Embed Size (px)
Citation preview

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Germano Melissano“Vita-Salute” - San Raffaele University – Milano (Italy)
Update sulla patologia aneurismatica nel Marfan

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano 2
Disclosures
No relevant disclosures
San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Clinical presentation of TAA or TAD
• Early onset
• Lack of typical risk factors
• Runs in the family
• (Syndromic features)
MFS / CTD
San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
TAA or TAD may have a genetic basisMFS is just the tip of the iceberg
John A. Elefteriades

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Syndromic TAA• Marfan syndrome FBN1
• Ehlers-Danlos syndrome
– Vascular COL3A1
– Kyphoscoliotic PLOD1
– Valvular COL1A2
– EDS/OI overlap COL1A1
– Periventricular heterotopia FLNA
• Shprintzen-Goldberg syndrome SKI
• Cutis laxa FBLN4, ELN
• Arterial tortuosity syndrome SLC2A10
• Loeys-Dietz syndrome I/II TGFBR1/2
• Aneurysm/osteoarthritis – LDS IIISMAD3
• Loeys-Dietz syndrome IV TGFB2
San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Diagnosis of MFS
Quite obvious when its key phenotypic characteristics are present,
quite challenging if not…
Variable phenotype: in many cases they don’t look like the archetypal MFS

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Marfan syndrome (MFS)
Deficiency of FIBRILLIN-1 (FBN1)
Clinical diagnosis based on the revised nosology
Bart Loeys et al. J Med Genet, 2010
San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
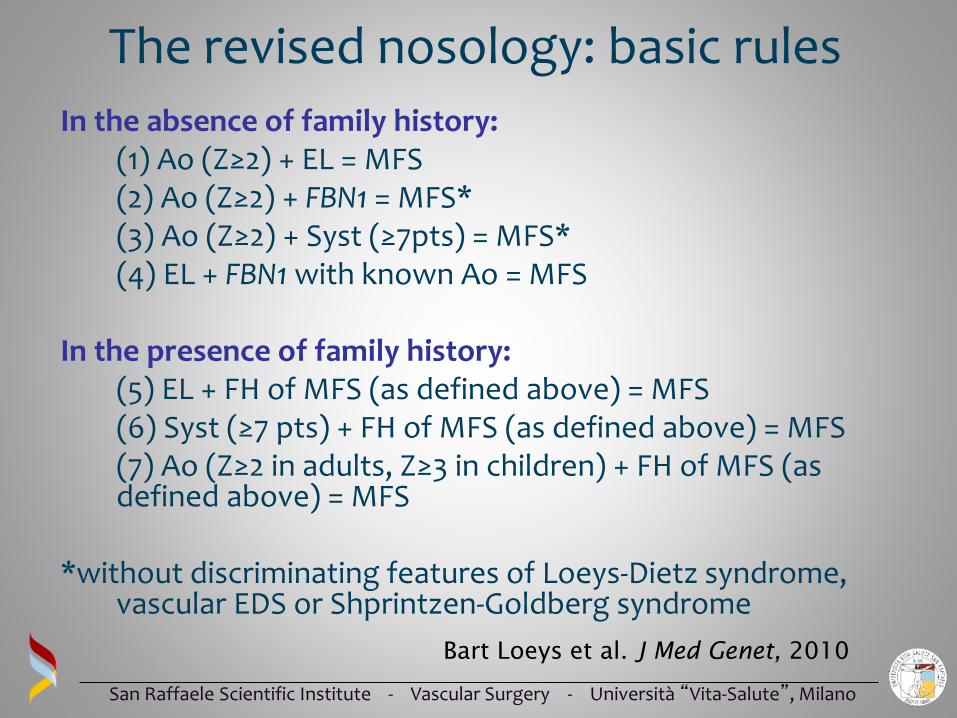
The revised nosology: basic rules
In the absence of family history:(1) Ao (Z≥2) + EL = MFS(2) Ao (Z≥2) + FBN1 = MFS*(3) Ao (Z≥2) + Syst (≥7pts) = MFS*(4) EL + FBN1 with known Ao = MFS
In the presence of family history:(5) EL + FH of MFS (as defined above) = MFS(6) Syst (≥7 pts) + FH of MFS (as defined above) = MFS(7) Ao (Z≥2 in adults, Z≥3 in children) + FH of MFS (as defined above) = MFS
*without discriminating features of Loeys-Dietz syndrome, vascular EDS or Shprintzen-Goldberg syndrome
Bart Loeys et al. J Med Genet, 2010

