Embed Size (px)
Citation preview
3/27/2012
1
Social Media
#BeatingBarriers@DyingMatters@SimonSimply
The Nature and Burden of Heart Failure
Professor T A McDonagh, King’s College Hospital, London. UK
3/27/2012
2
What is heart failure ?
Burden ?
Prevalence , incidence, trends, epidemic ?
Effect on patients-morbidity and mortality
The Nature and Burden of Heart Failure
Effect on society-costs
Problems
Solutions
Remaining unmet need
Many
End stage of all serious forms of CV disease
Pathology of myocardium, pericardium, endocardium
Simple: ESC (2005 and 2008 Guidelines)
Definition (s)
• Typical symptoms/signs
AND
• Objective Evidence of Cardiac Dysfunction
• (Activation of neurohormonal systems)
• (Reduction in longevity)
Burden: Epidemiology of HF…
Famine to feast…
Changes in definition, methods..“Classical Studies” to “Modern”
GuidelinesNot just symptoms/signs of heart failureNeed for cardiac dysfunction
Focus on systolic dysfunctionMore recently on PLVEF/HNEF/Diastolic Heart Failure
Common
Increasing
Fatal
Morbidity high
E pensi e
Heart Failure Epidemiology: Phraseology..
Expensive
? Epidemic

3/27/2012
3
Epidemiology of Heart Failure
Prevalence
0.8% (age 50-59)
9.1% (>80 yrs)
Incidence
0.2% (54 yrs)( y )
0.4% (85yrs)
The Natural History of Congestive Heart Failure; The Framingham Study. NEJM 1971 285; 1441
Heart Failure and Left Ventricular Dysfunction
Systolic Preserved Systolic Function
Symptomatic
Chronic Heart Failure
Asymptomatic Asymptomatic
Prevalence of Systolic Dysfunction UK
North Glasgow MONICA (McDonagh et al Lancet 1997)
2000, 25-74 yrs2.9%, 1.5% CHF,1.4% ASLVD (LVEF≤30%)6.4%(men) and 4.9% in (women) >65 years
Poole (Dorset) (Morgan et al BMJ 1999;318;368)
817 subjects 70-84 years7.5% LVD (12.2% men and 2.9% women)52% undiagnosed
Echoes (England) (Davies et al Lancet 2001)
LVD: 1.8% (72), 50% asymptomaticBorderline LVD: 3.5% (139)
Prevalence of LVD by age and sex
% with LVD
LVEF 30%
Age Group
F MF MF MF M
65-7455-6445-5435-44McDonagh et al Lancet 1997

3/27/2012
4
Heart Failure with Preserved Systolic Function ? Heart Failure with Preserved LVEF
No large conclusive study
ECHOES-3960 random sample>45 years
54/3960-1.3% HF and LVEF>40%
30 AF and 19 mod/severe valve disease
42 (1.1%) had definite HF and LVEF>50%
Davies MK et al Lancet 2001;358: 439–44
14
16
18
Incidence of Heart Failure
The Hillingdon Study
1.3/1000 (over 25yrs)
0
2
4
6
8
10
12
25-34 35-44 45-54 55-64 65-74 75-84 85+
Cowie MR et al EHJ 1999;20:421
Age
Scotland Epidemiology; CMR Scheme
CMR Scheme
GP,53 practices, 30741 patients
Read codes for HF
Representative of Scottish Population
Prevalence, incidence, consultation rates,PrescribingYou have to visit your GP !
Murphy N et al Heart 2004;90:1129–1136

3/27/2012
5
CMR GP Data
Overall=0.7 Overall=2/1000
Murphy N et al Heart 2004;90:1129–1136
Aetiology of Heart Failure; Bromley Study
Population of 290,000 South London
All incident HF cases identified over 15 months
HF incidence 0.9/1000/yr
99/135 under 75 years underwent angiography and MPS
25%-the aetiology was not CAD prior to angiography/MPS
Fox et al EHJ (2001) 22, 228–236
EHFS II-Acute HFCo-morbidities
Nieminen M et al EHJ 2006; 27, 2725–2736
Mortality of Prevalent HF (systolic and preserved LVEF)
ECHOES: 6162 randomly selected from 4 cohorts: the general population, diuretic users, prior clinical label of HF, and risk factors for HF
The 5-year survival ratesThe 5 year survival rates
93%, general population
69% of those with LVSD without HF,
62% with HF and no LVSD,
53% with HF and LVSD
Hobbs FD et al EHJ 2007 28:1128-1134

3/27/2012
6
Epidemiology Trends in Survival
Mortality (%) Hillingdon/Hastings (2004-5)
Hillingdon/ Bromley
(1995-7)
1.1
1.0
.9
.8
Hillingdon/Hastings 2004-5
59 deaths (51 cardiovascular)
Median follow up: 370 days
1 month 6
(4-8)
16
(13-20)
3 month 11
(8-14)
22
(19-25)
6 month 14
(11-17)
25
(22-29)
time (days)
2101801501209060300-30
Cum
ulat
ive
surv
ival
.7
.6
.5
.4
London studies 1995-7
p<0.00001
Mehta P et al EJHF 2008
Mortality Following Heart Failure Hospitalisation in England and Wales 2010-11
Validated life status on 27, 850 admissions for HF (1st position)
33.1% (9,223) patients died
• 32.0 % for men and 34.4% for women))
• 11.6 % during admission
• Mortality or readmission=51%
Mean Length of Stay 11 days Readmissions
6802 (20%) readmitted during the year.
Median number =1, up to 13
3 Readmissions4%
4 Readmissions1%
5 or more Readmissions1%
1 Readmission79%
2 Readmissions15%

3/27/2012
7
Economic Impact of Heart Failure
UK-1995, direct and additional costs of health care, estimated at £751 million (2% NHS expenditure)
Projected to rise to £905 million (1.9%)
McMurray et al EHJ 1998:19:9
Quality of Life and Heart Failure
ECHOES
426 definite heart failure compared to 385 randomly co pa ed to 385 a do ysampled subjects aged 45 years with no heart failure
HF significant impairment of all measured aspects of physical and mental health
Hobbs et al 2002;23:1867
Symptom Burden….in Advanced HF
Lack of Energy
Breathlessness-60%
Weakness or fatigue
Pain-78% (comparable to lung/colon cancer)
Insomnia
Depression
HF in the UK
UK (population 61,400,000)
Prevalence•I million (maybe 1.2)
Incidence•125,000
Mortality•Up to155,000 per annum
NYHA III/IV•300,000

3/27/2012
8
Is it an Epidemic ? Trends in Incidence
Levy et al NEJM;2002;347:1397
Men 1.3-2.3 yrs
Women 1 32
Trends in Survival for Scotland
Women 1.32.-1.79 yrs
Absolute survival poor in both sexes:
50% of men dead at 2.3 years and women 1.7 years
Jhund P et al Circulation 2009:119
1st Hospitalisations
Repeat Hospitalisations increased. Survivors at discharge readmitted at 1 year , 21% in 1986 to 32.7% in 2003
Jhund P et al Circulation 2009:119
HF in the UK Challenges-In Hospital Mortality (%)
10
12
14
16
0
2
4
6
8
2010/11 2008/9 2009/10 HCC EHFS II Optimise HF
EURO Ob Pilot

3/27/2012
9
HF in the UK Solutions…
ty %
ty %
- in clinical trials..
Ann
ual M
orta
litA
nnua
l Mor
talit
HF in the UK Solutions-Specialist and Multi-Professional Care
Cardiology FU
No Cardiology FU
HFN
No HFN
Heart Failure in the UK-Problems to be Faced
Yes
No
UK resident population mid 200861.4 million

3/27/2012
10
Projected Trend in Prevalence of HFnci diagnosis of heart failure, 2000 to 2020.
Stewart, S et al. Heart 2003;89:49-532% of all NHS expenditure set to rise…
When ?Disease Progression in Heart Failure
HF Management-”chronic O/P care interspersed with hospitalisation and aggressive rescue efforts”
Markers of Prognosis in CHFAge
Sex
Race
Climate
Aetiology
Chronic renal failure
Diabetes mellitus
Alcohol abuse
Depression
Social isolation
NYHA Class
Erythrocyte sedimentation rate
Haemoglobin
White cell count
ACE inhibitors
Beta-blockers
Aldosterone antagonists
Angiotensin receptor blockers
Atrial Fibrillation
Heart Rate Variability
QRS Duration
QT Dispersion
C-Reactive Protein
Angiotensin II
Chromogranin A
CA125
Tumour Necrosis
Factor
Interleukin-6
Heart Failure Survival
Score
Seattle HF Model
ADHERE ModelQuality of Life
Syncope
Angina
Elevated jugular venous pressure
Third heart sound
Tachycardia
Hypotension
Low body weight
Hyponatraemia
Hypokalaemia
Troponin T
Urate
Ventricular Tachycardia
Cardiothoracic ratio
Left ventricular dimensions
LVEF
RVEF
Peak VO2
Six minute walk test
pulmonary capillary wedge pressure
Adrenomedullin
Norepinephrine
Endothelin
Atrial Natriuretic Peptides
ADHERE Model
BNP/NT-pro-BNP
Severe symptoms, deteriorating QOL, ADL, frequent hospitalisations, low bp, descalation of Rx and impaired renal function
Despite Progress
Still have a huge problem
Fatal disease for most
Different disease trajectory to cancer
L di t bl
The Nature and Burden of Heart Failure
Less predictable
Imprecise ways of identifying those who need palliative care early
Challenge to provide it and integrate it with HF care or transition from HF to palliative care.
Available for all who need it
No just those in the right place at the right time….

3/27/2012
11
Heart failure & palliative care: challenges and opportunities
James BeattieConsultant Cardiologist
Heart of England NHS Foundation Trust,Birmingham
National Clinical Lead
Heart Improvement Programme
22 March 2012National Council for Palliative Care
Trustee
Dying matters!
“In Scotland, where I was born, death was viewed as imminent. In Canada, where I trained, death was seen as inevitable Inwas seen as inevitable. In California, where I live now, death is thought to be optional.”Ian Morrisonformer president of the
Institute for the Future
Causes of Death, England• Cancer 26%• Circulatory disorders 37%
- Cardiac disease 26%
“Thank God it’s not cancer…”
%- Stroke 11%
• Respiratory disease 14%• Nervous system 3%• Other 20%
n = 512,541 ONS, 2004
About 3000 CVD deaths / week

3/27/2012
12
Population dynamics will drive HF need
From pyramid to coffin
UK 2001: Healthy life expectancy - men 67 of 76 years- women 69 of 80 yearsParliamentary Office of
Science & Technology
Reality of ‘dying’ in the elderly
• Lengthy period of decline: uneven course
• Difficulty with prognostication
• Multiple chronic medical conditionsp
• Progressive losses: independence; control
• Heavy burden of symptoms: multifactorial
• Substantial care needs: often overwhelming for family caregivers
Proportion of all carers (20+ hours) who have poor self rated general health
Carer burden
Mean age of carers 53.6 years
rated general health
% of all carers in pr health9.4 - 12.612.6 - 14.814.8 - 16.916.9 - 19.519.5 - 23.9
Local Authority level:
Range: 9.4 – 23.9 %
Mean: 16.1 %
S.D.: 2.85 %
Harriet Young, Stamatis Kalogirou & Emily GrundyLondon School of Hygiene & Tropical Medicine ESRC / ONS Seminar, June 30 2006 Modified from Goodlin, S. J. JACC. 2009;54:386-396 Copyright ©2009

