Embed Size (px)
Citation preview

Central Annals of Otolaryngology and Rhinology
Cite this article: Kulasegarah J, O’Regan E, Kennedy S, Toner M, Timon C (2016) Prevalence of Multiple Primary Squamous Cell Carcinoma of the Upper Aerodiges-tive Tract in an Irish Tertiary Referral Center. Ann Otolaryngol Rhinol 3(6): 1110.
*Corresponding author
Jeyanthi Kulasegarah, Department of Otolaryngology, Head and Neck Surgery, St. James’s Hospital, Ireland, Tel: 00447710826106; Email:
Submitted: 16 March 2016
Accepted: 09 May 2016
Published: 10 May 2016
ISSN: 2379-948X
Copyright© 2016 Kulasegarah et al.
OPEN ACCESS
Keywords•Squamous cell carcinoma•Head and neck cancer•Second primary malignancy•Upper aerodigestive tract
Research Article
Prevalence of Multiple Primary Squamous Cell Carcinoma of the Upper Aerodigestive Tract in an Irish Tertiary Referral CenterJeyanthi Kulasegarah1*, Esther O’Regan2, Susan Kennedy3, Mary Toner4 and Conrad Timon5
1Department of Otolaryngology, Head and Neck Surgery, St. James’s Hospital, Ireland2Department of Histopathology, St. James’s Hospital, Ireland3Department of Histopathology, Royal Victoria Ear & Ear Hospital, Ireland4Department of Histopathology, St. James’s Hospital, Ireland5Department of Otolaryngology, Head and Neck Surgery, St. James’s Hospital, Ireland
Abstract
The elevated risk of second primary malignancy (SPM) in patients with head and neck squamous cell carcinoma (HNSCC) is well established. Despite the advances in loco regional control achieved by modern surgery and chemoradiation, survival with HNSCC has not meaningfully improved, in part due to continuing risk of development of SPMs in these patients. Our objective was to determine the prevalence of SPM among patients with HNSCC in Ireland. A retrospective study of patients diagnosed with two or more HNSCC between January 2000 and Jun 2012 was conducted in two tertiary referral centers. Out of a population of 604 patients, we identified 72patients (11.9%) with SPM. Our third primary malignancy prevalence rate was 3.0% (18 patients) while the fourth primary malignancy rate was 0.5% (3 patients). Fifty seven males and 15 females between ages of 36 to 78 (mean age 58.3 +/- SD 10.01) were reviewed. The majority of the population smoked tobacco (87.5%) and consumed alcohol (76.1%).Among patients with SPM, 68% (49 patients) had metachronous lesions while 32% (23 patients) had synchronous lesions. In conclusion, multiple primary tumours in patients with an index HNSCC are relatively common in Ireland and represent a significant obstacle to improvement in survival. Our SPM rate is 11.9% in keeping with current literature. Oral cavity and oropharynx are major sites for primary and SPM, which is well documented in the literature.
ABBREVIATIONSSPM: Second Primary Malignancy; HNSCC: Head and Neck
Squamous Cell Carcinoma; HPV: Human Papilloma Virus; SD: Standard Deviation; IQR: Interquartile range; OPSCC: Oropharyngeal Squamous Cell Carcinoma; OSCC: Oral cavity Squamous Cell Carcinoma; TNM: Tumour Nose Metastasis; AJCC: American Joint Committee on Cancer; INHANCE: International Head and Neck Cancer Epidemiology;18F-FDG-PET/CT: 2-deoxy-2-[fluorine-18] fluoro-D-glucose Positron emission tomography integrated with computed tomography
INTRODUCTIONThe elevated risk of second primary malignancy (SPM) in
patients with head and neck squamous cell carcinoma (HNSCC) is well established. Most of these tumours are located in the oral
cavity, oropharynx, larynx, lung and esophagus [1]. Despite the advances in loco regional control achieved by modern surgery and chemoradiation, survival with HNSCC has not meaningfully improved, in part due to the continuing risk of development of SPMs in these patients [2]. SPMs are the leading long term cause of mortality in HNSCC patients [3]. Approximately one-third of HNSCC deaths are attributable to SPMs [4,5], treble the number of deaths due to distant metastases [6].
