Embed Size (px)
Citation preview

Pressure ulcer prevention and treatment: The relationship between lean body mass, nutrition, and healing
Nutrition is a key part of comprehensive care and pressure ulcer prevention and treatment

Patients who are malnourished or who have low LBM are at increased risk for complications, including pressure ulcers1,3,7
Lean body mass (LBM) loss and malnutrition start prior to admission and accelerate through the continuum of care2–4
Complications increase with greater LBM loss and poor nutrition1*
Adequate lean body mass and proper nutrition play a critical role in patient health and recovery1
* In the absence of preexisting LBM loss.
27%of patients experienced a nutritional decline4
30%–50%of patients were malnourished upon admission2
admission
37%of patients experienced LBM loss in just 1–2 days3
during stay
ONS may help prevent pressure ulcers and improve pressure ulcer healing5,6
Poor nutrition is often a contributing cause of pressure ulcers5–6
Most of your patients don’t get the nutrition they need to maintain and rebuild LBM
Ensuring proper nutrition helps reduce the risk of pressure ulcers and also plays a role in pressure ulcer treatment5–6
• A 15-study meta-analysis demonstrated that oral nutritional supplements (ONS) were associated with a lower incidence of pressure ulcers in at-risk patients6
Fill the nutritional gap with ONS
or
Daily nutrition consumed
Percent of pressure ulcers where nutrition plays a role5
Poor nutrition a contributing
cause
What is LBM?LBM includes muscle, skin,
bone, and organs
Malnourished patients are at 200%–500% higher risk
for pressure ulcers7
Protein ConsumedResearch has shown that elderly
hospitalized patients who were served a meal containing 40 grams of protein consumed only 10 grams of protein,
half of which was from dessert8
Not a contributing
cause
% Loss of Total LBM Complications
10% Impaired immunity, increased infection, mortality increased by 10%
20%Decreased healing, weakness, increased infection,
thinning of the skin, mortality increased by 30%
30%Too weak to sit, new pressure ulcers develop, pneumonia,
wound healing ceases, mortality increased by 50%
40% Death, usually from pneumonia

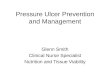
Ascension Health developed a bundle of interventions, which included nutrition, called SKIN to reduce the incidence of pressure ulcers in all at-risk patients9
Nutrition has been demonstrated to reduce facility-acquired pressure ulcers as part of a comprehensive program9
Evidence-based guidelines support nutrition intervention as part of pressure ulcer prevention and treatment
ESPEN recommends the use of ONS to reduce pressure ulcers and improve healing12‡
A nutrition protocol, including ONS, is an effective component of a comprehensive program9 Key associations promote proactive use of ONS10–12
Surface: Be sure patient is on the correct type of mattress
Incontinence: Offer toilet assistance every 2 hours
Keep turning: Reposition patient at least every 2 hours when in bed
Nutrition: Monitor patient nutrition, carry out nutrition orders, and record supplement and meal intake
According to chart reviews at Ascension Health, a nutrition consult was ordered for patients with pressure ulcers in 87% of cases; however, nutrition recommendations were followed only 35% of the time9
*Cited with permission from the NPUAP†Cited with Permission from the WOCN Society‡ESPEN=European Society for Clinical Nutrition and Metabolism
There were no new facility-acquired stage III/IV pressure ulcers during the last 18 months of the study
According to the National Pressure Ulcer Advisory Panel10*
“Offer high-protein mixed oral nutritional supplements (ONS) and/or tube feeding, in addition to the usual diet, to patients with nutritional risk and pressure ulcer risk because of acute or chronic diseases, or following a surgical intervention.” (Strength of Evidence = A).
WOCN Guidelines for Prevention and Management of Pressure Ulcers11†
“Elderly patients recovering from acute illness develop fewer pressure ulcers when given two daily nutritional supplement drinks.”
“Enteral nutrition support with high protein can significantly reduce the risk of development of pressure ulcers.”
Recommendation Grade
Pressure ulcer prevention
“Oral nutritional supplements, particularly with high protein content, can reduce the risk of developing pressure ulcers.”
A
Pressure ulcer treatment
“Based on positive clinical experience, enteral nutrition is also recommended in order to improve healing of pressure ulcers.”
C
1.94
2.27
2.58
1.40
2.14
2.35
LCL 0.38
UCL 2.8
2.20
1.81
2.99
1.88
2.41
2.09
1.85
2.10
2.87
1.98
0.73
0.50
1.28
1.41
2.00
1.18
1.40
1.23
0.81
0.00
1.00
2.00
3.00
4.00
Jan
04
Feb
04
Mar
04
Ap
r 04
May
04
Jun
04
Jul 0
4
Aug
04
Sep
04
Oct
04
Nov
04
Dec
04
Jan
05
Feb
05
Mar
05
Ap
r 05
May
05
Jun
05
Jul 0
5
Aug
05
Sep
05
Oct
05
Nov
05
Dec
05
Jan
06
Feb
06
Facility-acquired pressure ulcer ratio by month
After utilizing the SKIN bundle for 14 months, the incidence of pressure ulcers was reduced from >2% to <1%9

