Embed Size (px)
Citation preview

i
Prevalence and Risk Factors for Diabetes Chronic Complications in Harare,
Zimbabwe, 2014
By
SARAVOYE TAPERA
R983698N
Submitted in partial fulfillment of the requirements of the Masters Degree in
Medicine (Public Health) in the Health Sciences Faculty, University of Zimbabwe,
Harare
University of Zimbabwe
Department of Community Medicine
College of Health Sciences
August 2014
Supervisor: Professor S Rusakaniko

ii
DECLARATION
I certify that this dissertation is my original work and submitted for the Master in Public Health program. It
has not been submitted in part or in full to any university and or any publication.
Student:
Signature Date
Dr. Tapera Saravoye
I having supervised and read this dissertation i am satisfied that this is the original work of the author in
whose name it is being presented. I confirm that the work has been completely satisfactory for presentation
in the examination.
Academic Supervisor:
Signature Date
Professor S. Rusakaniko
Chairman:
Signature Date
Professor S. Rusakaniko

iii
Abstract
Background: Diabetes is a chronic condition which often causes severe long term complications which
compromise quality of life and burdens health care systems and can cause permanent disability and even
death. The incidence of diabetes and the associated complications in Harare as reported through surveillance
data has been on the increase. In order to reduce disease burden due to diabetes chronic complications,
prevalence and risk factors for diabetes chronic complications must be determined through studies.
Methods: A total of 284 diabetics attending diabetic clinics at Parirenyatwa and Harare Central Hospitals
were enrolled in this cross sectional analytic study. Interviewer administered questionnaires were used to
collect data. The occurrence of diabetes chronic complications and their associated risk factors were
analyzed. Written informed consent was sought and obtained from all the respondents.
Results: Overall, prevalence of diabetes chronic complications was high with 45% of respondents having at
least one diabetes chronic complication. Significant risk factors associated with diabetes chronic
complications were: age>50 years (OR=4.34, p<0.001); duration with diabetes>10 years (OR=2.36,
p<0.001); type 2 diabetes (OR=1.96, p=0.006); poor control of blood sugar (OR=2.30, p<0.001); poor
compliance to medication (OR=1.72, p=0.024); being obese or overweight (OR=1.90, p=0.008); low
physical activity (OR=2.27, p=0.001); high LDL-Cholesterol (OR=2.34, p=0.001) and hypertension
(OR=1.88 p=0.009). After logistic regression, independent risk factors were as follows: low physical activity
(adjusted OR=1.90, p =0.029); duration >10 years with diabetes (adjusted OR=5.34, p<0.001); high LDL-
Cholesterol (adjusted OR=1.84, p=0.039) and type 2 diabetes (adjusted OR=6.48, p<0.001).
Conclusion: Overall prevalence of diabetes chronic complications was high but comparable to other studies.
Several demographic, patho-physiologic and life-style related risk factors associated with diabetes chronic
complications were identified. There is need to comprehensively address all risk factors in order to reduce
diabetes chronic complications.
Acknowledgements

iv
I wish to extend my most profound gratitude to my supervisor Professor S. Rusakaniko for his supervision
throughout the study. I would also like to thank Dr Mangwiro and Dr Mafundikwa for allowing me to conduct
this study at their diabetic clinics and for their encouragement.
I would like to appreciate all the assistance that i got from staff at both diabetic clinics during data collection.
I would also want to thank all the respondents who volunteered to participate in the study. Without their
participation, this study would not have been successful.
Last but certainly not least, i would like to thank my wife Emma for her unwavering support.
Table of contents

v
Abstract………………………………………………………………………….............................................................................................ii
Acknowledgement…………………………………………………………………....................................................................................iii
List of acronyms...………………………………………………………................................................................................................vi
List of tables and figures................................................................................................................................................v
Chapter 1
1.1. Introduction............................................................................................................................................................1
1.2. Problem statement.................................................................................................................................................3
Chapter 2
2.1. Literature review....................................................................................................................................................4
2.2. Objectives...............................................................................................................................................................7
Chapter 3
3.1 Study design............................................................................................................................................................8
3.2 Study setting............................................................................................................................................................9
3.3. Sample size calculation.........................................................................................................................................10
3.4. Sampling and Data collection................................................................................................................................11
3.5. Data analysis.........................................................................................................................................................12
3.6. Permission to conduct the study..........................................................................................................................12
3.7. Ethical considerations...........................................................................................................................................12
Chapter 4
4.1. Results...................................................................................................................................................................13
4.2. Discussion..............................................................................................................................................................21
4.3. Conclusion.............................................................................................................................................................26
4.4. Recommendations................................................................................................................................................26
4.5. Study limitations...................................................................................................................................................27
REFERENCES.................................................................................................................................................................28
APPENDIX 1: ENGLISH QUESTIONNAIRE......................................................................................................................33
APPENDIX 2: SHONA QUESTIONNAIRE.........................................................................................................................38
APPENDIX 3: TOOLS FOR ANTHROPOMETRIC MEASUREMENTS.................................................................................42
APPENDIX 4: TOOLS FOR ASSESSING PHYSICAL ACTIVITY............................................................................................44
APPENDIX 5: ENGLISH CONSENT FORM.......................................................................................................................46
APPENDIX 6: SHONA CONSENT FORM.........................................................................................................................49
APPENDIX 7: MRCZ APPROVAL LETTER........................................................................................................................52
List of acronyms

vi
1. DM: Diabetes Mellitus
2. HbA1c%: Glycated Hemoglobin percentage
3. LDL-C: Low Density Lipoprotein-Cholesterol
4. HDL-C: High Density Lipoprotein-Cholesterol
5. BMI: Body Mass Index
6. DFS: Diabetic Foot Syndrome
7. EGFR: Estimated Glomerular Filtration Rate
8. MDRD: Modification of Diet in Renal Disease
9. MET: Metabolic Equivalence
10. WHO: World Health Organization
11. ART: Antiretroviral Therapy
12. HIV: Human Immunodeficiency Virus
13. AIDS: Acquired Immune Deficiency Syndrome
List of figures and tables

vii
Figures
Figure 1: New diabetes cases and diabetes chronic complications in Harare, 2010-2013..............................3
Figure 2: Conceptual framework for describing risk factors for diabetes chronic complications in Harare...9
Tables
Table 1: Sensitivity testing for optimal sample size calculation....................................................................10
Table 2: Prevalence of diabetes chronic complications among respondents at Parirenyatwa hospital’s diabetic
clinic, 2014………………………………………………………...………………………………13
Table 3: Prevalence of diabetes chronic complications among respondents at Harare hospital’s diabetic
clinic, 2014.....................................................................................................................................................14
Table 4: Demographic factors associated with diabetes chronic complications in Harare, 2014..................16
Table 5: Risk factors associated with diabetes chronic complications in Harare, 2014................................18
Table 6: Independent factors associated with diabetes chronic complications in Harare, 2014....................19
Table 7: Calculation of metabolic equivalence using physical activity in Harare, 2014...............................44
Table 8: Classification of level of physical activity in Harare, 2014.............................................................45

1
Chapter 1
1.1. INTRODUCTION
Diabetes is a chronic disease which results from either failure of the pancreas to produce enough insulin or
when the body fails to effectively use the insulin it produces. Insulin hormone regulates blood sugar
metabolism1.
There are two main types of diabetes mellitus. Type 1 diabetes often results from the body's failure to produce
insulin due to a variety of reasons. Insulin therapy is required for this type of diabetes. Type 2 diabetes is a
result of insulin hormone resistance. Treatment for this type of diabetes is oral medicines to control blood
sugar, 2.
Hyperglycemia is a manifestation of uncontrolled diabetes and in time leads to damage to many of the body's
systems, particularly the nerves and blood vessels1. Diabetes long term complications often reduce the
quality of life of patients increasing burdens to health care systems and if untreated early can lead to
permanent disability and even death. Chronic complications of diabetes mellitus are categorized as micro
vascular and macro vascular or a combination of both3. Common diabetes complications include heart
disease, stroke, peripheral artery disease, neuropathies (damage to nerves), nephropathy (damage to
kidneys), retinopathy (damage to eyes), cataracts and erectile dysfunction (among men).
Global disease burden of diabetes mellitus
The World Health Organization estimated that in 2013, nearly 382 million people had diabetes globally, and
type 2 diabetes was responsible for up to 90% of the cases2. According to the same organization, in 2011
diabetes resulted in 1.4 million deaths globally, making it the 8th leading cause of death. The total number
of people with diabetes is predicted to increase to 592 million by 2035. Majority of diabetes deaths (80%)
occur in developing countries. The highest increase in incidence of diabetes will occur in developing
countries probably due to urbanization and lifestyle changes1, 2. Type 2 diabetes is now a global health
problem due to population growth, aging population, rapid urbanization and rising prevalence of physical

2
inactivity and obesity. However, the morbidity and mortality caused by diabetes mellitus can be reduced
through regular and thorough screening of complications and their effective early treatment4.
Management of diabetes at Harare and Parirenyatwa Hospitals
Harare and Parirenyatwa Central Hospitals each has a diabetic clinic. These clinics were established to offer
specialized treatment and care to diabetic patients in Zimbabwe. Treatment of diabetes is usually oral
medication and or insulin injections. In addition to treatment, patients are also prescribed a diabetic diet and
are encouraged to maintain a lean weight and to exercise regularly.
Patients are monitored in order to diagnose, prevent and treat diabetes chronic complications. They are
referred for ophthalmic examination by eye specialists at Sekuru Kaguvi Hospital (SKH) at Parirenyatwa at
least once a year. The purpose of this examination is to diagnose and treat diabetic related eye complications
such as retinopathy, cataracts, glaucoma and blindness. Early forms of retinopathy are treated at Sekuru
Kaguvi Eye Hospital using laser therapy. At the diabetic clinics, patients are also routinely screened for
peripheral neuropathy, diabetic foot syndrome, stroke, heart disease and other diabetes chronic complications
and are offered appropriate prevention and treatment services. Diabetic patients are also routinely monitored
for physiological parameters such as lipid profile tests, renal function tests and glycated hemoglobin test for
long term control of blood sugar.
Screening for diabetes mellitus in Harare
The commonest test for screening for diabetes mellitus is a random blood sugar test. Unfortunately some
diabetics in Harare present late with complications and with no history of having been screened for diabetes.
1.2. PROBLEM STATEMENT

