Embed Size (px)
Citation preview
Turkis/i Neiirosurgery 9: 129 - 132, 1999
Presentation of Chiari iCraniocervical Tranma:
Baykal: C/iiari i Mal/ormaliol!
Malformation Af terA Case Report
Kraniyoservikal Travma Sonrasi Bulgu Veren Chiari iMalformasyonu: Olgu Sunumu
SÜLEYMAN BAYKAL, ERTUGRUL ÇAKIR, MURAT KARAKUS, KAYHAN KUZEYLI, AHMET SARI
KTU Medical Faculty Departments of Neurosurgery (SB,EÇ, KK, MK) and Radiology (AS), Trabzon, Turkey
Gelis Tarihi: 12.11.1998 <::> Kabul Tarihi: 3.8.1999
Abstract Reported is a unique case of Chiari imalforma tionwith syringomyelia and medullar hemorrhage, whichbecame symptomatic 4 days after a craniocervical traumawhen the patient was doing neck exercises. The patientmanifested respiratory arrest, tetraparesis, and persistentlower cranial nerve dysfunction. Magnetic resonanceimaging studies revealed a Chiari i ma!formation with alarge cervicothoracic syringomyelia defect and medullarhemorrhage. The patient underwent surgery but somesymptoms persisted after the operation. Type i Chiarima!formation should be included in the differential
diagnosis of patients who present with extremity weakness(upper or lower), lower cranial nerve palsy, or respiratoryarrest after trauma or neck exercises.
Key Words: Chiari ima!formation, craniocervical trauma,medullar hemorrhage, syringomyelia
INTRODUCTION
Chiari described congenital anomalies of thecraniocervicaljunction in 1891,dividing them into threegroups O). The association of syringomyelia withChiari malformation is well known. The number of
patients diagnosed with asymptomatic Chiari Imalformation has risen with the advent of magneticresonance imaging (MR!). In this artiele, we present acaseof acute neurological deterioration and respiratoryarrest in a patient with Chiari I malformation withsyringomyelia and medullar hemorrhage. Thesymptoms developed 4 days after craniocervical
Özet: Kraniyoservikal travmadan 4 gün sonra, boyunegzersizleri uygulamasi esnasinda semptomatik halegelen, Chiari i Malformasyonlu olgu sunulmaktadir.Egzersiz esnasinda tetraparezi ve respiratuvar arrestgelisti. Radyolojik degerlendirilmesinde servikalsyringomyeli ile birlikte olan Chiari imalformasyonu vemedüller kanama tespit edildi. Bu olgu; travma veyaboyun egzersizleri sonrasi ekstremite parezileri altkraniyal sinir lezyonlari ya da solunum sorunlari gelisenolgularda Chiari Malformasyonlarinin ayirici tanidadüsünülmesi geregini ortaya koymaktadir.
Anahtar Sözcükler: Chiari i malformasyonu,kraniyoservikal travma, meduller kanama, syringomyeli
trauma, when the patient was doing neck exercises.We discuss the case and review the literature. To our
knowledge, this is the first report of a case of Chiari Imalformation with medullar hemorrhage.
CASE REPORT
A previously healthy 20-year-old man wasinvolved in acar accident, and was transported to theemergency room of a local hospital. His only complaintwas neck pain. X-rays of the cervical spine and skullwere normaL. He was hospitalized for his neck pain,and began a physical therapy and rehabilitation
129
Tiirkish Neiirasiirgery 9: 129 - 132, 1999
program. On the fourth day of the exercise program,the patient went into pulmonary arrest while he wasdoing neck exercises. He was intubated andtransported to the intensiye care unit (lCV) formechanical ventilation. The patient was in seriouscondition. He was unconscious, had neither motor norverbal responses, and his pupils were isocoric andmyotic, with a very weak light reflex. There were noabnormal findings on repeat cervical radiographs. Atracheostomy was performed and mechanicalventilation was initiated. The patient was started oncorticosteroids.
On his second day in the ICV, the patient wasable to respond to commands. His pupils were isocoricand reactive to light, he had neither a gag reflex norpalate elevation, and he was moving all extremities attwo-fifth' s strength. Because the patiene s spontaneousrespiration was insufficient, mechanical ventilation wascontinued in synchronized intermittent mandatoryventilation mode.