The incidence of SPM varies across several studies, depending mainly on follow-up time and systematic screening of cases. The annual incidence of a SPM after a HNSCC was 3.8%, whereas it was 5.1% for a third tumour and 7.8% for a fourth tumour [5]. In three large series, Chuang et al [1], with 99,257 patients, Haughey et al [7], with 40,287 and Panosetti et al (8), with 9089 patients, the SPM incidence was 10.9%, 14.2% and 9.4% respectively. In
Central
Kulasegarah et al. (2016)Email:
Ann Otolaryngol Rhinol 3(6): 1110 (2016) 2/7
patients with index HNSCC, the SPM diagnosis occurs at a rate of 2% to 6% per year during the follow-up period [2].
To the best of our knowledge, no comprehensive data has been reported on the risk of SPM among HNSCC in Ireland. The specific objective of this research study is to answer the following questions on SPM of the HNSCC:
1) The prevalence of 2nd, 3rd and 4th primary malignancy in an Irish tertiary referral center.
2) What is the rate of synchronous and metachronous lesions?
3) Where are patients most likely to develop a SPM?
4) What is the time interval between primary and SPM among these patients?
5) What is the overall survival rate among patients with SPM?
MATERIALS AND METHODSThis retrospective study focused on patients who have been
diagnosed with HNSCC between January 2000 to June 2012, from two Irish tertiary referral centres. Prior to conducting this study, ethical approval was obtained from the Ethics Research Committee of our tertiary centres.
The Cancer Audit Programme of our unit collects data on all patients with HNSCC and the data is stored in a comprehensive database. The database contains information on patient demographics, date of diagnosis, ICD disease code, subsite of tumour, risk factors (smoking, alcohol, previous malignancy, and previous radiation treatment), treatment obtained (surgery/radiation/chemotherapy), and the presence of synchronous or metachronous tumours. All patients were staged according to the TNM Staging System.
An inquiry was then run for patients on this database as well as the pathology database for patients with multiple HNSCC for the years under review. All patients with an index invasive HNSCC of the upper aerodigestive tract were included. A SPM is defined as a subsequent invasive cancer developing after an index HNSCC. We excluded all malignant lesions that appeared outside the upper aerodigestive tract and also all second and successive head and neck tumours that were not squamous cell carcinomas. In our study, the criteria for SPM, is in accordance with that described by Warren and Gates [9] and modified by other studies of Human Papillomavirus (HPV)-associated HNSCC [10,11], as follows:
1) If the second cancer was of non-squamous cell origin, or developed in a different location, it was coded as an SPM.
2) If the second cancer was of both squamous cell carcinoma and developed in the same region as the index cancer, it was only coded as an SPM only if more than 60 months had passed since the index diagnosis and/or at least 2cm of normal mucosa between each lesion.
3) Synchronous tumours are defined as second cancers diagnosed at the same time (synchronous simultaneous) or within 6 months of the diagnosis of the index HNSCC
(synchronous non-simultaneous).
4) If they are diagnosed after 6 months, they are considered metachronous.
5) Metachronous second primary in the lung were all solitary lesions and diagnosed by thoracic specialists.
Statistical analysis was performed using IBM SPSS Statistics Version 21.0.0.0 software. Overall, the prevalence of SPM, third primary malignancy and fourth primary malignancy are presented. The threshold for statistical significance was set at p<0.05, and all tests were 2-sided. Fisher’s exact test was used to assess difference in clinical variables. Kaplen-Meier curves were generated and log-rank tests were performed to detect statistically significant differences. The end point of interest for overall survival was death from any cause. Follow-up time was calculated from the date of diagnosis until the date of death or last seen in the outpatients department.