3
The incidence of diabetes and the associated complications in Harare as reported through surveillance data
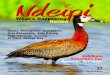
has been on the increase as shown in Figure 1.
Figure1: New cases and complications of diabetes mellitus reported in Harare, 2010-2013
As shown in figure 1, there was an increase in the number of new diabetic cases seen at Parirenyatwa and
Harare Central hospitals between 2010 and 2013. There was also an increase in number of diabetics
diagnosed with cataracts and diabetic foot. In addition to this increase, surveillance data from the National
Health Information at head office shows that the number of deaths due to diabetes at both Harare and
Parirenyatwa hospitals increased from 86 deaths in 2012 to 141 deaths in 2013. Overall prevalence of
diabetes chronic complications and the associated risk factors among diabetic patients in Harare is not
known. It is therefore necessary to determine prevalence and risk factors for chronic diabetic complications
as findings can inform diabetic patients and health care workers to better prevent and manage such risk
factors, improving the quality of life of diabetics and preventing severe disability and death.
Chapter 2
0
100
200
300
400
500
600
700
800
900
1000
2010 2011 2012 2013
Nu
mb
er
of
case
s
Year
New diabetic cases
Diabetic cases with cataracts
Diabetic cases with diabetic foot

4
2.1. LITERATURE REVIEW
Chronic complications of diabetes mellitus
Cardiovascular disease is responsible for the majority of cases of diabetic macro vascular complications.
Other macro vascular manifestations are cerebrovascular accidents (stroke) and peripheral vascular disease4.
The easiest screening test for peripheral vascular disease is palpation of peripheral pulses. Absence of
peripheral pulses on palpation is clinically significant for occlusive artery disease. More reliable and complex
methods such as angiography, continuous waveform Doppler scan and colour duplex ultrasound are
unavailable in most developing countries4, 5.
Erectile dysfunction, which occurs when a man can no longer get or keep an erection firm enough for sexual
intercourse is a result of both micro vascular and macro vascular complications. Psychological factors and
side effects of antihypertensive medicines may also be etiological factors for erectile dysfunction among
diabetics5, 6.
Diabetes is also associated with renal disease. Diabetic nephropathy is the kidney disease that occurs as a
result of diabetes induced damage to kidneys. It is the commonest cause of chronic renal failure globally and
in the sub-Saharan region and causes renal failure in one third of patients who require dialysis6.
Diabetic retinopathy results from diabetes induced damage to the retina and if untreated early can lead to
irreversible blindness5, 6, 7.
Another complication of diabetes mellitus is cataracts and cataracts are among the earliest complications of
diabetes mellitus and remain the leading cause of blindness globally and in the sub-Saharan region. Cataracts
occur at an earlier age and are up to 5 times more common in patients with diabetes8.
Prevalence of diabetes mellitus in Africa
While communicable diseases such as AIDS, malaria, and tuberculosis have continued to pose more
significant havoc in sub-Saharan Africa, it is now obvious that non-communicable diseases such as diabetes
mellitus are adding to the multiple disease burdens9. Sub-Saharan Africa is experiencing an increasing
prevalence of diabetes among other non-communicable diseases. The prevalence of diabetes in Africa3 has

5
been widely reported and varies between 1% and 20%. In Zimbabwe, the prevalence of diabetes was
estimated to be 10% among people aged 25 years or more12.
Prevalence of diabetes chronic complications
Diabetic chronic complications can cause disability and premature death. As the prevalence of diabetes
continues to increase, complications of diabetes are also likely to increase2, 3. There are huge variations in
prevalence of diabetes complications across the globe mainly due to the differences in methods used3.
Among Asian countries, the prevalence of diabetic retinopathy was 23.7% in India13 and 21.2% in Sri
Lanka14. In a study by Wijesuriya14 et al in Sri Lanka in 2011, prevalence of diabetes chronic complications
were: neuropathy (28%), heart disease (5.4%); stroke (0.8%); peripheral vascular disease (0.1%) and
nephropathy (33.3%).
Among European countries, Norway15 had a prevalence of retinopathy of 11% in persons with
known diabetes while in Poland16 it was 41.5%. Furthermore, in Poland, the prevalence of peripheral
neuropathy was 29%, nephropathy was 17% and diabetic foot syndrome was 8.3%.
A multinational observational study17 on diabetes long term complications, involving Asia, Africa, Europe
and South America showed that complication rates were 27% for macro vascular complications and 53.5%
for micro vascular complications17.
In some African countries the prevalence of retinopathy was as follows: 7% in Kenya18; 63% in South
Africa19; 32.5% in Malawi21 and 25% in Nigeria22. Prevalence of neuropathy was 27% in Cameroon23 and
10% in Tanzania24. Prevalence of nephropathy was 33% and 27% in two separate studies done at
Parirenyatwa diabetic clinic in Zimbabwe20, 34.
In a study by Raoeid25 et al in Benghazi in Lybia in 2010, prevalence of long term diabetic complications
among diabetics was as follows: cataracts (13%); diabetic peripheral artery disease (15%); diabetic
retinopathy (31%) and diabetes related heart disease (15%).
In sub-Saharan Africa, renal complications of diabetes are usually under diagnosed due to scarcity of
resources. In a study by Janmohamed24 et al in Tanzania, prevalence of diabetic renal disease among

6
diabetics was 83.7%. However, most of these patients were unaware of their condition and only 1.3% had a
prior diagnosis of diabetic nephropathy. In a cross sectional study by Ngassa49 et al in South Africa, the
prevalence of diabetes nephropathy was 33.6%.
Risk factors associated with diabetes chronic complications
Several studies have been carried out to identify factors associated with diabetes chronic complications in
both the developing and developed countries. In a study by Wijesuriya14 et al in Sri Lanka in 2011, significant
risk factors for diabetes chronic complications were: poor blood glucose control; hypertension; obesity and
high Low Density Lipoprotein-Cholesterol.
In a cross sectional hospital based survey by Li Z26 et al in China, significant risk factors for diabetes chronic
complications were: high Low Density Lipoprotein-Cholesterol; high HbA1c%; lack of exercise and longer
duration of diabetes mellitus.
In Europe, in a study in Italy by Nicolucci27 et al, risk factors for diabetes chronic complications were: male
sex; age >50 years; hypertension and having type 2 diabetes.
In a study in Poland by Kozek16et al, risk factors for diabetes chronic complications were: Diabetes duration,
age, high Low Density Lipoprotein-Cholesterol, cigarette smoking and alcohol consumption.
In a study in Germany by Muller N28 et al, there were significant associations between diabetic foot syndrome
and duration of diabetes as well as high blood pressure. However, smoking was not associated with diabetes
related chronic complications. In a study done by Klag29 et al in the United States of America, hypertension
was an independent risk factor for kidney failure among diabetic patients. Interventions for preventing
diabetes related renal disease must also target management of hypertension.
In across sectional study by Janmohamed24 et al in Tanzania, older age was associated with diabetes chronic
complications. In a cross sectional study by Ngassa49 et al in South Africa, risk factors for diabetes chronic
complications were: longer duration with diabetes, male sex, raised triglycerides and hypertension.
Studies have reported association between use of protease inhibitors (Anti Retro Viral drugs) and developing
type 2 diabetes30. However, the clinical presentation and range of complications of diabetes in HIV positive

7
individuals receiving ARV therapy are not different to those in individuals not on ARV therapy30. Glover25
et al in Malawi reported association between diabetes chronic complications with poor blood glucose control
(high Hb1c %), but found no association between ARV therapy and diabetes chronic complications.
We noted that previous studies in Zimbabwe were focusing on one or two chronic complications of diabetes.
We thus set out to determine the prevalence and risk factors for several diabetes chronic complications in
the Zimbabwean context, specifically in Harare.
Research questions
1. What is the prevalence of diabetes chronic complications in Harare?
2. What are the risk factors for diabetes chronic complications in Harare?
2.2. Objectives
Broad objective
To determine the prevalence and risk factors for diabetes chronic complications in Harare, 2014.
Specific objectives
1. To determine the prevalence of diabetes chronic complications in Harare, 2014.
2. To determine the demographic and socio-economic risk factors associated with diabetes chronic
complications in Harare, 2014.
3. To determine the life style risk factors associated with diabetes chronic complications in Harare,
2014.
4. To determine the patho-physiologic risk factors associated with diabetes chronic complications in
Harare, 2014.
5. To assess health system related factors associated with diabetes chronic complications at
Parirenyatwa and Harare Central hospitals’ diabetic clinics, 2014.
Chapter 3
METHODS

8
3.1. Study Design
An analytical cross sectional study was carried out. The occurrence and risk factors for diabetes chronic
complications among all the respondents were analyzed. A conceptual framework was used to identify
potential risk factors for diabetes chronic complications. The chronic complications analyzed were: diabetic
nephropathy; renal failure; diabetic foot syndrome (includes diabetic ulcers and critical limb ischemia);
amputation; stroke; heart failure; retinopathy; blindness and erectile dysfunction (among males).
The risk factors for diabetes chronic complications that were analyzed are shown in figure 2.
Figure 2: Conceptual framework: Risk factors for diabetes chronic complications in Harare, 2014.
(Conceptual framework adapted from Kozek E16 et al 2003)
Patho-physiological factors
Hypertension
High LDL-C
(>100mg/dl)
Poorly controlled
blood glucose
(HbA1c >7 %)
Type 2 diabetes
Duration with
diabetes
Demographic and socio-
economic factors
Age
Sex
Level of
education
Marital status
Employment
status

9
3.2. Study setting
The study was conducted at Parirenyatwa and Harare Central Hospitals’ diabetic clinics.
Study population
The study population was patients with confirmed diabetes mellitus attending the diabetic clinics at
Parirenyatwa and Harare Central Hospitals.
Inclusion criteria: We included patients aged 18 years and above with confirmed diabetes mellitus who
were attending the adult diabetic clinics at Harare and Parirenyatwa Central Hospitals.
Exclusion criteria
We excluded all those with confirmed diagnosis of diabetes but who were below 18 years of age. We also
excluded all who had not had any of the following performed: HbA1c %, serum creatinine, lipid profile and
recent ophthalmic examination by an eye specialist.
3.3. Sample size calculation
DIABETES
RELATED
CHRONIC
COMPLICATIONS
Health System related factors
Patient management
Screening for
complications
Self-care
Availability of
medicines
Life style- related factors
Smoking
Alcohol consumption
Low physical activity
Poor adherence to
treatment