As part of a comprehensive program,
The cost of ONS for prevention of pressure ulcers is negligible compared to the cost of pressure ulcer treatment9,13–16
Provide ONS to patients at risk for or with pressure ulcers
Therapeutic nutrition is a highly cost-effective intervention to help reduce and treat pressure ulcers9,13
References: 1. Demling RH. Eplasty. 2009;9:65-94. 2. Schiesser M, Kirchhoff P, Müller MK, et al. Surgery. 2009;145(5):519-526. 3. Pichard C, Kyle UG, Morabia A, et al. Am J Clin Nutr. 2004;79(4):613-618. 4. Incalzi RA, Gemma A, Capparella O, et al. Arch Intern Med.1996;156(4):425-429. 5. Voss AC, Bender SA, Ferguson ML, et al. J Am Geriatr Soc. 2005;53(9):1587-1592. 6. Stratton RJ, Ek A-C, Engfer M, et al. Ageing Res Rev. 2005;4(3):422-450. 7. Banks M, Bauer J, Graves N, et al. Nutrition. 2010;26(9):896-901. 8. Paddon-Jones D. In: Gussler J (ed): Role of Nutrition in the Accretion, Retention, and Recovery of Lean Body Mass, Report of the 110th Abbott Nutrition Research Conference; Selected Summaries. Columbus, Ohio: Abbott Nutrition, 2009; 12-18. 9. Gibbons W, Shanks HT, Kleinhelter P, et al. Jt Comm J Qual Patient Saf. 2006;32(9):488-496. 10. Dorner B, Posthauer ME, Thomas D; National Pressure Ulcer Advisory Panel. Adv Skin Wound Care. 2009;22(5):212-221. 11. Ratliff C, Tomaselli N. WOCN Guidelines for Prevention and Treatment of Pressure Ulcers, 2010. 12. Volkert D, Berner YN, Berry E, et al. Clin Nutr. 2006;25(2):330-360. 13. Bergstrom N, Braden B. J Am Geriatr Soc. 1992;40(8):747-758. 14. Department of Health and Human Services. Book 2. Federal Register. 2008;73:48433-49084. 15. Reddy M, Gill SS, Rochon PA. JAMA. 2006;296(8):974-984. 16. Frantz RA, Berquist S, Specht J. Adv Wound Care. 1995;8(1):36-45. 17. Russo CA, Steiner C, Spector W. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb64.pdf. Published December 2008. Accessed September 10, 2009. 18. Kerstein MD, Gemmen E, van Rijswijk L. Dis Manag Health Outcomes. 2001;9(11):651-663. 19. Holmes R, Macchiano K, Jhangiani SS, et al. Am J Nurs. 1987;87(10):1301-1303. 20. Braunschweig C, Gomez S, Sheehan PM. J Am Diet Assoc. 2000;100:1316-1322. 21. Berlowitz DR, Wilking SVB. J Am Geriatr Soc. 1989;37:1043-1050. 22. McWhirter JP, Pennington CR. BMJ. 1994;308:945-948. 23. Schoonhoven L, Grobbee DE, Donders AR, et al. Qual Saf Health Care. 2006;15(1):65-70. 24. Weekes E. Proc Nutr Soc. 1999;58:126A. 25. Frankel H, Sperry J, Kaplan L. Am Surg. 2007;73(12):1215-1217. 26. Versluyen V, et al. BMJ.1986;292:1311-1313. 27. Gibbons W, Shanks HT, Kleinhelter P, et al. Jt Comm J Qual Patient Saf. 2006;32(9):8731-8735. 28. Bourdel-Marchessen I, Barateau M, Rondeau V, et al. Nutrition. 2000;16(1):1-5. 29. Resnick HE, Heineman J, Stone R, et al. Diabetes Care. 2008;31(2):287-288. 30. Fromy B, Abraham P, Bouvet C, et al. Diabetes. 2002;51(4):1214-1217. 31. May PE, Barber A, D’Olimpio JT, et al. Am J Surg. 2002;183(4):471-479. 32. Clark RH, Feleke G, Din M, et al. JPEN J Parenter Enteral Nutr. 2000;24(3):133-139. 33. Williams JZ, Abumrad N, Barbul A. Ann Surg. 2002;236(3):369-375.