3/27/2012
13
HF care: battery-farm model
Spencer Tunick, Selfridges, London 2003
HF care – a protocol driven paradigm
Challenges• The culture of HF care favours a medical model and
is treatment focussed. • Discussing prognosis in the face of uncertainty is
difficult and health care professionals may bedifficult and health care professionals may be reluctant to undertake this.
• Patients may be disempowered by technicalities or lack capacity.
HF professionals should agree on prognostic markersthat might be used to trigger discussion and promoteadvance care planning.
• Deteriorating despite optimally tolerated
therapy
• Increasing functional dependence
• Progressive fatigue
Care transition pointers
og ess e at gue
• Low ejection fraction
• Recurring hospitalisations
• Emotional distress
• Carer exhaustion
• Patient requestO’Leary N et al. Eur J Heart Fail 2009, 11: 406-11
The needs of those with HF in the last year of life
• Symptom control• Coordination of their care• Information• Social supportSocial support • Psychological assessment and support• Rehabilitation• Expert care in the dying phase • Support for their carers• Staff with good communication skills
3/27/2012
14
Heart failure palliative care – clinical domains
Refractory /complexsymptoms
High riskof dying Dying
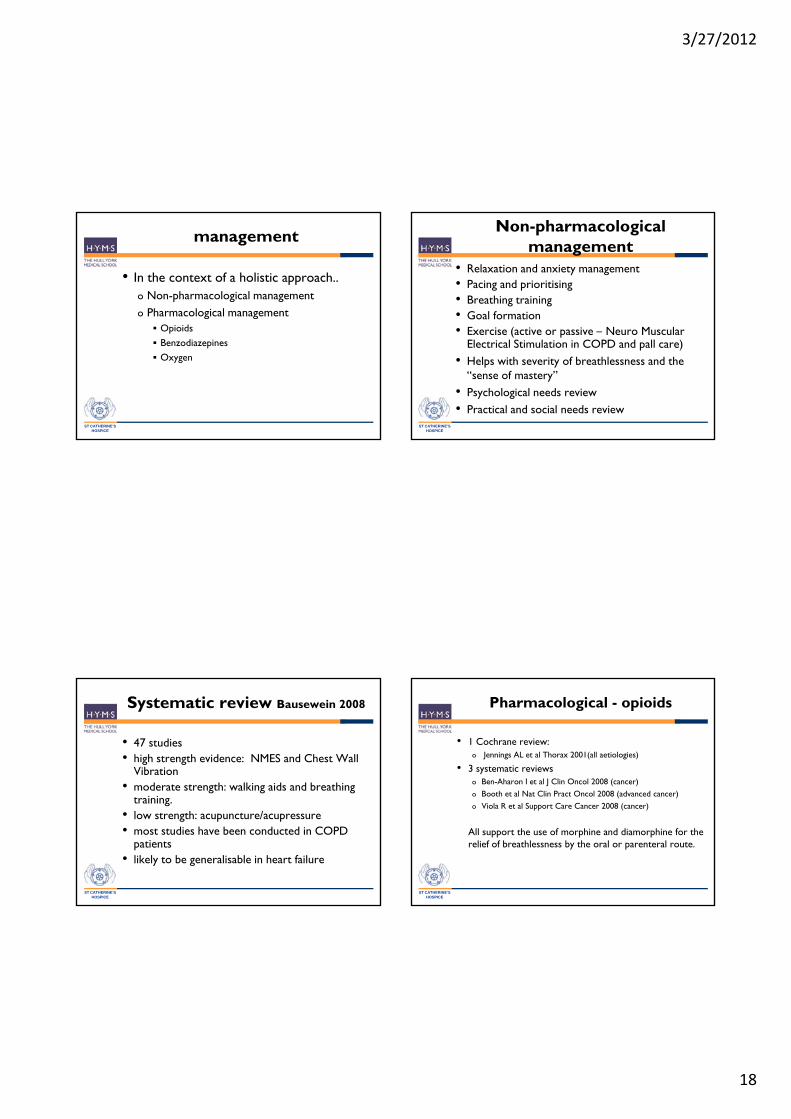
Prevalence of refractory symptoms
End of life symptomatic spectrum in HF
Dyspnoea 60-88%Fatigue 69-82%
Solano JP et al. J Pain Symp Man, 31: 58, 2006
Pain 63-80%Nausea 17-48%Anxiety 49%Depression 9-36%Confusion 18-32%
Mean of 6.7 symptoms/patient
Guidelines for symptom controland specialist palliative care referral for adult patients with end stage heart failure
Aug 2009
http://www.selcardiacnetwork.nhs.uk/files/PublishedCopyRD2266SELCNSymptomControlGuidelinesv5.pdf?PHPSESSID=4dc1e983a308b15cdd119d3f61e77b67
end-stage heart failure.
Service factors• Poor end of life
planning• Treatment focus• Poor palliative /
supportive care
Barriers to equitable and accessible heartfailure palliative care
Clinician Factors• Palliative care / general medicine /cardiology tension
• Technophobia
Patient factors• Disempowered• Unexplored /unrealistic goals
Disease factors• Need for dual
access• Low coverage in
diverse settings e.g. acute medicine /
nursing homes • Cancer bias
• Reluctance to address end of life issues
• Inadequate assessment skills
• Fear of defeat
• Stoicism• Reluctance to accept impending death
• Social isolation /poverty
treatment /palliativeapproaches
• Comorbidities• Lack of
predictability

3/27/2012
15
Who should coordinate end of life care?
• GP• Community matrons / case managers
About 90% of the last year of life is spent at home59% of deaths take place in hospital
• District / heart failure nurses• Community specialist palliative care team• Hospital specialists
– Palliative care– Cardiology– Other specialties
MDT working and good patient navigation essential
Doctors’ confidence in delivering end of life care
Nov 2008
Care coordinationEssential requirements for commissioning
end of life care
• Needs assessment
• Understanding the potential domains of need of patients & families
• Which service models are effective
• Development of service specifications that would facilitate best practicefamilies
• Knowledge of patient views
• Understanding where patients want choice
• Locally applicable strategy
facilitate best practice
• Assessment of service volumes required
• Accreditation of providers who can deliver
• An agreed price for services
Peter Tebbitt, 2007

3/27/2012
16
• A joint initiative between NHSImprovement and the End of Life Care Strategy programmes to drive care delivery.
End of life care in heart failure:a framework for implementation
• Concordant with the commissioning process in the QIPP environment
• Document launched June 2010
http://www.improvement.nhs.uk/document/endoflife/pdf
A challenge and an opportunity
‘Th i d f f th i ti ti t
Service development
‘There is a need for further investigation as towhether provision of palliative care according toa conventional oncology model is appropriate forpatients with heart failure’.
National Heart Failure Audit, Jan 2012
Palliative care for patients with heart failure
• A still evolving aspect of advanced HF care • Anticipatory palliative care increasingly embedded in
Key Messages
• Anticipatory palliative care increasingly embedded in ‘conventional’ general and specialist clinical practice
• Appropriate to all care settings• Challenges remain at point of care interfaces• An element of the NICE Quality Standards for
Chronic HF• Responsibility of all involved in HF care

3/27/2012
17
Symptom management
ST CATHERINE’SHOSPICE
Miriam Johnson
Some general principles
• Form the basis of the NYHA classification• Are prevalent in people with heart failure• Are prolonged
ST CATHERINE’SHOSPICE
• Have prognostic significance• Are often attributed to other things and
adapted to unless there is a crisis• Co-morbid conditions add to the problem• Often overlooked by clinicians
General principles of management
• Full assessment of the symptomo Holistic
• Optimise management of heart failure• Optimise management of co-morbidities
ST CATHERINE’SHOSPICE
• Reverse reversible contributing factors• Palliative the irreversible• Review• Include patient and family in decision making
• Check understanding• Check wishes
Breathlessness
o common and devastating o affects all aspects of lifeo major distress for both patient and caregiver
l t h lth i t
ST CATHERINE’SHOSPICE
o long-term health service support o trigger for unscheduled admissiono more difficult to treat than pain
o Only recently a focus for research
3/27/2012
18
management
• In the context of a holistic approach..o Non-pharmacological managemento Pharmacological management
O i id
ST CATHERINE’SHOSPICE
Opioids Benzodiazepines Oxygen
Non-pharmacological management
• Relaxation and anxiety management• Pacing and prioritising• Breathing training• Goal formation
ST CATHERINE’SHOSPICE
• Exercise (active or passive – Neuro Muscular Electrical Stimulation in COPD and pall care)
• Helps with severity of breathlessness and the “sense of mastery”
• Psychological needs review• Practical and social needs review
Systematic review Bausewein 2008
• 47 studies• high strength evidence: NMES and Chest Wall
Vibration• moderate strength: walking aids and breathing
ST CATHERINE’SHOSPICE
g g gtraining.
• low strength: acupuncture/acupressure• most studies have been conducted in COPD
patients• likely to be generalisable in heart failure
Pharmacological - opioids
• 1 Cochrane review:o Jennings AL et al Thorax 2001(all aetiologies)
• 3 systematic reviewso Ben-Aharon I et al J Clin Oncol 2008 (cancer)
B th t l N t Cli P t O l 2008 ( d d )
ST CATHERINE’SHOSPICE
o Booth et al Nat Clin Pract Oncol 2008 (advanced cancer)o Viola R et al Support Care Cancer 2008 (cancer)
All support the use of morphine and diamorphine for the relief of breathlessness by the oral or parenteral route.
3/27/2012
19
Opioids
• 1 adequately powered placebo RCTo Abernethy AP et al BMJ 2003 (multiple aetiology: 20mg MR
morphine )o Morning VAS 6.6mm; evening VAS 9.5mm improvement
• 1 pilot placebo RCT(CHF)
ST CATHERINE’SHOSPICE
1 pilot placebo RCT(CHF)o Johnson MJ et al EJHF 2002 (CHF 2.5-5mg IR morphine qds)o VAS improved with morphine by 23mm by D2 vs 13mm with
placebo
• 1 adequately powered placebo RCT (morphine/oxycodone) CHFo Oxberry SG et al EJHF 2011 Septembero All arms improved, none better than the others
3 month open label follow up
• Blinded preference at end of study
• Those who found opioids helpful could continue open label
• Continuers and non-continuers reviewed at 3 months
ST CATHERINE’SHOSPICE
• (intensity/global impression of change/SF-12/descriptors)
• 13 continued/20 didn’t• Statistical improvement in intensity of breathlessness,
global impression of change and physical SF-12 in continuers
• Non-continuers global impression deteriorated by a small amount
Therapeutic window
• 1 dose finding study (Currow D et al JPSM 2011; 42:388 - 399) o 10 – 30mg MR morphine titrated for one week then
long term on the dose of clinical benefito Drowsiness and constipation were main adverse
ST CATHERINE’SHOSPICE
pevents
o No cases of respiratory depression or opioid-related hospital admission
o Approximately two thirds net benefit
• Of those who improved, over 90% did so by 20mg per day
Barriers/facilitators
• Clinician survey (Rocker et al Chest 2008)
o Doctors’ fear of respiratory depression
o Cautious unless imminently dyingo Contact with palliative physicians increases
confidence
ST CATHERINE’SHOSPICE
• Patient interviews (Oxberry et al BMJ Supp & Pall Care 2012)
o Less opioiphobia than cancer patients – previous positive experiences
o Perceived that the doctor was worried about it though
o Faith in clinical team

