Embed Size (px)
Citation preview
The regulatory drug approval processfor industry mandates that in vitro and
in vivo studies be conducted to allowdrug-drug interactions (DDIs) to becomemore predictable and preventable.1 Phar-macokinetic cytochrome P450 (CYP)–based drug metabolism falls under thisguidance. The guidance recommendsdetection of potential CYP-mediatedDDIs for CYP isoenzymes CYP1A2,CYP2C9, CYP2C19, CYP2D6, CYP3A,CYP2C8, and CYP2B6.1,2 By identifyingagents that are likely to produce signifi-cant alterations in drug bioavailability byinhibiting or inducing these cytochromes,the expectation is that dose adjustments ordrug substitutions will be made in an at-tempt to prevent toxicity.3,4
Unfortunately, most in vivo and in vit-ro studies of potential CYP-mediatedDDIs evaluate only 2 drug profiles andapplication of the results to patients withchronic conditions taking complex mul-tidrug regimens is difficult. In light ofthis limitation, new guidelines from theFood and Drug Administration (FDA)
Prevalence and Risk of Potential Cytochrome P450–Mediated
Drug-Drug Interactions in Older Hospitalized Patients with
Polypharmacy
Julie Doan, Hubert Zakrzewski-Jakubiak, Julie Roy, Jacques Turgeon, Cara Tannenbaum
Drug Interactions
Author information provided at end of text.
© 1967-2013 Harvey Whitney Books Co. Allrights reserved. No part of this document maybe reproduced or transmitted in any form or byany means without prior written permission ofHarvey Whitney Books Co. For reprints of anyarticle appearing in The Annals, please [email protected]
BACKGROUND: As rates of polypharmacy rise and medication regimens becomemore complex, the risk of potential cytochrome P450 (CYP)–mediated drug-druginteractions (DDIs) is a growing clinical concern for older adults.
objective: To determine the prevalence of potential CYP-mediated DDIs in olderhospitalized adults with polypharmacy and analyze the relationship between thenumber of drugs dispensed and the probability of these interactions in this high-riskpopulation.
METHODS: A prospective 16-week cohort study was conducted among consecutivenew patients aged 65 years and older with polypharmacy (>5 drugs) admitted to acommunity hospital. The medication profiles of these patients were analyzed with anew multidrug cytochrome-specific software program. The prevalence of potentialCYP-mediated DDIs was determined, with the probability calculated as a function ofthe number of medications dispensed using multivariate Poisson regressionadjusted for age and sex. Comparative performance of the software program and astandard 2-drug alert program for detecting these DDIs was evaluated using theWilcoxon-Mann-Whitney rank-sum test. Pharmacists’ decisions to recommendmedication adjustment based on the probability of CYP-mediated DDIs wererecorded.
RESULTS: The prevalence of potential CYP-mediated DDIs detected among 275older adults with polypharmacy was 80%. The probability of at least 1 CYP-medi-ated DDI was 50% for persons taking 5-9 drugs, 81% with 10-14 drugs, 92% with15-19 drugs, and 100% with 20 or more drugs. Addition of each medication to a 5-drug regimen conferred a 12% increased risk of a potential CYP-mediated DDI afteradjustment for age and sex (OR 1.12; 95% CI 1.09-1.14). The multidrug softwareidentified a median increase of 3 (95% CI 2.5-3.5) potential CYP-mediated DDIs perpatient, compared to use of the standard 2-drug alert software. Pharmacists tar-geted patients for medication adjustment or close clinical monitoring in 23% ofcases.
CONCLUSIONS: The prevalence of potential CYP-mediated DDIs is high ingeriatric patients with polypharmacy. The risk of DDIs increases as a function ofthe number of medications dispensed. Pharmacists’ decision to intervene forpotential CYP-mediated DDIs depends on clinical judgment in addition to theoutput from drug alert software programs, but may be facilitated by a singlemulticomponent, multidrug potential CYP-mediated DDI assessment.
Ann Pharmacother 2013;47:324-32.
Published Online, 12 Mar 2013, theannals.com, doi: 10.1345/aph.1R621
324 n The Annals of Pharmacotherapy n 2013 March, Volume 47 theannals.com
at UZH Hauptbibliothek / Zentralbibliothek Zürich on July 7, 2014aop.sagepub.comDownloaded from
CYP450-Mediated Drug-Drug Interactions in Older Hospitalized Patients
The Annals of Pharmacotherapy n 2013 March, Volume 47 n 325theannals.com
and the International Conference on Harmonisation seek toimprove pharmacokinetic testing for geriatric patients andin patients with renal impairment.5,6 Until these new guide-lines come into force, clinicians must continue to rely onexisting information from 2-drug alert software programsto provide clinical support for minimizing drug interac-tions. Programs that display 2-drug alerts are unable to as-sess multidrug combinations simultaneously, and havevarying degrees of sensitivity and specificity.7,8 The result-ing uncertainty, inaccuracy, and information overload hasled to the phenomenon of “fatigue alert” or “pop-up fa-tigue” for clinicians verifying orders, further limiting theassessment of multidrug potential CYP-mediated DDIs inpatients with polypharmacy.9,10