RESULTSOur study identified 604 patients who were diagnosed with an
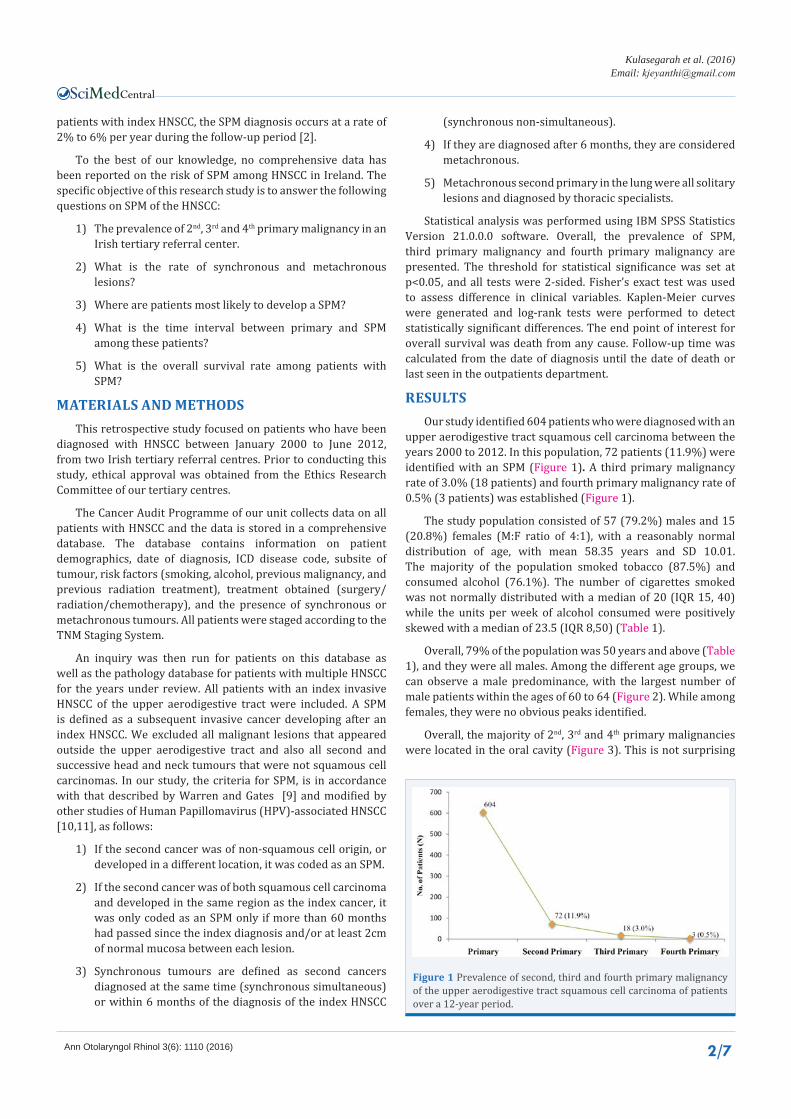
upper aerodigestive tract squamous cell carcinoma between the years 2000 to 2012. In this population, 72 patients (11.9%) were identified with an SPM (Figure 1). A third primary malignancy rate of 3.0% (18 patients) and fourth primary malignancy rate of 0.5% (3 patients) was established (Figure 1).
The study population consisted of 57 (79.2%) males and 15 (20.8%) females (M:F ratio of 4:1), with a reasonably normal distribution of age, with mean 58.35 years and SD 10.01. The majority of the population smoked tobacco (87.5%) and consumed alcohol (76.1%). The number of cigarettes smoked was not normally distributed with a median of 20 (IQR 15, 40) while the units per week of alcohol consumed were positively skewed with a median of 23.5 (IQR 8,50) (Table 1).
Overall, 79% of the population was 50 years and above (Table 1), and they were all males. Among the different age groups, we can observe a male predominance, with the largest number of male patients within the ages of 60 to 64 (Figure 2). While among females, they were no obvious peaks identified.
Overall, the majority of 2nd, 3rd and 4th primary malignancies were located in the oral cavity (Figure 3). This is not surprising
Figure 1 Prevalence of second, third and fourth primary malignancy of the upper aerodigestive tract squamous cell carcinoma of patients over a 12-year period.