3/27/2012
20
Benzodiazepines
• Simon S et al. Cochrane Database of Systematic Reviews 2010
There is no evidence that benzodiazepines are
ST CATHERINE’SHOSPICE
There is no evidence that benzodiazepines are beneficial for relieving breathlessness
[in practice, save for panic or dying distress. If an anxiety state, use an anxiolytic anti-depressant such as mirtazepine]
Palliative oxygen for breathlessness
• Frequently prescribedo 70% clinicians in one survey irrespective of O2 sats
Abernethy et al Pall Med 2007
o For refractory breathlessness (65%) or at patient’s request (35%)
ST CATHERINE’SHOSPICE
o More likely to be prescribed if have carer
• Consider part of standard of care• In Canada “palliative” O2 use = 30% budget
Evidence so far use of oxygen palliation of breathlessness
• 2 Cochrane reviewso Cranston JM, Crockett A, Currow D. 2008 (cancer, CHF, kyphoscoliosis)o Uronis H et al 2011 (mildly or non-hypoxaemic patients with COPD)
• 3 systematic reviews:o Booth S et al Respiratory Medicine 2004 (COPD, cancer, CHF)o Uronis HE et al British Journal of Cancer 2008 (mildly or non-hypoxaemic patients
)
ST CATHERINE’SHOSPICE
with cancer)o Ben-Aharon I et al Journal of Clinical Oncology 2008 (cancer)
• 1 cohort studyo Currow DC et al Palliat Med 2009 (palliative care: cancer 91.9% of baseline
cohort, but mainly respiratory or CV cause of breathlessness in those prescribed home O2)
• 1 placebo controlled trialo Abernethy AP et al Lancet 2010 (chronic lung disease, cancer, CVD)
Oxygen in CHF
• Stable heart failure patients do not usually desaturate therefore assess (eg with pulse oximeter)
• Few small studies; only one showed benefit to breathlessness and exercise tolerance, others did not
ST CATHERINE’SHOSPICE
confirm
• Remains a clinical uncertainty

3/27/2012
21
O2 Breathe• 1 placebo controlled trial
o Abernethy AP et al Lancet 2010 (chronic lung disease, cancer, CVD)
• 239 patients (US, UK, Aus)• Adult patients with refractory dyspnoea and
ST CATHERINE’SHOSPICE
• Adult patients with refractory dyspnoea and PaO2>55mmHg
• Randomised to 7 days oxygen or medical air delivered by concentrator
• Primary end point = average breathlessness on NRS over the last 3 days of the intervention arm
Intervention p=0.1925Time p<0.0001Intervention x time p=0.4433
Intervention p=0.8580Time p<0.0001Intervention x time p=0.8010

3/27/2012
22
Fatigue
Aetiology• Poor sleep
o timing and amount of diuretics, sleep apnoea, nocturnal hypoventilation, orthopnoea and PND
ST CATHERINE’SHOSPICE
yp , p
• Overdiuresis• Hypokalaemia• Renal failure• Anaemia• Depression
Handy hints for other symptoms
• Nausea – avoid cyclizine (anti-cholinergic)
• Insomnia – avoid amitryptiline (anti-cholinergic)
• Constipation avoid
ST CATHERINE’SHOSPICE
• Constipation – avoid Fybogel (fluid restriction)
• Burning legs – try Aq cream + menthol
• Itch – skin care (see Aq cream) and SSRI or ondansetron
Depression
• Major problem. • Wide estimates to prevalence. • Associated with increased re-admission and mortality.
• Aff t i l t i t
ST CATHERINE’SHOSPICE
• Affects involvement in own management• Affects communication• Affects compliance with treatment
• Treat as in any other conditiono Exerciseo CBTo Antidepressants (cardiac safe)
Subcutaneous furosemide
• Patients with heart failure may be able to be managed without diuretics at the very end of life
• Sub cut route can be used for furosemide and useful for when the IV route is lost or cannot be provided (eg if the
ST CATHERINE’SHOSPICE
patient wants to stay at home).
• Allows continuous infusion
• CSCI furosemide is starting to be used (audit 26 episodes used to attempt to restore fluid balance, successful in 73% with average weight loss of 5.5kg and avoidance of hospital admission) Zacharias H et al Pall Med 2011;25:658 - 663

3/27/2012
23
When to involve specialist palliative care?
• Persistent, complex symptoms• Other support needed, including for family• Difficult things to talk through
P f i l f
ST CATHERINE’SHOSPICE
• Preference in place of care• Local service configuration
• Problem based, not prognosis based• Extended team based, not “either/or”
summary
• Symptom management is a core skill for all health care professionals
• Assessment and regular review• Symptoms affect all domains of life so all
ST CATHERINE’SHOSPICE
• Symptoms affect all domains of life, so all domains must be assessed
• Assessment should be in the context of family, other caregivers and place of care
• SPC should be involved as appropriate irrespective of prognosis
Thank you for your attention

3/27/2012
24
The Power of Partnership Working:
Lessons from NCPC’s Heart Failure Nurse Surveyy
Jane Butler - Consultant NurseBart’s and The London NHS Trust
Partnership working…
• Removal of barriers to enable moving forward.
• Provide consistent co-ordinated and comprehensive carecomprehensive care.
• Develop a “whole person” approach.
• Access to a range of training and education.
• Develop a wider range of personal skills.
Background
Patients with heart (HF) have less access to supportive and palliative care than those with cancer. In the UK heart failure nurse specialists are well placed tonurse specialists are well placed to address this issue if given adequate education and access to specialist palliative care services.
Introduction
• 2 surveys by NCPC – (2005 – 2010)
• Questionnaire to heart failure nurses in England (2005) UK (2010)
• 152 responses published in Focus on Heart Failure: A national survey of heart failure nurses and their involvement with palliative care services (2006)care services (2006)
• 174 responses published in Strengthening the relationship between heart failure nurses and specialist palliative care: Results from two national surveys – 2005/2010
• What has happened in those 5 years

3/27/2012
25
Number of significant national strategies to improve care at the end of life
• End of Life Care Strategy – promoting high quality care for all adults at the end of life (2008)
• End of life care in heart failure; a framework for implementation (2010)(2010)
- Similarly for Scotland - Living and dying with advanced heart
failure: a palliative care approach (2008)
• British Heart Foundation and Marie Curie Cancer Care’s “Caring Together”
Methodology
• 2005 – Questionnaire developed by NCPC HF policy group
• Distributed to HFSN in England co-ordinated through the 32 regional cardiac Networks.
Methodology
• 2010 – themes from 2005 maintained but varied to accommodate developments in national policy
• New questions introduced to determine level ofNew questions introduced to determine level of professional experience with HF and PC
• Distributed through 28 cardiac Networks, BHF and local contacts
Findings: England
Responses:
2005 2010
152 174
Scotland (2010) 10
Northern Ireland (2010) 3
Wales (2010) 11

3/27/2012
26
Working as a heart failure nurse
Setting (respondents could tick multiple)
2005 (n=152 2010 (n = 174)
Primary care 106 70 % 125 72 %
Secondary care 104 68 % 83 48 %
Home visit 104 68 % 101 58 %
GP S i 38 25 % 40 23 %GP Surgeries 38 25 % 40 23 %
Care Homes (Nursing homes) 36 24 % 46 26 %
Care Homes (Personal Care) 20 13 % 32 18 %
Tertiary Care 13 9 % 10 6 %
Hospices 14 9 % 27 16 %
Others 15 10 % 22 13 %
Role of specialist palliative care…
2005 2010
97% 99%
“…many patients have had frequent
d i i [t h it l]
“I feel [the SPC team] link in very
appropriately, they are a good source
of support to myself within my
role…”readmissions [to hospital] and no longer want this but want to die and be
cared for at home. Palliative care can ensure their wishes are granted” “…[SPC is] also
important in offering support and advice to the patients family…”
Role of specialist palliative care…
“We have an advanced heart failure MDT whereby
specialist palliative care attend and provide any symptom management
advice however, it is us as heart failure nurses who
“Palliative care should be provided by the HF nurses already looking after the patients. It is the nurses’
responsibility to gain theprovide the `specialist` palliative care”
responsibility to gain the appropriate knowledge”
“We work closely with the community generalist palliative care team [however] I have
so far not encountered a patient with intractable symptoms that the generalist team
were unable to manage”
Provision of palliative care
What would improve access to specialist palliative care in your area? Tick as many as apply
Of respondents = 125
The existence of local pathways incorporating heart failure and palliative care
84 67%
Formalised partnerships between HF and primary care providers
58 46%p
HF nurses having ready access to specialist palliative care advice
29 23%
Access to other HF specialists 19 15%
Other (specify) 18 14%
GP’s having ready access to specialist palliative care advice
16 13%

3/27/2012
27
Referrals and guidelines
2005 2010
None 44 24
1 16 23
2 – 5 69 90
The number of nurses not referring at all has halved dropping from 29% to 14%
6 or more 22 29
TOTAL 151 166
Reasons for referral
*Removed for 2010
Reasons for referring(respondents could select more than one)
2005 (n=107) 2010 (n=142)
Symptom Control 93 87% 118 83%Symptom Control 93 87% 118 83%
End of Life Issues 73 68% N/A*
Communicating Difficult News 11 10% 18 13%
Hospice / PC unit admission 57 53% 97 68%
Ethical decision making 9 8% 35 25%
Other 8 7% 35 25%
Benefits of guidelines
A selection of local guidelines can be accessed at:
www.ncp.org.uk/page/HFNS-Survey
% nurses making one or more referrals to SPC
2005 2010
Referral criteria is in place 79% 94%
No referral criteria 55% 75%
End of life care tools
• Liverpool Care Pathway (LCP)
• Gold standards Framework (GSF)
• Preferred Priorities for Care (PPC)
2005 2010
Awareness of LCP 88% 99%
Implementation of LCP 49% 82%
Awareness of GSF 78% 96%
Implementation of GSF 53% 82%
Awareness of PPC 49% 83%
Implementation of PPC 25% 70%

3/27/2012
28
Training“I am yet to attend any formal palliative care
training for heart failure. I would like to learn more about symptom control and medication for end
of life symptoms”
“Still d ’t f l
“I would like to feel more confident in the
prescribing of palliative drug
therapy towards end of life”
“Still don’t feel comfortable in broaching or
starting end of life discussions”
“not an area I feel confident in beyond the basics…”
“I do not have the right skills [as a heart failure
nurse] to help these patients especially when it comes to
symptom management”
Findings: Scotland, Wales and Northern Ireland
• 24 responses
• 10 respondents from Scotland
• Everyone 23/23 thought SPC had a role in providing care for end stage heart failure.
• 9 out of 10 had been in contact with SPC services in the last year.Scotland
• 11 respondents from Wales
• 3 respondents from Northern Ireland
• As per England nurses made contact with SPC mainly for symptom management.
• Only 9/22 reported local criteria had been developed.
• Half 11/22 had not received palliative care training in their current post.
Limitations
• No national database of HFN – unknown numbers
• Exact proportions of respondents unknownExact proportions of respondents unknown
• Variety of job titles for HFN - may have missed out a significant proportion
• Change in questions between years may have affected the data
…Partnership working
• Maintains continuity of care.
• Avoids sense of abandonment of patient and families.
SPC i d d b t th i• SPC services are underused but there is a willingness to work together.
• Nature of chronic disease is shifting –need new competencies and skills.