Until recently there was no simple way to make intelli-gent predictions about the likelihood or severity of clinical-ly important multidrug potential CYP-mediated DDIs inolder adults with polypharmacy. However, cytochrome-specific multidrug analysis software is now available thatlists all of a patient’s medications and displays the relativeaffinity of each medication for each cytochrome isoen-zyme in a 1-page integrative color-coded matrix.11,12 Theprogram highlights, in a single table, all object and precipi-tant drugs metabolized by the same cytochrome that can beimplicated in potentially altering the bioavailability of theobject drug in excess of a conservative bioequivalencestandard of ±30%, based on pharmacokinetic data.1 Thebioequivalence standard of 30% was chosen based on con-servative regulatory definitions of bioequivalence forgeneric medication from the FDA13 and regulations appli-cable in the European Economic Area14 and Australia.15
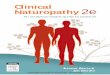
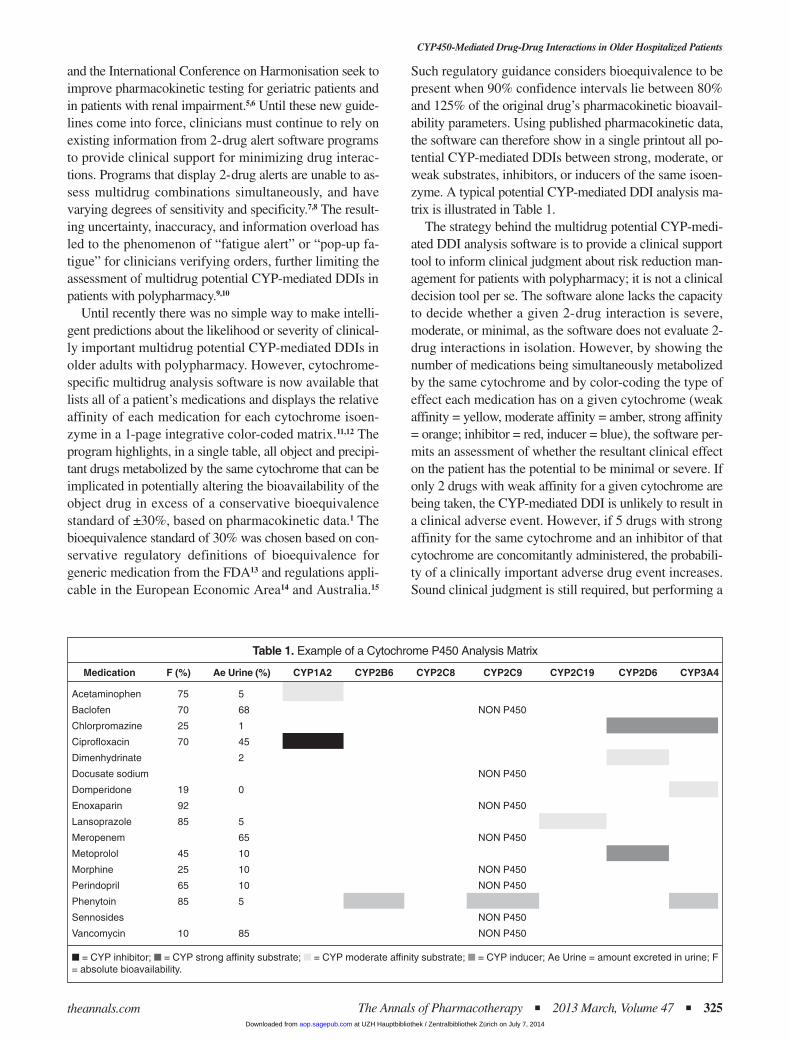
Such regulatory guidance considers bioequivalence to bepresent when 90% confidence intervals lie between 80%and 125% of the original drug’s pharmacokinetic bioavail-ability parameters. Using published pharmacokinetic data,the software can therefore show in a single printout all po-tential CYP-mediated DDIs between strong, moderate, orweak substrates, inhibitors, or inducers of the same isoen-zyme. A typical potential CYP-mediated DDI analysis ma-trix is illustrated in Table 1.
The strategy behind the multidrug potential CYP-medi-ated DDI analysis software is to provide a clinical supporttool to inform clinical judgment about risk reduction man-agement for patients with polypharmacy; it is not a clinicaldecision tool per se. The software alone lacks the capacityto decide whether a given 2-drug interaction is severe,moderate, or minimal, as the software does not evaluate 2-drug interactions in isolation. However, by showing thenumber of medications being simultaneously metabolizedby the same cytochrome and by color-coding the type ofeffect each medication has on a given cytochrome (weakaffinity = yellow, moderate affinity = amber, strong affinity= orange; inhibitor = red, inducer = blue), the software per-mits an assessment of whether the resultant clinical effecton the patient has the potential to be minimal or severe. Ifonly 2 drugs with weak affinity for a given cytochrome arebeing taken, the CYP-mediated DDI is unlikely to result ina clinical adverse event. However, if 5 drugs with strongaffinity for the same cytochrome and an inhibitor of thatcytochrome are concomitantly administered, the probabili-ty of a clinically important adverse drug event increases.Sound clinical judgment is still required, but performing a
Table 1. Example of a Cytochrome P450 Analysis Matrix
Medication F (%) Ae Urine (%) CYP1A2 CYP2B6 CYP2C8 CYP2C9 CYP2C19 CYP2D6 CYP3A4
Acetaminophen 75 5
Baclofen 70 68 NON P450
Chlorpromazine 25 1
Ciprofloxacin 70 45
Dimenhydrinate 2
Docusate sodium NON P450
Domperidone 19 0
Enoxaparin 92 NON P450
Lansoprazole 85 5
Meropenem 65 NON P450
Metoprolol 45 10
Morphine 25 10 NON P450
Perindopril 65 10 NON P450
Phenytoin 85 5
Sennosides NON P450
Vancomycin 10 85 NON P450
n = CYP inhibitor; n = CYP strong affinity substrate; n = CYP moderate affinity substrate; n = CYP inducer; Ae Urine = amount excreted in urine; F= absolute bioavailability.
at UZH Hauptbibliothek / Zentralbibliothek Zürich on July 7, 2014aop.sagepub.comDownloaded from

single multidrug assessment rather than multiple sequential2-drug assessments for patients with polypharmacy mayreduce fatigue alert and drug alert dismissal, as reported by20-40% of clinicians.9,10 DDI detection software aims tohelp the clinician predict and prevent complex CYP-medi-ated DDIs; ascertainment of whether or not these interac-tions translate to adverse clinical outcomes requires indi-vidual assessment.
The main objective of this study was to determine theprevalence and risk of potential CYP-mediated DDIsamong a cohort of older adults with polypharmacy admit-ted to a general community-based hospital. Secondary ob-jectives were to analyze the relationship between the num-ber of medications dispensed and the risk of potentialCYP-mediated DDIs, to compare the number of potentialCYP-mediated DDIs detected by the multidrug softwareversus a standard 2-drug alert software program, and to de-termine the frequency with which pharmacists intervene toreduce potential CYP-mediated DDIs.