10
Sensitivity testing for sample size calculation
In order to calculate optimal sample size, three different studies on prevalence of diabetic chronic
complications were used. The highest sample size (optimal sample size) was then chosen and the different
sample sizes calculated are shown in table 1.
Table 1: Sensitivity testing for optimal sample size calculation.
Prevalence Sample size Sample size, assuming 10%
non- response rate
Description of study
0.33 240 264 Mafundikwa20 et al. Prevalence of diabetic
nephropathy among diabetics at Parirenyatwa
0.27 213 235 Mafuratidze34 et al. Prevalence of diabetic
nephropathy among diabetics at Parirenyatwa
diabetic clinic, 2014.
0.22 186 205 Elbagir45 et al. Pattern of long term
complications in Sudanese diabetic patients,
1995.
Sample size calculation was based on Dobson’s formula [n=z2p (1-p)/d2]. The minimum sample size based
on test statistic z=1.645 and assuming a prevalence of diabetic nephropathy p=0.33 from a cross sectional
study by Mafundikwa20 et al, and an absolute precision (d) of 5%, assuming 10% non-response/refusal rate,
the minimum sample size calculated was 264.
3.4. Sampling and data collection tools
This cross sectional study was carried out at Parirenyatwa and Harare Central Hospitals’ diabetic clinics.
Study participants were recruited sequentially as they came to the clinics for routine care until the sample
size was reached. Participants were selected from both hospitals on a ratio of 1:1. A pre-tested, interviewer
administered questionnaire was used to collect data on demographics and risk factors for diabetes

11
complications from participants. Only chronic complications that developed after diagnosis of diabetes
mellitus were considered in the study. A review of patient cards and hospital records was done to objectively
assess patho-physiological risk factors for diabetes and to confirm specialist physician’s diagnosis of some
diabetes related chronic complications. Determination of retinopathy was based on the results of the last
examination by an eye specialist as was blindness.
Determination of nephropathy and renal failure was based on Estimated Glomerular Filtration Rate (EGFR),
using the most recent serum creatinine results. EGRF is calculated using the MDRD (Modification of Diet
in Renal Disease) study equation= [186 x (creatinine/88.4)-1.154 x (age-0.203) x (0.742 if female) x (1.21 if
black)]. EGFR is a better way of determining kidney function without necessarily doing a 24 hour urine
collection31. The MDRD equation is reported to be more accurate than the Cockroft-Gault equation31 for
calculating GRF. GFR is the best parameter of overall kidney function and should be measured or estimated
in all diabetic patients. An EGFR of > 60 ml/minute is considered normal kidney function; 15-59.99
ml/minute is diagnostic of nephropathy and < 15 ml/minute is diagnostic of kidney failure31.
Determination of level of physical activity was done using the STEP wise39 approach to Surveillance of
Chronic Diseases and Risk Factors Assessment tool. The level of physical activity was classified as high,
moderate and low. A set of standard questions were asked on respondents’ physical activities and those
activities were converted to Metabolic Equivalences (MET). The Metabolic Equivalence was then used to
classify level of physical activity.
Determination of Diabetic Foot Syndrome (DFS) was based on having non traumatic foot ulcer, gangrene,
absence of peripheral pulse or as diagnosed by a physician in the last 12 months. Latest results of glycated
haemoglobin and lipid profile test results were used to determine long term control of blood sugar and lipid
abnormalities respectively. The researcher also performed physical examination on all study participants to
determine obvious physical complications like stroke and amputation and to check for peripheral pulse
(posterior tibial artery). Weight was measured using a standard bath room scale and height was measured
using a rigid tape. Blood pressure was measured using a standard automated BP machine.

12
3.5. Data Analysis
Epi info version 3.5.1 was used to generate frequencies, proportions, means, odds ratios and their P values
and confidence intervals. Logistic regression analysis was done to come up with independent factors
associated with diabetes chronic complications, while simultaneously controlling for multiple confounding
variables.
3.6. Permission to conduct the study
Permission to conduct the study was sought and obtained from the Health Studies Office, Clinical Director
of Parirenyatwa Hospital, Harare Central Hospital’s Ethics Committee, Joint Research Ethics Committee
and the Medical Research Council of Zimbabwe.
3.7. Ethical considerations
The purpose of the study was clearly explained to each and every participant. Participants were assured that
there were no financial costs, injuries or risks which were expected during the study. Their participation was
voluntary and not coerced. Participants were free to discontinue with the study at any moment without any
negative consequences. Participants were also given information on who they could contact should they at
any time have any queries about their rights with regards to the study. No names or addresses of participants
were used during the study. All the information concerning the study was kept in privacy and confidentiality
was maintained. Written informed consent was obtained from the respondents who participated in the study.
Participants with obvious risk factors like poorly controlled blood glucose were counseled by the nursing
staff in the outpatients department.
Chapter 4
4.1. RESULTS
We interviewed 284 respondents from Harare and Parirenyatwa Hospitals’ diabetic clinics with half the
respondents from each clinic.
4.1.1. Prevalence of diabetes chronic complications among respondents from Parirenyatwa’s diabetic
clinic.

13
The occurrence of diabetes chronic complications among the respondents from Parirenyatwa hospital’s
diabetic clinic was assessed and the results are shown in the table 2.
Table 2: Prevalence of diabetes chronic complications among the respondents from Parirenyatwa
hospital’s diabetic clinic in Harare, 2014
Complication Prevalence, n=142 (%)
Nephropathy
Erectile dysfunction among male respondents (n=67)
42 (30.3)
20 (29.9)
Retinopathy
Diabetic foot syndrome
37 (26.1)
25 (17.6)
Cataracts 21 (14.8)
Heart failure 9 (6.3)
Stroke 3 (2.1)
Renal failure
Amputation
Blindness
3 (2.1)
2 (1.4)
0 (0%)
Among the 142 respondents from Parirenyatwa hospital’s diabetic clinic, 64 (45%) had at least one diabetes
chronic complication while 78 (55%) had no single diabetes related chronic complication. The prevalence
of specific diabetes chronic complications among all respondents from Parirenyatwa hospital’s diabetic
clinic (in descending order was as follows): nephropathy (30.3%); retinopathy (26.1%); diabetic foot
syndrome (17.6%); cataracts (14.8%); heart failure (6.3%); stroke (2.1%); renal failure (2.1%); amputation
(1.4%) and blindness (0%). Among the 67 male respondents, 20 (29.9%) reported erectile dysfunction.
4.1.2. Prevalence of diabetes chronic complications among respondents from Harare hospital’s
diabetic clinic.

14
The occurrence of diabetes chronic complications among the respondents from Harare hospital’s diabetic
clinic was assessed and the results are shown in the table 3.
Table 3: Prevalence of diabetes chronic complications among the respondents from Harare hospital’s
diabetic clinic, 2014
Complication Prevalence, n=142 (%)
Erectile dysfunction among male respondents (n=66)
Nephropathy
24 (36.4)
39 (27.5)
Retinopathy
Diabetic foot syndrome
29 (20.4)
24 (16.9)
Cataracts 22 (15.5)
Heart failure 8 (5.6)
Stroke 4 (2.8)
Renal failure
Blindness
Amputation
3 (2.1)
3 (2.1)
1 (0.7)
Among the 142 respondents from Harare hospital’s diabetic clinic, 65 (45.8%) had at least one diabetes
chronic complication while 77 (54.2%) had no single diabetes related chronic complication. The prevalence
of specific diabetes chronic complications among all respondents from Harare hospital’s diabetic clinic (in
descending order was as follows): nephropathy (27.5%); retinopathy (20.4%); diabetic foot syndrome
(16.9%); cataracts (15.5%); heart failure (5.6%); stroke (2.8%); renal failure (2.1%); blindness (2.1%) and
amputation (0.7%). Among the 66 male respondents, 20 (29.9%) reported erectile dysfunction.
4.1.3. Demographic factors associated with diabetes chronic complications in Harare (Parirenyatwa
and Harare Central Hospitals’ diabetic clinics)

15
Among the 284 respondents from the two diabetic clinics, 129 (45%) had at least one diabetes chronic
complication while 155 (55%) had no such complications. Demographic characteristics of respondents with
at least one diabetes chronic complication were compared with those without any diabetes chronic
complications and the results are shown in table 4.
Table 4: Demographic factors associated with diabetes chronic complications in Harare, 2014
Variable Category
Have diabetes
complication, n=129 (%)
Have no diabetes
complication, n=155 (%)
P value
Age group 18-28
29-39
40-49
50-60
>60
6 (4.7)
5 (3.9)
5 (3.9)
67 (51.9)
46 (35.7)
11 (7.1)
17 (11)
31 (20)
66 (42.6)
30 (19.4)
<0.001

16
Median age 57 (Q1=52; Q3=64) 52 (Q1=43; Q3=59) <0.001
Sex Male
Female
63 (48.8)
66 (51.2)
70 (45.2)
85 (54.8)
0.536
Marital
status
Single
Married
Divorced
Widowed
9 (7)
71 (55)
17 (13.2)
32 (24.8)
18 (11.6)
83 (53.5)
18 (11.6)
36 (23.2)
0.608
Level of
education
Primary
Secondary
Tertiary
68 (52.7)
42 (32.6)
19 (14.70
62 (40)
62 (40)
31 (20)
0.097
Employment
status
Employed
Self employed
Unemployed
Retired
37 (28.7)
18 (14)
36 (27.9)
38 (29.5)
38 (24.5)
32 (20.6)
40 (25.8)
45 (29)
0.499
The median age for those with diabetes related complications was 57 (Q1=52; Q3=64) and 52 (Q1=43; Q3=59)
for those without complications and the difference was statistically significant (p<0.001). Among the
demographic characteristics examined, age was significantly associated with diabetes chronic complications
(Odds ratio of 1.16 and p<0.001). The rest of the demographic factors were comparable among those that
developed diabetes complications and those that did not (p>0.05).
4.1.4. Risk factors for diabetes chronic complications in Harare (Parirenyatwa and Harare Central
Hospitals’ diabetic clinics)

