Embed Size (px)
Citation preview

PREOPERATIVE FACTORS ASSOCIATED WITH ANESTHESIA FAILURE
FOR PATIENTS UNDERGOING NON-SURGICAL ROOT CANAL THERAPY;
A NATIONAL DENTAL PRACTICE-BASED RESEARCH NETWORK
DPBRN STUDY
A THESIS
SUBMITTED TO THE FACULTY OF THE GRADUATE SCHOOL
OF THE UNIVERSITY OF MINNESOTA
BY
DUSTIN FREDERICK WEITZ
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS
FOR THE DEGREE OF
MASTER OF SCIENCE
Dr. Ronald Ordinola-Zapata, Dr. Donald Nixdorf, Dr. Scott McClanahan
AUGUST 2020

© Dustin Frederick Weitz, 2020

i
DEDICATION
To my wife Melissa Dawn Weitz, and my children Alexander Edward and Elizabeth
Anne Weitz, you have shown great strength and resiliency in supporting me during my
time as a resident.
To my father, Gerald Edward Weitz, D.D.S, thank you for being a great mentor and role
model.
To my mother, Consuelo Joyce Weitz, thank you for your unwavering kindness.
To my brother, Gerald Rockford Weitz, thank you for your sage advice and support.

ii
ACKNOWLEDGEMENTS
The following people have been instrumental in my development in dentistry and the
specialty of endodontics; with sincere gratitude and appreciation:
Dr. Scott McClanahan, Dr. Don Nixdorf, Dr. Ronald Ordinola-Zapata, and Dr. Carolina
Rodriguez-Figueroa for their knowledge and wisdom during my education.
Michael Shyne, M.S. for his expertise in biostatistics.
Our exceptional clinical faculty for their wealth of knowledge and experience:
Dr. Omar Abusteit, Dr. Ramon Aguirre, Dr. Dan Ang, Dr. Scott Doyle, Dr. Tom Karn,
Dr. Bob Kauffman, Dr. Debra Majerus, Dr. Philip McKenzie, Dr. Jeff Ryan, Dr. Jim
Spitzmueller, and Dr. Ken Zucker.
All my co-residents for their insights, support and friendship, with special thanks to:
Class of 2020 – Dr. Jeff Heyse and Dr. Chris Lai
Class of 2019 – Dr. J.T. Crepps, Dr. Colby Dimond, and Dr. Daryl Grigsby Jr.
Class of 2021 - Dr. Ashley Asano, Dr. Jonas Dale, Dr. Lisa Kandella, and Dr. Michael
Pham
Dr. W. Craig Noblett, for continuing tradition of excellence in endodontics at the
University of Minnesota.
University of Minnesota, Department of Graduate Endodontics Assistants and Staff.

iii
ABSTRACT
Introduction: Providing effective local anesthesia is a critical component of the RCT
treatment. Patients and providers are more satisfied if local anesthesia is successful. The
aim of this study was to analyze data collected by The National Dental Practice-Based
Research Network (DPBRN) during non-surgical root canal therapy to identify
preoperative factors associated with local anesthesia failure during treatment in the
private practice setting.
Methods: The DPBRN, consisting of 46 general dentists and 16 endodontists from five
geographic areas, enrolled 708 patients in the study, an analysis of patients treated in one
visit vs. multiple was done finding no statistical difference in failure rates between the
groups in any model. To standardize the treatment rendered, patients treated in multiple
appointments were excluded from the study, patients who had general anesthesia, IV
sedation or oral sedation were also excluded. Not all survey questionnaires were
completely filled out, patients with missing data for a given variable were noted as
missing in the analysis. Three methods for defining anesthesia failure: Method 1-patient
reported level of numbness, Method 2-provider reported quality of anesthesia, and
Method 3-provider reported use of supplemental anesthesia after initial injections
required to obtain adequate anesthesia during the procedure. Numerous pre-operative
factors were investigated and differences between failure groups, for each failure
measure, were estimated by chi-square tests of independence for categorical variables and
t-tests for numeric variables. A stepwise linear regression model using AIC statistic as
fitness criteria for each method was created to identify variables associated with failure
outcomes. The regression models give odds ratios for factors associated anesthesia
failure.
Results: Overall anesthesia failure rates were 4.90%, 14.61% and 29.96% for Methods
1, 2 and 3 respectively. Method 1 found provider experience, diabetes, current smoking
habit, patient expected outcome of treatment, sharp pain, and spontaneous pain to be
significant when analyzed individually. The regression model found provider experience,

iv
diabetes, preoperative fear, number of days in pain, sharp pain, spontaneous pain and
severe pain to be significantly correlated with anesthesia failure. Method 2 found
provider type, diabetes, pain interference in recreational and social activities, pain
provoked by stimulus, pain made worse by stress, percussion sensitivity, biting
sensitivity, and presence of a sinus tract to be significant when analyzed individually.
The regression model found provider experience, provider type, diabetes, and pain
interfering in recreation and social activities to be significantly correlated with anesthesia
failure. Method 3 found provider type, patient age, pain interference with daily activities,
sharp pain, pain provoked by stimulus, maxillary vs mandibular, presence of a periapical
radiolucency, responsiveness with cold, lingering pain with cold, and pulp vitality
confirmed with bleeding upon access to be significant when analyzed individually. The
regression model found provider experience, provider type, patient income from $10,000-
29,000, diabetes and pain interfering in recreational and social activities to be
significantly correlated with anesthesia failure.
Conclusions: The results from this study generally agree with prior studies finding that
symptomatic teeth with vital pulps have more anesthesia failures. Patient self-reported
history of diabetes was found to lead to more anesthesia failures in multiple models;
further research is needed to understand the mechanism of anesthesia failure related to
diabetes. Multiple models found results related to provider experience and provider
training found that more experienced providers and those with higher levels of training
had significantly fewer anesthesia failures. Pulpal anesthesia is more difficult to achieve
than soft tissue anesthesia. Prior research reveals oral surgery departments are
responsible for anesthesia training in most dental school and endodontic departments are
not involved; the results of this study indicate that endodontic departments should be
involved in a team approach with oral surgery departments regarding local anesthesia
training in dental schools to shorten the learning curve for providers.
Keywords: Endodontics, Local Anesthesia, Practice Based Research Network

v
TABLE OF CONTENTS
Dedication………………………….…………………………...………………….……...i
Acknowledgments……………………………………………………...…………………ii
Abstract…………………………………………………………………………………...iii
Table of Contents………………………………………………………………………….v
List of Tables.……………………………………………………………………………..vi
List of Figures……………………………………………...…………………………….vii
List of Appendices………………………………………………………………………viii
Introduction………………………………………………………………………………..1
Literature Review………………………………………………………………………….6
Specific Aims…………………………………………………………………………….15
Hypotheses……………………………………………………………………………….16
Null Hypotheses……………………………………………………………………….…17
Materials and Methods…………………………………………………………………...18
Results……………………………………………………………………………………28
Discussion………………………………………………………………………………..38
Conclusions…………………………………….………………………………………...57
References………………………………………………………………………………..58
Appendices……………………………………………………………………………….66

vi
LIST OF TABLES
Table 1. Anesthesia Failure Rate by Method….……………………...…………….……28
Table 2. Method 1: Significant Factors Associated with Anesthesia Failure……...…....31
Table 3. Method 1: Factors Associated with Anesthesia Failure in the Statistical
Regression Model………………...……………………………………………………...31
Table 4. Method 2: Significant Factors Associated with Anesthesia Failure…………...33
Table 5. Method 2: Factors Associated with Anesthesia Failure in the Statistical
Regression Model…………...…………………………………………………………...34
Table 6. Method 3: Significant Factors Associated with Anesthesia Failure……….......36
Table 7. Method 3: Factors Associated with Anesthesia Failure in the Statistical
Regression Model……………...………………………………………………………...37

vii
LIST OF FIGURES
Figure 1. Distribution for failure defined by patient reported numbness……...……..........22
Figure 2. Distribution for failure defined by provider reported quality of anesthesia..........23
Figure 3. Distribution for failure defined by use of supplemental anesthesia……...…..….24

viii
LIST OF APPENDICES
Appendix I – Patient Contact Form………………………….…….....……………….....65
Appendix II – Patient Survey Before Treatment……………………….…………...…...66
Appendix III – Dentist Survey Before Treatment…………………………………..........60
Appendix IV – Dentist Survey Post-Treatment……………………………………….....71
Appendix V – Patient Survey Immediately After Treatment……………………………73
Appendix VI – Dentist Pain and Anxiety Management Form…………………………...74
Appendix VII – Provider, Patient, and Tooth Characteristics by Number of Visits…….76
Appendix VIII – Anesthesia Failure Rates Method 1: Patient Reported Numbness…….79
Appendix IX - Anesthesia Failure Rates Method 2: Provider Reported Quality………..82
Appendix X – Anesthesia Failure Rates Method 3: Supplemental Anesthesia………….85

1
INTRODUCTION
The ability to provide safe and effective local anesthesia is perhaps the most
important skill a dentist can develop. Barclay perfectly summarized the importance of
local anesthesia in dentistry by stating, “The cornerstone to anxiety and pain control in
dentistry is a sympathetic, understanding and caring clinician, and one skilled in the use
of local anesthesia” (1). Achievement of profound local anesthesia prior to initiating root
canal therapy is a principal goal of every practitioner who provides endodontic treatment.
Endodontic treatment is more efficient and less traumatic for the patient and dentist if
painful sensations have been effectively eliminated. Despite our best efforts, in the eyes
of the public, root canal therapy often has a poor reputation due to a perceived association
with extreme pain causing many patients to be highly anxious prior to, and during the
procedure; most often pain is well managed however there are a number of patients who
do not experience adequate anesthesia (2, 3).
Kaufman et al. found anesthesia failure to vary by type of injection administered
and found an overall failure rate of 13.7% when surveying dentists regarding anesthesia
failure (4). A follow up study regarding patient perception of anesthesia found patient
reported anesthesia success to be 69.7%; 13.7% of patients reported being not numb
enough, 14.3% reported pain but it was manageable and 2.2% reported not being able to
complete treatment due to inadequate anesthesia (5). Sherman et al. evaluated anesthesia
success in endodontic procedures with maxillary infiltration anesthesia and mandibular
block anesthesia using the Gow-Gates technique with either 1.8ml 2% lidocaine with
1:100,000 epi or 1.7ml 4% articaine with 1:100,000 epi and found and overall 87.5%

2
success rate based on patient reported pain on access with no significant differences
between arch or type of anesthetic (6).
The origins of modern local anesthesia trace back to the work of Dr. Carl Koller
who in 1884 reported the successful use of cocaine in aqueous solution for a variety of
surgical procedures on the eye (7). The prominent American surgeon, Dr. William
Halsted, who is credited for devising the inferior alveolar nerve block, found cocaine to
be an indispensable part of his armamentarium; tragically addiction to cocaine and
subsequently morphine led to his death, illustrating the limitations and dangers of cocaine
and the need for new local anesthetic agents. A great leap forward was made by the work
of Alfred Einhorn who developed several ester local anesthetics and patented procaine in
1904. A textbook publication by German surgeon, Heinrich Braun, in 1905 brought
procaine worldwide attention, touting its safety and efficacy (8).
With advances in chemistry, advances in techniques were quick to follow. In his
1919 text “Conduction and Infiltration Anesthesia” published by the Novocol Chemical
Mfg. Co., Nevin illustrates and describes many of the infiltration and block anesthesia
techniques that are still in use today. Nevin (9) reported a 60% success rate in
anesthetizing maxillary premolar and molar teeth by injecting into the spheno-maxillary
fossa in what we now call a maxillary or V2 block. Even in this early text, anesthesia for
endodontics was recognized as more difficult than for other procedures; a chapter was
dedicated to anesthesia for pulp extirpation. The chapter stated “the pulps of incisors,
cuspids, bicuspids and quite often upper molar teeth” could be painlessly removed with
local infiltration, however it goes on to discuss block anesthesia, stating “the extirpation
of pulps under conduction anesthesia is not as a rule uniformly successful” (9). By 1925,

3
in the 7th edition of his text on anesthesia, Dr. Braun stated “Novocaine injected into the
tissues, is an ideal anesthetic, which renders cocaine completely unnecessary” (8). To
this day, Novocain, the trade name of procaine, is synonymous with dental local
anesthesia.
Although procaine was a significant improvement over cocaine for local
anesthesia, there were numerous drawbacks including brief duration of anesthesia related
to vasodilation, instability and significant allergic reactions (10, 11). In 1943, two
Swedish chemists, Nils Lofgren and Bengt Lunqvist, working at the Organic Chemistry
Institute of Stockholm University developed several new amide anesthetic compounds,
one of which was known as L.L.30 which would be developed and tested by Astra and
become known as lidocaine. Testing revealed lidocaine to be more effective, reliable,
safer and more stable than procaine (10). In the 1950s through the 1970s, many other
amide local anesthetics were developed with different properties; experimentation with
different concentrations of vasopressors also enhanced their clinical usefulness (11).
When deposited in tissue, local anesthetics work by diffusing through the neural
membrane and binding to voltage gated sodium channels causing them to stay closed,
blocking impulse conduction. Local anesthetics consist of an aromatic ring that is
lipophilic, an intermediate ester or amide chain with an amine component at the end of
the chain. The pKa, lipid solubility and protein binding properties differ for each local
anesthetic; these differences in properties account for their different clinical
characteristics. In brief, the pKa or ionization constant is the pH at which half of the
anesthetic exists in its lipid soluble state and half in its water-soluble state. The molecule
must be uncharged to cross the neural membrane to act on the sodium channels, the

4
closer the pKa of a given anesthetic is to the pH of the tissue, the fewer molecules will be
in the ionized form and will therefore be able to pass through the membrane. After
crossing the membrane, some of the molecules will become water soluble and can act on
the sodium channels. Lipid solubility determines the potency of an anesthetic because
more lipid soluble molecules remain in the membrane, acting as a reservoir that releases
molecules over time. Bupivacaine has high lipid solubility making it very potent and as
such is administered in a 0.5% solution compared to less lipid soluble anesthetics that
may be 2-4% in concentration when delivered. Differences in protein binding ability
effect the duration; when bound to proteins on the membrane surface, the molecules tend
to linger at the site rather than diffusing away and entering the systemic circulation (12,
13).
Despite advances in techniques and chemistry, achievement of profound local
anesthesia does not occur in every case. The possible reasons for failure are abundant
and can generally be placed into 4 categories: 1) poor technique, 2) anatomic variability,
3) inflammation and infection, and 4) psychological factors (3, 14).
Regardless of the exact mechanism for failure, the ability to identify pre-operative
factors that contribute to anesthesia failure is invaluable. The main objective of this
study is to analyze data previously collected by The National Dental Practice-Based
Research Network (15) to identify pre-operative factors, easily measured and/or
identified by the dental practitioner, that are associated with failure of local anesthesia
when performing endodontic therapy, thereby aiding the practitioner in developing a
successful anesthesia protocol. The study of anesthesia failure was not the original intent
of the data collected by The National Dental Practice-Based Research Network used in

5
this study, however valuable pre-operative and post-operative information was collected
allowing for the study of a multitude of variables that may contribute to anesthesia failure
during root canal treatment. This is the first study using a large practice-based research
network to examine pre-operative factors related to anesthesia failure during endodontic
therapy. The three methods for defining anesthesia failure in this study are: 1) patient
reported level of numbness during the procedure, reported immediately after treatment, 2)
dentist reported quality of anesthesia reported after treatment and 3) the use of
supplemental anesthesia, defined as anesthesia given above and beyond the normal
anesthesia protocol typically used by the practitioner.

