Embed Size (px)
Citation preview
Prescribing Bioptic Telescopes
Qualify, Demonstrate, Indoctrinate, Recruit
Henry A. Greene, OD, FAAO
Reading is a solitary activityMost responsive to low vision aids
high contrast controllable environment
Reading is the most easily replaced visual activity
talking books radio, TV sighted support
Distance Vision is a Social Activity
Seeing faces Interpersonal relations
Non-verbal body language Making eye contact
Avoidance of isolationQuality of life
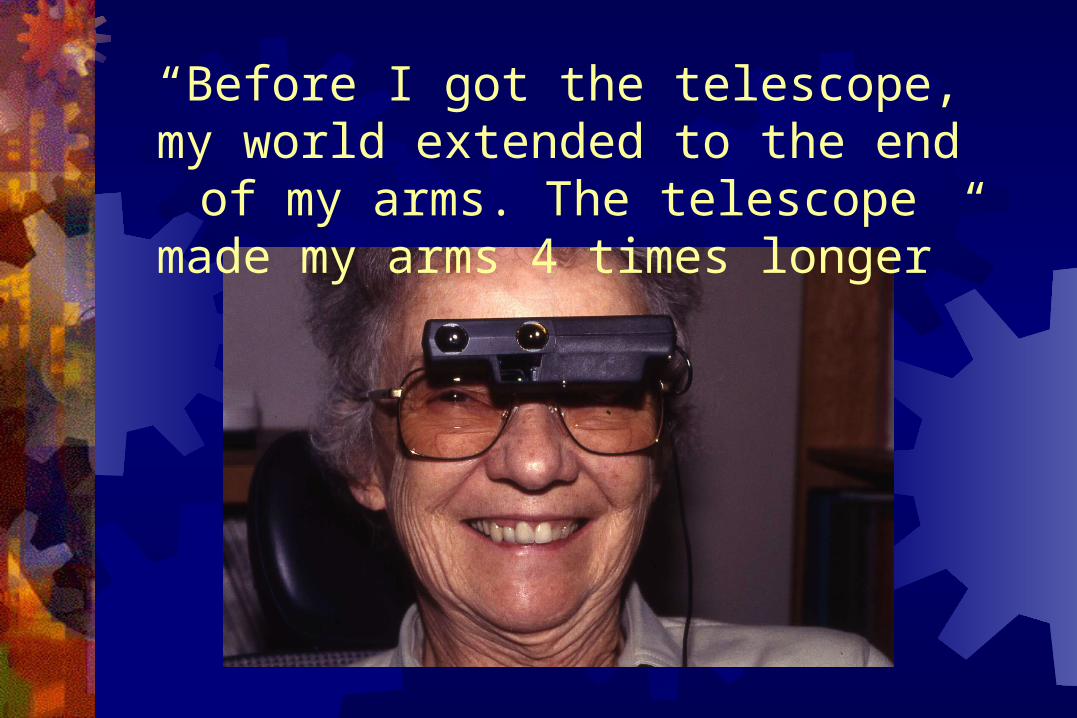
“Before I got the telescope, my world extended to the end of my arms. The
telescope made my arms 4 times longer”
“Visual Radius”Derived from Proximal Magnification
Moving closer makes the retinal image larger
The furthest distance at which one can discern facial features
Under normal illumination
Visual Acuity Correlate 2 feet = 20/200 1 foot = 20/400
The Telescope “Face” Test
A good response to high contrast targets is not prognostic
The face is a convenient low contrast target Seeing a face well through a TS at 8-10 feet is
prognostic of magnification response Poor response associated with edematous maculas
“Visual Radius” and “Social Range” “Social Range”- 3 to 15 feetExpand the “Visual Radius” sufficiently into
the “Social Range”Telescopes extend the visual radius by the
power of the deviceWith a 4x telescope:
2 feet becomes 8 feet 6 inches becomes 24 inches
TS Prescribing Paradigm Summary Identify the furthest distance that a face can be
seen- “Visual Radius” Confirm a favorable response to telescope
magnification- “Face Test” Extend the “Visual Radius” into the “Social Range” Establish realistic goals and expectations
Magnification is not natural.