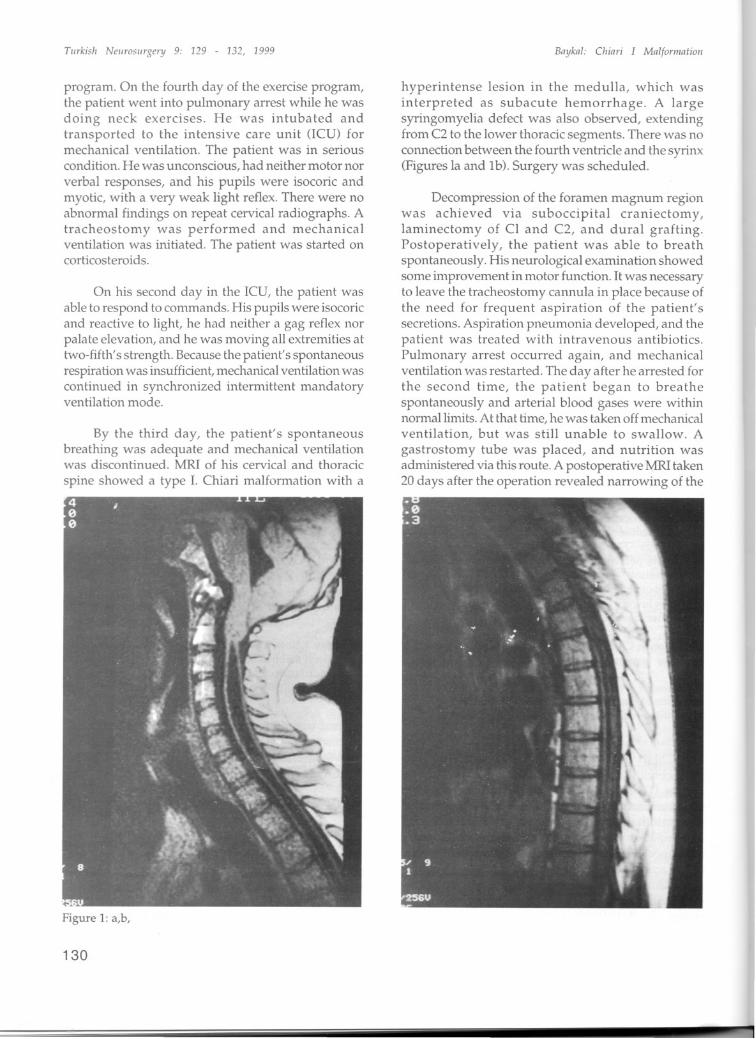
By the third day, the patient's spontaneousbreathing was adequate and mechanical ventilationwas discontinued. MRI of his cervical and thoracic
spine showed a type 1. Chiari malformation with a
Figure 1: a,b,
130
Bnyknl: Ciiinri J Mnlfaminliaii
hyperintense lesi0l1 in the medulla, which wasinterpreted as subacute hemorrhage. A largesyringomyelia defect was also observed, extendingfrom C2 to the lower thoracic segments. There was noconnection between the fourth ventride and the syrinx(Figures la and lb). Surgery was scheduled.
