Embed Size (px)
Citation preview
PRESSURE ULCER PREVENTION
AND MANAGEMENT
for clients of:
www.teamtsi.com • 800.765.8998
Content developed and presented by:
3030 N. Rocky Point Drive, Suite 240 Tampa, FL 33607
800.275.6252 • www.polaris-group.com

PRESSURE ULCER PREVENTION
Limited Copyright: May 2016, Polaris Group All materials are protected under the copyright laws.
The limited copyright allows the purchaser to copy for use but not for distribution.
FH32 - Developed by Polaris Group www.polaris-group.com Page 1 of 51
PRESSURE ULCER PREVENTION
POST TEST
1. New admits should be assessed for pressure ulcer risk including:
a. Use a standardized tool
b. Care plan based on risk factors and score
c. Communicate risk to staff
d. All of the above
2. Which of the following should be documented weekly for a pressure ulcer?
a. Location and stage
b. Size
c. Wound bed and edges
d. All of the above
3. A comprehensive assessment includes:
a. All pertinent risk factors regardless of score or CAA trigger
b. Pressure Ulcer CAA only
c. Braden’s or Norton’s Score only
d. All of the above
4. Which of the following should be care planned?
a. Pain
b. Moisture Management
c. Pressure reduction
d. All of the above
5. Which of the following are acceptable practices?
a. Turn every two hours in bed regardless of risk
b. Turn every two hours in chair
c. Turning schedule based on pressure tolerance
d. HOB raised higher than 30 degrees
FH32 - Developed by Polaris Group www.polaris-group.com Page 2 of 51
PRESSURE ULCER PREVENTION
POST TEST ANSWERS
1. New admits should be assessed for pressure ulcer risk including: D
a. Use a standardized tool
b. Care plan based on risk factors and score
c. Communicate risk to staff
d. All of the above
2. Which of the following should be documented weekly for a pressure ulcer?
a. Location and stage
D
b. Size
c. Wound bed and edges
d. All of the above
3. A comprehensive assessment includes:
a. All pertinent risk factors regardless of score or CAA trigger
A
b. Pressure Ulcer CAA only
c. Braden’s or Norton’s Score only
d. All of the above
4. Which of the following should be care planned? D
a. Pain
b. Moisture Management
c. Pressure reduction
d. All of the above
C 5. Which of the following are acceptable practices?
a. Turn every two hours in bed regardless of risk
b. Turn every two hours in chair
c. Turning schedule based on pressure tolerance
d. HOB raised higher than 30 degrees
FH32 - Developed by Polaris Group www.polaris-group.com Page 3 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Pressure Ulcer Program Management
1
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Pressure Ulcer Program Key Components
• QAC should ensure all Key Components are in place and effective1. Orientation and Education
2. Admission assessment/Initial Care planning
3. Ongoing Assessment & Monitoring for Effectiveness
4. Care Planning
• Interventions
5. Active Pressure Ulcer/New Pressure Ulcer
6. Pressure Ulcer, Trending, Reporting to QA
• Risk Team - Individual Investigations & Environment 2
FH32 - Developed by Polaris Group www.polaris-group.com Page 4 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Orientation & Education
• Orientation & Education – Direct Care Staff
• Standards of practice
• How to recognize and report skin issues
• Review issues such as friction/shear, pressure reduction and relief
– Licensed Nurses• As noted above
• How to stage pressure ulcers and identify early tissue damage
• Care planning for risk factors
• Treatment protocols 3
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Orientation & Education
• Complete a standardized Pressure Ulcer risk tool at time of admission.– Braden’s Tool
– Norton’s Tool
– Other tool
• Designed to identify Risk Factors and level of risk.
• Assists with initial care planning interventions
4
FH32 - Developed by Polaris Group www.polaris-group.com Page 5 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
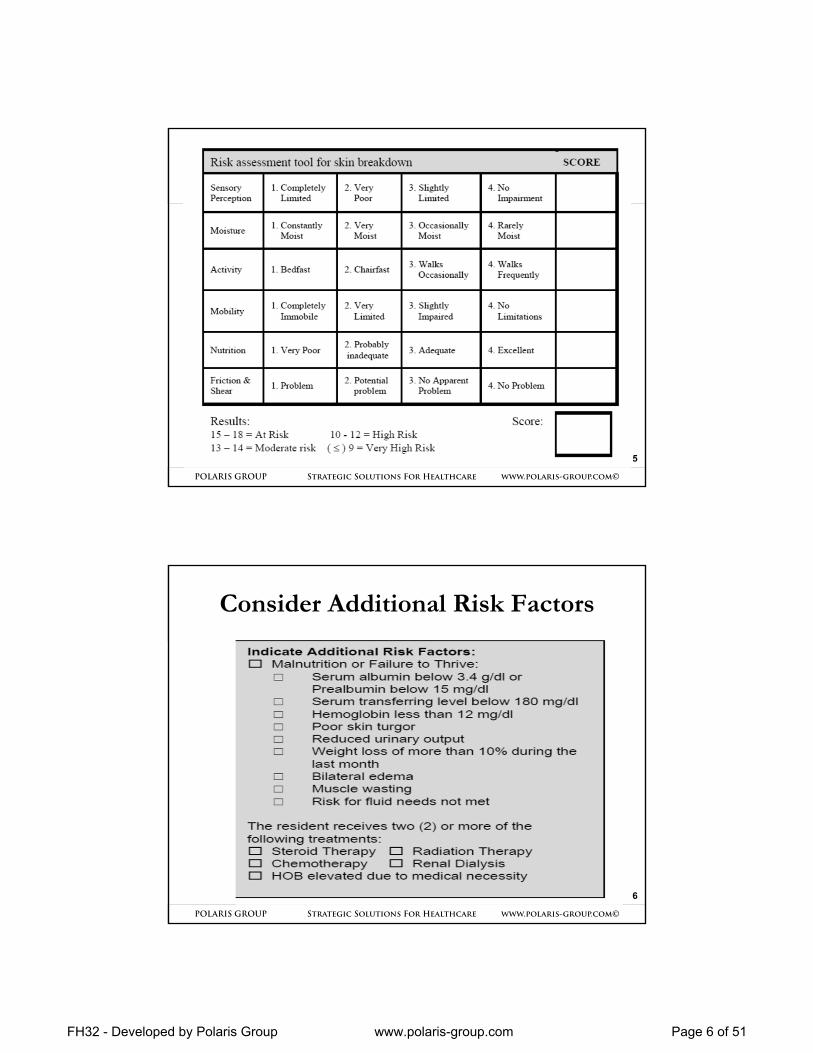
5
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Consider Additional Risk Factors
6
FH32 - Developed by Polaris Group www.polaris-group.com Page 6 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
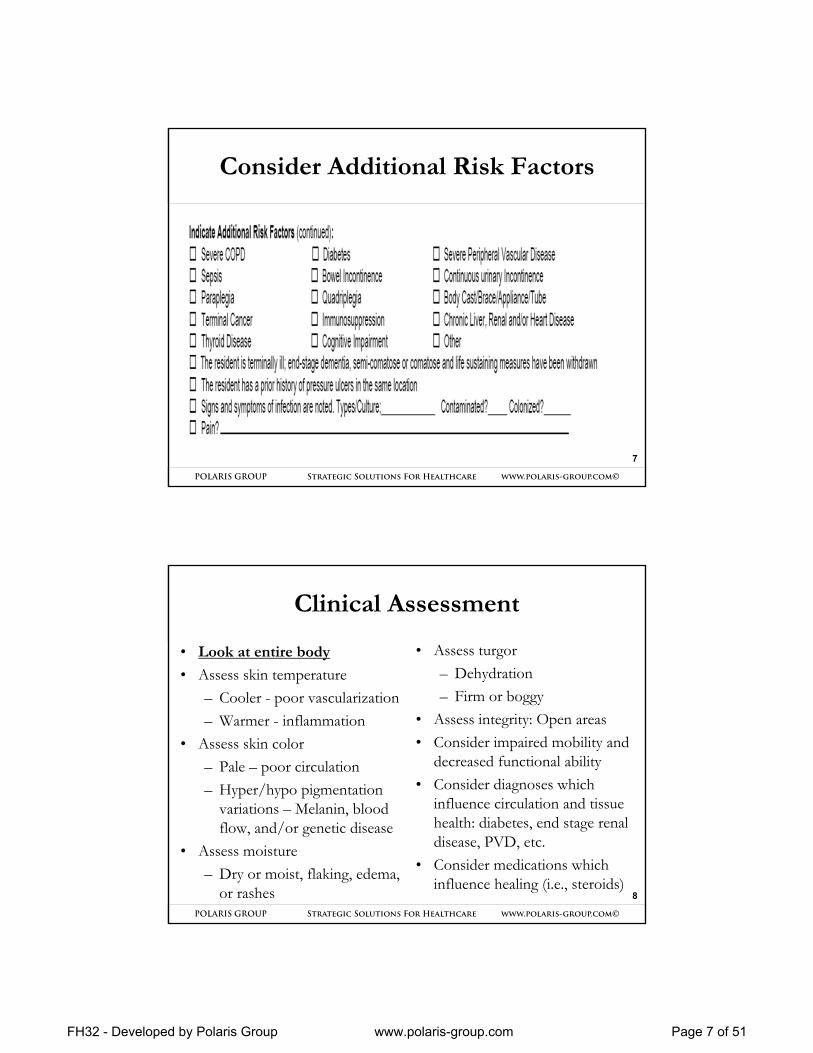
Consider Additional Risk Factors
7
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Clinical Assessment
• Look at entire body
• Assess skin temperature
– Cooler - poor vascularization
– Warmer - inflammation
• Assess skin color
– Pale – poor circulation
– Hyper/hypo pigmentation variations – Melanin, blood flow, and/or genetic disease
• Assess moisture
– Dry or moist, flaking, edema, or rashes
• Assess turgor
– Dehydration
– Firm or boggy
• Assess integrity: Open areas
• Consider impaired mobility and decreased functional ability
• Consider diagnoses which influence circulation and tissue health: diabetes, end stage renal disease, PVD, etc.
• Consider medications which influence healing (i.e., steroids)
8
FH32 - Developed by Polaris Group www.polaris-group.com Page 7 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
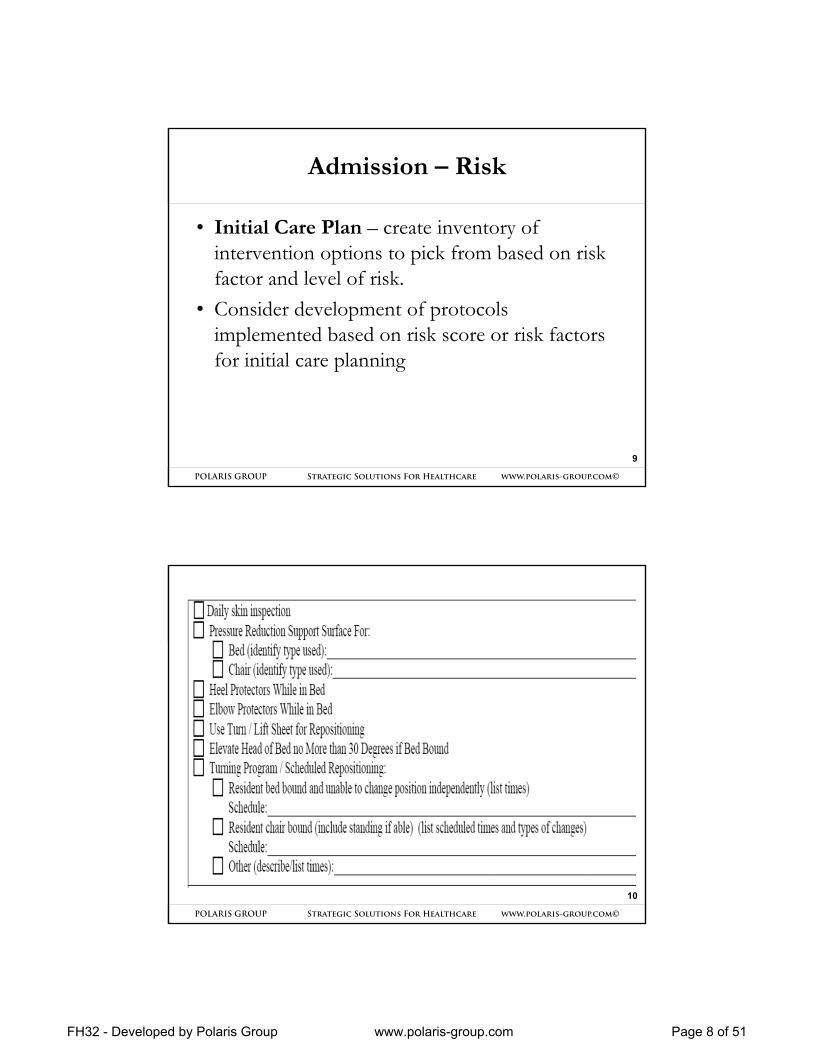
Admission – Risk
• Initial Care Plan – create inventory of intervention options to pick from based on risk factor and level of risk.
• Consider development of protocols implemented based on risk score or risk factors for initial care planning
9
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
10
FH32 - Developed by Polaris Group www.polaris-group.com Page 8 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
11
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
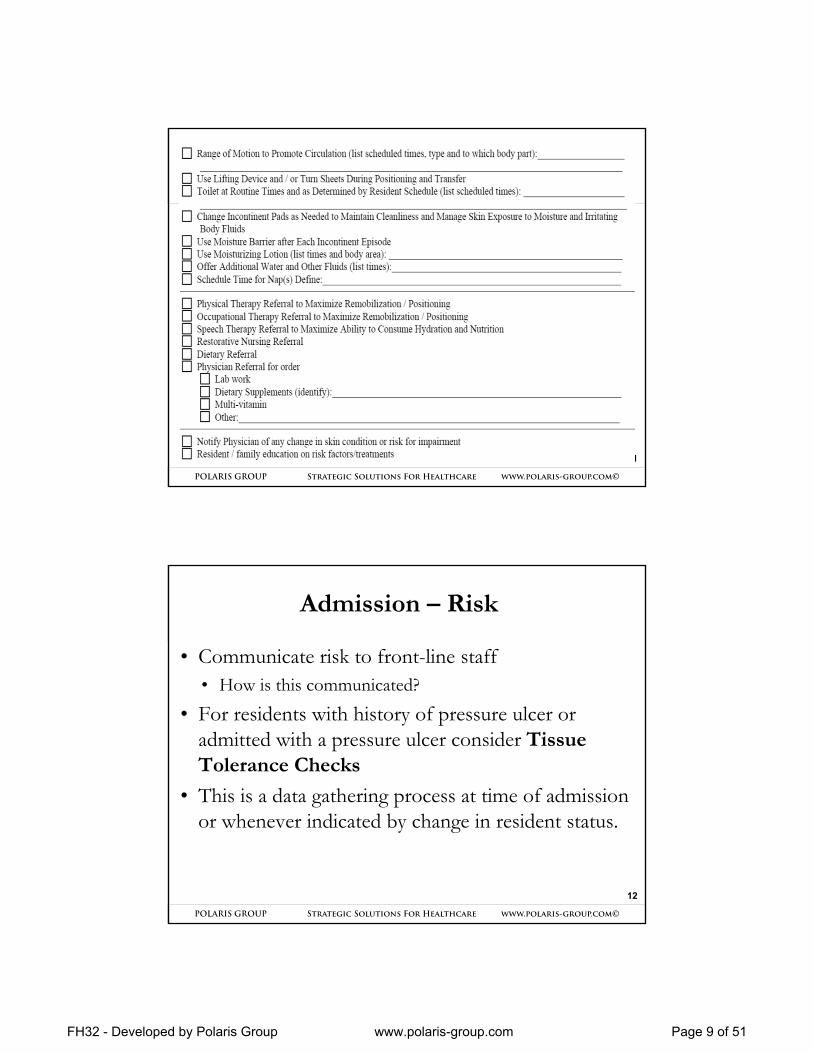
Admission – Risk
• Communicate risk to front-line staff • How is this communicated?
• For residents with history of pressure ulcer or admitted with a pressure ulcer consider Tissue Tolerance Checks
• This is a data gathering process at time of admission or whenever indicated by change in resident status.