17
We carried out bivariate analysis in order to determine risk factors associated with diabetes chronic
complications. The analysis was done on all potential risk factors on our conceptual framework. Odds
Ratios were the measure of association used and table 5 shows the results.
Table 5: Risk factors for diabetes mellitus related chronic complications in Harare, 2014
Variable Has diabetes
complication,
n=129 (%)
Has no diabetes
complication,
n=155 (%)
OR 95% CI P value
Age
>50
≤50
113 (87.6)
16 (12.4)
96 (61.9)
59 (38.1)
4.34
2.34-8.04
<0.001
Duration with
diabetes
>10 years
≤10 years
78 (60.5)
51 (39.5)
61 (39.4)
94 (60.6)
2.36
1.46-3.80
<0.001
Type of DM
Type 2
Type 1
82 (63.6)
47 (36.4)
73 (47.1)
82 (52.9)
1.96
1.22-3.16
0.006

18
Blood sugar
control
Poor (HbA1c% >7)
Good (HbA1c%
≤7)
72 (55.80)
57 (44.20)
55 (35.5)
100 (64.5)
2.30
1.42-3.71
<0.001
Compliance to
medication
Poor (missed ≥3
doses/week)
Good (missed <3
doses/week)
68 (52.7)
61 (47.1)
61 (39.4)
94 (60.6)
1.72
1.07-2.76
0.024
Body Mass Index
Overweight/Obese
Normal BMI
66 (51.2)
63 (48.80)
55 (35.5)
100 (64.5)
1.90
1.18-3.07
0.008
Physical activity
Low (less than 600
Met minutes per
week).
High/Moderate
68 (52.7)
61 (47.3)
51 (32.9)
104 (67.1)
2.27
1.40-3.68
0.001
LDL-Cholesterol
High LDL-C
Normal LDL-C
60 (46.5)
69 (53.5)
42 (27.1)
113 (72.9)
2.34
1.43-3.84
0.001
Hypertension
Yes
No
70 (54.3)
59 (45.7)
60 (38.7)
95 (61.3)
1.88
1.17-3.02
0.009
HIV
Positive
Negative
19 (14.7)
110 (85.3)
18 (11.6)
137 (88.4)
1.31
0.66-2.63
0.437
Alcohol
consumption
Yes
No
16 (12.4)
113 (87.6)
12 (7.7)
143 (92.3)
1.69
0.77-3.71
0.190
Smoking cigarettes
Yes
No
11 (8.5)
118 (91.5)
9 (5.8)
146 (94.2)
1.51
0.61-3.78
0.372
Respondents aged more than 50 years were 4.34 times more likely to develop diabetes complications when
compared to those aged ≤50 (p<0.001). Other significant risk factors for diabetes chronic complications
were: duration with diabetes of more than 10 years (OR=2.36, p<0.001); type 2 diabetes (OR=1.96,
p=0.006); poor control of blood sugar/high HbA1c% (OR=2.30, p<0.001); poor compliance to medication
(OR=1.72, p=0.024); being obese or overweight (OR=1.90, p=0.008);); high LDL-Cholesterol (OR=2.34,
p=0.001); hypertension (OR=1.88 p=0.009) and low physical activity (OR=2.27, p=0.001). Low physical
activity was classified as having less than 600 Met minutes per week of exercises. Consuming alcohol,
smoking cigarettes and being HIV positive were not associated with diabetes chronic complications.

19
4.1.5. Independent risk factors associated with diabetes chronic complications in Harare
(Parirenyatwa and Harare Central Hospitals’ diabetic clinics).
Multivariate analysis was done using logistic regression in order to identify independent risk factors for
diabetes chronic complications while simultaneously controlling for multiple confounders. All risk factors
with a p value of less than 0.25 (after bivariate analysis) were selected for analysis and table 6 shows the
results.
Table 6: Independent risk factors associated with diabetes chronic complications in Harare, 2014
Variable Adjusted OR 95% CI P value
Low physical activity (˂600 Met
minutes/week)
1.90 1.07-3.38 0.029
Duration > 10 years with
diabetes
5.34 2.30-12.40 <0.001
High LDL-Cholesterol 1.84 1.03-3.27 0.039
Type 2 diabetes mellitus 6.48 2.92-14.40 <0.001
Independent risk factors were as follows: low physical activity (adjusted OR=1.90, p =0.029); duration > 10
years with diabetes (adjusted OR=5.34, p<0.001); high LDL-Cholesterol (adjusted OR=1.84, p=0.039) and
type 2 diabetes (adjusted OR=6.48, p<0.001).
4.1.6. Patient management at diabetic clinics at Parirenyatwa and Harare hospitals
Clinicians at both clinics are managing to routinely screen patients for most complications. This is
commendable since selective testing (among symptomatic patients only) rather than screening will likely
miss most complications and physiological changes which in some instances are asymptomatic. For example,
all patients routinely undergo physiological tests for renal function, HbA1c% and lipid profile tests. In
addition all patients are encouraged to undergo annual ophthalmic examination by eye specialists. However

20
a review of respondents’ notes revealed that calculation of BMI (Body Mass Index) and the subsequent
counseling according to the BMI was not being routinely done. It also showed that patients were not being
routinely screened for foot lesions at the two clinics (patients were only examined if they had complains). It
was further observed that even though renal function tests were routinely done at both clinics, no calculation
of Estimated Glomerular Filtration Rate (EGFR) was done. This is worrying as GFR is the best parameter
of overall kidney function and should be determined for every diabetic patient in order to diagnose diabetic
nephropathy early and institute treatment before renal failure sets in. These issues show that even at tertiary
care setting, sometimes clinicians do not offer comprehensive care to diabetics.
It was noted that all oral diabetic medicines and insulin were readily available at Pharmacies in Harare,
including at the two hospitals under study. Most patients (89%) also had glucometers which they were using
to measure their glucose levels at home.
4.2. DISCUSSION
Overall, prevalence of diabetes complications was high with nearly half of diabetics (45%) having at least
one diabetes chronic complication. Given the prevalence of diabetes estimated to be 10% among people aged
25 years and above in Zimbabwe12, and that the population aged 25 years and above was 38.9% of the total
population in 2012 (according to census32 results), it can be estimated that 508 082 diabetics (out of 1 306
124 diabetics) have at least one chronic complication in Zimbabwe. While diseases such as AIDS, malaria
and TB continue to threaten Zimbabwe’s health care system, communicable diseases such as diabetes are
certainly adding to these multiple disease burdens in the country4.
Prevalence of nephropathy
A cross sectional study on prevalence of diabetic nephropathy at Parirenyatwa hospital by Mafundikwa20 et
al reported a prevalence of diabetic nephropathy of 33% which is comparable to the 27.5 and 30.3% from

21
our study. Another cross sectional study carried out at Parirenyatwa hospital’s diabetic clinic reported a
prevalence of diabetic nephropathy of 27.2% which again is comparable to the prevalence reported in our
study34. A cross sectional study on long term complications among diabetics in Sudan by Elbagir45 et al
reported a prevalence of nephropathy of 22%. In a cross sectional study on diabetes nephropathy in South
Africa49, the prevalence of diabetes nephropathy was 33.6% which again is consistent with our findings.
Prevalence of retinopathy, cataracts and blindness
In our study, the prevalence of retinopathy among respondents at the two clinics was 26.1 and 20.4%. Similar
prevalence was reported in India13, Sri Lanka14, Nigeria22 and Burkina Faso47. In Malawi21 however, the
prevalence of retinopathy was much higher at 32.5%. A study done at Parirenyatwa hospital by M C Bartels38
et al showed a prevalence of retinopathy of 36%. Visual impairment in diabetic retinopathy occurs due to
diabetes induced macular edema and diabetic retinopathy and can lead to irreversible blindness if not treated
early5, 6, 7.
Prevalence of cataracts among the two clinics in our study was 15.5 and 14.8%. This was similar to the
prevalence reported in Lybia25. Cataracts are among the earliest complications of diabetes mellitus. They
remain the leading cause of blindness, occurring at an earlier age and have been reported to be up to 5 times
more frequent in patients with diabetes. However, the pathogenesis of diabetic cataract development is not
fully understood8. It is however important to note that many diabetic patients with cataracts have undergone
surgical operations at Sekuru Kaguvi Hospital (SKH) at Parirenyatwa and have their sight restored.
The prevalence of blindness was 2.1% in this study. This was much higher than the 0.1% reported in China37.
However the study in China was limited to type 2 diabetes patients while our study included both type 1 and
type 2.
Prevalence of diabetic foot syndrome and amputation
The prevalence of diabetic foot syndrome among the two clinics in our study was 17.6 and 16.9%. Sensory
neuropathy is the primary cause of diabetic foot syndrome while lower limb arterial diseases are also
important etiological factors23. A cross sectional study in South Africa36 reported prevalence of diabetic foot

22
syndrome at 36.6%. However the study in South Africa included all foot problems since diagnosis of diabetes
was made while we limited the duration to the previous 12 months and this could have underestimated our
prevalence. Relatively very low prevalence was reported in China (0.7%) and this could be because in the
study in China, they only looked at diabetic foot ulcers which underestimated the prevalence37. The
prevalence of diabetic foot syndrome reported in our study could also be an underestimate of the true
prevalence of diabetic foot syndrome as studies have shown that Doppler diagnosis is much more sensitive
than the clinical methods that we used46. The prevalence of amputation among the two clinics in our study
was 1.4 and 0.7%. Similar prevalence was reported in South Africa36. Amputations have been shown to be
15 times more frequent in diabetic patients than in the general population43. Even when amputation has been
done, the remaining leg or foot and the patient’s life can be saved by regular monitoring. The diabetic
association of Zimbabwe is currently making efforts to establish diabetic foot clinics at Parirenyatwa and
Harare central hospitals in on order to improve foot care among diabetics with the ultimate aim of reducing
amputations.
Prevalence of heart failure
The prevalence of heart failure among the two clinics in our study was 6.3 and 5.6%. Assessment for
myocardial infarction was not done as electrocardiograms are not routinely done at the two clinics. Lack of
diagnostic facilities like coronary angiography limits the study of coronary artery diseases in Zimbabwe. In
a cross sectional study done in Lybia25, prevalence of heart conditions (including heart failure, angina and
myocardial infarction) was 13%. A study in Burkina Faso47 reported a prevalence of 8.7% and the study
included myocardial infarction, heart failure and angina unlike our study where we only looked at heart
failure. The development of heart failure among diabetics is a consequence of diabetes induced coronary
artery disease, cardiomyopathy and sometimes increased susceptibility to hypertension mediated heart
muscle damage44.
Prevalence of stroke

