Embed Size (px)
Citation preview
PRESCRIBING FOR THE
PSA AND FINALS
DR FRANCESCA BONORA
WHAT WE WILL COVER
• HOW TO PREPARE FOR THE PSA EXAM
• HOW SCENARIOS APPLY TO PRESCRIBING FOR FINALS
THE PSA EXAM
For full details of what could be asked:
prescribingsafetyassessment.ac.uk/aboutpsa
Click on PSA blueprint for November 2017 PDF
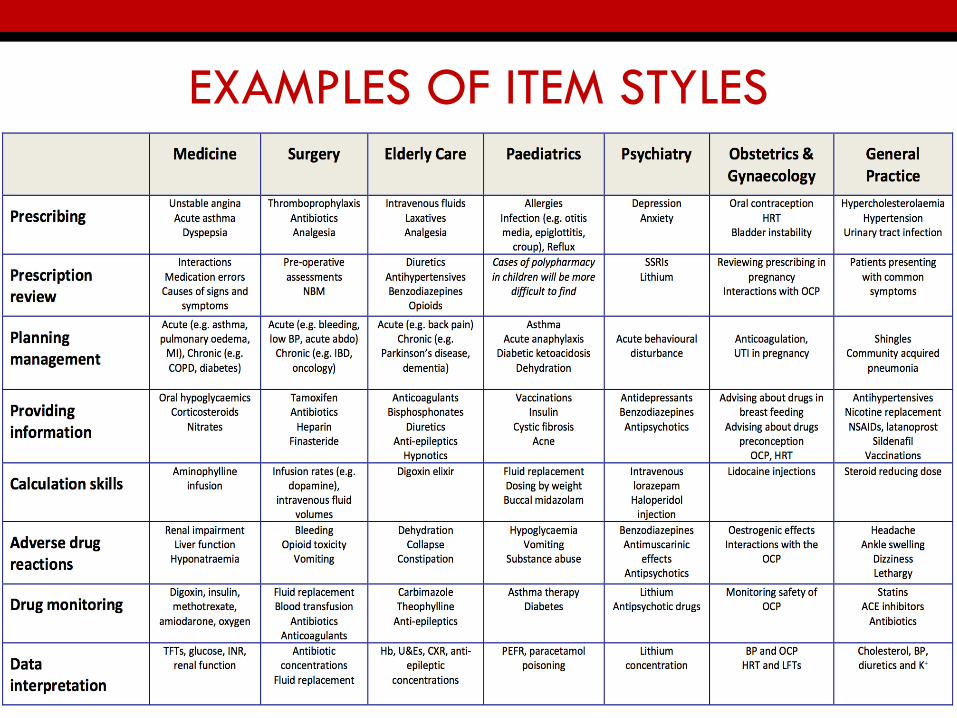
EXAMPLES OF ITEM STYLES
SECTION 1 – PRESCRIBING
• Decide on the most appropriate prescription (drug,
dose, route and frequency), based on the clinical
circumstances
• Write a safe, effective and legal prescription
• 8 questions worth 10 marks each
• Make sure you sign the prescriptions with
your full surname (not initials) – don’t lose
the easy marks
HOW TO PREPARE
• Exam is time pressured, so LEARN TREATMENT
ALGORITHMS:
• Acute conditions eg acute asthma attack, acute heart
failure
• Chronic conditions e.g. depression, reflux oesophagitis
• Presenting symptoms e.g. pain
• Find these in the back of the Oxford handbook
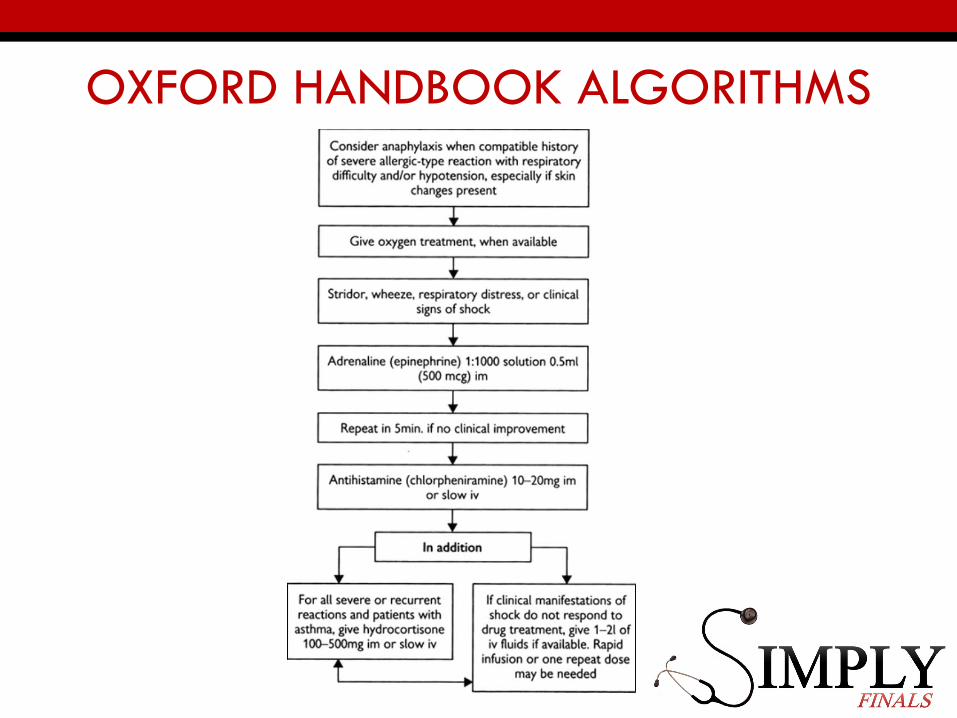
OXFORD HANDBOOK ALGORITHMS
THIS BOOK IS GREAT
PASS THE PSA, 1E, FEB 2014,
BY WILL BROWN BSC MBBS MRCP(UK) FHEA AND KEVIN W LOUDON
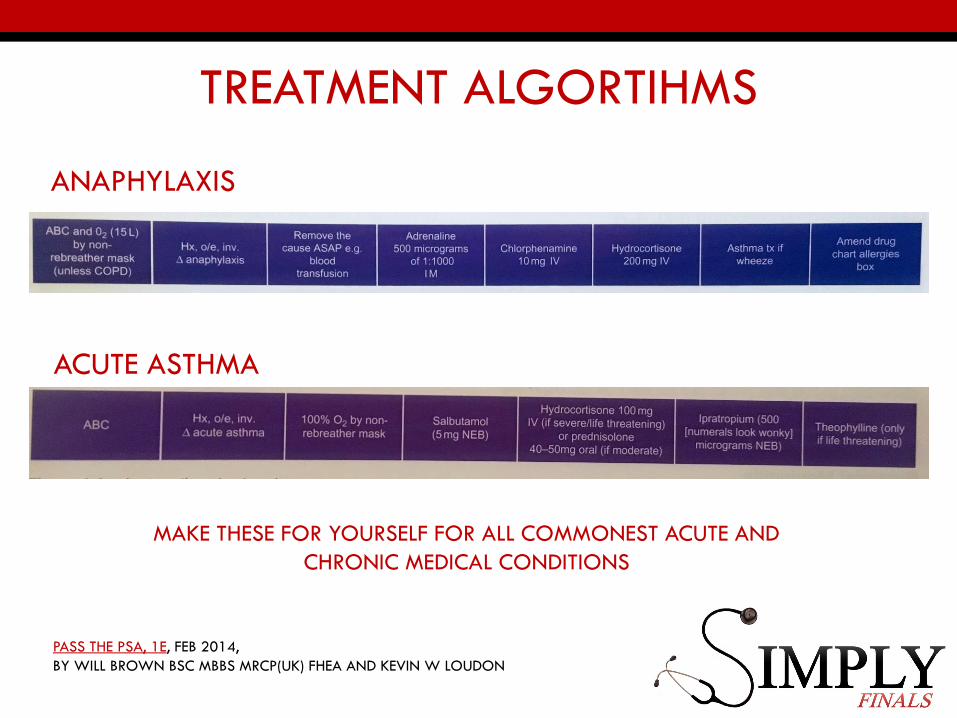
TREATMENT ALGORTIHMS
ANAPHYLAXIS
ACUTE ASTHMA
MAKE THESE FOR YOURSELF FOR ALL COMMONEST ACUTE AND
CHRONIC MEDICAL CONDITIONS
PASS THE PSA, 1E, FEB 2014,
BY WILL BROWN BSC MBBS MRCP(UK) FHEA AND KEVIN W LOUDON
HOW TO PREPARE
• If you can’t remember – use treatment summaries in the
online BNF during the exam
• CTRL + F is your best friend!
BNF TREATMENT SUMMARIES
CTRL + F
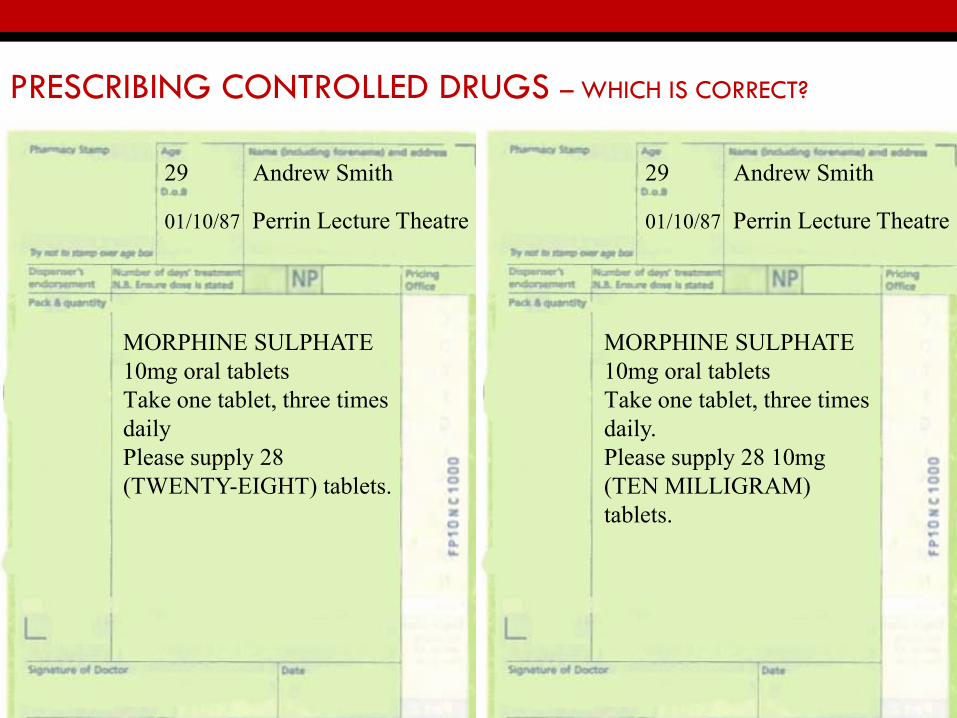
PRESCRIBING CONTROLLED DRUGS – WHICH IS CORRECT?