6
LITERATURE REVIEW
Endodontic procedures generally present the most challenges with local
anesthesia, particularly in cases with symptomatic irreversible pulpitis (2, 3, 16).
Methods of Assessing Local Anesthesia Success or Failure
A variety of methods to evaluate local anesthesia failure can be found in the
literature. Dobbs and DeVier were pioneers in the study of the clinical effectiveness of
dental local anesthesia who developed a patient and operator centered method for
evaluating anesthesia success in which Grade A represented anesthesia that was
acceptable to the operator and patient, Grade B was partial anesthesia where the patient
felt some pain but did not require any additional injections and Grade C was inadequate
anesthesia that required further injections (17). One example of using this technique was
Malamed’s study of the Gow-Gates mandibular block that evaluated over 4000 injections
at the University of Southern California; Grade A anesthesia was obtained in 91.9% of
cases and Grade B anesthesia in 5.35% of cases with a single injection giving an overall
failure rate of only 2.75%, compared to the reported failures of the traditional inferior
alveolar nerve block that varied from 4.9% to 29% failure with this grading system (18).
A caveat with this method is it does not mean the procedures were not completed; it only
means a supplemental injection was required which leads to one of the methods used in
this study with defining the use of supplemental anesthesia as a failure. Kaufman and
Weinstein used post-operative questionnaires given to both providers and patients to
assess anesthesia failure (4, 5).
Using pain during a dental procedure to evaluate anesthesia success on the surface
seems straightforward however pain perception is very complex and there are inherent

7
difficulties with this technique when studying anesthesia failure. Topazian discusses that
the sensation of pain in the absence of factors such as mood, lethargy and distraction is
relatively uniform and reproducible, however it is only a minor part of the pain
experience. The reaction to pain varies by the patient’s emotional state, age,
psychological make-up and racial, educational, cultural background and other factors; the
combination of all of these factors are what make up pain perception, even the operator’s
skill in distraction and suggestion may effect to perception of pain (19). When the pain
sensation is associated with the conditioned reaction to pain and the other peripheral
factors, one can see how the study of anesthesia success using perceived pain during a
stressful dental procedure stressful with numerous of patient preconceived notions can be
difficult. In recognition of this, investigators have tried to minimize these factors by
studying anesthesia in asymptomatic volunteers.
In the early 1980s several anesthesia studies used the electric pulp tester as part of
their evaluation method but not to define failure (20, 21). Dreven et al. were the first to
investigate the usefulness of the Analytic Technology Electric Pulp Tester (EPT) in
determining anesthesia failure and found that in teeth with normal and asymptomatic
pulps, an EPT reading of 80/80 guaranteed clinical analgesia, however in teeth with
symptomatic irreversible pulpitis, 80/80 predicted clinical analgesia only 73% of the time
(22). This finding lead to many studies defining anesthesia success and failure based on
the achievement of an EPT reading of 80/80 in asymptomatic patients. One of the first of
these studies compared 3 types of local anesthetics used for the periodontal ligament
injection finding 2% lidocaine with 1:100,000 to be more successful than 3% plain
mepivacaine and 2% plain lidocaine (23). Subsequent studies refined the definitions of

8
anesthesia success and failure requiring multiple consecutive readings of 80/80 with the
EPT being a failure and providing definitions for slow onset anesthesia, non-continuous
anesthesia and short duration anesthesia (24). The technique has been used in a multitude
of anesthesia studies on asymptomatic teeth that compared one anesthetic to another (23,
25, 26), one patient type to another (27) and one technique to another (28-31). Because
EPT studies are generally limited to normal and asymptomatic pulps, studies determining
anesthesia failure based on patient reported pain upon access were developed (32). This
type of study now typically uses a Heft-Parker visual analogue scale (33) to rate pain
upon endodontic access with no pain or mild pain considered an anesthesia success and
has been used in many studies (34-38). More recently, studies involving symptomatic
teeth have incorporated a Corah Dental Anxiety Scale to evaluate the effect of
preoperative anxiety on anesthesia (39, 40). As of 2015, The Ohio State University had
conducted at least 37 anesthesia studies using variations of these methods (41).
Reported Local Anesthesia Success and Failure Rates
Reported anesthesia failure rates show much variability. Kaufman et al. found
anesthesia failure to vary by type of injection administered and found an overall failure
rate of 13.7% when surveying dentists regarding anesthesia failure (4). When examining
patient self-reported anesthesia success, Weinstein et al. found 3 statistically significant
factors: 1) the greater the number of extra injections required, the higher the likelihood
of anesthesia failure, 2) patients with a history of not achieving profound local anesthesia
have a tendency for subsequent anesthesia failure, and 3) the greater the level of pre-
operative fear associated with the dental work, the greater chance of anesthesia failure;
the overall patient reported success rate was only 69.7% (5). Regarding endodontic

9
anesthesia, an overall failure rate in patients with symptomatic irreversible pulpitis was
found to be 12.5% encompassing both maxillary and mandibular teeth with no difference
between lidocaine or articaine with 1:100,000 epi (6). However, much lower success
rates have been reported even in asymptomatic teeth; such as mandibular success rates of
25%, 62% and 53% for the lateral incisor, first premolar and first molar respectively with
the inferior alveolar block; 16%, 44% and 38% with the Gow-Gates and 13%, 50% and
27% with the Vazirani-Akinosi technique for the same teeth respectively with none of the
techniques providing complete pulpal anesthesia (42).
To illustrate the variability in assessing success rates, one can look further at
studies comparing the Gow-Gates and Vazirani-Akinosi technique; in patients with
symptomatic irreversible pulpitis, Sherman et al. found a success rate of 87.5% (6), while
Aggarwal et al. found the inferior alveolar block to be successful 36% of the time, the
Vazirani-Akinosi 41% of the time and the Gow-Gates 52% of the time (43). Seeing the
discrepancy in these reported success rates, Click et al. examined the Gow-Gates and
Vazirani-Akinosi techniques in patients with symptomatic irreversible pulpitis and found
that with 3.6ml of 2% lidocaine with 1:100,000 epi, the Gow-Gates achieved lip
numbness 92% of the time with successful pulpal anesthesia upon endodontic access 35%
of the time, while the Vazirani-Akinosi block achieved lip numbness 63% of the time and
pulpal anesthesia 35% of the time (44). With variation of 13-87.5% in success rates,
confounding factors are likely involved.
Local Anesthesia Failures Related to Technique
A common issue with local anesthetic technique is depositing solution in an area
away from the targeted nerve; Roda et al. reviews the anatomy of the trigeminal nerve

10
and suggests inadequate knowledge of the anatomy can lead to missed blocks,
intramuscular and intravascular injections (45). Regarding the inferior alveolar block,
Milles suggests the 2 most common mistakes are positioning of the needle too far
medially and positioning the needle too far inferiorly (46). Needle deflection due the
position of the bevel has been speculated to cause inadvertent missed block anesthesia
however this idea was shown not be a factor by Steinkruger et al (28).
Various alternative blocks such as the maxillary nerve or V2 block for the upper
teeth and the Gow-Gates and Akinosi blocks for the mandibular teeth can be helpful (47-
49). When an initial block fails, alternative block injection techniques are often effective
(50). Saatchi et al. found that the combination of an inferior alveolar block and a Gow-
Gates block significantly improved the anesthesia success rate over either alone (51).
There is evidence that the addition of supplemental anesthesia in the form of PDL (2, 52)
or a buccal infiltration with 4% articaine (32, 53) increases local anesthesia success.
Kanaa et al. found either buccal infiltration with 4% articaine or intra-osseous injection
with 2% lidocaine with epinephrine to be superior to repeated inferior alveolar blocks or
the PDL, with the buccal infiltration being the best supplemental technique in mandibular
molars after initial failure (54).
Even the speed of injection may play a role in anesthesia failure; in a randomized
controlled clinical trial of asymptomatic patients, Kanaa et al. found for the inferior
alveolar nerve block that not only were slower injections of over 60 second more
comfortable than injections given in 15 seconds, they were also more effective in
achieving pulpal anesthesia (55). In contrast, Aggarwal et al. found that speed of
injection had no significant effect on success of the inferior alveolar nerve block in

11
symptomatic patients, however, double the amount of anesthetic was used. Aggarwal et
al. found agreement that the slow deposition was more comfortable for patients (56).
Rood speculated that rapid injection could cause enough pressure in the tissue to separate
fascial spaces and allowing the anesthetic to escape from the intended target area (57).
Aggarwal found increasing the volume of anesthetic improves and efficacy of the
inferior alveolar block in patients with irreversible pulpitis (38), however Fowler et al.
found no difference and attributed Aggarwal’s finding to be related to the small sample
size (58). In another study with over 3000 patients, Fowler et al. found that by doubling
the volume of anesthetic to 3.6ml, there were significantly less missed inferior alveolar
blocks, but this is different than achieving pulpal anesthesia (41). In the maxillary arch,
doubling the volume of anesthetic from 1.8ml to 3.6ml did not increase the efficacy but
provided a longer duration of anesthesia which can play a role in patient perception of
anesthesia success in longer procedures (59).
In a review of techniques that can be used for successful anesthesia in teeth with
symptomatic irreversible pulpitis, Nusstein et al. argues that the most effective way to
anesthetize the “hot tooth” when conventional techniques have failed are to use the intra-
osseous injection, periodontal ligament injection, buccal infiltration with articaine and the
intrapulpal injection; techniques that are not significant for improving anesthesia success
were stated to be anesthetic type, volume, alternative blocks, bevel position, and
premedication with ibuprofen, acetaminophen, methylprednisolone or triazolam (16). In
an updated review, supplemental anesthesia was again stated to be the best way to
manage initial anesthesia failure; several additional factors that were found to not be
significant were discussed including premedication with acetaminophen with

12
hydrocodone, ketorolac or alprazolam, use of liposomal bupivacaine, the use of buffered
anesthetics, and different concentrations of epinephrine (60). Nitrous oxide was found to
improve the success rate of the inferior alveolar block, but not enough to eliminate the
use of supplemental anesthesia (61).
Local Anesthesia Failures Related to Anatomic Factors
Different that anesthesia failure based on missing the normal anatomy, accessory
innervation that is not common to all patients can play a role in local anesthesia failure.
Frommer et al. found that mylohyoid nerve can contain sensory nerves from mandibular
teeth and can lead to anesthesia failure (62). Cross arch innervation exists in the
mandibular incisors (57) and can be successfully overcome with labial infiltration (29,
57, 63). Loetscher et al. found the posterior superior alveolar nerve to be involved in first
molar innervation 100% of the time and in 28% of first molars, the middle superior
alveolar nerve contributed requiring an additional buccal infiltration (64). Other anatomic
considerations not related to accessory innervation, rather related to individual body
variation include a wide flaring mandible, a wide or long ramus, bulky musculature and
abundance of adipose tissue, and edentulism (46).
Local Anesthesia Failures Related to Inflammation
Inflammation and infection may have a significant impact on the efficacy of local
anesthetics. Rood demonstrated that inflammation significantly increases the evoked
action potential of peripheral nerves making it more difficult to be blocked by local
anesthetics (65). Many practitioners believe that local pH plays a significant role in
anesthesia failure however Punnia-Moorthy et al. found the pH changes in inflammation
to be relatively small due to an increased buffering capacity of the inflamed tissue (66).

13
Increased blood flow in inflammation may allow for faster uptake into the systemic
circulation, lowering the efficacy however concentrations of 1:50,000 epinephrine vs.
1:200,000 epinephrine had no significant difference in anesthesia success of the inferior
alveolar nerve block in patients with irreversible pulpitis (67). In response to tissue
injury, sprouting of sensory nerves can occur increasing the number of pain related
receptors (68). During inflammation, concentrations of neuropeptides such as calcitonin
gene related peptide are altered and this may alter the capacity of the local anesthetics to
function (69). Similarly, Caviedes-Bucheli et al. found that inflammation from occlusal
trauma causes an increase in the levels of substance P, which can lead to sensitization of
the nerves(70). Neurons also contain multiple types of sodium channels, in the presence
of inflammation, tetrododoxin resistant sodium channels can become upregulated (71, 72)
and these TTX resistant sodium channels require a 3-4 times greater concentration of
local anesthetic to block nerve conduction than the TTX sensitive channels (73, 74).
Local Anesthesia Failures Related to Psychological Factors
Melzack and Wall famously discuss the complexities of pain conduction and
describe that a neurophysiologic reaction set off by impending or current tissue damage is
not adequate to describe pain conduction and a psychological component plays a role
(75). The effect of topical anesthetic on injection pain is controversial, Cho et al. found
that the use of topical anesthetic reduce both pain on needle insertion and pain during
deposition of the anesthetic solution; the highly anxious patient had more pain with
injections however the use of topical anesthetic reduced the effect that anxiety had on
pain with injection (76). For many patients, the idea of having a dental local anesthetic
injection induces fear which can result in insufficient anesthesia resulting in even more

14
fear (77). Lin discussed the idea of pain catastrophizing in dental patients which refers to
having exaggeratedly negative thoughts about anticipated or actual pain. Patients with a
greater tendency to catastrophize may tend to avoid treatment and may also have altered
sensations of pain (78). Central sensitization may play a role in local anesthesia failures
and could require pharmacological management and/or treatment with a cognitive-
behavioral therapist (3).
Practice-Based Research Networks
Practice-based research started becoming common in the medical literature in the
early 1980s and has continued to evolve and improve, eventually becoming a part of
dental research (79). A multitude of studies have been carried out using dental practice-
based networks. In endodontics, Nixdorf et al. found that it is feasible to conduct large-
scale prospective cohort studies in the field of endodontics (15). Subsequently studies
related to persistent dentoalveolar pain after endodontic therapy (80-82), predictors of
severe postoperative pain after endodontic therapy (83), reduction in pain after
endodontic therapy (84), the validity of preoperative sensibility testing to the visualized
status of the pulp during endodontic therapy (85) have been completed using data from a
practice based network. The success and impact of practice-based dental research has led
to larger networks with more providers and patients enrolled (86).