23
The prevalence of stroke among the two clinics in our study was 2.1 and 2.8%. This prevalence is consistent
with results of other studies in Sudan45. Prevalence of stroke among diabetics may appear low because of
the mortality associated with this complication.
Prevalence of erectile dysfunction among male diabetics
In our study, the occurrence of erectile dysfunction among the male respondents from the two clinics was
36.4 and 29.9%. The erectile dysfunction was self-reported and was diagnosed when a man could no longer
get or keep an erection firm enough for sexual intercourse. Erectile dysfunction tends to occur at an earlier
age in diabetics when compared to non diabetics48. Studies elsewhere showed prevalence of erectile
dysfunction among diabetics of 34%48 which is comparable to our study findings. Among male respondents
with erectile dysfunction, 67% did not seek treatment for their condition, despite the availability of treatment.
Diabetic micro vascular and macro vascular complications coupled with psychological and situational factors
contribute to erectile dysfunction. Erectile dysfunction can also be a side effect of medicines commonly
prescribed to men with diabetes, such as antihypertensive and antidepressants5, 6.
Risk factors associated with chronic diabetes complications
This study identified several risk factors for diabetes chronic complications which were also identified in
literature.
Age
Being older than 50 years was a significant risk factor for diabetes chronic complications. This is consistent
with results of other studies16, 17, 24, 26, 27, 40, 41, 42, 49. Old age is a non-modifiable risk factor.
Duration with diabetes
Duration with diabetes was significantly associated with diabetes chronic complications. This is consistent
with results of other studies 26, 27, 28, 34, 49.
Type of diabetes
Type 2 diabetes was an independent risk factor for diabetes complications and similar findings were reported
in other studies27. Type of diabetes is another non modifiable risk factor, however literature has shown that

24
the incidence of type 2 diabetes can be reduced through lifestyle changes, reducing obesity and increasing
level of physical activity4.
Glycated hemoglobin (HbA1c) percentage
Poorly controlled blood sugar was a significant risk factor for diabetes chronic complications. Similar
findings were reported in Africa, Asia and Europe14, 17, 26, 30, 31. The fact that nearly half of respondents (45%)
had high HbA1c % implies that there is poor control of blood sugar. Control of blood glucose requires a
combination of using correct dose of medication, being adherent to treatment and carefully controlling
calorie intake and physical activity.
Compliance to medication
Missing at least 3 doses of medication per week was a significant risk factor for diabetes chronic
complications. Poor compliance to medication can lead to poor control of blood sugar, increasing the risk of
diabetes chronic complications. Since diabetes is a lifelong condition, diabetics have to be on medication for
a very long duration and this can sometimes lead to treatment fatigue.
Body Mass Index (BMI)
Being overweight or obese was significantly associated with diabetes chronic complications. Similar
findings were reported in other studies in Africa and Asia14, 17.
Physical activity
Low physical activity (that is less than 600 Met minutes per week) was an independent risk factor for diabetes
chronic complications. Similar findings were reported in China26. In our study, 42% of respondents were
classified as low physical activity.
LDL-Cholesterol
High Low Density Lipoprotein-Cholesterol (LDL) was an independent risk factor for diabetes chronic
complications. Similar findings were reported in other studies16, 17, 26, 31, 49.
Hypertension

25
Being hypertensive was significantly associated with diabetes chronic complications. Similar findings were
reported in several other studies14, 17, 27, 28, 29, 31, 49. In our study, nearly half of respondents were hypertensive
(46%) and this shows the high burden of hypertension among diabetics.
Alcohol consumption, smoking and HIV status
Alcohol consumption was not associated with diabetes chronic complications. However, studies elsewhere
found an association with alcohol consumption16. In our study, only 28 respondents (9.9%) reported
consumption of alcohol and this could have underestimated any possible association. Smoking was not
associated with diabetes complications. Similar finding were made in Germany28.
There was also no association with HIV status. Similar findings were reported in Malawi25. Studies elsewhere
have demonstrated an association between HIV and development of type 2 diabetes mellitus, however the
clinical presentation and complications of diabetes in HIV infected patients were similar to those in patients
who are HIV negative30.
4.3. Conclusion
The overall prevalence of diabetes chronic complications was high. The prevalence of individual diabetes
chronic complications was high and comparable to regional and local prevalence from previous studies.
Complications with high prevalence were: nephropathy; retinopathy; diabetic foot syndrome and cataracts
and these are increasing disease burden in Harare. These complications are a result of several risk factors
that were identified in this study. Among demographic factors analyzed, age (>50 years) was significantly
associated with diabetes chronic complications. Significant patho-physiologic risk factors associated with
diabetes chronic complications were: poorly controlled blood sugar levels (high Hb1c %); high Low Density
Lipoprotein-Cholesterol; hypertension; having type 2 diabetes mellitus and duration with diabetes greater
than10 years. Life-style related factors which were significantly associated with diabetes chronic
complications were: low physical activity; being obese or overweight and poor compliance to medication.

26
After adjusting for confounding using multivariate analysis, independent risk factors for diabetes chronic
complications were: low physical activity; high Low Density Lipoprotein-Cholesterol; duration with
diabetes greater than 10 years and having type 2 diabetes mellitus. In order to reduce prevalence of diabetes
chronic complications, all the risk factors identified will need to be comprehensively addressed.
4.4. Recommendations
1. Physicians at Parirenyatwa and Harare hospitals’ diabetic clinics should intensify screening of
diabetics for chronic complications as early diagnosis and treatment can prevent severe disability and
death.
2. Diabetics and the general population in Harare should be encouraged to adopt healthier lifestyles,
particularly weight reduction among obese and overweight individuals through physical activities
and eating low calorie, high fibre diet since physical inactivity, obesity and high Low Density
Lipoprotein-Cholesterol were all risk factors for diabetes complications. The health promotion
officers at Harare and Parirenyatwa should spearhead this campaign.
3. More studies on risk factors for diabetes related chronic complications should carried out in
Zimbabwe by Public Health Officers particularly in rural settings as such literature is scarce in
Zimbabwe.
4.5. Study Limitations
We carried out an analytic cross sectional study and the retrospective nature of our study design makes it
impossible to draw any conclusion about causal relationship between risk factors identified and the
development of diabetes chronic complications. It is also important to state that respondents were
consecutively sampled as they reported for care at the diabetic clinics. This consecutive sampling could
affect the impacts of the study, particularly generalization.

27
REFERENCES
1. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis
and classification of diabetes mellitus. Geneva, World Health Organization, 1999
(WHO/NCD/NCS/99.2).
2. WHO fact sheet 2014. http://www.who.int/mediacentre/factsheets/fs312/. Last accessed on
19/05/2014.
3. http://www.afro.who.int/en/zimbabwe/zimbabwe-publications/1773-diabetes-mellitus.html. Last
accessed on 19/05/2014.
4. Leung GM, Lam K. HKMJ 2000; 6:61-69.
5. Beach KW, Bedford GR. Diabetes Care. 1998; 11:464-71.
6. Rema M, Pradeepa R. Indian Med J Res. 2007; 125:297-311.

28
7. Harney F. Medicine. 2006; 34(3):95-97.
8. Klein B E, Klein R, Moss SE. Incidence of cataract surgery in the Wisconsin Epidemiologic Study of
Diabetic Retinopathy. American Journal of Ophthalmology. 1995; 119:295-301.
9. Nambuya AP, Whitehead H, Mulvany D, Kennedy R, Hadden DR. The presentation of newly-
diagnosed diabetic patients in Uganda. Q J Med.1996; 89: 705-710.
10. Keil JE, Knapp RG, Lack-land DT, Gazes PG, Tyroler HA. Mortality rates and risk factors for
coronary disease in black as compared with white men and women. N Engl J Med. 1993; 329: 73-77.
11. Elamin A, Omer MI, Zein K, Tuvemo T. Epidemiology of childhood type I diabetes in Sudan, 1987–
1990. Diabetes Care. 1992; 15: 1556-1560.
12. Ministry of Health and Child Welfare, Zimbabwe National Health Strategy for Zimbabwe 2009-2013:
Equity and Quality in Health: A People’s Right. MOHCW, Zimbabwe, 2009
13. Ramachandran A, Snehalatha C, Viswanathan V. Current Science. 2002; 83 (12):1472-76.
14. M.A. Wijesuriya, W.K. De-Abrew, A. Weerathunga, A. Perera, L. Association of chronic
complications of type 2 diabetes with the biochemical and physical estimations in subjects attending
single visit screening for complications. Journal of Diabetology. 2012; 1:3
15. Sundling V, Jansson RW, E, Gulbrandsen P. Retinopathy and visual impairment in diabetes, impaired
glucose tolerance and normal glucose tolerance: the Nord-Trondelag Health Study (the HUNT study)
Acta Ophthalmol. 2012; 90(3):237-43
16. Kozek E, Fross K, Marcinowska A, Sieradzki J. Chronic complications and risk factors in patients
with diabetes mellitus-retrospective analysis. Przeglad Lekarsi. 2003; 60(12):773-8.
17. Litwak L, Hussein Z, Malek R, Prusty V, Khamseh ME. Prevalence of diabetes complications in
people with type 2 diabetes mellitus and its association with baseline characteristics in the
multinational study. Diabetology and Metabolic Syndrome. 2013; 5(1):57.
18. ATP III Panel. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in
Adults. National Cholesterol Education Program (NCEP). Adult Treatment Panel III (ATP III), 2001

29
19. Krauss RM, Siri PW. Dyslipidemia in type 2 diabetes. Med Clin North Am .2004; 88: 897-908.
20. Mafundikwa A, Ndhlovu CE, Gomo Z. The prevalence of diabetic nephropathy in adult patients with
insulin dependent diabetes mellitus attending Parirenyatwa Diabetic Clinic, Harare. The Central
African Journal of Medicine. 2007; 53(1-4):1-6.
21. Glover SJ, Cohen DB, Harding SP, Hofland HW, Zijlstra EE, Allain TJ. Prevalence of diabetic
retinopathy, cataract and visual impairment in patients with diabetes in sub-Saharan Africa. Br J
Ophthalmology. 2012; 96(2):156-62.
22. Mbanya JC, Sobngwi E. Diabetes micro vascular and macro vascular disease in Africa. J
Cardiovascular Risk. 2003; 10: 97-103.
23. Ndip E. A, Tchakonte B, Mbanya J.C. A study of the prevalence and risk factors of foot problems in
a population of diabetic patients in Cameroon. The International Journal of Lower Extremity Wounds.
2006; 5 (2); 83-8.
24. Janmohamed MN, Kalluvya SE, Mueller A, Kabangila R, Smart LR, Downs JA, Peck RN. Prevalence
of chronic kidney disease in diabetic adult out-patients in Tanzania. BMC Nephrology. 2013; 14:184.
25. R.B. Roaeid, O.A. Kadiki. Prevalence of long-term complications among Type 2 diabetic patients in
Benghazi, Libya. Journal of Diabetology. 2011; 3:5.
26. Li Z, Guo SQ, Liu WX, Zhang YL, Yang L, Ma WB, Liu DW, Tang LM. A case-control study on
risk factors of type 2 diabetes mellitus related chronic complications in Baoding city. Zhonghua Liu
Xing Bing Xue Za Zhi. 2009; 30(12):1291-6.
27. Nicolucci A, D, Scorpiglione N, Carinci F, Capani F, Tognoni G, Benedetti MM. A comprehensive
assessment of the avoidability of long-term complications of diabetes. A case-control study. Diabetes
Care. 1996; 19(9):927-33.
28. Muller N, Busch M, Eidner G, Kloos C, Hunger-Battefeld W, Muller UA. Diabetic foot syndrome
and renal function in type 1 and 2 diabetes mellitus show close association. Wolf, Nephrology Dialysis
Transplantation. 2009; 24(6):1896-901.