3/27/2012
29
Key messages and recommendations
• Build on a growing relationship
• Joined-up care available on a 24/7 basisJoined up care available on a 24/7 basis
• Extend access to training
• Continue to work in partnership
• Moving forward together
Conclusions
• HFNS recognise palliative care as a priority for their advanced HF patients.
• HFNS provide general palliative care and increasingly link with SPC.increasingly link with SPC.
• Developing multidisciplinary working with SPC professionals and formalising local care pathways may foster further collaboration and improve patient care without overloading SPC services.
Beating the Barriers 22.03.12
Good Practice –Caring Together:
Early insights, ambitions andambitions and
challengesDr Mike Knapton
Associate Medical Director BHFDr Teresa Tate, FRCP FRCR
Medical Adviser,Marie Curie Cancer Care

3/27/2012
30
Caring TogetherBetter end of life care for people with
heart failure
Caring Together objectives (1)The Caring Together programme aims to develop pioneering models of palliative care for patients in the advanced stages of heart failure which:
• meet the needs of patients and carers
• complement the optimal management of heart failure
• promote equity of access to palliative care for heart failure patients
• acknowledge the patient’s preferences in place of care
• enable increased choice of place of care for patients
• improve coordination of care among stakeholders
Caring Together objectives (2)We plan to commission robust, independent
evaluations of the programme. These will involve action research to refine the original working model and a formal evaluation of its efficacy to contribute additional learning to the evidence base regarding the palliative care needs of patients in the advanced stages of heart failure.
We will also intend to develop a model which will be applicable elsewhere in Scotland as well as in the rest of the UK.
Core Components of the model (1)
• Referral criteria for Caring Together (LVSD)
– a diagnosis of heart failure (NYHA stage III or IV)a diagnosis of heart failure (NYHA stage III or IV)
– progressive distressing or debilitating symptoms despite optimal cardiological therapy
(identified by increased/changing needs)

3/27/2012
31
Core Components of the model (2)
• A comprehensive assessment of identified patients that includes – A cardiological reviewA cardiological review
– Holistic needs assessment
– Anticipatory Care Plan ACP (where appropriate)
Core Components of the model (3)
• Identification of an appropriate care manager, who takes a key role in managing, directing and coordinating the care of an individual patient
– Heart Failure Nurse for LVSD patientsHeart Failure Nurse for LVSD patients
• Training and education of professionals involved in the care of these patients
– Needs identified through training need analysis
Core Components of the model (4)
• An approach to multidisciplinary working to ensure coordinated planning and delivery of care
• Joint working and professional development across palliative care and cardiology teams, in acute and community settings
Local implementation of core components
Three pilot sites:North-East Glasgow, Inverclyde and S GSouth-West Glasgow

3/27/2012
32
Local challenges specific to pilot site
• Lack of GP representation on facilitation group: lack of buy in from primary care team
• Service very dependent on HFSN who have a pre-exisiting interest in palliative care
• Patient in care homes – outside of HFSN remit to visit care homes -DNs able to provide care management
• Large geographical area – equity of service in all areas?
• Leadership
• Patient perceptions
• Prognostic vs needs based assessment
• Financial climate
Description of Pilot Site
• Patients referred to or known to HFSN.
• Seen at heart failure clinic for complex symptoms, cardiologist led.
• Treatment optimised.
• HFSN starts holistic assessment process (may have already been started)..
• Patients identified as in palliative phase discussed at MDT with specialist palliative care team.
• HFSN liaises with primary care team. May do joint visit with DN.
• DN may be appointed as care manager.
• Referrals to specialist palliative care as appropriate.
CareCare--Plus Tower HamletsPlus Tower Hamlets
Supporting carers looking after people with end stage Supporting carers looking after people with end stage
heart failureheart failure
Lyn MiddletonLyn Middleton

3/27/2012
33
What is a Carer?What is a Carer?
A Carer is someone who provides significant and substantial unpaidA Carer is someone who provides significant and substantial unpaid
help and support to a partner, child, relative, friend or neighbour whohelp and support to a partner, child, relative, friend or neighbour who
could not manage without their help? This could be due to age,could not manage without their help? This could be due to age,
physical or mental illness, addiction or disability.physical or mental illness, addiction or disability.
BasicallyBasically--the Carer is the person who manages 24/7 the Carer is the person who manages 24/7
when all the professionals have ‘finished for the day’.when all the professionals have ‘finished for the day’.
What is CareWhat is Care--Plus?Plus?
•• 3 year research project funded by the Kings Fund 3 year research project funded by the Kings Fund ‘Partners in Health’ programme‘Partners in Health’ programme
•• CrossCross--sectoral partnership between the Carers Centre sectoral partnership between the Carers Centre Tower Hamlets, LB Tower Hamlets Adults Social Tower Hamlets, LB Tower Hamlets Adults Social Services and Tower Hamlets PCTServices and Tower Hamlets PCT
•• Provides support services for carers (aged 18+) caring Provides support services for carers (aged 18+) caring for patients suffering from end stage heart failure (NYHA for patients suffering from end stage heart failure (NYHA stages 3 & 4) in Tower Hamlets.stages 3 & 4) in Tower Hamlets.
AimAim
To demonstrate that investment in providing better qualityTo demonstrate that investment in providing better quality
services for the carer leads to significant, tangible &services for the carer leads to significant, tangible &
measurable benefits for the patient, the carer, Local measurable benefits for the patient, the carer, Local
Authority social care and NHS Primary & Acute CareAuthority social care and NHS Primary & Acute Care
commissioners.commissioners.
Why Did We Need CareWhy Did We Need Care--Plus?Plus?
•• Poor access to EOLC for patients with anything other Poor access to EOLC for patients with anything other than a cancer diagnosisthan a cancer diagnosis
•• Changes in national social policy contextChanges in national social policy context•• Escalating costs of all service provision means becoming Escalating costs of all service provision means becoming
better at targeting needbetter at targeting need•• Personalisation, choice & control agendaPersonalisation, choice & control agendagg•• Patients / families want to make most of final months of Patients / families want to make most of final months of
lifelife•• No time to waste waiting for numerous assessmentsNo time to waste waiting for numerous assessments•• Retain independence, mobility & quality of life for as long Retain independence, mobility & quality of life for as long
as possibleas possible•• We don’t get 2We don’t get 2ndnd chances to get it right in EOLCchances to get it right in EOLC
3/27/2012
34
CareCare--Plus research was based upon two main themes Plus research was based upon two main themes and set out to answer the following:and set out to answer the following:
1. Does providing better co1. Does providing better co--ordination of care enable ordination of care enable patients and carers to enact their own choices for EOLCpatients and carers to enact their own choices for EOLCpatients and carers to enact their own choices for EOLC patients and carers to enact their own choices for EOLC (e.g Preferred Place of Care or PPC) & help them to (e.g Preferred Place of Care or PPC) & help them to better control and improve the end of life experience? better control and improve the end of life experience?
2. Does the provision of a higher level of carer support 2. Does the provision of a higher level of carer support services & earlier intervention services & earlier intervention
–– prevent individual difficulties from reaching crisis pointprevent individual difficulties from reaching crisis point–– allow health and social care providers to forecast allow health and social care providers to forecast
future usagefuture usage–– Enable better support planning and delivery of betterEnable better support planning and delivery of betterEnable better support planning and delivery of better Enable better support planning and delivery of better
services to those who need them most services to those who need them most –– reduce the need to use more intensive / expensive reduce the need to use more intensive / expensive
health and social care services at a later stage i.e. health and social care services at a later stage i.e. emergency bed days, emergency respite for the emergency bed days, emergency respite for the patient and/or carer, avoid caring role breakdown?patient and/or carer, avoid caring role breakdown?
The Benefits (1)The Benefits (1)For the patient & carer:For the patient & carer:
-- Improved Choice & Control Improved Choice & Control -- Improved Quality of LifeImproved Quality of Life-- Fast track access to services Fast track access to services -- Better quality of support services at the time they are Better quality of support services at the time they are neededneededSingle point of accessSingle point of access one contact number forone contact number for-- Single point of access Single point of access -- one contact number for one contact number for everythingeverything
-- Early intervention & advocacy avoids escalationEarly intervention & advocacy avoids escalation-- PersonPerson--centred delivery i.e. What is needed not ‘what centred delivery i.e. What is needed not ‘what we can offer’we can offer’
-- A flexible & responsive service geared towards theirA flexible & responsive service geared towards theirindividual needsindividual needs
The Benefits (2)The Benefits (2)For Commissioners: For Commissioners:
-- integrated approach to service delivery addressing integrated approach to service delivery addressing all health & social care needsall health & social care needs
-- flexible & responsive serviceflexible & responsive service-- tailored to individual needtailored to individual need-- single point of accesssingle point of accessgg-- significant cost savings on emergency bed day significant cost savings on emergency bed day
usage usage -- enable more effective forward planning of enable more effective forward planning of services & budgetsservices & budgets
-- iimproved communication between service mproved communication between service providers, patient & carersproviders, patient & carers

3/27/2012
35
How Did We Achieve This?How Did We Achieve This?
Provided an enhanced Carer Support service tailored to specific needsProvided an enhanced Carer Support service tailored to specific needsof carers and patients, including:of carers and patients, including:
•• A community based coA community based co--ordinator liaising / negotiating fast track ordinator liaising / negotiating fast track access protocols to health & social care services access protocols to health & social care services
•• Holistic assessment of carers & patients support needsHolistic assessment of carers & patients support needs•• Early intervention & advocacy in any areaEarly intervention & advocacy in any area•• 1:1 Emotional support1:1 Emotional support•• Advice & informationAdvice & information•• Home based delivery organised around patient /carer needsHome based delivery organised around patient /carer needs•• Dedicated Carers Welfare Benefits service Dedicated Carers Welfare Benefits service •• Stress management Stress management ––Counselling, complementary therapiesCounselling, complementary therapies•• Carers respite breaksCarers respite breaks•• Financial support (emergency grants fund, applications to charitable Financial support (emergency grants fund, applications to charitable
funders)funders)•• Bereavement planning & post bereavement supportBereavement planning & post bereavement support•• Carers Direct Payments assessmentsCarers Direct Payments assessments
Carers/Patients ExperienceCarers/Patients Experience
•• “Generally I think it is the knowledge of knowing somebody is there “Generally I think it is the knowledge of knowing somebody is there to assist you, makes you feel like you are not on your own, and you to assist you, makes you feel like you are not on your own, and you can do it.”can do it.”
•• “Yes, he was so patient and helpful . . . We feel comfortable with “Yes, he was so patient and helpful . . . We feel comfortable with him and feel we can talk to him about anything even if it’s of a him and feel we can talk to him about anything even if it’s of a personal nature, things we wouldn’t even tell our GP.”personal nature, things we wouldn’t even tell our GP.”
•• “If I ever had a problem, [the Care Plus Coordinator] would be the “If I ever had a problem, [the Care Plus Coordinator] would be the first person I would call. It is wonderful to know that he is at the end first person I would call. It is wonderful to know that he is at the end of the phone.”of the phone.”
•• “I can’t believe Tower Hamlets can afford this service, it has offered “I can’t believe Tower Hamlets can afford this service, it has offered us so much and has made both our lives so much easier.”us so much and has made both our lives so much easier.”
Source: CareSource: Care--Plus Yr 2 Evaluation ReportPlus Yr 2 Evaluation Report--Arup, Dec 2008Arup, Dec 2008
Professional’s Experience of CareProfessional’s Experience of Care--PlusPlus
‘Health care professionals who have referred patients into the project‘Health care professionals who have referred patients into the project
have reported that they have been freed up to carry out their primaryhave reported that they have been freed up to carry out their primary
role and develop a more satisfactory relationship with patients aroundrole and develop a more satisfactory relationship with patients around
di l d Cli i i d f i l i t i d t f thdi l d Cli i i d f i l i t i d t f thmedical need. Clinicians and professionals interviewed as a part of themedical need. Clinicians and professionals interviewed as a part of the
project overwhelmingly said that the service works extremely well andproject overwhelmingly said that the service works extremely well and
that they have a great deal of confidence referring their patients to thethat they have a great deal of confidence referring their patients to the
project ‘ project ‘
(Source: LBTH Health Scrutiny Panel End of Life Care in Tower Hamlets report to(Source: LBTH Health Scrutiny Panel End of Life Care in Tower Hamlets report to
Cabinet, May 2009)Cabinet, May 2009)
Criteria for admission to CareCriteria for admission to Care--PlusPlus
•• the patient must live in Tower Hamlets, the patient must live in Tower Hamlets,
•• be suffering from End Stage Heart Failure be suffering from End Stage Heart Failure --NYHA Stage NYHA Stage 3 or 4 (see table)3 or 4 (see table)
•• the carer must be aged over 18the carer must be aged over 18the carer must be aged over 18 the carer must be aged over 18
•• the referring cardiac consultant, GP or other health the referring cardiac consultant, GP or other health professional must answer the ‘surprise question’ i.e. professional must answer the ‘surprise question’ i.e. “Would you be surprised if the patient is still alive in 12 “Would you be surprised if the patient is still alive in 12 months time?” If the answer is yes, the referral is months time?” If the answer is yes, the referral is accepted.accepted.

