Embed Size (px)
Citation preview

PreOP XRT: Oral fluoropyrimidines in randomized trials
n
NSABP R 04 open
1600Cape vs. FU infusional (+/- Oxaliplatin 2x2 factorial)
German Group open
ca. 180Cape vs. FU infusional (pre- and postOP)
Spanish Group ECCO 2005
149UFT/FA vs. FU/FAno difference in pCR, local failure, toxicity

No Bolus-FU anymore in Coloncancer
5FU inf / FAAndré et al., J Clin Oncol
2003
CapecitabinTwelves et al., NEJM 2005

Präoperative Radiochemotherapie des Rektumkarzinoms

Rödel, Arnold et al., Int J Radiation Oncology Biol Physics 2008
Phase I/II Trial: Preoperative Radiotherapywith CAPOX and Cetuximab
No increase of toxicity,
No increase of
perioperative complication rate

Tumor regression grading (Dworak and Keilholz 1997)
Cet-Capox-RT Capox-RT*
(n=46) (n=103)
Complete Regression 9% 19%
Good Regression (50 - 99%) 38% 55%
Moderate Regression (25 - 50%)
Poor Regression (< 25) 53% 26%
No Regression *Rödel, Liersch, Arnold et al., J Clin Oncol 2007
Rödel, Arnold et al., Int J Radiation Oncology Biol Physics 2007

Phase II trials with intensified preoperative Radiochemotherapy N pts. pCR (%)
1 FU / Cape 9 – 21
2FU / Cape Oxali 16 – 33
FU / Cape Irino 18 – 32
3
1Cape Cetuximab 40 5
2Cape Oxali Cetuximab 49 9
3Cape Irino Cetuximab 20 25
4Cape Irino Cetuximab 10 20
Arnold et al., Eur J Cancer 2005 (Suppl.); 1Machiels, Ann Oncol 2007; 2Arnold, ASCO 2007, 3Hofheinz et al., Int J Radiat Oncol Biol Phys 2006; 4Bertolini ASCO 2007

Bevacizumab RT in rectal cancer
N chemotherapy
Willett et al., ASCO 2007
22 5FU CI 50.4 Gy No increase in toxicitypCR: 22%
Czito et al., ASCO 2007
11 XELOX 50.4 Gy Lowered dose of Capecitabine due to diarrhea
Privitera et al., ASCO 2007
11 XELOX (6) XELIRI (5)
45.0 Gy. 3 pts.: hypertension, no further toxicity

Colon cancer stage III:Oxaliplatin combinations > FU/FA
André T et al., NEJM, 2004; Wolmark N et al., ASCO 2005
MOSAIC NSABP C07

Overall survival data: Supporting Oxaliplatin Combinations
De Gramont et al., ASCO 2007
Kolon-Ca. St. III 71%
Rektum-Ca. St. II/III 38%

CHemotheRapyOr No chemotherapy In CLEarmargins after neoadjuvantchemoradiationin locally advanced rectal cancer (CHRONICLE).
With 800 patients and p<0.05:
Primary endpoint: 3-yr DFS-85% power to detect a 10% increase ie. 40% -50%
Secondary endpoints: overall survival, toxicity
RA
ND
OM
IZA
TIO
N
Patients with locally advanced
rectal cancer
Capecitabine + Oxaliplatin
6 courses
Follow-up only
Pre-operative chemoradiation min 45Gy and
fluoropyrimidine based
chemotherapy
RO resection achieved

baseline assessment
within 14 days prior to
randomization
INVESTI-GATIONAL
ARM
capecitabine
oxaliplatin
RTx
RA
ND
OM
IZA
TIO
N
locally advanced
rectal cancer
clinical stage T3 or T4 or any node-positive disease
ECOG PS <2
CONTROL ARM
capecitabine
RTx
INVESTI-GATIONAL
ARM
capecitabine
oxaliplatin
6 cycles
CONTROL ARM
capecitabine
6 cycles
follow-up
follow-up
max.2 weeks days 1-38 4-6 weeks
SU
RG
ER
Y(T
ME)
SU
RG
ER
Y(T
ME)
6-8 weeks 18 weeks 5 years
Treatment Arms in PETACC-6

CapecitabineOxaliplatin
RTx
RA
ND
OM
IZA
TIO
N
Locally Advanced
Rectal Cancer
Stage II
or III
5-FUOxaliplatin
RTx
FOLFOX + Bevacizumab12 cycles *
FOLFOX12 cycles *
SU
RG
ER
Y(T
ME)
5-FURTx
CapecitabineRTx
RA
ND
OM
IZA
TIO
N
NSABP R-04
* Patients with neoadjuvant oxaliplatin receive up to 9 courses followed by 5-FU/Leucovorin with (arm II) or without
(arm I) bevacizumab for up to 3 courses.
US-Intergroup trial E5204
NSABP US-Intergroup Trial - Rectal Cancer
N = 2100N = 1606
2 x 2 factorial

Rödel et al. JCO 2007
Phase II Trial: Pre- and Postoperative (Radio-) Chemotherapy with XELOX

Neadjuvant XELOX followed by Chemoradiationin MRI defined Poor-Risk Rectal Cancer
SOxaliplatin
xeloda
Poor Risk: ≥ 5mm into perirectal fat or ≤ 1mm to mesorectal fasciaT3 at or below levatorsT1-4N2
CR+PR:88%
CR+PR:97%
pCR:24%
Chau I. et al. J Clin Oncol 2006
n=77

Predictors for pCR with Neoadjuvant Treatment
Response % No Response % p
TS 0,20
low 3 14 18 86
high 10 32 21 68
P53 0,71
negative 2 15 11 85
positive 11 26 31 74
VEGF 0,31
negative 7 33 14 67
positive 5 17 24 83
p21 0,74
negative 4 18 8 82
positive 8 25 24 75
Negri et al. Br J Cancer 2008

Preoperative Radiochemotherapy in Rectal Cancer: VEGF as Prognostic factor?
Giralt et al. Oncology 2006

Molecular Prognostic Factors
To select the right patient for the right treatmentintensity
Save toxicity and money
Increase survival for those who need it
But still 40-50% of the patients still die!!!!!