15
SPECIFIC AIMS
1) To determine which, if any, preoperative patient, tooth and provider characteristics
investigated by The National Dental Practice-Based Research Network are significantly
associated with local anesthetic failure during single appointment root canal therapy
when using patient self-reported level of numbness to define failure.
2) To determine which, if any, preoperative patient, tooth and provider characteristics
investigated by The National Dental Practice-Based Research Network are significantly
associated with local anesthetic failure during single appointment root canal therapy
when using dentist reported quality of anesthesia to define failure.
3) To determine which, if any, preoperative patient, tooth and provider characteristics
investigated by The National Dental Practice-Based Research Network are significantly
associated with local anesthetic failure during single appointment root canal therapy
when defining anesthesia failure as the use of supplemental anesthesia above and beyond
what the practitioner would use as their standard anesthetic protocol.

16
HYPOTHESES
1) There are preoperative patient, tooth and provider characteristics investigated by The
National Dental Practice-Based Research Network that are significantly associated with
local anesthetic failure during single appointment root canal therapy when using patient
self-reported level of numbness to define failure.
2) There are preoperative patient, tooth and provider characteristics investigated by The
National Dental Practice-Based Research Network that are significantly associated with
local anesthetic failure during single appointment root canal therapy when using dentist
reported quality of anesthesia to define failure.
3) There are preoperative patient, tooth and provider characteristics investigated by The
National Dental Practice-Based Research Network that are significantly associated with
local anesthetic failure during single appointment root canal therapy when defining
anesthesia failure as the use of supplemental anesthesia above and beyond what the
practitioner would use as their standard anesthetic protocol.

17
NULL HYPOTHESES
1) There are no preoperative patient, tooth and provider characteristics investigated by
The National Dental Practice- Based Research Network that are significantly associated
with local anesthetic failure during single appointment root canal therapy when using
patient self-reported level of numbness to define failure.
2) There are no preoperative patient, tooth and provider characteristics investigated by
The National Dental Practice-Based Research Network that are significantly associated
with local anesthetic failure during single appointment root canal therapy when using
dentist reported quality of anesthesia to define failure.
3) There are no preoperative patient, tooth and provider characteristics investigated by
The National Dental Practice-Based Research Network that are significantly associated
with local anesthetic failure during single appointment root canal therapy when defining
anesthesia failure as the use of supplemental anesthesia above and beyond what the
practitioner would use as their standard anesthetic protocol.

18
MATERIALS AND METHODS
Overview
This investigation examines pre-operative factors associated with local anesthesia
failure in single appointment initial orthograde root canal therapy through the analysis of
existing data collected as part of an observational study conducted by the National Dental
Practice-Based Research Network (DPBRN) for the purpose of studying pain and quality
of life burden associated with initial, non-surgical root canal therapy (15). The mission
of the National Dental Practice-Based Network is “To improve oral health by conducting
dental practice-based research and by serving dental professionals through education and
collegiality.” The history, administrative structure, study development process, and
recruitment and retention of dental practices are described by Gilbert, et al (79). Three
methods for defining anesthesia failure were used: 1) patient reported level of numbness
during the procedure, 2) provider reported quality of anesthesia reported after treatment,
and 3) supplemental anesthesia administered after initial injections. For standardization
purposes, the investigation was limited to teeth in which the root canal therapy was
completed in a single appointment. A sensitivity analysis was completed between the 1
visit and 2+ visit groups looking for differences in anesthesia failure rates and no
difference was found, see table 1.
Study Design and Setting
Forty-six general dentists and 16 endodontists from 5 geographic areas in the
United States and Europe were recruited, trained and calibrated for the data collection
portion of the study by the DPBRN; patient enrollment and baseline patient
characteristics were collected over 6 months with questionnaires completed by the

19
providers before and immediately after treatment with patient questionnaires completed
at before treatment, immediately after treatment and 1 week, 3 months and 6 months after
obturation (15). This study analyzed baseline data and data from questionnaires
completed by the patients and dental practitioners immediately prior to and immediately
following the root canal therapy. Preoperative and postoperative questionnaires can be
found in appendices 1-5. Exact endodontic technique for cleaning, shaping and
obturating were not calibrated but rather based on the clinicians’ experience and training.
Patient Eligibility and Recruitment
After training and calibration by DPBRN staff, practitioners screened 1081
consecutive patients who met eligibility requirements for the study. Participation was
voluntary. Inclusion criteria were patient age between 19 and 70 with a permanent tooth
requiring initial non-surgical root canal therapy. Exclusion criteria were iatrogenic pulp
exposure, prior enrollment in the study (each patient could only have one tooth involved
in the investigation), prior endodontic therapy initiated for the tooth, significant and
obvious cognitive impairment, inability to read, understand and complete the patient
questionnaire gathering baseline information and any patient who did not feel they could
provide follow-up information. Of the 1081 patients screened, 708 of the enrolled
participants completed the study.
Defining Anesthesia Failure
Review of the literature reveals multiple techniques for measuring anesthesia
failure in procedure-based studies with the two broad categories being patient reported
quality of anesthesia and provider reported quality of anesthesia (4, 5). It was also noted
that in procedure-based studies, the necessity of using of supplemental anesthesia to

20
complete the procedures has been used as a method to determine failure (18). The survey
questions in this dataset allow for evaluated anesthesia failure with 3 methods.
For Method 1, patient reported level of numbness during the root canal was used
to determine failure. Appendix V is the questionnaire completed by the patient
immediately after the completion of the treatment before leaving the dental office.
Question 2 (Q09P1NUMB) reads “Please rate how numb your tooth felt during the root
canal treatment (mark one): a. the tooth was not numb enough, b. the tooth was numb
enough, or c. the tooth was too numb.” For the purposes of this study, answer “a” was
considered a failure in Method 1.
For Method 2, provider reported quality of anesthesia was used to determine
failure. Appendix VI is the questionnaire completed by the provider immediately after
treatment. Question 5 (Q07D1ANESQ) reads “During the root canal procedure, what
was your impression about the quality of the local anesthesia? (mark one that is
representative of the entire procedure) a. Excellent, patient felt ‘nothing’, b. Adequate,
patient experienced non-painful sensations, c. Marginal, patient experienced some pain,
and d. Less than marginal, patient experienced a lot of pain.” For the purposes of this
study, answers of “c” or “d” were considered a failure in Method 2.
For Method 3, provider reported use of supplemental anesthesia was used to
determine failure. The questionnaire in Appendix VI was also used for this method.
Question 8 reads “Were any of the following necessary to obtain adequate anesthesia to
perform treatment? (mark all that apply) a. Second injection of the same type into the
same location, b. Second injection of the same type into a slightly different location, c.
Block anesthesia technique different from the previously provided (e.g., Gow-Gates or

21
PSA), d. Periodontal ligament (PDL) injection, e. Intraosseous injection other than PDL
(e.g., Stabident or X-tip), f. Intrapulpal injection, g. None of the above.” When entered
into the Microsoft Excel spreadsheet, all were entered as either “1” yes, or “0” no. By
answering yes to answer “g” providers indicated that no supplemental anesthesia was
used (Q07D1NONE). For the purposes of this study, when “g” was unanswered,
supplemental anesthesia was required to perform treatment and this was considered a
failure in Method 3.
Inclusion/Exclusion Criteria
For the purposes of this investigation, 24 patients were excluded due to the use of
general anesthesia, 3 were excluded due to the use of intravenous sedation, 2 were
excluded due to the use of enteral sedation, all of which could affect the perception of
anesthesia quality and 8 questionnaires were not fill out regarding the use of general, IV
or oral conscious sedation and were excluded for this reason. Appendix VI contains the
dentist survey regarding pain and anxiety management. Any patients with incomplete
questionnaires for each method were excluded; 3 in method 1 and 8 in method 3. Any
remaining patients who required multiple treatment appointments for obturation were
excluded. Figures 1-3 show the exclusion process for each method with patient
distribution.

22
Method 1: Patient Reported Level of Numbness
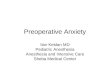
Figure 1. A flowchart depicting the inclusion criteria and distribution of patients using patient self-reported level numbness reported immediately after treatment to define anesthesia failure (Q09P1NUMB). “Numb enough” and “too numb” are considered as anesthesia success, “not numb enough” is considered a failure. Overall anesthesia failure rate was 4.90% (26/531) with this method.
Patients and teeth receiving RCTn=708
Anesthesia Failuren=26
Anesthesia Successn=505
Patients and teeth included in studyn=531
Excluded (n=177)*General anesthesia used during treatment
(PMGENANES) n=24*IV sedation used during treatment
(PMIVSEDA) n=3*Oral sedation used during treatment
(PMAXIOL) n=2* Questionnaires not completed regarding
sedation n=8*Patients not obturated at 1st appointment
(Q07D1RCT) n=137*Patients not reporting level of numbness
(n=3) (Q09P1NUMB)

23
Method 2: Provider Reported Quality of Anesthesia
Figure 2. A flowchart depicting the inclusion criteria and distribution of patients using provider reported quality of anesthesia to define anesthesia failure (Q07D1ANESQ). Data was reported as 1=Excellent, patient felt nothing, 2=Adequate, patient experienced non-painful sensations, 3=Marginal, patient experienced some pain and 4=Less than marginal, patient experienced a lot of pain. For this method, reports of 3 and 4 defined an anesthesia failure. Overall anesthesia failure was 14.61% (78/534) with this method.
Patients and teeth receiving RCTn=708
Anesthesia Failuren=78
Anesthesia Successn=456
Patients and teeth included in studyn=534
Excluded (n=174)*General anesthesia used during treatment
(PMGENANES) n=24*IV sedation used during treatment
(PMIVSEDA) n=3*Oral sedation used during treatment
(PMAXIOL) n=2*Questionnaires not completed regarding
sedation n=8*Patients not obturated at 1st appointment
(Q07D1RCT) n=137

24
Method 3: Supplemental Anesthesia Administered After Initial Injections
Figure 3. A flowchart depicting the inclusion criteria and distribution of patients with the use of supplemental anesthesia to define failure (Q07D1NOANES). Overall anesthesia failure was 29.96% (160/534) with this method.
Patients and teeth receiving RCTn=708
Anesthesia Failuren=160
Anesthesia Successn=374
Patients and teeth included in studyn=534
Excluded (n=171)*General anesthesia used during treatment
(PMGENANES) n=24*IV sedation used during treatment
(PMIVSEDA) n=3*Oral sedation used during treatment
(PMAXIOL) n=2*Questionnaire not completed regarding
sedation n=8*Questionnaire not completed regarding
supplemental anesthesia (Q07D1NOANES) n=3
*Patients not obturated at 1st appointment(Q07D1RCT) n=134

25
Preoperative Factors Studied
Provider related characteristics were provider experience (GRADYR) and
provider type (SPETY). More experienced was defined as 10 years or more in practice
and less experienced defined as less than 10 years in practice. Provider type was either
general dentist or endodontist.
Appendix II contains the questionnaire related to the following patient related
characteristics. Patient characteristics studied were age (Q04P0AGE), gender
(Q0P0GENDER), ethnicity (Q04P0HISP), race (Q04P0RACE), level of education
(Q04P0EDU), annual household income (Q04P0INCOME), dental insurance coverage
(Q04P0DENINS), self-reported history of diabetes (Q04P0DIAB), current smoker
(Q04P0SMKNOW), lifetime smoking of at least 100 cigarettes (Q04P0LFSMK100),
preoperative fear level either high or low (Q04P0FEAR), patient expected outcome for
the tooth either favorable or unfavorable (Q04P0OUTC), and did the patient suffer from
chronic body pain, as in body pain present for at least 4 days a week for the past 3 months
(Q04P0BODYPA). Preoperative fear level responses were converted to binary with
“very much” and “quite a lot” being high fear and “a little” and “not at all” were
considered low fear. Expected outcome for the tooth was converted to binary with
“poor” being unfavorable and “very good”, “good”, and “fair” being favorable.
Appendix II also contains questions related to patient quality of life related to
tooth pain. Patient reported quality of life characteristics studied were how many days in
the week prior to treatment did tooth pain keep the patient from their usual activities
(Q04P0NOACDAY), in the week prior to treatment, how much did tooth pain interfere
daily activities (Q04P0NODAC), in the week prior to treatment, how much did tooth pain

26
interfere with recreation, social or family activities (Q04P0NOREC) and in the week
prior to treatment, how much did tooth pain interfere with work, including housework
(Q04P0NOWRK).
Subjective patient reported characteristics related to tooth pain were studied based
on answers from the questions in Appendix II. These characteristics were the number of
days in the week prior to treatment with tooth pain (Q04P0PADAY), was the tooth pain
chronic, as in present at least 8 hours a day for 15 days or more a month for the past 3
months (Q04P0TOOTHPA), was pain medication taken (Q04P0PAMED), pain quality in
the 7 days prior to treatment reported as none (Q04P0NONE), dull (Q04P0DULL), sharp
(Q0P0SHRP), aching (Q04P0ACH), throbbing (Q0P0THROB), burning (Q04P0BURN),
shooting (Q04P0SHOOT), or electric (Q04P0ELECT); spontaneous pain in the 7 days
prior to treatment (Q04P0SPON), pain provoked by using the tooth or an irritant in the 7
days prior to treatment (Q04P0PROV), factors that make the pain worse including
nothing, never gets worse (Q04P0NOWRS), nothing, gets worse all by itself
(Q04P0WORSE), biting or chewing (Q04P0BITE), cold or hot food or drink
(Q04P0TEMP), or stress (Q04P0STRES), and pain levels including pain level
immediately prior to treatment (Q04P0NWPAIN), worst level pain in the week prior to
treatment (Q04P0WSTPAIN), and average pain level in the week prior to treatment
(Q04P0AVGPAIN). Pain levels were reported on a scale of 1 to 10 with 0 being “no
pain” and 10 being “pain as bad as could be”. The pain level data was converted to
binary with pain levels 7-10 being severe pain and 0-6 being not severe.
Objective provider reported tooth characteristics were studied based answers to
questions in Appendices III and IV. These characteristics were tooth type

27
(Q05D0TONUM), presence of a periapical radiolucent lesion (Q05D0ENDO),
percussion sensitivity (Q05D0PERC), biting sensitivity (Q05D0BITE), responsive to
cold (Q05D0COLD), lingering pain with cold (Q05D0COLDPROL), periodontal health
determined by deepest pocket depth (Q05D0DEEP), pulp vitality confirmed by bleeding
upon access (Q07D1BLEED), presence of a sinus tract (Q07D1FISTULA), and presence
of swelling (Q07D1SWELL). Tooth type was reported by tooth number from 1-32; the
data was converted to binary in two ways, maxillary or mandibular and molar or non-
molar based on universal tooth number. Deepest periodontal pocket depth was reported
in millimeters and 1-3mm was considered healthy and 4-12mm was considered diseased
which is consistent with the most recent staging criteria for periodontal disease (87).
Statistical Procedures
Descriptive statistics were generated for all included survey variables. Differences
between failure groups, for each failure measure, were estimated by chi-square tests of
independence for categorical variables and t-tests for numeric variables. Stepwise linear
regression model selection was used to identify variables associated with failure
outcomes. The stepwise algorithm used the AIC statistic as fitness criteria and was
allowed to both add and remove variables, starting with the null model.
All analyses were conducted with R (version 4.0.2) and a significance level of 0.05 was
used for all hypothesis tests.