Methods
POPULATION AND SETTING
A 16-week prospective cohort study was conducted in alarge community-based hospital in the Montreal area. Allconsecutive patients aged 65 years of age and older newlyadmitted to the nonsurgical wards were recruited to thestudy between September 2010 and March 2011. Patientswere eligible for inclusion if the admitting prescription or-ders contained a minimum of 5 prescription-based oralmedications, including as-needed medication and any newin-hospital prescriptions. Patients could participate in thestudy only once; the drug profiles of patients who werereadmitted to hospital during the 16-week study periodwere not reanalyzed. The study was approved by the studycenter’s Research Ethics Committee. All 15 pharmacistsworking in the hospital’s pharmacy unit provided writteninformed consent to participate in the study.
EXPOSURES AND OUTCOMES
Each new patient’s pharmaceutical profile was exposedto the multidrug potential CYP-mediated DDI detectionsoftware (InterMedRx) as well as to the standard 2-drugalert software used at the hospital (FirstDataBank). Thenumber and types of prescriptions per patient, and the po-tential CYP-mediated DDIs generated by each of the soft-ware programs were recorded. The primary outcome wasthe frequency of potential CYP-mediated DDIs detectedper patient with the multidrug software. A secondary out-come was the difference in the number of potential CYP-mediated DDIs detected by the multidrug software com-pared to the standard 2-drug alert software.
A process analysis was conducted to determine the rateand types of intervention by hospital pharmacists on poten-tial CYP-mediated DDIs detected in a sample of CYP out-put analyses for 52 patients with additional potential CYP-mediated DDIs compared to the standard software. Thesubsample of 52 patients was selected based on at least 1of the potential CYP-mediated DDIs detected by the mul-tidrug software appearing on a list of recognized drug in-teractions from Stockley’s Drug Interactions online,16
Thomson Reuter’s MicroMedex system,17 or in Hansten &Horn’s Drug Interactions Analysis and Management text-book.18 The types of interventions performed by the phar-macists were recorded and categorized descriptively as:follow-up of clinical signs, symptoms, or laboratory tests; achange in the timing of administration of the drug; or dosemodification, substitution, or complete discontinuation ofthe drug class. Pharmacists provided information on theirdecision to intervene and the reasons why. Demographicdata for each patient were collected from the summarysheets available on the hospital’s digitized archive systemafter discharge. At no time during the study were patientscontacted by the study researchers.
STATISTICAL ANALYSIS
The prevalence of potential CYP-mediated DDIs wasdetermined by the number of patients in the cohort forwhom 1 or more potential CYP-mediated DDIs were de-tected by the multidrug software. Poisson regression wasused to estimate the risk of these interactions as a functionof the number of medications dispensed. Age as a contin-uous variable and sex as a binary variable were adjustedfor in multivariate analyses. The distribution of potentialCYP-mediated DDIs was skewed, so to compare the num-ber of interactions detected by the 2 software programs,the median number of potential CYP-mediated DDIs de-tected by each program was calculated along with totaland interquartile ranges. The comparative performance ofthe 2 software programs was evaluated using the Wilcox-on-Mann-Whitney rank-sum test.19 The difference be-tween the 2 software programs was quantified using theHodges-Lehmann estimator, which is the median of allpossible differences in outcomes between the 2 exposures.A nonparametric 0.95 confidence interval for the Hodges-Lehmann estimator was calculated for this estimate. Anal-yses were conducted using SAS version 9.2. The samplesize for this study was driven by the ability to detect oneadditional potentially clinically relevant potential CYP-mediated DDI per 5 patients compared to use of the stan-dard software. To be able to detect a difference of 0.2DDIs per patient with a standard deviation of 1, an α errorof 0.05, and a power of 90%, 216 patients needed to be re-cruited.19
326 n The Annals of Pharmacotherapy n 2013 March, Volume 47 theannals.com
J Doan et al.
at UZH Hauptbibliothek / Zentralbibliothek Zürich on July 7, 2014aop.sagepub.comDownloaded from
Results
PREVALENCE AND RISK OF POTENTIAL CYP-MEDIATED
DDIs AS A FUNCTION OF THE NUMBER OF MEDICATIONS
DISPENSED
Two hundred seventy-five consecutive patients receiv-ing 5 or more drugs upon hospital admission were eligiblefor inclusion. Patients were a mean (SD) age of 83.0 (8.3)years (range 65-103) and 56% were female. Participantsreported an average of 6.7 (3.4) comorbidities and weretaking a mean 13.9 (5.3) drugs (median 13, range 5-30) atthe time of admission.