30
29. Klag MJ, Whelton PK, Randall BL, Neaton JD, Brancati FL, Ford CE, et al. N Engl J Med. 1996;
334:13-8
30. Dube MP. Disorders of glucose metabolism in patients infected with human immunodeficiency
virus. Clin Infect Dis. 2000; 31:1467-1476.
31. Gross JL, Silveiro SP, Canani LH, Caramori ML, Zelmanovitz T (January 2005). "Diabetic
nephropathy: diagnosis, prevention, and treatment". Diabetes Care. 28 (1): 164-75.
32. Zimbabwe Population Census Report 2012, page 18.
33. Zimbabwe Demographic Heath Survey, 2010-11.
34. Erisi Mafuratidze, Kurai Chako, Danai Tavonga Zhou. Over 27% of Type 2 Diabetic Patients Studied
at Parirenyatwa Diabetic Clinic in Zimbabwe has Evidence of Impaired Renal Function. International
Journal of Scientific and Technology Research. 2014; 3(3).
35. Kim SI, Kim SJ. Prevalence and risk factors for cataracts in persons with type 2 diabetes mellitus.
Korean Journal of Ophthalmology. 2006; 20 (4): 201-4.
36. Levitt NS, Bradshaw D, Zwarenstein MF, Bawa AA, Maphumolo S. Audit of public sector primary
diabetes care in Cape Town, South Africa: high prevalence of complications, uncontrolled
hyperglycemia, and hypertension. Diabetic Med 1997; 14:1073-1078.
37. Zhaolan Liu, Chaowei Fu, Weibing Wang, Bia Xu. Prevalence of chronic complications of type 2
diabetes mellitus on outpatients-a cross sectional hospital based survey in Urban China. Health and
Quality of Life Outcomes. 2010; 8:62.
38. M C Bartels, B M Macheka, S Guramatunhu, J J Scheenloop, J S Stilma. Background Diabetic
Retinopathy in Harare, Zimbabwe. Tropical Doctor. 1999; 29: 189.
39. www.who.int/chp/steps/manual. Last accessed on 24/06/14.
40. Morgan CL, Currie CJ, Stott NC, Smithers M, Butler CC, Peters JR: The prevalence of multiple
diabetes-related complications. Diabet Med. 2000; 17(2):146-151.

31
41. Chen SJ, Liu JH, Shih HC, Chou P, Tsai CY, and Tung TH: Prevalence and associated factors of lens
opacities among Chinese type 2 diabetics in Kinmen, Taiwan. Acta Diabetologica. 2008; 45(1):7-13.
42. Cyganek K, Malecki MT, Wolkow P, Skupien J, Bobrek J, Czogala M, Klupa T, Sieradzki J: Clinical
risk factors and the role of VDR gene polymorphisms in diabetic retinopathy in Polish type 2 diabetes
patients. Acta Diabetol. 2006; 43(4):114-120.
43. Jacobs J, Sena M, Fox N: The cost of hospitalization for the late complications of diabetes in the
United States. Diabetic Med. 1991; 8:523-529.
44. Bell DS. Diabetic cardiomyopathy. Diabetes Care. 2003; 26: 2949-2951.
45. Elbagir MN, Eltom MA, Mahadi EO, Berne C. Pattern of long-term complications in Sudanese
insulin-treated diabetic patients. Diabetes Res Clin Pract. 1995; 30: 59-67.
46. Lester FT. Amputations in patients attending a diabetic clinic in Addis Ababa, Ethiopia. Ethiop Med
J. 1995; 33: 15-20.
47. PY Drabo, J Kabore, A Lengani. Complications of diabetes mellitus at the hospital Centre of
Ouagadougou. Bulletin de Lasociete de pathologie exotique. 1996; 89 (3): 191-5.
48. Giorgia De Berardis, Maurizio Belfiglio. Erectile dysfunction and Quality of life in type 2 diabetic
patients. Diabetes Care. 2002; 25 (2): 284-291.
49. Ngassa Piotie, Van Zyl D.G, Rheeder P. A cross sectional study on diabetic nephropathy in a tertiary
care clinic in South Africa. JEMDSA. 2015; 20 (1); 67-73.

32
DATA COLLECTION TOOLS
APPENDIX 1: ENGLISH QUESTIONNAIRE
Questionnaire no…………..
Date…………
Name of Hospital (a) Harare Central Hospital (b) Parirenyatwa Central Hospital
Part A: Demographic data
1. What was your age at your last birthday?...................in years
2. Sex (observe only) (a) Female (b) Male
3. What is your marital status? (a) Single (b) married (c) divorced (d) widowed
4. What is the highest level of education that you attained? (a) Never went to school (b ) Primary
(c)Secondary (d) Tertiary
5. What is your current Religion? (a) Orthodox (b) Traditional (c) Pentecostal (d) Apostolic (e) Muslim (f)
None
6. Employment status? (a) Employed (b) self-employed (c) Unemployed (d) Retired (e) Student (f)
other (specify)………………………

33
7. Are there any of your family members who had or currently have diabetes mellitus? (a) Yes (b) No
8. If yes to question 7, did this family member(s) experience any chronic diabetes complications (a) yes (b)
no
9. If yes to question 8, what complications did the family member experience?...............................................
Part B: Factors associated with diabetic complications
10. For how long have you been known to have diabetes mellitus?............in years
11. What is the type of your diabetes? (a) Type 1, (b) Type 2. (Check hospital cards to confirm)
12. What medication are you taking for diabetes? (a) Insulin (b) Oral hypoglycemic (c) both insulin and oral
hypoglycemic (d) Diet only (e) Other (specify)……………………......
13. Do you always take your medication as prescribed? (a) Yes (b) No
14. How often in the last one week did you fail to take your medication? (a) Once (b) Twice (c) Three times
(d) Four or more times
15. Where you diagnosed with any chronic diabetes complication? (a) Yes (b) no [NB: Check cards and all
records to verify the specific complications diagnosed]
16. If you were diagnosed with a diabetes complication, what was/were the specific complication(s) and
when were you diagnosed? [Check cards and all records to
confirm]........................................................................
Smoking habits
17. Do you currently smoke cigarettes? (a) Yes (b) no
18. If you don’t smoke currently, where you a smoker at some point in your life? (a) Yes (b) No
19. If you smoke cigarettes, for how many years have you been smoking?...........years.
20. If you smoke, how many cigarettes do you smoke per day on average?.........
Alcohol consumption
21. Have you ever consumed any alcohol such as beer, wine, and spirits? (a) Yes (b) No
22. Do you currently drink alcohol? (a) Yes (b) No

34
23. Have you consumed any alcohol within the past 30 days? (a) Yes (b) No
24. During the past I month, on how many occasions did you drink at least one standard alcoholic drink? [A
“standard drink” is defined as the amount of alcohol contained in standard glass of beer or wine.]
………………
25. During the past 30 days, when you drank alcohol, how many standard drinks on average did you drink
during one occasion?...........................
26. During the last 1 month, how many times did you drink six or more standard drinks in a single drinking
occasion?..............
Assessment of level of physical activity (Source: STEPwise39 approach to Surveillance of Chronic Diseases
and Risk Factors Assessment Instrument-World Health Organization-Geneva).
I am now going to ask you about the time that you spend doing physical activities in a week.
(a) Work
27. Does your usual work involve vigorous-intensity activity [e.g. carrying or lifting heavy loads, or
construction work or digging] for at least 10 mins continuously? (a) Yes (b) No
28. In a week, on how many days do you do vigorous intensity activities as part of your usual
work?..............
29. Approximately, how much time do you spend doing vigorous-intensity activities at work on a
day?........(in minutes).
30. Does your work involve moderate-intensity activity [e.g. carrying light loads, brisk walking etc] for
at least 10 mins continuously? (a) Yes (b) No
31. In a week, on how many days do you do moderate intensity activities as part of your usual work?.......
32. How much time do you spend doing moderate-intensity activities at work on a day?..........
(b)Travel
The following questions do not include the physical activities at work that you have mentioned. I will ask
you about the usual way you travel. [For example going to work or going for shopping].

