Embed Size (px)
Citation preview
Presentation One:Areas of development and potential problems for ASH
Deborah ArnottDirector
UK Tobacco Control Achievements
2002-2007Ad Ban 2002Tobacco tax increases continue each yearSmuggling strategy developed and improvedStop Smoking Services maintained and funding increased over timeHealth Promotion marketing funding increased over timeWHO FCTC ratified 2004Smokefree Legislation 2007
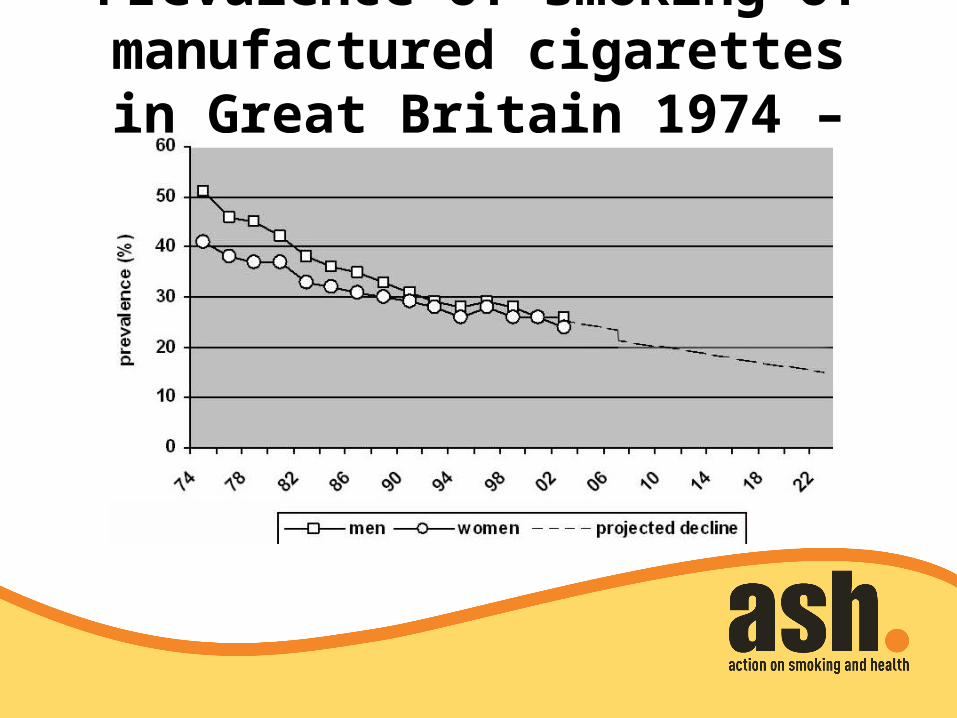
Prevalence of smoking of manufactured cigarettes in Great Britain 1974 –
2022
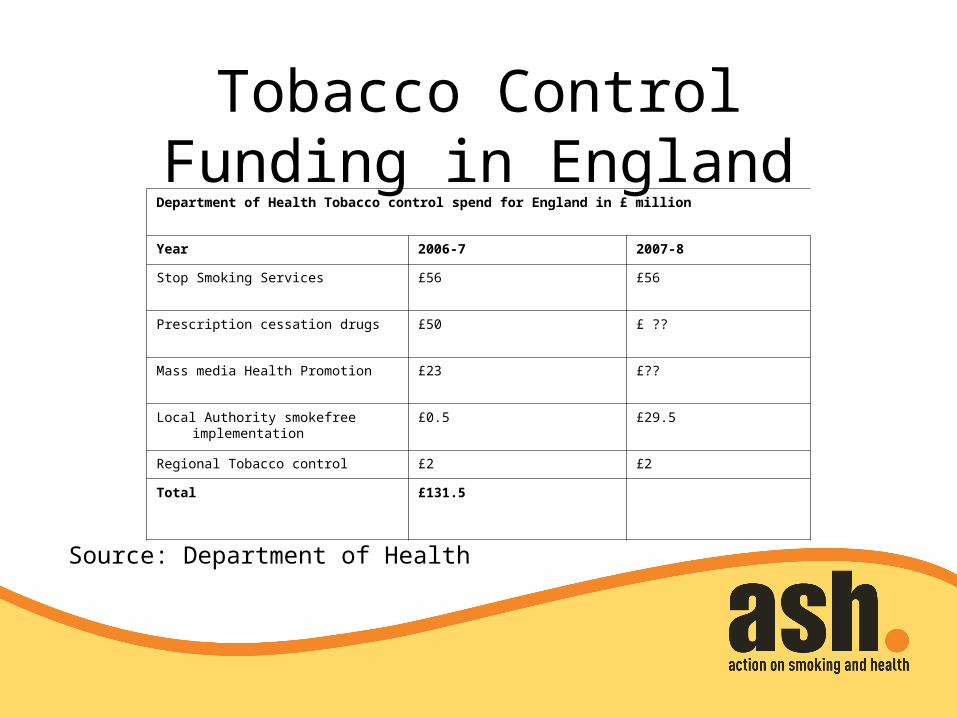
Tobacco Control Funding in England
Department of Health Tobacco control spend for England in £ million
Year 2006-7 2007-8
Stop Smoking Services £56 £56
Prescription cessation drugs £50 £ ??
Mass media Health Promotion £23 £??