Central
Kulasegarah et al. (2016)Email:
Ann Otolaryngol Rhinol 3(6): 1110 (2016) 3/7
Figure 2 Distribution of the study population according to age groups and gender (N=72).
Figure 3 Overall distribution of tumour site among primary, second, third and fourth primary malignancy.
Table 1: Baseline characteristics of the study population.
Characteristics Subjects (N=72)
Mean Age 58.4+/-10.1 (25-78)
Under 50 years 15 (20.8%)
Over 50 years 57 (79.2%)
Gender
Males 57 (79.2%)
Female 15 (20.8%)
Tobacco Smoking
Ever-smokers 63 (87.5%)
Non-smokers 9 (12.5%)
Median Number of Cigarettes/Week 20 (IQR 15, 40)
Alcohol
Ever-drinkers 54 (76.1%)
Non-drinkers 17 (23.9%)
Median Number of Units/Week 23.5 (IQR 8,50)
Abbreviations: IQR: Interquartile Range
as lesions within this region are easily identified by the GP or when patients attend their follow-up visits at the head and neck outpatient clinic. A more detailed analysis (Table 2) using Fisher’s test, of the locations of the index tumour and SPM in the head and neck showed there was significant association between the location of the index tumour and the location of the SPM (p=0.018). Further detailed analysis of tumour sites (Table
2), showed that in the majority of oropharyngeal squamous cell carcinoma (OPSCC) (62.5%), the SPM was also located within the oropharynx, similarly for primary oral cavity squamous cell carcinoma (OSCC), SPMs were located in the oral cavity (56.8%). However, for hypopharyngeal and laryngeal cancers, SPMs were located mainly within the oropharynx, oral cavity, or lung.
Among patients with SPM, 68% (49 patients) had metachronous lesions while 32% (23 patients) had synchronous lesions. Synchronous simultaneous lesion occurred in 21 patients (91.3%) and synchronous non-simultaneous tumours were found in 2 patients (8.7%). Six patients (33%) with a SPM developed a synchronous third primary malignancy and 11 patients (67%) developed a metachronous third primary malignancy. All 3 patients with a fourth primary malignancy developed a metachronous lesion.
Index tumour and SPM were categorized according to the tumour, node, metastasis (TNM) staging system according to the 7th Edition of the American Joint Committee on Cancer (AJCC) Staging Manual. The specific TNM staging of each patient is then tabulated to give a numerical status of Stage I, II, III, or IV. The percentage of patients with an index tumour diagnosed at an early stage (Stages I&II) was 51.4%, increasing up to 57% for the SPM and 72.2% for third primary tumour (Table 3). The number of patients with advanced tumour (Stages III&IV) decreased from 47.2% for the index tumour to 40.3% for SPM and 22.2% for a third tumour (Table 3). This progressive decrease in the number of patients with advanced stage is possible due to regular follow-up in the head and neck outpatient clinic. We found no significant association between early and late stage disease between index tumour and SPM (p=0.462).
The mean time interval between the index tumour and SPM was about 3 years and 8 months (44.1 months), while the median time interval was 12 months (Table 4). Among the 18 patients with a third primary malignancy, the mean time interval between SPM and third primary malignancy was about 2 years and 6 months (30.22 months), with a median time interval of 13 months.
The overall 2-year and 5-year survival rate from the index tumour to SPM and SPM to third primary is shown in (Table 5). The overall 5-year survival rate from index tumour to SPM was 29.2%, while from the SPM to third primary malignancy was 16.7%. The overall survival curves were calculated in chronological order using the Kaplan-Meier method (Figure 4). There were no significant differences in the overall survival rate of patients in relation to the chronology of appearance of their multiple primary malignancies (p=0.647).
