Embed Size (px)
Citation preview

Prevalence of Developmental and Inflammatory Lesions in Nonmolar First-Trimester Spontaneous Abortions
RAYMOND W, REDLINE, MD, MICHAEL ZARAGOZA, AND TERRY HASSOLD, PHD
The management of patients with first-trimester spontaneous abortions is handicapped by two problems: difficulty in recognizing conceptions that abort because of abnormal karyotypes and an incomplete understanding of what causes abortions with normal karyotypes. Our goals in this study were to define features useful in distinguishing normal from abnormal karyotype and to identify pathological processes contributing to abortions with a normal karyotype. The study population consisted of 668 well-characterized first-trimester spontaneous abortions derived from a larger study of 1,054 consecutively karyotyped spontaneous abortions. Clinical fac- tors increased in specimens with normal karyotype were maternal age younger than 20 years (P = .0003) and autoimmune markers (P = .0474). Developmental features associated with abnormal karyo- type were developmental stage less than 6 weeks (P = .0017), hy- dropic villi greater than 1 mm (P = .0004), and villi with two or more dysmorphic features (P = .0001). Developmental stage greater than 11.5 weeks was increased with normal karyotype (P = .0001). Histo- logical features increased in specimens with a normal karyotype were
Spon taneous abor t ions are i m p o r t a n t causes o f reproduc t ive loss tha t are poor ly u n d e r s t o o d and diffi- cult to treat. 1-5 O n e p r o b l e m limiting progress in this area is the difficulty in subclassifying pat ients into appropr ia te t r e a tmen t groups. T he first and mos t funda- menta l dis t inct ion be tween pa t ien t g roups is karyotype, yet it is no t practical to karyotype all abor t ion speci- mens. Conceptuses with a b n o r m a l karyotypes are intrin- sically a b n o r m a l and have little o r no chance o f reach- ing term. Those with n o r m a l karyotype abor t fo r a variety o f reasons, i nc lud ing n o n c h r o m o s o m a l anoma- lies, exposure to teratogens, unde r ly ing ma te rna l dis- ease, o r failure o f the m o t h e r to a c c o m m o d a t e the fetal allograft. Major progress in p reven t ing spon t aneous abor t ion is unlikely until these latter processes are clearly d is t inguished a nd be t te r unde r s tood .
We analyzed data f r o m a large popula t ion-based study o f 1,054 consecutively ka ryo typed spon t aneous abor t ions access ioned in ou r d e p a r t m e n t over a 43- m o n t h per iod. O u r goals were to d e t e r m i n e the preva- lence, significance, a nd predict ive value o f specific clinical and pa tho logica l factors in karyotically def ined subsets o f abort ions . Par t icular emphasis was p laced on
From the Departments of Pathology and Genetics, Case Western Reserve, Cleveland, OH. Accepted for publication October 13, 1998.
Supported by a grant from the National Institutes of Health (R01 HD21341).
Address correspondence and reprint requests to Raymond W. Redline, MD, Department of Pathology, University Hospitals Health System, University Hospitals of Cleveland, 11100 Euclid Ave, Cleve- land, OH 44106.
Copyright © 1999 by W.B. Saunders Company 0046-8177/99/3001-0017510.00/0
93
chronic intervillositis (P = .0003), increased perivillous fibrin deposi- tion with intermediate trophoblast (P = .0006), decidual plasma cells (P --- .0040), deciduitis without plasma cells (P = .0660), and chronic villilis (P = .1581). Overall, 19% of samples with a normal karyotype versus 8% with abnormal karyotype had one or more of these findings (P < .0001). Autoimmune markers, chronic intervillositls, and in- creased perivillous fibrin with intermediate trophoblast all had positive predictive values greater than 85% for normal karyotype, whereas dysmorphic villi had a positive predictive value of 90% for abnormal karyotype. Patients with recurrent spontaneous abortion and normal karyotype were more likely to have one or more of the histological features listed above (31%) than patients with normal karyotype and no prior abortions (13%) and patients with recurrent abortion and abnormal karyotype (11%). HUM PATHOL 30:93-100. Copyright © 1999 by W.B. Saunders Company
Key words: chromosomal anomalies, chronic intervillositis, periv- illous fibrin, plasma cells, recurrent abortion.
identifying pat terns dist inguishing patients with ch romo- somally n o r m a l abor t ions and a his tory o f r e c u r r e n t miscarriage.
MATERIALS AND METHODS
Study Population The Case Western Reserve University Spontaneous Abor-
tion Survey was a population-based study of 1,054 consecu- tively karyotyped spontaneous abortions of 20 weeks of gesta- tion or less accessioned in the Pathology Department of University Hospitals of Cleveland over a 43-month period from August 20, 1993 to March 26, 1997. 6 University hospitals and its affiliates serve a well-defined multiracial population of private and staff patients from the Eastern Cuyahoga County region. All patients in the system with threatened, incomplete, or missed abortions had curettage performed in the clinics, outpatient department, or operating rooms of the hospital, and all of these specimens were submitted to Pathology. Specimens were examined before fixation by a single patholo- gist (R.W.R.) and a trained technician, who separated the tissue into fetal, villous, and endometrial fractions. All speci- mens had three or more tissue blocks submitted for paraffin embedding, after which routine hematoxylin and eosin-stained slides were prepared. One slide corresponded to the tissue sub- mitted for karyotype (exclusively villous), and the remaining slides contained a mixture of fetal, villous, and maternal tissues.