Local Authority smokefree implementation
£0.5 £29.5
Regional Tobacco control £2 £2
Total £131.5
Source: Department of Health
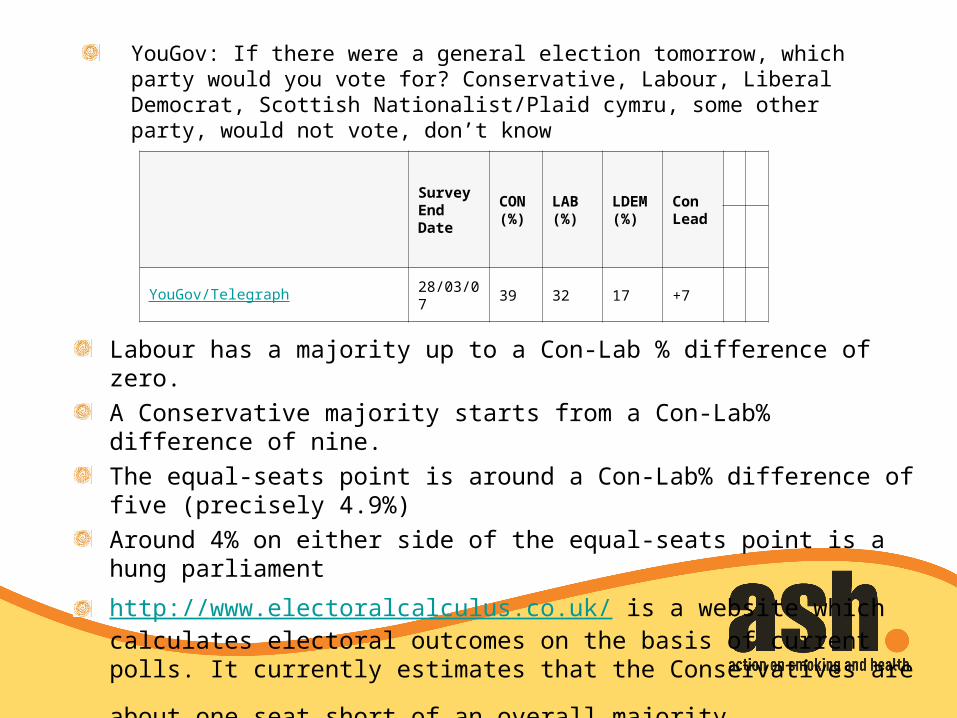
YouGov: If there were a general election tomorrow, which party would you vote for? Conservative, Labour, Liberal Democrat, Scottish Nationalist/Plaid cymru, some other party, would not vote, don’t know
Survey End Date
CON (%)
LAB (%)
LDEM (%)
Con Lead
YouGov/Telegraph 28/03/07 39 32 17 +7
Labour has a majority up to a Con-Lab % difference of zero.
A Conservative majority starts from a Con-Lab% difference of nine.
The equal-seats point is around a Con-Lab% difference of five (precisely 4.9%)
Around 4% on either side of the equal-seats point is a hung parliament
http://www.electoralcalculus.co.uk/ is a website which calculates electoral outcomes on the basis of current polls. It currently estimates that the
Conservatives are about one seat short of an overall majority.
RELEVANT POLITICAL ISSUESGovernment targets
Health inequalities – target is to reduce health inequalities by 10% by 2010 as measured by infant mortality and life expectancy at birth. Furthermore, to tackle the underlying causes of health inequalities by reducing adult smoking rates to 21% or less by 2010, with a reduction in prevalence among routine and manual groups to 26% or less;Child poverty - target is to reduce child poverty by a quarter by 2004-5 and eliminate the problem by 2020.
HEALTH INEQUALITIES AND CHILD POVERTY
THE CENTRE GROUND IN POLITICS Gordon Brown "We have taken a significant number of children out of poverty
but there is a lot more we have to do ... any statistics that show there is a bigger challenge makes me want to redouble our efforts.“
Oliver Letwin “Today, I can confirm that David Cameron's Conservatives are committed to the government target of ending child poverty by 2020. It is an aspiration, not a pledge, because we do not know how far from it we will be when we enter government…. It is not the commanding state but the supportive state that we need: enabling society to support, inspire, mentor and lead young people out of deprivation.”
Liberal Democrat policy document “Liberal Democrats see reducing health inequalities as a key policy aim. It will require working across a wide range of departments, since some of the key factors involved - most particularly economic and educational opportunities - lie outside the remit of the Department of Health. But the NHS can play an important role in addressing the serious inequalities that remain in the decisions people take over health and lifestyle, and the access they have to healthcare services.”
HEALTH INEQUALITIES AND CHILD POVERTY
CENTRAL TO TOBACCO CONTROLFrom 1973 to 2003 smoking prevalence among the most affluent in the UK halved to only
16%. [1]Among the most deprived, however, smoking rates over the same period remained the same at 70%. 1Around two thirds of the observed difference in risk of death across social class groups in middle age is caused by tobacco.1Three quarters of poor families smoke, spending a seventh of their disposable income on cigarettes.[2] Children are almost three times as likely to become regular smokers if both their parents smoke, than if neither does.[3]
[1] Jarvis, M. J. and Wardle, J (2005) Social patterning of health behaviours: the case of cigarette smoking. In: Marmot, M. and Wilkinson, R. (eds) Social Determinants of Health. Oxford: Oxford University Press,2nd edition.
[2] Marsh A and McKay S (1994) Poor Smokers. London: Policy Studies Institute[3] Office for National Statistics (1997) Teenage Smoking Attitudes in 1996. London: ONS