3/27/2012
36
ClassClass Patient SymptomsPatient Symptoms
Class I (Mild)Class I (Mild) No limitation of physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, or dyspnoea (shortness of breath).
Class II (Mild) Class II (Mild) Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in fatigue, palpitation, or dyspnoea.
NYHA Heart Failure Classification
dyspnoea.
Class III Class III (Moderate) (Moderate)
Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes fatigue, palpitation, or dyspnoea.
Class IV (Severe) Class IV (Severe) Unable to carry out any physical activity without discomfort. Symptoms of cardiac insufficiency at rest. If any physical activity is undertaken discomfort is increased.
Stage 3 or 4 =End of Life stage or 6-12 months
In practice, Care-Plus means:- Referrals accepted by phone, fax & email, response time of 48 hrs to contact carer
- Assessment ordinarily within 5 working days & outcomes reported back to referrer as standard
- Home visits if desired as standard
- Referrals e.g OT, social care teams, Carers Handyman Service, Carers Relief Service, Link Age Plus, St Hilda’s, housing providers
- Feedback of patient/carer experiences enable providers to address issues
- Explanation of patient/carer choices and entitlements in lay terms
- Assessment of Carers one-off Direct Payments
- Liaison between all services providing health & social care services including GP, District & Heart Failure nurse team, hospital teams & ward staff, St Joseph’s Hospice, Palliative Care teams, Cardiac Outpatients, Out of Hours services
- Debt / welfare benefits/ financial management support including unlocking occupational pensions for carers forced to give up work to care
-Temporary equipment loan: wheelchair, mobile phones
- Priority access to emergency Samaritan grants fund
- Access to services at the time they are needed. i.e. Defined pathways and protocols where an earlier and more intensive intervention can be shown to be beneficial to patient and/or carer providing fast track referral, assessment and response
- Single point of access & information for carers & professionals
- Community based co-ordinator whose role it is to link with and bring together health & social care services in a way that benefits patient, carer and family
- Better design and co-ordination of services i.e. identifying & providing what is needed by people during EOLC rather than ‘this is what we offer’,
- Independent advocacy for patient and carers to challenge the barriers in existing systems & provide support when things go wrong
- A range of tailored services to support and help the carer to manage in their caring role for as long as they feel able or want to do so.
- Improved communication between professionals, patient, carer and family,
- A voluntary sector provider able to flex & bend according to service user need
Case Audit OutcomesCase Audit Outcomes--March 2012March 2012•• 132 unpaid carers caring for 128 patients132 unpaid carers caring for 128 patients
•• 4860 contacts 4860 contacts ––carers / patients or professionalscarers / patients or professionals
•• 2732 hours of pure casework2732 hours of pure casework
•• 37 deaths to date 37 deaths to date -- 29 at home, 8 in hospital29 at home, 8 in hospital
•• 1138 emergency bed days used for 37 deceased patients during last 12 1138 emergency bed days used for 37 deceased patients during last 12 months of life months of life -- total cost =£2,845,000 THPCT assumes 2 unplanned total cost =£2,845,000 THPCT assumes 2 unplanned admissions in last year of life i.e. 37 days @ £2500 per day or £92,500 per admissions in last year of life i.e. 37 days @ £2500 per day or £92,500 per y y @ p y py y @ p y ppatient.patient.
•• 8 patients used total of 712 Emergency bed days8 patients used total of 712 Emergency bed days--average 89 per patientaverage 89 per patientThe remainder used 426 bed days between them bringing down average The remainder used 426 bed days between them bringing down average usage for that group of patients to just 14.68 bed days per patientusage for that group of patients to just 14.68 bed days per patient
•• Average expenditure on bed days per CareAverage expenditure on bed days per Care--Plus patient =£76,891Plus patient =£76,891
•• Emergency bed days saved=646 saving £1,615,000 or 17 days per patientEmergency bed days saved=646 saving £1,615,000 or 17 days per patient
•• Of the 37 deaths, 6 patients did not use any emergency bed days & were Of the 37 deaths, 6 patients did not use any emergency bed days & were cared for entirely at home where they chose to be cared for entirely at home where they chose to be
3/27/2012
37
Case Audit Outcomes (2)Case Audit Outcomes (2)• 15 patients died after 18 months or more on Care-Plus
• Very high satisfaction (97.6%) levels amongst both carers & patients using Care-Plus services
• 2 complaints re poor hospital EOLC, 1 investigation by Healthcare Commission
• Almost every case involved housing issues-repairs, adaptations, medical transfers, bidding for properties, parking, access ramps, overcrowding tenancy inheritance maintaining mobility of carer &overcrowding, tenancy inheritance, maintaining mobility of carer & patient & their ability to avoid becoming housebound & isolated from social networks & their communities.
• Additional welfare benefits obtained in 92% of cases
• Grant applications have provided fridge/freezers, cookers, beds & bedding, driving lessons for carers, wheelchairs, portable nebulisers, washing machines, used cars, LBTH Leisure Cards, holidays
• Bereavement counselling referrals = nil
Service CostsService Costs
Heart Failure only Heart Failure only --£144k per year £144k per year -- 3 3 ftefte staff for 225 staff for 225 patients & their carers patients & their carers
or or
the cost of 57.6 emergency bed daysthe cost of 57.6 emergency bed days
Heart Failure & COPD Heart Failure & COPD -- £226k per year£226k per year-- 5 5 ftefte staff for staff for caseload of 375 patients & their carerscaseload of 375 patients & their carers
oror
the cost of 90 emergency bed daysthe cost of 90 emergency bed days
For more information contact:For more information contact:
CareCare--Plus CoPlus Co--ordinatorordinatorThe Carers CentreThe Carers Centre
21 21 BrayfordBrayford SquareSquare
StepneyStepney
LondonLondonLondonLondon
E1 0SGE1 0SG
Tel: 020 7790 1765Tel: 020 7790 1765
Fax: 020 7791 5575Fax: 020 7791 5575
www.carerscentretowerhamlets.org.ukwww.carerscentretowerhamlets.org.uk
Email: Email: [email protected]@carerscentretowerhamlets.org.uk
Or Or [email protected]@carerscentretowerhamlets.org.uk
Any Questions?Any Questions?

3/27/2012
38
DYING MATTERS, ADVANCE CARE PLANNING & ETHICAL DILEMMAS
www.ncpc.org.uk www.dyingmatters.org
BEATING THE BARRIERS
March 2012
SIMON CHAPMAN
Director of Policy & Parliamentary Affairs
In 20 minutes
• Dying Matters – let’s talk about it
• Leading to advance care planning
Ethi l dil
www.ncpc.org.uk www.dyingmatters.org
• Ethical dilemmas
“Many consider death to be the last great taboo in our society and ….most of us find it hard to engage in advance with the way
www.ncpc.org.uk
it hard to engage in advance with the way in which we would like to be cared for at
the end of life.”
End of Life Care Strategy, Department of Health, 2008
www.dyingmatters.org

3/27/2012
39
The Dying Matters Coalition
• Set up by the National Council for Palliative Care, the umbrella charity for all those involved in palliative care, to support the 2008 End of Life Care Strategy
• It is a broad based, inclusive national Coalition, working in partnership, with over 16,000 members from across the NHS,
www.ncpc.org.uk
p p ,voluntary and independent health & care sectors, social care, housing, faith, community and retirement organisations, schools, legal, insurance, funeral & wider commercial sectors.
•“Support changing knowledge, attitudes and behaviours towards death, dying and bereavement, and through this to make ‘living and dying well’ the norm.”
Our Mission:
Our Greatest Fear
How scared are you of the following happening to you?
• Dying in pain 83%
• Dying alone 67%
www.ncpc.org.uk
• Being told you are dying 62%
• Dying in hospital 59%
Compare with:
• Going bankrupt 41%
• Divorce/end of a long-term relationship 39%
• Losing your job 38%ComRes 2011
Taboos have consequences
• Deciding not to talk is just that – a decision....
• Our families & carers may not know what we want
• If we don’t discuss, anticipate and plan, it makes “ ”
www.ncpc.org.uk
unplanned “crisis care” and hospital admission more likely
• Impact on funerals – what would s/he want?
• Bad care impacts bereavement
• Harder to challenge bad care
• No Dress Rehearsals – we only get one chance to get it right
www.dyingmatters.org www.ncpc.org.uk www.dyingmatters.org

3/27/2012
40
Different triggers;Similar conversations
www.ncpc.org.uk
THE END OF LIFE CARE STRATEGY
“The most important objective is to ensure that people’s individual needs, their priorities, their preferences for end of life care are identified, they are documented, they are reviewed, they are respected and acted upon wherever
www.ncpc.org.uk www.ncpc.org.uk
possible. Now that message has to go out everywhere within the NHS and I think that’s the important starting point for everything else…”
Alan Johnson, Secretary of State for Health, speaking on Radio 4’s Today programme at the launch of the End of Life Care strategy, on 16 July 2008
ADVANCE CARE PLANNING (ACP)
• ACP is a continuing & voluntary process of discussion between an individual and their care providers. ACP discussions may include:– The individual’s concerns– Their important values or personal goals for care
www.ncpc.org.uk www.ncpc.org.uk
Their important values or personal goals for care– Their understanding about their illness and prognosis– Their preferences for types of care or treatment that may be
beneficial in the future and the availability of these
• If an individual wishes their family & friends may be included
• The Mental Capacity Act (2005) provides an underlying legal framework. The person’s views must be taken into account.
• Preferred Priorities of Care is a tool that can capture this
Some possible examples
• “If I am being washed, I prefer showers to baths• I am allergic to lanolin; please don’t put me in lambswool
clothes or give me hand cream with lanolin in it• I hate boiled eggs and I love Marmite
www.ncpc.org.uk www.ncpc.org.uk
• I hate boiled eggs, and I love Marmite• I want to stay at home as long as I can• No, not the Archers, please no.• Bach for me please, not Coldplay• I‘m ready to die, please don’t give me antibiotics again• I am frightened of injections and needles• Please could my grandson look after the cat?”
3/27/2012
41
How can people use the MCA to express/protect their wishes & choices if incapacitated?
• Appoint a proxy decision-maker under an LPA
• Refuse specific treatments in advance
• In anticipation of other people assessing their best f
www.ncpc.org.uk www.ncpc.org.uk
interests in the future:
– Nominate somebody to be consulted (friend/relative)
– Identify who should not be consulted
– Make written statements about their values, priorities & preferences – these must be taken into account (Advance Care Planning)
Interested family, friends & carers
• Protected decision-making for all professional and informal carers (if they reasonably believed a person lacked capacity & the act was in his/her best interests)
www.ncpc.org.uk www.ncpc.org.uk
interests)
• They must be consulted about the person’s best interests where practicable
• Challenge decisions, if felt not to be in best interests
• Be appointed as a Lasting Power of Attorney
• Apply to be appointed as a Deputy by the court
Some ethical & practical dilemmas
• Managing discussing & living with uncertainty
• Clinically assisted nutrition & hydration
www.ncpc.org.uk
Clinically assisted nutrition & hydration
• Antibiotics
• ICDs
• Relationship between person at eol & carers
• Right approach rather than right answer?www.dyingmatters.org
ICDs
• Discussion at implantation
• Deactivation
Aft d th
www.ncpc.org.uk
• After death:
• Part of the person’s body
• Removal
• Part of the person’s estate
www.dyingmatters.org