12
FH32 - Developed by Polaris Group www.polaris-group.com Page 9 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
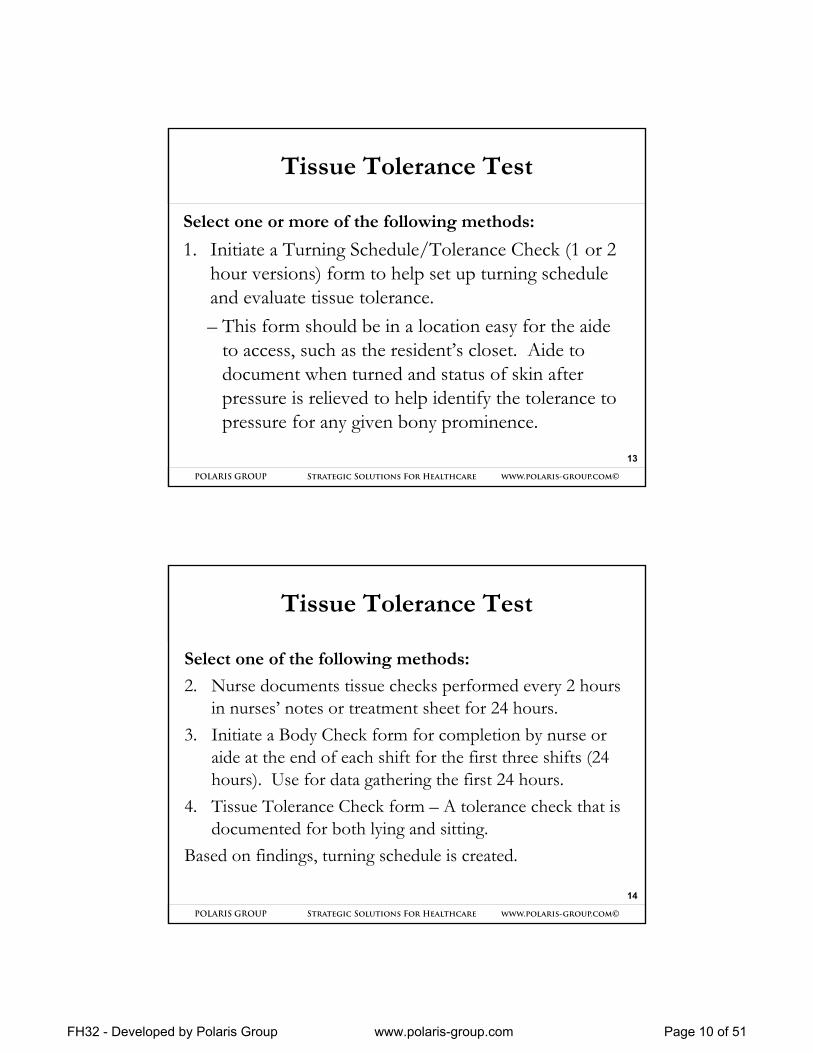
Tissue Tolerance Test
Select one or more of the following methods:
1. Initiate a Turning Schedule/Tolerance Check (1 or 2 hour versions) form to help set up turning schedule and evaluate tissue tolerance.
– This form should be in a location easy for the aide to access, such as the resident’s closet. Aide to document when turned and status of skin after pressure is relieved to help identify the tolerance to pressure for any given bony prominence.
13
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Tissue Tolerance Test
Select one of the following methods:
2. Nurse documents tissue checks performed every 2 hours in nurses’ notes or treatment sheet for 24 hours.
3. Initiate a Body Check form for completion by nurse or aide at the end of each shift for the first three shifts (24 hours). Use for data gathering the first 24 hours.
4. Tissue Tolerance Check form – A tolerance check that is documented for both lying and sitting.
Based on findings, turning schedule is created.
14
FH32 - Developed by Polaris Group www.polaris-group.com Page 10 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
15
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
16
FH32 - Developed by Polaris Group www.polaris-group.com Page 11 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
17
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
18
FH32 - Developed by Polaris Group www.polaris-group.com Page 12 of 51

POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Ongoing Assessment & Monitoring
• Full RAI – Pressure Ulcer CAA– Admission
– Annual
– SCSA
• Quarterly Pressure Ulcer Risk Tool or at time of SCSA
• Risk Team – reviews– 24-hour report
– New Pressure Ulcer
– Change in condition
19
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
#16 Pressure Ulcer
20
FH32 - Developed by Polaris Group www.polaris-group.com Page 13 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
#16 Pressure Ulcer
21
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
#16 Pressure Ulcer(s)
Existing pressure ulcer(s) (M0100)Assess location, size, stage, presence and type of drainage, presence of odors, condition of surrounding skin
– Note if eschar or slough is present
– Assess for signs of infection such as the presence of foul odor, increasing pain, surrounding skin is reddened (erythema) or warm, or there is a presence of purulent drainage
– Note whether granulation tissue (required for healing) is present and the wound is healing as expected
22
FH32 - Developed by Polaris Group www.polaris-group.com Page 14 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
If the ulcer does not show signs of healing despite treatment, consider complicating factors
– Elevated bacterial level in the absence of clinical infection
– Presence of exudate, necrotic debris or slough in the wound, too much granulation tissue or odor in the wound bed
– Underlying osteomyelitis (bone infection)
#16 Pressure Ulcer(s), continued
Existing pressure ulcer(s) (M0100)
23
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
#16 Pressure Ulcer(s), continued
Extrinsic risk factorsPressure
– Requires staff assistance to move sufficiently to relieve pressure over any one site
– Confined to a bed or chair all or most of the time
– Needs special mattress or seat cushion to reduce or relieve pressure
– Requires regular schedule of turning 24
Friction and shear
– Slides down in the bed
– Moved by sliding rather than lifting
Maceration
– Persistently wet, especially from fecal incontinence, wound drainage or perspiration
FH32 - Developed by Polaris Group www.polaris-group.com Page 15 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
#16 Pressure Ulcer(s), continued
Intrinsic risk factors
Immobility (G0100)
Altered mental status
– Delirium limits mobility
– Cognitive loss (C0500, C0700-C1100)
Incontinence (H0300, H0400)
Poor nutrition
Medications Antipsychotics (N0400A)
Antidepressants (N0400C)
Antianxiety agents (N0400B)
Sedatives/hypnotics (N0400D)
Steroids
Narcotics
25
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
#16 Pressure Ulcer(s), continued
Diagnosis and conditionsDelirium (C1600)
Comatose (B0100)
Cancer (I0100)
Peripheral vascular disease (I0900)
Diabetes (I2900)
Alzheimer’s disease (I4200)
Cerebrovascular accident (I4500)
Other dementia (I4800)
Hemiplegia/hemiparesis (I4900)
Paraplegia (I5000), quadriplegia (I5100)
Multiple sclerosis (I5200)
Depression (D0300, D0600, I5800)
Edema
Severe pulmonary disease (I6200)
Sepsis (I2100)
Terminal illness (O0100K)26
FH32 - Developed by Polaris Group www.polaris-group.com Page 16 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
#16 Pressure Ulcer(s), continued
Diagnosis & conditions, cont.Chronic or end-stage renal (I1500), liver or heart disease (I0400, I0600)
Pain (J0300)
Dehydration (J1500D, I8000)
Shortness of breath (J1100)
Recent weight loss (K0300)
Malnutrition (I5600)
Decreased sensory perception
Recent decline in activities of daily living (G0100-G0600)
27
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
#16 Pressure Ulcer(s), continued
Treatments and other factorsChemotherapy (A0100A)
Radiation therapy (A0100B)
Ventilator or respirator (A0100F)
Renal dialysis (A0100J)
Functional limitation in range of motion (G0400)
Head of bed elevated most or all of the time
Physical restraints (P0100)
Bedfast (G0800) or wheelchair bound
Devices that can cause pressure, such as oxygen (A0100C) or indwelling catheter (H0100A) tubing, TED hose, casts, splints, etc
Newly admitted or readmitted
History of healed pressure ulcer(s)
28
FH32 - Developed by Polaris Group www.polaris-group.com Page 17 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
#16 Pressure Ulcer(s) Summary
Pressure Ulcers Focus: To assist in treatment and prevention of pressure sores.
• Identify risk factors to develop preventive care plan.
• Include all factors medical and functional.
• Evaluate effectiveness of current treatment regime.
• Indicate pressure relief and reduction.
• Indicate pain management.
• Reference Pressure Ulcer Risk score.
29
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Ongoing Assessment & Monitoring
• System in place to communicate turning schedules
• Systems in place to monitor that turning schedules are followed.– Documentation as “done”
– Observations and rounds
30
FH32 - Developed by Polaris Group www.polaris-group.com Page 18 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Ongoing Assessment & Monitoring
• Systems to perform body checks – Aide report any unusual skin concerns immediately
with follow-up by nurse
– Body Check form turned in after showers/bath
– Body Checks performed by nurses
• Documented with follow-up if new skin issue discovered.
• QA – How often does nurse discover a Stage 1 or greater that was not already reported?
31
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning
• Develop care plan protocols by risk factor and/or by Stage of Pressure Ulcer
• Ensure necessary equipment is available.
• Medical Director approves any treatment protocols.
32
FH32 - Developed by Polaris Group www.polaris-group.com Page 19 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Skin/Sensory Perception • Treat dry skin with moisturizers
• Apply moisture creams after showers/bath
• Avoid massage over bony prominence
• Avoid hot water, use mild cleansing soap
• Avoid friction
• Avoid shearing
• Teach resident who is capable to shift position every 15 minutes in chair
33
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Immobility/inability to reposition self in bed
• Maintain elevation of head of bed at lowest possible degree
• Head of bed should never be raised over 30 degrees unless medically indicated
• Position off of back when in bed
• Provide pressure redistribution for pressure points
34
Reposition in General:
• No more than every 2 hours in bed
• No more than every hour in chair
• All wheelchairs need a pressure relief cushion
• Micro-shifting is not acceptable standard
• When in chair, “Off-load” for a minute is best practice
• Never position on the trochanter
FH32 - Developed by Polaris Group www.polaris-group.com Page 20 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Immobility/inability to reposition self in bed
• Pressure reduction: Surface that reduces pressure but does not consistently maintain interface pressure below capillary closing pressure. Use on resident who can be turned and whose breakdown is confined to one surface OR residents at RISK.
– Mattress overlays (gel, foam, water); replacement mattress – utilize mattress with built in pressure reduction
• Pressure relief: Surface that consistently maintains capillary pressure thus maintaining blood supply to tissue. Use on residents who cannot be turned to relieve pressure or who have breakdown involving multiple sites or deep tissue involvement.
– Low air bed or air fluidized beds
35
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Immobility/inability to reposition self in bed
• Elevate heals and elbows off of bed using heel and elbow protectors.
• Use wedges and pillows to avoid bony prominences touching each other.
• Avoid positioning on trochanter at all times.
• Trapeze or side rail used to help reposition.
• Keep off pressure ulcer until resolved when possible. 36
Immobility/inability to reposition self in bed
• Pressure relieving devices
– Sheepskin
– Pillows
– Gel cushion/pad/mattress overlay
– Egg Crate (4”)
– Ear protectors
– Ankle/heel protectors
– Foot Cradle
FH32 - Developed by Polaris Group www.polaris-group.com Page 21 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Inability to reposition self in chair
• Pressure relieving devices
– Sheepskin
– Pillows
– Gel cushion/pad/mattress overlay
– Egg Crate (4”)
– Arm rest pads
– Ear protectors
– Ankle/heel protectors
37
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Inability to reposition self in chair
• Do not use donuts.
• Shift position every hour in chair based on tissue tolerance to pressure points.
• Pressure reduction: Surface that reduces pressure but does not consistently maintain interface pressure below capillary closing pressure. Use on resident who can be turned and whose breakdown is confined to one surface.
– Chair cushions (foam, gel, air)
• Use wedges and pillows to avoid bony prominences from touching each other.
• Keep off pressure ulcer until resolved when possible.
• Supportive Devices
– Back wedge
– Pillow between knees
– Pillow between bony prominences
– Pillow under arm
– Neck support 38
FH32 - Developed by Polaris Group www.polaris-group.com Page 22 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Risk for friction/shear when moving
• Use a draw sheet for turning or repositioning.
• Use lifting device for transfers.
• Maintain elevation of head of bed at lowest possible degree.
• Do not elevate greater than 30 degrees unless medically indicated.
Moisture: Incontinence of urine or bowel
• Peri-care after each incontinence. Use moisture barrier per procedures.
• Encourage adequate fluid intake.
• Offer additional fluids per procedures.
• Whirlpool bath or equivalent once a week.
39
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Moisture: Perspiration/other
• Use cloths to decrease skin to skin contact.
• Apply moisture barrier.
• Apply moisture absorbing device.
PVD
• Heel protectors in bed (Seamless)
• Elevate heels off bed
• Heel protectors in chair (Seamless)
• Ensure well fitting shoes/slippers
• Foot cradle
• Prevent injury to ankles/feet/toes
40
FH32 - Developed by Polaris Group www.polaris-group.com Page 23 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Diabetes
• Heel protectors in bed
• Float heels
• Elevate heels off bed is preferred method
• Heel protectors in chair
• Ensure well fitting shoes/slippers
• Clean well between toes
• Nurse to keep toenails trimmed
• Foot cradle
• Prevent injury to ankles/feet/toes
Edema
• Heel protectors in bed
• Elevate heels off bed
• Elevate foot of bed
• Elevate legs in chair
• Elevate upper extremities on pillows
• Heel protectors in chair
• Ensure well fitting shoes/slippers
• Clean well between toes
• Nurse to keep toenails trimmed
• Foot cradle 41
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Nutrition- Underweight/malnourished/losing weight/abnormal labs• Notify Dietary Manager for referral to Registered Dietician for
Stage 2 or greater
• Increase protein in diet as recommended by RD
• Provide nourishment per protocol
• Provide Supplement per protocol
• Multivitamin with minerals, Zinc (not proven to be affective), and Vitamin C for Stage 2 or greater
• Ensure fluid needs are met
• Offer additional fluids 42
FH32 - Developed by Polaris Group www.polaris-group.com Page 24 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Nutrition- Underweight/malnourished/losing weight/abnormal labs• Notify Dietary Manager for referral to Registered Dietician
for Stage 2 or greater
• Increase protein in diet as recommended by RD
• Provide nourishment per protocol
• Provide Supplement per protocol
• Multivitamin with minerals, Zinc (not proven to be affective), and Vitamin C for Stage 2 or greater
• Ensure fluid needs are met
• Offer additional fluids 43
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Other Medical Concerns (e.g. pain, cancer, terminal, failure to thrive, radiation, or chemotherapy)
• Assess and treat for pain
• Provide pain medication prior to treatment
• Skin care per procedures/orders based on concern
• Monitor Cast edges
• Petal cast edges
Self-directing Care/Behaviors
• Resident and family aware of risks of refusing to follow Pressure Ulcer prevention interventions - i.e. refuses to stay of right side, repositions self to desired side, etc.
• Refuses Supplements
• Refuses medications
44
FH32 - Developed by Polaris Group www.polaris-group.com Page 25 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Care Planning by Risk Factor
Actual Pressure Ulcer Stage 2-4:
• Refer to Registered Dietician
• Refer to therapy
• Obtain lab values: sample lab helpful to pressure ulcer management
– BUN
– TOTAL SERUM PROTEIN
– CREATININE
– LDH
– CBC
– HCT
– HGB
– SERUM ALBUMIN
– PRE-ALBUMIN (TRANSTHYRETIN)
– TOTAL LYMPHOCYTE COUNT 45
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Actual Stage 3 and 4:• Assess for appropriateness of an Indwelling Catheter
• Refer to Therapy for Part B screen for wound care and positioning
• Consider referral to Wound Specialist
46
FH32 - Developed by Polaris Group www.polaris-group.com Page 26 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Active Pressure Ulcer
• At time pressure ulcer is discovered, a licensed nurse must assess area.
• Documentation should at a minimum include:– Location
– Stage
– Size
– Depth
– Surrounding tissue
– Drainage 47
• Documentation can be in nurses’ notes and/or Pressure Ulcer Flow sheet.
• Notify physician and implement orders
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Active Pressure Ulcer
• Notify family
• Add to 24 hour report
• Update care plan – to new PU
• Refer to Dietary Manager
• Skin Nurse/DON should review and ensure pressure ulcer flow sheet is complete and accurate.
• Risk team ensure care plan is reviewed and revised to any new risk factors/changes in interventions
48
FH32 - Developed by Polaris Group www.polaris-group.com Page 27 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Active Pressure Ulcer
• Pressure Ulcer Flow Sheet should include the following:
– Location of wound (i.e., left trochanter, sacrum)
– Stage of wound
• Stage 1, 2, 3 or 4
• Unstageable
• Suspected Deep Tissue Injury
– Size of wound (use a measuring guide from RAI)
• Length (cm)
• Width (cm)49
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Active Pressure Ulcer
• Pressure Ulcer Flow Sheet should include the following:
– Depth of wound• Insert sterile, flexible 6 inch cotton tipped applicator gently into
the deepest part of the wound
• Grasp with thumb and forefinger at skin surface and withdraw.
• Measure distance from the tip of fingers in centimeters.
– Undermining/Tunneling• Document if present or absent.