Capecitabin / Oxaliplatin = 5FU/FS / Oxaliplatin
NO16966; Cassidy et al., ASCO 2007 1.Line
HR 1.04
NO16967; 2nd lineRothenberg et al., ASCO 2007
HR 1.03
AIO 1.Line
Porschen et al.,
JCO 2007
HR 1.17
TTD 1.Line
Diaz Rubio et al.,
JCO 2007
HR 1.18
France 1.Line
Ducreux et al.,
ASCO 2007
HR 1.00
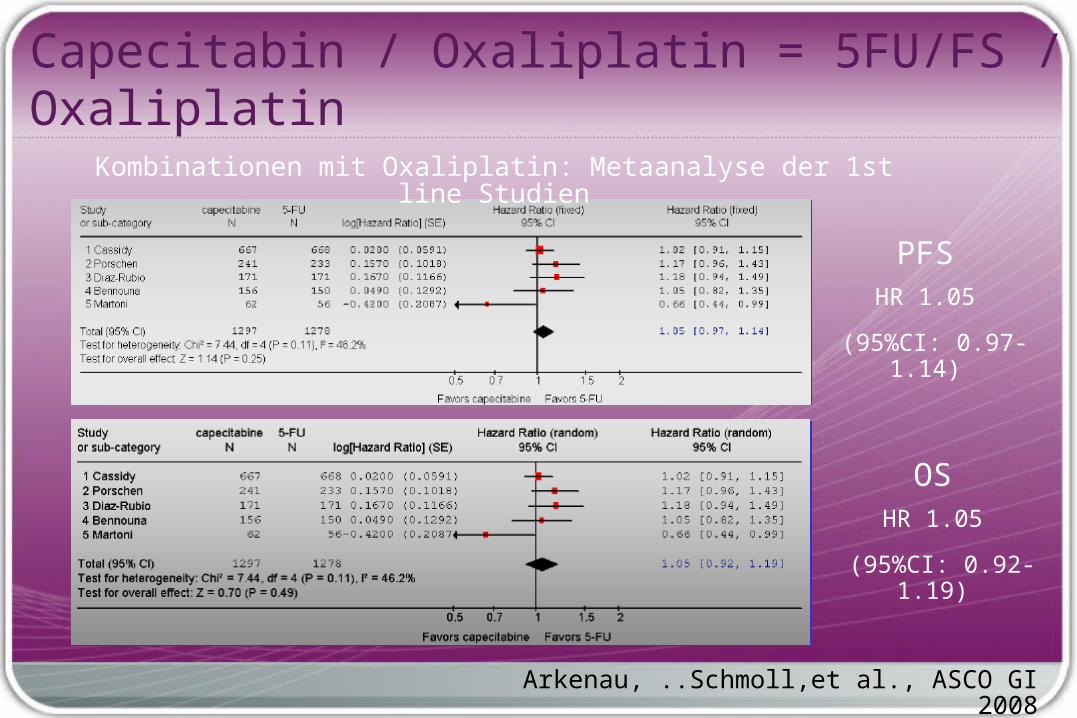
Arkenau, ..Schmoll,et al., ASCO GI 2008
Kombinationen mit Oxaliplatin: Metaanalyse der 1st line Studien
PFSHR 1.05
(95%CI: 0.97-1.14)
OSHR 1.05
(95%CI: 0.92-1.19)
Capecitabin / Oxaliplatin = 5FU/FS / Oxaliplatin

Potentielle Molekulare Targets - Kolon-Ca.Growth factors, Rezeptoren,
HER family, EGFR, IGF I/II Rec.…
Angiogenese und Extracelluläre Matrix
VEGF(R), MMPs, Integrine,..
Mechanismus für Cell Survival und Regulation der Apoptose
Cyclin abh. Kinasen, mTOR, cGMP, COX2, p53, bcl-2 … Proteasom
Tumor-assozierte AntigeneGangliosides, CEA, MAGE,
EpCam
Intracelluläres Signaling
Ras, raf, MAPK, MEK, ERK, PKC, PI3K –IGF I/II

Saltz et al., ASCO 2007
RR-Rate gleich FOLFOX-beva 9.4 mos PFS 1 Monat besser XELOX-beva 9.3 mos.
FOLFOX / XELOX +/- BevacizumabN=1400
Gesamtüberleben gleich

CRYSTAL-Studie
Van Cutsem et al., ASCO 2007

FOLFOX-4 + Cetuximab
FOLFOX-4
EGFR-exprimierende
mCRC Patienten
Strata:ECOG 0-1,2
n=169
n=168
OPUS-Studie
Bokemeyer et al., ASCO 2007

Cetuximab Kombinationen
N Rem.-Rate
Steigerung mit Cetuximab
p
CALGBFOLFOX or
FOLFIRI 238 + 14% 0.03
OPUS FOLFOX 337 + 10% 0.06
CRYSTAL FOLFIRI 1200 + 8% 0.004
Vennok et al., ASCO 2006; Bokemeyer et al., ASCO 2007; Van Cutsem et al., ASCO 2007

CRYSTAL - Studie: PFS
Van Cutsem et al., ASCO 2007