Constraints of Magnification Working Distance Shallow Dept of Field Narrow Field of View
Constraints on the patient Unnatural working distances Disorientation Inconvenience Fatigue
What are bioptics? Eyeglasses with a miniature built-in telescope Allow use of normal and magnified vision by simply
tilting the head- like “upside down bifocals” Do not interfere with walking Help you see things further away:
Spotting- like the use of rear and side view mirrors Continuous tasks- TV, computer
Best for midrange and beyond Not ideal for reading
Basic Optical Concepts
Galilean vs. Keplerian Larger objective lens:
Brighter image Shallower depth of field
Larger, multi-element eyepiece: wider FOV
Longer eye-relief: Narrower FOV
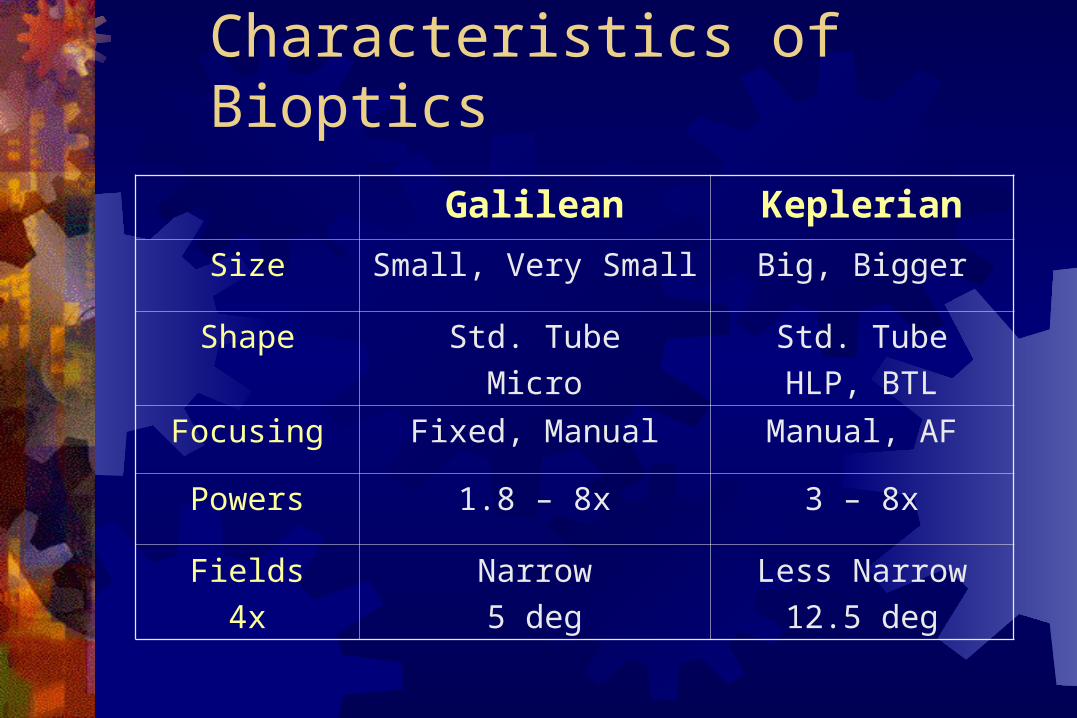
Characteristics of Bioptics
Galilean Keplerian
Size Small, Very Small Big, Bigger
Shape Std. Tube
Micro
Std. Tube
HLP, BTL
Focusing Fixed, Manual Manual, AF
Powers 1.8 – 8x 3 – 8x
Fields
4x
Narrow
5 deg
Less Narrow
12.5 deg
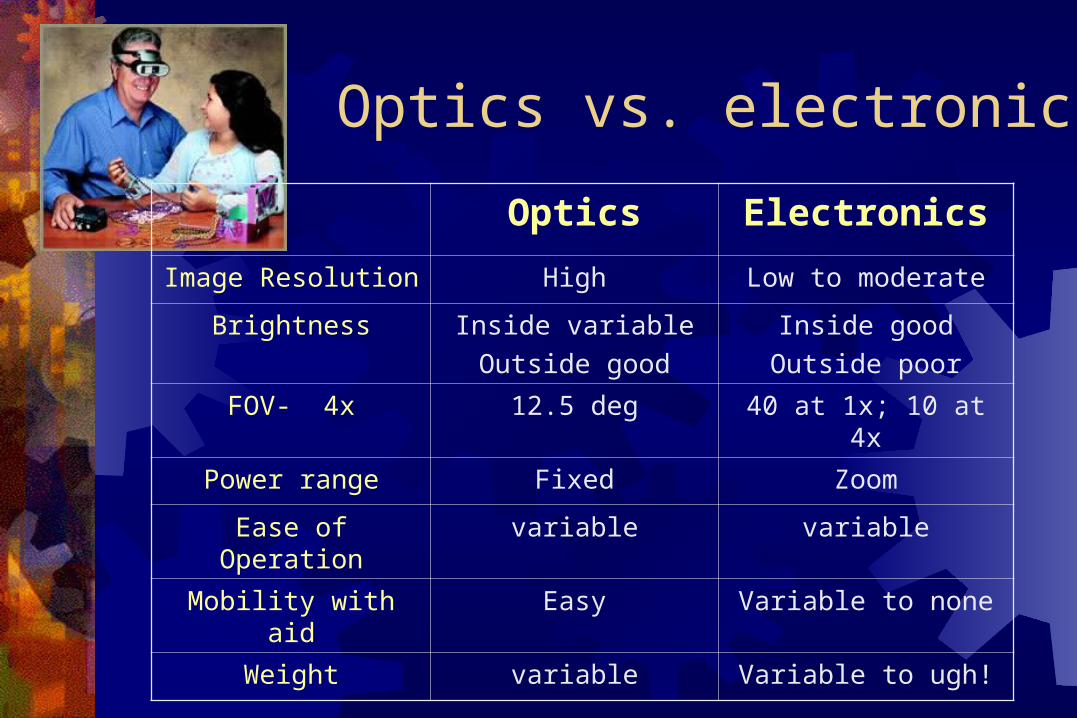
Optics vs. electronics
Optics Electronics
Image Resolution High Low to moderate
Brightness Inside variable
Outside good
Inside good
Outside poor
FOV- 4x 12.5 deg 40 at 1x; 10 at 4x
Power range Fixed Zoom
Ease of Operation variable variable
Mobility with aid Easy Variable to none
Weight variable Variable to ugh!
How much power?
Enough magnification to achieve the goal Acuity demand:
Average ~20/40 goal High ~20/30 goal
Sporting events? More than 6x is tough to keep stable on the head More than 7x- time for binoculars
How much Field?
What is a degree? How much FOV is enough?
It’s never enough- minimum ~ 5 deg Use comparisons- TV; rear view mirror It gets more natural
Maximize for close distances Let the patient compare using handhelds
4x12 Keplerian vs. 3x Galilean
User issues regarding bioptics Low Vision Device Use Among Veterans
Watson, et.al., OVS, 74:5, May 1997 200 veterans, 740 devices, 130 spectacle TS
Issues: Wider FOV- 83% Autofocus- 79% More power- 78% Brighter image- 49% Less noticeable 16%
When to AF and when to not…
Acuity between 20/70 and 20/200 Room and mid-range activities
Not for >20’
Dexterity issues Tremors, Paresis
Application issues Hands-free activities
Courtesy CNN
Which eye? Or both?