• If present, measure involvement. One method to document is to describe in relation to a clock face, i.e., 2 cm undermining from 12 – 3 o’clock, 6 cm tunnel at 7 o’clock
50
FH32 - Developed by Polaris Group www.polaris-group.com Page 28 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Active Pressure Ulcer
• Pressure Ulcer Flow Sheet should include the following:
– Size and depth of sinus track
• Surrounding skin (peri-wound)
• Intact
• Pink/red
• White/gray/pallor
• Dark red/purple
51
• Black
• Swollen
• Maceration
• Rash
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Active Pressure Ulcer
• Pressure Ulcer Flow Sheet should include the following: – Wound Edges
– Rolled edges
– Red
– Hard
– Induration
– Macerated
– Intact
– Undermining52
– Wound Bed
– Epithelial Tissue: New skin growing in superficial ulcer. Light pink and shiny.
– Granulation Tissue: Pink or red tissue with moist granular appearance
– Slough: Yellow or white tissue that adheres to the sound bed.
– Eschar: Necrotic tissue, black or brown on color, dry and scab-like.
FH32 - Developed by Polaris Group www.polaris-group.com Page 29 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Active Pressure Ulcer
• Pressure Ulcer Flow Sheet should include the following:
– Drainage / Exudate, describe type (e.g. serous, purulent)
• Color
• Odor if present, describe
• Amount
53
• Infection: describe cellulites, inflammatory process, fever, and culture results if taken.
• Pain; presence or absence
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Active Pressure Ulcer
• Weekly Progress written on Pressure Ulcer flow sheet
• Risk Team reviews weekly as to progress – ensure care plan is current and documentation is complete
• If not improvement noted within 2 weeks, consider notifying physician to review/change orders
54
FH32 - Developed by Polaris Group www.polaris-group.com Page 30 of 51
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Trending and Reporting to QA
• All new pressure ulcers are added to a Pressure Ulcer Tracking system/form/log.
• Log is kept current at all time by assigned nurse.
• Risk Team reviews all pressure ulcers and monitors progress of pressure ulcer weekly.
• Pressure Ulcers are reported monthly to Risk Committee/QA.– Total number of pressure ulcers; and by stage
– Total number of residents with pressure ulcers
– Total acquired pressure ulcers; and by stage55
POLARIS GROUP Strategic Solutions For Healthcare www.polaris-group.com©
Trending and Reporting to QA
• Quality Measures are printed monthly and Prevalence of Stage 1-4 Pressure Ulcers – both short and long stay measures high risk are reviewed and pressure ulcers are investigated. – Investigation includes evaluation of standards and implementation
of care plan.
• Pressure Ulcer trends are reported to quarterly Quality Assessment and Improvement Committee.
• Pressure Ulcer trends are shared with staff through routine meetings and inservices.
56
FH32 - Developed by Polaris Group www.polaris-group.com Page 31 of 51
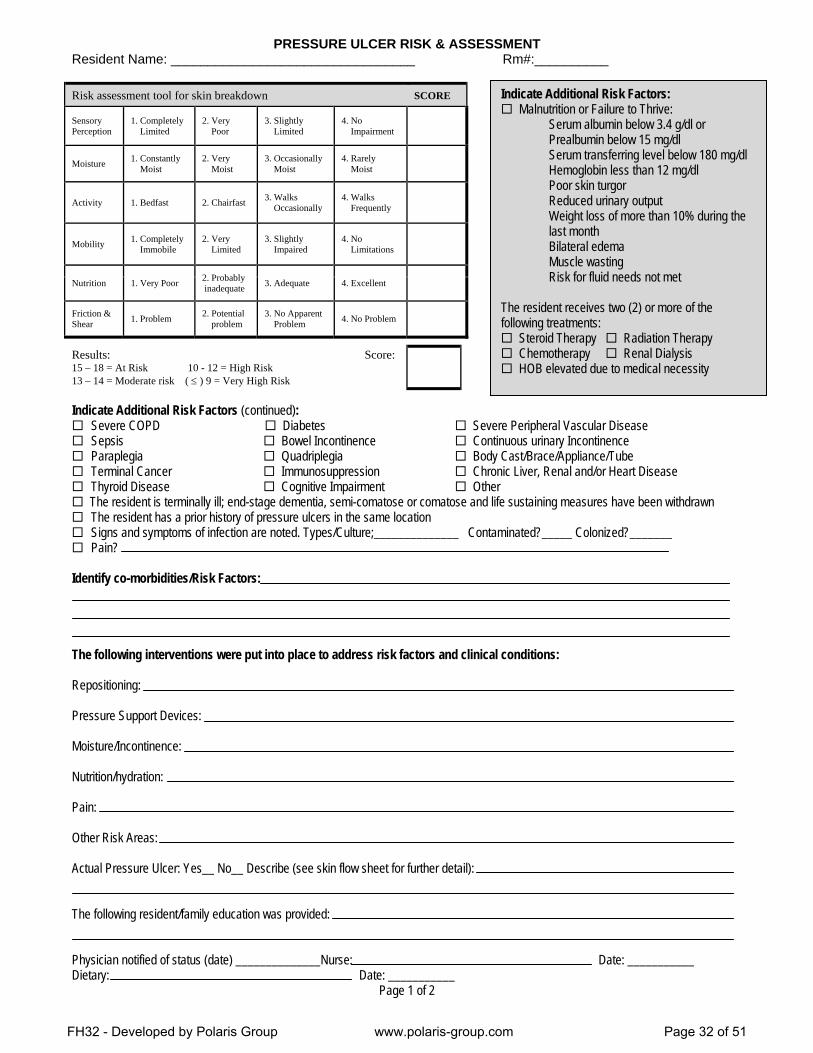
PRESSURE ULCER RISK & ASSESSMENT Resident Name: _________________________________ Rm#:__________
Results: Score: 15 – 18 = At Risk 10 - 12 = High Risk 13 – 14 = Moderate risk ( ≤ ) 9 = Very High Risk
Indicate Additional Risk Factors (continued):
Severe COPD Diabetes Severe Peripheral Vascular Disease Sepsis Bowel Incontinence Continuous urinary Incontinence Paraplegia Quadriplegia Body Cast/Brace/Appliance/Tube Terminal Cancer Immunosuppression Chronic Liver, Renal and/or Heart Disease Thyroid Disease Cognitive Impairment Other The resident is terminally ill; end-stage dementia, semi-comatose or comatose and life sustaining measures have been withdrawn The resident has a prior history of pressure ulcers in the same location Signs and symptoms of infection are noted. Types/Culture;______________ Contaminated?_____ Colonized?_______ Pain?
Identify co-morbidities/Risk Factors: The following interventions were put into place to address risk factors and clinical conditions: Repositioning: Pressure Support Devices: Moisture/Incontinence: Nutrition/hydration: Pain: Other Risk Areas: Actual Pressure Ulcer: Yes__ No__ Describe (see skin flow sheet for further detail): The following resident/family education was provided: Physician notified of status (date) ______________Nurse: Date: ___________ Dietary: Date: ___________
Page 1 of 2
Risk assessment tool for skin breakdown SCORE
Sensory Perception
1. Completely Limited
2. Very Poor
3. Slightly Limited
4. No Impairment
Moisture 1. Constantly Moist
2. Very Moist
3. Occasionally Moist
4. Rarely Moist
Activity 1. Bedfast 2. Chairfast 3. Walks Occasionally
4. Walks Frequently
Mobility 1. Completely Immobile
2. Very Limited
3. Slightly Impaired
4. No Limitations
Nutrition 1. Very Poor 2. Probably inadequate 3. Adequate 4. Excellent
Friction & Shear 1. Problem 2. Potential
problem 3. No Apparent Problem 4. No Problem
Indicate Additional Risk Factors: Malnutrition or Failure to Thrive: � Serum albumin below 3.4 g/dl or
Prealbumin below 15 mg/dl � Serum transferring level below 180 mg/dl � Hemoglobin less than 12 mg/dl � Poor skin turgor � Reduced urinary output � Weight loss of more than 10% during the
last month � Bilateral edema � Muscle wasting � Risk for fluid needs not met
The resident receives two (2) or more of the following treatments:
Steroid Therapy Radiation Therapy Chemotherapy Renal Dialysis HOB elevated due to medical necessity
FH32 - Developed by Polaris Group www.polaris-group.com Page 32 of 51
Date Progress Notes Resident: MR#: RM#:
Page 2 of 2
FH32 - Developed by Polaris Group www.polaris-group.com Page 33 of 51
Page 1 of 2
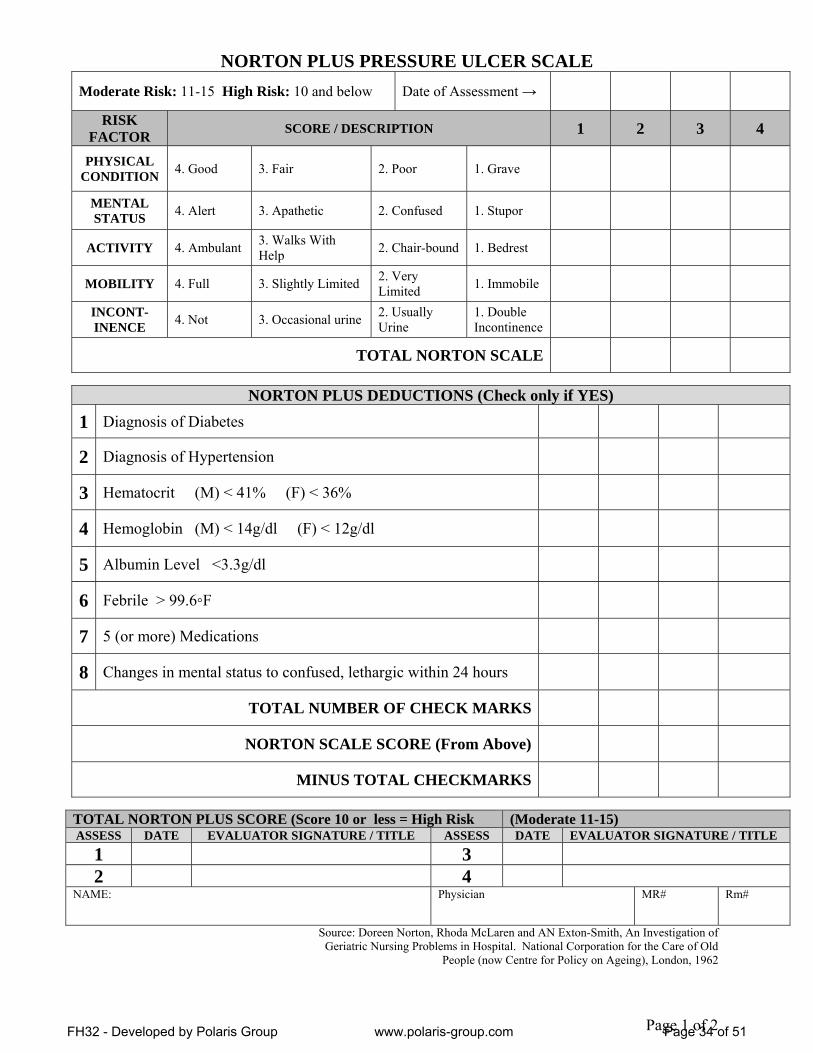
NORTON PLUS PRESSURE ULCER SCALE
Moderate Risk: 11-15 High Risk: 10 and below Date of Assessment →
RISK FACTOR SCORE / DESCRIPTION 1 2 3 4
PHYSICAL CONDITION 4. Good 3. Fair 2. Poor 1. Grave
MENTAL STATUS 4. Alert 3. Apathetic 2. Confused 1. Stupor
ACTIVITY 4. Ambulant 3. Walks With Help 2. Chair-bound 1. Bedrest
MOBILITY 4. Full 3. Slightly Limited 2. Very Limited 1. Immobile
INCONT-INENCE 4. Not 3. Occasional urine 2. Usually
Urine 1. Double Incontinence
TOTAL NORTON SCALE
NORTON PLUS DEDUCTIONS (Check only if YES)
1 Diagnosis of Diabetes
2 Diagnosis of Hypertension
3 Hematocrit (M) < 41% (F) < 36%
4 Hemoglobin (M) < 14g/dl (F) < 12g/dl
5 Albumin Level <3.3g/dl
6 Febrile > 99.6◦F
7 5 (or more) Medications
8 Changes in mental status to confused, lethargic within 24 hours
TOTAL NUMBER OF CHECK MARKS
NORTON SCALE SCORE (From Above)
MINUS TOTAL CHECKMARKS
TOTAL NORTON PLUS SCORE (Score 10 or less = High Risk (Moderate 11-15) ASSESS DATE EVALUATOR SIGNATURE / TITLE ASSESS DATE EVALUATOR SIGNATURE / TITLE
1 3 2 4
NAME: Physician MR# Rm#
Source: Doreen Norton, Rhoda McLaren and AN Exton-Smith, An Investigation of Geriatric Nursing Problems in Hospital. National Corporation for the Care of Old
People (now Centre for Policy on Ageing), London, 1962
FH32 - Developed by Polaris Group www.polaris-group.com Page 34 of 51
Page 2 of 2
Date Progress Notes Resident: MR#: RM#:
FH32 - Developed by Polaris Group www.polaris-group.com Page 35 of 51
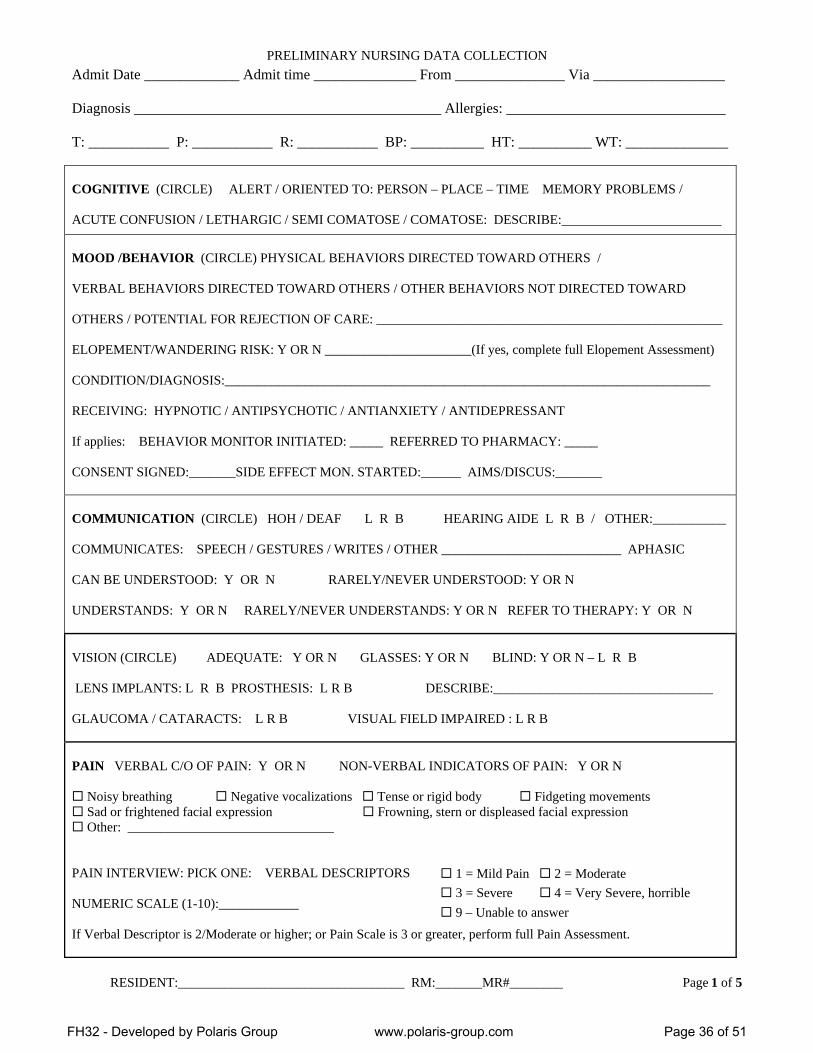
PRELIMINARY NURSING DATA COLLECTION
RESIDENT:__________________________________ RM:_______MR#________ Page 1 of 5
Admit Date _____________ Admit time ______________ From _______________ Via __________________ Diagnosis __________________________________________ Allergies: ______________________________ T: ___________ P: ___________ R: ___________ BP: __________ HT: __________ WT: ______________ COGNITIVE (CIRCLE) ALERT / ORIENTED TO: PERSON – PLACE – TIME MEMORY PROBLEMS / ACUTE CONFUSION / LETHARGIC / SEMI COMATOSE / COMATOSE: DESCRIBE:________________________
MOOD /BEHAVIOR (CIRCLE) PHYSICAL BEHAVIORS DIRECTED TOWARD OTHERS /
VERBAL BEHAVIORS DIRECTED TOWARD OTHERS / OTHER BEHAVIORS NOT DIRECTED TOWARD
OTHERS / POTENTIAL FOR REJECTION OF CARE: ____________________________________________________
ELOPEMENT/WANDERING RISK: Y OR N ______________________(If yes, complete full Elopement Assessment)
CONDITION/DIAGNOSIS:_________________________________________________________________________
RECEIVING: HYPNOTIC / ANTIPSYCHOTIC / ANTIANXIETY / ANTIDEPRESSANT If applies: BEHAVIOR MONITOR INITIATED: _____ REFERRED TO PHARMACY: _____ CONSENT SIGNED:_______SIDE EFFECT MON. STARTED:______ AIMS/DISCUS:_______ COMMUNICATION (CIRCLE) HOH / DEAF L R B HEARING AIDE L R B / OTHER:___________
COMMUNICATES: SPEECH / GESTURES / WRITES / OTHER ___________________________ APHASIC
CAN BE UNDERSTOOD: Y OR N RARELY/NEVER UNDERSTOOD: Y OR N
UNDERSTANDS: Y OR N RARELY/NEVER UNDERSTANDS: Y OR N REFER TO THERAPY: Y OR N
VISION (CIRCLE) ADEQUATE: Y OR N GLASSES: Y OR N BLIND: Y OR N – L R B
LENS IMPLANTS: L R B PROSTHESIS: L R B DESCRIBE:_________________________________
GLAUCOMA / CATARACTS: L R B VISUAL FIELD IMPAIRED : L R B
PAIN VERBAL C/O OF PAIN: Y OR N NON-VERBAL INDICATORS OF PAIN: Y OR N
Noisy breathing Negative vocalizations Tense or rigid body Fidgeting movements Sad or frightened facial expression Frowning, stern or displeased facial expression Other: _______________________________
PAIN INTERVIEW: PICK ONE: VERBAL DESCRIPTORS
NUMERIC SCALE (1-10):____________
If Verbal Descriptor is 2/Moderate or higher; or Pain Scale is 3 or greater, perform full Pain Assessment.