Decompression of the foramen magnum regionwas achieved via suboccipital craniectomy,laminectomy of CL and C2, and dural grafting.Postoperatively, the patient was able to breathspontaneously. His neurological examination showedsome improvement in motor function. it was necessaryto leave the tracheostomy cannula in place because ofthe need for frequent aspiration of the patient'ssecretions. Aspiration pneumonia developed, and thepatient was treated with intravenous antibiotics.Pulmonary arrest occurred again, and mechanicalventilation was restarted. The day after he arrested forthe second time, the patient began to breathespontaneously and arterial blood gases were withinnormal limits. At that time, he was taken off mechanicalventilation, but was still unable to swallow. Agastrostomy tube was placed, and nutrition wasadministered via this route. A postoperative MRI taken20 days after the operation revealed narrowing of the
TilI'kisii NCllrosiirgery 9: 129 - 132, 1999
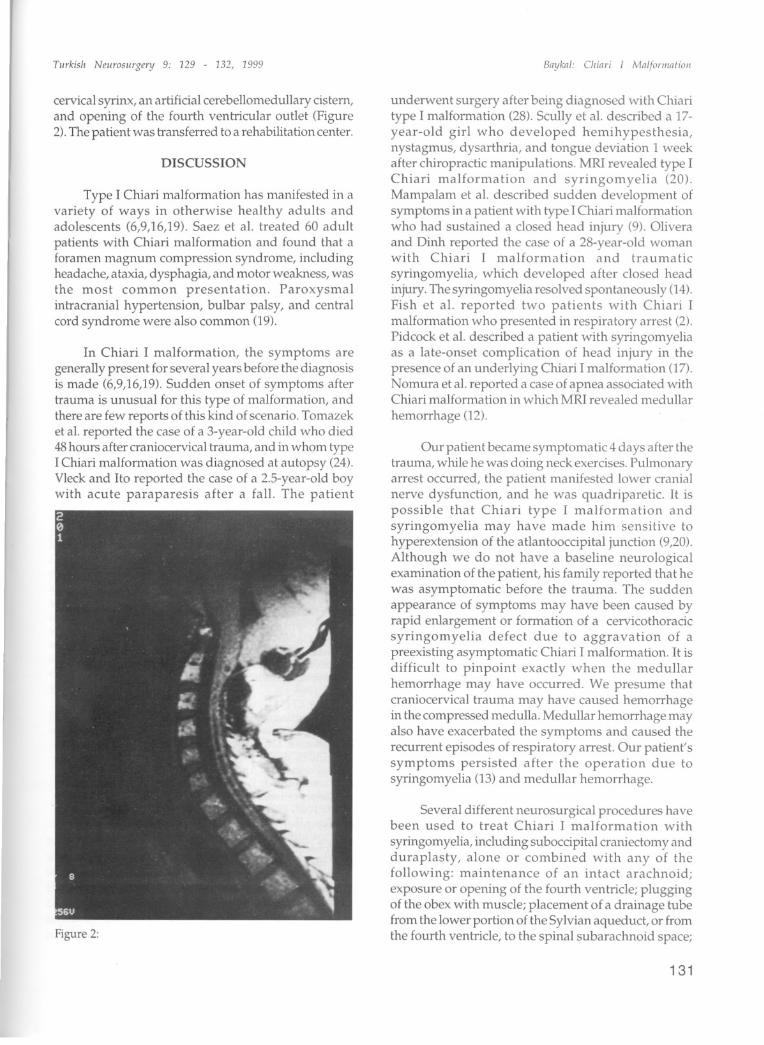
cervical syrinx, an artificial cerebeiiomeduiiary cistem,and opening of the fourth ventricular outlet (Figure2). The patient was transferred to a rehabilitation center.
DISCUSSION
Type i Chiari malformation has manifested in avariety of ways in otherwise healthyadults andadolescents (6,9,16,19). Saez et aL. treated 60 adult
patients with Chiari malformation and found that aforamen magnum compression syndrome, ineludingheadache, ataxia, dysphagia, and motor weakness, wasthe most common presentation. Paroxysmalintracranial hypertension, bulbar palsy, and centralcord syndrome were also common (19).
In Chiari I malformation, the symptoms aregeneraiiy present for several years before the diagnosisis made (6,9,16,19). Sudden onset of symptoms af tertrauma is unusual for this type of malformation, andthere are few reports of this kind of scenario. Tomazeket aL.reported the case of a 3-year-old child who died48 hours after craniocervical trauma, and in whom typeI Chiari malformation was diagnosed at autopsy (24).Vleck and ito reported the case of a 2.5-year-old boywith acute paraparesis af ter a fall. The patient
Figure 2:
Baykal: Cliia!'i 1 Malfomiafiol!
underwent surgery af ter being diagnosed with Chiaritype I malformation (28). Scuiiy et aL.described a 17year-old girl who developed hemihypesthesia,nystagmus, dysarthria, and tongue deviation 1 weekafter chiropractic manipulations. MRI revealed type IChiari malformation and syringomyelia (20).Mampalam et aL. described sudden development ofsymptoms in a patient with type I Chiari malformationwho had sustained a elosed head injury (9). Oliveraand Dinh reported the case of a 28-year-old womanwith Chiari I malformation and traumatic
syringomyelia, which developed af ter elosed headinjury. The syringomyelia resolved spontaneously (14).Fish et aL. reported two patients with Chiari Imalformation who presented in respiratory arrest (2).Pidcock et aL.described a patient with syringomyeliaas a late-onset compIication of head injury in thepresence of an underiying Chiari I malformation (17).Nomura et aL.reported a case of apnea associated withChiari malformation in whichMRI revealed medullar
hemorrhage (12).