Cytogenetics Villous tissue was processed by standard methods for
karyotypic analysis. Cells harvested after 1 to 3 weeks of culture were stained for standard Q banding, and 10 or more cells per culture were analyzed for most cases. Mosaicism was defined as two or more identical nonmodal cells amongst the 10 or more cells analyzed. Karyotype was successful in 832 of

HUMAN PATHOLOGY Volume 30, No. 1 (January 1999)
1,054 cases (79%), 778 of which aborted in the first trimester of pregnancy (earlier than 14 weeks developmental age). The following cases were excluded: complete and partial moles (n = 7 and 21, respectively), samples with insufficient villous tissue for histological analysis (n = 60), and samples with 46,XX karyotype having more than 20% maternal tissue on the slide, which corresponded to the tissue submitted for karyotype (n = 22). Molar gestations were excluded because their unique phenotype made them difficult to compare with nonmolar conceptuses. Phenotypic characterization of our molar cases has been previously published. 6~ The remaining 668 cases (86% of successfully karyotyped first-trimester abor- tions) formed the basis for this study. The 350 cases with abnormal karyotypes were separated into five groups: nonmo- saie single and double trisomies (n = 215 and 10, respec- tively), nonmolar triploidy (n = 43), monosomy X (n = 15), tetraploidy (n = 15), and others (n = 33; nine mosaic triso- mies, nine simple translocations, two autosomal monosomies, and 13 cases with a variety of other abnormalities including marker chromosomes and complex karyotypes),
Clinical Features Maternal age was available in all cases. Obstetric data
(previous spontaneous abortions, preterm deliveries, and infertility problems) and medical history (diabetes, chronic hypertension, autoimmune markers) were obtained from requisitions accompanying study specimens. Relevant data was provided with most specimens but analyses stratified for history of previous spontaneous abort ion were limited to cases in which the presence or absence of prior spontaneous abortions was explicitly specified.
Pathological Analysis Pathological features were assessed by a single pathologist
(R.W.R.). To obtain an estimate of intraobserver variation, we compared the final evaluation of cases done after completion of the study with an earlier set of observations per formed on 100 cases early in the specimen collection phase of the study.
Developmental Phenotype Assignment of developmental stage (<6.0 weeks, 6.0 to
11.5 weeks, and 11.5 to i4.0 weeks from the last menstrual period) was based on a staged set of elective abort ion specimens available in our laboratory, the diameter of the chorionic sac, and a variety of other developmental criteria that have previously been described in detail. 6 The stages used co r r e spond to primary vasculogenesis and secondary villous formation (<6.0 weeks),9,10 branching of primitive mesenchy- mal villi (6.0 to 8.5 weeks),11 presence of immature intermedi- ate stem villi and apposition of amnion to chorion (8.5 to 11.5 weeks), 9,11 and establishment of the definitive placenta with polarization of the chorion laevae and complete maternal arterial perfusion of the intervillous space (>11.5 weeks);9,12 The relationship between our assessment of developmental stage and clinically estimated gestational age has been dis- cussed previously. 6 For the purposes of this study, we com- bined the 6.0- to 8.5- and 8.5- to l l .5-week stages, which are the most difficult to distinguish from one another, into a single group.
Spontaneous abortions also were classified into three major groups based on criteria developed by Rushton. is In brief, these groups were defined as follows: group 1--anembry- onic abortions ("blighted ova") with rare or absent fetal
vessels containing a mixture of hydropic and hyalinized villi; group 2--involuting abortions with numerous fetal vessels +- fetal tissue; and group 3--fresh abortions with well-preserved villi _+ fetal tissue. Group 3 cases were generally associated with hemorrhagic or necrotic gestational endometr ium and a clinical history of threatened, complete, or incomplete abor- tion. The presence or absence of fetal tissue was defined by histology and excluded extraembryonic fetal structures such as umbilical cord, yolk sac, amnion, or circulating fetal blood cells. Although not a specific focus of this study, many first-trimester cases with abnormal karyotypes had embryonic anomalies, as did a number of second-trimester cases with normal karyotype. Only three cases of first-trimester abortion with normal karyotype had anomalies (one club foot, one nodular disorganized embryo, one dysmorphic facies). Dys- morphic villi were defined by the presence of at least two of the following four elements: irregular villous contour, mul- tiple villous trophoblast inclusions, villous stromal karyomegaly (nucleus more than 3 times larger than adjacent nuclei), and mazelike branching fetal vascular pattern. 6 Hydropic villi were defined as round to oval edematous villi measuring larger than 1 mm in maximum diameter as measured on the microscopic slide.
Histological Features (Data From Kaplan et a114 and Redline 15)
Chronic villitis (vi!litis of unknown cause) was defined as lymphohistiocytic infiltration of villous stroma with fibrosis or necrosis and negative bacterial stains. Chronic intervillosifis cases lacked villitis and were separated into two groups: diffuse chronic intervillositis consisting of a monomorphic popula- tion of monocyte-macrophages diffusely packing the intervil- lous space with or without accompanying fibrin and focal intervillositis consisting of a less extensive and mixed inflam- matory infiltrate, including lymphocytes, monocyte-macro- phages, and neutrophils: Cases with mixed inflammatory infiltrates were stained for bacteria and spirochetes using silver impregnation techniques as previously discussed. 16 Dif- fuse perivillous fibrin with intermediate trophoblast was defined as a uniform near-total obliteration of the intervillous space by a combination of inflammatory cells and fibrin-like material, with the latter predominating. Controversy exists regarding the exact nature of this fibrin-like material. It may represent true fibrin, extracellular matrix proteins, or a combination of both. For the purposes of clarity, it is referred to as fibrin in this report. This fibrin is characteristically heavily infiltrated by intermediate trophoblast and overlaps with maternal floor infarction as defined for second- and third-trimester placentas. Many of the patients with perivillous fibrin in our study also had either chronic intervillositis or chronic villitis. Decidual plasma cells were identified in the maternal endomyometr ium by typical cytological features. Deciduifis (other) consisted of clusters of mononuclear cells, often surrounding decidual arteries, and subjectively greater in extent than that normally seen with first-trigAester gesta- tion.