28
RESULTS
Initially an analysis of the provider, patient and tooth characteristics being
investigated for the entire group of 708 study participants was done. The results are
shown in Appendix VI. The statistically significant differences between the 1 visit and
2+ visit groups were provider type, age, patient education level, dull pain in the 7 days
prior to treatment, pain provoked by using the tooth or other stimulus in the 7 days prior
to treatment, severe pain at the time of treatment, average severe pain in the week prior to
treatment, presence of a periapical radiolucency, percussion sensitivity, biting sensitivity
and swelling. Calculation of overall anesthesia failure by each method described and by
number of appointments is shown in Table 1, there is a trend toward more failures in the
multiple appointment treatment group but the differences between single visit and
multiple visit groups is not statistically significant. In Table 1, the 7 missing, 3 missing
and 6 missing from each group represent the questionnaire not being completed for these
variables.
Table 1. Overall Anesthesia Failure Rates by Method

29
The overall anesthesia failure rates were 4.90% for Method 1, 14.61% for Method
2 and 29.96% for Method 3. After overall failure rates were calculated, the dataset was
trimmed to include only single treatments completed in a single visit. As discussed in the
literature review, reported anesthesia failure rates are quite variable, but the overall rates
noted with all three of the methods used fall withing the previously reported range with a
tendency toward the lower end of the previously reported rates. The failure rates
associated with the individual preoperative factors studied were compared to the overall
fail rates to determine statistical significance. The results for Method 1 are shown in
Appendix VIII. The results for Method 2 are shown in Appendix IX. The results for
Method 3 are shown in Appendix X. Not all questionnaires were filled out completely,
for each variable, the number missing corresponds to the incomplete questionnaires.
Method 1: Patient Reported Numbness
When evaluating anesthesia failure by patient reported numbness, provider
experience, history or diabetes, current tobacco smoking, tendency to catastrophize,
presence of sharp tooth pain in the 7 days prior to treatment and presence of spontaneous
tooth pain in the 7 days prior to treatment had statistical significance when analyzed
individually, see Appendix VIII. No other investigated variables showed statistical
significance. Table 2 summarizes the preoperative factors with statistical significance
when compared individually to the overall failure rate.
Using the regression model that accounts for interaction between the variables
less experienced providers, patients with no dental insurance coverage, history of
diabetes, high levels of preoperative fear, number of days in pain, severe pain at the time
of the appointment, and swelling were positively correlated with anesthesia failure.

30
Patients experiencing sharp pain in the 7 days prior to treatment, spontaneous pain in the
7 days prior to treatment and patients with average pain being severe in the 7 days prior
to treatment were negatively correlated with anesthesia failure. Table 3 summarizes the
factors in the regression model and gives odds ratios with confidence intervals for
statistical significance; the asterisk signifies statistical significance.
Of the factors in the regression model only provider experience, history of
diabetes, high fear, sharp tooth pain present in the 7 days prior to treatment, spontaneous
tooth pain in the 7 days prior to treatment, severe tooth pain at the time of the treatment
and number of days in pain were statistically significant. Patients treated by a less
experienced provider had a 3.620 times chance of anesthesia failure. Patients with a self-
reported history of diabetes had a 10.980 times chance of anesthesia failure. Patients
with high preoperative fear had a 3.800 chance of anesthesia failure. Patients with sharp
tooth pain in the 7 days prior to treatment had a 0.081 times chance of anesthesia failure.
Patients with spontaneous tooth pain had 0.159 times chance of anesthesia failure.
Patients with severe tooth pain at the time of treatment had a 16.249 times chance of
anesthesia failure. The previous variables were all binary, regarding the number of days
in pain, the odds ratio is interpreted differently because it deals with the number of days
in the week prior to treatment that the patient experienced pain, the odds ratio of 1.332
means that patients with pain for 2 days had a 1.332 time chance or anesthesia failure
compared to those with 1; patients with pain for 3 days prior to treatment had a 1.332
times high chance of anesthesia failure than those with pain for 3 days and so on up to 7
days. Therefore, the patient in pain for 7 days had a 9.324 times higher chance of
anesthesia failure than the patient in pain for 1 day.

31
Table 2. Method 1: Significant Factors Associated with Anesthesia Failure
Overall
n=531
Anesthesia Failure
n=26
Anesthesia Success
n=505
Percentage Failure Rate
4.90%
P value
Provider characteristics More experienced 431 17 414 3.90% 0.0145 Less Experienced 77 8 69 10.4% Patient characteristics Diabetes history 58 9 49 15.51% 0.0001 No diabetes history 460 17 443 3.70% Current smoker 82 0 82 0.00% 0.0248 Current non-smoker 445 26 419 5.84% Expected outcome favorable 520 23 497 4.42% 0.0005 Expected outcome fair 11 3 8 27.27% Tooth characteristics Sharp pain 148 2 146 1.35% 0.0172 No sharp pain 377 24 353 6.37% Spontaneous pain 231 7 234 3.03% 0.0425 No spontaneous pain 280 19 261 6.79%
Table 3. Method 1: Factors Associated with Anesthesia Failure in the Statistical Regression Model

32
Method 2: Provider Reported Quality of Anesthesia
When evaluating anesthesia failure by provider reported quality of anesthesia,
provider type, history or diabetes, level of tooth pain interfering with ability to take part
in recreational activities, presence of tooth pain that was provoked by stimulus during the
7 days prior to treatment, presence of tooth pain made worse by stress in the 7 days prior
to treatment, percussion sensitivity at the time of treatment and presence or absence of a
sinus tract at the time of treatment had statistical significance when analyzed
individually. No other investigated variables showed statistical significance, see
Appendix IX. Table 4 summarizes the preoperative factors with statistical significance
when compared individually to the overall failure rate.
Using the regression model that accounts for interaction between the variables
less experienced providers, general dentists, patient income from $30,000-49,999, history
of diabetes, preoperative opioid pain medication taken, pain interfering with recreational
activities, presence of burning tooth pain in the 7 days prior to treatment, presence of pain
made worse by stress, presence of a periapical radiolucent lesion, and teeth with
percussion sensitivity were positively correlated with anesthesia failure. Income levels of
less than $10,000 and $10,000-29,000, number of days pain interfered with usual daily
activities, pain interfering with work, and periodontally healthy teeth were all negatively
correlated with anesthesia failure. Table 5 summarizes the factors in the regression
model and gives odds ratios with confidence intervals for statistical significance; the
asterisk signifies statistical significance.
Of the factors in the regression model only provider experience, provider type,
income level $10,000-29,000, history of diabetes, and rating of pain interference with

33
recreational activities had statistical significance. Patients treated by a less experienced
provider had a 2.061 times chance of anesthesia failure. Patients treated by a general
dentist had a 2.027 times chance of anesthesia failure. Patient with an income level of
$10,000-29,000 had a 0.241 chance of anesthesia failure. Patients with a self-reported
history of diabetes had a 2.570 times chance of anesthesia failure. Patients with higher
ratings of how much pain interfered with recreation activities in the week prior to
treatment had a 1.670 times chance of anesthesia failure.
Table 4. Method 2: Significant Factors Associated with Anesthesia Failure
Overall
n=534
Anesthesia Failure
n=78
Anesthesia Success
n=456
Percentage Failure Rate
14.61%
P value
Provider characteristics General dentist 194 38 156 19.59% 0.0138 Endodontist 340 40 300 11.76% Patient characteristics Diabetes history 58 14 44 24.13% 0.0351 No diabetes history 460 63 397 13.37% Tooth characteristics Pain not provoked by stimulus 255 29 226 11.37% 0.0319 Pain provoked by stimulus 266 48 218 18.05% Stress makes pain worse 34 9 25 26.47% 0.0449 Stress doesn’t worsen pain 490 68 422 13.87% Not percussion sensitive 207 21 186 10.14% 0.0202 Percussion sensitive 327 57 270 17.43% Not biting sensitive 237 24 213 10.13% 0.0084 Biting sensitive 296 54 242 18.24% Sinus tract present 46 2 44 4.35% 0.0416 Sinus tract absent 474 73 401 15.40% Quality of life characteristics (reported on a scale of 1-10)
How much has tooth pain interfered with recreational or social activities from 1-10?
2.14 (+/-2.87)
1.34 (+/-2.37)
0.0195

34
Table 5. Method 2: Factors Associated with Anesthesia Failure in the Statistical Regression Model
Method 3: Use of Supplemental Anesthesia
When evaluating anesthesia failure by defined by the use of supplemental
anesthesia provider type, patient age, tooth pain interference with daily activities, tooth
pain provoked by stimulus in the 7 days prior to treatment, sharp tooth pain in the 7 days
prior to treatment, tooth type maxillary vs mandibular, presence of a periapical
radiolucency, responsive to cold, lingering response to cold, and pulp vitality confirmed
by bleeding upon access all had statistical significance when analyzed individually. No
other investigated variables showed statistical significance, see Appendix X. Table 6
summarizes these preoperative factors when compared individually to the overall failure
rate.
Using the regression model that accounts for interaction between the variables
general dentists, male patients, patients taking opioids for tooth pain management,
patients with higher rating of tooth pain effecting daily activities in the 7 days prior to

35
treatment, patients taking any medication for tooth pain management, burning tooth pain
in the 7 days prior to treatment, shooting tooth pain in the 7 days prior to treatment, tooth
pain provoked by stimulus, tooth pain that is made worse by nothing (always present) in
the 7 days prior to treatment, teeth with percussion sensitivity, teeth responsive to cold
and periodontally healthy teeth were positively correlated with anesthesia failure. Non-
molar teeth were negatively correlated with anesthesia failure. Table 7 summarizes the
factors in the regression model and gives odds ratios with confidence intervals for
statistical significance; the asterisk signifies statistical significance.
The factors in the regression model with statistical significance were patients
treated by a general dentist, male patients, patients with higher ratings of pain affecting
daily activities, patients not taking any pain medication for tooth pain, pain provoked by
stimulus or using the tooth, teeth responsive to cold and periodontally healthy teeth.
Patients treated by a general dentist had a 2.170 times chance of anesthesia failure. Male
patients had a 1.919 times chance of anesthesia failure. Patients with higher rating of
tooth pain interfering with daily activities had a 1.200 times chance of anesthesia failure
for each higher level of rating of the interference; therefore a patient reporting an
interference rating of 10 would have a 12 times higher chance of anesthesia failure than a
patient reporting a rating of 1 for pain interference with daily activities. Patients taking a
pre-operative medication for pain had a 0.587 times chance of anesthesia failure. Patients
with tooth pain provoked by using the tooth or any other stimulus in the 7 days prior to
treatment had a 1.656 times chance of anesthesia failure. Patients with teeth responsive
to cold testing had a 2.383 times chance of anesthesia failure and periodontally healthy
teeth had a 2.168 times chance of anesthesia failure.

36
Table 6. Method 3: Significant Factors Associated with Anesthesia Failure
Overall
n=534
Anesthesia Failure n=160
Anesthesia Success
n=374
Percentage Failure Rate
29.96%
P value
Provider characteristics General dentist 194 75 119 38.66% 0.0009 Endodontist 340 85 255 25.00% Patient characteristics Age 45.03
(+/-12.60) 48
(+/-13.11) 0.0123
Tooth characteristics Sharp pain 148 57 91 38.51% 0.0102 No sharp pain 377 102 275 27.05% Pain provoked by stimulus 266 90 176 33.83% 0.0476 Pain not provoked by stimulus 255 66 189 25.88% Maxillary 321 83 238 25.85% 0.0110 Mandibular 213 77 136 36.15% PARL present 218 54 164 24.77% 0.0281 PARL absent 312 105 207 33.65% Not responsive to cold 282 65 217 23.05% 0.0002 Responsive to cold 249 94 155 37.75% Lingering cold response 191 75 116 39.27% 0.0004 No lingering cold response 339 83 256 24.48% Vital pulp 278 103 175 37.05% 0.0002 Non-vital pulp 256 57 199 22.27% Quality of life characteristics (reported on a scale of 1-10)
How much has tooth pain interfered with daily activities from 1-10?
2.18 (+/-2.83)
1.57 (+/-2.43)
0.0194

37
Table 7. Method 3: Factors Associated with Anesthesia Failure in the Statistical Regression Model

38
DISCUSSION
Exclusion of Teeth Requiring Multiple Appointments to Complete RCT
In cases where treatment was carried out over multiple visits, the treatment
rendered at the first visit was difficult to standardize and therefore the study was limited
to root canal therapy completed in a single appointment. A potential source of bias arises
in that failure of local anesthesia may have been a factor for not completing the treatment
at the first appointment. This is very unlikely because it was addressed in the
questionnaires completed by the provider. Appendix 4 is the questionnaire completed by
the dentist immediately after treatment, as part of question 3, the dentist reports if there
was an “Inability to complete treatment due to discomfort during treatment”
Q07D1INCOMP. There was only 1 of the 708 cases with this reported, regardless, a
sensitivity analysis of the single visit treatment group vs the multiple visit group was
completed to ensure the exclusion of the multiple visit treatment group was appropriate.
Single vs. multiple visit endodontic therapy is a controversial topic however each
technique has specific advantages for different clinical scenarios; multiple visit treatment
considered a reasonable protocol, however multiple systematic reviews point toward
single appointment treatment having fewer complications, superior outcomes (88).
In the total group of 708 patients, general dentists completed root canal treatment
in one visit in 67.12% (194/289) of cases, while endodontists completed root canal
treatment in 89.00% (340/382) of cases and the difference was statistically significant
with p<0.0001. Patient education level showed significance; however, the clinical
relevance may be questionable because the n numbers become somewhat small when
divided amount the 5 groups. Of the pain at time of treatment variables, patients with