1 = Mild Pain 2 = Moderate 3 = Severe 4 = Very Severe, horrible 9 – Unable to answer
FH32 - Developed by Polaris Group www.polaris-group.com Page 36 of 51
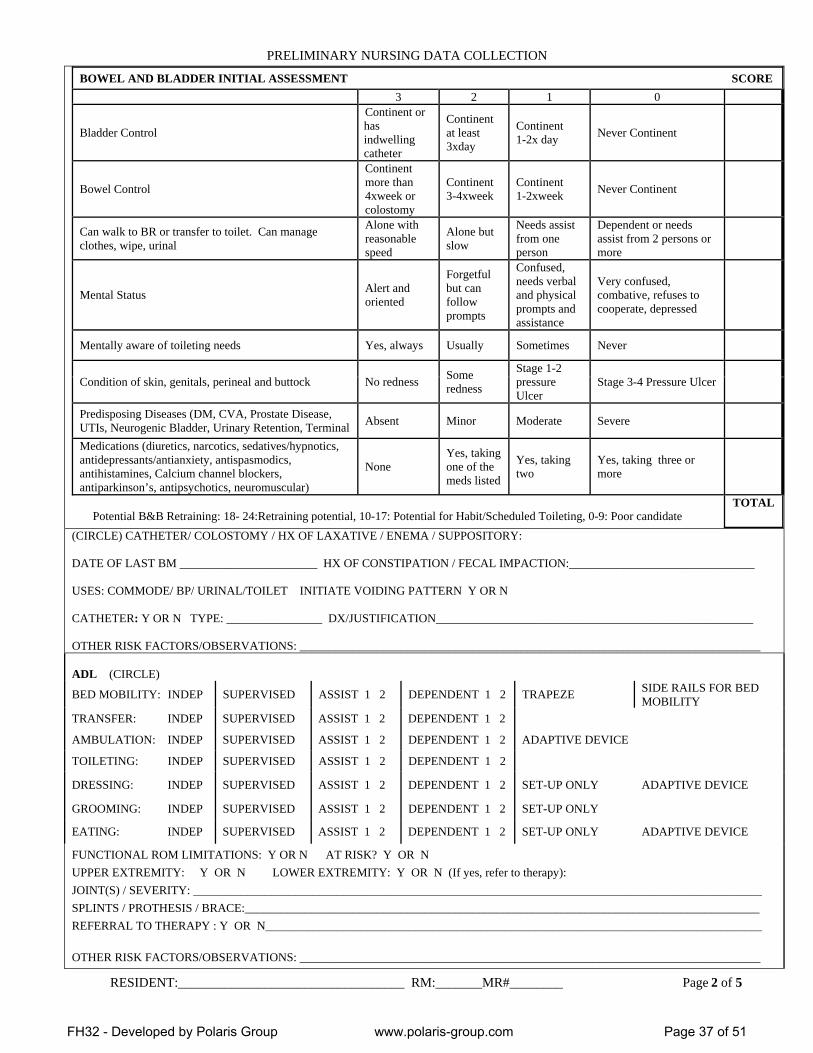
PRELIMINARY NURSING DATA COLLECTION
RESIDENT:__________________________________ RM:_______MR#________ Page 2 of 5
BOWEL AND BLADDER INITIAL ASSESSMENT SCORE 3 2 1 0
Bladder Control
Continent or has indwelling catheter
Continent at least 3xday
Continent 1-2x day Never Continent
Bowel Control
Continent more than 4xweek or colostomy
Continent 3-4xweek
Continent 1-2xweek Never Continent
Can walk to BR or transfer to toilet. Can manage clothes, wipe, urinal
Alone with reasonable speed
Alone but slow
Needs assist from one person
Dependent or needs assist from 2 persons or more
Mental Status Alert and oriented
Forgetful but can follow prompts
Confused, needs verbal and physical prompts and assistance
Very confused, combative, refuses to cooperate, depressed
Mentally aware of toileting needs Yes, always Usually Sometimes Never
Condition of skin, genitals, perineal and buttock No redness Some redness
Stage 1-2 pressure Ulcer
Stage 3-4 Pressure Ulcer
Predisposing Diseases (DM, CVA, Prostate Disease, UTIs, Neurogenic Bladder, Urinary Retention, Terminal Absent Minor Moderate Severe
Medications (diuretics, narcotics, sedatives/hypnotics, antidepressants/antianxiety, antispasmodics, antihistamines, Calcium channel blockers, antiparkinson’s, antipsychotics, neuromuscular)
None Yes, taking one of the meds listed
Yes, taking two
Yes, taking three or more
Potential B&B Retraining: 18- 24:Retraining potential, 10-17: Potential for Habit/Scheduled Toileting, 0-9: Poor candidate
TOTAL
(CIRCLE) CATHETER/ COLOSTOMY / HX OF LAXATIVE / ENEMA / SUPPOSITORY:
DATE OF LAST BM _______________________ HX OF CONSTIPATION / FECAL IMPACTION:_______________________________
USES: COMMODE/ BP/ URINAL/TOILET INITIATE VOIDING PATTERN Y OR N CATHETER: Y OR N TYPE: ________________ DX/JUSTIFICATION_____________________________________________________ OTHER RISK FACTORS/OBSERVATIONS: _____________________________________________________________________________ ADL (CIRCLE)
BED MOBILITY: INDEP SUPERVISED ASSIST 1 2 DEPENDENT 1 2 TRAPEZE SIDE RAILS FOR BED MOBILITY
TRANSFER: INDEP SUPERVISED ASSIST 1 2 DEPENDENT 1 2
AMBULATION: INDEP SUPERVISED ASSIST 1 2 DEPENDENT 1 2 ADAPTIVE DEVICE
TOILETING: INDEP SUPERVISED ASSIST 1 2 DEPENDENT 1 2
DRESSING: INDEP SUPERVISED ASSIST 1 2 DEPENDENT 1 2 SET-UP ONLY ADAPTIVE DEVICE
GROOMING: INDEP SUPERVISED ASSIST 1 2 DEPENDENT 1 2 SET-UP ONLY
EATING: INDEP SUPERVISED ASSIST 1 2 DEPENDENT 1 2 SET-UP ONLY ADAPTIVE DEVICE
FUNCTIONAL ROM LIMITATIONS: Y OR N AT RISK? Y OR N UPPER EXTREMITY: Y OR N LOWER EXTREMITY: Y OR N (If yes, refer to therapy): JOINT(S) / SEVERITY: _______________________________________________________________________________________________ SPLINTS / PROTHESIS / BRACE:______________________________________________________________________________________ REFERRAL TO THERAPY : Y OR N___________________________________________________________________________________ OTHER RISK FACTORS/OBSERVATIONS: _____________________________________________________________________________
FH32 - Developed by Polaris Group www.polaris-group.com Page 37 of 51
PRELIMINARY NURSING DATA COLLECTION
RESIDENT:__________________________________ RM:_______MR#________ Page 3 of 5
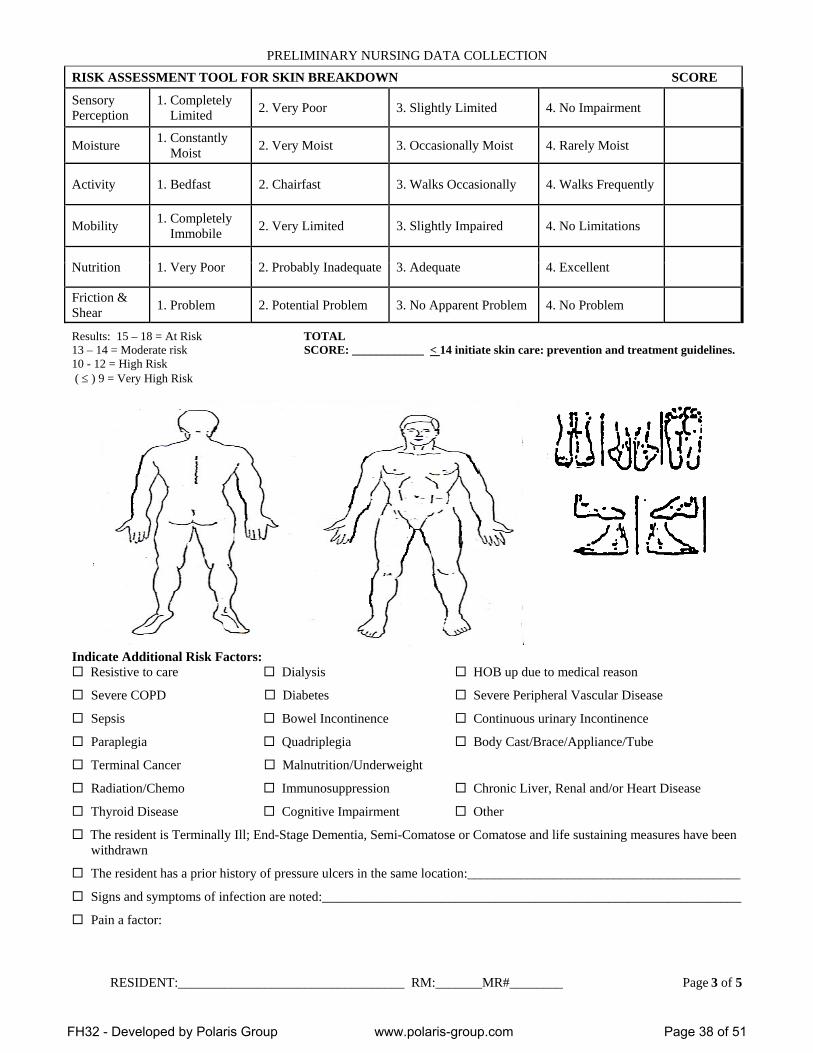
RISK ASSESSMENT TOOL FOR SKIN BREAKDOWN SCORE
Sensory Perception
1. Completely Limited 2. Very Poor 3. Slightly Limited 4. No Impairment
Moisture 1. Constantly Moist 2. Very Moist 3. Occasionally Moist 4. Rarely Moist
Activity 1. Bedfast 2. Chairfast 3. Walks Occasionally 4. Walks Frequently
Mobility 1. Completely Immobile 2. Very Limited 3. Slightly Impaired 4. No Limitations
Nutrition 1. Very Poor 2. Probably Inadequate 3. Adequate 4. Excellent
Friction & Shear 1. Problem 2. Potential Problem 3. No Apparent Problem 4. No Problem
Results: 15 – 18 = At Risk TOTAL 13 – 14 = Moderate risk SCORE: ____________ < 14 initiate skin care: prevention and treatment guidelines. 10 - 12 = High Risk ( ≤ ) 9 = Very High Risk
Indicate Additional Risk Factors: Resistive to care Dialysis HOB up due to medical reason
Severe COPD Diabetes Severe Peripheral Vascular Disease
Sepsis Bowel Incontinence Continuous urinary Incontinence
Paraplegia Quadriplegia Body Cast/Brace/Appliance/Tube
Terminal Cancer Malnutrition/Underweight
Radiation/Chemo Immunosuppression Chronic Liver, Renal and/or Heart Disease
Thyroid Disease Cognitive Impairment Other
The resident is Terminally Ill; End-Stage Dementia, Semi-Comatose or Comatose and life sustaining measures have been withdrawn
The resident has a prior history of pressure ulcers in the same location:_________________________________________
Signs and symptoms of infection are noted:_______________________________________________________________
Pain a factor:
FH32 - Developed by Polaris Group www.polaris-group.com Page 38 of 51
PRELIMINARY NURSING DATA COLLECTION
RESIDENT:__________________________________ RM:_______MR#________ Page 4 of 5
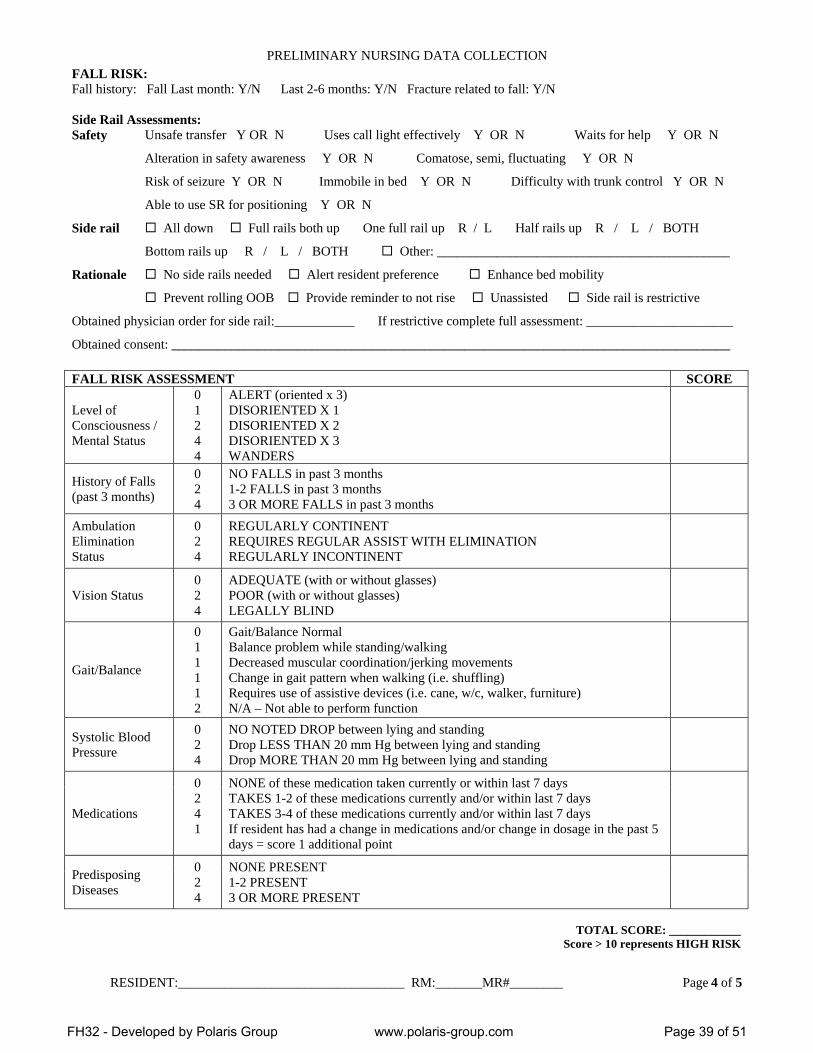
FALL RISK: Fall history: Fall Last month: Y/N Last 2-6 months: Y/N Fracture related to fall: Y/N Side Rail Assessments: Safety
Unsafe transfer Y OR N Uses call light effectively Y OR N Waits for help Y OR N
Alteration in safety awareness Y OR N Comatose, semi, fluctuating Y OR N
Risk of seizure Y OR N Immobile in bed Y OR N Difficulty with trunk control Y OR N
Able to use SR for positioning Y OR N
Side rail
All down Full rails both up One full rail up R / L Half rails up R / L / BOTH
Bottom rails up R / L / BOTH Other: ____________________________________________
Rationale