Statistical Analysis Chi-square analysis or Fisher's exact tests were used for
group data. Significance was set at P = .05. Positive and negative predictive values of clinical and pathological vari- ables for predicting karyotype were calculated as true positives/ total positives and true negatives/total negatives, respectively,
94

SPONTANEOUS ABORTION AND KARYOTYPE (Redline et al)
and a positive predictive value of 85% or greater was arbi- trarily chosen as useful.
RESULTS
Clinical History
Normal karyotype was more f requent in the sponta- neous abort ion specimens of mothers younger than 20 years of age (P = .0003) and in those with auto immune markers ( P = .0474) (Tables 1 and 2). The specific au to immune markers in the six patients with normal karyotype were frank systemic lupus erythematosus (two patients), positive antinuclear antibody (three patients), and ant iphospholipid antibodies (one pa- tient). Patients with a history of prior spontaneous abort ion were more likely to have a normal karyotype (5.0% v 2.6%) and age greater than 35 was more common in patients with an abnormal karyotype (35% v 24%), but nei ther finding reached statistical signifi- cance. The increase in patients older than 35 years of age in cases with abnormal karyotype was attributable to trisomic cases (43% over 35 years of age for trisomy v 24% for normal karyotype and 26% for abnormal karyotypes o ther than trisomy, P < .0001). Adverse obstetric factors o ther than pr ior spontaneous abort ion (infertility, pr ior p re te rm delivery, or uterine malforma- tion) and a history of ei ther diabetes or essential hypertension were u n c o m m o n and equivalent in the two groups. Auto immune markers had a positive predic- tive value of 86% for normal karyotype, whereas the positive predictive value of o ther clinical variables was poor. A general finding applicable to all variables studied was that absence of a feature had little or no predictive value (ie, low predictive value of the negative, Table 2).
Developmental Features
Normal karyotype was significantly more common in abort ion specimens of late developmental stage (>11.5 weeks, P = .0001). Abnormal karyotype was associated with early developmental stage (<6 weeks,
P = .0017), dysmorphic villi ( P = .0001), and villous hydrops (>1 mm diameter, P = .0004) (Tables 2 and 3). Early developmental stage was most common with trisomy and tetraploidy. Dysmorphic and hydropic villi were increased in all subgroups of chromosomal abnor- mality. The association of dysmorphic villi with abnor- mal karyotype was equally strong after exclusion of triploid cases (P < .0001, 87% positive predictive value). The propor t ion of cases in each Rushton group (see Materials and Methods) and the presence or absence of fetal tissue by histological examination differed little in specimens with normal versus abnormal karyotype. Of the developmental features evaluated, only the pres- ence of dysmorphic villi had a high positive predictive value (90%) for abnormal karyotype.
Idiopathic Chronic Inflammation and Fibrin Deposition
The presence of one or more histological abnor- malities indicative of chronic inflammation or fibrin deposition was significantly increased in abortions with a normal karyotype (19% v 8%, P < 0.0001, Table 4). Individual lesions significantly increased with normal karyotype were chronic intervillositis, increased perivil- lous fibrin with intermediate trophoblast, and decidual plasma cells. Deciduitis without plasma cells (P = .0660) and chronic villitis (P = .1581) were increased but did not reach statistical significance. The predictive value of a positive result was highest for chronic intervillositis (93%) and increased perivillous fibrin with intermedi- ate trophoblast (85%) (Table 2). These two lesions are shown in Figure 1. Finally, in the limited number of cases in which pr ior spontaneous abort ion status was known (n = 50), the prevalence of one or more histo- logical abnormalities was 31% in recur ren t aborters with normal karyotype versus 13% in first-time aborters with a normal karyotype, 11% in recurrent aborters with an abnormal karyotype, and 0% in first-time aborters with an abnormal karyotype (Table 4). These results did not achieve statistical significance because of small numbers.
TABLE ]. Clinical History of Women With Nonmolar First-Trimester Spontaneous Abortions by Karyotype
Maternal Age (y) Clinical History
Karyotype N <20 20-35 >35 Previous Obstetric Hypertension Autoimmune
SAB* (Other) * or Diabetes Markers
Normal 46,XY 145 18 101 26 46,XX 173 21 103 49 Total 318 39 (12)t 204 (64) 75 (24)
Abnormal Trisomy 225 5 124 96 Triploidy 43 4 35 4 Monosomy X 34 5 22 6 Tetraploidy 15 0 11 4 Others 33 1 18 13 Total 350 15 (4) 212 (61) 123 (35)
6 2 1 3 10 4 4 3 16 (5) 6 (2) 5 (2) 6 (2)
7 4 3 1 1 1 0 0 0 0 0 0 0 0 0 0 1 2 1 0 9 (3) 7 (2) 4 (1) 1 (<1)
*Obstetric (other) = infertility, previous preterm delivery, or uterine malformation. tNumber of patients (percentage of total). Abbreviation: SAB, spontaneous abortion.