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Revised nosology: systemic score
2 points
3 points+
Bart Loeys et al. J Med Genet, 2010

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
1 point
Revised nosology: systemic score
Bart Loeys et al. J Med Genet, 2010

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Wrist AND thumb sign – 3 (Wrist OR thumb sign – 1)
Pectus carinatum deformity – 2 (pectus excavatum or chest asymmetry - 1)
Hindfoot deformity – 2 (plain pes planus – 1)
Protrusio acetabuli – 2
Pneumothorax – 2
Dural ectasia – 2
Reduced US/LS AND increased arm/height AND no severe scoliosis – 1
Scoliosis or thoracolumbar kyphosis – 1
Reduced elbow extension – 1
Facial features (3/5) – 1
(dolichocephaly, enophtalmos, downslanting palpebral fissures, malar
hypoplasia, retrognathia)
Skin striae – 1
Myopia > 3 diopters - 1
Mitral valve prolapse (all types) – 1
Systemic score ≥ 7 = MFS

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
CTD = problem in extra cellular matrix (ECM)
• ECM: Important proteins (collagen, fibrillin, elastin etc.) = biomechanicalproperties…But also …
• Regulates cytokines, TGFBeta, etc.
• It is plausible that TGFBeta signaling islinked to TAA in both syndromic and non-syndromic disease
• Role of angiotensin receptor blockers(Losartan)

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Aortic repair in Marfan: Topics of concern
1. Indications
2. Operative technique
3. Recurrent aneurysm
4. Role of TEVAR

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Teflon felt reinforcement
Tension free anastomosis
Proximal anastomosis Distal anastomosis
San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
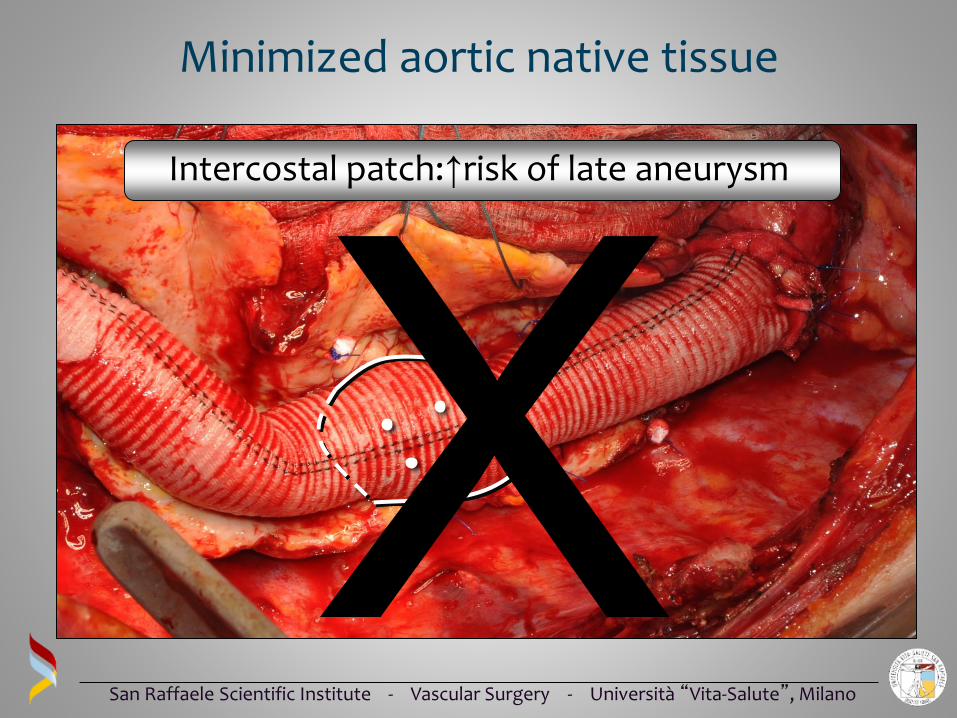
Intercostal patch:↑risk of late aneurysm
Minimized aortic native tissue

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Recurrent patch aneurysm

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Selective bypass in index procedure

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
•Male, 27 years old
•Bentall intervention
•Mitral valve repair
Surgical clinical case
Arachnodactyly
Pectus excavatumDolichostenomelia