DISCUSSIONBillroth [12] was the first to describe the concept of multiple
neoplasm. Then in 1932, Warren and Gates [9] defined the criteria classifying multiple neoplasm, while Slaughter et al [13] in 1953, coined the term of “field cancerization’ in an attempt to define carcinogenesis of multiple neoplasms of the upper aerodigestive tract. The risk of SPM among patients with HNSCC is a complex phenomenon, which can be affected by multiple factors simultaneously.

Central
Kulasegarah et al. (2016)Email:
Ann Otolaryngol Rhinol 3(6): 1110 (2016) 4/7
Second Primary Malignancy (SPM)Total
Hypopharynx Larynx Lung Oesophagus Oral Cavity Oropharynx
Primary M
alignancy
Hypopharynx
N 1 0 3 1 2 5 12
% within PM 8.3% 0.0% 25.0% 8.3% 16.7% 41.7% 100.0%
% of Total 1.4% 0.0% 4.2% 1.4% 2.8% 6.9% 16.7%
Larynx
N 1 1 3 0 6 0 11
% within PM 9.1% 9.1% 27.3% 0.0% 54.5% 0.0% 100.0%
% of Total 1.4% 1.4% 4.2% 0.0% 8.3% 0.0% 15.3%
Lung
N 1 0 0 0 1 0 2
% within PM 50.0% 0.0% 0.0% 0.0% 50.0% 0.0% 100.0%
% of Total 1.4% 0.0% 0.0% 0.0% 1.4% 0.0% 2.8%
Nasopharynx
N 0 0 0 0 0 1 1
% within PM 0.0% 0.0% 0.0% 0.0% 0.0% 100.0% 100.0%
% of Total 0.0% 0.0% 0.0% 0.0% 0.0% 1.4% 1.4%
Oesophagus
N 0 1 0 0 0 0 1
% within PM 0.0% 100.0% 0.0% 0.0% 0.0% 0.0% 100.0%
% of Total 0.0% 1.4% 0.0% 0.0% 0.0% 0.0% 1.4%
Oral Cavity
N 4 2 4 0 21 6 37
% within PM 10.8% 5.4% 10.8% 0.0% 56.8% 16.2% 100.0%
% of Total 5.6% 2.8% 5.6% 0.0% 29.2% 8.3% 51.4%
Oropharynx
N 0 0 1 0 2 5 8
% within PM 0.0% 0.0% 12.5% 0.0% 25.0% 62.5% 100.0%
% of Total 0.0% 0.0% 1.4% 0.0% 2.8% 6.9% 11.1%
Total
N 7 4 11 1 32 17 72
% within PM 9.7% 5.6% 15.3% 1.4% 44.4% 23.6% 100.0%
% of Total 9.7% 5.6% 15.3% 1.4% 44.4% 23.6% 100.0%
Table 2: Detailed distribution of tumour site with primary tumour and SPM.
Value df Asymp. Sig. (2-sided)
Fishers exact test 48.475 30 .018
Table 3: AJCC Staging of HNSCC among patients with index, second, third and fourth primary malignancy.
Stage Index TumourN (%)
Second TumourN (%)
Third TumourN (%)
Fourth TumourN (%)
I 22 (30.6%) 30 (41.7%) 7 (38.9%) 1 (33.3%)
II 15 (20.8%) 11 (15.3%) 6 (33.3%) 1 (33.3%)
III 10 (13.9%) 9 (12.5%) 1 (5.6%)
IV 24 (33.3%) 20 (27.8%) 3 (16.7%) 1 (33.3%)(NB. Staging information from the 7th Edition of the AJCC Staging Manual) Abbreviations: AJCC: American Joint Committee on Cancer
Table 4: Time Interval between Multiple Primary Malignancies.