95
HUMAN PATHOLOGY Volume 30, No. 1 (January 1999)
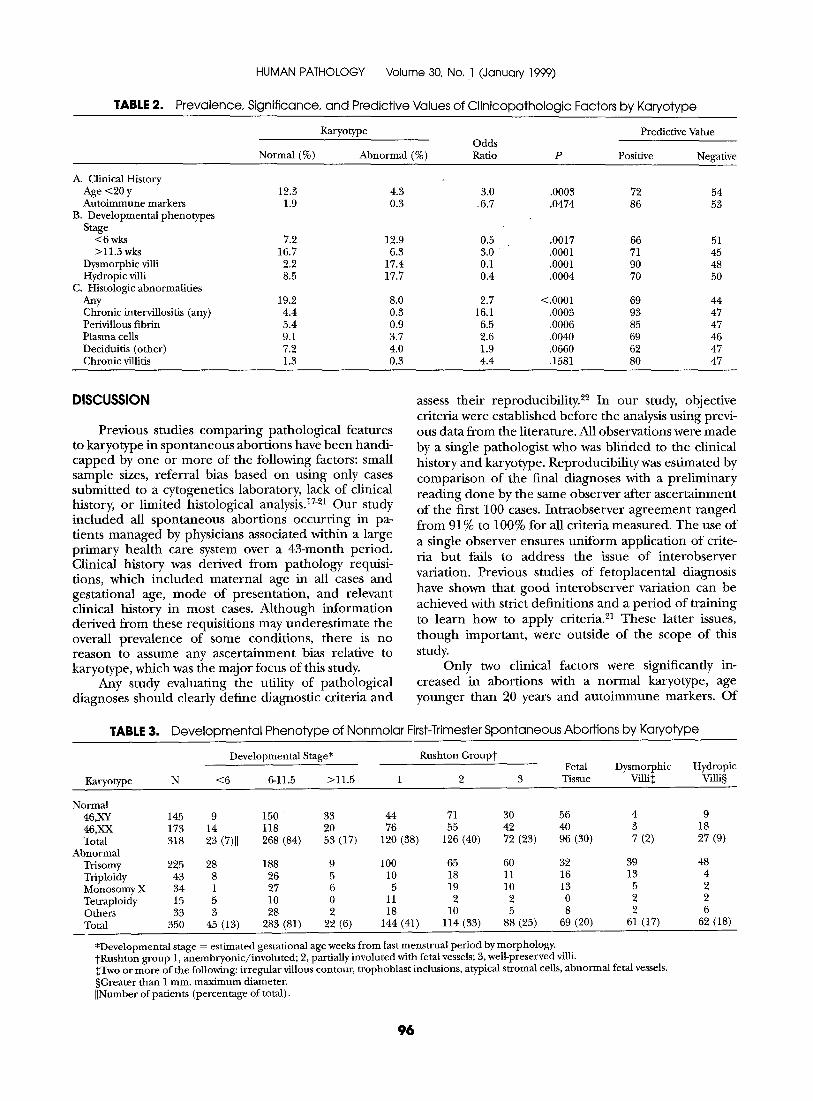
TABLE 2. Prevalence, Significance, and Predictive Values of Clinicopathologic Factors by Karyotype
Karyotype Predictive Value Odds
Normal (%) Abnormal (%) Ratio P Positive Negative
A. Clinical History Age <20 y 12.3 4.3 3.0 Autoimmune markers 1.9 0.3 .6.7
B. Developmental phenotypes Stage
<6 wks 7.2 12.9 0.5 >11.5 wks 16.7 6.3 3.0
Dysmorphic villi 2.2 17.4 0.1 Hydropic villi 8.5 17.7 0.4
C. Histologic abnormalities Any 19.2 8.0 2.7 Chronic intervillositis (any) 4.4 0.3 16.1 Perivillous fibrin 5.4 0.9 6.5 Plasma cells 9.1 3.7 2.6 Deciduitis (other) 7.2 4.0 1.9 Chronic villitis 1.3 0.3 4.4
.0003 72 54
.0474 86 53
.0017 66 51
.0001 71 45
.0001 90 48
.0004 70 50
<.0001 69 44 .0003 93 47 .0006 85 47 .0040 69 46 .0660 62 47 .1581 80 47
DISCUSSION
Previous studies comparing pathological features to karyotype in spontaneous abortions have been handi- capped by one or more of the following factors: small sample sizes, referral bias based on using only cases submitted to a cytogenefics laboratory, lack of clinical history, or limited histological analysis. 17-21 Our study included all spontaneous abortions occurring in pa- tients managed by physicians associated within a large primary health care system over a 43-month period. Clinical history was derived from pathology requisi- tions, which included maternal age in all cases and gestafional age, mode of presentation, and relevant clinical history in most cases. Although information derived from these requisitions may underestimate the overall prevalence of some conditions, there is no reason to assume any ascertainment bias relative to karyotype, which was the major focus of this study.
Any study evaluating the utility of pathological diagnoses should clearly define diagnostic criteria and
assess their reproducibility. 22 In our study, objective criteria were established before the analysis using previ- ous data from the literature. All observations were made by a single pathologist who was blinded to the clinical history and karyotype. Reproducibility was estimated by comparison of the final diagnoses with a preliminary reading done by the same observer after ascertainment of the first 100 cases. Intraobserver agreement ranged from 91% to 100% for all criteria measured. The use of a single observer ensures uniform application of crite- ria but fails to address the issue of interobserver variation. Previous studies of fetoplacental diagnosis have shown that good interobserver variation can be achieved with strict definitions and a period of training to learn how to apply criteriaY These latter issues, though important, were outside of the scope of this study.