39
dull pain and provoked pain were more often treat in a single appointment with statistical
significance. The 2+ visit group had a higher percentage of patients with percussion pain,
biting pain, severe pain with statistical significance, showing a trend that providers
appear to treat patients in more pain in multiple visits. Patients with swelling at the initial
visit accounted for a higher percentage of the 2+ visit group with statistical significance.
One possible explanation would be that patients with swelling and severe pain are
worked into emergency appointments typically in general dentistry practices that do not
allow time to complete the entire root canal therapy. Dull pain which is typically less
severe and pain that had to be provoked, meaning it was not constant are often easier for
patients to manage possibly explaining their trend to be treated in a single appointment in
a regularly scheduled appointment. The presence of a periapical radiolucent lesions
accounted for a higher percentage of the 2 visit groups with statistical significance. Teeth
with large periapical lesions are likely necrotic with bacteria in the canal and the use of
calcium hydroxide as a intracanal medicament has been shown to reduce these bacterial
levels, explaining the trend toward 2+visits (89). Regardless of the reasoning behind the
2+ visits, treatment completed could not be standardized so the study was limited to
single visit root canal therapy. Table 1 shows there was no significant difference
between the single appointment and multiple appointment treatment groups with regards
to anesthesia failure.
Methods of Defining Anesthesia Failure
Patient reported numbness was chosen as the patient centered method for defining
anesthesia failure. In appendix 5, Question 1 (Q09P1PAIN) asks patients to rate the
intensity of pain during the root canal procedure on a scale of 1 to 10. Another patient

40
centered method for determining failure would be to use this information to define
failure, however when surveying the data, there were various inconsistencies such as one
patient reporting 10 out of 10 pain during the procedure while also reporting being numb
enough. The most plausible explanation being a short momentary intense pain that did
not leave the patient feeling the anesthesia was inadequate. Only 10 out of the 539
patients in the single appointment group reported pain intensity of 7 out of 10 or greater
which would likely would have underestimated the failure rate, being only 1.86%
reporting a failure making it difficult to draw any useful conclusions.
With the dentist reported methods of anesthesia failure, both have potential
problems. The reported quality of anesthesia could be skewed in that there could have
been an initial failure after which the dentist may have used multiple types of
supplementary anesthesia and eventually made the patient quite comfortable, causing the
dentist to report the quality of anesthesia was excellent. With the use of supplemental
anesthesia as a failure, the rate is likely inflated in that the question does not specify
when the supplemental anesthesia was given. The only supplemental anesthesia that can
definitively be said to occur after initiation of treatment is the intrapulpal injection which
accounted for 81 of the 163 cases with supplemental anesthesia use. Intrapulpal
injections require a tight fitting area for the needle to enter the pulp chamber and provide
only pressure anesthesia of relatively short duration and is only employed after initial
anesthesia failure (90). It is unlikely intrapulpal injections were given prophylactically.
For the other types of supplemental anesthesia, it is certainly possible that the
providers administered local anesthetic, waited, then tested the tooth and then gave
supplemental anesthesia prior to initiation of the root canal if needed. If this was the

41
case, the patient would likely not have reported an anesthesia failure because treatment
had not been initiated, and the dentist would likely also have reported anesthesia quality
as a success, possibly accounting for the discrepancies among the methods. Many
providers consider anesthesia a strategy and not a single technique for all situations and
may treat for symptomatic “hot” teeth differently by giving supplemental anesthesia
before a failure occurs (16, 60).
Failure by Provider Characteristics
Operator experience was found to be significant when analyzed individually in
Method 1 and in regression models for Method 1 and Method 2 making it likely that it is
not just statistically significant but also truly clinically significant for anesthesia success
and failure. In 1998, Jim Dower (91) published the results of a survey, pertaining to local
anesthesia training in dental schools, 96% of institutions completed the survey. He found
that in 85% of schools, the oral and maxillofacial surgery departments were solely
responsible for the local anesthesia training and the department of endodontics was not
responsible for training in any institution. The institutions averaged 20 hours of training
with a broad range of faculty to student ratio ranging from 1:1 to 1:30 but typically
having a 1:4 ratio during the clinical instruction when injections were being administered.
The survey also found a general lack of protocol for dealing with failed anesthesia (91).
Arguably oral and maxillofacial surgeons have the most training on anatomy and
precision of placement of anesthesia blocks, however achieving pulpal anesthesia is much
more difficult than achieving soft tissue anesthesia. A prime example being the Gow-
Gate vs Vazirani-Akinosi study by Click et al (44). When studying the PDL injection,
Malamed both found anesthesia always successful for extractions but only 60%

42
successful for endodontics (92) is another example. A more contemporary study of local
anesthesia training in dental schools was a systematic review of the literature by Kary
(93) which found 3 methods of training: didactic with textbooks and lectures dental
students performing injection on each other, and using anatomic models. Unfortunately,
none of the studies in the review addressed efficacy, student confidence or patient
satisfaction and no definitive curriculum recommendations could be made based on the
review. Perhaps Dr. Dower’s study (91) should be reproduced and if the current trends
are similar, the departments of endodontics could take a more active role in anesthesia
training in partnership with the departments of oral and maxillofacial surgery. Not only
would patient’s benefit but the dentists would as well, Simon et al. surveyed 3000
practicing dentists and found 18.8% of the dentists surveyed reconsidered dentistry as a
career choice due to the constant stress associated with administering local anesthesia
(94).
The prudent practitioner should routinely test for profound pulpal anesthesia prior
to initiating operative or endodontic procedures. As far back as 1884, in a rebuttal of an
article reporting the failure of cocaine hydrochlorate to produce local anesthesia, William
Halsted critiqued his colleague’s technique, giving multiple reasons for the reported
anesthesia failure; his final point, apparently scolding his colleague was “there suggests
itself the propriety of testing the sensibility before cutting” (95). Techniques for
determining pulpal anesthesia prior to initiating the procedure have been described. Most
endodontists routinely use a cold test prior to initiating treatment knowing that soft tissue
lip numbness is not reliable for determining pulpal anesthesia. However, a negative cold
test can predict profound pulpal anesthesia 88-92% of the time (96, 97). No response to

43
the electric pulp tester at 80/80 has been shown to be reliable for determining anesthesia
in normal and asymptomatic teeth 100% of the time after 3.6ml of 2% lidocaine with
1:100,000 epi, but only 73% of the time in teeth with symptomatic irreversible pulpitis
(22). Even integrating just this technique into anesthesia training in dental schools would
be quite beneficial.
General dentists had significantly higher failure rates when analyzed individually
in Method 2 and Method 3. Also, in the regression models for Method 2 and Method 3,
general dentists were significant for positive correlation with anesthesia failure, meaning
they were statistically more likely to have anesthesia failures with an odds ratios in both
models pointing to an approximately double the chance for an anesthesia failure
compared to the endodontists in this study. Endodontists have the advantage of
additional training in local anesthesia and are experienced in routinely dealing with
pulpal anesthesia. One could argue that this also points to the notion that endodontic
departments should be actively involved in local anesthesia training in the dental school
setting.
Failure by Patient Characteristics
Patient reported history of diabetes showed statistical significance when analyzed
individually in Method 1 and Method 2. It was also found to be positively correlated
with anesthesia failure in the regression models for Method 1and Method 2. In the
regression model for Method 1, it was found that patients with a self-reported history of
diabetes had a 10.980 times higher chance of anesthesia failure, with Method 2 patients
had a 2.570 times higher chance of failure. There is a dearth of literature in dentistry
relating diabetes to local anesthesia success and failure. From the medical literature

44
Ozturk et al. found diabetes mellitus was not significantly correlated to spinal anesthesia
failure (98). Baeriswyl et al. found diabetes had a faster onset of peripheral nerve
blockade with prolonged duration of anesthesia using a combination of 1% lidocaine and
0.5% bupivacaine during foot surgery (99). Cuvillon et al. found longer duration of
anesthesia with sciatic nerve blocks with ropivacaine in diabetic patient (100). Gebhard
et al. report a higher local anesthesia success for supraclavicular branchial plexus blocks
with 2% mepivacaine in diabetic patients and speculate that nerve fibers in diabetics may
be more sensitive to local anesthesia potentially caused by microvascular damage seen
with diabetes or that diabetic neuropathy leads to decrease sensation making it appear
that the anesthetic is more successful (101). The findings of these studies appear to
contrast with the findings of this study; however, these were studies dealt with confirmed
diabetics rather than self-reported. The pulp has a unique microvascular structure and
relation of neurons to the smooth muscle of the microvasculature (102-104). It is
possible that microvascular changes in the pulp and other diabetic changes that could
affect neurons may be different compared to the large fiber neuropathy demonstrated in
the peripheral nerves in these medical studies. However, providers are not routinely
injecting into the pulp for primary anesthesia, rather tending toward block anesthesia and
local infiltration. Based on the findings of this study, dental providers should expect
higher rates of anesthesia failure in endodontic procedures in diabetic patients. More
research specifically designed to investigate diabetes and dental local anesthesia is
needed.
Current smokers had no reported anesthesia failures using Method 1 which was
statistically significant. There were only 82 patients in the current smoker group which

45
may have kept it from the regression model. Future studies could examine the
relationship with smoking and dental anesthesia. The analgesic effects of nicotine are
documented. Ditre, et al. discuss that nicotine has a strong analgesic effect in animals
that is present in humans but to a lesser extent, however difficulty in quitting smoking
may be related to the pain inhibiting effects (105). It is possible that the vasoconstriction
associated with smoking could cause the local anesthetic to remain at the intended site
and as it would more slowly enter the systemic circulatory system, prolonging and
enhancing its effect. Age was found to be a significant when analyzed individually in
Method 3 but in no other models, the difference in age for success was 45.03 (+/-12.60)
and 48.09 (+/-13.11), with this difference being so small, this variable is likely not
clinically significant. Gender was found to be significant in regression model for Method
3 with male patients having a 1.919 times chance of anesthesia failure defined by the use
of supplemental anesthesia, this was the only model finding significance with gender.
The use of supplemental anesthesia to define failure has potential issues as previously
discussed, with this being the only method finding significance for age and gender, the
clinical relevance is questionable. Studies specifically relating to gender or age and local
anesthesia failure or success are lacking providing an opportunity for future investigation.
Patient fear levels did not show statistical significance in any model when
evaluated individually. In the regression models, high preoperative fear was positively
correlated with anesthesia failure in Method 1 with these highly fearful patients having a
3.8 times chance of having anesthesia failure. Studies looking specifically at dental
anesthesia failure or success related to anxiety levels are lacking however, many the
anesthesia success studies at The Ohio State University incorporate a Corah Anxiety

46
Scale (39), these studies have not found statistical significance with anxiety but it is not
the primary outcome in any of the studies and typically found relatively high anxiety
levels that were attributed to the symptomatic irreversible pulpitis and emergency
treatment needed (35, 44, 61, 106, 107). The result from this study, incorporated
emergent and routinely scheduled endodontic treatment suggests preoperative patient
anxiety levels influence anesthesia success and failure and a well-designed study
specifically investigating this factor is needed. Somewhat related, studies examining the
effect of pre-operative anxiolytics do exist and have found no significant difference in
anesthesia success with the use of preoperative anxiolytics (108, 109). Different from
fear, patients with a fair expected outcome for the treatment compared to excellent or
good had a statistically higher chance of anesthesia failure, 27.27% vs 4.42%, when
analyzed individually in Method 1, compared to the overall failure rate of 4.90%.
It is interesting that in Method 1, which is the model centered on the patients’
perspective of anesthesia failure, both these psychological related variables had statistical
significance. Catastrophizing patients were relatively rare, only 11/531. Highly fearful
patients were more common, representing 89/531 patients. Even though these variables
did not present significance in the other models and are relatively rare, clinicians should
take care to question patients regarding pre-operative fear and expected outcome and
understand that fearful patients and those that tend to catastrophize are more likely to be
dissatisfied with the level of numbness during root canal therapy even though the
provider reported level of anesthesia may be adequate. To explore what techniques may
make these patients comfortable during treatment, more research is needed. Weinstein, et
al. noted evidence that patients with high levels of fear associated with dental treatment

47
and those with a history of failed local anesthesia tended to have subsequent failures (5),
this evidence could influenced by catastrophizing patients. Lin discusses that
catastrophizing patients ruminate over the idea of pain and tend to magnify the effects of
pain and show inadequate coping to pain (78).
In the regression model for Method 2 patients with lower annual income at
$10,000-29,000 had fewer anesthesia failures, these patients had a 0.241 times chance of
anesthesia failure compared to those with income levels of less than $10,000 and those
with $30,000 and above. This suggest that patients with lower socioeconomic status may
tolerate pain more than patients with higher socioeconomic status. This finding was
isolated and not consistent amongst the models making this conclusion dubious. Further
research is needed in this area to draw firm conclusions.
Failure by Tooth Related Characteristics
Questions related to the subjective quality of tooth pain are pertaining only to the
period of 7 days prior to treatment, objective findings were recorded by the dentist on the
day of treatment. Base on the AAE Glossary of Endodontic Terms (110): sharp pain,
spontaneous pain, severe pain, exaggerated pain in response to a stimulus, responsiveness
to cold, lingering response to cold are related to symptomatic irreversible pulpitis;
percussion sensitivity and presence of a periapical radiolucent lesion are related to apical
periodontitis; biting sensitivity may be related to pulpitis, apical periodontitis or both;
swelling and sinus tract are related to necrotic pulp with possible exception of a
periodontal abscess or hemorrhage/inflammation from trauma. The idea that
symptomatic teeth are more difficult to anesthetize is well established (3, 16, 22, 60, 97).