Chronology of appearance
Mean (Months) Median (Months)
Estimate Std. Error95% CI
Estimate Std. Error95% CI
Lower Bound Upper Bound Lower
Bound Upper Bound
1st – 2nd 44.097 7.040 30.299 57.896 12.000 3.711 4.727 19.273
2nd – 3rd 30.222 9.595 11.416 49.028 13.000 3.182 6.763 19.237
3rd – 4th 57.000 30.172 .000 116.137 51.000 35.109 .000 119.814
Overall 41.828 5.827 30.408 53.248 13.000 3.210 6.709 19.291
Abbreviations: Std: Standard

Central
Kulasegarah et al. (2016)Email:
Ann Otolaryngol Rhinol 3(6): 1110 (2016) 5/7
The incidence of SPM varies across several studies. In three large case series, Chuang et al [1] with 99,257 patients, Haughey et al [7] with 40,287 patients, and Panosetti et al [8] with 9,089 patients, the SPM incidence was 10.9%, 14.2% and 9.4% respectively. The rate of SPM in our series was 11.9%. Leon et al [14] with a series of 3,631 patients had a SPM rate of 23.1%, third primary malignancy rate of 4.1% and fourth primary malignancy rate of 0.96%. This study has a third and fourth primary malignancy rate of 3% and 0.5% respectively.
A mean age of over 50 years, male predominance and a large proportion of smokers (87.5%) and alcohol drinkers (76.1%) which were in line with the expected risk factors for the HNSCC population investigated in this study. Jones et al [15] established the two risk factors to diagnose SPM; male gender and with an age profile of less than 60 years. Tobacco and alcohol consumption are estimated to be responsible for 72% of HNSCC in the general population, with 4% due to alcohol alone, 33% due to tobacco alone, and 35% due to tobacco and alcohol combined, as reported by the International Head and Neck Cancer Epidemiology (INHANCE) consortium [16].
In relation to the location of the SPM, Panosetti et al [8] found that SPM have a tendency to follow a respiratory axis (larynx-lung) or a digestive axis (pharynx-esophagus). Leon et al [5]
agreed that when the index tumour was located in the larynx, the SPM is most likely to be located in the lungs; when the index tumour was located in the hypopharynx, the SPM was preferably located in the digestive axis; and when the index tumour was located in the oral cavity and oropharynx, the SPM appears to be located in the oral cavity and oropharynx. Our results agree with the literature: when the index tumour is located in the larynx, the SPM is more likely to be in the lung; and when the index tumour is located in the oral cavity and oropharynx, the SPM is more likely to be in the oral cavity and oropharynx respectively. However, we found that hypopharyngeal primary tumours had a tendency to develop SPM in the lung and not esophagus. We did have one patient with an esophageal SPM, whose index tumour was in the hypopharynx. Moertel [17,18] and De Vries [19] noted that SPM were more common in patients with an index tumour in the oral cavity, and this hypothesis was supported in our series, where 44.4% of patients developed a SPM in the oral cavity. This compares with rates of 23.6% in the oropharynx, 9.7% in the hypopharynx and 5.6% in the larynx.
The majority of SPM are metachronous, occurring more than 6 months after an index HNSCC. The prevalence of synchronous SPM in patients with HNSCC ranges from 1% to 6% (2, 4, 5, 13). In a meta-analysis completed by Haughey et al [7], the prevalence of synchronous SPM reported in the literature ranged between 0.8% and 18%. In the 604 patients within this series with an index HNSCC, 3.8% had a second synchronous neoplasm within the head and neck region.
Our results indicate that almost 50% of index HNSCC was diagnosed at a late stage (Stage III and IV). This percentage continues to drop with subsequent malignancies, from 43% for SPM down to 27.8% for third primary malignancy. Early diagnosis of subsequent malignancies is probably due to regular attendance of patients to the outpatients department. After treatment of the primary tumour, it is important to maintain rigorous follow-up of patients and always investigate their complaints and any suspicious lesions so that SPMs can be detected while they are limited and treated with a high likelihood of cure. Triple endoscopy (laryngoscopy, bronchoscopy and esophagoscopy) and positron emission tomography integrated with computed tomography (18F-FDG-PET/CT) are two modalities used to successfully detect SPMs. Haerle et al [20] concluded that 18F-FDG-PET/CT is superior to triple endoscopy to detect SPM, however with a higher number of false positive cases.