3/27/2012
42
Difficult Conversations series Helping professionals and carers talk more openly about the end of life
www.ncpc.org.uk www.dyingmatters.org
Difficult Conversations for people with COPD
www.ncpc.org.uk
Planning ahead
www.ncpc.org.uk www.dyingmatters.org

3/27/2012
43
Talking about ICD DeactivationICD Deactivation
Annie MacCallumProfessional Lead for Specialist Services
Gloucestershire Care Services
Implantable cardioverter-defibrillator (ICD)
ICD Evidence
• Treatment of choice for risk of sudden cardiac death from ventricular arrhythmias
• Superior to Antiarrhythmic drugs in primary and secondary prevention of Sudden Cardiac Deathy p
• As indications for ICD continue to expand the population of patients with devices continues to grow.
• Guidelines focus on device indications, implantation and training

3/27/2012
44
ICD Implants 1999 – 2009Clinical Audit of Heart Rhythm Device Implantation in 2009
ICD Deactivation Why is this important?
• All patients will ultimately reach end of life• From underlying heart condition• From another terminal illness• Improving ‘dying process’ in ICD patients• Improving dying process in ICD patients
presents unique challenges• ICD deactivation discussions rare• Ethical dilemmas• Most patients die with active ICD
Clinical importance
• Terminally ill people may develop hypoxia, sepsis, pain, heart failure and electrolyte disturbance
• Risk of increasing arrhythmia and• Risk of increasing arrhythmia and frequency of shocks
• Shocks can be physically painful and psychologically distressing for patients and families.
“His defibrillator kept going off…. It went off 12 times in one night…..He went in and they looked at it… they said they adjusted it and sent him home The next day weit and sent him home. The next day we had to take him back because it was happening again. It kept going off and it wouldn’t stop going off.”
Lampert R et al. Heart Rhythm (2010) 7 (7). 1008-1026
3/27/2012
45
Deactivation Guidelines
• Up to date guidelines addressing the legal, ethical and religious principles underlying device deactivation either by patient request or at end of life
• Led to development of consensus statements in Europe and USA to support clinicians based on legal and ethical principles as well as clinical, scientific and technical experience
Consensus Statements
• EHRA expert Consensus Statement on the management of cardiovascular
• HRS Expert Consensus Statement on the Management of Cardiovascular
implantable electronic devices in patients nearing end of life or requesting withdrawal of therapy
Padeletti L et al. Europace (2010)12.1480-1489
Implantable Electronic Devices (CIEDs) in patients nearing end of life or requesting withdrawal of therapy
Lampert R et al. Heart Rhythm (2010) 7 (7). 1008-1026
Consensus Statements
• Increasing number of Health Care Professionals (HCP) treating ICD patients have cared for dying patients and participated in device deactivation
• Understanding of device deactivation variesg
• HCP uneasiness discussing device management at end of life
• Few patients and families discuss deactivation prior to the days preceding death even if Do Not Resuscitate order is in place
Timely Discussion
• Treat each person as an individual. One communication option will not suit everyone
• ICD deactivation options should be included in pre-implantation informed consentp p
• At time of implantation the possibility of deterioration in health and ICD deactivation could be discussed if appropriate
• If not at implantation the subject could be discussed at later follow up sessions

3/27/2012
46
Timely Discussion
• Or if the patient is becoming more ill and not returning to former good health
• When considering advanced care planning and natural death ICD deactivation shouldand natural death, ICD deactivation should form part of the discussion
• ICD physician should be informed if there is a new significant diagnosis or significant change in patient health
Talking about it
• Equip staff with skills to open the subject E.g. Advanced communication courses
• Encourage open discussions if patients and families ask about thisand families ask about this
• Signpost to other help if necessary
• Direct enquirers to further information –Specialist Team, Arrhythmia Nurse
Signposting
• British Heart Foundation bhf.org.uk
• Arrhythmia Alliance www.heartrhythmcharity.org.uk
Informed Consent
• Ethical and legal obligation • Mode of deactivation discussed• Clarify legal and ethical right to refuse• Can always reconsider if decision changes• Can always reconsider if decision changes• A copy of the signed consent for
deactivation must be included in medical record
• Mental capacity or not, all are due equal concern and respect
3/27/2012
47
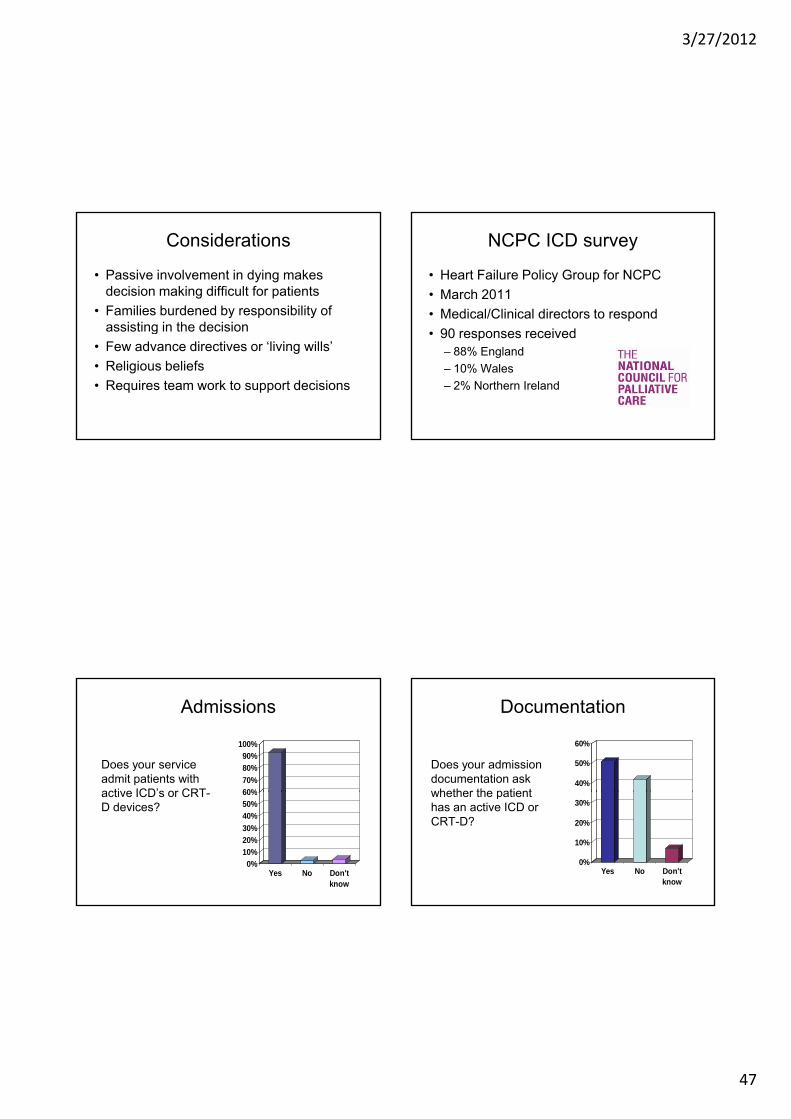
Considerations
• Passive involvement in dying makes decision making difficult for patients
• Families burdened by responsibility of assisting in the decisionassisting in the decision
• Few advance directives or ‘living wills’
• Religious beliefs
• Requires team work to support decisions
NCPC ICD survey
• Heart Failure Policy Group for NCPC
• March 2011
• Medical/Clinical directors to respond
• 90 responses received– 88% England
– 10% Wales
– 2% Northern Ireland
Admissions
Does your service admit patients with active ICD’s or CRT 60%
70%
80%
90%
100%
active ICD s or CRT-D devices?
0%
10%
20%
30%
40%
50%
60%
Yes No Don'tknow
Documentation
Does your admission documentation ask whether the patient
40%
50%
60%
whether the patient has an active ICD or CRT-D?
0%
10%
20%
30%
Yes No Don'tknow

3/27/2012
48
Documentation
• 42% (29/69) had another prompt for documenting active ICD or CRT-D– Pathway documentation e.g. Liverpool Care
P thPathway
– Device prompt on electronic patient record
– Referral form
– Access to hospital notes
– Verbal liaison with local HFSN
Shocks
• Only 4 out of 36 services reported an ICD shock delivered while in their care– 2 services said that a patient received multiple
shocksshocks
• 5 didn’t know if shock had happened– 3 Hospice
– 1 NHS
– 1 Hospice at home
ICD Deactivated under the care of service in last 12 months
Patient Services Percentage
None 9 25%
1 17 47%
2 5 14%
3 2 6%
4 1 3%
5 or more 1 3%
Don’t know 1 3%
Formal Deactivation Policy?
• The survey prompted some sites to formulate one!
• Some felt best to
13%
13%
13%Yes
Yes• Some felt best to deal with on case by case basis as numbers small
• 25% (12/48) ICD policy linked with DNR policy
61%
YesRegional
No
Don'tKnow

3/27/2012
49
ICD Deactivation Policy
• Consult with key health professionals in formulating policy
• Consult with palliative care
I l ti t t ti• Involve patient representatives
• Consider pathway for forward planning and urgent scenarios
• Must cover an entire health community
• Circulate and communicate widely
Summary
• Increase knowledge and understanding within MDT about ICD deactivation
• Access to legal and expert support if necessary to assist in decision makingnecessary to assist in decision making
• Consider mental capacity issues
• Involve patients, families and MDT
• Promote local ICD deactivation policy widely
Any questions

3/27/2012
50
Sarah Bowater
Discussing End of Life in Adult Congenital Heart Disease
Sarah BowaterQueen Elizabeth Hospital, Birmingham
22nd March 2012
Congenital heart disease – the size of the problem
Affects 1 in 145 births
Increasing numbers: 50 years ago: 25% survival to adulthood y g >90% survival now Predicted annual increase of 2500 adults with ACHD
DoH model in 2000: Total number in UK: approx 130,000 Simple: 63,257 Complex: 16, 878
The patients Simple:
Curative surgery or un-operated
Only very simple have normal life expectancy
Complex: Complex: Un-operated
“Curative” surgery
Palliative surgery

3/27/2012
51
Survival in ACHD
Engelfriet et al. EHJ 2005;26:2325-2333
Mode of death in ACHD
Oechslin et al. Am J Cardiol 2000 Nov 15; 86(10):1111-6
Fontan operation 81.6% 15 year survival rate
Ohuchi et al. Ann Thorac Surg2011 Oct;92(4):1457-1466
10% of adults in NYHA III/IV
Engelfriet et al. EHJ 2005;26:2325-2333
Hypoplastic Left Heart Syndrome
70% of newborns now expected to reach adulthood
Early survivors now reaching ACHD clinics
Survival does not imply continued success
After Norwood stage 3