MORPHINE SULPHATE 10mg oral tabletsTake one tablet, three times dailyPlease supply 28 (TWENTY-EIGHT) tablets.
MORPHINE SULPHATE 10mg oral tabletsTake one tablet, three times daily.Please supply 28 10mg(TEN MILLIGRAM) tablets.
29 Andrew Smith
01/10/87 Perrin Lecture Theatre
29 Andrew Smith
01/10/87 Perrin Lecture Theatre
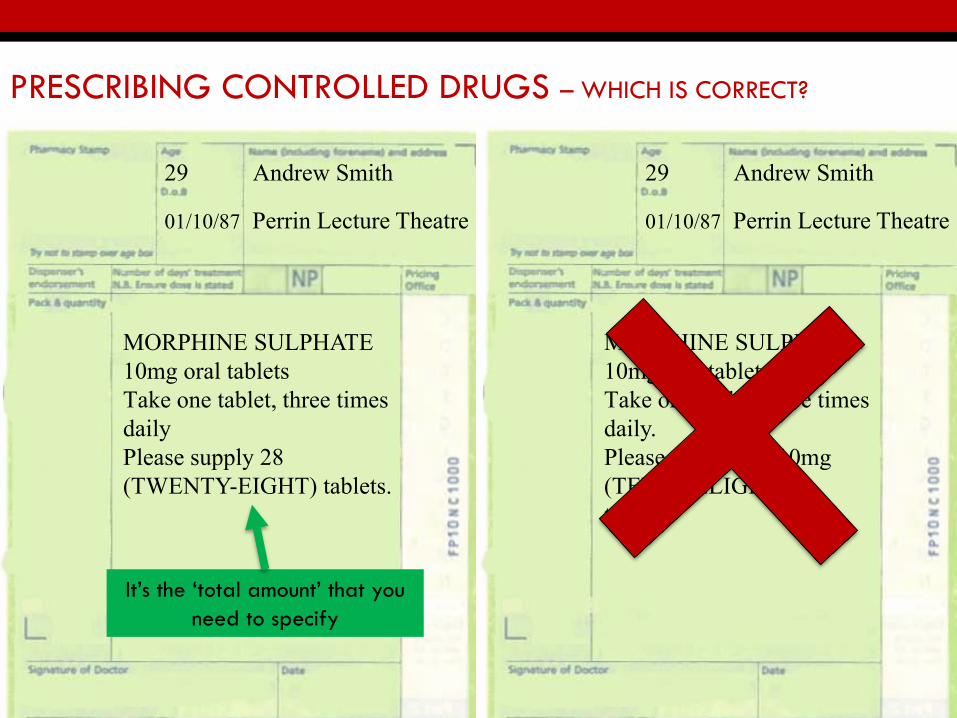
PRESCRIBING CONTROLLED DRUGS – WHICH IS CORRECT?
MORPHINE SULPHATE 10mg oral tabletsTake one tablet, three times dailyPlease supply 28 (TWENTY-EIGHT) tablets.
MORPHINE SULPHATE 10mg oral tabletsTake one tablet, three times daily.Please supply 28 10mg (TEN MILLIGRAM) tablets.
It’s the ‘total amount’ that you
need to specify
29 Andrew Smith
01/10/87 Perrin Lecture Theatre
29 Andrew Smith
01/10/87 Perrin Lecture Theatre
PRESCRIBING CONTROLLED DRUGS
• Include the name and address of the patient.
• State the name and strength of the drug
• State the dose and frequency
• TOTAL AMOUNT must be written in WORDS AND FIGURES
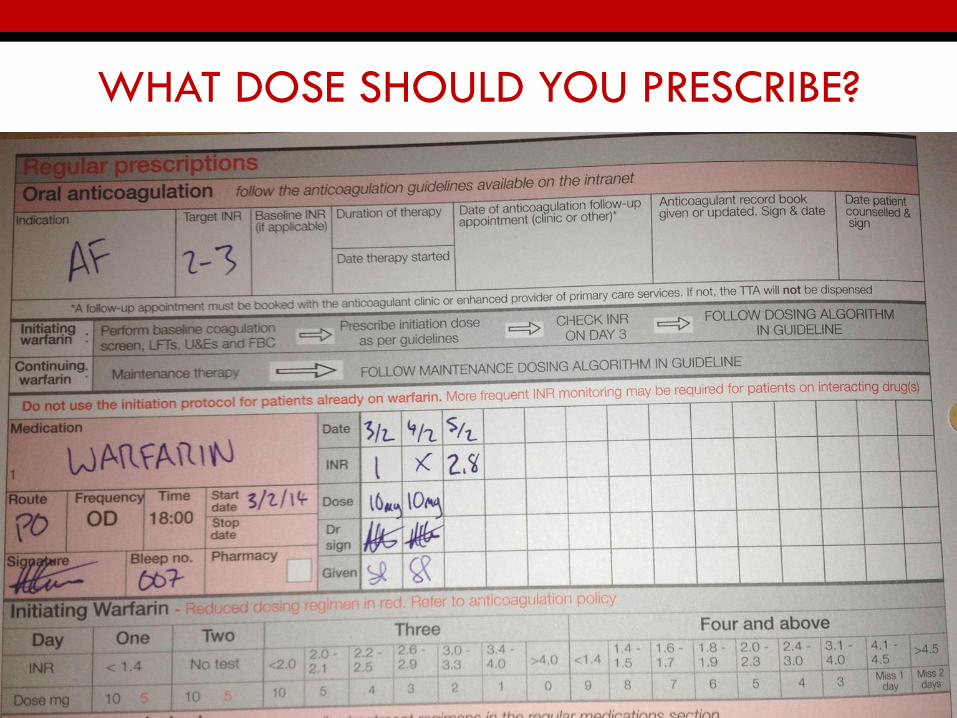
WHAT DOSE SHOULD YOU PRESCRIBE?
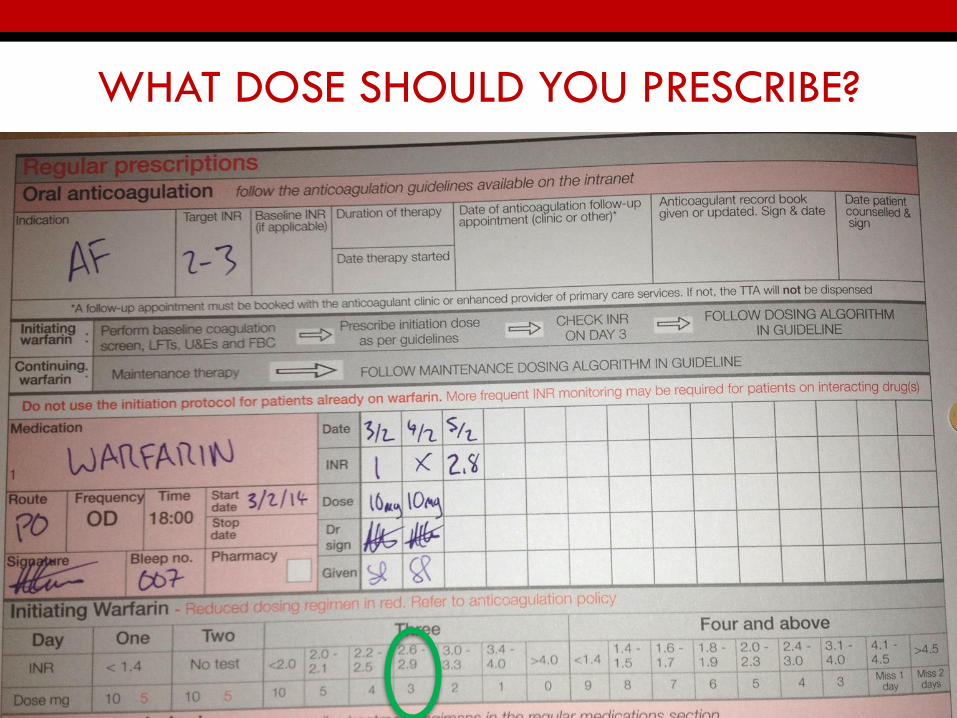
WHAT DOSE SHOULD YOU PRESCRIBE?
SECTION 2 – PRESCRIPTION REVIEW
• Identify prescriptions (drugs, doses or routes) that are
inappropriate, unsafe or ineffective from amongst the
current list of prescribed medicines
• 8 items worth 4 marks each
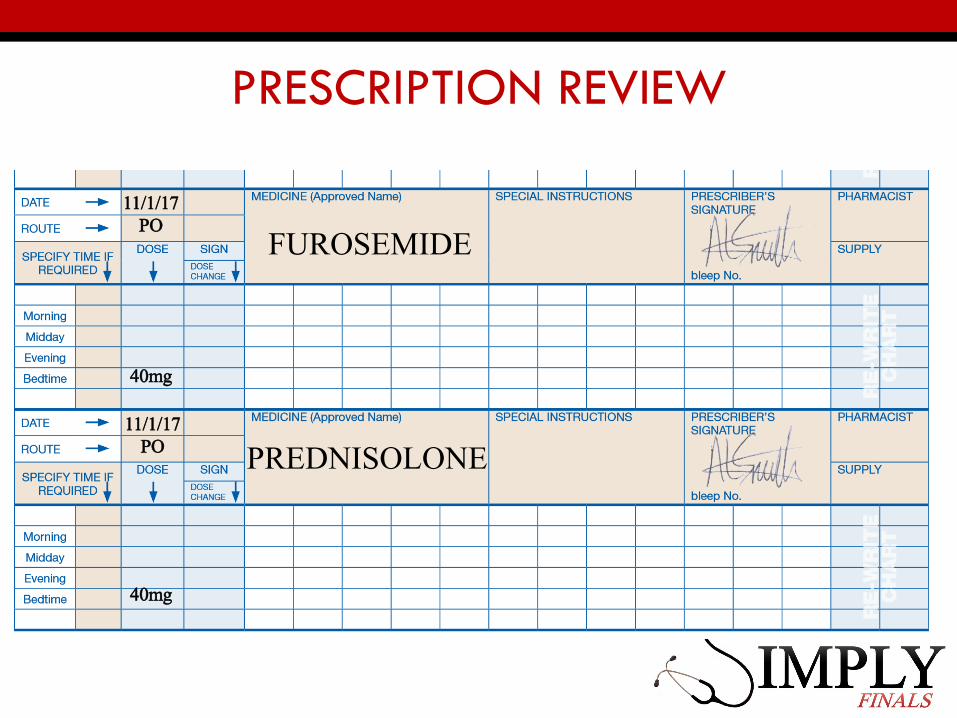
PRESCRIPTION REVIEW
FUROSEMIDE
PREDNISOLONE11/1/17
PO
11/1/17PO
40mg
40mg
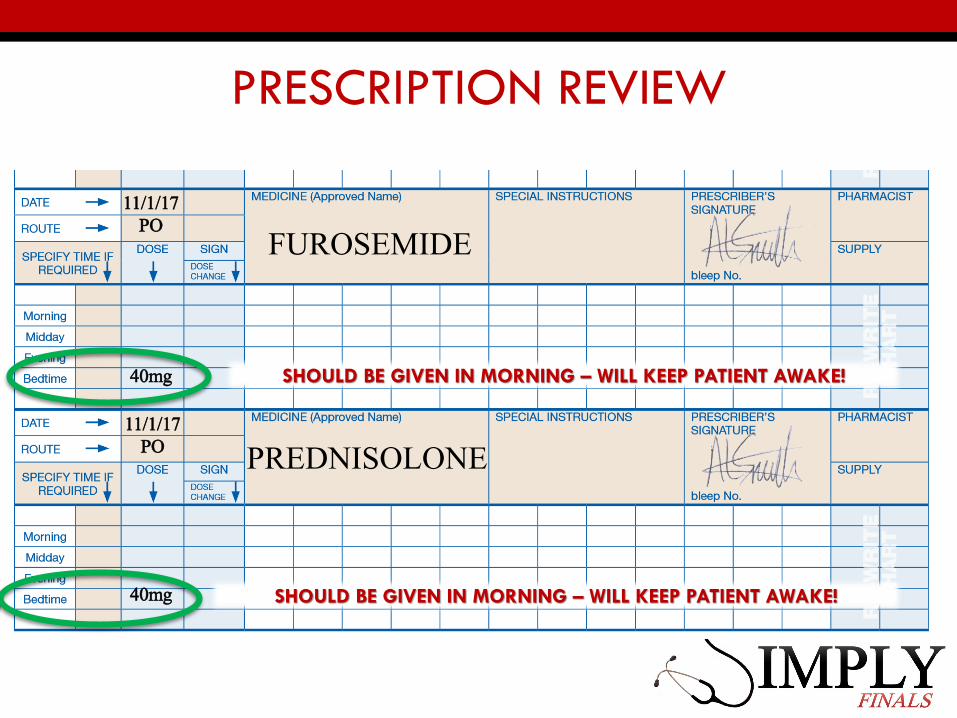
PRESCRIPTION REVIEW
FUROSEMIDE
PREDNISOLONE11/1/17
PO
11/1/17PO
40mg
40mg
SHOULD BE GIVEN IN MORNING – WILL KEEP PATIENT AWAKE!