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Aortic involvement
17 cm
Heart
Left kidney
28 cm

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Tutto schermo
Left kidney
Heart
Aneurysm
Spleen
San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
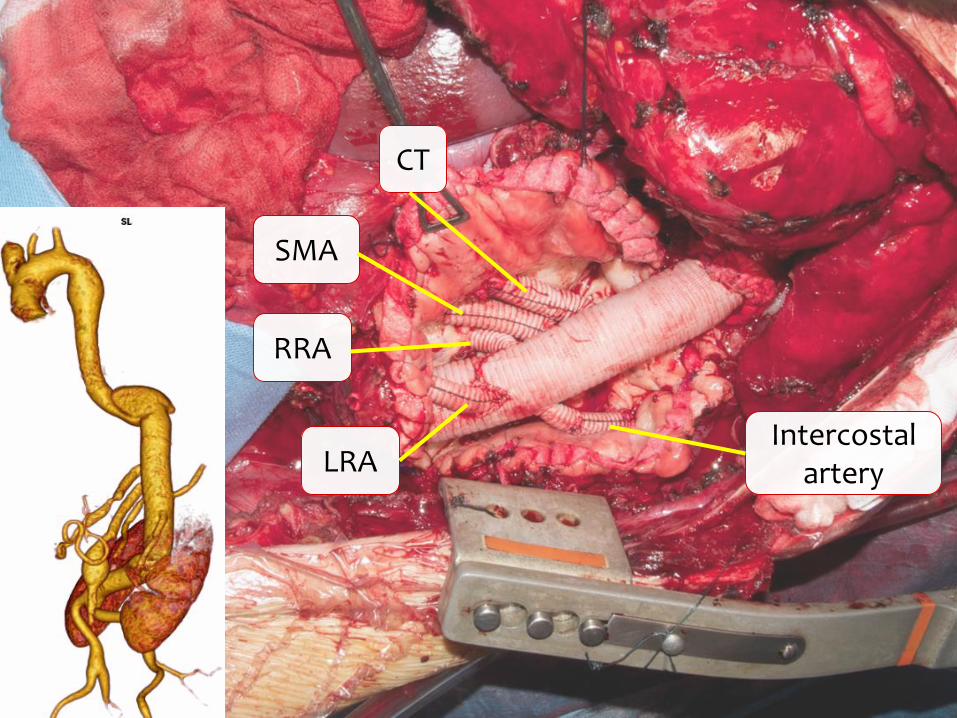
TAAA open repair
CT
SMA
RRA
LRAIntercostal
artery