3/27/2012
52
Issues that we face
Change from life-prolonging to palliative approach
Young patients
Unpredictable prognosis
Often no “trigger”
Difficulty in identifying dying phase
Lack of experience
Complex physiology
Our patients’ perspectives…..
“I survived before…what’s different
this time?”
“You’re too young to have a heart problem”
Young patients Different perceptions of risk
Parents Children of their own
Discussing end of life
Proactive approach leads to “better dying experience”
Little data regarding end of life preferences and care in ACHDACHD
Early discussions beneficial in acquired heart failure
Life time condition – when to discuss?
Discussing end of life – are we any good? Tobler et al1
Survey of 200 patients and 48 doctors 1% patients reported end of life discussion vs 50% doctors Patients in favour of starting discussions earlier Independent of disease complexity and socioeconomic factors
Tobler et al2 48 hospital deaths from ACHD 5 patients had documented end of life discussions (3 prior to admission) 9 patients referred to Palliative Care services
1. Int J Cardiol 2012 Mar;155(3):383-3872. Palliative Med 2012 Jan;26(1):72-9
3/27/2012
53
Our practice in Birmingham
Appropriate timing of transition to adult care
Honesty and openness
Individualised approachpp
Team approach to decision making
Specialist ACHD Nurse-led counselling sessions
Palliative Care team involved when appropriate
When we haven’t managed it well
18y old male Complex congenital heart disease under the care of paediatricians
Transferred from DGH with worsening heart failure Angry that not at his familiar paediatric centre
R l li Reluctant to listen to us
Decision made not suitable for transplantation Bad news broken by relative strangers – little trust Friday before BH weekend, most of team away Rapid deterioration and died 2 days later without seeing palliative care
team
When we have managed it well (1) 49y old male
Late Fontan operation for tricuspid atresia
Admitted with increasing peripheral oedema and dyspnoea
Transplant discussed and assessment commenced early
CMR demonstrated massive thrombus in Fontan circulation
Supportive care in hospital and community
Died 6 weeks after discharge
When we have managed it well (2) 46 year old female
Eisenmenger syndrome
Collapse in 2010 followed by slow deterioration
Offers of formal Palliative Care input rejected
Talks regarding prognosis limited by patient
Direct contact with team regarding concerns
Died in local hospital of heart failure after short admission

3/27/2012
54
What next…
Large increases in numbers of adults with complex CHD
Early identification
Early discussion
Collaboration with other ACHD units
Learn from other specialities
“I urge you to continue to be positive when possible…..there are times when a cold clinical appraisal can have a negative effect I guess that to make such a effect…. I guess that to make such a judgement is one of the most difficult things you do.”
Getting care right in every setting:Supporting older people with
heart failure in hospitalheart failure in hospitalJohn Baxter
Consultant in Care of the ElderlySunderland Royal Hospital

3/27/2012
55
bgs.org.uk
BRITISH SOCIETY FORHEART FAILURE
bsh.org.uk
Sunderland: The promised land
� Population 330,000
� 8.3% aged >75
� 98% Caucasian
Hi h d f i l� High degree of social deprivation
� High mortality rates– IHD 865/100,000 pop
65-74 (Nat av 661)
…..died peacefully in hospital, thanks to Dr Baxter
Getting the care right in hospital
� Case Identification– Facilitating high quality care
� Advance care planning– Advance statement
Best interest decision– Best interest decision– Palliative care registers
� End of life care in hospital– Recognising a dying patient– Managing expectations– Liverpool Care of the dying pathway

3/27/2012
56
Place of Death: CHF patients 2001-07
60
70
80
90
0
10
20
30
40
50
Deaths
HomeHospital
� At home
� Privacy and dignity
� Surrounded by loved onesones
� Symptom free
� At home
� Privacy and dignity
� Surrounded by loved ones
� BUT…
� Don’t want to be a burden to my loved onesones
� Symptom free
ones
� NOT YET!!!!

3/27/2012
57
� At home
� Privacy and dignity
� Surrounded by loved ones
� BUT…
� Don’t want to be a burden to my loved onesones
� Symptom free
ones
� NOT YET!!!!
CHF EOL: Case Identification
� The surprise question:– Would you be surprised if your patient died
within the next 12 months?
COTE CHF Survival
� Mean survival improving– Now 2.6 years
� Stable CHF patients
survivalmonths
120.00100.0080.0060.0040.0020.000.00
Cu
m S
urv
ival
1.0
0.8
0.6
0.4
0.2
0.0
LVDD-censored
EF<40%/DescrLVSD-censored
LVDDEF<40%/DescrLVSD
ECHO
Survival Functions
� Stable CHF patients– Mean age 82
– 10% mortality per year
0 15 30 45 60 75
Months
0.0
0.2
0.4
0.6
0.8
1.0
Sur
viva
l
Kaplan-Meier Survival Curve for Hear Failure Data

3/27/2012
58
A POOR PROGNOSIS IS FOUND IN CHF PATIENTS WITH ANY OF THE FOLLOWING:
� High symptom burden both physical and psychological despite optimal treatment
� Intractable oedema despite high dose loop and thiazide diureticsTh d i i h i l i h d d CHF� Three admissions to hospital with decompensated CHF in last 6 months
� Progressive deterioration in renal function� Cardiac cachexia, resistant hyponatraemia, low serum
albumen, comorbidity with poor prognosis.� Advanced age
The Surprise question The Surprise question
Adverse Prognostic Markers

3/27/2012
59
The Surprise question
Adverse Prognostic Markers
Patient Wishes
Getting the care right in hospital
� Case Identification– Facilitating high quality care
� Advance care planning– Advance statement
Best interest decision– Best interest decision– Palliative care registers
� End of life care in hospital– Recognising a dying patient– Managing expectations– Liverpool Care of the dying pathway

3/27/2012
60
Cognitive Impairment is Common
� Stable Chf patients
� EF<40%
� 53% in Italian StudiesZuccala J Neurol
29%N=150
– Zuccala J Neurol Neurosurg Psy 1997
MMSE<24
Jones et al Age and Ageing (2003) 32:
suppl 1;4
Are CHF patients on a palliative care register?
60
70
80
90
0
10
20
30
40
50
Palliative Care Register
YesNo
Getting the care right in hospital
� Case Identification– Facilitating high quality care
� Advance care planning– Advance statement
Best interest decision– Best interest decision– Palliative care registers
� End of life care in hospital– Recognising a dying patient– Managing expectations– Liverpool Care of the dying pathway

3/27/2012
61
National CHF audit
� 42% CHF admissions managed on cardiology wards
� Mortality– 6% cardiology wards
– 12% General wards
� 4% CHF inpatients receive specialist palliative care input
Primary care presentation
1: Urgent referral for people with
previous myocardial infarction
Assessment and diagnosis
3: 2-week assessment and
diagnosis
4: 6 week
Management
6: Multidisciplinary heart failure team
7: Treatment with
Admitted patients
10: Management plans for people
admitted to hospital
Moderate to severe chronic heart failure
13: Specialist and palliative care for
people with moderate to
severe chronic heart failure
NICE QUALITY STANDARDS for CHF 2011
2: Measuring serum natriuretic
peptides
4: 6-week assessment and
diagnosis
7: Treatment with ACE inhibitors, ARBs and BB
8: Cardiac rehabilitation programme
9: Monitoring stable chronic heart failure
11: Contribution of
multidisciplinary heart failure team to management
plans
12: Hospital discharge and follow-up care
Recognising a patient is dying
� Adverse Prognostic Markers
� Early Warning Score– Systolic BP
– Heart Rate
– Respiratory rate
– Temperature
– AVPU
How to recognise a CHF patient is dying

3/27/2012
62
Sentenced to death on the NHSSentenced to death on the NHS
Patients with terminal illnesses are being made to die prematurely under an NHS scheme to help end their lives, leading
doctors have warned.
� Team based decision
� Patient and carer i linvolvement
� Regular review
� Not suitable for all dying patients
3/27/2012
63
Will LCDP control symptoms in dying CHF patients?
� PRN anticipatory meds for LCDP– Diamorphine 2.5mg subcut PRN
– Hyoscine 400 mcg subcut PRN
– Cyclizine 50mg subcut PRN
– Midazolam 2.5mg subcut PRN
Do LCDP PRN drugs control symptoms?
Symptoms controlled
PRN drugs changedto regular
N=98
Getting the care right in hospital
� Case Identification– Facilitating high quality care
� Advance care planning– Advance statement
Best interest decision– Best interest decision– Palliative care registers
� End of life care in hospital– Recognising a dying patient– Managing expectations– Liverpool Care of the dying pathway
Getting care right in every setting:Supporting older people with
heart failure in hospitalheart failure in hospitalJohn Baxter
Consultant in Care of the ElderlySunderland Royal Hospital
3/27/2012
64
Beating The Barriers –Supporting Patients in the
Community
Dr Nigel RowellGP, The Endeavour Practice
Middlesbrough
Declaration
I do solemnly swear that I have taken money from Menarini, Servier, Pfizer and Boehringer
in exchange for my intellect.
I needed the cash for my boat.
Which my wife knows nothing about.
Heart Failure Quality Standards andPrimary Care
No.1 Patients with ?HF and prev. MI referred urgently
No.2 Use BNP in suspected HF
Off d i dNo.5 Offer education and support
No.7 offer ACEI and BB
No.9 Review status/meds and U/Es 6 monthly
No.13 Moderate‐severe CHF have access to HF Specialist and Palliative Care Service

3/27/2012
65
How many patients are there?
• Incidence 1% per annum overall but up to 12% in 80 yrs+ (Cowie 1999)
• Prevalence 1.6%
G d QO fi 0 %• GP data – QOF figures 0.7%
• 65 patients on our list of 7,100
How do Heart Failure Patients present?
• About 30% Chronic : 70% Acute
• Earlier pick up will improve outcome
• Emergency admissions high mortality
• New MI/ Dysrhythmia accounts for decompensation
• 50:50 achievable through selected screening
Finding them after they hit hospital acutely
• Elderly don’t like to bother us
• See tablets as a “course”
• Feel better – “job done”
• End up back in
• Co‐morbidities
3/27/2012
66
Bolton The Urgent Care Clinical Dashboard
Name NHS Number DoB Type Date Time Provider Specialty Additional Information
Pennock, Lucy 633 864 7851 30/08/96 Admission 20/03/12 22:06 South Tees PaediatricsEmergency - A&E Dept/Dental Casualty - JCUH Ward 21
Ahmed, Hiwa 710 314 5903 09/04/10 Admission 20/03/12 19:43 South Tees PaediatricsEmergency - Bed Bureau - JCUH Paediatric Day Unit
Thistlethwaite, Jacqueline 484 850 3337 01/03/60 Admission 20/03/12 15:48 South Tees General MedicineEmergency - A&E Dept/Dental Casualty - JCUH Ambulatory Emergency Care Dept
Wiles, Ann 464 360 8714 14/08/36 Admission 20/03/12 12:34 South Tees General MedicineEmergency - GP - JCUH Ambulatory Emergency Care Dept
Mccabe, Lilly-Isobelle 700 696 5403 15/01/10 Admission 20/03/12 10:41 South Tees PaediatricsEmergency - A&E Dept/Dental Casualty - JCUH Paediatric Day Unit
Mccormick, Louisa 430 383 8918 03/05/28 Admission 20/03/12 06:38 South Tees Accident & EmergencyEmergency - A&E Dept/Dental Casualty - JCUH Ward 37
Phillips, Margaret 448 308 1772 27/06/53 Admission 19/03/12 10:55 South Tees Anaesthetics & Itu Emergency - Bed Bureau - JCUH Main Itu
Mendum, Phyllis 422 676 2770 18/01/42 Admission 18/03/12 21:10 South Tees Geriatric MedicineEmergency - A&E Dept/Dental Casualty - JCUH Ward 28
Escritt, Susan 484 870 7269 01/04/64 Admission 18/03/12 14:38 South Tees Geriatric MedicineEmergency - A&E Dept/Dental Casualty - JCUH Ward 28
Perry, Iris 412 982 2039 24/07/21 Admission 17/03/12 13:55 South Tees General MedicineEmergency - Bed Bureau - JCUH Acute Assessment Unit Female
Richards E a 436 467 4729 23/03/26 Admission 17/03/12 12 50 So th Tees General MedicineEmergency - Other Means - JCUH Acute Assessment Unit Female
Dashboard: Emergency Admissions
Richards, Eva 436 467 4729 23/03/26 Admission 17/03/12 12:50 South Tees General Medicine Assessment Unit Female
Smith, Jean 430 920 1016 12/12/46 Admission 16/03/12 13:00 North Tees General Medicine Emergency - A&E Dept/Dental Casualty
Richmond, David 450 565 0723 20/11/52 Admission 16/03/12 11:40 South Tees General MedicineEmergency - GP - JCUH Ambulatory Emergency Care Dept
Cheesebrough, Patricia 430 524 1013 16/05/38 Admission 15/03/12 22:41 South Tees General MedicineEmergency - Bed Bureau - JCUH Acute Assessment Unit Female
Roche, Lewis 640 191 0887 31/07/99 Admission 15/03/12 22:00 South Tees Trauma and OrthopaedicsEmergency - A&E Dept/Dental Casualty - JCUH Ward 22
Stephens, Lucy 430 749 5764 15/07/32 Admission 15/03/12 21:00 South Tees General MedicineEmergency - A&E Dept/Dental Casualty - JCUH Acute Assessment Unit Female
Collett, Jane 430 511 5921 26/10/30 Admission 15/03/12 13:46 South Tees General MedicineEmergency - Bed Bureau - JCUH Ambulatory Emergency Care Dept
Webster, Leslie 484 850 6506 02/04/60 Admission 15/03/12 10:47 South Tees General MedicineEmergency - Bed Bureau - JCUH Ambulatory Emergency Care Dept
Mcdermott, William 430 501 0747 21/03/28 Admission 14/03/12 18:00 South Tees General MedicineEmergency - Bed Bureau - JCUH Acute Assessment Unit Male
Taragos, Alexander 704 484 5711 03/04/70 Admission 14/03/12 05:53 South Tees General MedicineEmergency - Bed Bureau - JCUH Acute Assessment Unit Male

