Embed Size (px)
Citation preview

Nephrology 1998; 4, 101–104
Dialysis
Prevalence of hepatitis B and hepatitis C in haemodialysispatientsMARISA G SANTOS, ROMINA A DANGUILAN, ERNESTO T QUE, RENE P BALMACEDAAND BENITA S PADILLA
National Kidney and Transplant Institute, East Avenue, Quezon City, Philippines
Summary: The prevalence of hepatitis B surface antigen (HBsAg), hepatitis B exposure and antibodiesagainst the hepatitis C virus (anti-HCV) was assessed in 86 haemodialysis patients at the National Kidneyand Transplant Institute (NKTI) using the commercial radioimmunoassay and ortho HCV ELISA assay. Ofthe 86 patients included in the study, 42 were male with a mean age of 44.9 years and a mean duration ofdialysis of 2.4 years. Forty-four were female with a mean age of 48.4 years and a mean duration of dialysisof 2.3 years. Hepatitis B exposure was 57% and 12.8% of haemodialysis patients were positive for HBsAg,whereas 39.8% of patients were positive for anti-HCV. There was a significant correlation (P=0.00007)between anti-HCV positivity and the length of time on haemodialysis. However, there was no significantcorrelation found between the number of blood transfusions received and anti-HCV positivity. There wasalso no significant correlation found between HBsAg and antibodies to hepatitis B core antigen (anti-HBc)positivity and the number of blood transfusions or the length of time on haemodialysis, nor between hepatitisB and C exposure and elevated aminotransferase levels.
Key words: haemodialysis, hepatitis B, hepatitis C.
INTRODUCTION hepatitis must be considered in the differential diagnosis.Non-A, non-B hepatitis is thought to be the currentmajor cause of hepatitis in haemodialysis units.2Patients undergoing chronic haemodialysis potentially
Infection with the hepatitis C virus (HCV) hashave an increased risk of exposure to viral hepatitis.emerged as a problem in dialysis centres especiallyThey may be exposed to viruses from other patients bybecause of the uncertainty regarding its mode ofcrowding and by the use of common equipment. Intransmission among patients undergoing regularaddition, many haemodialysis patients received multiplehaemodialysis treatment. The hepatitis C virus is ofblood transfusions prior to the availability ofclinical importance because of its high rate oferythropoetin and in the Philippines, continue to do sochronicity, with a propensity to insidious progressionif they are unable to support the additional financialto cirrhosis, and the increased risk of hepatocellularburden entailed with regular erythropoietin injections.carcinoma.3The risk of hepatitis B infection for such patients was
The objectives of this study are to determine therecognized many years ago. Problems due to hepatitis Bprevalence of patients positive for antibodies to HCVhave been reduced by the availability of immunization,(anti-HCV) in the haemodialysis unit at the NKTI; toperiodic testing, isolation of infected patients, use ofdetermine the prevalence of patients positive for hepatitisdedicated machines and by improved disinfectantB surface antigen (HBsAg) and antibodies to hepatitisprocedures.1 Despite these control measures, someB core antigen (anti-HBc) in the same population; tohaemodialysis patients develop elevated amino-determine if there is an association between hepatitis Btransferase (ALT) levels. These elevations are usuallyand C exposure and elevated ALT levels; to determinetransient and mild, with an unclear aetiology. Viralif there is an association between the number of bloodtransfusions received as well as the length of time ondialysis with anti-HCV; and, to determine if there is anCorrespondence: RA Danguilan, Department of Nephrology,association between the number of blood transfusionsNational Kidney and Transplant Institute, East Avenue, Quezon City,received as well as the length of time on dialysis andPhilippines.
Accepted for publication 17 September 1997. HBsAg and anti-HBc positivity.