48
Patients reporting sharp tooth pain had statistical significance when analyzed
individually in Method 1 with a failure rate of 1.35% vs. 6.37% when sharp pain was
absent; the overall failure rate was 4.90% (26/531). In Method 3 sharp pain was
statistically significant with a failure rate of 38.51% (57/138) when present vs. 27.05%
(102/377) when absent; the overall failure rate was 29.96% (160/534). With the
regression models, sharp tooth pain was negatively correlated with anesthesia failure in
Method 1 and patients with sharp pain had a 0.081 times chance of an anesthesia failure,
making it the most negatively correlated variable with anesthesia in any of the models,
the 1.35% failure rate is also the lowest of any of the significant variables analyzed
individually. These results are conflicting making it difficult to interpret and making this
clinical relevance questionable. The Method 3 results are more in line with the well-
established view that teeth with irreversible pulpitis are more difficult to anesthetize.
Patient reports of spontaneous pain were found to be statistically significant when
analyzed individually in Method 1 with the presence of spontaneous pain being
significant for fewer anesthesia failures with a rate of 3.03% (7/231) vs. 6.79% (19/280)
when present compared to the overall failure rate of 4.90% (26/531). In the regression
model for Method 1, presence of spontaneous pain was significant for a 0.159 times
chance of anesthesia failure, meaning there was much less chance of anesthesia failure in
this model. With spontaneous pain related to irreversible pulpitis, these finding are at
odds with the well-established view that teeth with symptomatic irreversible are more
difficult to anesthetize suggesting a possible unknown confounder affecting the finding.
With both a history of sharp and spontaneous pain in the week prior being associated
with fewer failures in the patient centered Method 1 model, one can speculated that

49
patients were pleased with the treatment and that anesthesia was adequate in relation to
relieve the preoperative pain.
Pain provoked by using the tooth or with any other irritation was significant when
analyzed individually in Method 2 and Method 3, also in the regression model for
Method 1 and Method 3. In Method 2 the overall failure rate was 14.61% (78/534), when
pain was provoked the failure rate was 18.05% (48/266) vs 11.37% (29/255) when not
provoked, making provoked pain inversely related to anesthesia failure. Likewise, in
Method 3 provoked pain was significant for anesthesia failure; the overall failure rate in
Method 3 was 29.96% (160/374), with pain provoked by stimulus it was 33.83% (90/266)
vs. 25.88% (66/255) when not. In the regression model for Method 3, patients with tooth
pain provoked by stimulus had a 1.656 times chance of anesthesia failure. With pain
provoked by stimulus being associated with pulpitis, the overall trend is in agreement
with the well-established view that symptomatic teeth are more difficult to anesthetize.
In Method 3, results for variables related to the diagnosis of irreversible pulpitis
were in agreement that pulp vitality is associated with anesthesia failure, with significant
findings as follows: responsiveness to cold was related to anesthesia failure with a failure
rate of 37.75% (94/249) vs 23.05% (65/282) when not responsive to cold; lingering
response to cold had a failure rate of 39.27% (75/191) and 24.48% (83/339) when absent;
pulp vitality confirmed with presence of bleeding upon access had a failure rate of
37.05% (103/278) and 22.27% (57/256) when bleeding upon access was absent. The
overall failure rate for Method 3 was 29.96% (160/534). In the regression model for
Method 2, teeth responsive to cold had a 2.383 times chance of anesthesia failure which
was significant. Presence of severe pain was shown to be positively correlated with

50
anesthesia failure in the regression model in Method 1, patients with severe pain at the
time of treatment were 16.249 times more likely to experience anesthesia failure by self-
reported level of numbness. This is the highest odds ratio of any variable in any of the
models although the confidence interval is very wide; clinicians should expect patients in
severe pain will be more difficult to anesthetize and consider testing for adequate
anesthesia and using supplemental techniques prior to initiating endodontic procedures.
The findings are consistent with symptomatic teeth being more difficult to anesthetize (3,
16, 22, 60, 97).
Regarding other subjective pain related variables, pain made worse with stress
had statistical significance in Method 2 with tooth pain made worse having a failure rate
of 26.47% (9/36) vs. 13.87% (68/490) in patients without this pain. The sample size is
relatively small. Studies regarding pain made worse by stress and anesthesia failure or
success are nonexistent and can be considered as a component of future studies.
Several variables related to apical periodontitis had statistical significance.
Percussion and biting sensitivity had statistical significance when evaluated individually
in Method 2. Presence of a periapical radiolucent lesion when evaluated individually was
significant in Method 3. No factors related to apical periodontitis were found to be
significant in the regression models. Teeth with percussion sensitivity and biting
sensitivity had more anesthesia failures based on provider reported quality of anesthesia.
Percussion sensitive teeth had a failure rate of 17.43% (57/327) vs. 10.14% (21/207) in
teeth without. Teeth with biting sensitivity had a failure rate of 18.24% (54/296) vs.
10.13% (24/237) of teeth without. The overall failure rate for Method 2 was 14.61%
(78/534). In Method 3, teeth with a periapical lesion had a failure rate of 24.77%

51
(54/218) vs 33.65% (105/312) with no PARL. Teeth with apical periodontitis may be
associated with teeth with pulpitis, necrotic pulps, or occlusal trauma (111). For a
periapical lesion to be visible on a radiograph the erosion of the cortical plate must have
occurred (112, 113) often indicating that they are likely long standing and associated with
pulpal necrosis. With radiographic techniques and interpretation not being standardized
in this study, the presence of apical lesions is likely underestimated. The presence of a
sinus tract will always be associated with a necrotic pulp in teeth that are not previously
treated. In Method 2, the presence of a sinus tract was inversely associated with
anesthesia failure with statistical significance. Teeth with a sinus tract had an anesthesia
failure rate of only 4.35% (2/46) vs. 15.40% (73/474) of those without with the overall
failure rate for Method 2 being 14.16% (78/534). Of note, while not showing statistical
significance, the failure rate of anesthesia in Method 1 when a sinus tract was present was
0% (0/46). These findings agree with each other pointing to necrotic teeth having fewer
anesthesia failures. A potential exception exists with percussion and bite sensitivity
which were found to be higher in the early stages of apical periodontitis in vital teeth by
Owatz, et al (114), possibly explaining the higher failure rates found in Method 2 with
biting and percussion sensitivity.
Another exception to necrotic teeth being less symptomatic would be teeth with
acute apical abscesses and tissue swelling. Teeth with associated swelling did not show a
significant a correlation with anesthesia failure in any model. There is a lack of studies
directly dealing with local anesthesia failure in the presence of an acute apical abscess.
The difficulty of patient recruitment for a prospective study is obvious with this typically
being urgent or emergent treatment. The often cited change in pH in the presence of

52
infection has disproven (66) and the findings of this study are in agreement. Other
changes in tissue related to infection and inflammation may play a role such as the
upregulation of TTX resistant receptors (73, 74), nerve sprouting (68, 69) and changes in
neuropeptide levels (70).
The only remaining tooth related characteristic significantly associated with
anesthesia failure were mandibular teeth when analyzed individually in Method 3 and
periodontally healthy teeth, which were found to have a 2.168 times chance of anesthesia
failure in the regression model for Method 3. Mandibular teeth had a 36.15% (77/213)
failure rate vs maxillary 25.85% (83/321) in Method 3 compared to the overall failure
rate of 29.96% (160/534). Mandibular molars are often associated with anesthesia
difficulties (16), the finding of this study are in agreement. The literature regarding the
study of periodontal status and anesthesia success or failure is lacking. One potential
explanation for this finding is that chronic apical abscesses can drain through the
periodontal pocket, manifesting as periodontal disease instead of a sinus tract. If this was
not recognized as a sinus tract, but rather periodontal disease it could explain this result in
that periodontally healthy teeth would be more likely to have a vital pulp when a tooth
with a sinus tract via the periodontal pocket would be necrotic and thereby less likely to
have an anesthesia failure. Only pocket depths were recorded and the most current
periodontal staging and grading is not based solely on pocket depth, rather interdental
clinical attachment loss (87). Without the documentation of recession, the study likely
overestimated the number of teeth that are periodontally healthy. Oddly, this study found
that diabetes was significantly correlated with anesthesia failure and periodontal health
was also correlated with anesthesia failure. In a systematic review, Borgnakke, et al.

53
found periodontal disease to be associated with poor glycemic control, diabetic
complications and the development of type 2 diabetes mellitus although the amount of
evidence was small, it was significant (115). In a consensus report from the American
Association of Periodontology and the European Federation of Periodontology, Chapple
and Genco discuss the presence of a large body of evidence supporting the independent
relationship of glycemic control and periodontal inflammation, with emerging evidence
relating periodontal disease and incidence of diabetes, as well as evidence that
periodontal disease adversely affects diabetic complications and glycemic control (116).
More research is needed related to diabetes and periodontal disease and their effects on
local anesthesia.
Failure Related to Quality of Life Impact of Tooth Pain
Tooth pain with a greater impact on quality of life factors was found to significant
in multiple methods in this study. Tooth pain with a greater level of interference with
recreational and social activities was found to be significantly associated with anesthesia
failure in Method 2 when analyzed individually with failures reporting an average level
of 2.14 (+/- 2.87) and successes reporting an average level of 1.34 (+/-2.37). In the
regression model for Method 2, the greater interference with recreation and social
activities caused patients to have a 1.670 times chance anesthesia failure for each higher
level of interference reported on a scale of 1 to 10; a person reporting a level of 10 would
have a 16.70 times higher chance of failure compared to a person reporting a level of 1.
Tooth pain with a greater level or interference with daily activities was found to be
statistically significant in Method 3 when analyzed individually. In the regression model
for Method 3, the greater interference with daily activities cause patients to have a 1.200

54
times chances of failure with each higher level of interference reported, thus a person
reporting an interference level of 10 would have a 12.00 times chance of anesthesia
failure compared to a person reporting a level of 1. In the regression model for Method
1, the number of days in the week prior to treatment was positively correlated with
anesthesia failure with a 1.332 times chance of failure for each day the patient
experienced pain, thus a patient who experienced pain for all 7 days prior to treatment
would have a 9.324 times chance of anesthesia failure. When looked at together, these
factors show pain that is more disruptive, whether by intensity, duration, or some other
manner, is associated with anesthesia failure. These results would be in agreement with
the well-established concept of symptomatic teeth being more difficult to anesthetize.
Failure Related to Preemptive Administration of Pain Medication
The patient questionnaire asks about any pain medication taken in the 7 days prior
to treatment and the regression model for Method 3 found that any type of pain
medication taken the week prior to treatment was negatively correlated with anesthesia
failure with a 0.587 times chance of anesthesia failure. This finding is in contrast to high
quality studies providing a high level of evidence have previously have shown that the
preoperative administration of ibuprofen had no effect on anesthesia success (34), the
combination of acetaminophen and ibuprofen had no effect (106), and acetaminophen
with hydrocodone also had no effect (35). Because of the limitation in the methodology,
the evidence in these previous studies is more compelling.
Although not specifically examined in this study, there were 36 patients in the
single appointment treatment group that used nitrous oxide during the procedure, this
group did not have markedly different anesthesia failure rates however an observation

55
that was not examined statistically was that none of these patients reported severe pain
during the procedure and only one reported moderate pain, the remaining 35 reported
only mild or no pain. The reported maximum levels of pain during the procedure were
higher when nitrous oxide was not used. This observation appears to be in agreement
with Stanley (61) and the use of nitrous oxide can improve anesthesia success and
quality.
Study Strengths and Limitations
Using data from the DPBRN provided a large sample size of teeth that were
undergoing endodontic treatment which is the population of interest in symptomatic
teeth. While calibration of multiple providers in these types of studies could be
considered a limitation, it could also be a strength because regardless of individual
technique overall trends in anesthesia failure can be investigated in a large scale practice
based network; with the large number of providers, individual operator technique
becomes less important.
Reliability between different data collectors/raters and reliability of the same
individual at different times can be problematic (117). The lack of a standardized
anesthesia protocol is a limitation; this may be the explanation for difference with
provider training and experience that were observed. An inherent limitation in survey
based studies is differences in interpretation of the questions by individual patients and
providers.
The most significant limitation of this study is that because it is exploratory in
nature, it was not specifically powered or designed to examine factors associated with
local anesthesia failure. It is possible several of the findings may be spurious. However,

56
being an effectiveness study and not an efficacy study allows a broad range of factors to
be investigated providing direction for future studies. Selection bias is a limitation in this
type of investigation with a possibility that the groups may differ systematically from the
population of interest leading to errors in association. Randomized, prospective
controlled clinical trials will certainly provide a higher level of evidence. Although a
multitude of variables were investigated, there are many more that were not such as
depression, anxiety, sleep quality, case difficulty, procedural mishaps, and many more.
Several of the confidence intervals in the regression models were very large mostly
explained by the low anesthesia failure rates leading to relatively low sample sizes.
Ideally future studies of this type should have a larger sample size.
The potential limitations with defining local anesthesia failure were previously
discussed in the results section, it is possible that patients did not report anesthesia failure
because it was addressed appropriately during treatment and their overall experience was
favorable when their symptoms were resolved with the treatment.

57
CONCLUSIONS
All of the null hypotheses were rejected, and the alternate hypotheses accepted;
statistically significant preoperative factors related to local anesthesia failure during non-
surgical root canal therapy were identified with all methods. Depending upon the method
used, the overall anesthesia failure rate ranged from 4.90% to 29.96%. With few
exceptions, the overall findings of this investigation agree with previous studies that
symptomatic teeth, with pulpitis and/or apical periodontitis, have higher local anesthesia
failure rates. It was found that teeth with necrotic pulps have less anesthesia failure in
multiple of the methods used in this study. The correlation of history of diabetes and
anesthesia failure is a novel finding and should be a focus of further research. Another
important novel finding was that endodontists and more experienced providers seem to be
better equipped to prevent anesthesia failures. Provider experience based on time in
practice and by provider type was found often in the various methods used in this
investigation without conflicting results between methods. The body of research in local
anesthesia is creating a paradigm shift from the question of which block technique is
better to the idea that local anesthesia is a process and can be tailored to the given clinical
scenario. As providers gain more experience with time and training, they likely come to
understand this and modify their techniques accordingly. The specialty of endodontics
has greatly contributed to the understanding of local anesthetics in dentistry, the gap may
lie in the passing of that knowledge to the new dentist. There appears to be tremendous
opportunity to impact the profession of dentistry for both dentists and patients if
endodontic departments engage in a team approach in local anesthesia training.

