Embed Size (px)
Citation preview

BALONES
FÁRMACOACTIVOS
Mecanismo de acción
Evidencia científica
Dra. Lucía Martínez Carnovale
Unidad Funcional del Acceso Vascular (FUVA)
Hospital de Terrassa, CST. Barcelona

INTRODUCCIÓN
Las fístulas arteriovenosas son los accesos vasculares de
elección
Una de la principal causa de disfunción son las estenosis

NUEVA GUÍA ESPAÑOLA

ANGIOPLASTIA SIMPLE
Menos invasiva
Menor morbilidad
No requiere colocación de un CVC
PRINCIPAL DESVENTAJA
Alta tasa de re-estenosis lo que condiciona la necesidad de realizar de
forma periódica procedimientos intervencionistas adicionales para
mantener la permeabilidad del acceso

SE PUEDEN MEJORAR LOS
RESULTADOS DE LA PTA SIMPLE?



BALONES
FÁRMACO-ACTIVOS
Son balones de angioplastia recubiertos de paclitaxel
Sus resultados han demostrado ser superiors en lesiones arteriales
coronarias y fémoro-popliteas

Diferencias histológicas entre
venas y arterias
Diferencias en el patrón de flujo sanguineo
Incremento en el índice de proliferación
en las re-estenosis
CONSIDERACIONES EN FAV

PACLITAXEL
Agente citotóxico y antiproliferativo que estabiliza los microtúbulos
durante la metafase de la mitosis celular
Presenta liberación rápida y retención prolongada
Muy hidrofílico por lo que penetra rapidamente por las membranas
celulares

BALONES EN EL MERCADO
Existe una variedad de balones DEB de 0.035-, 0.018-, y 0,014 pulgadas
para el tratamiento de la enfermedad arterial periférica y la angioplastia
coronaria

MECANISMO DE ACCIÓN
Después de la pre-dilatación de la estenosis el balón farmacoactivo se centra a través
de toda la zona tratada
Se recomienda inflado durante 2,2-minutos transfiere una dosis terapéutica óptima de
la droga a la superficie endoluminal
El Paclitaxel difunde en la pared del vaso
Se mantiene 30 días después del tratamiento para inhibir la re-estenosis en la pared
del vaso al tiempo que permite que el lumen se restaurare y re-endotelice
Evidencia de picos de efectos farmacológicos a los 90 días

EVIDENCIA CIENTÍFICA
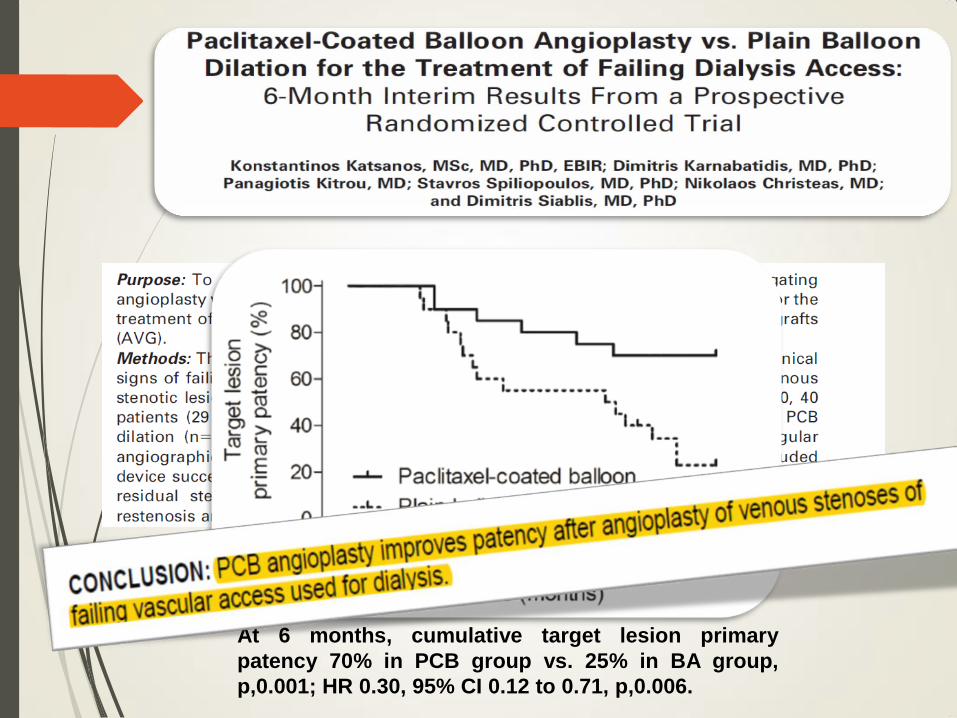
At 6 months, cumulative target lesion primary
patency 70% in PCB group vs. 25% in BA group,
p,0.001; HR 0.30, 95% CI 0.12 to 0.71, p,0.006.