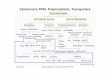
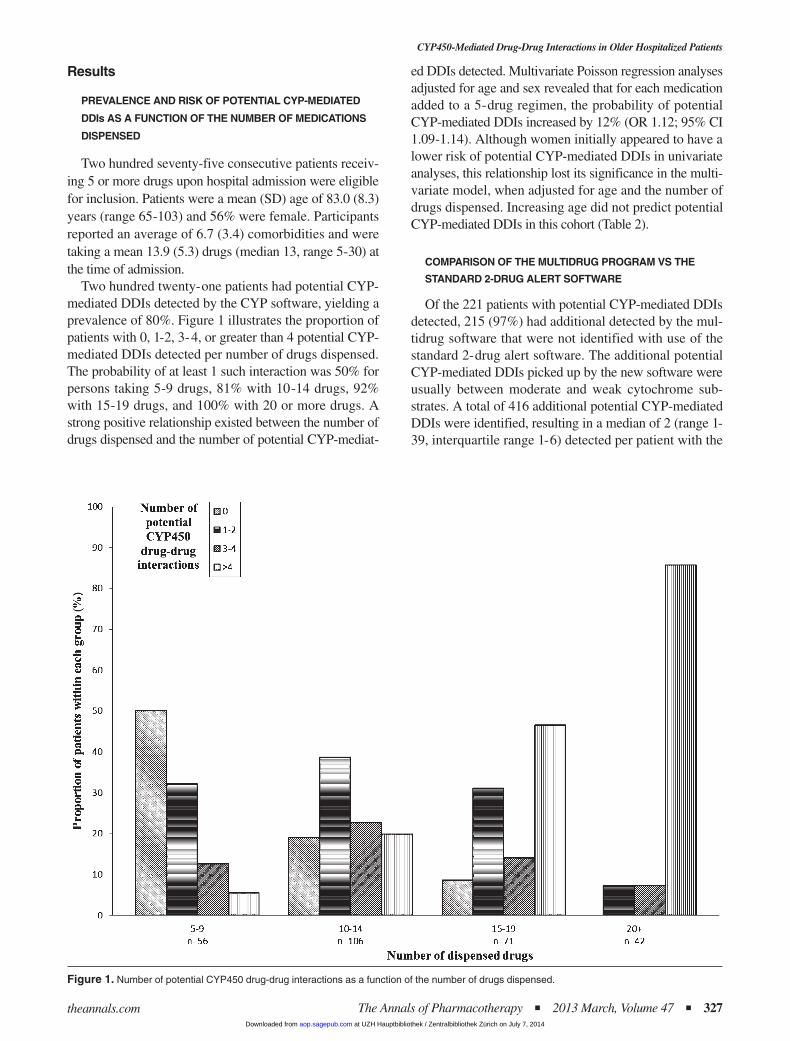
Two hundred twenty-one patients had potential CYP-mediated DDIs detected by the CYP software, yielding aprevalence of 80%. Figure 1 illustrates the proportion ofpatients with 0, 1-2, 3-4, or greater than 4 potential CYP-mediated DDIs detected per number of drugs dispensed.The probability of at least 1 such interaction was 50% forpersons taking 5-9 drugs, 81% with 10-14 drugs, 92%with 15-19 drugs, and 100% with 20 or more drugs. Astrong positive relationship existed between the number ofdrugs dispensed and the number of potential CYP-mediat-
ed DDIs detected. Multivariate Poisson regression analysesadjusted for age and sex revealed that for each medicationadded to a 5-drug regimen, the probability of potentialCYP-mediated DDIs increased by 12% (OR 1.12; 95% CI1.09-1.14). Although women initially appeared to have alower risk of potential CYP-mediated DDIs in univariateanalyses, this relationship lost its significance in the multi-variate model, when adjusted for age and the number ofdrugs dispensed. Increasing age did not predict potentialCYP-mediated DDIs in this cohort (Table 2).
COMPARISON OF THE MULTIDRUG PROGRAM VS THE
STANDARD 2-DRUG ALERT SOFTWARE
Of the 221 patients with potential CYP-mediated DDIsdetected, 215 (97%) had additional detected by the mul-tidrug software that were not identified with use of thestandard 2-drug alert software. The additional potentialCYP-mediated DDIs picked up by the new software wereusually between moderate and weak cytochrome sub-strates. A total of 416 additional potential CYP-mediatedDDIs were identified, resulting in a median of 2 (range 1-39, interquartile range 1-6) detected per patient with the
CYP450-Mediated Drug-Drug Interactions in Older Hospitalized Patients
The Annals of Pharmacotherapy n 2013 March, Volume 47 n 327theannals.com
Figure 1. Number of potential CYP450 drug-drug interactions as a function of the number of drugs dispensed.
at UZH Hauptbibliothek / Zentralbibliothek Zürich on July 7, 2014aop.sagepub.comDownloaded from

multidrug software. One outlier patient had 39 potentialCYP-mediated DDIs detected, while the remaining pa-tients had a range of 1-20 identified with the multidrugsoftware. The standard software detected a median of 0 po-tential CYP-mediated DDIs per patient (range 0-4, in-terquartile range 0-1). Among patients with interactions,use of the multidrug software increased the number of po-tential CYP-mediated DDIs detected by 3 (95% CI 2.5-3.5; p < 0.001), with a range of 0-36 additional potentialinteractions detected per patient. Removal of the outlier pa-tient with 39 potential CYP-mediated DDIs from the analy-ses did not significantly change the additional number ofpotential, CYP-mediated DDIs detected.
FREQUENCY OF PHARMACISTS’ INTERVENTIONS
Follow-up with the hospital pharmacists was performedusing a subsample of 52 patients. Based on the number andtype of interactions displayed on the InterMedRx printout,the clinical status of the patient, the possibility for drugsubstitution, and the pharmacist’s judgment, interventionswere made in 12 of 52 patients (23%). Medication discon-tinuation was recommended for 3 CYP-mediated DDIs,medication substitution for 3, dose adjustment for 2, andclose clinical monitoring for 4.
Table 3 provides examples of potential CYP-mediatedDDIs that were judged by pharmacists to warrant medica-tion substitution, discontinuation, or dose adjustment to re-duce potentially clinically relevant effects. Common rea-sons for taking action to modify the risk of a potentiallyrelevant CYP-mediated DDI were (1) when therapeuticfailure or increased toxicity from one of the interactingsubstrates was thought to underlie the condition that pre-cipitated the patient’s admission (eg, uncontrolled neu-ropsychiatric symptoms in a patient with dementia); (2)when an equally efficacious alternative with a lower risk ofpotential CYP-mediated DDIs was available at similar costfor a condition that required treatment; and (3) when oneof the medications had no clear indication. Among the re-maining 77% cases for which no action was deemed nec-essary, the rationale most frequently provided was that the
interacting substrates were prescribed prior to hospitaliza-tion and did not appear to be adversely affecting the pa-tients’ current clinical status. A number of these examplesare provided in Table 3.
Discussion
Findings from this study suggest that 80% of olderadults with polypharmacy admitted to the nonsurgicalwards of a general medical hospital have potential CYP-mediated DDIs. The number of these potential interactionsis positively related to the number of medications dis-pensed, with 5 medications conferring a 50% risk and 20medications guaranteeing a 100% risk of at least 1 poten-tial CYP-mediated DDI. Use of a multidrug drug interac-tion software led to detection of an additional 3 potentialCYP-mediated DDIs per patient compared to use of a stan-dard 2-drug alert software program. Fifteen percent of pa-tients underwent a change to their medication regimen as aresult of the pharmacists’ interpretation of risk according tothe potential interaction analysis matrix, and close clinicalmonitoring was recommended in an additional 8%.