58
REFERENCES
1. Barclay JK. Current status of education in anesthesia and sedation in New Zealand, 1988. Anesthesia progress. 1989;36(4-5):214. 2. Walton RE, Torabinejad M. Managing local anesthesia problems in the endodontic patient. J Am Dent Assoc. 1992;123(5):97-102. 3. Hargreaves KM, Keiser K. Local anesthetic failure in endodontics. Endodontic Topics. 2002;1(1):26-39. 4. Kaufman E, Weinstein P, Milgrom P. Difficulties in achieving local anesthesia. The Journal of the American Dental Association. 1984;108(2):205-8. 5. Weinstein P, Milgrom P, Kaufman E, Fiset L, Ramsay D. Patient perceptions of failure to achieve optimal local anesthesia. Gen Dent. 1985;33(3):218-20. 6. Sherman MG, Flax M, Namerow K, Murray PE. Anesthetic Efficacy of the Gow-Gates Injection and Maxillary Infiltration with Articaine and Lidocaine for Irreversible Pulpitis. Journal of Endodontics. 2008;34(6):656-9. 7. Koller C. ON THE USE OF COCAINE FOR PRODUCING ANÆSTHESIA ON THE EYE. The Lancet. 1884;124(3197):990-2. 8. Hadda SE. Procaine: Alfred Einhorn’s ideal substitute for cocaine. The Journal of the American Dental Association. 1962;64(6):841-5. 9. Nevin M. Conduction and infiltration anesthesia with novol procaine tablets. New York (State): New York (State): Novocol Chemical Mfg. Co., 1919; 1919. 10. Gordh T. XYLOCAIN–A NEW LOCAL ANALGESIC. Anaesthesia. 1949;4(1):4-9. 11. Malamed S. LOCAL-ANESTHETICS - DENTISTRYS MOST IMPORTANT DRUGS. Journal Of The American Dental Association. 1994;125(12):1571-6. 12. Becker DE, Reed KL. Essentials of local anesthetic pharmacology. Anesth Prog. 2006;53(3):98-108; quiz 9-10. 13. Moore PA, Hersh EV. Local anesthetics: pharmacology and toxicity. Dent Clin North Am. 2010;54(4):587-99. 14. Wong MK, Jacobsen PL. Reasons for local anesthesia failures. J Am Dent Assoc. 1992;123(1):69-73. 15. Nixdorf DR, Law AS, Look JO, Rindal DB, Durand EU, Kang W, et al. Large-scale Clinical Endodontic Research in The National Dental Practice-Based Research Network: Study Overview and Methods. Journal of Endodontics. 2012;38(11):1470-8. 16. Nusstein JM, Reader A, Drum M. Local Anesthesia Strategies for the Patient With a “Hot” Tooth. Dental Clinics of North America. 2010;54(2):237-47. 17. Dobbs EC, De Vier C. L-Arterenol as a Vasoconstrictor in Local Anesthesia. The Journal of the American Dental Association. 1950;40(4):433-6. 18. Malamed SF. The Gow-Gates mandibular block: Evaluation after 4,275 cases. Oral Surgery, Oral Medicine, Oral Pathology. 1981;51(5):463-7. 19. Topazian RG. Pain thresholds and factors which modify them. Oral Surgery, Oral Medicine, Oral Pathology. 1957;10(11):1192-203.

59
20. Montagnese TA, Reader A, Melfi R. A comparative study of the Gow-Gates technique and a standard technique for mandibular anesthesia. Journal of Endodontics. 1984;10(4):158-63. 21. Kaufman E, Leresche L, Sommers E, Dworkin SF, Truelove EL. Intraligamentary anesthesia: a double-blind comparative study. The Journal of the American Dental Association. 1984;108(2):175-8. 22. Dreven LJ, Reader A, Beck FM, Meyers WJ, Weaver J. An evaluation of an electric pulp tester as a measure of analgesia in human vital teeth. Journal of Endodontics. 1987;13(5):233-8. 23. Schleder JR, Reader A, Beck M, Meyers WJ. The periodontal ligament injection: A comparison of 2% lidocaine, 3% mepivacaine, and 1:100,000 epinephrine to 2% lidocaine with 1: 100,000 epinephrine in human mandibular premolars. Journal of Endodontics. 1988;14(8):397-404. 24. Vreeland DL, Reader A, Beck M, Meyers W, Weaver J. An evaluation of volumes and concentrations of lidocaine in human inferior alveolar nerve block. Journal of Endodontics. 1989;15(1):6-12. 25. Robertson D, Nusstein J, Reader A, Beck M, McCartney M. The anesthetic efficacy of articaine in buccal infiltration of mandibular posterior teeth. The Journal of the American Dental Association. 2007;138(8):1104-12. 26. Mason R, Drum M, Reader A, Nusstein J, Beck M. A Prospective, Randomized, Double-blind Comparison of 2% Lidocaine With 1:100,000 and 1:50,000 Epinephrine and 3% Mepivacaine for Maxillary Infiltrations. Journal of Endodontics. 2009;35(9):1173-7. 27. Droll B, Drum M, Nusstein J, Reader A, Beck M. Anesthetic efficacy of the inferior alveolar nerve block in red-haired women. J Endod. 2012;38(12):1564-9. 28. Steinkruger G, Nusstein J, Reader A, Beck M, Weaver J. The significance of needle bevel orientation in achieving a successful inferior alveolar nerve block. The Journal of the American Dental Association. 2006;137(12):1685-91. 29. Yonchak T, Reader A, Beck M, Meyers WJ. Anesthetic efficacy of unilateral and bilateral inferior alveolar nerve blocks to determine cross innervation in anterior teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92(2):132-5. 30. Jung I-Y, Kim J-H, Kim E-S, Lee C-Y, Lee SJ. An Evaluation of Buccal Infiltrations and Inferior Alveolar Nerve Blocks in Pulpal Anesthesia for Mandibular First Molars. Journal of Endodontics. 2008;34(1):11-3. 31. Nist RA, Reader A, Beck M, Meyers WJ. An evaluation of the incisive nerve block and combination inferior alveolar and incisive nerve blocks in mandibular anesthesia. Journal of Endodontics. 1992;18(9):455-9. 32. Nusstein J, Reader A, Nist R, Beck M, Meyers WJ. Anesthetic efficacy of the supplemental intraosseous injection of 2% lidocaine with 1:100,000 epinephrine in irreversible pulpitis. J Endod. 1998;24(7):487-91. 33. Heft MW, Parker SR. An experimental basis for revising the graphic rating scale for pain. Pain. 1984;19(2):153-61.

60
34. Oleson M, Drum M, Reader A, Nusstein J, Beck M. Effect of Preoperative Ibuprofen on the Success of the Inferior Alveolar Nerve Block in Patients with Irreversible Pulpitis. Journal of Endodontics. 2010;36(3):379-82. 35. Fullmer S, Drum M, Reader A, Nusstein J, Beck M. Effect of preoperative acetaminophen/hydrocodone on the efficacy of the inferior alveolar nerve block in patients with symptomatic irreversible pulpitis: a prospective, randomized, double-blind, placebo-controlled study. J Endod. 2014;40(1):1-5. 36. Aggarwal V, Jain A, Kabi D. Anesthetic efficacy of supplemental buccal and lingual infiltrations of articaine and lidocaine after an inferior alveolar nerve block in patients with irreversible pulpitis. J Endod. 2009;35(7):925-9. 37. Nusstein J, Kennedy S, Reader A, Beck M, Weaver J. Anesthetic Efficacy of the Supplemental X-tip Intraosseous Injection in Patients with Irreversible Pulpitis. Journal of Endodontics. 2003;29(11):724-8. 38. Aggarwal V, Singla M, Miglani S, Kohli S, Singh S. Comparative evaluation of 1.8 mL and 3.6 mL of 2% lidocaine with 1:200,000 epinephrine for inferior alveolar nerve block in patients with irreversible pulpitis: a prospective, randomized single-blind study. J Endod. 2012;38(6):753-6. 39. Corah NL. Development of a Dental Anxiety Scale. Journal of Dental Research. 1969;48(4):596-. 40. Corah NL, Gale EN, Illig SJ. Assessment of a dental anxiety scale. The Journal of the American Dental Association. 1978;97(5):816-9. 41. Fowler S, Reader A, Beck M. Incidence of missed inferior alveolar nerve blocks in vital asymptomatic subjects and in patients with symptomatic irreversible pulpitis. J Endod. 2015;41(5):637-9. 42. Goldberg S, Reader A, Drum M, Nusstein J, Beck M. Comparison of the anesthetic efficacy of the conventional inferior alveolar, Gow-Gates, and Vazirani-Akinosi techniques. J Endod. 2008;34(11):1306-11. 43. Aggarwal V, Singla M, Kabi D. Comparative evaluation of anesthetic efficacy of Gow-Gates mandibular conduction anesthesia, Vazirani-Akinosi technique, buccal-plus-lingual infiltrations, and conventional inferior alveolar nerve anesthesia in patients with irreversible pulpitis. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology. 2010;109(2):303-8. 44. Click V, Drum M, Reader A, Nusstein J, Beck M. Evaluation of the Gow-Gates and Vazirani-Akinosi Techniques in Patients with Symptomatic Irreversible Pulpitis: A Prospective Randomized Study. Journal Of Endodontics. 2015;41(1):16-21. 45. Roda RS, Blanton PL. The anatomy of local anesthesia. Quintessence Int. 1994;25(1):27-38. 46. Milles M. The missed inferior alveolar block: a new look at an old problem. Anesth Prog. 1984;31(2):87-90. 47. Wong JD, Sved AM. Maxillary nerve block anaesthesia via the greater palatine canal: A modified technique and case reports. Australian Dental Journal. 1991;36(1):15-21.

61
48. Gow-Gates GAE. Mandibular conduction anesthesia: A new technique using extraoral landmarks. Oral Surgery, Oral Medicine, Oral Pathology. 1973;36(3):321-8. 49. Akinosi JO. A new approach to the mandibular nerve block. British Journal of Oral Surgery. 1977;15(1):83-7. 50. Meechan JG. How to overcome failed local anaesthesia. British dental journal. 1999;186(1):15. 51. Saatchi M, Shafiee M, Khademi A, Memarzadeh B. Anesthetic Efficacy of Gow-Gates Nerve Block, Inferior Alveolar Nerve Block, and Their Combination in Mandibular Molars with Symptomatic Irreversible Pulpitis: A Prospective, Randomized Clinical Trial. J Endod. 2018;44(3):384-8. 52. Aggarwal V, Singla M, Miglani S, Kohli S. Efficacy of Articaine Versus Lidocaine Administered as Supplementary Intraligamentary Injection after a Failed Inferior Alveolar Nerve Block: A Randomized Double-blind Study. J Endod. 2019;45(1):1-5. 53. Kanaa MD, Whitworth JM, Corbett IP, Meechan JG. Articaine and lidocaine mandibular buccal infiltration anesthesia: a prospective randomized double-blind cross-over study. J Endod. 2006;32(4):296-8. 54. Kanaa MD, Whitworth JM, Meechan JG. A prospective randomized trial of different supplementary local anesthetic techniques after failure of inferior alveolar nerve block in patients with irreversible pulpitis in mandibular teeth. J Endod. 2012;38(4):421-5. 55. Kanaa MD, Meechan JG, Corbett IP, Whitworth JM. Speed of injection influences efficacy of inferior alveolar nerve blocks: a double-blind randomized controlled trial in volunteers. J Endod. 2006;32(10):919-23. 56. Aggarwal V, Singla M, Miglani S, Kohli S, Irfan M. A Prospective, Randomized Single-blind Evaluation of Effect of Injection Speed on Anesthetic Efficacy of Inferior Alveolar Nerve Block in Patients with Symptomatic Irreversible Pulpitis. Journal of Endodontics. 2012;38(12):1578-80. 57. Rood JP. Some anatomical and physiological causes of failure to achieve mandibular analgesia. Br J Oral Surg. 1977;15(1):75-82. 58. Fowler S, Reader A. Is a Volume of 3.6 mL Better than 1.8 mL for Inferior Alveolar Nerve Blocks in Patients with Symptomatic Irreversible Pulpitis? Journal of Endodontics. 2013;39(8):970-2. 59. Mikesell A, Drum M, Reader A, Beck M. Anesthetic efficacy of 1.8 mL and 3.6 mL of 2% lidocaine with 1:100,000 epinephrine for maxillary infiltrations. J Endod. 2008;34(2):121-5. 60. Drum M, Reader A, Nusstein J, Fowler S. Successful pulpal anesthesia for symptomatic irreversible pulpitis. The Journal of the American Dental Association. 2017;148(4):267-71. 61. Stanley W, Drum M, Nusstein J, Reader A, Beck M. Effect of nitrous oxide on the efficacy of the inferior alveolar nerve block in patients with symptomatic irreversible pulpitis. J Endod. 2012;38(5):565-9.

62
62. Frommer J, Mele FA, Monroe CW. The Possible Role of the Mylohyoid Nerve in Mandibular Posterior Tooth Sensation. The Journal of the American Dental Association. 1972;85(1):113-7. 63. Pogrel MA, Smith R, Ahani R. Innervation of the mandibular incisors by the mental nerve. J Oral Maxillofac Surg. 1997;55(9):961-3. 64. Loetscher CA, Walton RE. Patterns of innervation of the maxillary first molar: A dissection study. Oral Surgery, Oral Medicine, Oral Pathology. 1988;65(1):86-90. 65. Rood JP, Pateromichelakis S. Inflammation and peripheral nerve sensitisation. British Journal of Oral Surgery. 1981;19(1):67-72. 66. Punnia-Moorthy A. Buffering capacity of normal and inflamed tissues following the injection of local anaesthetic solutions. Br J Anaesth. 1988;61(2):154-9. 67. Aggarwal V, Singla M, Miglani S, Kohli S. Comparison of the anaesthetic efficacy of epinephrine concentrations (1 : 80 000 and 1 : 200 000) in 2% lidocaine for inferior alveolar nerve block in patients with symptomatic irreversible pulpitis: a randomized, double-blind clinical trial. International Endodontic Journal. 2014;47(4):373-9. 68. Taylor PE, Byers MR, Redd PE. Sprouting of CGRP nerve fibers in response to dentin injury in rat molars. Brain Research. 1988;461(2):371-6. 69. Byers MR, Taylor PE, Khayat BG, Kimberly CL. Effects of injury and inflammation on pulpal and periapical nerves. Journal of Endodontics. 1990;16(2):78-84. 70. Caviedes-Bucheli J, Azuero-Holguin MM, Correa-Ortiz JA, Aguilar-Mora MV, Pedroza-Flores JD, Ulate E, et al. Effect of Experimentally Induced Occlusal Trauma on Substance P Expression in Human Dental Pulp and Periodontal Ligament. Journal of Endodontics. 2011;37(5):627-30. 71. Pinto V, Derkach VA, Safronov BV. Role of TTX-sensitive and TTX-resistant sodium channels in Adelta- and C-fiber conduction and synaptic transmission. J Neurophysiol. 2008;99(2):617-28. 72. Gold MS. Tetrodotoxin-Resistant Na<sup>+</sup> Currents and Inflammatory Hyperalgesia. Proceedings of the National Academy of Sciences of the United States of America. 1999;96(14):7645-9. 73. Scholz A. Mechanisms of (local) anaesthetics on voltage-gated sodium and other ion channels. British Journal of Anaesthesia. 2002;89(1):52-61. 74. Roy ML, Reuveny E, Narahashi T. Single-channel analysis of tetrodotoxin-sensitive and tetrodotoxin-resistant sodium channels in rat dorsal root ganglion neurons. Brain Research. 1994;650(2):341-6. 75. Melzack R, Wall PD. Pain Mechanisms: A New Theory. Science. 1965;150(3699):971-9. 76. Cho S-Y, Kim E, Park S-H, Roh B-D, Lee C-Y, Lee S-J, et al. Effect of Topical Anesthesia on Pain from Needle Insertion and Injection and Its Relationship with Anxiety in Patients Awaiting Apical Surgery: A Randomized Double-blind Clinical Trial. Journal of Endodontics. 2017;43(3):364-9.