No side rails needed Alert resident preference Enhance bed mobility
Prevent rolling OOB Provide reminder to not rise Unassisted Side rail is restrictive
Obtained physician order for side rail:____________ If restrictive complete full assessment: ______________________
Obtained consent: ____________________________________________________________________________________
FALL RISK ASSESSMENT SCORE
Level of Consciousness / Mental Status
0 1 2 4 4
ALERT (oriented x 3) DISORIENTED X 1 DISORIENTED X 2 DISORIENTED X 3 WANDERS
History of Falls (past 3 months)
0 2 4
NO FALLS in past 3 months 1-2 FALLS in past 3 months 3 OR MORE FALLS in past 3 months
Ambulation Elimination Status
0 2 4
REGULARLY CONTINENT REQUIRES REGULAR ASSIST WITH ELIMINATION REGULARLY INCONTINENT
Vision Status 0 2 4
ADEQUATE (with or without glasses) POOR (with or without glasses) LEGALLY BLIND
Gait/Balance
0 1 1 1 1 2
Gait/Balance Normal Balance problem while standing/walking Decreased muscular coordination/jerking movements Change in gait pattern when walking (i.e. shuffling) Requires use of assistive devices (i.e. cane, w/c, walker, furniture) N/A – Not able to perform function
Systolic Blood Pressure
0 2 4
NO NOTED DROP between lying and standing Drop LESS THAN 20 mm Hg between lying and standing Drop MORE THAN 20 mm Hg between lying and standing
Medications
0 2 4 1
NONE of these medication taken currently or within last 7 days TAKES 1-2 of these medications currently and/or within last 7 days TAKES 3-4 of these medications currently and/or within last 7 days If resident has had a change in medications and/or change in dosage in the past 5 days = score 1 additional point
Predisposing Diseases
0 2 4
NONE PRESENT 1-2 PRESENT 3 OR MORE PRESENT
TOTAL SCORE: ____________ Score > 10 represents HIGH RISK
FH32 - Developed by Polaris Group www.polaris-group.com Page 39 of 51
PRELIMINARY NURSING DATA COLLECTION
RESIDENT:__________________________________ RM:_______MR#________ Page 5 of 5
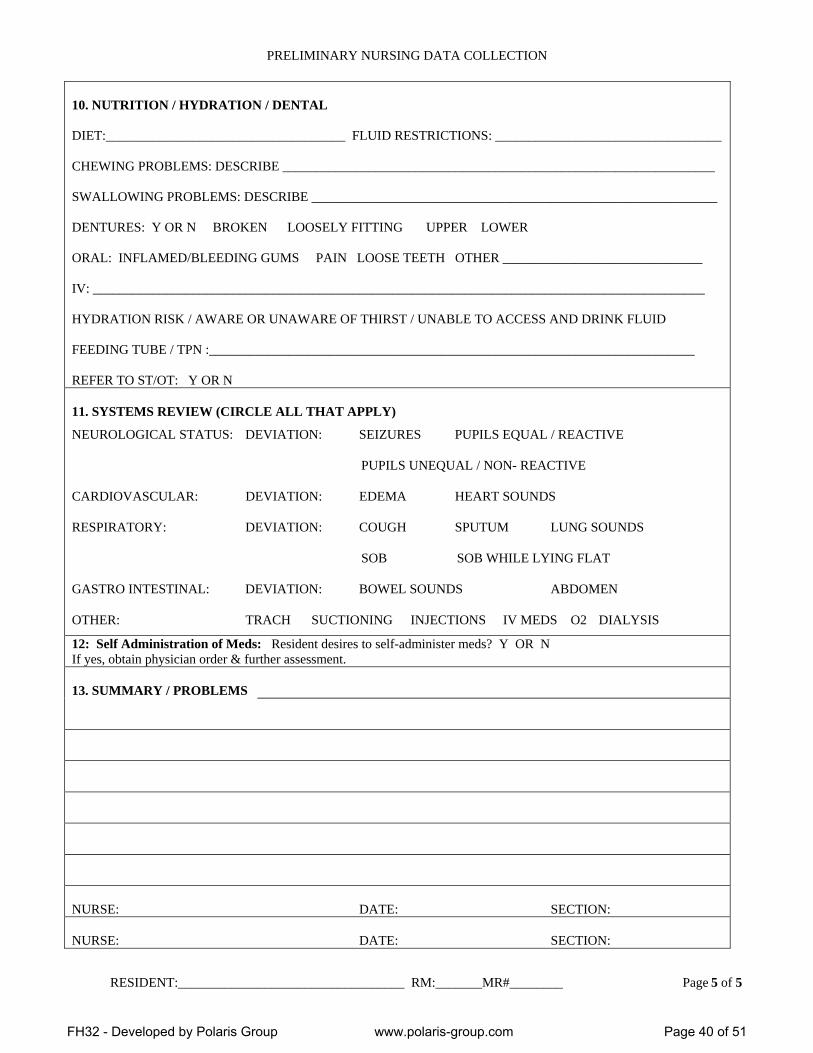
10. NUTRITION / HYDRATION / DENTAL
DIET:____________________________________ FLUID RESTRICTIONS: __________________________________
CHEWING PROBLEMS: DESCRIBE _________________________________________________________________
SWALLOWING PROBLEMS: DESCRIBE _____________________________________________________________
DENTURES: Y OR N BROKEN LOOSELY FITTING UPPER LOWER
ORAL: INFLAMED/BLEEDING GUMS PAIN LOOSE TEETH OTHER ______________________________
IV: ____________________________________________________________________________________________
HYDRATION RISK / AWARE OR UNAWARE OF THIRST / UNABLE TO ACCESS AND DRINK FLUID
FEEDING TUBE / TPN :_________________________________________________________________________
REFER TO ST/OT: Y OR N 11. SYSTEMS REVIEW (CIRCLE ALL THAT APPLY)
NEUROLOGICAL STATUS: DEVIATION: SEIZURES PUPILS EQUAL / REACTIVE
PUPILS UNEQUAL / NON- REACTIVE
CARDIOVASCULAR: DEVIATION: EDEMA HEART SOUNDS
RESPIRATORY: DEVIATION: COUGH SPUTUM LUNG SOUNDS
SOB SOB WHILE LYING FLAT
GASTRO INTESTINAL: DEVIATION: BOWEL SOUNDS ABDOMEN
OTHER: TRACH SUCTIONING INJECTIONS IV MEDS O2 DIALYSIS
12: Self Administration of Meds: Resident desires to self-administer meds? Y OR N If yes, obtain physician order & further assessment. 13. SUMMARY / PROBLEMS
NURSE: DATE: SECTION: NURSE: DATE: SECTION:
FH32 - Developed by Polaris Group www.polaris-group.com Page 40 of 51
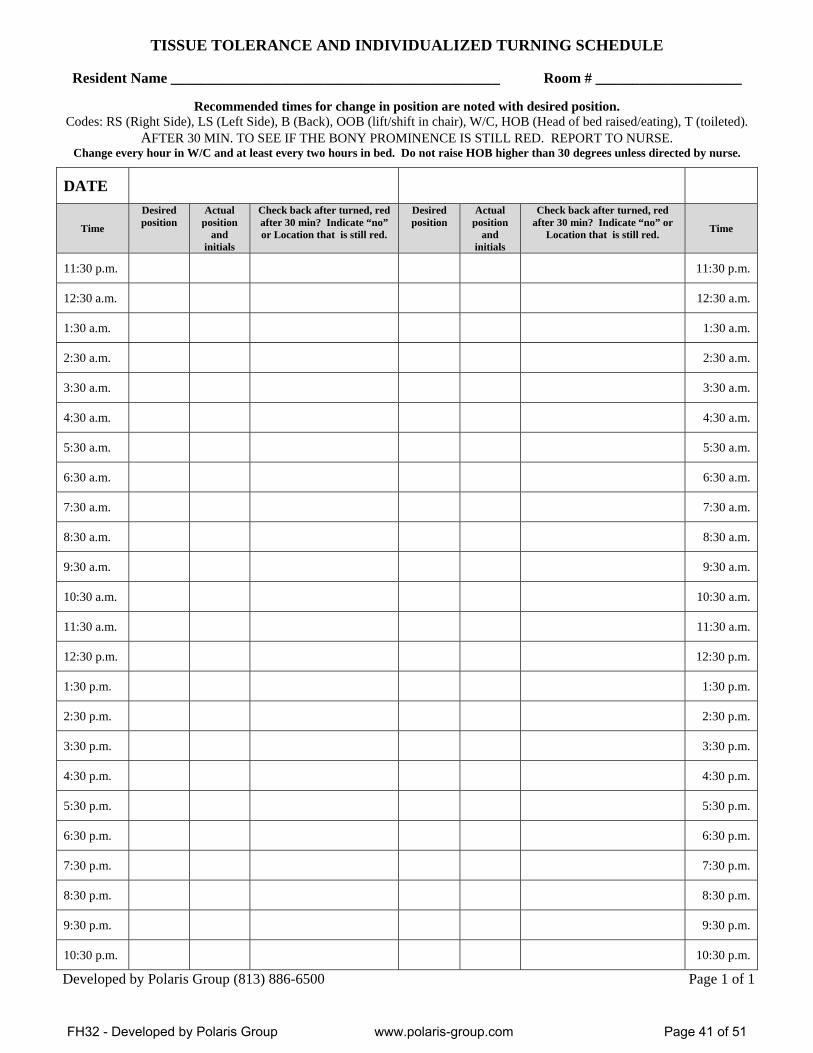
TISSUE TOLERANCE AND INDIVIDUALIZED TURNING SCHEDULE
Resident Name _____________________________________________ Room # ____________________
Recommended times for change in position are noted with desired position. Codes: RS (Right Side), LS (Left Side), B (Back), OOB (lift/shift in chair), W/C, HOB (Head of bed raised/eating), T (toileted).
AFTER 30 MIN. TO SEE IF THE BONY PROMINENCE IS STILL RED. REPORT TO NURSE. Change every hour in W/C and at least every two hours in bed. Do not raise HOB higher than 30 degrees unless directed by nurse.
Developed by Polaris Group (813) 886-6500 Page 1 of 1
DATE
Time
Desired position
Actual position
and initials
Check back after turned, red after 30 min? Indicate “no” or Location that is still red.
Desired position
Actual position
and initials
Check back after turned, red after 30 min? Indicate “no” or
Location that is still red. Time
11:30 p.m. 11:30 p.m.
12:30 a.m. 12:30 a.m.
1:30 a.m. 1:30 a.m.
2:30 a.m. 2:30 a.m.
3:30 a.m. 3:30 a.m.
4:30 a.m. 4:30 a.m.
5:30 a.m. 5:30 a.m.
6:30 a.m. 6:30 a.m.
7:30 a.m. 7:30 a.m.
8:30 a.m. 8:30 a.m.
9:30 a.m. 9:30 a.m.
10:30 a.m. 10:30 a.m.
11:30 a.m. 11:30 a.m.
12:30 p.m. 12:30 p.m.
1:30 p.m. 1:30 p.m.
2:30 p.m. 2:30 p.m.
3:30 p.m. 3:30 p.m.
4:30 p.m. 4:30 p.m.
5:30 p.m. 5:30 p.m.
6:30 p.m. 6:30 p.m.
7:30 p.m. 7:30 p.m.
8:30 p.m. 8:30 p.m.
9:30 p.m. 9:30 p.m.
10:30 p.m. 10:30 p.m.
FH32 - Developed by Polaris Group www.polaris-group.com Page 41 of 51
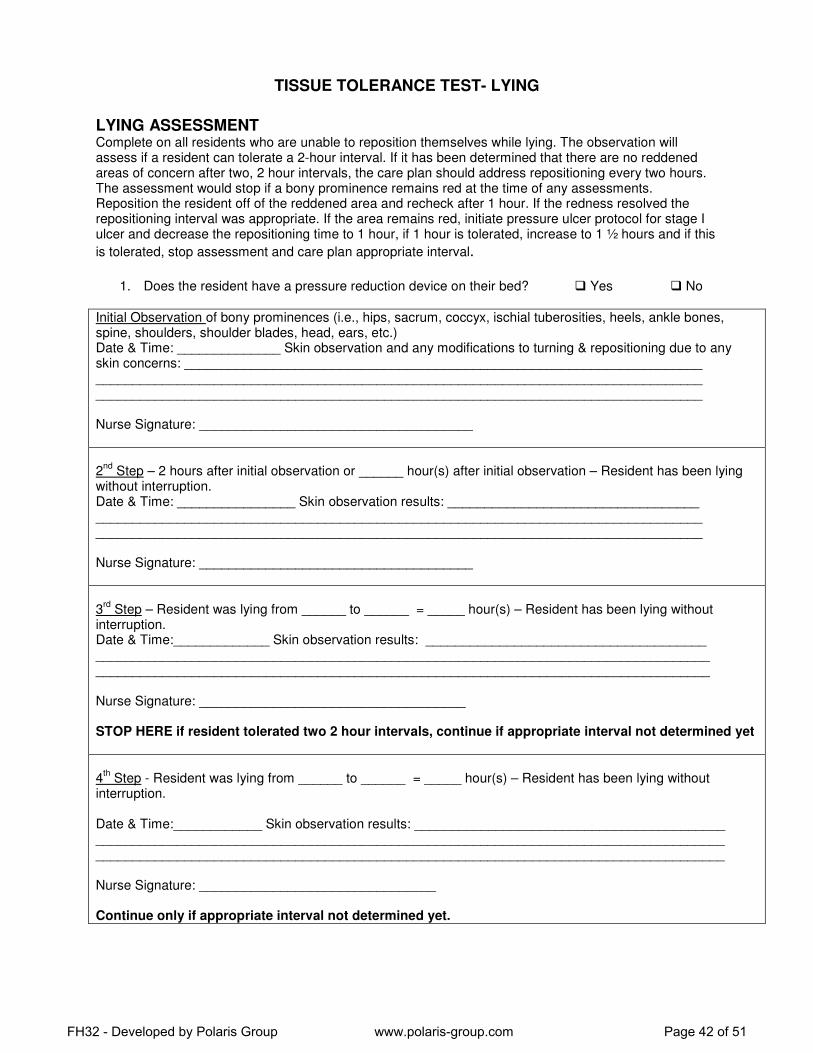
TISSUE TOLERANCE TEST- LYING
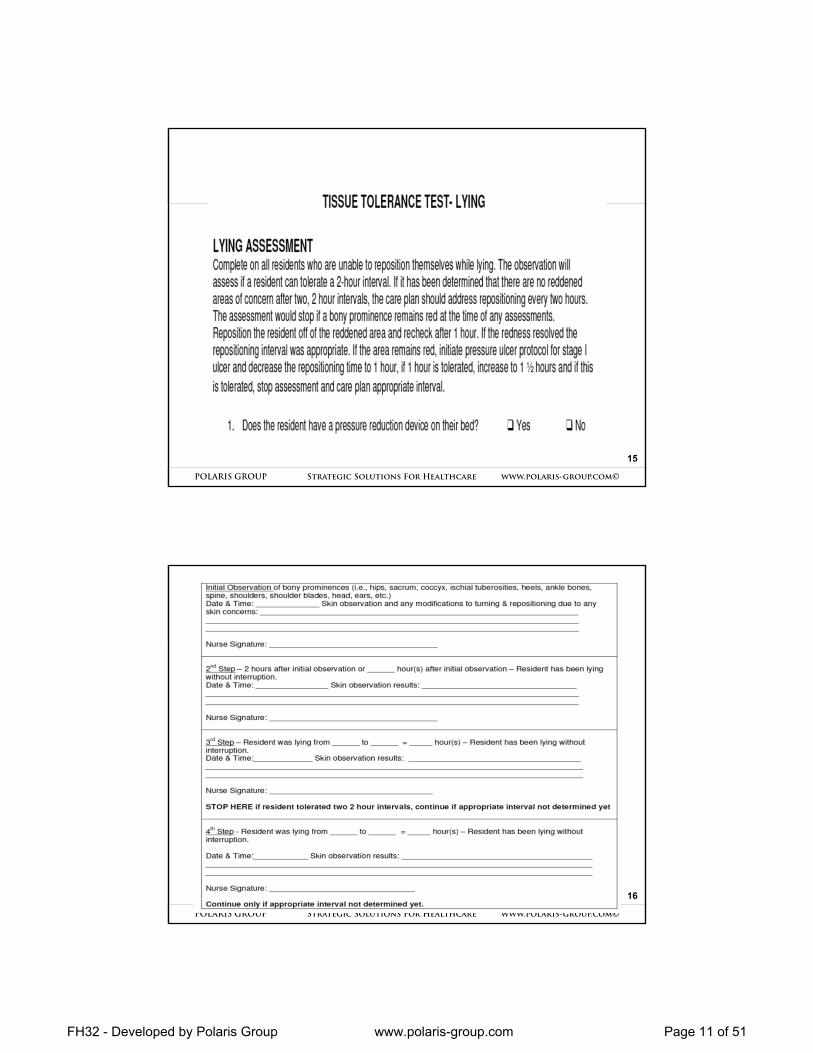
LYING ASSESSMENT Complete on all residents who are unable to reposition themselves while lying. The observation will assess if a resident can tolerate a 2-hour interval. If it has been determined that there are no reddened areas of concern after two, 2 hour intervals, the care plan should address repositioning every two hours. The assessment would stop if a bony prominence remains red at the time of any assessments. Reposition the resident off of the reddened area and recheck after 1 hour. If the redness resolved the repositioning interval was appropriate. If the area remains red, initiate pressure ulcer protocol for stage I ulcer and decrease the repositioning time to 1 hour, if 1 hour is tolerated, increase to 1 ½ hours and if this
is tolerated, stop assessment and care plan appropriate interval.