35
Do you walk or use a bicycle cycle for at least 10 minutes continuously to get to and from places? (a) Yes
(b) No
33. If yes, in a week, on how many days do you walk or cycle for a minimum of 10 minutes continuously
to go to and from places? (a) Yes (b) No
34. Approximately, how much time do you spend walking or cycling for travel on a day?............minutes
(c) Recreational activities
The next questions do not include the work and transport activities that you have already mentioned above.
I will ask you about recreational activities, sports and fitness related exercises.
35. Do you do any vigorous intensity recreational, sports or fitness related exercises [e.g playing football
or running] for at least 10 mins continuously? (a) Yes (b) No
36. In a week, on how many days do you do any of these exercises?........
37. How much time do you spend doing these exercises on a typical day?....... minutes
38. Do you do moderate-intensity recreational, sports or fitness related exercises [e.g. very brisk walking,
cycling or playing volleyball]? (a) Yes (b) No
39. If yes to question 38, in a week, on how many days do you do such exercises?..........................days
40. How much time do you spend doing those exercises on a typical day...
Hypertension
41. Are you currently hypertensive? (a) Yes (b) No
42. If you are hypertensive, for how long have you been hypertensive………..in years?
43. If you are hypertensive, is your BP well controlled? (a) Yes (b) No. [Check hospital cards to confirm
with last three results, including the one done on day of interview].
Miscellaneous
44. Is your blood sugar level well controlled? (a) Yes (b) No. (Check hospital cards to confirm level of
HB 1C%, RBS). [NB. Good glycaemia control is Hb 1C<7%]

36
45. Have you ever been tested for HIV before? (a) Yes (b) No
46. If yes, are you at liberty to disclose your HIV status to me? (a) Yes (b) No,
47. If yes, what is your HIV status (a) Negative (b) positive
48. If HIV positive are you on anti-retroviral therapy? (a) Yes (b) No
49. If on ART, for how long have you been on treatment? (Specify) .......................in years
a) < 36 months b) > 36months
[This section is for males only, if female, skip to question 50].
50. Are you currently experiencing erectile dysfunction? (a) Yes (b) No
51. If you are experiencing erectile dysfunction, how long have you been having this problem?.......in
years
52. Have you sought treatment for this problem? (a) Yes (b) No and if yes what treatment did you
seek?(specify)..............................
53. Is the erectile dysfunction now better? (a) Yes (b) No

37
APPENDIX 2: SHONA QUESTIONNAIRE
Questionnaire no……
Zuva…………
Zita re Chipatara (a) Harare Central Hospital (b) Parirenyatwa Central Hospital
GWARO REMIBVUNZO
Chikamu chokutanga
1. Mune makore mangani ekuzvarwa?.....................
2. (a) Murume (b) mukadzi…………….
3. Makaroorwa/ roora here? [ ] Ndakaroorwa [ ] Ndakafirwa [ ] Tiri kubika mapapoto [ ]
Handisati ndawanika [ ] Takarambana
4. Makagumira gwaro ripi kuchikoro? [ ] Handina kuenda kuchikoro [ ] Primary [ ] Secondary
[ ] Tertiary
5. Munopinda chitendero chipi?
a) Apostolic b) Pentecostal c) Anglican d) Catholic e) zvimwe..........................................
6. Munoshanda here? (a) ndinoshanda (b) ndinozvishandira (c) Handishandi (d)Ndakabuda basa
nekukura
7. Pane vemumhuri menyu vaimbova kana vatori nechirwere cheshuga here? (a) Hongu (b) Kwete
8. Kana varipo, pane vakamboita zvimwe zvirwere zvaikonzerwa nechirerwere cheshuga here? (a)
Hongu (b) Kwete

38
9. Kana varipo vakaita zvirwere izvozvo, mungadoma zvirwere zvacho
here?..................................................................................
Chikamu chechipiri
10. Mava nemakore magani mabatwa chirwere cheshuga?........................
11. Makanzi chirwere chenyu cheshuga imhando ipi? (a) Type 1 (b) Type 2.
12. Munoshandisa mishonga ipi pachirwere cheshuga? (a) jekiseni (b) mapiritsi(c) majekiseni nemapiritsi
(e) zvimwe……………………......
13. Munotora mushonga nguva dzese here? (a) Hongu (b) Kwete
14. Pasvondo rapfuura, makakanganwa kutora mushonga kangani? (a) Handina (b) Kamwe (c) Kaviri (d)
Katatu zvichikwira.
15. Makambonzi mune chimwe chirwere chakakonzerwa neshuga here? (a) Hongu (b) Kwete [Ndichatarisa
mabhuku enyu ndiongorere]
16. Kana makambobatwa chirwere ichocho chakanzi ndechipi?............................. [Ndichatarisa mabhuku
enyu ndiongorere]
Zvekuputa fodya
17. Parizvino munoputa fodya here? (a) Hongu (b) Kwete
18. Kana musingaputi fodya parizvino, makamboiputa here? (a) Hongu (b) Kwete
19. Kana muchiputa fodya, mava nemakore mangani muchiputa?...
20. Kana muchiputa fodya, munoputa midzanga mingani pazuva?.....
Kumwa doro
21. Makambomwa doro here? (a) Hongu (b) Kwete
22. Parizvino munomwa doro here? (a) Hongu (b) Kwete
23. Pamazuva makumi matatu apfuura, makambomwa doro kangani?.....
24. Pamazuva makumi matatu apfuura, makambomwa mukombe wedoro umwe kana kupfuura kangani?.....
25. Pamazuva makumi matatu apfuura, makamwa mikombe yedoro mingani pazuva rimwe chete?.....

39
26. Pamazuva makumi matatu apfuura, makambomwa doro pazuva rimwe zvekudarika mikombe mitanhatu
kangani?.......
Ongororo yemabasa anosimbisa muviri
Ndava kuda kubvunza nguva yamunotora muchiita mabasa.
Mabasa
27. Basa ramunoita rakaomarara zvakanyanya here? [muenzaniso: kutakura zvinorema, kuchera, kuvaka]
(a) Hongu (b) Kwete
28. Pasvondo rimwe chete, munoita mabasa akoma zvakanyanya mazuva mangani?..........
29. Pasvondo rimwechete, munotora maminetsi mangani muchiita basa rakaoma zvakanyanya?...
30. Munomboita basa rakaoma zvishoma here rakafanana nekufamba muchikasika kana kutakura
zvisingaremi kwemaminetsi gumi kana kupfuura? (a) Hongu (b) Kwete
31. Pasvondo rimwechete, munoita basa rakaoma zvishoma kwemazuva mangani?...
32. Pazuva rimwechete, munotora maminetsi mangani muchiita basa rakaoma zvishoma?...
(b) Mafambiro amunoita kuenda kwakasiyana-siyana, kusanganisira kuenda kubasa
Mibvunzo inotevera inobvunza kubata kwenyu kumwe kusiri kwandambobvunza pamusoro apo. Ndava
kuda kuziva mafambiro enyu kuenda kunzvimba dzakasiyana-siyana sekuenda kubasa, kukereke kana
kuzvitoro. Munofamba here kana kuti munoshandisa bhasikoro kwekanguva kanosvika maminetsi gumi
kana muchienda kubasa? (a) Hongu (b) Kwete
33. Pasvondo rimwechete munofamba kana kutasva bhasikoro mazuva mangani?....
34. Pazuva rimwechete munofamba kana kutasva bhasikoro kwemaminetsi mangani?...
(c) Mamwewo mabasa ekutandara
Zvandava kubvunza hazvisi zvandambobvunza pamusoro apo zvekuenda kubasa ne mafambiro enyu. Ndava
kubvunza zvamunoita kusimbisa muviri uye muchitandara zvenyu makadekara.
35. Munoita zvekusimbisa muviri zvakaomarara here sekumhanya kana kutamba nhabvu? (a) Hongu
(b) Kwete

40
36. Pasvondo rimwe, munoita izvi mazuva mangani?..
37. Pazuva rimwe, munoita izvi kwemaminetsi mangani?..
38. Munoita zvekusimbisa muviri zvakaoma zvishoma here sekufambisa kana kutasva bhasikoro? (a)
Hongu (b) Kwete
39. Pasvondo rimwe, munoita izvi ka kangani?....
40. Pazuva rimwe munoita izvi kwemaminetsi mangani?...
Chirwere che BP
41. Mune chirwere che BP here? (a) Hongu (b) Kwete
42. Kana muine chirwere che BP, mava nemakore mangani muinacho?..
43. Kana muine chirwere che BP, BP yenyu iri kuita zvakanaka here? (a) Hongu (b) Kwete [Ndichatarisa
mumabhuku enyu kuti ndione kuti ndizvo here].
Imwewo mibvunzo
44. Shuga yenyu iri kugara yakaderera sezvinodiwa here? (a) Hongu (b) Kwete [Ndichatarisa mumabhuku
enyu kuti ndione kuti ndizvo here].
45. Makamboongororwa ropa kutarisa HIV here? (a) Hongu (b) Kwete
46. Kana makatorwa ropa, makasununguka here kundiudza kuti zvakamira sei? (a) Hongu (b) Kwete
47. Kana makasununguka nditaurirei henyu kuti zvakamira sei? (a) Negative (b) positive
48. Kana makanzi mune hutachiona hwe HIV, munomwa mapiritsi acho here? (a) Hongu (b) Kwete
49. Kana muchimwa mapiritsi acho, mava nenguva yakadini muchiamwa?..….
[Mibvunzo inotevera ndewevarume chete, kana muri mudzimai musapindure].
50. Muri kuita dambudziko rekusimba kwenhengo yenyu zvekutadza bonde here? (a) Hongu (b) Kwete
51. Kana muine dambudziko iroro, mava nenguva yakadini?...
52. Makambotsvaga rubatsiro here ne dambudziko iroro (a) Hongu (b) Kwete
53. Parizvino zvava nane here? (a) Hongu (b) Kwete

41
APPENDIX 3: TOOLS FOR ANTHROPOMETRIC MEASUREMENTS
Questionnaire number................
1. (a) Weight………..kilograms
(b) Height………metres
(c) Body Mass Index=weight/height2 [kg/m2]………………..
(d) Classification of BMI: 1. Underweight: <18.5kg/m2
2. Normal range: 18.5-24.99kg/m2
3. Overweight: 25-29.99kg/m2
4. Obese: >30kg/m2
Results of investigations and examinations done [Check all patient cards and notes]
2. (a) Hb 1C %.............................
Comments: Poor glycaemic control (i) Yes [>7%] (ii) No [<or=7%]
(a) Serum creatinine………………………
Serum urea………………
Estimated Glomerular Filtration rate using the MDRD equation = [186 x (creatinine/88.4)-1.154 x (age-
0.203) x (0.742 if female) x (1.21 if black)] =………………….
Classification of EGFR: Normal [>60]………
Nephropathy [15-59]……..
Chronic renal failure [<15]………
(c) Lipid profile results……………………………………………………………………………..
Comments: High LDL-Cholesterol [>100] (i) Yes (ii) No