Only two clinical factors were significantly in- creased in abortions with a normal karyotype, age younger than 20 years and autoimmune markers. Of
TABLE 3. Developmental Phenotype of Nonmolar First-Trimester Spontaneous Abortions by Karyotype
Developmental Stage* Rushton Groupt Fetal Dysmorphic
Karyotype N <6 6-11.5 >11.5 1 2 3 Tissue Villi++
Normal 46,XY 145 9 150 33 44 71 30 46,XX 173 14 118 20 76 55 42 Total 318 23 (7)]] 268 (84) 53 (17) 120 (38) 126 (40) 72 (23)
Abnormal Trisomy 225 28 188 9 100 65 60 Triploidy 43 8 26 5 10 18 11 Monosomy X 34 1 27 6 5 19 10 Tetraploidy 15 5 10 0 11 2 2 Others 33 3 28 2 18 10 5 Total 350 45 (13) 283 (81) 22 (6) 144 (41) 114 (33) 88 (25)
Hydropic Villi§
56 4 9 40 3 18 96 (30) 7 (2) 27 (9)
32 39 48 16 13 4 13 5 2 0 2 2 8 2 6
69 (20) 61 (17) 62 (18)
*Developmental stage = estimated gestational age weeks from last menstrual period by morphology. tRushton group 1, anembryonic/involuted; 2, partially involuted with fetal vessels; 3, well-preserved villi. ++Two or more of the following: irregular villous contour, trophoblast inclusions, atypical stromal cells, abnormal fetal vessels. §Greater than 1 mm. maximum diameter. ][Number of patients (percentage of total).
96
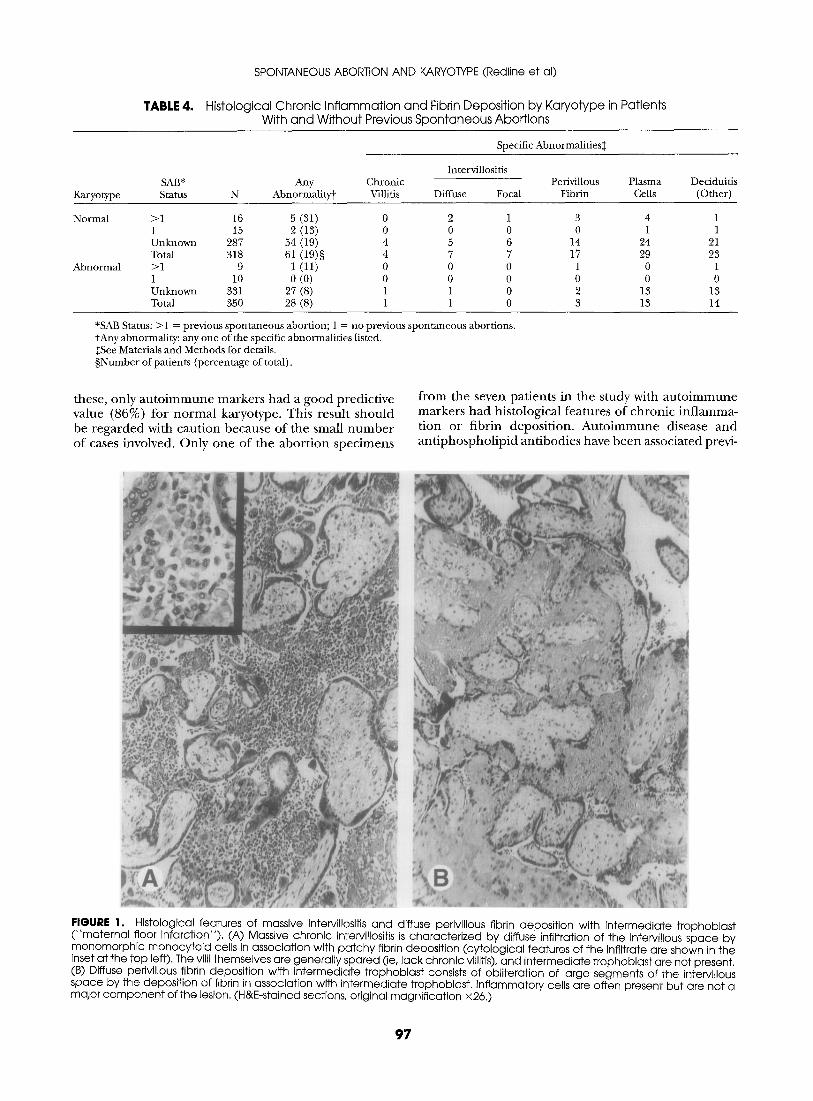
TABLE 4.
SPONTANEOUS ABORTION AND KARYOTYPE (Redline et al)
Histological Chronic Inf lammation and Fibrin Deposition by Karyotype in Patients With and Without Previous Spontaneous Abortions
Karyotype
Specific Abnormalities$
Intervillositis SAB* Any Chronic Perivillous Plasma Status N Abnormality~ Villitis Diffuse Focal Fibrin Cells
Deciduitis (Other)
Normal
Abnormal
>1 16 5 (31) 0 2 1 3 4 1 1 15 2 (13) 0 0 0 0 1 1 Unknown 287 54 (19) 4 5 6 14 24 21 Total 318 61 (19)§ 4 7 7 17 29 23 >1 9 l (11) 0 0 0 1 0 1 1 10 0 (0) 0 0 0 0 0 0 Unknown 331 27 (8) 1 1 0 2 13 13 Total 350 28 (8) 1 1 0 3 13 14
*SAB Status: >1 = previous spontaneous abortion; 1 = no previous spontaneous abortions. mAny abnormality: any one of the specific abnormalities listed. ++See Materials and Methods for details. §Number of patients (percentage of total).