SHOULD BE GIVEN IN MORNING – WILL KEEP PATIENT AWAKE!
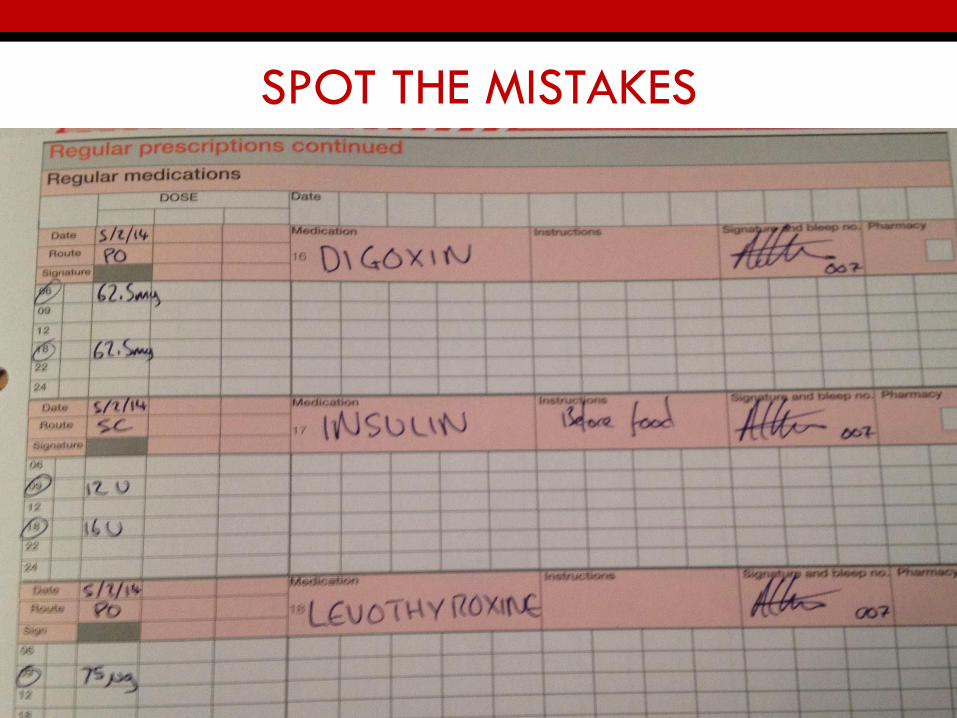
SPOT THE MISTAKES
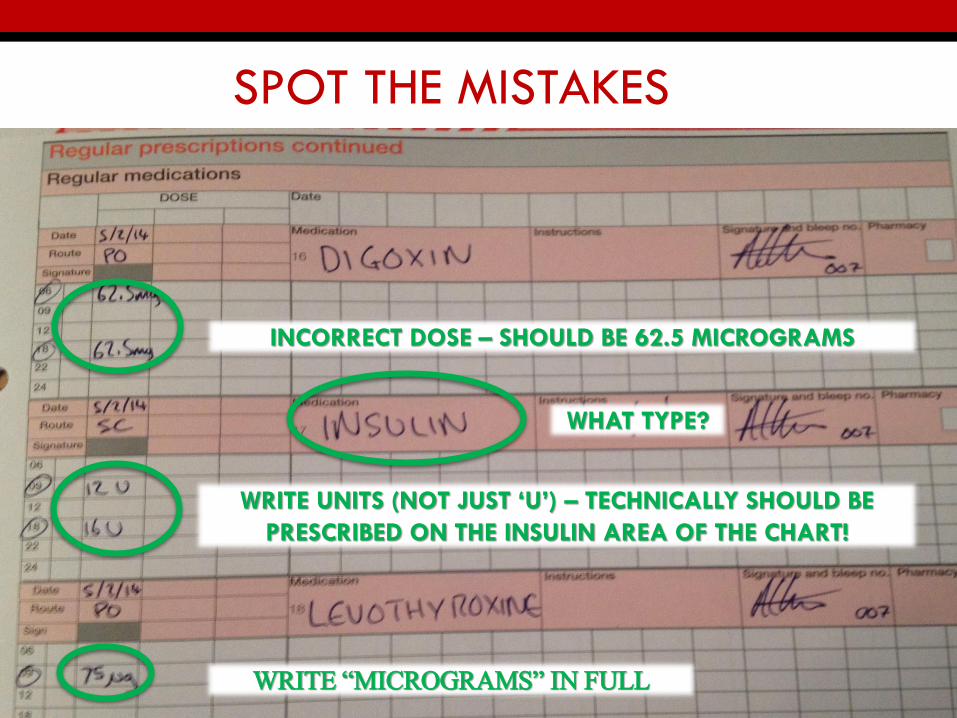
SPOT THE MISTAKES
INCORRECT DOSE – SHOULD BE 62.5 MICROGRAMS
WRITE UNITS (NOT JUST ‘U’) – TECHNICALLY SHOULD BE
PRESCRIBED ON THE INSULIN AREA OF THE CHART!
WRITE “MICROGRAMS” IN FULL
WHAT TYPE?
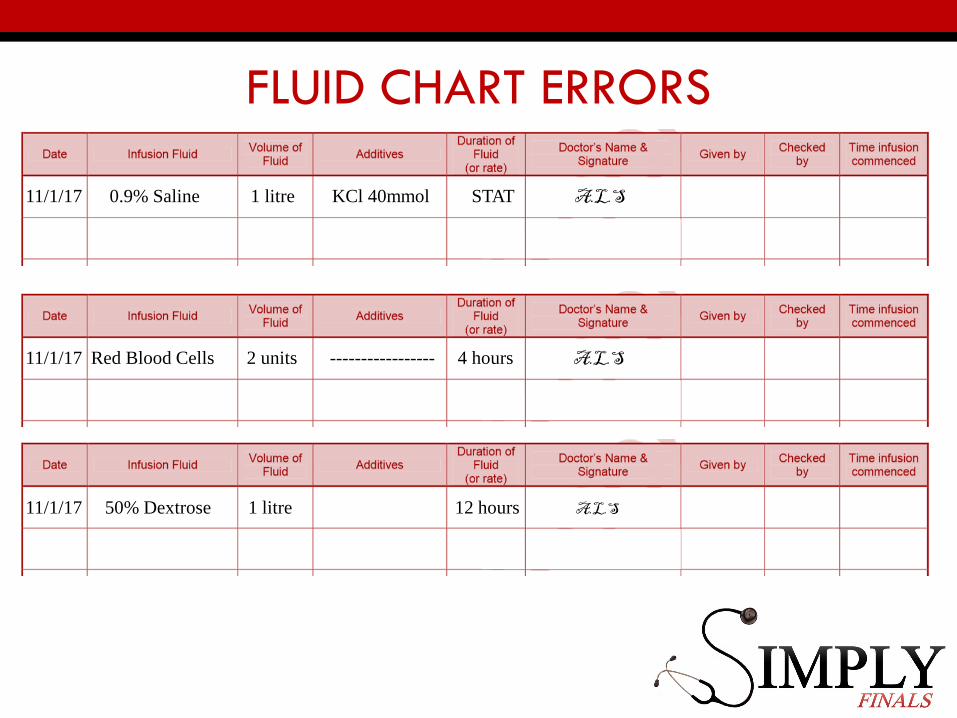
FLUID CHART ERRORS
11/1/17 0.9% Saline 1 litre KCl 40mmol STAT A.L.S
11/1/17 Red Blood Cells 2 units ----------------- 4 hours A.L.S
11/1/17 50% Dextrose 1 litre 12 hours A.L.S
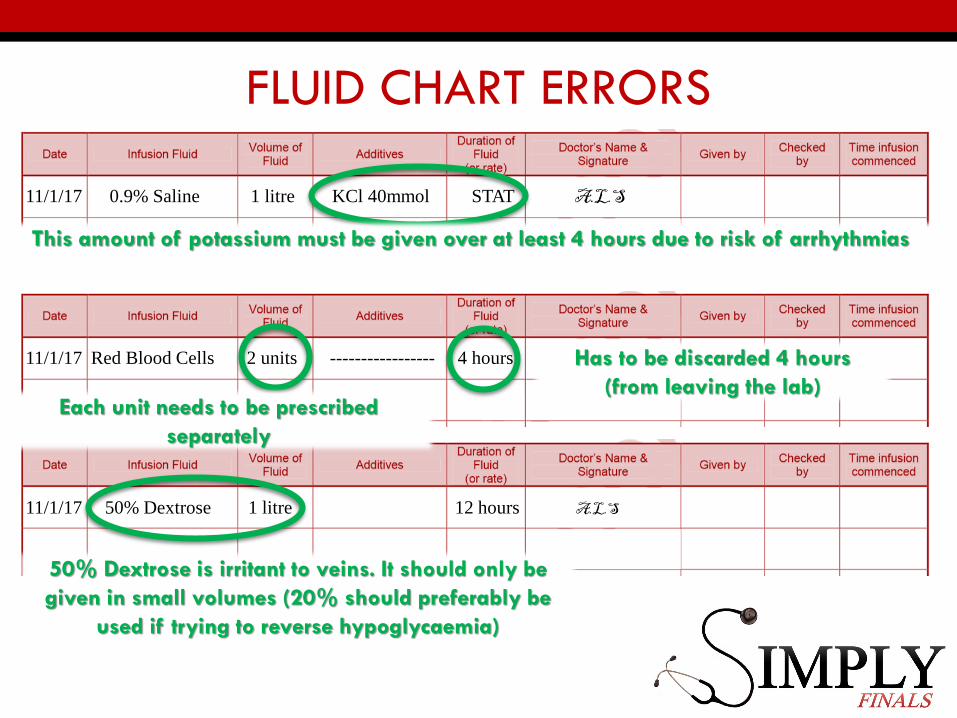
FLUID CHART ERRORS
11/1/17 0.9% Saline 1 litre KCl 40mmol STAT A.L.S
11/1/17 Red Blood Cells 2 units ----------------- 4 hours A.L.S
11/1/17 50% Dextrose 1 litre 12 hours A.L.S
This amount of potassium must be given over at least 4 hours due to risk of arrhythmias
Each unit needs to be prescribed
separately
Has to be discarded 4 hours
(from leaving the lab)
50% Dextrose is irritant to veins. It should only be
given in small volumes (20% should preferably be
used if trying to reverse hypoglycaemia)
SECTION 3 – PLANNING MANAGEMENT
• Deciding which treatment would be most appropriate to
manage a particular clinical situation
• 8 items worth 2 marks each
• Choose most appropriate treatment from list of 5
COMMON ACUTE CONDITIONS
KNOW THE TREATMENT ALGORITHMS FOR:
• STEMI
• NSTEMI
• ACUTE LEFT VENTRICULAR FAILURE
• TACHYCARDIA WITH PULSE
• ANAPHYLAXIS
• ACUTE ASTHMA EXACERBATION
• PNEUMONIA
• PE
• GI BLEED
• BACTERIAL MENINGITIS
• SEIZURE
• STATUS EPILEPTICUS
• STROKE
• HYPERGLYCEMIA
• DKA AND HHS
• AKI
• POISONING
COMMON CHRONIC CONDITIONS
KNOW THE TREATMENT ALGORITHMS FOR:
• HYPERTENSION • CHRONIC HEART FAILURE • STROKE PREVENTION
• STABLE ANGINA • CHRONIC ASTHMA • COPD• DIABETES • INSOMNIA • CONSTIPATION• DIARRHOEA • PAIN
SECTION 4 – PROVIDING INFORMATION
• Decide the most important piece of information that
should be provided to patients to allow them to choose
whether to take the medicine and to enhance its safety
and effectiveness
• Six items worth 2 marks
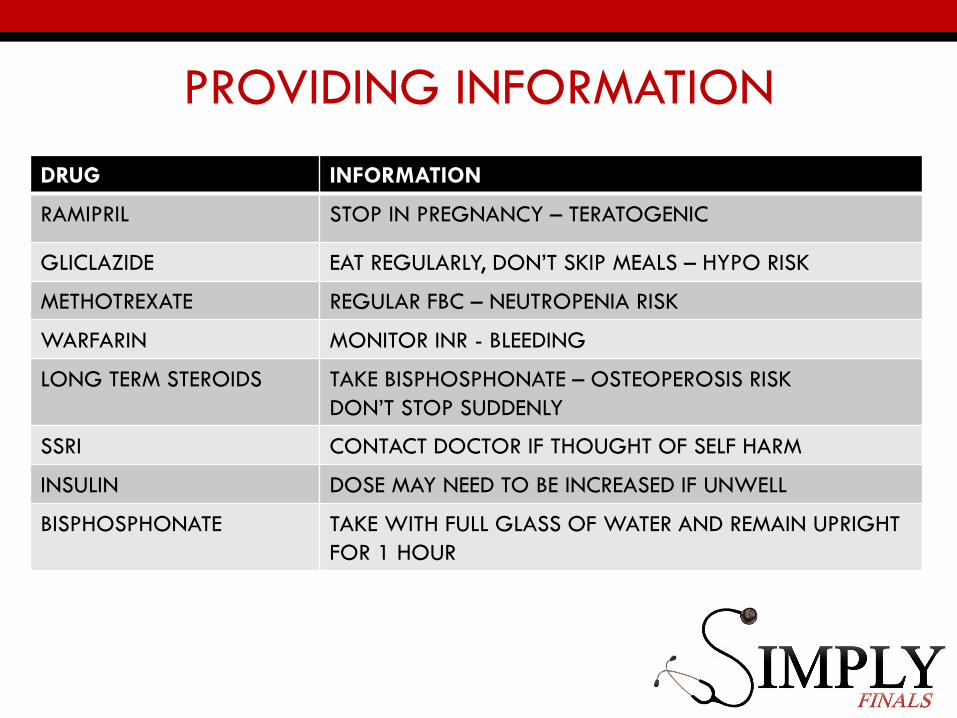
PROVIDING INFORMATION
DRUG INFORMATION
RAMIPRIL STOP IN PREGNANCY – TERATOGENIC
GLICLAZIDE EAT REGULARLY, DON’T SKIP MEALS – HYPO RISK