1. Does the resident have a pressure reduction device on their bed? � Yes � No
Initial Observation of bony prominences (i.e., hips, sacrum, coccyx, ischial tuberosities, heels, ankle bones, spine, shoulders, shoulder blades, head, ears, etc.) Date & Time: ______________ Skin observation and any modifications to turning & repositioning due to any skin concerns: ______________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ Nurse Signature: _____________________________________
2
nd Step – 2 hours after initial observation or ______ hour(s) after initial observation – Resident has been lying
without interruption. Date & Time: ________________ Skin observation results: __________________________________ __________________________________________________________________________________ __________________________________________________________________________________ Nurse Signature: _____________________________________
3
rd Step – Resident was lying from ______ to ______ = _____ hour(s) – Resident has been lying without
interruption. Date & Time:_____________ Skin observation results: ______________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ Nurse Signature: ____________________________________ STOP HERE if resident tolerated two 2 hour intervals, continue if appropriate interval not determined yet
4
th Step - Resident was lying from ______ to ______ = _____ hour(s) – Resident has been lying without
interruption. Date & Time:____________ Skin observation results: __________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Nurse Signature: ________________________________ Continue only if appropriate interval not determined yet.
FH32 - Developed by Polaris Group www.polaris-group.com Page 42 of 51
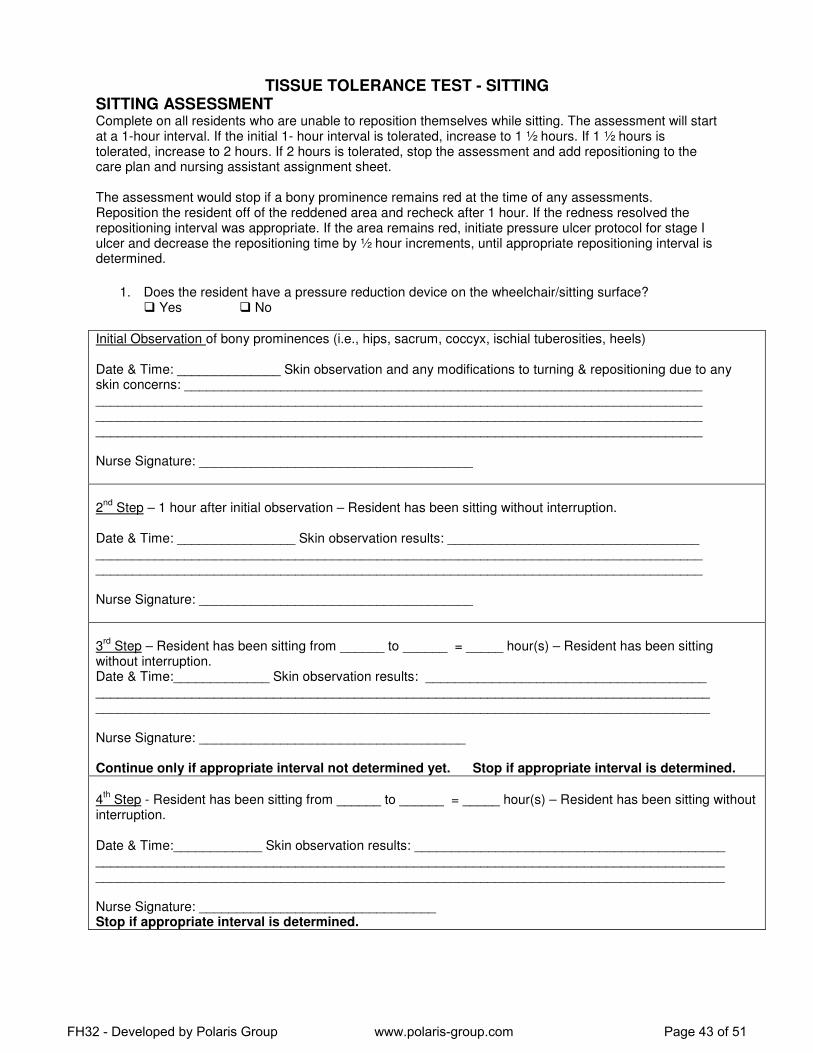
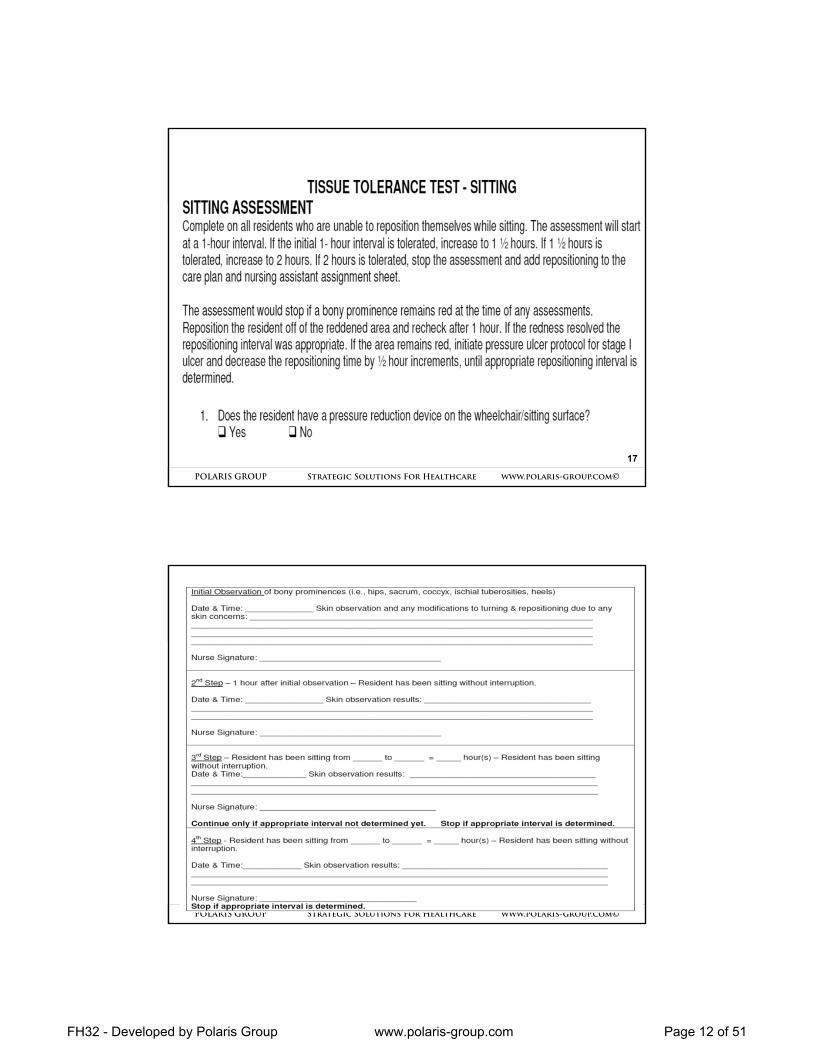
TISSUE TOLERANCE TEST - SITTING SITTING ASSESSMENT Complete on all residents who are unable to reposition themselves while sitting. The assessment will start at a 1-hour interval. If the initial 1- hour interval is tolerated, increase to 1 ½ hours. If 1 ½ hours is tolerated, increase to 2 hours. If 2 hours is tolerated, stop the assessment and add repositioning to the care plan and nursing assistant assignment sheet. The assessment would stop if a bony prominence remains red at the time of any assessments. Reposition the resident off of the reddened area and recheck after 1 hour. If the redness resolved the repositioning interval was appropriate. If the area remains red, initiate pressure ulcer protocol for stage I ulcer and decrease the repositioning time by ½ hour increments, until appropriate repositioning interval is determined.
1. Does the resident have a pressure reduction device on the wheelchair/sitting surface? � Yes � No
Initial Observation of bony prominences (i.e., hips, sacrum, coccyx, ischial tuberosities, heels) Date & Time: ______________ Skin observation and any modifications to turning & repositioning due to any skin concerns: ______________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ Nurse Signature: _____________________________________
2
nd Step – 1 hour after initial observation – Resident has been sitting without interruption.
Date & Time: ________________ Skin observation results: __________________________________ __________________________________________________________________________________ __________________________________________________________________________________ Nurse Signature: _____________________________________
3
rd Step – Resident has been sitting from ______ to ______ = _____ hour(s) – Resident has been sitting
without interruption. Date & Time:_____________ Skin observation results: ______________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ Nurse Signature: ____________________________________ Continue only if appropriate interval not determined yet. Stop if appropriate interval is determined.
4
th Step - Resident has been sitting from ______ to ______ = _____ hour(s) – Resident has been sitting without
interruption. Date & Time:____________ Skin observation results: __________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Nurse Signature: ________________________________ Stop if appropriate interval is determined.
FH32 - Developed by Polaris Group www.polaris-group.com Page 43 of 51
Developed by Polaris Group (813) 886-6500 Page 1 of 1
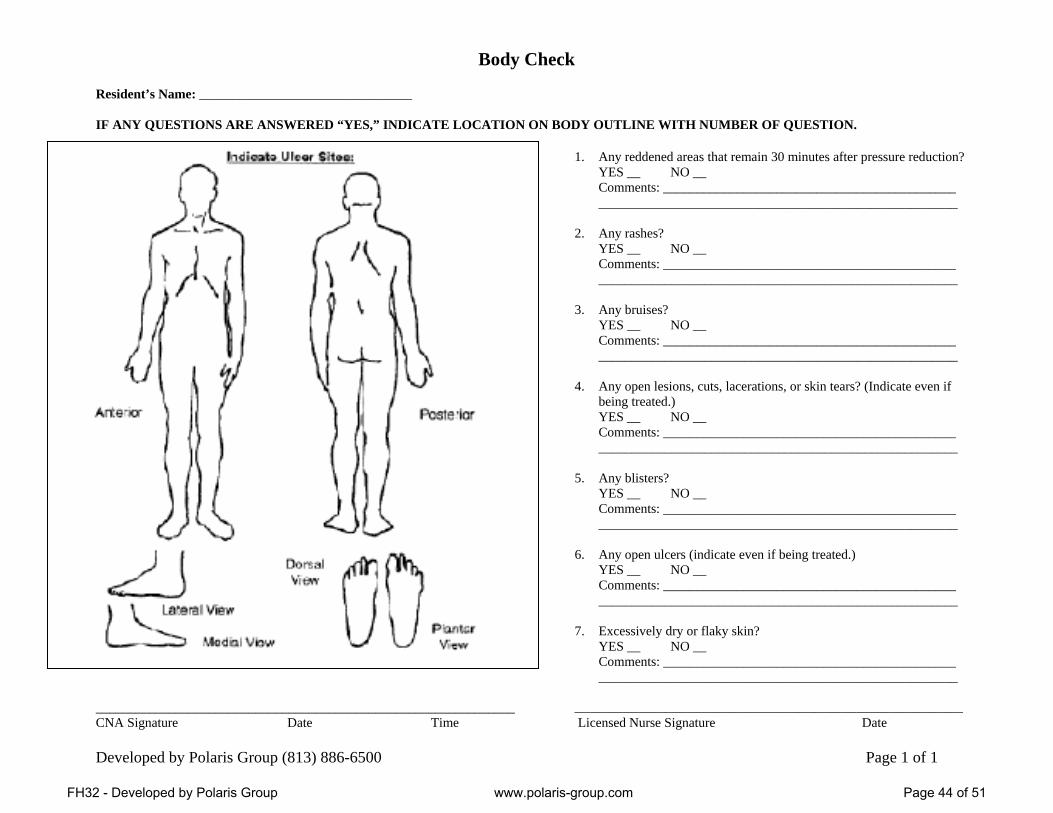
Body Check
Resident’s Name: ________________________________ IF ANY QUESTIONS ARE ANSWERED “YES,” INDICATE LOCATION ON BODY OUTLINE WITH NUMBER OF QUESTION.