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
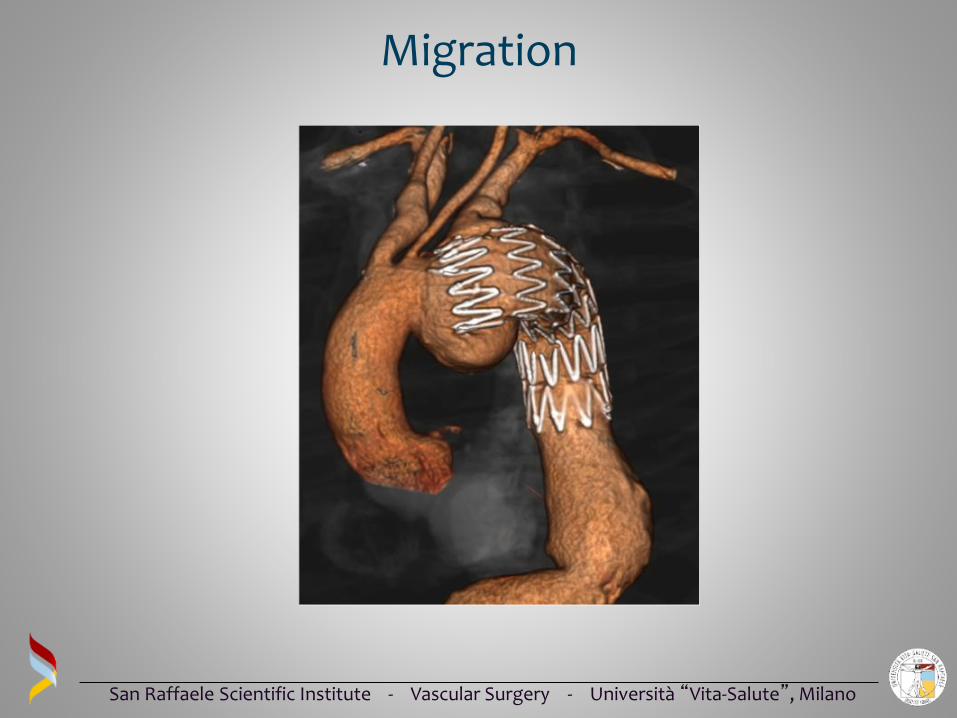
Role of TEVAR in Marfan
•Commonly hostile anatomy
•Aortic/neck dilatation
•Migration
•Retrograde/antegrade dissection
•Recurrent aneurysm
San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Migration
San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
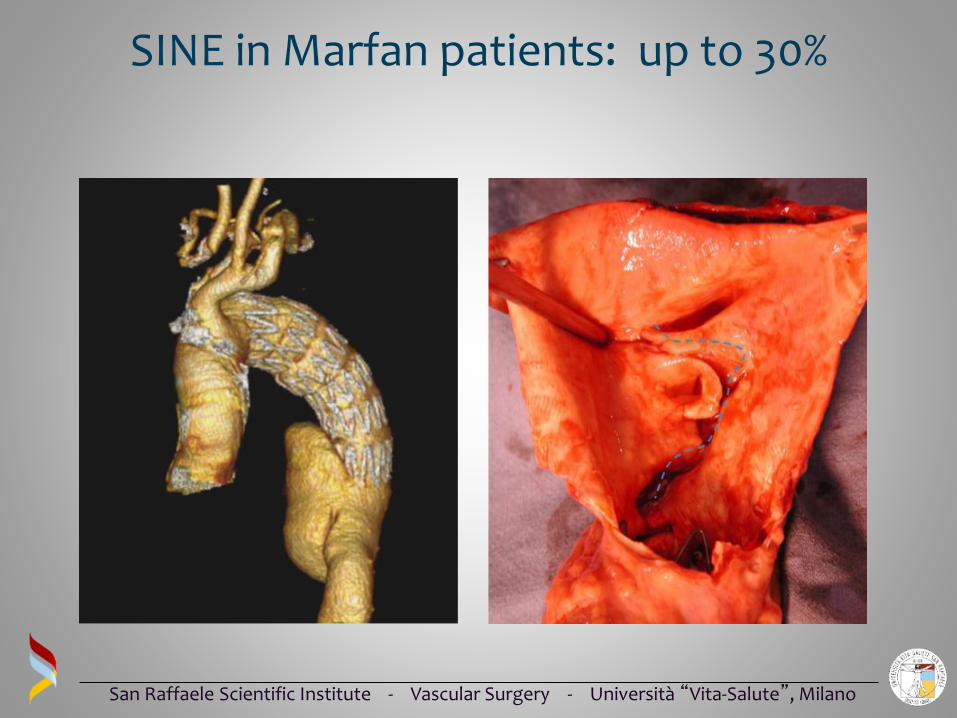
SINE in Marfan patients: up to 30%
San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
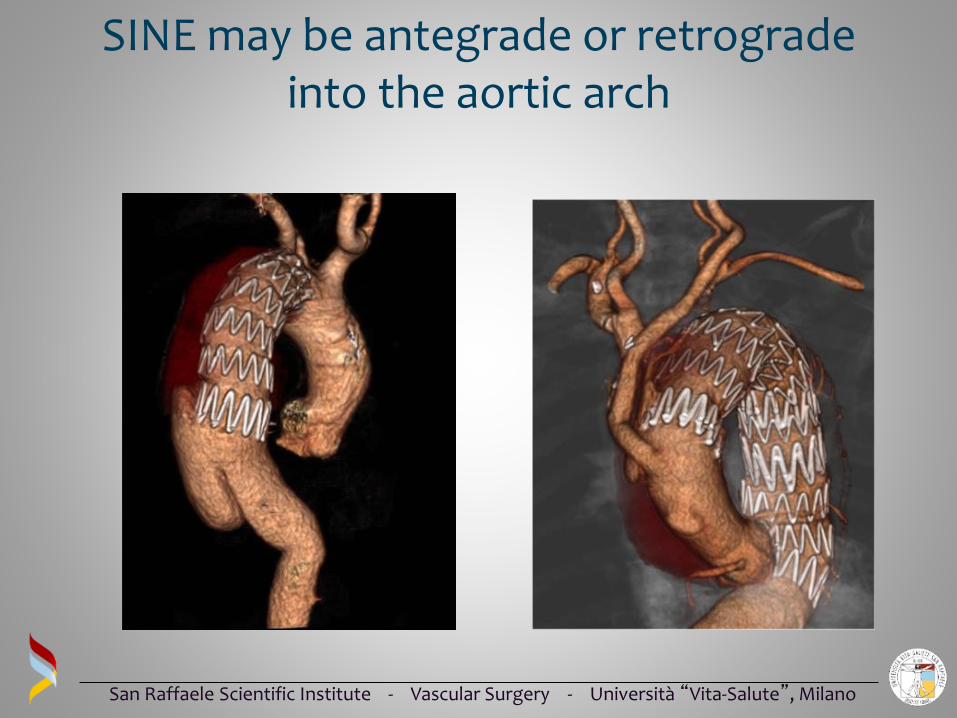
SINE may be antegrade or retrograde into the aortic arch