3/27/2012
67
Name NHS Number DoB Type Date Time Provider Specialty Additional Information30/08/96 A&E Attendance 20/03/12 20:31 South Tees N/A Overdose
10/04/70 A&E Attendance 20/03/12 17:19 South Tees N/A Chest Pain
20/09/47 A&E Attendance 20/03/12 15:03 South Tees N/A Muscle/Tendon Injury To Multiple Site
07/07/84 A&E Attendance 20/03/12 11:39 South Tees N/A Contusion To Wrist
09/09/97 A&E Attendance 20/03/12 09:11 South Tees N/A Contusion To Digit
15/01/10 A&E Attendance 20/03/12 08:44 South Tees N/A Contusion To Head
01/03/60 A&E Attendance 20/03/12 05:40 South Tees N/A Soft Tissue Inflamation To Hip
03/05/28 A&E Attendance 20/03/12 05:19 South Tees N/A Nerve Injury To Lower Leg
21/11/94 A&E Attendance 20/03/12 01:49 South Tees N/A Joint Injury To Neck
09/04/10 A&E Attendance 19/03/12 23:32 South Tees N/A Other
24/07/34 A&E Attendance 19/03/12 21:19 South Tees N/A Other
15/04/93 A&E Attendance 19/03/12 21:16 South Tees N/A Head Injury
12/08/06 A&E Attendance 19/03/12 20:45 South Tees N/A Head Injury
11/02/74 A&E Attendance 19/03/12 20:09 South Tees N/A Sprain/Ligament Injury To Multiple Site
09/04/10 A&E Attendance 19/03/12 14:54 South Tees N/A Gastrointestinal Condition
Dashboard: A&E Attendances
09/04/10 A&E Attendance 19/03/12 14:54 South Tees N/A Gastrointestinal Condition
25/10/04 A&E Attendance 19/03/12 13:44 South Tees N/A Muscle/Tendon Injury To Ankle
27/06/53 A&E Attendance 19/03/12 07:49 South Tees N/A
11/03/10 A&E Attendance 19/03/12 01:57 South Tees N/A Gastrointestinal Condition
07/11/73 A&E Attendance 19/03/12 01:06 South Tees N/A Chest Pain
18/01/42 A&E Attendance 18/03/12 19:42 South Tees N/A
08/04/09 A&E Attendance 18/03/12 18:42 South Tees N/A Diagnoses Not Classifiable
23/07/79 A&E Attendance 18/03/12 17:57 South Tees N/A Ent Conditions
01/04/64 A&E Attendance 18/03/12 14:03 South Tees N/A
25/10/40 A&E Attendance 18/03/12 12:04 South Tees N/A Sprain/Ligament Injury To Wrist
22/12/96 A&E Attendance 18/03/12 11:48 South Tees N/A Local Infection To Toe
13/09/59 A&E Attendance 18/03/12 11:12 South Tees N/A
25/04/61 A&E Attendance 18/03/12 07:53 South Tees N/A Uroligical Conditions (incl Cystitis)
Name NHSNumber DoB Type Date Time Provider Specialty Additional Information11/12/55 Discharge 20/03/12 17:27 South Tees Nephrology Admission Date/Time: 12/03/12 16:14
14/08/36 Discharge 20/03/12 14:37 South Tees General Medicine Admission Date/Time: 20/03/12 12:34
01/04/64 Discharge 19/03/12 14:12 South Tees Geriatric Medicine Admission Date/Time: 18/03/12 14:38
12/12/46 Discharge 18/03/12 12:10 North Tees General Medicine Admission Date/Time: 16/03/12 13:00
31/03/81 Discharge 18/03/12 12:00 South Tees Gastroenterology Admission Date/Time: 12/03/12 18:53
31/07/99 Discharge 17/03/12 13:59 South Tees Trauma and Orthopaedics Admission Date/Time: 15/03/12 22:00
20/11/52 Discharge 16/03/12 19:21 South Tees General Medicine Admission Date/Time: 16/03/12 11:40
Dashboard: Emergency Admission Discharges
16/05/38 Discharge 16/03/12 16:34 South Tees General Medicine Admission Date/Time: 15/03/12 22:41
02/04/60 Discharge 15/03/12 13:04 South Tees General Medicine Admission Date/Time: 15/03/12 10:47
03/04/70 Discharge 15/03/12 11:10 South Tees General Medicine Admission Date/Time: 14/03/12 05:53
27/06/53 Discharge 14/03/12 18:30 South Tees General Medicine Admission Date/Time: 13/03/12 22:47
30/03/38 Discharge 14/03/12 15:49 South Tees General Medicine Admission Date/Time: 13/03/12 22:55
19/11/57 Discharge 14/03/12 15:20 South Tees Clinical Haematology Admission Date/Time: 28/02/12 23:30
Now you are in the system‐meet the Practice Team!
• Coding Team
• Receptionist
• Manager
• Prescribing teamPrescribing team
• Appointments secretary
• HCA Technicians ‐ 2
• Nurses ‐ 3
• Doctors ‐ 5
The Primary Health care Team
• Heart Failure Specialist Nurse
• District Nurse
• McMillan/Hospice team/Marie Curie
• O.T. / Social Worker
• Dietetics/Pharmacist
• Welfare Rights Advisor
• Mental health team
• (GPSI in Heart Failure)

3/27/2012
68
What we do – Planned Chronic Disease Management
• Keep an eye on the co‐morbidities
• Annual Check up
• Bloods 1w prior
• Nurse led – Nurse PractitionerNurse led Nurse Practitioner
• BNP used freely / ECG
• Holistic assessment including mood, exercise, diet
• GP appointment –same day and home visit if needed
• Provide a medical “home”
Plan according to “Care Planning”RCGP 2011
• HCA for bloods
• Health promotion
• Patient sent results• Patient sent results
• Reflection and planning
• MDT paper review
• GP/ Practice Nurse appointment
And access to….
• Intermediate care – assessment e.g. GPSI in HF and palliative care
• Intermediate care – respite/rehab
• LabsLabs
• X‐ray
• Cardiac Rehab
• Secondary care
• Psychological therapies
Quality and Outcomes Framework
Indicator Points Thresholds
Records
HF1 A Register of HF 4
Initial Diagnosis
Confirmed by Echo after 2006 6 40‐90%Confirmed by Echo after 2006 or Specialist Assessment
6 40 90%
Ongoing management
LVSD with ACEI/ARB 10 40‐80%
ACEI/ARB AND beta‐blocker 9 40‐60%
And 6 points for Palliative Care ( 3 for a register
and 3 for Quarterly reviews

3/27/2012
69
What’s missing
• HF with Preserved Ejection Fraction
• Valves
• Aldosterone Blockade
• Treatment Plan
• Target Doses
• Exclusions apply
Recognising the closing overs
• Refractory symptoms despite optimal Rx
• 3 hospital admissions with decompensation in last 6 months
• Dependent for more than 3 activitiesDependent for more than 3 activities
• Cardiac cachexia
• Hyponatraemia
• Albumin <25
• Serious co‐morbidity
What are we trying to achieve?
• Avoid a “Nora P” scenario
• Ease passage
• Avoid inappropriate admission and investigation
C f h• Comfort the carers
• Make memory for family less painful and grieving less difficult
• Knowing we have the next generation to care for

3/27/2012
70
EoL in action
• Primary Care IS responsive
• Close relationship with family carries the day
• Worked as a team before
• Know strengths and weaknesses
• Hospice and sec care for advice and backup
• Cost of home care vs. hospice vs. hospital
How could we improve?
• Earlier pick up – use BNP more (monitoring?)
• Better Communications – all around
• Review twice yearly
• Aim for target doses
• Repeat ECGs
• Refer for devices more
• Dedicated Commissioning Champion
Improving – later on
• Add patients to GSF register
• Ensure benefits/DS1500
• Be proactive with frequent flyers (Community Matron?)Matron?)
• Try and pick up in chronic phase
• Ensure review by HF consultant
• Treatment plan
• Communication!!

3/27/2012
71
Heart Failure Quality Standards andPrimary Care
No.1 Patients with ?HF and prev. MI referred urgently
No.2 Use BNP in suspected HF
Off d i dNo.5 Offer education and support
No.7 offer ACEI and BB
No.9 Review status/meds and U/Es 6 monthly
No.13 Moderate‐severe CHF have access to HF Specialist and Palliative Care Service
Thanks for Listening
Ceri GriffithsCeri GriffithsCommunity Matron
Coventry and WarwickshirePartnership Trust

3/27/2012
72
Specialist HF Nurse led interventions
Preventing admissions / facilitating di hdischarges
Emotional and Psychological support
Education and Teaching
Ongoing HF Management
Care Co-ordinationPsycho-social
support
Family and Carer Support
Bereavement Support
Advanced Care Planning
Patient
Social / Environmental
Physical
•Physiotherapy
Psychological / Emotional
•Social care support•Financial advice / DS1500•Occupational Therapy •Respite•Hospice Day Services
Physiotherapy•Pulmonary / Cardiac
rehabilitation classes•Fatigue, Anxiety and
Breathlessness clinics•Equipment
•Clinical Psychology•Patient and Carer support
groups•Spiritual support•Specialist Palliative Care
Time / capacity
Changing ethos of HF care
Lack of palliative knowledge/skills
Timely referrals
Prognostication issues
Suitable patient identificationg /
Accessing social care packages
Disjointed services / locality differences
Reluctance to prescribe for adequate symptom control
Delayed hospital discharges
Withdrawing treatment
3/27/2012
73
Holistic approach and assessments of needs Early and proactive identification of patients
with Heart Failure R ti i l i f E d f Lif di i i Routine inclusion of End of Life discussions in HFNS role
Key worker approach – Coordination and continuity of care
Education and training for both SPC and HFN
http://dyingmatters.nativeye.com/beating‐the‐barriers