METHOTREXATE REGULAR FBC – NEUTROPENIA RISK
WARFARIN MONITOR INR - BLEEDING
LONG TERM STEROIDS TAKE BISPHOSPHONATE – OSTEOPEROSIS RISK
DON’T STOP SUDDENLY
SSRI CONTACT DOCTOR IF THOUGHT OF SELF HARM
INSULIN DOSE MAY NEED TO BE INCREASED IF UNWELL
BISPHOSPHONATE TAKE WITH FULL GLASS OF WATER AND REMAIN UPRIGHT
FOR 1 HOUR
SECTION 5 – CALCULATION SKILLS
• Making an accurate drug dosage calculation based on
numerical information
• Recording answer accurately with appropriate units of
measurement
• 8 items worth 2 marks
MAKE SURE YOU PRACTICE
• Correct number of tablets to achieve a required dose
• Making necessary dose adjustments based on weight or
body surface area
• Diluting a drug for administration in an infusion pump
DRUG RATIOS
1% means
• 1g in 100ml or 10mg in 1ml for weight/volume (w/v)
calculations
• 1g in 100g for weight/weight calculations
ADRENALINE RATIOS
• ANAPHYLAXIS
• 0.5mg = 0.5ml of 1 in 1,000 IM
• Remember 1 in 1,000 means: 1g in 1000 ml or 1000mg in 1000ml or 1ml in 1mg
• Therefore 0.5ml = 0.5mg
• CARDIAC ARREST
• 1mg = 10ml of 1 in 10,000 IV
• Remember 1 in 10,000 means: 1g in 10,000 ml or 1,000mg in 10,000ml or 1mg in 10ml
Dosage Calculations
Always convert to the same units and then:
D (What you want) x V (volume it is in) = Dose
H (What you’ve got)
Try some practice questions:http://www.drugs.smd.qmul.ac.uk/drugs/html5/Prescribing5/AN-781CE9AF-87B9-F0E4-01F9-205B0DCC08BA.html
https://www.abdn.ac.uk/medical/electives/elective_information/.../PSA_Tutorial.pdf
SECTION 6 – ADVERSE DRUG REACTIONS
• Likely adverse reactions to specific drugs, potentially
dangerous interactions, managing adverse effects of a
drug
• 8 items worth 2 marks each
ADVERSE DRUG REACTIONS
‘THE CTRL + F SECTION’
• Adverse effects caused by commonly prescribed drugs such as calcium channel blockers, beta2-agonists, non-steroidal anti-inflammatory drugs, aminoglycoside antibiotics, etc.
• Most likely drug to have caused adverse effect e.g. renal impairment, hepatic dysfunction, hypokalaemia, urinary retention, etc.
• Potential interactions between medicines e.g. warfarin-statins, NSAIDs-ACE inhibitors
• How to treat an adverse drug reaction e.g. acute anaphylaxis, excessive anticoagulation, drug-induced hypoglycaemia, diuretic-induced dehydration etc.