these, only a u t o i m m u n e markers had a good predict ive value (86%) for n o r m a l karyotype. This resul t shou ld be r ega rded with cau t ion because of the small n u m b e r of cases involved. On ly one of the a b o r t i o n spec imens
f rom the seven pat ients in the study with a u t o i m m u n e markers had histological features of ch ron ic in f l amma- t ion or f ibr in deposi t ion . A u t o i m m u n e disease a n d a n t i p h o s p h o l i p i d an t ibodies have b e e n associated previ-
FIGURE 1. Histological features of massive intervillositis and diffuse perivillous fibrin deposition with intermediate trophoblast ("maternal floor infarction"). (A) Massive chronic intervillositis is characterized by diffuse infiltration of the intervillous space by monomorphic monocytoid cells in association with patchy fibrin deposition (cytological features of the infiltrate are shown in the inset at the top left). The villi themselves are generally spared (ie, lack chronic villitis), and intermediate trophoblast are not present. (B) Diffuse perivillous fibrin deposition with intermediate trophoblast consists of obliteration of large segments of the intervillous space by the deposition of fibrin in association with intermediate trophoblast. Inflammatory cells are often present but are not a major component of the lesion. (H&E-stained sections, original magnification x26.)
97

HUMAN PATHOLOGY Volume 30, No, 1 (January 1999)
ously with recurrent abortion, but karyotype data have not routinely been available. 2~-25
A number of clinical factors commonly thought to be predictive of karyotype were similar in the two groups. 2~3° Advanced maternal age was increased in the subset of cases with trisomy but not in the abnormal karyotype group as a whole. In part this may reflect a trend toward delayed childbearing resulting in a gen- eral increase in older mothers. Obstetric factors such as recurrent abortion and infertility and maternal medical conditions such as diabetes or hypertension also were not overrerpresented in either group. The finding that chromosomal abnormalities are not infrequent in pa- tients with recurrent abortion and infertility has been reported previously. 26,31 Possible explanations include genetic predisposition to abnormal gametogenesis or defects in the normal surveillance mechanisms that eliminate abnormal conceptuses at a stage before recog- nition of pregnancy. No good data exist to support either of these suggestions.
In our analysis of developmental features, we found that abortions with abnormal karyotype were more likely to occur at an early developmental age (<6 weeks), whereas those with normal karyotype were more likely to abort later (>11.5 weeks). There was considerable overlap between the two groups, and the ability of developmental age to predict karyotype was low. A second measure of developmental phenotype separates abortions into groups based on the timing of fetal /embryonic loss. is Group 1 abortions are anembry- onic gestations with changes suggesting either failure of embryonic development or very early embryonic death. Group 2 gestations show changes roughly paralleling those seen in intrauterine fetal deaths at later gesta- tions, and Group 3 abortions have changes suggesting very recent death. The proport ion of cases in each group was virtually identical for abortions with normal and abnormal karyotype. Previous data suggesting that groups 2 and 3 were more common in abortions with normal karyotype may be due to the inclusion of second-trimester abortions, which usually have a nor- mal karyotype and are virtually never anembryonic. Hydropic villi greater than 1 mm in diameter were significantly increased with abnormal karyotype, espe- cially in trisomic conceptuses, but approximately 10% of the normal karyotype group also had hydropic villi, and the predictive value of this feature was low.
The only developmental feature predictive of abnor- mal karyotype was villous dysmorphism. Dysmorphic villi were useful when present (17% with abnormal karyotype v 3% with normal karyotype), but most cases with chromosomal abnormalities lacked this feature. A standard definition of dysmorphic villi does not exist, but most observers would agree on some combination of irregular villous contour, trophoblast inclusions, atypical stromal cells, and an abnormal fetal vascular pattern. 17-22 These patterns tend to cluster together, and we required that at least two of the four criteria be present for diagnosis. Previous studies have found an association between dysmorphic villi and abnormal
karyotype, but some have argued that this relationship is entirely accounted for by the triploid subgroup. 2° In our study, dysmorphic villi were significantly associated with and strongly predictive of abnormal karyotype, even after the exclusion of triploid gestation. The specific karyotypes other than triploidy that most com- monly had dysmorphic villi in our study were trisomies 7, 8, 13, 16, and 18 and monosomy X (data not shown).