Our patient became symptomatic 4 days after thetrauma, while he was doing neck exercises. Pulmonaryarrest occurred, the patient manifested lower cranialnerve dysfunction, and he was quadriparetic. it ispossible that Chiari type I malformation andsyringomyelia may have ma de him sensitive tohyperextension of the atlantooccipital junction (9,20).Although we do not have abaseline neurologicalexamination of the patient, his family reported that hewas asymptomatic before the trauma. The suddenappearance of symptoms may have been caused byrapid enlargement or formation of a cervicothoracicsyringomyelia defect due to aggravation of apreexisting asymptomatic Chiari I malformation. it isdifficult to pinpoint exactly when the medullarhemorrhage may have occurred. We presume thatcraniocervical trauma may have caused hemorrhagein the compressed medulla. MeduHar hemorrhage mayalso have exacerbated the symptoms and caused therecurrent episodes of respiratory arrest. Our patient'ssymptoms persisted af ter the operation due tosyringomyelia (13) and meduiiar hemorrhage.
Several different neurosurgical procedures havebeen used to treat Chiari I malformation with
syringomyelia, ineluding suboccipital craniectomy andduraplasty, alone or combined with any of thefollowing: maintenance of an intact arachnoid;exposure or opening of the fourth ventriele; pluggingof the obex with musele; placement of a drainage tubefrom the lower portion of the Sylvian aqueduct, or fromthe fourth ventriele, to the spinal subarachnoid space;
131
Tiirkish Neiirosiirgenj 9: 129 - 132, 1999
ventriculoperitoneal shunting; terminalventriculostomy; shunting from the syrinx to thesubarachnoid space, pleura or peritoneum; intermittentpercutaneous aspiration of the syrinx; andlumboperitoneal shunting (3-8,1O,1l,15,16,18, 19,2123,25-27).
The use of MRI has shown that treatment which
eliminates the syrinx may not improve the clinicalsymptoms, presumably because of irreversible cordinjury that may have occurred prior to treatment.Many patients res po nd best to simple bonedecompression with duraplasty, leaving thearachnoid intact (6-8,10,13,21).
In conclusion we have presented a unique caseof Chiari I malformation with posttraumaticsyringomyelia and intramedullary hemorrhage.Chiari I malformation must be included in the
differential diagnosis for patients who present withtetraparesis or paraparesis, lower cranial nervedysfunction, recurrent respiratory arrest, orcerebellar signs after closed head injury orchiropractic manipulation.
Correspondence: Süleyman BaykalKTU Lojmanlari 27/761080- Trabzon- Turkey
REFERENCES
1. Chiari H: Ueber Veranderungen des Kleinhirns infolgevon Hydrocephalie des Grosshins. Deutsch MedWochenschr 17:1172-1175,1891
2. Fish DR, Howard RS, Wiles CM, Simon L:Respiratoryarrest: a complication of cerebellar ectopia in adults. JNeurol Neurosurg Psychiatry. 51(5): 714-716, 1988
3. Garcia-Uria i, Leunda G, Carillo R, Bravo G:Syringomyelia after posterior fossa decompression. JNeurosurg 54:380-383, 1981
4. Gardner WJ, Angel J: The mechanism of syringomyeliaand its surgical corrections. Clin Neurosurg 6:131140,1959
5. Gardner Wl, Bell HS, Poolos PN, Dolm DF, SteinbergM: Terminal ventriculostomy for syringomyelia. JNeurosurg 46:609-617, 1977
6. Levy Wl, Mason L, Hahn JF: Chiari malformationpresenting in adults: A surgical experience in 127cases.Neurosurgery 12:377-390, 1983
7. Logue V, Edwards MR: Syringomyelia and its surgicaltreatment - an analysis of 75 patients. J NeurolNeurosurg Psychiatry 44:273-284,1981