The prevalence of patients with potential CYP-mediatedDDIs in this population of community-dwelling older adultsadmitted to a general hospital was identical to the 80% preva-lence of potential CYP-mediated DDIs found in a specializedgeriatric center in Montreal,11 and similar to the 73% and68% prevalence reported on general adult and geriatric psy-chiatry units, respectively, in Sheffield, UK.20 A cross-sec-tional study of 900 patients from 6 different populations inthe Netherlands revealed that geriatric, psychogeriatric, andpsychiatric patients present a 2-fold higher risk of being treat-ed with at least 1 drug metabolized by CYP2D6 compared tothe general population.21 As CYP3A4 and CYP2D6 are re-sponsible for the metabolism of 93% of drugs undergoinghepatic oxidation in the geriatric population,11 our study sug-gests that as the number of medications metabolized by theCYP system increases, so too does the risk that at least 2drugs in a multidrug regimen will share a common metabolicpathway and interact.3,4 Ten percent and 5% of white peopleare poor metabolizers or ultrarapid metabolizers of CYP2D6
328 n The Annals of Pharmacotherapy n 2013 March, Volume 47 theannals.com
J Doan et al. CYP450-Mediated Drug-Drug Interactions in Older Hospitalized Patients
Table 2. Estimated Regression Coefficients and Corresponding Standard Errors for Crude and Multivariate Poisson Regression of Number of Drugs on the Number of Potential CYP450 Interactions
Crude Multivariatea
Estimated Estimated Estimated EstimatedRegression Standard Odds Ratio, Regression Standard Odds Ratio,
Covariate Coefficient Error p Value 95% CI Coefficient Error p Value 95% CI
Number of drugs 0.12 0.01 <0.001 1.13 (1.10-1.15) 0.12 0.01 <0.001 1.12 (1.09-1.14)
Increasing age (years) –0.01 0.62 0.51 1.00 (0.98-1.01) 0.002 0.01 0.78 1.00 (–0.01 to 0.02)
Female sex –0.29 0.14 0.04 0.75 (0.56-0.99) 0.18 0.13 0.15 1.20 (–0.07 to 0.42)
aMultivariate analyses are adjusted for the other covariables.
at UZH Hauptbibliothek / Zentralbibliothek Zürich on July 7, 2014aop.sagepub.comDownloaded from

substrates, respectively, which lends further uncertainty topredicting which potential CYP-mediated DDIs warrant in-tervention in order to avoid suboptimal outcomes.22
Although DDIs are strongly associated with adverse drugevents,23,24 the pharmacists in our study judged that exposureto a potential drug interaction did not always warrant inter-vention. In the absence of validation studies showing a con-sistent correlation between potential CYP-mediated DDIsand actual drug-induced effects, risk management requiresthe pharmacist to make a clinical judgment about medicationsubstitution. There currently exists no standardized method ofcategorizing and determining the clinical relevance of poten-tial DDIs, due to a continued lack of information about thequality of the evidence base for DDIs and the unique set ofpatient risk factors that contribute to or diminish patient harmin the presence of CYP-mediated DDIs.25 Principles of ap-propriate geriatric prescribing recommend that medicationthat is equally or more effective for treating the same condi-tion but that introduces a substantially lower risk of adversedrug events should be preferentially substituted for medica-tions that incur greater risk.26 Sound clinical judgment, reduc-tion of polypharmacy, and increased use of lower risk phar-macologic or nonpharmacologic alternatives remain thesafest strategies to reduce risk. In our study, the CYP-mediat-
ed DDI matrices sensitized pharmacists to interactions thatcould be contributing to patients’ symptoms, and substitu-tions and adjustments were performed in a quarter of cases topreemptively reduce risk.
Clinicians may disagree whether monitoring, medica-tion substitution, dose adjustment, scheduling changes, ordrug discontinuation should be recommended for potentialCYP-mediated DDIs, even when clinical practice guide-lines exist.11 Decisions are predictably most straightfor-ward when a strong inhibitor or inducer is involved in theinteraction and the patient is symptomatic. Interventionswill be more variable when substrates with equally weakor moderate affinities for the same CYP isoenzyme are ad-ministered simultaneously and more than one course of ac-tion is deemed acceptable. For example, data from Table 3suggest that risperidone could have been discontinued inthe case of the potential CYP3A4 DDI between carba-mazepine and risperidone if the indication for risperidonewere reassessed. The dose of venlafaxine could have beenreduced if potential toxicity was a concern because of thepotential CYP2D6 DDI between metoprolol and venlafax-ine. However, health care providers may reasonably judgethat an interaction is not clinically significant enough towarrant intervention, or that medication adjustment is not
CYP450-Mediated Drug-Drug Interactions in Older Hospitalized Patients
The Annals of Pharmacotherapy n 2013 March, Volume 47 n 329theannals.com
Table 3. Examples of Cytochrome P450–Mediated Drug-Drug Interactions Detected Resulting in Medication Adjustment or No Medication Adjustment
Isoenzyme Interactions Pharmacists’ Recommendation and Rationale
Risk reduction action taken
3A4 Phenytoin (inducer) + donepezil (weak Substitute donepezil with rivastigmine (no hepatic metabolism) to prevent reducedaffinity substrate) therapeutic efficacy
3A4 Diltiazem (strong affinity substrate) + Substitute simvastatin with rosuvastatin (metabolized by CYP2C9) to lessen myalgias insimvastatin (moderate affinity substrate) a pain pt. due to increased bioavailability
3A4 Losartan (prodrug) + atorvastatin Substitute losartan with valsartan (no hepatic metabolism) to increase therapeutic(moderate affinity substrate) efficacy in a cardiovascular pt. with uncontrolled lipid levels
3A4 Fluconazole (inhibitor) + amlodipine Dose reduction for amlodipine in an unstable pt. with hypotension due to increased(moderate affinity substrate) bioavailability; to be reassessed when fluconazole is discontinued
3A4 Quinine (weak affinity substrate) + Discontinue quinine because of lack of proven efficacy for nocturnal leg cramps anddextromethorphan (weak affinity substrate) increased risk of long QT interval syndrome in a pt. with arrhythmias
2D6 Amiodarone (inhibitor) + metoprolol Dose reduction of metoprolol and monitor bradycardia due to increased bioavailability(moderate affinity substrate) of metoprolol in a pt. with falls
2D6 Amiodarone (inhibitor) + amitriptyline Discontinue amitriptyline because of increased risk of toxicity in a pt. with cognitive(weak affinity substrate) impairment and orthostatic hypotension