Finally, in what we consider to be the most impor- tant result of the study, we found that a group of partially overlapping histological findings indicative of chronic inflammation or perivillous fibrin deposition were significantly increased in patients with normal karyotype. These findings affected only a subgroup (19%) of cases and werepart icularly frequent in pa- tients with recurrent spontaneous abortion (31%). The increased prevalence of these findings in patients with previous abortions was limited to cases with a normal karyotype, arguing against nonspecific changes related to prior curettage. Chronic inflammation of the de- cidua was more common but less specific for normal karyotype than lesions of intervillous space and villous stroma, which were seen almost exclusively with normal karyotype. Although chronic inflammatory lesions have been previously reported in as many as 13% of first- trimester abortions, 17 to our knowledge only one previ- ous study has correlated these changes with karyotype. 19 This latter study identified chronic intervillositis and decidual perivasculitis as increased in chromosomally normal abortions. Chronic inflammation or fibrin depos- its in spontaneous abortions also could relate to non- chromosomal genetic defects in either the mother or fetus. Two recently described molecular defects that potentially could lead to early pregnancy losses associ- ated with chronic inflammation and fibrin deposition are abnormalities in tryptophan metabolism and factor V Leiden mutations. 32,3~
In our study, decidual inflammation was associated with normal karyotype only in the presence of plasma cells. Endometrial plasma cells are a well-recognized indicator of persistent antigenic stimulation in the uterus of both pregnant and nonpregnant patients. Patients with endometrial plasma cells often present with uterine bleeding and infertility, and they have an increased incidence of chronic villitis during preg- nancy. 1~,s4,35 Our finding of decidual plasma cells in patients with recurrent abortions correlates with a recent flow cytometric study that showed an increased proport ion of decidual B-lymphocytes in these pa- tients. ~6
Diffuse perivillous fibrin with intermediate tropho- blast, also known as maternal floor infarction, is strongly associated with recurrent reproductive failure but has usually been described at later gestational ages. 37 The term maternal floor infarction is unfortunate, because there is no evidence to suggest that the lesion has any relationship to ischemia or vascular occlusion. Patients with maternal floor infarction often have a history of prior first-trimester abortions. The underlying cause of maternal floor infarction is unknown, but an associa-
98

SPONTANEOUS ABORTION AND KARYOTYPE (Redline et al)
tion with maternal au to immune disease has been found in some studies. 38 The exact nature of the perivillous fibrin remains controversial and may vary f rom case to case. Most observers agree that it consists of some combinat ion of true fibrin and trophoblast-derived extracellular matrix products. 39
Idiopathic diffuse or massive chronic intervillositis has been repor ted in occasional patients with recur ren t abort ion and may represent an inappropriate immune response to trophoblast antigens. 4°,41 Intervillositis is believed to occur in association with increased local levels of tumor necrosis factor-alpha and gamma inter- feron. 41,42 Interestingly, both of these cytokines have been shown to increase the expression of leukocyte adhesion molecules on trophoblast in vitro. 43 Both cytokines are also markedly elevated in placental blood samples f rom women with placental malaria, which is also characterized by diffuse chronic intervillositis. 44 The eight patients with diffuse chronic intervillositis repor ted in this study are a subset of 14 patients that we have identified in our institution with this lesion. Eight of the 14 patients have a history of recur ren t spontane- ous abortion, and several of the others have a history of intrauterine growth retardation or second-trimester loss (unpublished results). None of the patients in our series have any indication of underlying infections as de te rmined by special stains, elevated white blood cell counts, or o ther clinical history.
To summarize our study, we found that abortion with normal karyotype occurs more frequently in young patients at late developmental stages. These abortions lack dysmorphic villi and are occasionally associated with maternal au to immune abnormalities. A distinct subgroup of specimens, many of whom are f rom pa- tients with recur ren t abortion, have histological indica- tors of chronic inflammation or fibrin deposition. Further investigation of these latter patients will be of interest to see whether they respond to various immuno- modulatory therapies currently under investigation such as intravenous immunoglobul in administration or pro- gesterone supplementation.
Acknowledgment. T h e au tho r s t h a n k D e b r a Ozan, Elise Milley, a n d L u A n n J u d i s for t echn ica l assistance.
REFERENCES
1. Bennett MJ, Edmonds DK: Spontaneous and recurrent abor- tion. Chicago, IL, Blackwell Scientific Publications, 1987
2. Stirrat GM: Recurrent miscarriage l: Definition and epidemi- ology. Lancet 336:673-675, 1990
3. Stirrat GM: Recurrent miscarriage II: Clinical associations, causes, and management. Lancet 336:728-733, 1990
4. Coulam CB: Epidemiology of recurrent spontaneous abor- tion. AmJ Reprod Immunol 26:23-27, 1991
5. HemminkiE: Treatment of miscarriage: Current practice and rationale. Obstet Gyneco191:247-253, 1998
6. Redline RW, Hassold T, Zaragoza MV: Prevalence of the partial molar phenotype in triploidy of maternal and paternal origin. HuM PATHOL 28:505-511, 1998
7. Keep D, Zaragoza M, Hassold T, et al: Very early complete hydatidiform mole. HUM PATHOL 27:708-713, 1996
8. Zaragoza MV, Keep D, Genest DR, et al: Early complete hydafidiform moles contain inner cell mass derivatives. Am J Med Genet 70:273-277, 1997