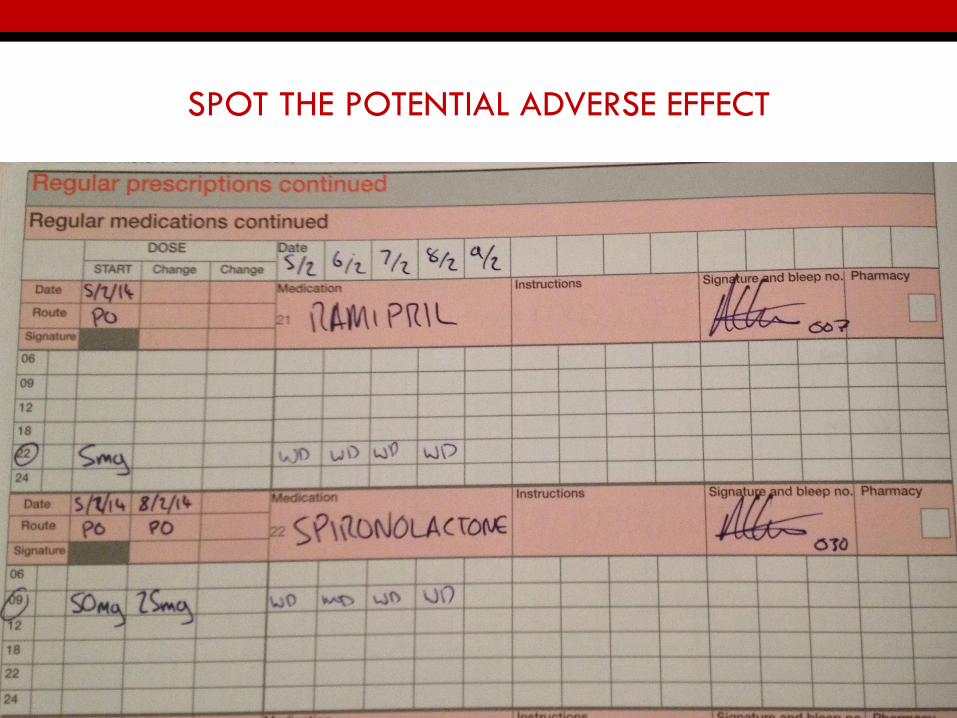
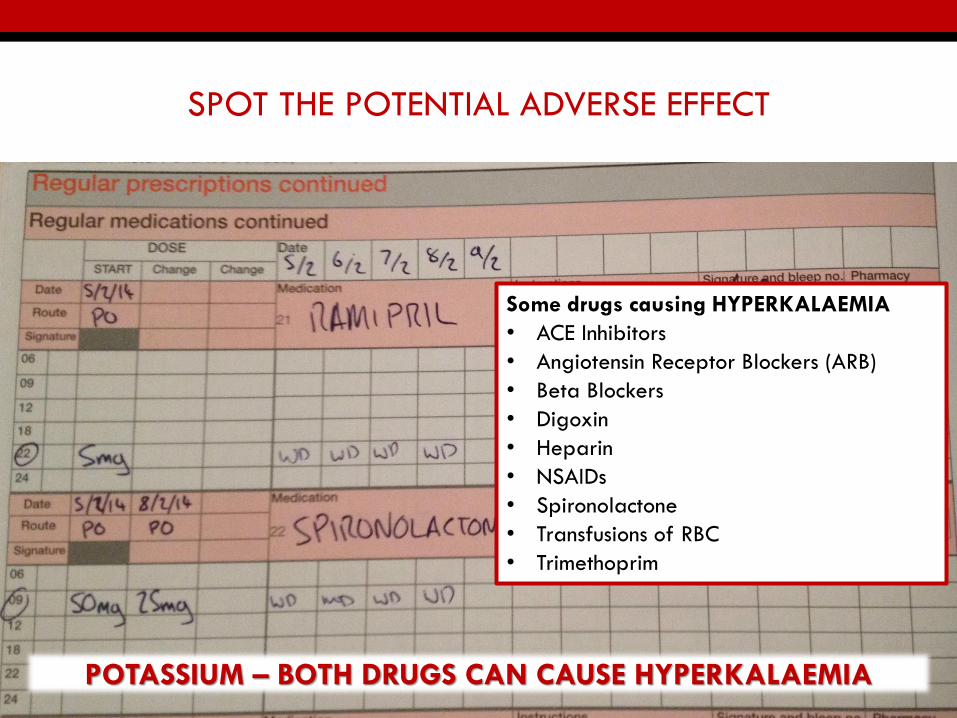
SPOT THE POTENTIAL ADVERSE EFFECT
SPOT THE POTENTIAL ADVERSE EFFECT
POTASSIUM – BOTH DRUGS CAN CAUSE HYPERKALAEMIA
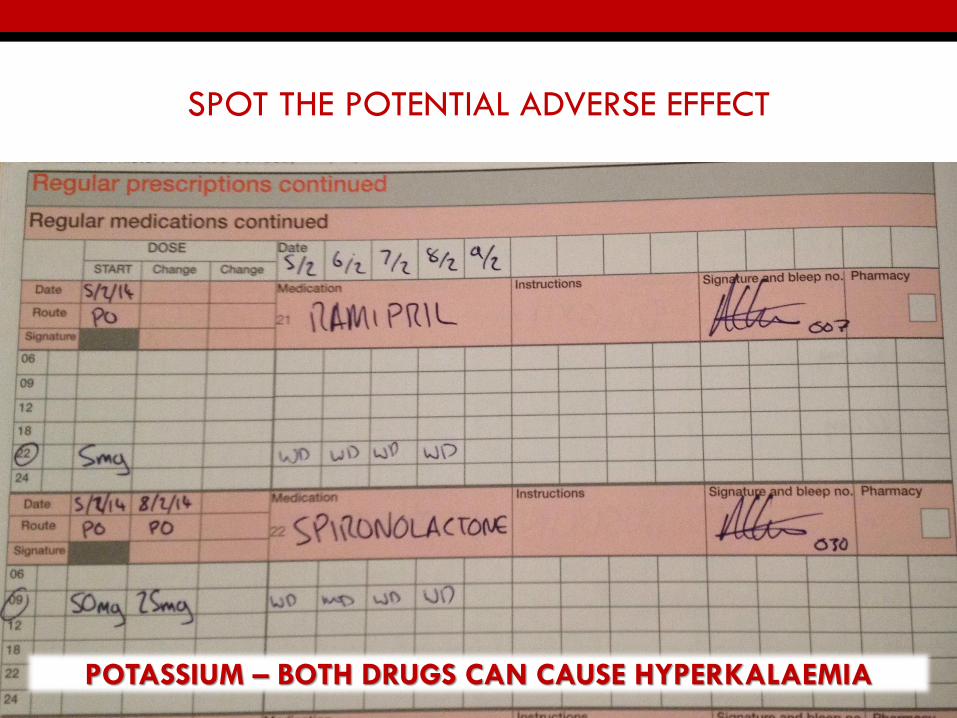
SPOT THE POTENTIAL ADVERSE EFFECT
POTASSIUM – BOTH DRUGS CAN CAUSE HYPERKALAEMIA
Some drugs causing HYPERKALAEMIA
• ACE Inhibitors
• Angiotensin Receptor Blockers (ARB)
• Beta Blockers
• Digoxin
• Heparin
• NSAIDs
• Spironolactone
• Transfusions of RBC
• Trimethoprim
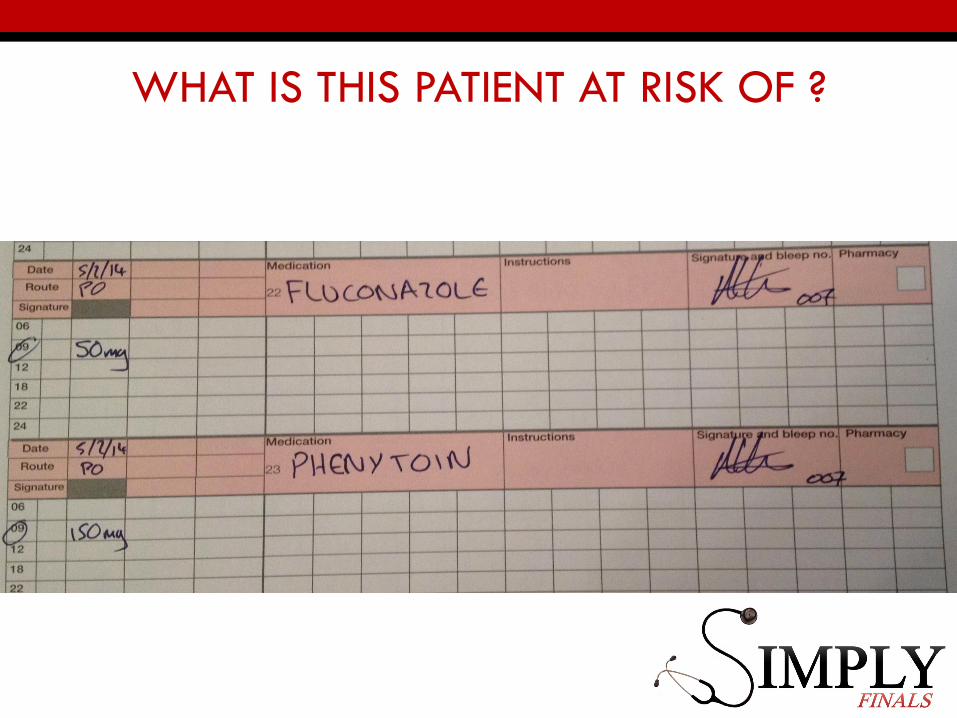
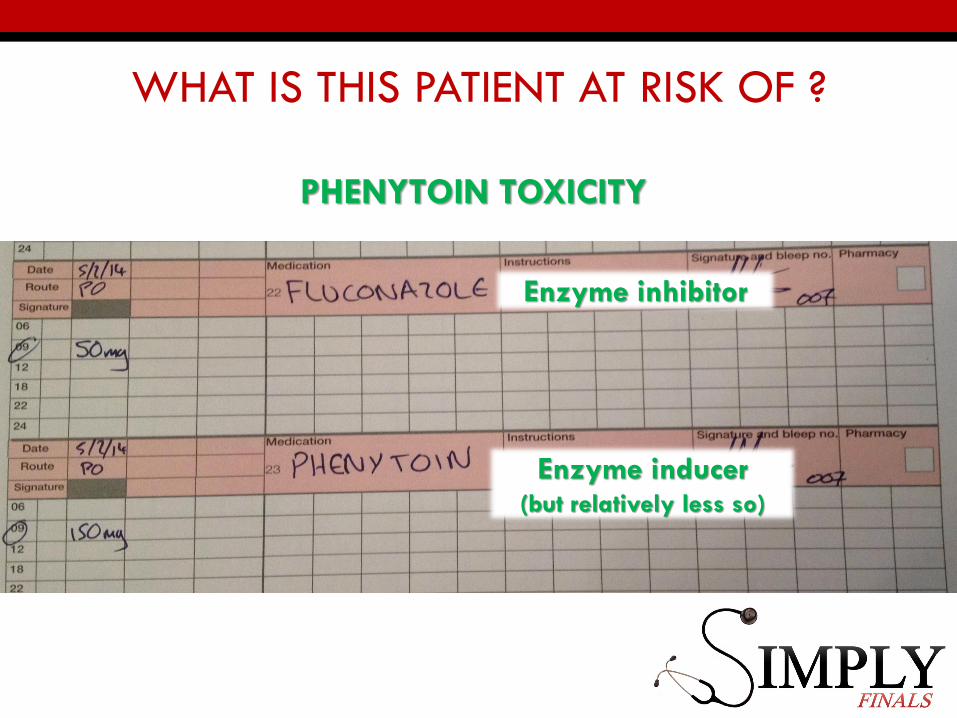
WHAT IS THIS PATIENT AT RISK OF ?
WHAT IS THIS PATIENT AT RISK OF ?