2D6 Metoprolol (moderate affinity substrate) + Discontinue diphenhydramine in a pt. with confusion because of increased risk ofdiphenhydramine (moderate substrate) cognitive toxicity due to higher bioavailability
No risk reduction action taken
3A4 Diltiazem (strong affinity substrate) + No modification required; chronic use; international normalized ratio within therapeuticwarfarin (strong affinity substrate) limit and blood pressure is well controlled
3A4 Amlodipine (moderate affinity substrate) + No modification required; chronic use; reduced bioavailability of the active metaboliteclopidogrel (prodrug and weak substrate) of clopidogrel may lead to diminished efficacy but pt. is stable
3A4 Carbamazepine (inducer) + risperidone No modification required; chronic use; reduced bioavailability of risperidone may lead(weak affinity substrate) to diminished clinical efficacy but pt. is stable
3A4 Warfarin (strong affinity substrate) + No modification required; chronic use; increased bioavailability of alfuzosin could leadalfuzosin (weak affinity substrate) to accrued toxicity (eg, hypotension) but pt. asymptomatic
2D6 Metoprolol (moderate affinity substrate) + No modification required; chronic use; increased bioavailability of venlafaxine couldvenlafaxine (weak affinity substrate) lead to accrued toxicity (eg, somnolence) but pt. is stable
at UZH Hauptbibliothek / Zentralbibliothek Zürich on July 7, 2014aop.sagepub.comDownloaded from

possible in the absence of therapeutic substitutes. PotentialCYP-mediated DDIs were dismissed in our study whenthe offending drugs had been used over long periods oftime and the patient was experiencing no adverse effects.Patient monitoring and medication adjustment were rec-ommended in only 23% of cases. This 1 in 4 increased ef-fort at DDI prevention due to use of a new multidrug soft-ware in a busy community hospital could arguably bedeemed significant. Interestingly, the rate of interventionwas lower than the 40% intervention rate observed amongspecialized geriatric pharmacists during an earlier project.11
Many health organizations endorse or use medicationmanagement information technology to improve patientsafety.27 The majority of computerized interventions to op-timize prescribing for the elderly has been aimed at theprescribing physician.27,28 Pharmacists may be betterequipped than physicians to manage complex CYP-medi-ated DDIs in the elderly based on their extensive trainingin pharmacokinetics and oxidative hepatic metabolism.Research needs to evaluate how the 2 disciplines can workconjointly to reduce the independent impact of CYP-medi-ated DDIs during the already complex evaluation of anolder patient’s medication profile.
Limitations of this study include the assessment of phar-macists’ interventions in the context of a research protocol,which may not reflect real-life findings. Furthermore, inpa-tient medication use may not reflect outpatient medicationuse, so the findings from this study may not be generaliz-able to the outpatient setting. There has been no validationwork on the correlation of the multidrug software’s outputwith actual measured CYP activity levels in individual pa-tients, which is a limitation of all clinical decision-supportprograms.25 Only potential CYP-mediated DDIs were eval-uated in this study, not clinical outcomes. A randomizedcontrolled trial is needed to determine the impact of themultidrug drug interaction software on the prevention ofclinically significant outcomes in geriatric patients.
Use of a multidrug analysis matrix rather than a pair-wise listing of potential DDIs enabled a more detailed ap-praisal of pharmacokinetic multidrug potential CYP-mediat-ed DDIs by hospital pharmacists treating older patients withpolypharmacy. The prevalence of such interactions is high inolder adults admitted to the hospital, and increases as a func-tion of the number of medications consumed. While manyCYP-mediated DDIs may not warrant medication adjust-ment, strategies that raise awareness of potential interactionsand that increase application of geriatric prescribing princi-ples should be implemented to reduce polypharmacy andaugment rates of safer medication management.
Julie Doan PharmD MSc, Clinical Pharmacist, Sir Mortimer-B DavisJewish General Hospital, Faculty of Pharmacy, Université de Mon-tréal, Montréal, Quebec, Canada Hubert Zakrzewski-Jakubiak PharmD MSc, Clinical Pharmacist,Faculty of Pharmacy, Université de Montréal
Julie Roy PhD, Clinical Pharmacist, Sir Mortimer-B Davis JewishGeneral Hospital and Faculty of Pharmacy, Université de MontréalJacques Turgeon PhD, Director, Centre de Recherche du CentreHospitalier de l’ Université de Montréal; Professor of Pharmacy, Uni-versité de MontréalCara Tannenbaum MD MSc, Associate Professor of Medicine andPharmacy, Université de MontréalCorrespondence: Dr. Tannenbaum, [email protected]/Online Access: www.theannals.com/cgi/reprint/aph.1R621
Conflict of interest: Dr. Turgeon developed and currently marketsthe IntermedRx software used in this study. All other authors reportedno conflict of interest.
Financial support: This study was funded by the Michel-SaucierEndowed Chair in Geriatric Pharmacology, Health and Aging. Thesponsor had no role in the conduct, analysis, or interpretation of thestudy results.
© 1967-2013 Harvey Whitney Books Co. All rights reserved. No partof this document may be reproduced or transmitted in any form orby any means without prior written permission of Harvey WhitneyBooks Co. For reprints of any article appearing in The Annals, pleasecontact [email protected]
References
1. Huang SM, Strong JM, Zhang L, et al. New era in drug interaction evalu-ation: US Food and Drug Administration update on CYP enzymes, trans-porters and the guidance process. J Clin Pharmacol 2008;48:662-70.
2. Shimada T, Yamazaki H, Mimura M, Inui Y, Guengerich FP. Interindividualvariations in human liver cytochrome P-450 enzymes involved in the oxi-dation of drugs, carcinogens and toxic chemicals: studies with liver micro-somes of 30 Japanese and 30 Caucasians. J Pharmacol Exp Ther 1994;270:414-23.
3. Shapiro LE, Shear NH. Drug interactions: proteins, pumps, and P-450s.J Am Acad Dermatol 2002;47:467-84.
4. Mann HJ. Drug-associated disease: cytochrome P450 interactions. CritCare Clin 2006;22:329-45.
5. Zhang L, Xu N, Xiao S, et al. Regulatory perspectives on designing phar-macokinetic studies and optimizing labeling recommendations for pa-tients with chronic kidney disease. J Clin Pharmacol 2012;52:79S-90S.