102 MG Santos et al.
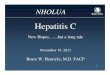
Table 1 Duration of haemodialysis (in years) according toMATERIALS AND METHODShepatitis markers
This is a retrospective study of all the patients (n=86) Hepatitis markers Number Mean (SD)∗ P value†who were undergoing regular haemodialysis sessions at
HBsAGthe NKTI from August 1994 to February 1995. DuringNegative 75 2.3 (1.3) 0.75this period, it was the policy of the haemodialysis unitPositive 11 2.4 (2.5)to dedicate machines for those positive for HBsAg.
Anti-HBcThe haemodialysis nursing staff followed universal Negative 35 2.4 (1.2) 0.76precautions when dealing with all haemodialysis patients. Positive 47 2.3 (2.1)At this time patients found to have anti-HCV were Anti-HCVtreated as regular patients. Routine haemodialysis Negative 50 1.8 (0.8) 0.00007procedures were used with a 4 h treatment duration, 2 Positive 33 3.2 (1.5)or 3 times a week using cellulose acetate dialysers and
HBsAg, hepatitis B surface antigen; Anti-HBc, antibodies toan acetate bath for majority of patients. Sera from the the hepatitis B core antigen; Anti-HCV, antibodies against86 dialysis patients using different dialysis machines and the hepatitis C virus; ∗ Standard deviation; † Significant attreatment rooms were tested. HBsAg, anti-HBs and P<0.00001.anti-HBc were determined by commercial radio-immunoassays. Hepatitis B envelope antigen (HBeAg)was determined for those found positive for HBsAg.The presence of anti-HCV was tested using an
transfusions, and 21% had more than five trans-immunosorbent (ELISA) assay (ortho HCV) whichfusions. The primary renal disease was chronicdetects antibodies to three different regions of HCV:glomerulonephritis (52%) followed by diabeticc22–3 (structural region) which encodes the RNAnephropathy (19.8%) and hypertensive nephrosclerosisbinding nucleocapsid protein, c200 (non-structural(14%).regions 3 and 4) and NS5 (non-structural region) that
Among the hepatitis markers, the prevalence rate ofencodes the viral polymerase. The assay is a three-stageHBsAg was 12.8%, anti-HBc was 57.3% and anti-HCVtest carried out in a microwell coated with a combinationwas 39.8%.of recombinant hepatitis C virus antigen. The colour
As can be seen from Table 1, there was no significantintensity is measured with a microwell readerdifference in the duration of haemodialysis between(photometer) designed to measure light absorbance.those exposed and not exposed to hepatitis B (P=0.75)Transaminases were measured by standard methods.and between those positive for anti-HBc as comparedThe normal range for ALT at the NKTI laboratory waswith those negative for anti-HBc (P=0.76). However,0.12–0.88 ukat/L. An abnormal ALT was defined as aanti-HCV positive patients had a significantly highervalue greater than twice the upper limit of normal.mean duration of dialysis than that of the anti-HCVThe following data were collected by chart review fornegative patients; that is, 3.2 years (S.D. of 1.5) vs 1.8each patient: age at the start of dialysis, sex, primaryyears (SD of 0.8) (P=0.0007).renal disease, number of blood transfusions from the
There was no correlation between anti-HBc and anti-start of dialysis, and duration of dialysis. None of theHCV positivity with the number of blood transfusionspatients were intravenous (i.v.) drug abusers.received (P=0.69 and P=0.28, respectively). DuringStatistical analysis used were the chi-square or Fischer’sthis period, blood for transfusion was routinely testedexact test when comparing two groups for nominalfor HBsAg and for anti-HCV.variables and independent t-test for continuous variables.
A normal ALT level was observed in 63.6% of HBsAgStatistical significance was a P-value of less than 0.05.positive patients and 69.3% of HBsAg negative patients.The difference was not statistically significant (P=0.73).The proportion of patients with elevated ALT levelswere the same for the anti-HBc negative and anti-HBc
RESULTS positive patients (28.6% and 36.2%, respectively, P=0.47) and likewise for those patients who were anti-Of the 86 patients enrolled in the study, 42 (48.8%)HCV negative and those who were anti-HCV positivewere males with a mean age of 44.9 (SD of 15.6) years(P=24% vs 42.45, P=0.08).and mean duration of dialysis of 2.4 years (SD of 1.4).
Forty-four (51.2%) were females with a mean age of48.4 years (SD of 13.4) and mean duration of dialysisof 2.3 years (SD of 1.2). Both sexes were comparable in DISCUSSIONage (P=0.27) and duration of haemodialysis (P=0.64).
Half of the patients did not receive any blood The prevalence of hepatitis B exposure in haemodialysispatients at the NKTI is 57%, with 12.8% of patientstransfusions, 21% received less than or equal to five