PHENYTOIN TOXICITY
Enzyme inhibitor
Enzyme inducer(but relatively less so)
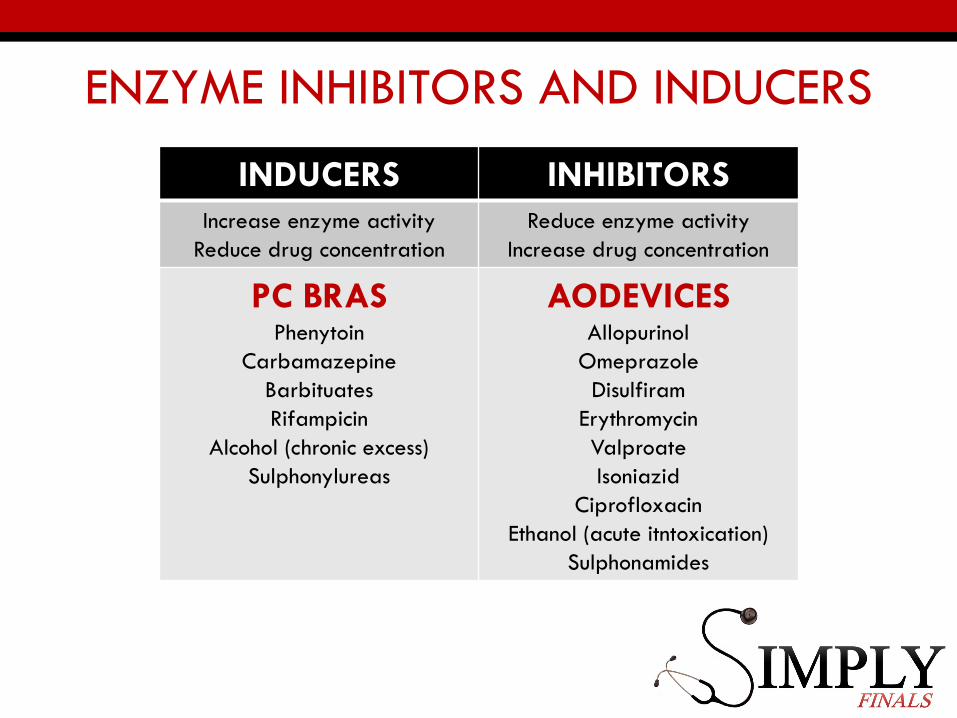
ENZYME INHIBITORS AND INDUCERS
INDUCERS INHIBITORS
Increase enzyme activity
Reduce drug concentration
Reduce enzyme activity
Increase drug concentration
PC BRASPhenytoin
Carbamazepine
Barbituates
Rifampicin
Alcohol (chronic excess)
Sulphonylureas
AODEVICESAllopurinol
Omeprazole
Disulfiram
Erythromycin
Valproate
Isoniazid
Ciprofloxacin
Ethanol (acute itntoxication)
Sulphonamides
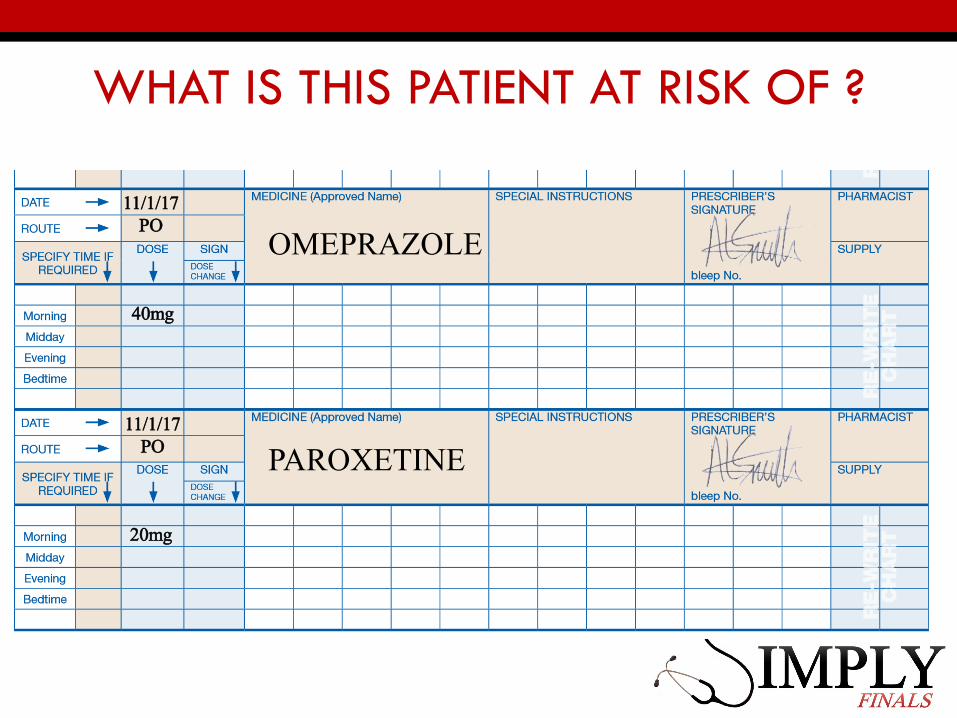
WHAT IS THIS PATIENT AT RISK OF ?
OMEPRAZOLE
PAROXETINE11/1/17
PO
11/1/17PO
20mg
40mg
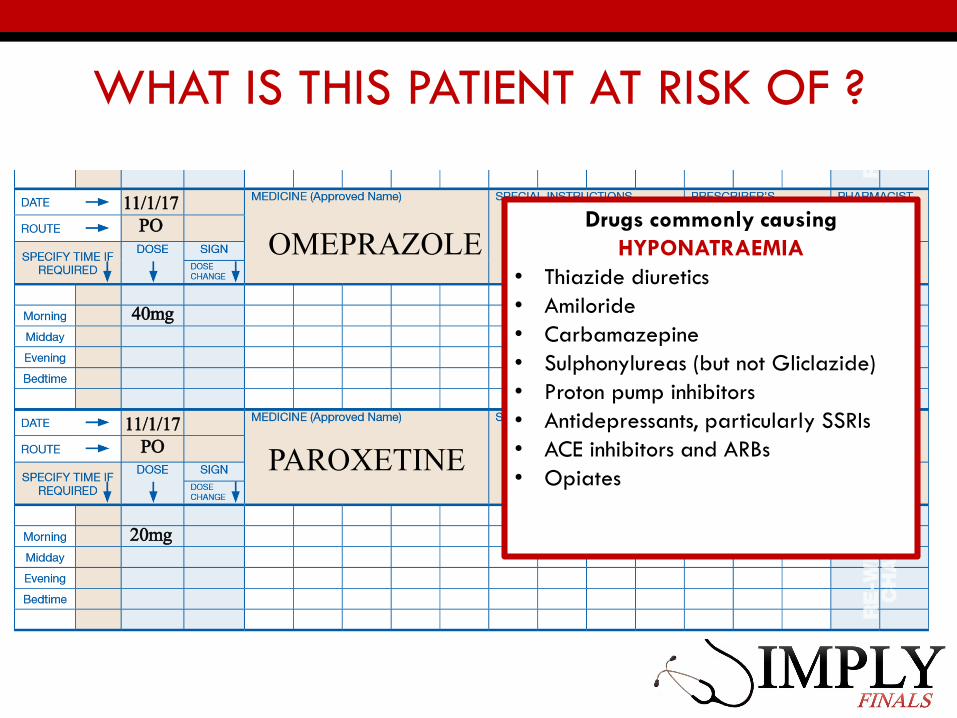
WHAT IS THIS PATIENT AT RISK OF ?
OMEPRAZOLE
PAROXETINE11/1/17
PO
11/1/17PO
20mg
40mg
Drugs commonly causing
HYPONATRAEMIA
• Thiazide diuretics
• Amiloride
• Carbamazepine
• Sulphonylureas (but not Gliclazide)
• Proton pump inhibitors
• Antidepressants, particularly SSRIs
• ACE inhibitors and ARBs
• Opiates
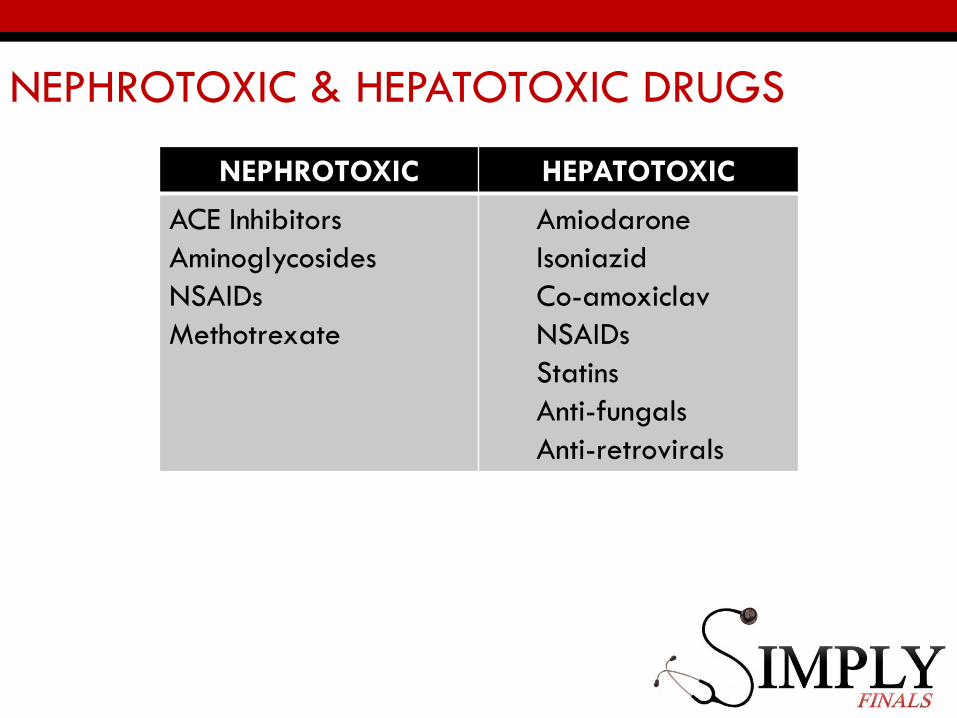
NEPHROTOXIC & HEPATOTOXIC DRUGS
NEPHROTOXIC HEPATOTOXIC
ACE Inhibitors
Aminoglycosides
NSAIDs
Methotrexate
Amiodarone
Isoniazid
Co-amoxiclav
NSAIDs
Statins
Anti-fungals
Anti-retrovirals
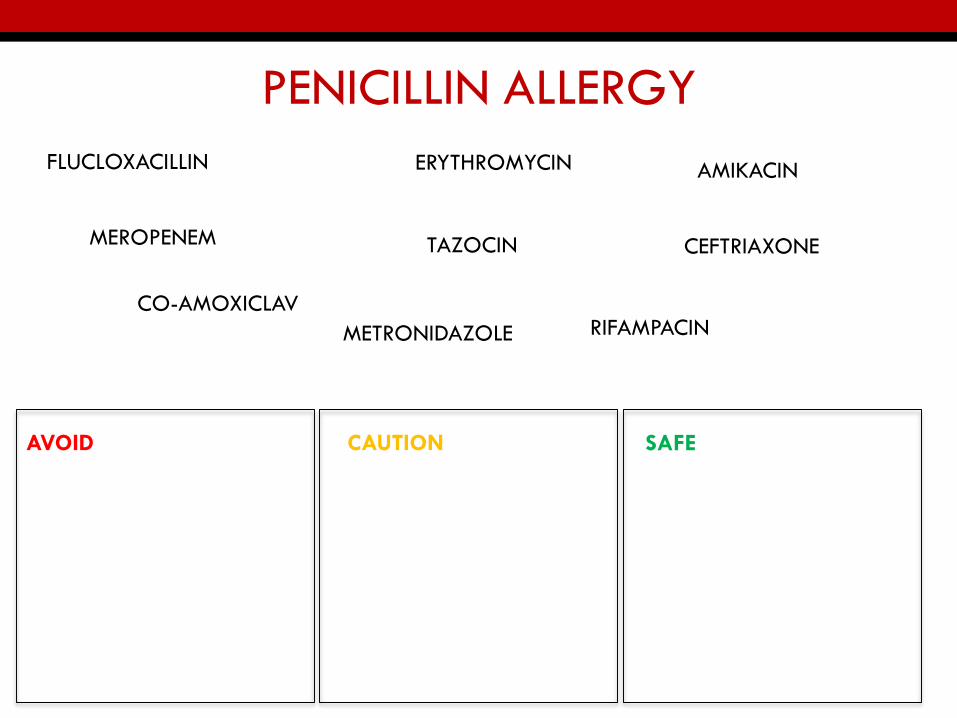
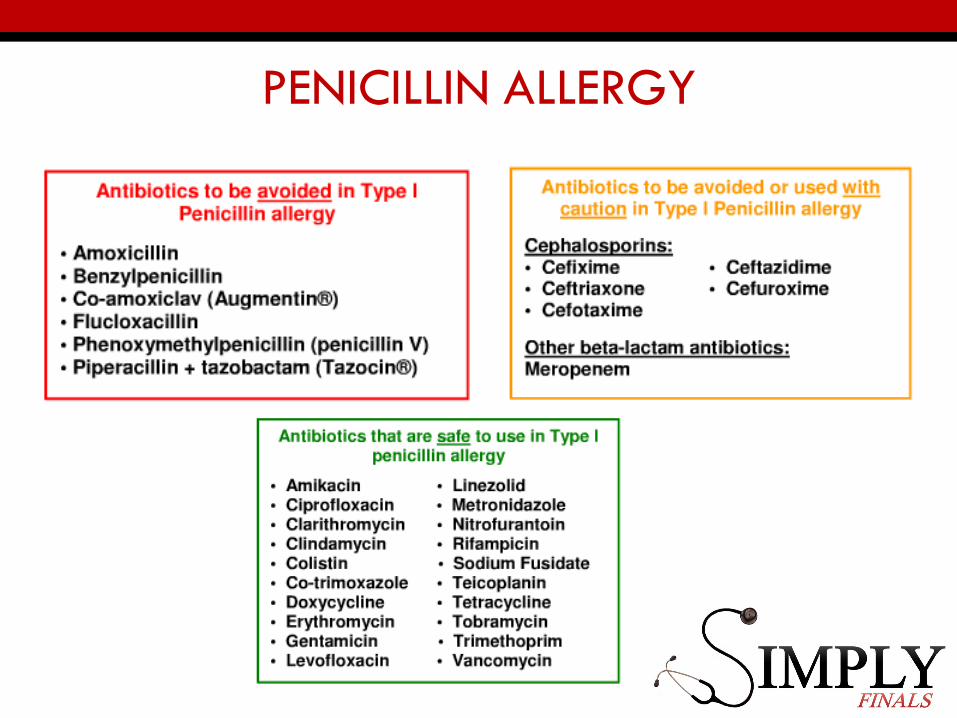
PENICILLIN ALLERGY
AVOID CAUTION SAFE
FLUCLOXACILLIN
TAZOCIN
CO-AMOXICLAV
CEFTRIAXONEMEROPENEM
AMIKACIN
METRONIDAZOLE
ERYTHROMYCIN
RIFAMPACIN
PENICILLIN ALLERGY
ALLERGIC REACTION MANAGEMENT
A patient recently given Tazocin despite a Type 1 Penicillin allergy develops shortness of breath, stridor and a widespread urticarial rash.