42
(d) Eye examination by specialist ophthalmologist [in the last 1
year]……………………………………………
Comments: [1].Specialist’s diagnosis of retinopathy (i) Yes (ii) No [2] Specialist’s diagnosis of cataracts
(i) Yes (ii) No [3] Specialist’s diagnosis of blindness (i) Yes (ii) No
(e) Stroke [in the last 1
year]…………………………………………………………………………………….
Comments: Stroke (i) Yes (ii) No
(f) Results of foot examination-to be done by researcher (including peripheral pulses-tibial, popliteal,
femoral pulses, diabetic foot syndrome, amputation in the last 1 year)………………………………………
Comments: [1] Diabetic foot syndrome (i) Yes (ii) No [2] Amputation done (i) Yes (ii) No
(g) Heart failure as diagnosed by physician in the last 1 year (i) Yes (ii) No

43
APPENDIX 4: TOOLS FOR ASSESSING PHYSICAL ACTIVITY
Calculation of metabolic equivalence
Metabolic equivalence was calculated using intensity of physical activity as shown in table 7.
Table 7: Calculation of Metabolic Equivalents (MET) of diabetic patients in Harare, 2014. (Source: STEP
wise39 approach to Surveillance of Chronic Diseases and Risk Factors Assessment Instrument. World Health
Organization)
Domain Intensity of activity MET value MET-minutes/week
Work (e.g. construction related work,
lifting loads or digging )
Moderate
Vigorous
4
8
.............
.............
Transport (e.g. walking, cycling) Moderate
Vigorous
4
8
.............
..............
Recreational activity (e.g. playing
volley ball, running or football.)
Moderate
Vigorous
4
8
.............
Total MET-minutes/week ..............
Intensity of physical activity was measured in Metabolic Equivalents (MET), which is essentially the ratio
of an individual’s working metabolic rate relative to his/her resting metabolic rate and was classified as
shown in table 7. The MET-minutes per week were calculated by multiplying the MET value for each activity
by the number of days the activity was done each week multiplied by number of the minutes spend
performing each activity. The number of MET-minutes per week for each activity were then be added to get

44
the total number of MET-minutes per week which in turn were used to classify physical activity into high,
moderate and low as per WHO STEP wise guidelines39.
Classification of level of physical activity
Classification of level of activity was assessed as shown in table 8.
Table 8: Classification of Level of Physical Activity in Harare, 2014. (Source: STEP wise39 approach to
Surveillance of Chronic Diseases and Risk Factors Assessment Instrument. World Health Organization)
Classification Description of level of physical activity
High ≥3 days of vigorous-intensity activity with a minimum of 1500 MET-minutes per week,
or
7 days of moderate or vigorous intensity activity with a minimum of 3000 MET-minutes
per week.
Moderate ≥3 days of vigorous-intensity activity of ≥20 mins per day, or
≥5 days of moderate-intensity activity of ≥30 mins per day, or
≥5 days of moderate or vigorous-intensity activity with a minimum of 600 MET-mins
per week.
Low Any person who does not meet any of the above two criteria

45
CONSENT FORMS
APPENDIX 5: ENGLISH CONSENT FORM
Introduction
Topic: Prevalence and Risk Factors for Diabetes Mellitus Related Chronic Complications in Harare, 2014.
Principal investigator: Tapera Saravoye [MBchB (UZ)]
Phone number: 0772 889622
What you should know before you consent:
This consent is meant for you to familiarize yourself with the purpose, risks, and benefits of this research
study.
Participation in this study is on voluntary basis.
There is no monetary benefit for participating in this study.
The aim of this research is to gain knowledge on prevalence and risk factors for diabetes related
chronic complications and this will help diabetic patients in Harare and this will help you and other
diabetics.
You are allowed to decline participation in this study now and even during the interview if you feel
that you are no longer comfortable with continuing.
There is no penalty for refusing to participate in this study.
Please review this consent form carefully.
Ask any questions before you make your decision.
Purpose

46
You are being asked to participate in a study on: Prevalence and Risk Factors for Diabetes Mellitus Related
Chronic Complications in Harare, 2014. The aim of the study is to gain knowledge on prevalence and risk
factors for diabetes related chronic complications in Harare.
Procedures and duration
We are going to be conducting interviewer administered interviews. During the interview we are going to
ask you a set of 53 questions and this is expected to take at most 20 minutes of your time. You are allowed
not to answer some of the questions if you are not comfortable with answering them. We will measure your
weight, height and perform a physical examination on you. You are allowed to decline this examination if
you feel uncomfortable at any moment during the examination.
Voluntary Participation
It’s important for you to know that participation in this study is voluntary and that refusal to participate does
not have any negative consequences on you. You will still have access to the diabetic clinic services now
and in future. You are allowed to decline participation at any time during the interview.
Confidentiality
We will not include your name on the questionnaire when you agree to participate in this study. Results of
this study will be shared with Harare and Parirenyatwa Hospitals and the University of Zimbabwe. The
purpose of this sharing is for the community in general to benefit as well from our findings.
Risks
We do not anticipate any physical risks due to participation in this study.
Benefits
We do not promise that you will receive financial or material benefits from this study. However your
participation in this study may be a chance for you to know more about the risk factors for diabetes related
chronic complications.
Additional Costs
There will be no further costs to you for your participation in this study.

47
Answers to Questions
Ask any questions with regards to this study that you have on areas that you don’t clearly understand.
Authorization
You are making a decision whether or not to participate in this study. Your signature indicates that you have
read and understood the information provided above, all your questions were answered, and you have
decided to participate.
Name of research participant (print) Date
Signature of respondent or legally authorized representative Time
You will be given a copy of this consent form to keep
If you have any questions concerning this study or concerns beyond those answered by the investigator,
including questions about the research, your rights as a research subject or research related injuries, or if you
feel that you have been treated unfairly and would like to talk to someone other than the researcher, please
feel free to contact Medical Research Council of Zimbabwe (MRCZ) on telephone 04-791792 or 791193.

48
APPENDIX 6: SHONA CONSENT FORM
TSAMBA YECHITENDERANO
Kutanga
Musoro weTsvakiridzo: Ongororo yehuwandu nezvikonzero zve zvirwere zvinounzwa nekuda kwekuva
nechirwere cheshuga muguta re Harare, gore ra2014.
Muongorori: Tapera Saravoye [MBchB (UZ)]
Nhare: 0772 889622
E-mail: [email protected]
Zvamunofanirwa kuziva musati mapinda mutsvakiridzo iyoyi:
Tsamba yechitenderano iyi inobatsira kuti muve neruzivo rwune udzamu pamusoro pe tsvakiridzo
Hamumanikidzwe kupinda muongororo iyi
Hapana mari yamuchapiwa nekupinda muongororo iyi
Tsvakiridzo iyi iri kuitwa kuti tigoziva zvimwe zvangokonzera gomarara rechibereko
Munobvumirwa kuramba kuenderera mberi netsvakiridzo iyi nyangwe mavapakati payo
Hapana zvakashata zvinoitika nyangwe mukaramba kupinda tsvakiridzo iyi.
Bvunzayi mibvunzo yamunoda musati mapinda mutsvakiridzo iyi
Chinangwa chetsvakiridzo iyi
Murikukumbirwa kuti mupinde mutsvakiridzo ine musoro unoti: Ongororo yehuwandu nezvikonzero zve
zvirwere zvinounzwa nekuda kwekuva nechirwere cheshuga muguta re Harare, gore ra2014. Tino tarisira
kuwana zvinokenzera nehuwandu hwezvirwere zvinokonzerwa nekuda kwechirwere cheshuga kana tapedza
ongororo iyi.
Zvatichange tichiita muongororo iyi

49
Tichakubvunzayi mibvunzo inokwana makumi mashanu nemitatu maererano nezvetsvakiridzo iyi.
Tinotarisira kuita maminitsi makumi maviri pamibvunzo iyoyi. Muchazokumbirwawo kuongororwa muviri
wenyu pamwe chete nekupimiwa uremu neurefu hwenyu.
Kupinda kwenyu mutsvakiridzo
Zvakakosha kuti muzive kuti kupinda kwenyu mutsvakiridzo iyi kuda kwenyu uye hamumanikidzwe.
Mukaramba zvenyu hapana chakashata chinoitika kwamuri uye munobvumirwa kuuya kumakiriniki
ezvekurapwa kwechirwere cheshuga nyangwe maramba kupinda mutsvakiridzo iyi.
Kuvimbika kweongororo
Patsvakiridzo iyoyi hapana patinonyora zita renyu. Zvichabuda muongororo iyi kuti tichazviturirawo
kuzvipatara zve Harare ne Parirenyatwa uye neUniversity yeZimbabwe. Chinagwa chekutaurirana newamwe
ndechekuti vanhu vemuguta reHarare vagobatsirikawo nezvinenge zvabuda muongororo iyi.
Kushungurudzika
Hapana kushungurudzika kwatinotarisira mutsvakiridzo iyi. Tichakuongororai tichitarisa zvirwere zvingava
zvakakonzerwa nechirwere cheshuga pamuviri wenyu pamwe nokupima urefu neuremu hwenyu.
Zvakanakira kuvamuongororo iyi
Hapana mari kana zvimwe zvinhu zvamunopihwa mutsvakiridzo iyi asi kuvamo kwenyu mutsvakiridzo iyi
kunobatsira kuti imi mugoziva zvakawanda maererano nezvirewere zvinokonzerwa nechirwere cheshuga.
Mumwe muripo
Hapana mari dzamunotarisirwa kubhadhara kuti muvemuongororo iyi.
Mibvunzo ingavapo
Kana paine mibvunzo yamuinayo makasununguka kuibvunza.
Kubvuma kwenyu kupinda mutsvagiridzo
Mave pachidanho chekuti munyore kuti munoda kupinda here mutsvakiridzo kana kuti hamudi. Kana
mukasaina apa zvinoreva kuti manzwisisa zviri muchitenderano chino uye mapindirana nazvo kuti munoda
kuva mutsvakiridzo iyi.

50
Zita remupinduri (nyorai nemavara makuru) Zuva
Runyoro rwechibvumirano rwemupinduri Zuva
Muchapihwawo imwe tsamba yechitenderano yamuchanochengeta kumba
Kana mune mibvunzo isina kupindurwa nemuongorori zvichisanganisira mibvunzo pamusoro peongororo
ino, kodzero dzenyu kana mibvunzo yakanangana nekubatwa kwamaitwa muongororo ino, kana kusabatwa
zvakanaka kwamunenge maitwa makasununguka kuridza nhare paboka reMedical Research Council of
Zimbabwe panhamba dzerunhare dzinoti: 04-791792 kana kuti pa 791193.

51
APPENDIX 7: MRCZ APPROVAL LETTER

52