Hepatitis in haemodialysis patients 103
positive for HBsAg. In countries such as those in which has reduced the need for blood transfusions aswell as the availability of routine screening for anti-Southern Asia and Tropical Africa the prevalence ofHCV of donor blood. In the present study, less than 5%patients positive for HBsAg ranges from 7 to 20% andof patients received blood transfusions.that of anti-HBs ranges from 70 to 95%.4 However, in
Increased ALT levels, being a marker of inflammatoryNorth America and Europe the prevalence is low withliver disease, may indicate that a patient is potentiallyonly 0.2–0.5% positive for HBsAg and 20–55% positiveinfectious and may therefore contribute to transmissionfor anti-HBs.4
of the virus in the haemodialysis unit.8 However, in theThe Philippines is highly endemic for hepatitis B aspresent study elevated ALT levels were not significantlyshown by the prevalence rate of HBsAg positivity rangingcorrelated with hepatitis B and C exposure.from 8.8–12% and a hepatitis B exposure from 52 to
58%.4 It can be seen from this data that the prevalencefor HBsAg and exposure to hepatitis B is the same forboth healthy patients and those on dialysis. Thereforebeing on dialysis is no longer a risk factor for HBsAg
CONCLUSIONpositivity at the present time. This is probably becauseof the availability of the hepatitis B vaccine and the use
There is a very high prevalence rate of antibodies toof dedicated haemodialysis machines for HBsAg positiveHCV in the haemodialysis unit at the NKTI. Thepatients.possibility of transmission of the virus within the unitThe prevalence of antibodies to HCV in healthyshould be recognized. The length of time onpeople in Italy is 0.9–1.1% while that in Japan is 0.7%,haemodialysis correlated with the presence of antibodiesand in the USA is 0.1%.5 The Liver Study Groupto HCV which strongly supports the haemodialysisled by Dr Ernesto Domingo (unpublished observations)environment as a source of transmission of this disease.found a prevalence of 5.2% (range 0.9–17.6%) amongOn the other hand, the number of blood transfusionshealthy, unpaid Filipino blood donors. The prevalencewas no longer found to be a risk factor for hepatitis Brate of 39.8% found in the haemodialysis unit at theor C transmission. Because HCV infection can leadNKTI is extremely high. The possibility of transmissionto chronic liver disease, cirrhosis and hepatocellularwithin the haemodialysis unit should be stronglycarcinoma measures should be made to try to control itsconsidered.spread in the haemodialysis unit. HCV infection mayThe difference in prevalence rates for anti-HCValso be an additional risk factor for complications forpositivity in haemodialysis patients reported in variouspatients who will subsequently undergo transplantation.countries is unknown. One possibility is the varied lengthThe spread of HCV infection within the haemodialysisof time on dialysis of the different populations studied.unit may possibly be controlled with the adherence ofIn this study, hepatitis C but not hepatitis B was foundstrict universal precautions and possibly by the use ofto be significantly associated with a longer length ofdedicated haemodialysis machines for anti-HCV positivetime on dialysis. This data is in accordance with previouspatients.reports of a positive relationship between anti-HCV
positivity and the length of time on dialysis.5–7 Thelonger the duration of dialysis, the greater the chanceof becoming positive for antibodies to HCV. Again itseems that the haemodialysis environment is important
REFERENCESin the transmission of HCV.Possible routes of transmission of HCV infection in 1. Alter MJ, Favero MS, Maynard JE, Bonino F. Impact of infection
the haemodialysis unit may be through contact of control strategies on the incidence of dialysis-associated hepatitispatients with contaminated environmental surfaces (i.e. in the United States. J. Infect. Dis. 1986; 153: 1149.
2. Zeldis JB, Depner TA, Kuramoto IK, Gish RG, Holand PV. Thegloves, clamps, swabs, dressings and needles), or it mayprevalence of hepatitis C virus antibodies among hemodialysisoccur through extracorporeal circulation and bloodpatients. Ann. Int. Med. 1990; 112: 958.transfusions. In a recent study by Van der Poel et al.,
3. Martin P, Friedman L. Chronic viral hepatitis and the managementnine out of 26 patients (26%) who were initially anti- of chronic renal failure. Kidney Int. 1995; 47: 1231–41.HCV negative demonstrated sero-conversion or clinical 4. Muller G, Zabaleta M, Arminio A, Colmenares C, Capriles F.hepatitis after receiving anti-HCV positive donor blood.8
Risk factors for dialysis-associated hepatitis C in Venezuela. KidneyInt. 1992; 41: 1055–58.Although the present study did not show a greater risk
5. Lin DY, Lin HH, Huang C, Fon Liaw Y. High incidence of hepatitisof infection from either hepatitis B or C with the numberC virus infection in hemodialysis patients in Taiwan. Am. J.of blood transfusions. This is in contrast with otherKidney Dis. 1993; 21 (3): 288–91.studies showing a direct relationship between the
6. Hardy NM, Sandoni S, Danielson S, Wilson WJ. Antibody topresence of anti-HCV and the number of blood hepatitis C virus increases with time on hemodialysis. Clin.transfusions.5,9,10 However, this risk may no longer be Nephrology 1992; 38: 44–8.
7. Van der Poel CL, Reesink HW, Schaasberg W et al. Infectivity ofvery important with the availability of erythropoietin

104 MG Santos et al.
blood seropositive for hepatitis C virus antibodies. Lancet 1990; Comparison of three different tests for assessment of hepatitis Cvirus in dialysis patients. Perit. Dial. Int. 1995; 15: 241–5.335: 558.
8. Hung KY, Chen WY, Yang CS, Lee SH, Wu DJ. Hepatitis B and 10. Chiaramonte S, Tagger A, Ribero ML, Grossi A, Milan M, LaGreca G. Prevention of viral hepatitis in dialysis units: IsolationC in hemodialysis patients. Dialysis and Transpl. 1995; 24 (3):
135–9. and technical management of dialysis. Nephron 1992; 61:287–9.9. Castelnovo C, Lunghi G, de Vecchi A, Grancini A, Como G.













![Hepatitis screening Chinese [Kompatibilitetstilstand] 2014/Oral presentations...collaboration with the Chinese community High prevalence of hepatitis B infections (6%) Low prevalence](https://img.pdfslide.net/doc/110x75/5e175694a1c2c52b8c4f477f/hepatitis-screening-chinese-kompatibilitetstilstand-2014oral-presentationscollaboration.jpg)