Start Here
No
No additional nutrition intervention
Add Juven®*2 times per day31–33
Reassess every 24 hours
Known CKD?
Yes No
Yes
No
Yes
No
Yes
Known diabetes or hyperglycemia?29,30
Suggested intervention27
1. ONS 2 times per day6,12,28 (Patient receives 2 bottles of Ensure® Muscle Health* or Ensure® Clinical Strength* [8 fl oz] per day)
2. Nutrition consult
Suggested intervention27
1. CKD-specific meal plan
2. ONS 2 times per day6,12,28 (Patient receives 2 bottles of Nepro® with Carb Steady® [8 fl oz] per day)
3. Nutrition consult
Suggested intervention27
1. Diabetes-specific meal plan
2. ONS 2 times per day6,12,28
(Patient receives 2 Glucerna® Shakes [8 fl oz] per day)
3. Nutrition consult
Patient at nutritional risk? Risk factors present?22
• Poor nutrition labs19,20 • Age >50 years22–24 • Surgery25,26
• Poor dietary intake21 AND/OR • Over/underweight20,23 • Friction/shear
• Facility-specific scale • Poor skin condition23 • Confined to bed
Decision tree for oral nutritional supplements (ONS)
Pressure ulcer identified?
* Ensure Clinical Strength twice daily has 3 g Revigor™ (Ca HMB). Juven twice daily has 3 g of Revigor. Revigor is self-affirmed GRAS up to 6 g per day.
• The estimated annual per-patient cost for pressure ulcers ranges from $11,000 to $70,000, with 73% of costs associated with nursing care13–16
• Pressure ulcers extend the average hospital stay by 5–13 days, resulting in an increase in per-patient cost17,18
* “Twice-daily nutritional supplementation can be provided at $1 per day–$13 per person for an average 13-day stay. $11,000 all-in cost to care for a pressure ulcer/$13 per person for nutritional supplementation = 846 people fed.”
=The additional cost of
treating 1 pressure ulcerNutritional support for 846 patients
The cost of treating just 1 pressure ulcer can provide 13 days of nutritional supplementation for 846 patients12*

Hospital Stay
As part of a comprehensive program,
Intervene with oral nutritional supplements to support pressure ulcer prevention and improve pressure ulcer healing
©2011 Abbott Laboratories Inc. 77761/February 2011www.abbottnutrition.com
Percent of pressure ulcers where nutrition plays a role5
Pre-Admission
Aligned with evidence-based guidelines, ONS helps reduce the risk of pressure ulcers and also plays a role in pressure
ulcer treatment6
Provide ONS to patients at risk for or with pressure ulcers
Lean Body Mass (LBM) loss and malnutrition start prior to admission and accelerate through the continuum of care2–4
Loss of LBM can result in serious complications, including impaired wound healing and development of pressure ulcers1
Poor nutrition a contributing
cause
Not a contributing
cause