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Distal progression of disease

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Open conversion for distal progression
San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
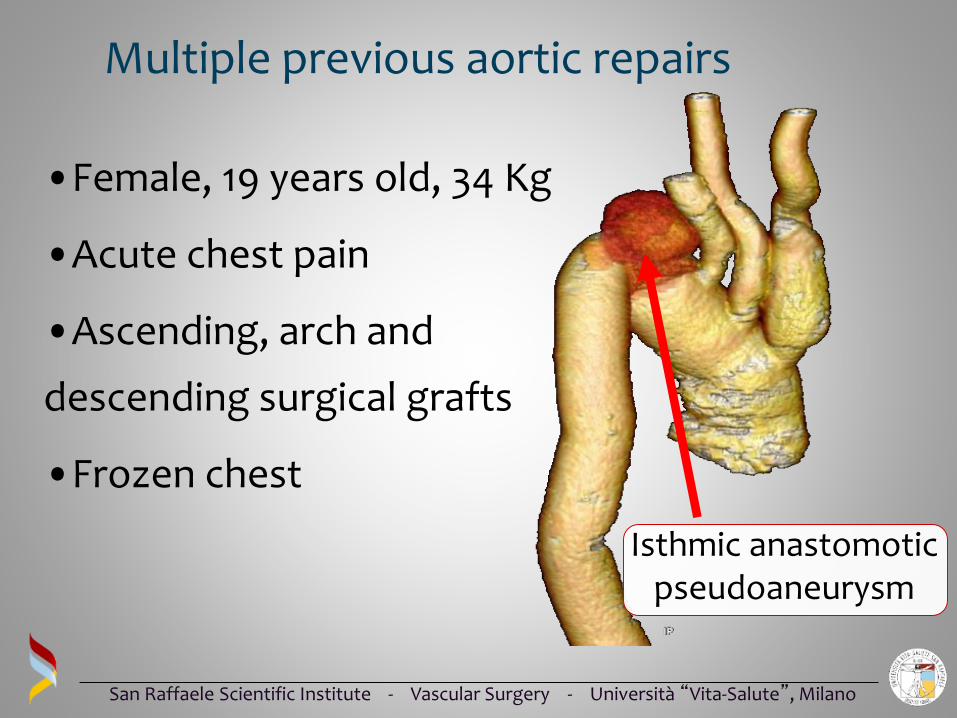
Multiple previous aortic repairs
•Female, 19 years old, 34 Kg
•Acute chest pain
•Ascending, arch and
descending surgical grafts
•Frozen chest
Isthmic anastomotic pseudoaneurysm

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Endovascular clinical case
Pseudoaneurysm
exclusion
Post operative CT scan
Custom-made
stentgraft landing into
the previous surgical
grafts

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Hybrid or total Endo: “ALL or NONE”

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Refer these patients to a Marfan Center
• Medical therapy, follow up
• Screen for genetic disease
• Evaluate family members

San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano
Conclusions
• New clinical entities recognized
• Diagnostic criteria revised
• New non surgical therapies tested
• Surgical improvements
30 years of research equaled
30 years of additional life expectancy
San Raffaele Scientific Institute - Vascular Surgery - Università “Vita-Salute”, Milano