Prescribe for the dominant eye if at all possible Suppression difficulties significantly undermine acceptance
Binocular systems- Challenging to keep aligned- Very stiff frame, Beecher Wider FOV, Acuity and CST summation, no suppression issues,
lessens impact of scotomas Binocular Working distance fixed
Monocular is easier
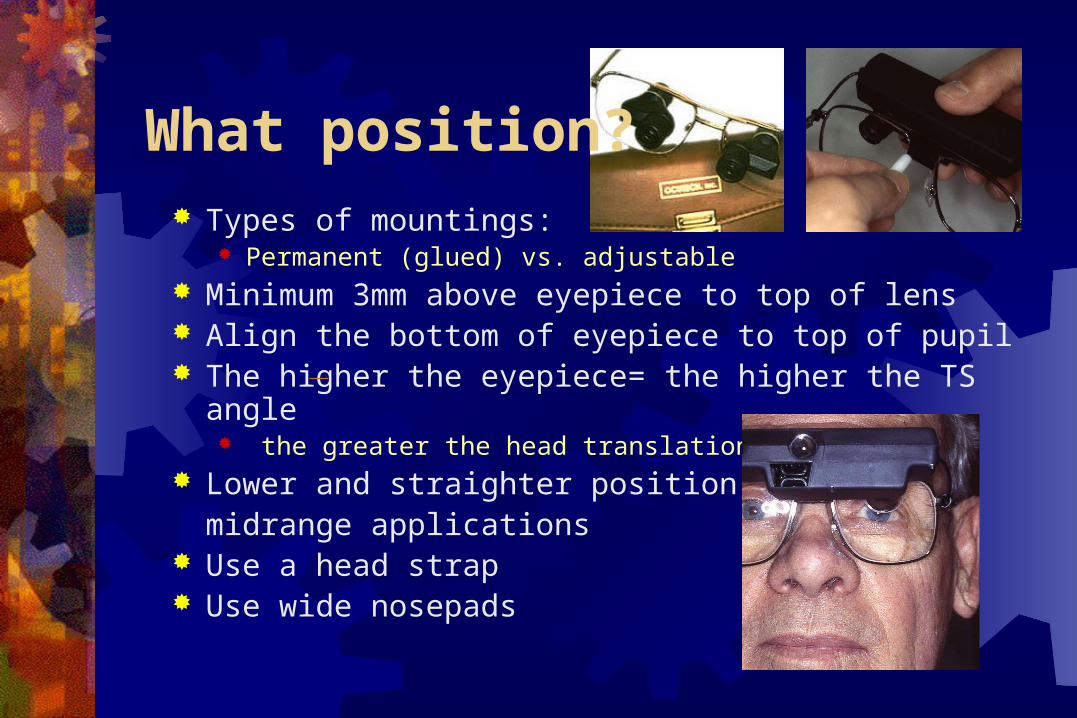
What position? Types of mountings:
Permanent (glued) vs. adjustable Minimum 3mm above eyepiece to top of lens Align the bottom of eyepiece to top of pupil The higher the eyepiece= the higher the TS angle
the greater the head translation Lower and straighter position for
midrange applications Use a head strap Use wide nosepads
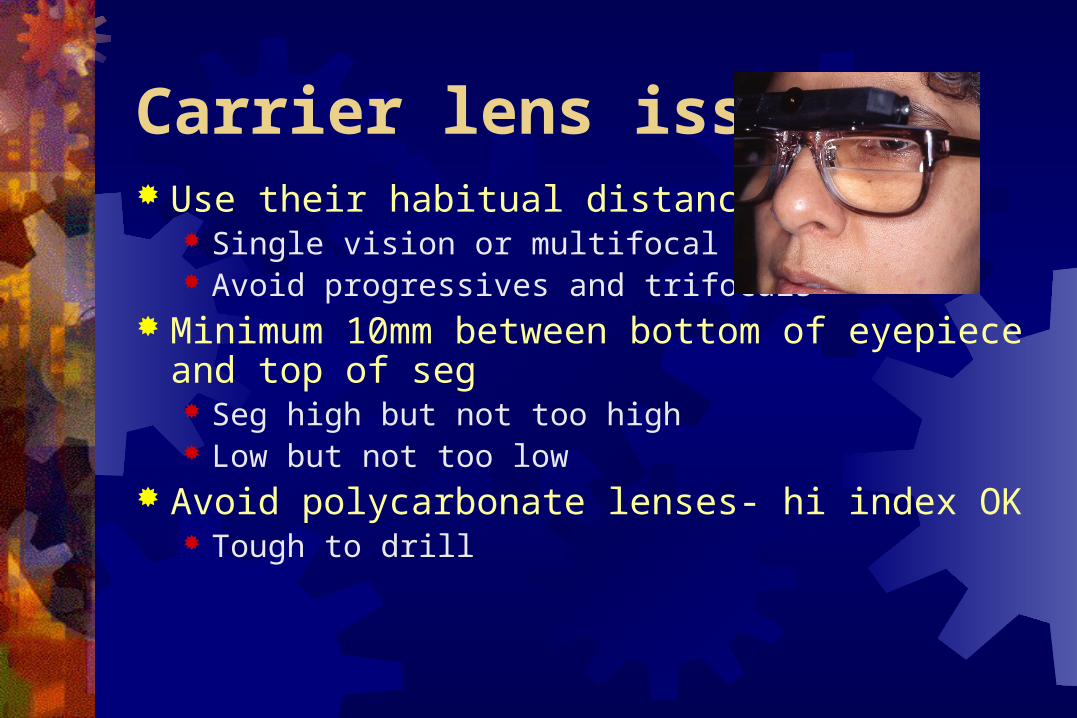
Carrier lens issues Use their habitual distance Rx
Single vision or multifocal Avoid progressives and trifocals
Minimum 10mm between bottom of eyepiece and top of seg Seg high but not too high Low but not too low
Avoid polycarbonate lenses- hi index OK Tough to drill
Qualify the PatientNot all patients are bioptic candidates
Establish a prognosis for likely success The Clinical Evaluation
Address Finances and Appearance This is not cheap-- “Is it worth it to you?” “It looks a little unusual-- will you wear it?”
You’ll have to learn to use it Are you prepared to make the effort?
Qualify the patient:Establish a telescope prognosis Hard Signs
1. VA between 20/70 and 20/300 (faces >2 feet)VA gain with 4x TS? Fluency