6. International Conference on Harmonisation. E7(R1): studies in support ofspecial populations: geriatrics. www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E7/Q_As/E7R1_Final_Concept_Paper.pdf (accessed 2012 Sept 24).
7. Abarca J, Colon LR, Wang VS, et al. Evaluation of the performance ofdrug-drug interaction screening software in community and hospitalpharmacies. J Manag Care Pharm 2006;12:383-9.
8. Sweidan M, Reeve JF, Brien JA, et al. Quality of drug interaction alertsin prescribing and dispensing software. Med J Aust 2009;190:251-4.
9. Lapane KL, Waring ME, Schneider KL, et al. A mixed method study ofthe merits of e-prescribing drug alerts in primary care. J Gen Intern Med2008;23:442-6.
10. Magnus D, Rodgers S, Avery AJ. GPs’ views on computerized drug inter-action alerts: questionnaire survey. J Clin Pharm Ther 2002;27:377-82.
11. Zakrzewski-Jakubiak H, Doan J, Lamoureux P, Singh D, Turgeon J, Tan-nenbaum C. Detection and prevention of drug-drug interactions in the hos-pitalized elderly: utility of a new cytochrome p450–based software. Am JGeriatr Pharmacother 2011;9:461-70. doi: 10.1016/j.amjopharm.2011.09.006.
12. Turgeon J. InterMED -Rx. Harmony and optimal therapy in the use ofmedication. http://ws-ddi.intermed-rx.ca/ (accessed 2012 Jul 16).
13. US Food and Drug Administration. Guidance for industry on drug interac-tion studies—study design, data analysis, implications for dosing, and label-ing recommendations, February 2012. www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm292362.pdf(accessed 2012 Jun 8).
14. European Medicines Agency. Committee for medicinal products for humanuse. Guideline on the investigation of bioequivalence. www.ema.europa.eu/
330 n The Annals of Pharmacotherapy n 2013 March, Volume 47 theannals.com
J Doan et al.
at UZH Hauptbibliothek / Zentralbibliothek Zürich on July 7, 2014aop.sagepub.comDownloaded from

docs/en_GB/document_library/Scientific_guideline/2010/01/WC500070039.pdf (accessed 2011 Jun 8).
15. Birkett DJ. Generics—equal or not? Australian Prescriber 2003;26(4):85-7. 16. The Pharmaceutical Press. Stockley’s drug interactions. www.medicines
complete.com/mc/stockley/current/ (accessed 2010 Sept 1).17. Micromedex. Thomson Reuters. www.thomsonhc.com/home/dispatch
(accessed 2010 Sept 1).18. Hansten PD, Horn JR, eds. Drug interactions analysis and management.
St. Louis, MO: Wolters Kluwer Health, Inc., 2010.19. Fleiss JL, Levin B, Cho Paik M, eds. Statistical methods for rates and
proportions. 3rd ed. New York: John Wiley & Sons, 2003.20. Davies SJ, Eayrs S, Pratt P, Lennard MS. Potential for drug interactions
involving cytochromes P450 2D6 and 3A4 on general adult psychiatricand functional elderly psychiatric wards. Br J Clin Pharmacol 2004;57:464-72.
21. Mulder H, Heerdink ER, van Iersel EE, Wilmink FW, Egberts ACG.Prevalence of patients using drugs metabolized by cytochrome P4502D6 in different populations: a cross-sectional study. Ann Pharmacother2007;41:408-13. doi: 10.1345/aph.1H482
22. Zhou SF. Polymorphism of human cytochrome P4502D6 and its clinicalsignificance: part II. Clin Pharmacokinet 2009;48:761-804. doi: 10.2165/11318070-000000000-00000
23. Hines LE, Murphy JE. Potentially harmful drug-drug interactions in theelderly: a review. Am J Geriatr Pharmacother 2011;9:364-77. doi: 10.1016/j.amjopharm.2011.10.004
24. Mallet L, Spinewine A, Huang A. The challenge of managing drug inter-actions in elderly people. Lancet 2007;370:185-91.
25. Hines LE, Malone DC, Murphy JE. Recommendations for generating,evaluating, and implementing drug-drug interaction evidence. Pharma-cotherapy 2012;32:304-13. doi: 10.1002/j.1875-9114.2012.01024
26. Gallagher P, Barry P, O’Mahony D. Inappropriate prescribing in the el-derly. J Clin Pharm Ther 2007;32:113-21.
27. McKibbon KA, Lokker C, Handler SM, et al. The effectiveness of inte-grated health information technologies across the phases of medicationmanagement: a systematic review of randomized controlled trials. J AmMed Inform Assoc 2012;19:22-30.
28. Calabretto J-P,Warren J, Bird L. Pharmacy decision support: where is it?A systematic literature review. Int J Pharm Pract 2005;13:157-64. doi: 10.1211/ijpp.13.3.0001
EXTRACTO
Prevalencia y Riesgo Potencial de Interacciones MedicamentosasMediadas por el Citocromo P450 en Pacientes AncianosPolimedicados Hospitalizados
J Doan, H Zakrzewski-Jakubiak, J Roy, J Turgeon, C Tannenbaum
Ann Pharmacother 2013;47:324-32.
INTRODUCCIÓN: A medida que se incrementan las tasas de polifarmacia ylos tratamientos farmacológicos se hacen más complejos, crece lapreocupación por las potenciales interacciones medicamentosasmediadas por el citocromo P450 (pCYP450-DDI) en las personasmayores.
OBJETIVO: El propósito de este estudio fue determinar la prevalencia delas pCYP450-DDIs en personas mayores polimedicadas hospitalizadasy analizar la relación entre el número de medicamentos dispensados y laprobabilidad de pCYP450-DDIs en esta población de alto riesgo.