63
77. Fiset L, Milgrom P, Weinstein P, Getz T, Glassman P. Psychophysiological responses to dental injections. The Journal of the American Dental Association. 1985;111(4):578-83. 78. Lin C-S. Pain catastrophizing in dental patients. The Journal of the American Dental Association. 2013;144(11):1244-51. 79. Gilbert GH, Williams OD, Rindal DB, Pihlstrom DJ, Benjamin PL, Wallace MC. The Creation and Development of the Dental Practice-Based Research Network. The Journal of the American Dental Association. 2008;139(1):74-81. 80. Nixdorf DR, Law AS, John MT, Sobieh RM, Kohli R, Nguyen RHN. Differential Diagnoses for Persistent Pain after Root Canal Treatment: A Study in the National Dental Practice-based Research Network. Journal of Endodontics. 2015;41(4):457-63. 81. Nixdorf RD, Law SA, Lindquist JK, Reams HNG, Cole RE, Kanter RK, et al. Frequency, impact, and predictors of persistent pain after root canal treatment: a national dental PBRN study. PAIN. 2016;157(1):159-65. 82. Hryvenko I. Long-term Outcome of Patients with Persistent Pain Following Root Canal Treatment: The National Dental Practice-Based Research Network. 2018. 83. Law AS. Predicting Severe Pain after Root Canal Therapy in the National Dental PBRN. Journal of dental research /. 2014;94(3_suppl):37-43. 84. Law AS, Nixdorf DR, Rabinowitz I, Reams GJ, Smith JA, Torres AV, et al. Root Canal Therapy Reduces Multiple Dimensions of Pain: A National Dental Practice-based Research Network Study. Journal of Endodontics. 2014;40(11):1738-45. 85. Pigg M, Nixdorf DR, Nguyen RHN, Law AS. Validity of Preoperative Clinical Findings to Identify Dental Pulp Status: A National Dental Practice-Based Research Network Study. Journal of Endodontics. 2016;42(6):935-42. 86. Gilbert GH, Williams OD, Korelitz JJ, Fellows JL, Gordan VV, Makhija SK, et al. Purpose, structure, and function of the United States National Dental Practice-Based Research Network. Journal of Dentistry. 2013;41(11):1051-9. 87. Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. Journal of Clinical Periodontology. 2018;45(S20):S149-S61. 88. Moreira MS, Anuar ASN-S, Tedesco TK, Dos Santos M, Morimoto S. Endodontic Treatment in Single and Multiple Visits: An Overview of Systematic Reviews. Journal of Endodontics. 2017;43(6):864-70. 89. Vera J, Siqueira JF, Ricucci D, Loghin S, Fernández N, Flores B, et al. One- versus Two-visit Endodontic Treatment of Teeth with Apical Periodontitis: A Histobacteriologic Study. Journal of Endodontics. 2012;38(8):1040-52. 90. Meechan JG. Supplementary routes to local anaesthesia. Int Endod J. 2002;35(11):885-96. 91. Dower JS. A survey of local anesthesia course directors. Anesthesia progress. 1998;45(3):91. 92. Malamed SF. The periodontal ligament (PDL) injection: An alternative to inferior alveolar nerve block. Oral Surgery, Oral Medicine, Oral Pathology. 1982;53(2):117-21.

64
93. Kary AL, Gomez J, Raffaelli SD, Levine MH. Preclinical Local Anesthesia Education in Dental Schools: A Systematic Review. Journal of Dental Education. 2018;82(10):1059-64. 94. Simon JF, Peltier B, Chambers D, Dower J. Dentists troubled by the administration of anesthetic injections: long-term stresses and effects. Quintessence international (Berlin, Germany : 1985). 1994;25(9):641. 95. Halsted SW. PRACITAL COMMENTS ON THE USE AND ABUSE OF COCAINE; SUGGESTED BY ITS INVARIABLY SUCCESSFUL EMPLOYMENT IN MORE THAN A THOUSAND MINOR SURGICAL OPERATIONS. Survey of Anesthesiology. 1984;28(2):156-. 96. Cohen HP, Cha BY, Spångberg LSW. Endodontic anesthesia in mandibular molars: A clinical study. Journal of Endodontics. 1993;19(7):370-3. 97. Hsiao-Wu GW, Susarla SM, White RR. Use of the Cold Test as a Measure of Pulpal Anesthesia During Endodontic Therapy: A Randomized, Blinded, Placebo-Controlled Clinical Trial. Journal of Endodontics. 2007;33(4):406-10. 98. Ozturk I, Kilic B, Demiroglu M, Alptekin H, Yazicioglu D, Oguz E, et al. EFFECT OF DIABETES MELLITUS ON SPINAL ANESTHESIA FAILURE. Acta Medica Mediterranea. 2017;33(3):417-21. 99. Baeriswyl M, Taffé P, Kirkham KR, Bathory I, Rancati V, Crevoisier X, et al. Comparison of peripheral nerve blockade characteristics between non-diabetic patients and patients suffering from diabetic neuropathy: a prospective cohort study. Anaesthesia. 2018;73(9):1110-7. 100. Cuvillon P, Reubrecht V, Zoric L, Lemoine L, Belin M, Ducombs O, et al. Comparison of subgluteal sciatic nerve block duration in type 2 diabetic and non-diabetic patients. Br J Anaesth. 2013;110(5):823-30. 101. Gebhard ER, Nielsen CK, Pietrobon AR, Missair AA, Williams AB. Diabetes Mellitus, Independent of Body Mass Index, Is Associated With a "Higher Success" Rate for Supraclavicular Brachial Plexus Blocks. Regional Anesthesia and Pain Medicine. 2009;34(5):404-7. 102. Okamura K, Kobayashi I, Matsuo K, Taniguchi K, Ishibashi Y, Izumi T, et al. An immunohistochemical and ultrastructural study of vasomotor nerves in the microvasculature of human dental pulp. Archives of Oral Biology. 1995;40(1):47-53. 103. Takahashi K, Kishi Y, Kim S. A scanning electron microscope study of the blood vessels of dog pulp using corrosion resin casts. Journal of Endodontics. 1982;8(3):131-5. 104. Kim S. Microcirculation of the dental pulp in health and disease. Journal of Endodontics. 1985;11(11):465-71. 105. Ditre JW, Brandon TH, Zale EL, Meagher MM. Pain, Nicotine, and Smoking: Research Findings and Mechanistic Considerations. Psychological Bulletin. 2011;137(6):1065-93. 106. Simpson M, Drum M, Nusstein J, Reader A, Beck M. Effect of combination of preoperative ibuprofen/acetaminophen on the success of the inferior alveolar nerve block in patients with symptomatic irreversible pulpitis. J Endod. 2011;37(5):593-7.

65
107. Schellenberg J, Drum M, Reader A, Nusstein J, Fowler S, Beck M. Effect of Buffered 4% Lidocaine on the Success of the Inferior Alveolar Nerve Block in Patients with Symptomatic Irreversible Pulpitis: A Prospective, Randomized, Double-blind Study. Journal of Endodontics. 2015;41(6):791-6. 108. Lindemann M, Reader A, Nusstein J, Drum M, Beck M. Effect of Sublingual Triazolam on the Success of Inferior Alveolar Nerve Block in Patients with Irreversible Pulpitis. Journal of Endodontics. 2008;34(10):1167-70. 109. Khademi AA, Saatchi M, Minaiyan M, Rostamizadeh N, Sharafi F. Effect of Preoperative Alprazolam on the Success of Inferior Alveolar Nerve Block for Teeth with Irreversible Pulpitis. Journal of Endodontics. 2012;38(10):1337-9. 110. AAE Glossary of Endodontic Terms 10th Edition March 2020. Available at www.aae.org/specialty/clinical-resources/glossary-endodontic-term/. 111. Abbott PV. Classification, diagnosis and clinical manifestations of apical periodontitis. Endodontic Topics. 2004;8(1):36-54. 112. Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesions in bone: I. The Journal of the American Dental Association. 1961;62:152-60. 113. Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesions in bone: II. The Journal of the American Dental Association. 1961;62(6):708-16. 114. Owatz CB, Khan AA, Schindler WG, Schwartz SA, Keiser K, Hargreaves KM. The Incidence of Mechanical Allodynia in Patients With Irreversible Pulpitis. Journal of Endodontics. 2007;33(5):552-6. 115. Borgnakke WS, Yl€Ostalo PV, Taylor GW, Genco RJ. Effect of periodontal disease on diabetes: systematic review of epidemiologic observational evidence. Journal of Periodontology. 2013;84(4 Suppl):S135-S52. 116. Chapple ILC, Genco R. Diabetes and periodontal diseases: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. Journal of Clinical Periodontology. 2013;40(s14):S106. 117. Goldman M, Pearson AH, Darzenta N. Reliability of radiographic interpretations. Oral Surgery, Oral Medicine, Oral Pathology. 1974;38(2):287-93.

66
APPENDIX I – Patient Contact Form
DPBRN Study 17-18 – Patient Contact Form Version 033110 Page 1 of 1
CONTACT INFORMATION The following information will be kept separate from your answers to protect your privacy. This information will be sent directly to research staff and will only be used to contact you in the future for reminder calls, follow up questions, and mailing your compensation at 1 week, 3 months, and 6 months. Mailing may take 4-6 weeks after the receipt of each survey. PLEASE PRINT YOUR INFORMATION Date / / 201 mm dd y (QPMON QPDAY QPYEAR) or QPDATE Name: QPNAME Address:________________________________________ QPADDR City, State, Zip:__________________________________ QPCSZ
Telephone number: QPPHONE
Cell phone number: QPCELL
The best time to call is QPCALLTM
E-mail address: QPEMAIL
Please provide a contact name and phone number of a friend or relative who lives at a different address so that we may contact him/her in case we cannot reach you: Name: QPALTNAME Phone:________________________________________ QPALTPHONE
Please leave this form with your dentist’s staff.

67
APPENDIX II – Patient Survey Before Treatment
DPBRN Study 17-18 -- FORM 04 Version 033110 Page 1 of 4
Patient Survey — Before Treatment Please mark answers with an “X” in the corresponding box. It is very important that the responses be recorded within the space allotted. Example: X When recording numerical responses, such as amounts or dates, one number should be entered into each box. Example: 0 1 / 0 3 / 20 1 0
Today’s Date / 201 mm dd y
(Q04P0MON Q04P0DAY Q04P0YEAR) or Q04P0DATE Complete Questions 1 through 10 before the tooth is numbed.
1. Are you fearful about today’s appointment? Q04P0FEAR
a. Not at all b. A little c. Quite a lot d. Very much
2. I feel that the treatment outcome for my tooth will turn out (mark one): Q04P0OUTC
a. very good. b. good. c. fair. d. poor. Q04P0PADAY
3. How many days in the past week have you had tooth pain? Days (If no pain, please write “0”)
4. Have you taken anything for the pain (over-the-counter or prescription medication, herbal, other) in the last 7 days? Q04P0PAMED
a. Yes b. No
IF PAIN WAS NOT PRESENT IN THE PAST 7 DAYS, SKIP TO QUESTION #11 5. Pain quality (mark all that apply)
a. none Q04P0NONE b. dull Q04P0DULL c. sharp Q04P0SHRP d. aching Q04P0ACH e. throbbing Q04P0THROB f. burning Q04P0BURN g. shooting Q04P0SHOOT h. electric Q04P0ELECT
6. Does this pain? (mark all that apply) a. start all by itself for no known reason (spontaneous) Q04P0SPON b. start after the tooth is used or irritated (provoked) Q04P0PROV

68

69

70

71
APPENDIX III – Dentist Survey Before Treatment
DPBRN Study 17-18 -- FORM 05 Version 033110 Page 1 of 1
Dentist Survey – Before Treatment (Diagnosis) Please mark answers with an “X” in the corresponding box. It is very important that the responses be recorded within the space allotted. Example: X When recording numerical responses, such as amounts or dates, one number should be entered into each box. Example: 0 1 / 0 3 / 201 0
Visit Date / / 201 mm dd y (Q05D0MON Q05D0DAY Q05D0YEAR) or Q05D0DATE NOTE: Do not continue until patient consent obtained
Q05D0TONUM
1. Which tooth is to be treated with a root canal? (Universal numbering system: 01- 32)
2. Does the tooth exhibit a radiolucency of endodontic origin (periradicular or apical)? Q05D0ENDO a. Yes b. No
Physical Exam
3. Was the tooth tender to percussion? Q05D0PERC a. Yes b. No
4. Was the tooth tender to biting pressure? Q05D0BITE
a. Yes b. No
5. Did the tooth respond to cold testing (if no, skip to question 7)? Q05D0COLD
a. Yes b. No
6. Was the response to cold testing prolonged compared to adjacent teeth? Q05D0COLDPROL
a. Yes b. No
7. What was the greatest probing depth for this tooth? mm Q05D0DEEP
8. What was the location of this greatest probing depth? Q05D0DEEPLOC
a. Mesial b. Distal c. Buccal d. Lingual

72
APPENDIX IV – Dentist Survey Post-Treatment

73

74
APPENDIX V – Patient Survey Immediately After Treatment
DPBRN Study 17-18 -- FORM 09 Version 033110 Page 1 of 1
Patient Survey – Immediately After Treatment Please complete before you leave the office today.
Please mark answers with an “X” in the corresponding box. It is very important that the responses be recorded within the space allotted. Example: X When recording numerical responses, such as amounts or dates, one number should be entered into each box. Example: 0 1 / 0 3 / 20 1 0
1. How intense was your tooth pain during the root canal on a 0 to 10 scale, where 0 is "no pain" and 10 is "pain as bad as could be"? Q09P1PAIN
No Pain Pain as bad as could be
0 1 2 3 4 5 6 7 8 9 10
2. Please rate how numb your tooth felt during the root canal treatment (mark one). Q09P1NUMB a. The tooth was not numb enough. b. The tooth was numb enough. c. The tooth was too numb.
3. Please rate how your feelings of fear compared to the actual experience. Q09P1FEAR a. Does not apply – I was not afraid. b. The experience was better than I feared. c. The experience was about what I feared. d. The experience was worse than what I feared.

75
APPENDIX VI – Dentist Pain and Anxiety Management Form

76

77
APPENDIX VII – Provider, Patient and Tooth Characteristics by Number of Visits

78

79

80
APPENDIX VIII – Anesthesia Failure Rates Method 1: Patient Reported Numbness

81

82

83
APPENDIX IX – Anesthesia Failure Rates Method 2 – Provider Reported Quality

84

85

86
APPENDIX X – Anesthesia Failure Rates Method 3: Supplemental Anesthesia

87

88