8. Logue V: 14th Crookshank lecture. Syringomyelia. Aradiodiagnostic and radiotherapeutic saga. Clin Radiol22:2-16, 1971
9. Mampalam TJ, Andrews BT, Geib D, Ferriero D, PittsLH: Pres en ta tion of type i Chiari malformation afterhead trauma. Neurosurgery 23(6):760-762, 1988
132
Baykal: C/iiari i Mallorliiatioii
10. Matsumato T, Symon L: Surgical management ofsyringomyelia - current results. Surg Neurol 32:258265, 1989
11. Milhorat TH, Johnson WD, Miler JI, Bergland RM,Hollenberg-Sher J: Surgical management ofsyringomyelia based on magnetic resonance imagingcriteria. Neurosurgery 31:231-245, 1992
12 Nomura S, Akimura T, Eguchi Y, Shiroyama Y, lto H,Saito T: Apnea associated with Chiari malformation:medullary hemorrhage revealed by MR!. Childs NervSyst. 9(6): 348-349, 1993
13. Oldfield EH, Murazsko K, Shawker TH, Patronas NJ:Pathophysiology of syringomyelia associated withChiari imalformation: Implications for diagnosis andtreatment. J Neurosurg 80:3-15, 1994
14. Olivera WC, Dinh DH: Chiari i malformation withtraumatic syringomyelia and spontaneous resolution:case report and literature review. Neurosurgery 30(5):758- 760, 1992
15. Park TS, Cail WS, Broaddus WC, Walker MG:Lumboperitoneal shunt combined with myelotomy fortreatment of syringohydromyelia. J Neurosurg 70: 721727,1989
16. Paul KS, Lye RH, Strang FA, Dutton J: Arnold-Chiarimalformation - review of 71 cases. J Neurosurg 58:183187, 1983
17. Pidcock-FS, Sandel -ME, Faro -S: The Iate onset ofsyringomyelia after traumatic brain injury: associationwith Chiari i malformation. Arch Phys Med Rehabil.75(6): 695-698, 1994
18. Rhoton AL Jr: Microsurgery of Arnold-Cl1iarimalformation in adults with and without hydromyelia.J Neurosurg 45:473-483, 1976
19. Saez RJ, Onofrio BM, Yanagihara T: Experience withArnold -C hi ari ma!formation, 1960 to 1970. JNeurosurg 45:416-22, 1976
20. Scully RF, Mark EI, McNeely BU: Weeklyclinicopathological exercises, Case 3 - 1987. N Engl JMed 316:150-157,1987
21. Tachibana S, Iida H, Yada K: Significance of positiveQueckenstedt test in patients with syringomyeliaassociated with Arnold-Chiari ma!formations. JNeurosurg 67-71, 1992
22. Tator CH, Briceno C: Trea tment of syringomyelia witha syringosubarachnoid shunt. Can J Neurol Sci 15: 4857,1988
23. Tator CH, Meguro K, Rowed DW: Favorable resultswith syringosubarachnoid shunts for treatment ofsyringomyelia. J Neurosurg 56:517-523, 1982
24. Tomazek DE, Tyson GW, Bouldin T, Hansen AR:Sudden death in a child with an occult hindbrainmalformation. Ann Emerg Med 13:101-103, 1984
25. Vassilouthis J, Papandreou A, Anagnostaras S, et al:Thecoperitoneal shunt for syringomyelia. J Neurosurg76: 1047, 1992 (Letter)
26. Venes JL, DiPietro MA, Dauser RC: Arnold-Chiari typei malformation: a pediatric neurosurgical approach.Contemp Neurosurg 10:1-5, 1988
27. Vengsarkar U, Panchal VG, Tripathi PD, Patkar SV,Agarwal A,Doshi PK, Kamat MM: Percutaneousthecoperitoneal shunt for syringomyelia. Report ofthree cases. J Neurosurg 74:827-831, 1991
28. Vleck BW, lto B: Acute paraparesis secondary toArnold-Chiari type i ma!formation and neckhyperflexion. Ann NeuroI21:100-101, 1987


![Rx161 Arnold-Chiari Malformationfinalcopy0048502.netsolhost.com/.../pdfs/RXforms/Arnold_Chiari_Malformation.pdfArnold-Chiari malformation [Chiari malformation (CM)] is a congenital](https://img.pdfslide.net/doc/110x75/5ab9a8f17f8b9ac60e8e5491/rx161-arnold-chiari-malforma-malformation-chiari-malformation-cm-is-a-congenital.jpg)