MÉTODOS: Se realizó un estudio prospectivo de cohortes de 16 semanasde duración entre los nuevos pacientes, de 65 años o más, polimedicados(>5 medicamentos) que ingresaron en un hospital comunitario. Seanalizaron los perfiles de medicación de estos pacientes con un nuevoprograma informático específico para analizar interacciones mediadaspor el citocromo entre varios medicamentos. Se determinó laprevalencia de pCYP450-DDIs. La probabilidad de una pCYP450-DDIse calculó en función del número de medicamentos dispensados
utilizando la regresión de Poisson ajustada para edad y sexo. Se utilizó eltest de Wilcoxon y Mann–Whitney para comparar los resultadosobtenidos con el programa específico empleado y los logrados con unprograma estándar para detectar pCYP450-DDIs entre dosmedicamentos. Se registraron las decisiones de recomendar ajustes en lamedicación que tomaron los farmacéuticos basándose en la probabilidadde pCYP450-DDIs.
RESULTADOS: La prevalencia de pCYP450-DDIs detectada entre laspersonas mayores polimedicadas fue del 80% (n = 275). La probabilidadde una pCYP450-DDI fue del 50% para los que tomaban de 5 a 9fármacos, 81% con de 10 a 14 fármacos, 92% con 15 a 19 y 100% conmás de 20. La adición de cada nuevo fármaco en un tratamiento con 5fármacos incrementa el riesgo de una pCYP450-DDI en 2% después deajustar por edad y sexo (OR 1.12, 95% IC 1.09-1.14). El programautilizado identificó media de 3 (95% IC 2.5-3.5) pCYP450-DDIs máspor paciente que las detectadas utilizando el programa estándar queanaliza los medicamentos de dos en dos. Los farmacéuticosseleccionaron a los pacientes para realizar ajustes de tratamiento o paramonitorización clínica estrecha en el 23% de los casos.
CONCLUSIONES: La prevalencia de pCYP450-DDIs es alta en lospacientes geriátricos polimedicados. El riesgo de interaccionesmedicamentosas aumenta con el número de medicamentos dispensados.La decisión farmacéutica de intervenir por una pCYP450-DDI dependede su criterio clínico además de los resultados que indiquen losprogramas informáticos de interacciones, pero puede verse facilitada conuna herramienta que permita valorar las pCYP450-DDI entre múltiplesmedicamentos simultáneamente.
Traducido por Juan del Arco
RÉSUMÉ
Prévalence et Risques d`Interactions Médicamenteuses Potentielles liéesaux Cytochromes P450 chez les Patients Hospitalisés âgés etPolymédicamentés
J Doan, H Zakrzewski-Jakubiak, J Roy, J Turgeon, C Tannenbaum
Ann Pharmacother 2013;47:324-32.
MISE EN CONTEXTE: Étant donné qu’il y a une augmentation dupourcentage de personnes agées polymédicamentées et de complexitédes traitements médicamenteux, le risque d’interactions potentiellesentre médicaments liées aux cytochromes P450 (IMMp-CYP450)devient une préoccupation clinique plus importante en gériatrie.
OBJECTIF: Le but de l’étude était de déterminer la prévalence des IMMp-CYP450 chez des patients hospitalisés âgés et polymédicamentés, ainsiqu’analyser la relation entre le nombre de médicaments servis et laprobabilité IMMp-CYP450 au sein de cette population à haut risque.
MÉTHODE: Une étude prospective de cohorte de 16 semainesconsécutives a été menée auprès de patients de 65 ans ou plus,polymédicamentés (plus de 5 médicaments au profil) et nouvellementadmis au sein d’un hôpital communautaire. Les profils médicamenteuxde ces patients ont été analysés à l’aide d’un nouveau logiciel dedétection d’interactions multiples liées au CYP450. La prévalence desIMMp-CYP450 a été déterminée. La probabilité des IMMp-CYP450 aété calculée en fonction de la quantité de médicaments servis à l’aided’une régression de Poisson multivariée ajustée pour l’âge et le sexe. Laperformance comparative du logiciel d’analyses multiples desinteractions liées au CYP450 par rapport à la performance d’un logicield’analyse conventionnel (analyse bilatérale entre 2 médicaments) a étéévaluée à l’aide du test de la somme des rangs Wilconxon-Mann-Whitney. Les décisions des pharmaciens de recommander uneréévaluation des traitements basés sur les probabilités des IMMp-CYP450 ont été colligées.
RÉSULTATS: La prévalence des IMMp-CYP450 détectées chez des adultesâgés polymédicamentés était de 80% (n = 275). La probabilité d’uneIMMp-CYP450 était de 50% pour les personnes dont le profil incluait 5-9 médicaments, 81% si le profil incluait 10-14 médicaments, 92% si leprofil incluait 15-19 médicaments et 100% si le profil incluait 20médicaments ou plus. L’addition de chaque nouveau médicament à unprofil médicamenteux de 5 médicaments a conféré 12% d’augmentationdu risque d’une IMMp-CYP450 après ajustement pour l’âge et le sexe(rapport de cotes 1.12; IC 1.09-1.14). Le logiciel d’analyse multiples d’
CYP450-Mediated Drug-Drug Interactions in Older Hospitalized Patients
The Annals of Pharmacotherapy n 2013 March, Volume 47 n 331theannals.com at UZH Hauptbibliothek / Zentralbibliothek Zürich on July 7, 2014aop.sagepub.comDownloaded from

IMMp-CYP450 a identifié une augmentation médiane de 3 IMMp-CYP450 par patient comparativement au logiciel conventionnel. Lespharmaciens ont décidé d’ajuster la posologie ou d’effectuer unmonitorage étroit dans 23% des cas.
CONCLUSIONS: La prévalence des IMMp-CYP450 est élevée au sein de lapopulation gériatrique polymédicamentée. Le risque d’interactionsmédicament-médicament augmente en fonction de la quantité demédicaments servis. La décision d’intervenir des pharmaciens est baséesur le jugement clinique et sur les outils informatiques disponibles quigénèrent des alertes. Or, un outil qui peut analyser simultanément demultiples IMMp-CYP450 pourrait faciliter cette prise de décision.
Traduit par J Roy, H Zakrzewski-Jakubiak
332 n The Annals of Pharmacotherapy n 2013 March, Volume 47 theannals.com
J Doan et al.
at UZH Hauptbibliothek / Zentralbibliothek Zürich on July 7, 2014aop.sagepub.comDownloaded from