1. Any reddened areas that remain 30 minutes after pressure reduction? YES __ NO __ Comments: ____________________________________________ ______________________________________________________
2. Any rashes? YES __ NO __ Comments: ____________________________________________ ______________________________________________________
3. Any bruises? YES __ NO __ Comments: ____________________________________________ ______________________________________________________
4. Any open lesions, cuts, lacerations, or skin tears? (Indicate even if being treated.) YES __ NO __ Comments: ____________________________________________ ______________________________________________________
5. Any blisters? YES __ NO __ Comments: ____________________________________________ ______________________________________________________
6. Any open ulcers (indicate even if being treated.) YES __ NO __ Comments: ____________________________________________ ______________________________________________________
7. Excessively dry or flaky skin? YES __ NO __ Comments: ____________________________________________ ______________________________________________________
_______________________________________________________________ _________________________________________________________________________ CNA Signature Date Time Licensed Nurse Signature Date
FH32 - Developed by Polaris Group www.polaris-group.com Page 44 of 51
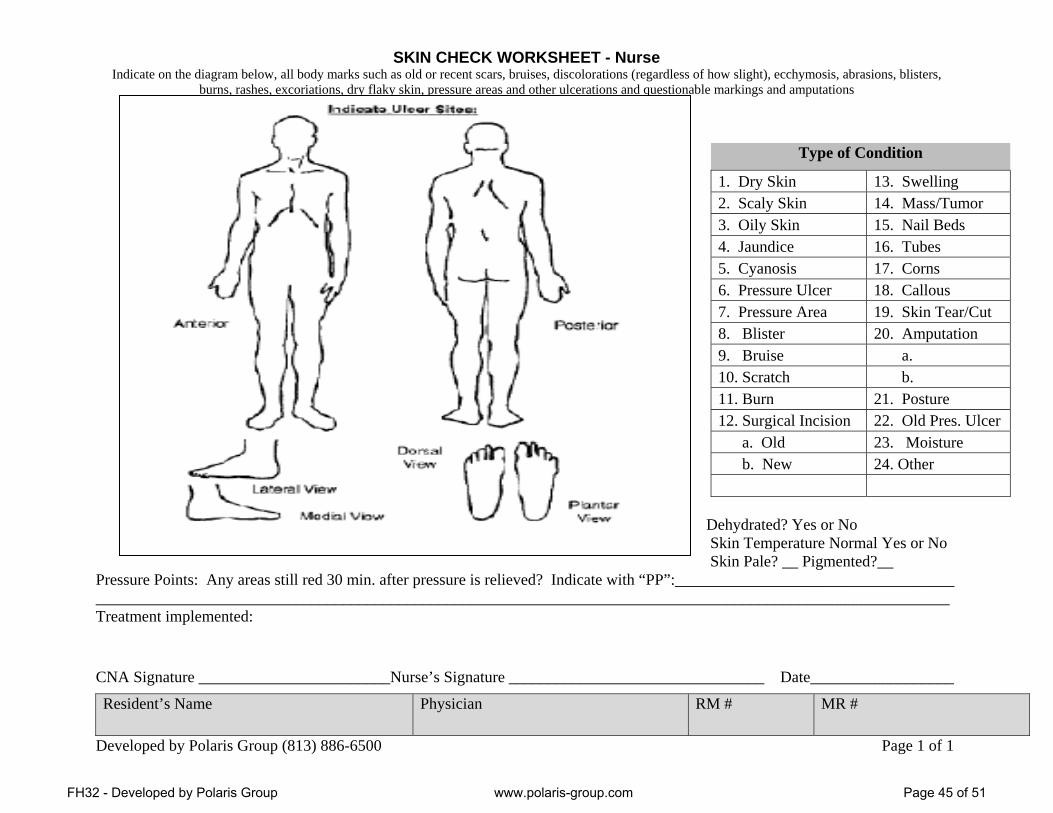
SKIN CHECK WORKSHEET - Nurse Indicate on the diagram below, all body marks such as old or recent scars, bruises, discolorations (regardless of how slight), ecchymosis, abrasions, blisters,
burns, rashes, excoriations, dry flaky skin, pressure areas and other ulcerations and questionable markings and amputations
Type of Condition
1. Dry Skin 13. Swelling 2. Scaly Skin 14. Mass/Tumor 3. Oily Skin 15. Nail Beds 4. Jaundice 16. Tubes 5. Cyanosis 17. Corns 6. Pressure Ulcer 18. Callous 7. Pressure Area 19. Skin Tear/Cut 8. Blister 20. Amputation 9. Bruise a. 10. Scratch b. 11. Burn 21. Posture 12. Surgical Incision 22. Old Pres. Ulcer a. Old 23. Moisture b. New 24. Other
Dehydrated? Yes or No Skin Temperature Normal Yes or No Skin Pale? __ Pigmented?__ Pressure Points: Any areas still red 30 min. after pressure is relieved? Indicate with “PP”:___________________________________ ___________________________________________________________________________________________________________ Treatment implemented:
CNA Signature ________________________Nurse’s Signature ________________________________ Date__________________
Resident’s Name Physician RM # MR #
Developed by Polaris Group (813) 886-6500 Page 1 of 1
FH32 - Developed by Polaris Group www.polaris-group.com Page 45 of 51
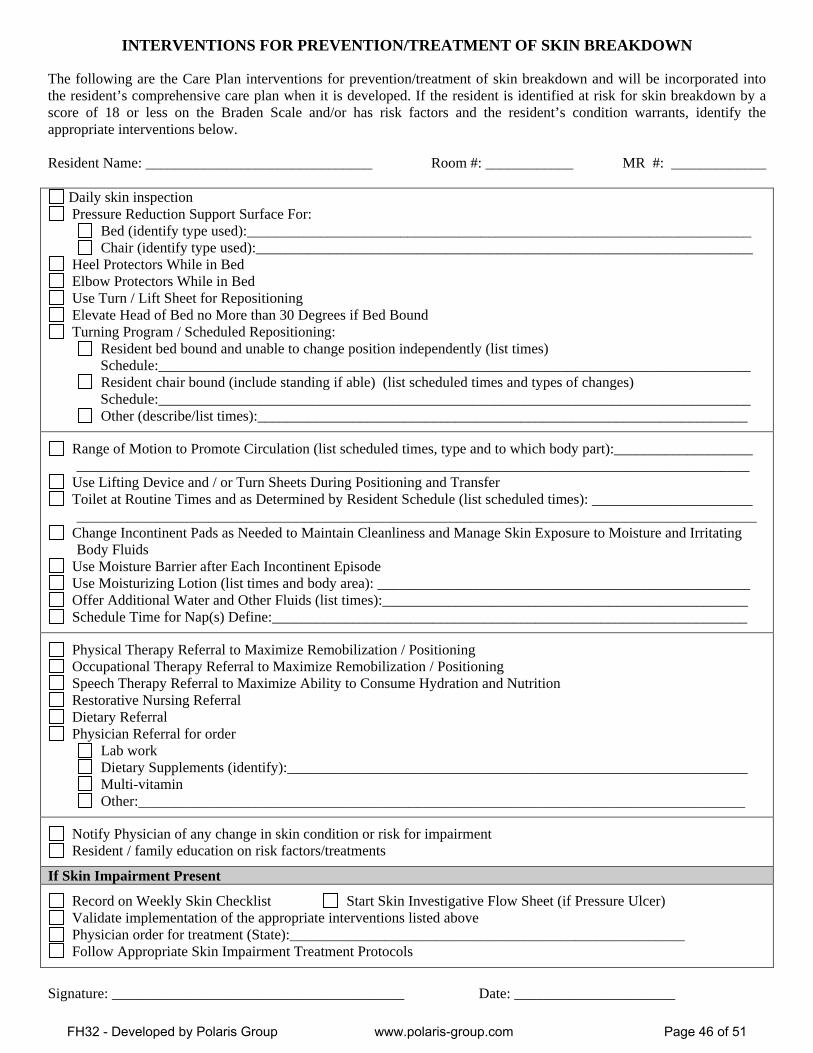
INTERVENTIONS FOR PREVENTION/TREATMENT OF SKIN BREAKDOWN
The following are the Care Plan interventions for prevention/treatment of skin breakdown and will be incorporated into the resident’s comprehensive care plan when it is developed. If the resident is identified at risk for skin breakdown by a score of 18 or less on the Braden Scale and/or has risk factors and the resident’s condition warrants, identify the appropriate interventions below. Resident Name: _______________________________ Room #: ____________ MR #: _____________ Daily skin inspection
Pressure Reduction Support Surface For: Bed (identify type used):_____________________________________________________________________ Chair (identify type used):____________________________________________________________________
Heel Protectors While in Bed Elbow Protectors While in Bed Use Turn / Lift Sheet for Repositioning Elevate Head of Bed no More than 30 Degrees if Bed Bound Turning Program / Scheduled Repositioning:
Resident bed bound and unable to change position independently (list times) Schedule:_________________________________________________________________________________
Resident chair bound (include standing if able) (list scheduled times and types of changes) Schedule:_________________________________________________________________________________
Other (describe/list times):___________________________________________________________________
Range of Motion to Promote Circulation (list scheduled times, type and to which body part):___________________ ____________________________________________________________________________________________
Use Lifting Device and / or Turn Sheets During Positioning and Transfer Toilet at Routine Times and as Determined by Resident Schedule (list scheduled times): ______________________
_____________________________________________________________________________________________ Change Incontinent Pads as Needed to Maintain Cleanliness and Manage Skin Exposure to Moisture and Irritating
Body Fluids Use Moisture Barrier after Each Incontinent Episode Use Moisturizing Lotion (list times and body area): ___________________________________________________ Offer Additional Water and Other Fluids (list times):__________________________________________________ Schedule Time for Nap(s) Define:_________________________________________________________________
Physical Therapy Referral to Maximize Remobilization / Positioning Occupational Therapy Referral to Maximize Remobilization / Positioning Speech Therapy Referral to Maximize Ability to Consume Hydration and Nutrition Restorative Nursing Referral Dietary Referral Physician Referral for order
Lab work Dietary Supplements (identify):_______________________________________________________________ Multi-vitamin Other:___________________________________________________________________________________
Notify Physician of any change in skin condition or risk for impairment Resident / family education on risk factors/treatments
If Skin Impairment Present
Record on Weekly Skin Checklist Start Skin Investigative Flow Sheet (if Pressure Ulcer) Validate implementation of the appropriate interventions listed above Physician order for treatment (State):______________________________________________________ Follow Appropriate Skin Impairment Treatment Protocols
Signature: ________________________________________ Date: ______________________
FH32 - Developed by Polaris Group www.polaris-group.com Page 46 of 51
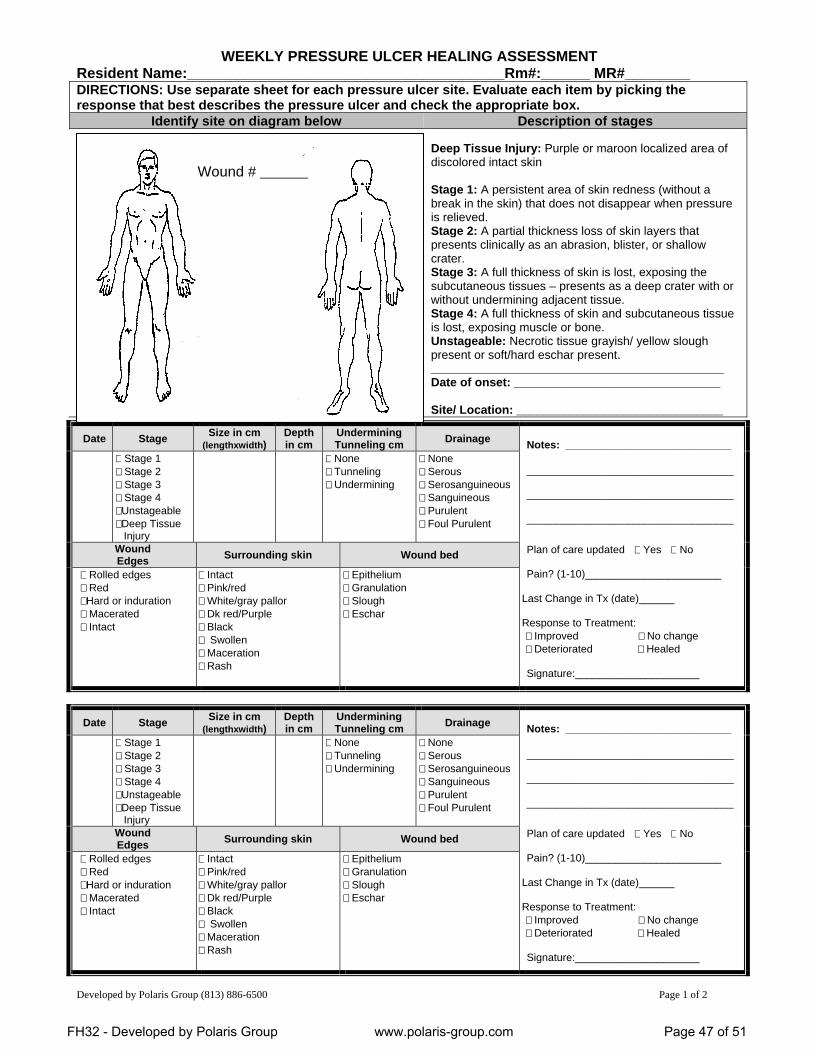
WEEKLY PRESSURE ULCER HEALING ASSESSMENT Resident Name:_______________________________________Rm#:______ MR#________ DIRECTIONS: Use separate sheet for each pressure ulcer site. Evaluate each item by picking the response that best describes the pressure ulcer and check the appropriate box.
Identify site on diagram below Description of stages
Deep Tissue Injury: Purple or maroon localized area of discolored intact skin Stage 1: A persistent area of skin redness (without a break in the skin) that does not disappear when pressure is relieved. Stage 2: A partial thickness loss of skin layers that presents clinically as an abrasion, blister, or shallow crater. Stage 3: A full thickness of skin is lost, exposing the subcutaneous tissues – presents as a deep crater with or without undermining adjacent tissue. Stage 4: A full thickness of skin and subcutaneous tissue is lost, exposing muscle or bone. Unstageable: Necrotic tissue grayish/ yellow slough present or soft/hard eschar present. ____________________________________________ Date of onset: _______________________________ Site/ Location: _______________________________
Date Stage Size in cm (lengthxwidth)
Depth in cm
Undermining Tunneling cm Drainage
Notes: ____________________________ Stage 1
Stage 2 Stage 3 Stage 4 Unstageable Deep Tissue
Injury
None Tunneling Undermining
None Serous Serosanguineous Sanguineous Purulent Foul Purulent
___________________________________ ___________________________________ ___________________________________
Wound Edges Surrounding skin Wound bed Plan of care updated Yes No
Rolled edges Red Hard or induration Macerated Intact
Intact Pink/red White/gray pallor Dk red/Purple Black Swollen Maceration Rash
Epithelium Granulation Slough Eschar
Pain? (1-10)_______________________ Last Change in Tx (date)______ Response to Treatment: Improved No change Deteriorated Healed Signature:_____________________
Date Stage Size in cm (lengthxwidth)
Depth in cm
Undermining Tunneling cm Drainage
Notes: ____________________________ Stage 1
Stage 2 Stage 3 Stage 4 Unstageable Deep Tissue
Injury
None Tunneling Undermining
None Serous Serosanguineous Sanguineous Purulent Foul Purulent
___________________________________ ___________________________________ ___________________________________
Wound Edges Surrounding skin Wound bed Plan of care updated Yes No
Rolled edges Red Hard or induration Macerated Intact
Intact Pink/red White/gray pallor Dk red/Purple Black Swollen Maceration Rash
Epithelium Granulation Slough Eschar
Pain? (1-10)_______________________ Last Change in Tx (date)______ Response to Treatment: Improved No change Deteriorated Healed Signature:_____________________
Developed by Polaris Group (813) 886-6500 Page 1 of 2
Wound # ______
FH32 - Developed by Polaris Group www.polaris-group.com Page 47 of 51
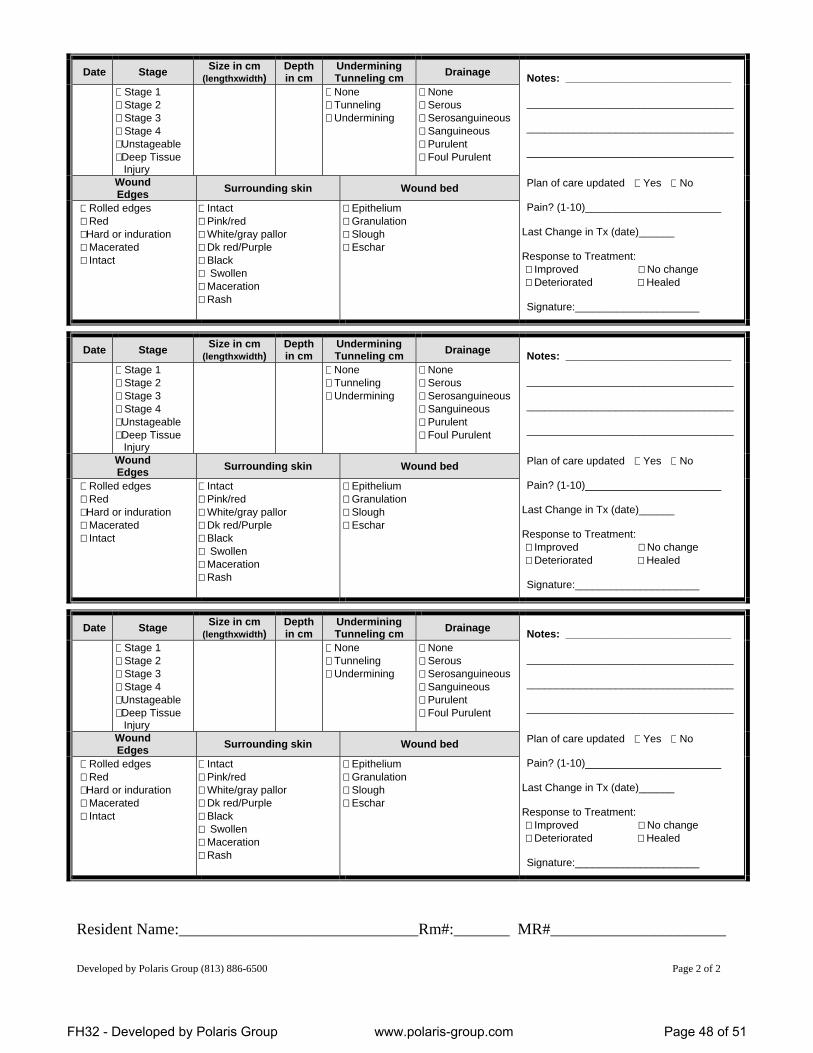
Date Stage Size in cm (lengthxwidth)
Depth in cm
Undermining Tunneling cm Drainage
Notes: ____________________________ Stage 1
Stage 2 Stage 3 Stage 4 Unstageable Deep Tissue
Injury
None Tunneling Undermining
None Serous Serosanguineous Sanguineous Purulent Foul Purulent
___________________________________ ___________________________________ ___________________________________
Wound Edges Surrounding skin Wound bed Plan of care updated Yes No
Rolled edges Red Hard or induration Macerated Intact
Intact Pink/red White/gray pallor Dk red/Purple Black Swollen Maceration Rash