Choose 3 appropriate treatments:
A) Chlorphenamine 4mg, POB) Adrenaline 10ml of 1:10000, IVC) Adrenaline 10ml of 1:10000, IMD) Adrenaline 0.5ml of 1:1000, IVE) Adrenaline 0.5ml of 1:1000, IMF) Hydrocortisone 200mg, IVG) Chlorphenamine 10mg, IV
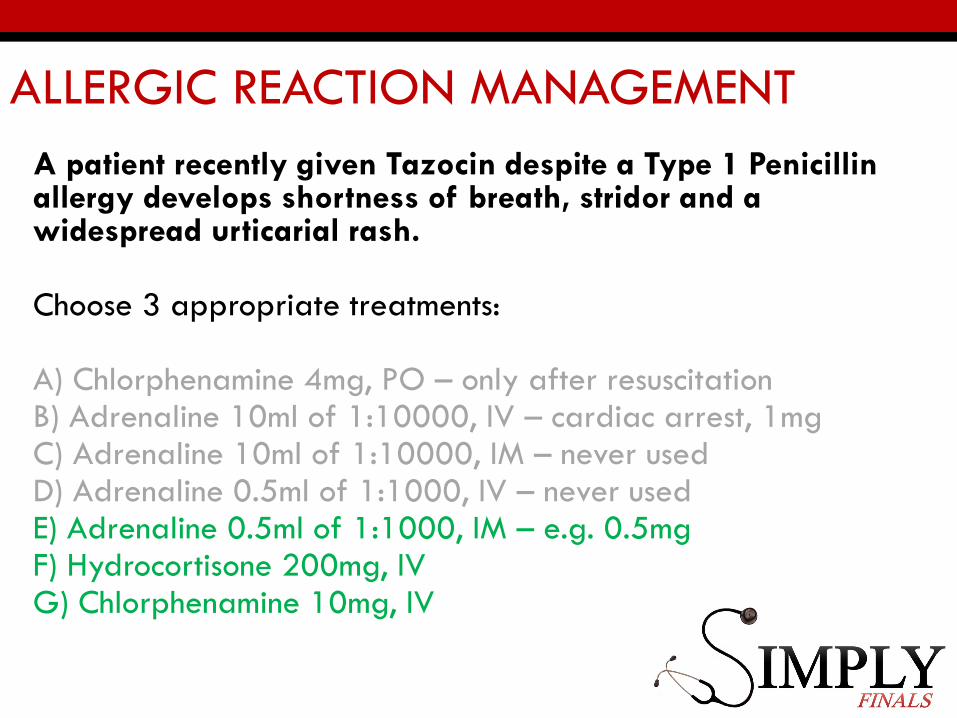
ALLERGIC REACTION MANAGEMENT
A patient recently given Tazocin despite a Type 1 Penicillin allergy develops shortness of breath, stridor and a widespread urticarial rash.
Choose 3 appropriate treatments:
A) Chlorphenamine 4mg, PO – only after resuscitationB) Adrenaline 10ml of 1:10000, IV – cardiac arrest, 1mgC) Adrenaline 10ml of 1:10000, IM – never usedD) Adrenaline 0.5ml of 1:1000, IV – never usedE) Adrenaline 0.5ml of 1:1000, IM – e.g. 0.5mgF) Hydrocortisone 200mg, IVG) Chlorphenamine 10mg, IV
SECTION 7 - DRUG MONITORING
• How to monitor the beneficial and harmful effects of
medicines.
• 8 items worth 2 marks
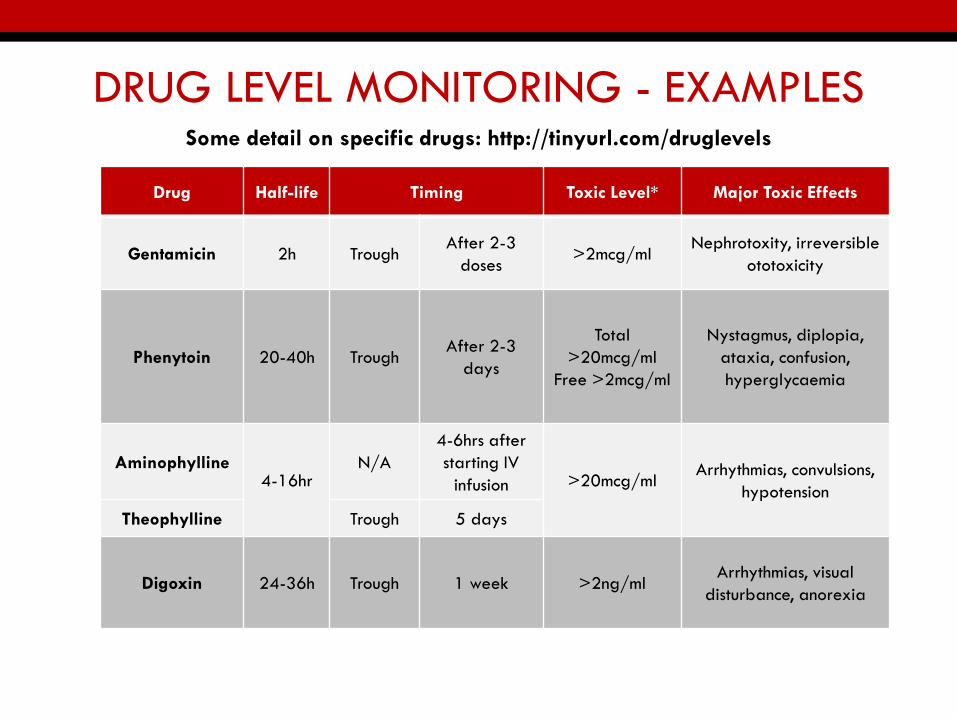
DRUG LEVEL MONITORING - EXAMPLES
Drug Half-life Timing Toxic Level* Major Toxic Effects
Gentamicin 2h TroughAfter 2-3
doses>2mcg/ml
Nephrotoxity, irreversible
ototoxicity
Phenytoin 20-40h TroughAfter 2-3
days
Total
>20mcg/ml
Free >2mcg/ml
Nystagmus, diplopia,
ataxia, confusion,
hyperglycaemia
Aminophylline4-16hr
N/A
4-6hrs after
starting IV
infusion >20mcg/mlArrhythmias, convulsions,
hypotension
Theophylline Trough 5 days
Digoxin 24-36h Trough 1 week >2ng/mlArrhythmias, visual
disturbance, anorexia
Some detail on specific drugs: http://tinyurl.com/druglevels
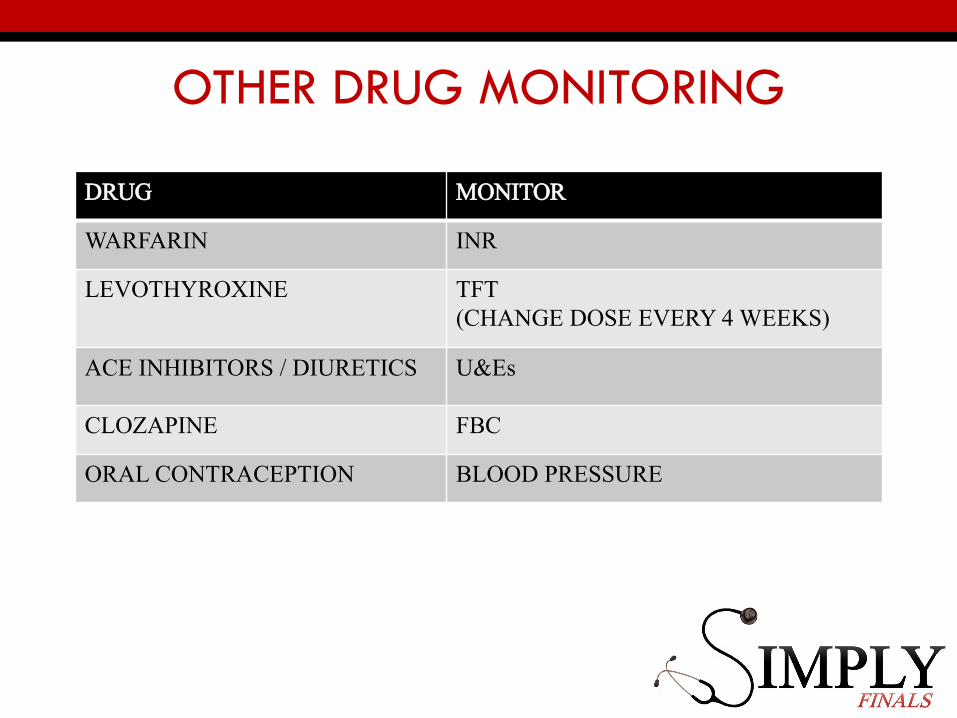
OTHER DRUG MONITORING
DRUG MONITOR
WARFARIN INR
LEVOTHYROXINE TFT (CHANGE DOSE EVERY 4 WEEKS)
ACE INHIBITORS / DIURETICS U&Es
CLOZAPINE FBC
ORAL CONTRACEPTION BLOOD PRESSURE
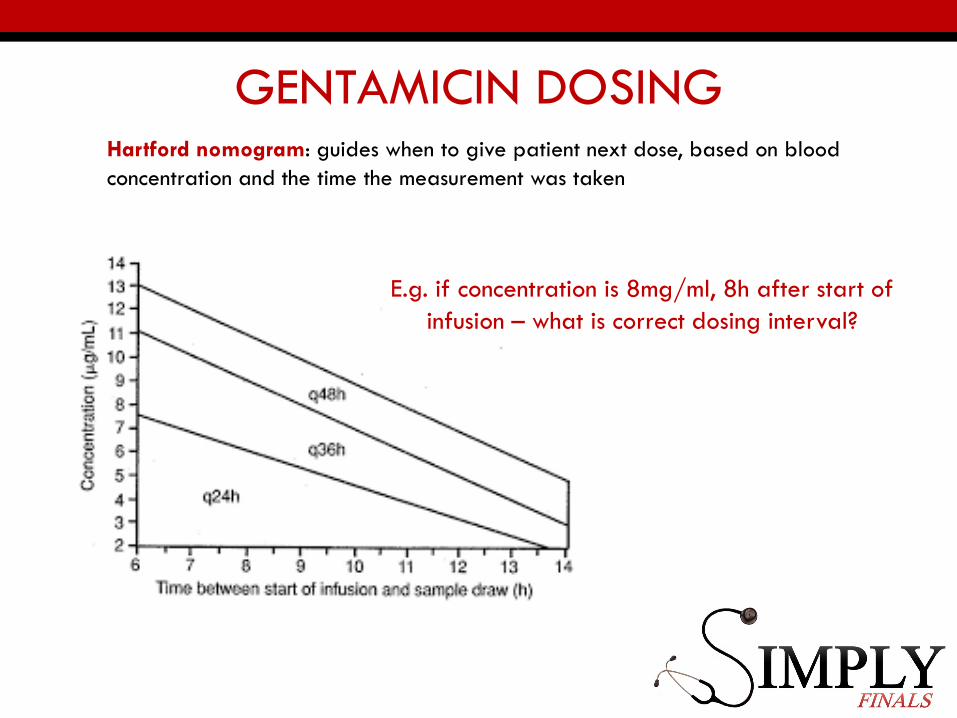
GENTAMICIN DOSINGHartford nomogram: guides when to give patient next dose, based on blood
concentration and the time the measurement was taken
E.g. if concentration is 8mg/ml, 8h after start of
infusion – what is correct dosing interval?
