Embed Size (px)
Citation preview

Prepared by:
Donna Tydings, MS, RN, CNS-BC, CCRN
September 2013
Copywrite 2013 This presentation may not be duplicated without permission of the author


The first formal consensus in 1965
◦ American Nurses Association (ANA) published an historical position paper recommending baccalaureate-in-nursing (BSN) preparation as entry level
◦ 1978, the ANA House of Delegates again endorsed BSN as entry level to commence in 1985
2003, New York State Board for Nursing unanimously approved a motion to require BS preparation within 10 years of initial licensure in New York State

Patients are sicker and more frail
Management of multiple co-morbidities and chronic illnesses
Patient care is increasingly complex
Earlier discharges demand more patient education and preparation
Diversity of the patient population
Never events (29 preventable events where no payment is received)
Interactions with multiple agencies and providers
Scientific advances
Information management systems are more complex
More technology
Requirements for the analysis and synthesis of data from the EMR
Value based purchasing (payment for quality outcomes)

A wider variety of competencies
◦ Health policy
◦ Healthcare financing
◦ Leadership and leading care coordination
◦ Quality improvement
◦ Systems thinking
◦ Research and evidence-based practice
◦ Community/public health
◦ Ethics


2003 groundbreaking work by Aiken, Clarke, Cheung, Sloan, and Silber published in the Journal of the American Medical Association.
Examined whether the proportion of RNs prepared at the BS level or higher was associated with surgical patient mortality or failure to rescue.
After adjustments for patient and hospital characteristics, nurse staffing and experience, and whether the surgeon was board certified, the researchers found that a 10% increase in BS-prepared RNs was associated with a 5% decrease in the likelihood of patient mortality within 30 days of admission and the odds of failure to rescue.

Aiken, Clarke, Sloane, Lake, and Cheney (2008) examined the effects of nurse-practice environment on patient outcomes.
After controlling for nurse staffing and educational preparation, they concluded that “surgical mortality rates were more than 60% higher in poorly staffed hospitals with the poorest patient care environments than in hospitals with the better care environments in the sample, the best nurse staffing levels, and the most highly educated nurses” (p. 228).
The researchers go on to estimate that 40,000 patient deaths per year could be averted by maximizing all three variables.

2007 Canadian study by Tourangeau et al., examined nursing-related determinants of acute medical patients’ 30-day mortality.
Established 45% of the variance was explained by eight nurse-related predictors, one of which was baccalaureate preparation.
Every 10% increase in the proportion of BS-prepared RNs was associated with nine fewer deaths per 1000 discharged patients.

Studies by:
Estabrooks, Midodzi, Cummins, Ricker, and Giovanneti (2005), VandenHeed et al. (2009)
Focused review of 15 research manuscripts by Tourangeau, Cranley, and Jeffs (2006)
Found that among other factors, BS preparation contributed to decreased patient mortality.

Kendall-Gallagher, Aiken, Sloane, and Cimiotti (2011) studied whether staff nurses with specialty certification positively impacted mortality and failure to rescue.
Researchers determined
BS-and-higher educational preparation decreased mortality and failure-to-rescue rates by 6%
Specialty certification decreased these rates by an additional 2%, but only among nurses with BS or higher education.

Aiken et al. (2011) examined the relationship between work environment, nurse education, and staffing on patient mortality and failure to rescue.
First study to reveal “the conditional circumstances under which particular nursing investments yield the best outcomes” (p. 1047).
Nursing work environment was critical to achieving positive patient outcomes.
However, they concluded that a 10% increase in BS-prepared RNs decreased the likelihood of patient death or failure to rescue by approximately 4%, regardless of the work environment.

Blegen, Goode, Park, Vaughn and Spetz (2013) is the first to demonstrate a relationship between higher proportions of BS-prepared RNs with nurse sensitive indicators other than patient death and failure to rescue.
The hospitals with higher proportions of BS-prepared RNs “…had lower rates of HAPUs, postoperative DVT/PE, and LOS as well as failure to rescue and CHF mortality” (p. 4).

BS-prepared RNs are more likely to remain in their current jobs (NYONE, n.d.)
◦ Reduction of nurse turnover saves approximately $82,000 per RN (Jones, 2008)
Hospitals with higher proportions of BS-prepared RNs enjoy lower rates of HAPUs and LOS (Blegen, et al., 2013)
◦ Through reduction of hospital acquired pressure ulcers, NYS can save approximately $104 million each year (Zimmermann, Miner & Zittel, 2010).
◦ Decreased LOS is not only cost averting but also potentially revenue generating as patient capacity is expanded.
When 60% of NYS nurses are prepared at the BS level the state can project 6000 fewer surgical deaths annually (NYONE, n.d.)
The value of decreasing patient mortality is incalculable.


A recommendation reported in the Institute of Medicine, Future of Nursing, Leading Change, Advancing Health.
The report calls for 80% of the nursing workforce to be BS prepared by 2020.
This recommendation is based on literature revealing improved patient outcomes as organizations increase their proportion of BS-prepared RNs.

The American Nurses Credentialing Center (ANCC) Magnet Recognition Program® added source of evidence
◦ Applicants must outline their plan to reach the 80% recommendation by 2020

In 2005, legislation was introduced to amend the NYS Nurse Practice Act to require nurses to obtain a BS degree within 10 years of original licensure
Steadily increasing support for this bill
Grandparent students enrolled in associate degree programs and currently licensed RNs
Includes provisions to place a RN’s license on hold if BSN achievement does not occur within 10 years of initial licensure
Provides for an extension beyond 10 years when extenuating circumstances arise
Diploma and associate degree programs would continue, and graduates from these programs would continue to be eligible for licensure.