Epithelium Granulation Slough Eschar
Pain? (1-10)_______________________ Last Change in Tx (date)______ Response to Treatment: Improved No change Deteriorated Healed Signature:_____________________
Date Stage Size in cm (lengthxwidth)
Depth in cm
Undermining Tunneling cm Drainage
Notes: ____________________________ Stage 1
Stage 2 Stage 3 Stage 4 Unstageable Deep Tissue
Injury
None Tunneling Undermining
None Serous Serosanguineous Sanguineous Purulent Foul Purulent
___________________________________ ___________________________________ ___________________________________
Wound Edges Surrounding skin Wound bed Plan of care updated Yes No
Rolled edges Red Hard or induration Macerated Intact
Intact Pink/red White/gray pallor Dk red/Purple Black Swollen Maceration Rash
Epithelium Granulation Slough Eschar
Pain? (1-10)_______________________ Last Change in Tx (date)______ Response to Treatment: Improved No change Deteriorated Healed Signature:_____________________
Date Stage Size in cm (lengthxwidth)
Depth in cm
Undermining Tunneling cm Drainage
Notes: ____________________________ Stage 1
Stage 2 Stage 3 Stage 4 Unstageable Deep Tissue
Injury
None Tunneling Undermining
None Serous Serosanguineous Sanguineous Purulent Foul Purulent
___________________________________ ___________________________________ ___________________________________
Wound Edges Surrounding skin Wound bed Plan of care updated Yes No
Rolled edges Red Hard or induration Macerated Intact
Intact Pink/red White/gray pallor Dk red/Purple Black Swollen Maceration Rash
Epithelium Granulation Slough Eschar
Pain? (1-10)_______________________ Last Change in Tx (date)______ Response to Treatment: Improved No change Deteriorated Healed Signature:_____________________
Resident Name:______________________________Rm#:_______ MR#______________________ Developed by Polaris Group (813) 886-6500 Page 2 of 2
FH32 - Developed by Polaris Group www.polaris-group.com Page 48 of 51
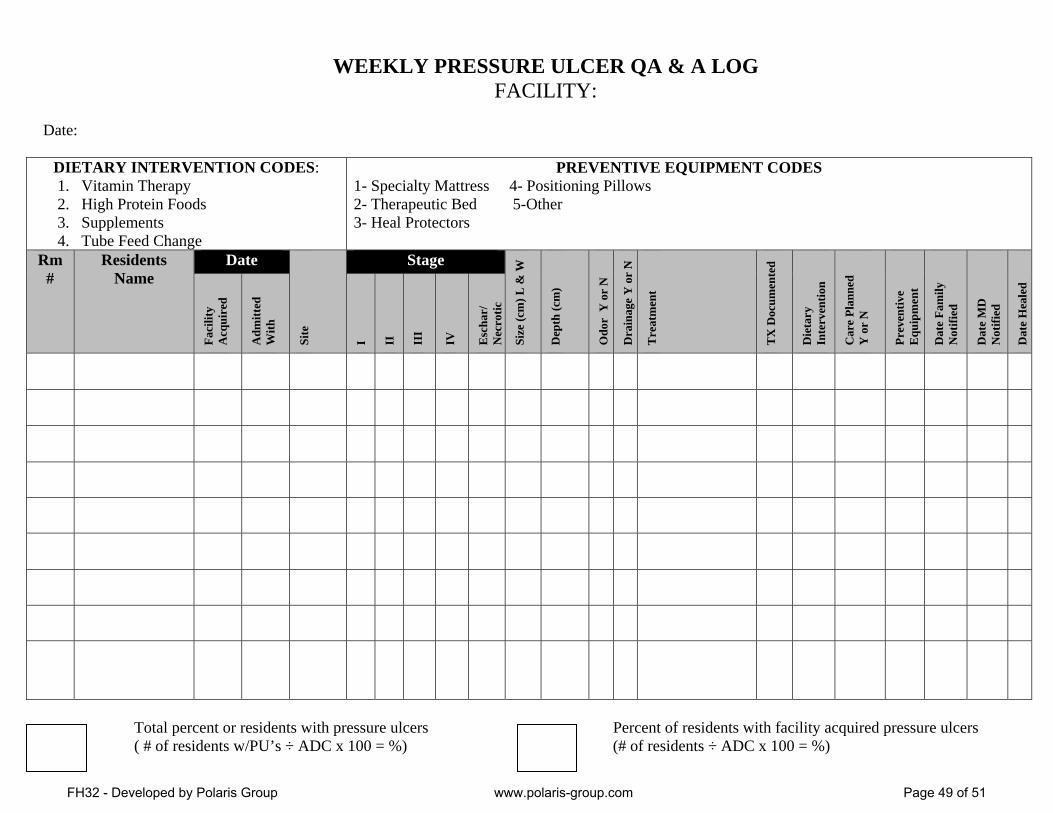
WEEKLY PRESSURE ULCER QA & A LOG
FACILITY: Date:
DIETARY INTERVENTION CODES: 1. Vitamin Therapy 2. High Protein Foods 3. Supplements 4. Tube Feed Change
PREVENTIVE EQUIPMENT CODES 1- Specialty Mattress 4- Positioning Pillows 2- Therapeutic Bed 5-Other 3- Heal Protectors
Rm #
Residents Name
Date
Site
Stage
Size
(cm
) L &
W
Dep
th (c
m)
Odo
r Y
or
N
Dra
inag
e Y
or
N
Tre
atm
ent
TX
Doc
umen
ted
Die
tary
In
terv
entio
n
Car
e Pl
anne
d
Y o
r N
Prev
entiv
e E
quip
men
t
Dat
e Fa
mily
N
otifi
ed
Dat
e M
D
Not
ified
Dat
e H
eale
d
Faci
lity
Acq
uire
d
Adm
itted
W
ith
I II
III
IV
Esc
har/
N
ecro
tic
Total percent or residents with pressure ulcers Percent of residents with facility acquired pressure ulcers ( # of residents w/PU’s ÷ ADC x 100 = %) (# of residents ÷ ADC x 100 = %)
FH32 - Developed by Polaris Group www.polaris-group.com Page 49 of 51
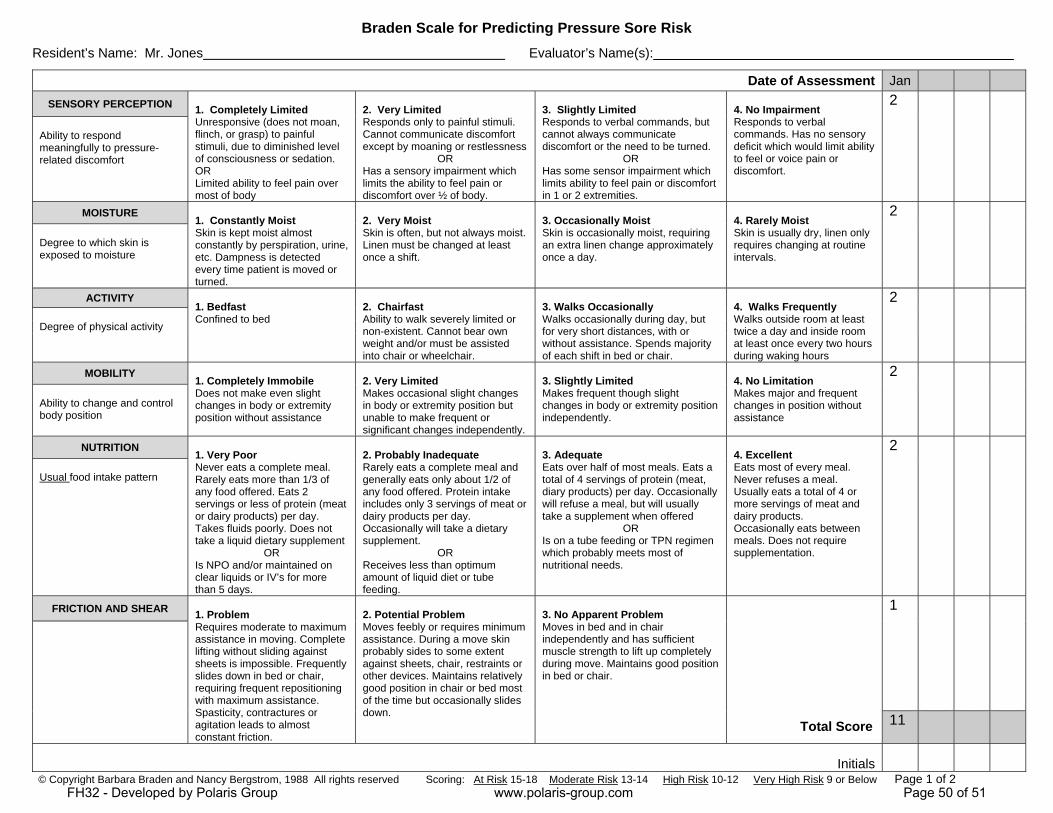
Braden Scale for Predicting Pressure Sore Risk
Resident’s Name: Mr. Jones Evaluator’s Name(s):
Date of Assessment Jan
SENSORY PERCEPTION 1. Completely Limited Unresponsive (does not moan, flinch, or grasp) to painful stimuli, due to diminished level of consciousness or sedation. OR Limited ability to feel pain over most of body
2. Very Limited Responds only to painful stimuli. Cannot communicate discomfort except by moaning or restlessness
OR Has a sensory impairment which limits the ability to feel pain or discomfort over ½ of body.
3. Slightly Limited Responds to verbal commands, but cannot always communicate discomfort or the need to be turned.
OR Has some sensor impairment which limits ability to feel pain or discomfort in 1 or 2 extremities.
4. No Impairment Responds to verbal commands. Has no sensory deficit which would limit ability to feel or voice pain or discomfort.
2
Ability to respond meaningfully to pressure-related discomfort
MOISTURE 1. Constantly Moist Skin is kept moist almost constantly by perspiration, urine, etc. Dampness is detected every time patient is moved or turned.
2. Very Moist Skin is often, but not always moist. Linen must be changed at least once a shift.
3. Occasionally Moist Skin is occasionally moist, requiring an extra linen change approximately once a day.
4. Rarely Moist Skin is usually dry, linen only requires changing at routine intervals.
2
Degree to which skin is exposed to moisture
ACTIVITY 1. Bedfast Confined to bed
2. Chairfast Ability to walk severely limited or non-existent. Cannot bear own weight and/or must be assisted into chair or wheelchair.
3. Walks Occasionally Walks occasionally during day, but for very short distances, with or without assistance. Spends majority of each shift in bed or chair.
4. Walks Frequently Walks outside room at least twice a day and inside room at least once every two hours during waking hours
2
Degree of physical activity
MOBILITY 1. Completely Immobile Does not make even slight changes in body or extremity position without assistance
2. Very Limited Makes occasional slight changes in body or extremity position but unable to make frequent or significant changes independently.
3. Slightly Limited Makes frequent though slight changes in body or extremity position independently.
4. No Limitation Makes major and frequent changes in position without assistance
2
Ability to change and control body position
NUTRITION 1. Very Poor Never eats a complete meal. Rarely eats more than 1/3 of any food offered. Eats 2 servings or less of protein (meat or dairy products) per day. Takes fluids poorly. Does not take a liquid dietary supplement
OR Is NPO and/or maintained on clear liquids or IV’s for more than 5 days.
2. Probably Inadequate Rarely eats a complete meal and generally eats only about 1/2 of any food offered. Protein intake includes only 3 servings of meat or dairy products per day. Occasionally will take a dietary supplement.
OR Receives less than optimum amount of liquid diet or tube feeding.
3. Adequate Eats over half of most meals. Eats a total of 4 servings of protein (meat, diary products) per day. Occasionally will refuse a meal, but will usually take a supplement when offered
OR Is on a tube feeding or TPN regimen which probably meets most of nutritional needs.
4. Excellent Eats most of every meal. Never refuses a meal. Usually eats a total of 4 or more servings of meat and dairy products. Occasionally eats between meals. Does not require supplementation.
2
Usual food intake pattern
FRICTION AND SHEAR 1. Problem Requires moderate to maximum assistance in moving. Complete lifting without sliding against sheets is impossible. Frequently slides down in bed or chair, requiring frequent repositioning with maximum assistance. Spasticity, contractures or agitation leads to almost constant friction.
2. Potential Problem Moves feebly or requires minimum assistance. During a move skin probably sides to some extent against sheets, chair, restraints or other devices. Maintains relatively good position in chair or bed most of the time but occasionally slides down.
3. No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move. Maintains good position in bed or chair.
Total Score
1
11
Initials
© Copyright Barbara Braden and Nancy Bergstrom, 1988 All rights reserved Scoring: At Risk 15-18 Moderate Risk 13-14 High Risk 10-12 Very High Risk 9 or Below Page 1 of 2 FH32 - Developed by Polaris Group www.polaris-group.com Page 50 of 51
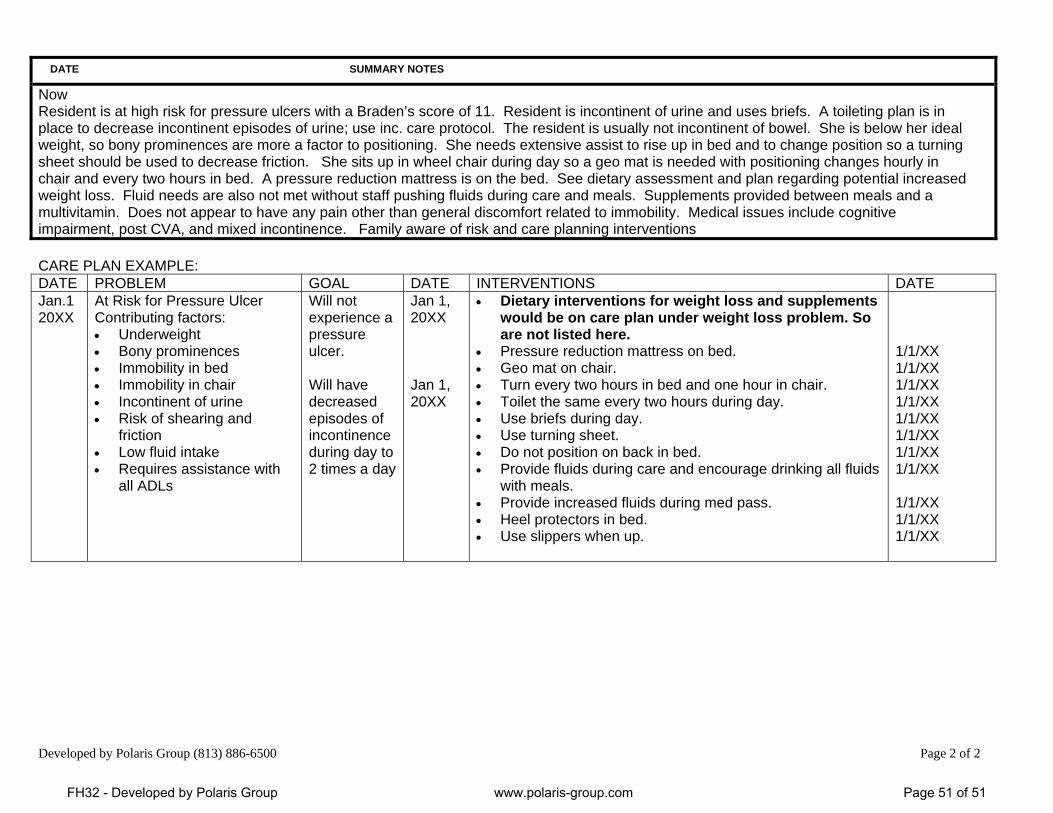
DATE SUMMARY NOTES
Now Resident is at high risk for pressure ulcers with a Braden’s score of 11. Resident is incontinent of urine and uses briefs. A toileting plan is in place to decrease incontinent episodes of urine; use inc. care protocol. The resident is usually not incontinent of bowel. She is below her ideal weight, so bony prominences are more a factor to positioning. She needs extensive assist to rise up in bed and to change position so a turning sheet should be used to decrease friction. She sits up in wheel chair during day so a geo mat is needed with positioning changes hourly in chair and every two hours in bed. A pressure reduction mattress is on the bed. See dietary assessment and plan regarding potential increased weight loss. Fluid needs are also not met without staff pushing fluids during care and meals. Supplements provided between meals and a multivitamin. Does not appear to have any pain other than general discomfort related to immobility. Medical issues include cognitive impairment, post CVA, and mixed incontinence. Family aware of risk and care planning interventions CARE PLAN EXAMPLE: DATE PROBLEM GOAL DATE INTERVENTIONS DATE Jan.1 20XX
At Risk for Pressure Ulcer Contributing factors: • Underweight • Bony prominences • Immobility in bed • Immobility in chair • Incontinent of urine • Risk of shearing and
friction • Low fluid intake • Requires assistance with
all ADLs
Will not experience a pressure ulcer. Will have decreased episodes of incontinence during day to 2 times a day
Jan 1, 20XX Jan 1, 20XX
• Dietary interventions for weight loss and supplements would be on care plan under weight loss problem. So are not listed here.
• Pressure reduction mattress on bed. • Geo mat on chair. • Turn every two hours in bed and one hour in chair. • Toilet the same every two hours during day. • Use briefs during day. • Use turning sheet. • Do not position on back in bed. • Provide fluids during care and encourage drinking all fluids
with meals. • Provide increased fluids during med pass. • Heel protectors in bed. • Use slippers when up.
1/1/XX 1/1/XX 1/1/XX 1/1/XX 1/1/XX 1/1/XX 1/1/XX 1/1/XX 1/1/XX 1/1/XX 1/1/XX
Developed by Polaris Group (813) 886-6500 Page 2 of 2
FH32 - Developed by Polaris Group www.polaris-group.com Page 51 of 51





