2. Response to low contrast targetFaces at 10 feet through 4x12 TS
3. Better eye is dominant Soft Signs
1. Appropriate goals: mid-range and beyond2. Motivation: appearance, enthusiasm3. Dexterity
Test and demonstrate with Handheld Telescopes first
Handheld 4x12- prefocus! Determine the dominant eye
Which eye do they take the TS to?
Evaluate response to faces at ~10 ft Poor response undermines prognosis
Needs brighter image
Show: Narrow FOV- challenges in finding the target Shallow DOF- challenges in keeping clear Need to refocus- challenges in doing the activity
Demonstrate Bioptics next
Get them out of the exam chair Present the concept of the “Magnification Factor”
With a 4x TS- What you see at 2’, you’ll see it at 8’
Realistic experiences= realistic expectations The “Eye Chart” is NOT the “real world” “Grocery Store,” CRT, Pictures on walls Sit in the “living room” (Waiting room) Outside- signs, flowers, faces
Use your assistant Have family accompany
Recruiting the Patient
“We can teach them to ride the bike,
but they have to do the pedaling.” The patient’s job:
To want to improve their vision To make the effort to learn to use it To be frustrated To invest time and $
Training Techniques Sighting through eyepiece
Give them a tour of the device Translation
Switching between carrier and eyepiece Localization
Aiming and Switching Tracking
Moving targets Near localization and hand-eye coordination
Finding the target