Australia
Belgium
Canada
Denmark
Finland
Ireland
Italy
Netherlands
New Zealand
Norway
Philippines
Spain
Thailand
Turkey

% US BS-
Prepared RNs
% US
MS/doctorate-
prepared RNs
% US Total RNs
prepared at BS or
higher degree
% NYS BS-
prepared RNs
% NYS
MS/doctorate-
prepared RNs
% NYS Total RNs
prepared at BS or
higher degree
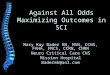
2000 32.8 10.3 43.1 32.2 14.2 46.4
2004 34.7 13.2 47.9 33.4 16.4 49.8
2008 36.8 13.2 50.0 34.8 16.7 51.5
Percentage of All US and NYS RNs with BS, MS, and Doctoral Degrees
U.S. Department of Health and Human Services Health Resources and Services Administration, 2010

Initial BS Graduate
◦ 1000 Bachelors
◦ 197 Masters
◦ 18 Doctorate
◦ 215 total graduate degree
Initial ADN Graduate
◦ 1000 Associates
◦ 215 Bachelors
◦ 58 Masters
◦ 9 Doctorate
◦ 67 total graduate degree
Aiken, 2011


Recent recommendations are to increase the proportion of BS-prepared RNs
This initiative is supported by numerous esteemed groups and organizations

More BS-prepared RNs can:
◦ Improve patient outcomes and save lives
◦ Conserve healthcare dollars
◦ Function as strong and effective nursing leaders
◦ Ensure adequate nursing faculty and nurse researchers in the future
◦ Preserve credibility of the US in the global healthcare market
◦ Enhance the professionalism of nursing

WHY NOT?

Act to amend the education law, in relation to the educational preparation for practice of professional nursing, (2013). Retrieved from http://assembly.state.ny.us/leg/?bn=A03103&term=2013
Act to amend the education law, in relation to the educational preparation for practice of professional nursing, (2013). Retrieved from http://assembly.state.ny.us/leg/?term=2013&bn=S00628
Aiken, L. (2011). Nurses for the future. New England Journal of Medicine, 364, 196-198.
Aiken, L., Cimiotti, J., Sloane, D., Smith, H., Flynn, L., & Neff, D. (2011). Effects of nurse staffing and nurse education on patient deaths in hospitals with different nurse work environments. Medical Care, 12, 1047-1053.
Aiken, L., Clarke, S., Cheung, R., Sloane, D., & Silber, J. (2003). Educational levels of hospital nurses and surgical patient mortality. Journal of the American Medical Association, 290, 1617-1623.

Aiken, L., Clarke, S., Sloane, D., Lake, E., & Cheney, T. (2008). Effects of hospital care environment on patient mortality and nurse outcomes. Journal of Nursing Administration, 38, 223-229.
American Nurses Credentialing Center. (2008). Magnet Recognition Program Application Manual. Silver Springs, MD: American Nurses Credentialing Center.
Blegen, M., Goode, C., Park, S., Vaughn, T., & Spetz, J. (2013). Baccalaureate education in nursing and patient outcomes. Journal of Nursing Administration, 31, 33-39.
Estabrooks, C., Midodzi, W., Cummings, G., Ricker, K., & Giovanneti, P. (2005). The impact of hospital nursing characteristics on 30-day mortality. Nursing Research, 54, 74-84.
Institute of Medicine. (2010). Transforming education. In The Future of Nursing: Leading Change, Advancing Health (pp. 163-219). Washington, DC: The National Academies Press.

Jones, C. (2008). Revisiting nurse turnover costs: Adjusting for inflation. Journal of Nursing Administration, 38, 11-18.
Kendall-Gallagher, D., Aiken, L., Sloane, D., & Cimiotti, J. (2011). Nurse specialty certification, inpatient mortality, and failure to rescue. Journal of Nursing Scholarship, 43, 188-194.
New York Organization of Nurse Executives. (n.d.). Educational advancement of the nursing profession (A3103; S628) executive summary.
Tourangeau, A., Doran, D., Hall, L., Pallas, L., Pringle, D., Tu, J., & Cranley, L. (2007). Impact of hospital nursing care on 30-day mortality for acute medical patients. Journal of Advanced Nursing, 57, 32-44.

Tourangeau, A., Cranley, L., & Jeffs, L. (2006). Impact of nursing on hospital patient mortality: A focused review and related policy implications. Quality and Safety in Health Care, 15, 4-8.
U.S. Department of Health and Human Services Health Resources and Services Administration. (2010). The registered nurse population findings from the 2008 national sample survey of registered nurses. Retrieved from http://bhpr.hrsa.gov/healthworkforce/rnsurveys/rnsurveyfinal.pdf
VandenHeed, K., Lasaffre, E., Diya, L., Vleugels, A., Clarke, S., Aiken, L., & Sermeus, W. (2009). The relationship between inpatient cardiac surgery mortality and nurse numbers and educational level: analysis of administrative data. International Journal of Nursing Studies, 46, 796-803.
Zimmermann, D. T., Miner, D. C. & Zittel, B. (2010). Advancing the education of nurses: A call to action. Journal of Nursing Administration, 40, 529-533.