ENSAYOS CLÍNICOS EN
CURSO CLINICALTRIALS.GOV

Trial
Name
DCB n= Primary Outcome
Proportion of patients with primary patency of AVF at 6
months
Double-blind comparison of the proportion of primary
patency at 6 months after treatment of stenosis of AVF by
conventional angioplasty + additional angioplasty. Primary
patency is defined as absence of reintervention for stenosis
at initial angioplasty site.
Adequate functioning of the hemodialysis access at 6
months.
Period of adequate functioning of the hemodialysis access
after treatment, defined according to the NKF-DOQI
protocol criteria
DEB after
CB
ELUTAX®
DCB
40 Time to worsening of dialysis fistula function at one year
Late luminal loss at 6 months
Late luminal loss is defined as the difference between the
minimum lumen diameters after angioplasty and at the end
of the 6-month follow-up angiogram.
DEBAPTA IN.PACT®
DCB
125
ABISS* LUTONIX®
DCB
Catheter
150
APERTO APERTO®
DCB
150

DEBAVAS ADVANCE
® 18 PTX
120 Primary patency of the vascular access after endovascular
angioplasty of a stenosis with drug-eluting balloon
compared with treatment with plain-balloon
[ Time Frame: at 12 months ]
DEBEFF* LUTONIX®
DCB
Catheter
70 Primary patency at 6 months Patency of AVF without any
additional procedures. Patency is defined as supporting HD
with a pump speed of at least 300ml/min.
Restenosis rate at 6 months
Incidence of >50% stenosis at the treatment site
Freedom from target lesion revascularizationat 12 months.
Percentage of patients that do not need any
revascularization proceeding during the following twelve
months after catheter insertion.
Primary Patency: 6 months. Patency is defined as the
interval following index procedure intervention until
clinically driven reintervention of the target lesion or access
thrombosis.
Safety: Freedom from any serious adverse event(s)
involving the AV access circuit
• Proportion of subjects with freedom from any
serious adverse event(s) involving the AV access
circuit Time Frame: 30 days.
Proportion of subjects with target lesion primary patency
at 6 Months. Defined as the interval following index
procedure until clinically-driven reintervention of the target
lesion or access thrombosis, through 6 months. Clinically-
driven reintervention is defined as a lesion that has ≥50%
stenosis and at least one clinical, physiological or
hemodynamic abnormality attributable to the stenosis
defined in the K/DOQI guidelines.
Time to end of target lesion primary patency* is
determined through AVF imaging when patient is referred
for a re-intervention, at any point during follow-up (1-3
years).
*Primary patency fails when any of the following occur:
1. Clinically driven re-intervention to the treatment
segment
2. Thrombotic occlusion that includes the treatment
segment
3. Surgical intervention that excludes the treatment
segment from the access circuit
4. Abandonment of the AVF due to an inability to retreat
the treatment segment
DEB
Cephalic
LEGFLOW
® DCB
50
FISBAL Unknown
Brand
134
PAVE* LUTONIX®
DCB
Catheter
211
LUTONIX
AV IDE
LUTONIX®
DCB
Catheter
285
LUTONIX
AV
Registry
LUTONIX®
DCB
Catheter
300

• Proportion of subjects with freedom from any
serious adverse event(s) involving the AV access
circuit Time Frame: 30 days.
Proportion of subjects with target lesion primary patency
at 6 Months. Defined as the interval following index
procedure until clinically-driven reintervention of the target
lesion or access thrombosis, through 6 months. Clinically-
driven reintervention is defined as a lesion that has ≥50%
stenosis and at least one clinical, physiological or
hemodynamic abnormality attributable to the stenosis
defined in the K/DOQI guidelines.
Time to end of target lesion primary patency* is
determined through AVF imaging when patient is referred
for a re-intervention, at any point during follow-up (1-3
years).
*Primary patency fails when any of the following occur:
1. Clinically driven re-intervention to the treatment
segment
2. Thrombotic occlusion that includes the treatment
segment
3. Surgical intervention that excludes the treatment
segment from the access circuit
4. Abandonment of the AVF due to an inability to retreat
the treatment segment
PAVE* LUTONIX®
DCB
Catheter
211
LUTONIX
AV
Registry
LUTONIX®
DCB
Catheter
300
CONSIDERACIONES FINALES
El uso de DEB en la angioplastia de estenosis de AV es segura y
efectiva
Ofrece intervalos superiores libres de intervención comparados
con los balones tradicionales
Reduce las restenosis sin complicaciones derivadas de los
dispositivos
Es necesario determinar las lesiones candidatas a este tratamiento
La evidencia científica en este campo es limitada
GRACIAS POR VUESTRA ATENCIÓN!!!
![Ivyspring TheranosticsVascular remodeling in this case is not as defined as in balloon-induced injury [24]. Compared to reste-nosis after balloon angioplasty, the pathophysiology](https://img.pdfslide.net/doc/110x75/609a0f421b44ac1253479b50/ivyspring-vascular-remodeling-in-this-case-is-not-as-deined-as-in-balloon-induced.jpg)




