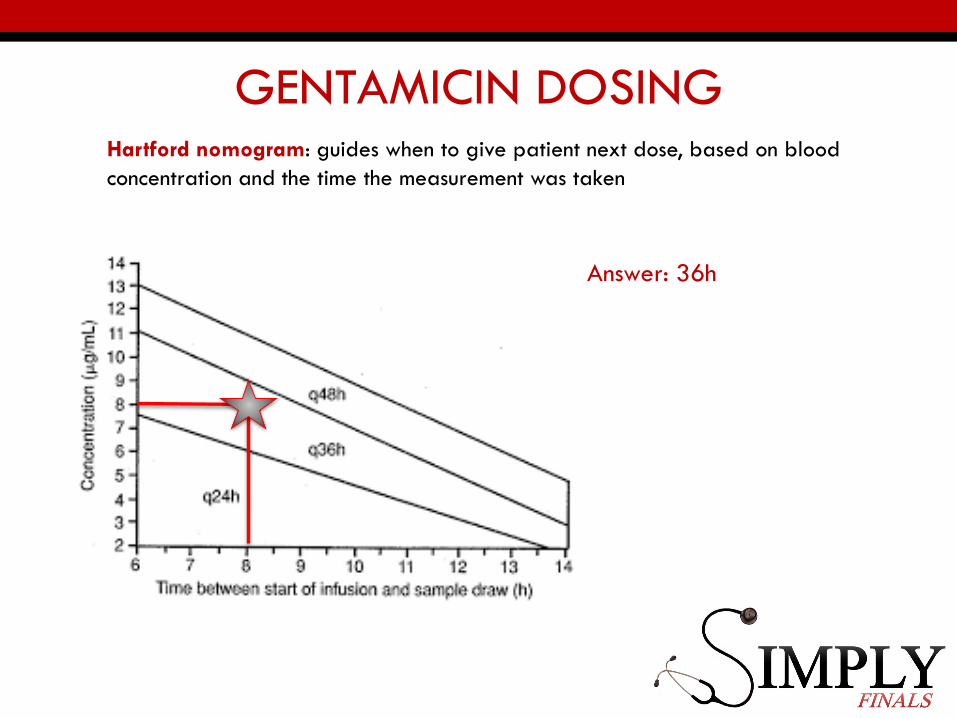
GENTAMICIN DOSINGHartford nomogram: guides when to give patient next dose, based on blood
concentration and the time the measurement was taken
Answer: 36h
SECTION 8 – DATA INTERPRETATION
• Make an appropriate change to a prescription based on
results of investigations
• 6 items worth 2 marks
PARACETAMOL OVERDOSEActivated charcoal: consider if >150mg/kg has been taken within
a 1 hour period.
N-acetylcysteine (NAC):
• Single overdose – check level at 4h and use the nomogram (use
nomogram when OD has been taken between 4-8h ago)
• If plasma concentration levels are above the treatment line then
you need to treat
• Staggered overdose (>1h) – cannot accurately calculate levels so
treat
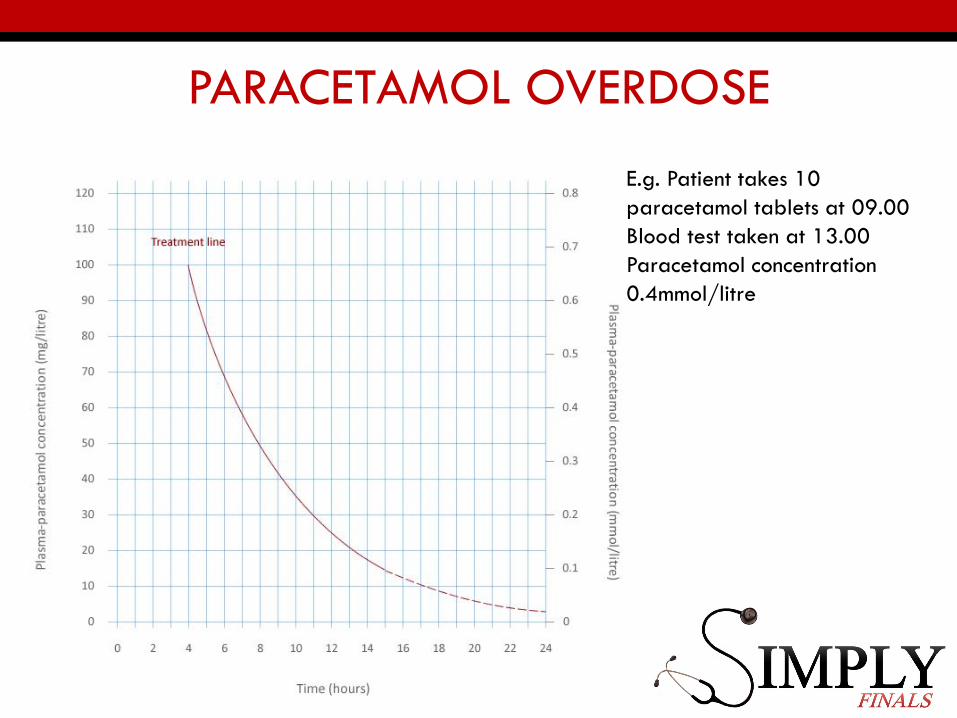
PARACETAMOL OVERDOSE
E.g. Patient takes 10
paracetamol tablets at 09.00
Blood test taken at 13.00
Paracetamol concentration
0.4mmol/litre
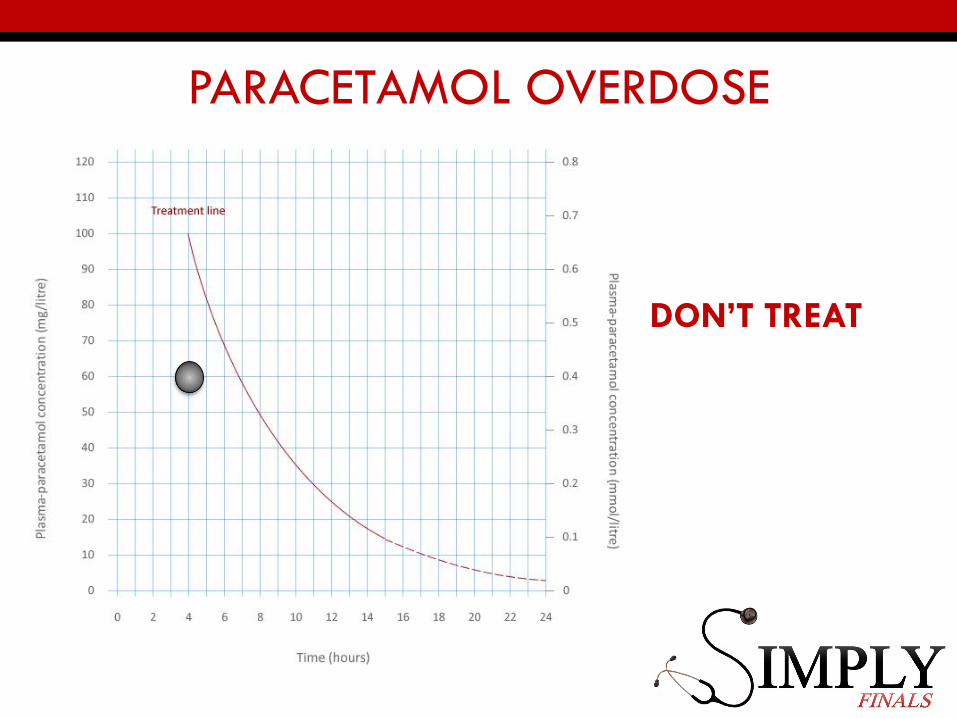
PARACETAMOL OVERDOSE
DON’T TREAT
PRESCRIBING SCENARIOS FINALS
• All the same scenarios in different formats
• OSCES• Prescribe warfarin
• Prescribe an IM injection eg vitamin B12
• Spot the prescription errors
• Write fluid prescription and calculate drip rates
• Presenting a history and giving treatment recommendations eg hypertension
• WRITTEN PAPER• Know your treatment algorithms for acute and chronic conditions
• Data interpretation questions – remember side effects of drugs and how they can affect blood results
GOOD [email protected]