, pp 371374.
Shere DM, Wang N, Howard OT, Peterson JC, Miller ME, Metlay LA, Abramowicz J S (1992): An infant with trisomy 9 mosaicism pre- senting as a complete trisomy 9 by amniocentesis. Prenat Diagn
Smart RD, Viljoen DL, Fraser B (1988): Partial trisomy 9-further de- lineation of the phenotype. Am J Med Genet 31:947-951.
Sutherland GR, Carter RF, Morris LL (1976): Partial and complete trisomy 9: delineation of a trisomy 9 syndrome. Hum Genet
12131-37.
321133-140.















![Prenatal diagnosis of mosaic trisomy 2 and literature review...trisomy 2. For case 1, cytogentic analysis showed a karyotype of mos 47,XY,+2[8]/46,XY[19] as shown in Fig.1. Of 27 colonies](https://img.pdfslide.net/doc/110x75/60facf977ba85d6edf705492/prenatal-diagnosis-of-mosaic-trisomy-2-and-literature-review-trisomy-2-for.jpg)