9. Hertig A. Human Trophoblast. Springfield, IL, CC Thomas, 1968, p 137
10. Kalousek DK, Neave C: Pathology of abortion, the embryo, and the previable fetus, in Wigglesworth JS, Singer DB (eds): Textbook of Fetal and Perinatal Pathology. Boston, MA, Blackwell Scientific Publications, 199l, pp 123-160
11. Benirschke K, Kaufmann P: Pathology of the Human Pla- centa (ed 3). NewYork, NY, Springer-Verlag, 1995, pp 28-33
12. Jaffe R, Jauniaux E, HustinJ: Maternal circulation in the first trimester human placenta: Myth or reality: Am J Obstet Gynecol 176:695-705, 1997
13. Rushton DI: The classification and mechanisms of spontane- ous abortion. Perspect Pediatr Pathol 8:269-287, 1984
14. Kaplan C, Lowell DM, Salafia C: College of American Pathologists Conference XIX on The Examination of the Placenta: Report of the Working Group on the Definition of Structural Changes Associated with Abnormal Function in the Maternal/Fetal/Placental Unit in the Second and Third Trimesters. Arch Pathol 115:709-716, 1991
15. Redline RW: Disorders of the placental parenchyma, in Lewis S, Perrin E (eds) : Pathology of the Placenta: Contemporary Issues in Surgical Pathology (ed 2). NewYork, NY, Churchill Livingston, 1998, pp 161-184
16. Redline RW: Recurrent villitis of bacterial etiology. Pediatr Pathol 6:995-1002, 1996
17. Ornoy A, Salamon-Arnon J, Ben-Zur Z, et al: Placental findings in spontaneous abortions and stillbirths. Teratology 24:243- 252, 1981
18. Novak R, et al: Histologic analysis of placental tissue in first trimester abortions. Pediatr Pathol 8:477-482, 1988
19. Salafia C, Maier D, Vogel C, et ah Placental and decidual histology in spontaneous abortion: Detailed description and correla- tions with chromosome number. Obstet Gyneco182:295-303, 1993
20. Van Lijnschoten G, ArendsJW, Leffers P, et al: The value of histomorphological features of chorionic villi in early spontaneous abortion for the prediction of karyotype. Histopathology 22:557-563, 1993
21. Genest GR, Roberts D, Boyd T, et al: Fetoplacental histology as a predictor of karyotype: A controlled study of spontaneous first trimester abortions. HUM PATHOL 26:201-209, 1995
22. Vanlijnschoten G, Arends JW, Delafuente, et al: Intra- observer and inter-observer variation in the interpretation of histologi- cal features suggesting chromosomal abnormality in early abortion specimens. Histopathology 22:25-29, 1993
23. Out HJ, Bruinse HW, Derksen RMWM: Anti-phospholipid antibodies and pregnancy loss: Review. Hum Reprod 6:889-897, 1991
24. Nayar R, Lage JM: Placental changes in a first trimester missed abortion in maternal systemic lupus erythematosus with antiphospholipid syndrome: A case report and review of the litera- ture. HUM PATHOL 27:201-206, 1996
25. Iijima T, Tada H, HidakaY, et ah Effects of autoantibodies on the course of pregnancy and fetal growth. Obstet Gyneco190:364-369, 1997
26. Cowchock FS, Gibas Z, Jackson LG: Chromosome errors as a cause of spontaneous abortion: The relative importance of maternal age and obstetric history. Fertil Steri159:1011-1014, 1993
27. Tulppala M, Paluosa T, Ramsay T, et al: A prospective study of 63 couples with a history of recurrent spontaneous abortion: Contrib- uting factors and outcome of subsequent pregnancies. Hum Reprod 8:774-770, 1993
28. Hakim RB, Gray RH, Zacur H: Infertility and early pregnancy loss. AmJ Obstet Gyneco1172:1510-1517, 1995
29. Coulam CB, Wagenknecht D, McIntyreJA, et al: Occurrence of other reproductive failures among women with recurrent spontane- ous abortion. AmJ Reprod Immunol 25:96-98, 1991
30. Miodovnik M, Lavin JR Knowles HC, et ah Spontaneous abortion among insulin-dependent diabetic women. Am J Obstet Gyneco1150:372-376, 1984
31. Coulam CB, Stephenson M, Stern U, et ah Immunotherapy
99

HUMAN PATHOLOGY Volume 30, No. 1 (January 1999)
for recurrent pregnancy loss: Analysis of results from clinical trials. AmJ Reprod Immuno135:352-359, 1996
32. Munn DH, Zhou M, Attwood JT, et al: Prevention of allogeneic fetal rejection by tryptophan metabolism. Science 281:1191- 1193, 1998
33. Ridker PM, Miletich JP, Buring JE, et al: Factor V Leiden mutation as a risk factor for recurrent pregnancy loss. Ann Intern Med 128:1000-1003, 1998
34. Rotterdam H: Chronic endometritis: A clinicopathologic study. Pathol Annu II:209-222, 1978
35. Czernobilsky B: Endometritis and infertility. Fertil Steril 30:119-130, 1978
36. Lachapelle MH, Miron P, Hemmings R, et al: Endometrial T, B, and NK cells in patients with recurrent spontaneous abortion: Altered profile and pregnancy outcome. J Immunol 156:4027-4034, 1996
37. Andres RL, Kuyper W, Resnik R, et al: The association of maternal floor infarction of tile placenta with adverse perinatal outcome. AmJ Obstet Gynecol 163:935-938, 1990
38. Mandsager NT, Bendon R, Mostello D, et al: Maternal floor
infarction of placenta: Prenatal diagnosis and clinical significance. Obstet Gyneco183:750-754, 1994
39. Frank HG, Malekzadefi F, Kertschanska S, et al: Immunohis- tochemistry of two different types of placental fibrinoid. Acta Anat 150:55, 1994
40. Jacques SM, Qureshi F: Chronic intervillositis of the pla- centa. Arch Pathol Lab Med 117:1032-1035, 1993
41. Doss BJ, Greene ME Hill J, et al: Massive chronic intervillosi- tis associated with recurrent abortions. HUM PATHOL 26:1245-1251, 1995
42. Hill JA, Melling GC, Johnson PM: Immunohistochemical studies of human uteroplacenta] tissues from first-trimester spontane- ous abortion. AmJ Obstet Gynecol 173:90-96, 1995
43. Xiao J, Garcia Lloret G, Winklerlowen B, et al: ICAM-1- mediated adhesion of peripheral blood monocytes to the maternal surface of placental syncytiotrophoblasts: Implications for placental villitis. AmJ Patho1150:1845-1860, 1997
44. Fried M, Muga RO, Misore AO, et al: Malaria elicits type 1 cytokines in the human placenta: IFN-y and TNF-a associated with pregnancy outcomes.J Immuno1160:2523-2530, 1998
100





