In the present series, of the 72 SPM with a median follow-up of 12 years and a maximum follow-up of up to 27 years, the overall 2-year and 5-year survival rate of patients with SPM was 43.1% and 29.2% respectively. Rennemo et al [21] identified that in patients who developed SPM, the overall median survival rate was 6 years with a 5-year survival rate of 16%. In a study by Priante et al [22], 5-year survival after SPM diagnosis was 26%.
Panosetti et al [8] identified a better survival rate in metachronous SPM than in synchronous SPM (55% and 18% in 5 years respectively). Two other studies also showed better survival rates for metachronous tumours. Di Martino et al [23] study showed the 5-year post SPM survival rate was significantly higher in the metachronous tumours (26%) than in synchronous tumours (11.9%; p<0.001). In the study by Lin et al [24], the
Table 5: The overall 2-year and 5-year survival rate of patients with multiple primary malignancies.
Second Primary Malignancy
Third Primary Malignancy
Overall 2-year survival 43.1% 33.3%
Overall 5-year survival 29.2% 16.7%
Figure 3 Overall distribution of tumour site among primary, second, third and fourth primary malignancy.

Central
Kulasegarah et al. (2016)Email:
Ann Otolaryngol Rhinol 3(6): 1110 (2016) 6/7
5-year overall survival rate for synchronous tumours was 29.4% and for metachronous it was 70% (p=0.003). The present series supports the literature that there is a significantly better survival rate among patients with metachronous lesion (41.2%) than in synchronous SPM (29.4%, p<0.001).
There is little doubt that smoking tobacco and alcohol abuse are major causes of HNSCC. Leon et al [25] stated that the 5-year survival rates of 5% for smokers and 20% for non-smokers, while Schwaltz et al [26] found the 5-year survival rate of 6% for alcohol drinkers and 27% for non-drinkers. We found that smoking tobacco and consuming alcohol significantly altered the 2-year overall survival rate among our patients. However, we could not evaluate the influence of continuing to smoke and alcohol consumption on the appearance of SPM as the information was not available.
The risk of SPM in patients who continued to smoke was 2.9 and for those who continued to consume alcohol was 5.2 [25]. Graces et al [27] described a trend where patients with HNSCC, who continued to smoke cigarettes, were more likely to develop tobacco related cancers than those who remained abstinent. However, Wynder et al [28] found that ceasing smoking and consuming alcohol did not prevent the development of SPM. In an attempt to prevent a SPM among patients with HNSCC, it is crucial that head and neck surgeons strongly dissuade patients from the use of tobacco and excessive alcohol consumption following diagnosis of index tumour.
CONCLUSIONIn conclusion, multiple primary tumours in patients with an
index HNSCC are relatively common in Ireland and represent a significant obstacle to improvement in survival. Our SPM rate is 11.9% in keeping with current literature. Oral cavity and oropharynx are major sites for primary and SPM, which is well documented in the literature.
ACKNOWLEDGEMENTSMany thanks to the Royal Victoria Eye and Ear Research
Foundation Fund for financial support.
REFERENCES1. Chuang SC, Scelo G, Tonita JM, Tamaro S, Jonasson JG, et al. Risk of
second primary cancer among patients with head and neck cancers: A pooled analysis of 13 cancer registries. Int J Cancer. 2008; 123: 2390-2396.
2. Morris LG, Sikora AG, Hayes RB, Patel SG, Ganly I. Anatomic sites at elevated risk of second primary cancer after an index head and neck cancer. Cancer Causes Control. 2011; 22: 671-679.
3. Vikram B. Changing patterns of failure in advanced head and neck cancer. Arch Otolaryngol. 1984; 110: 564-565.
4. Sturgis EM, Miller RH. Second primary malignancies in the head and neck cancer patient. Ann Otol Rhinol Laryngol. 1995; 104: 946-954.
5. León X, Quer M, Diez S, Orús C, López-Pousa A, Burgués J. Second neoplasm in patients with head and neck cancer. Head Neck. 1999; 21: 204-210.
6. Garavello W, Ciardo A, Spreafico R, Gaini RM. Risk factors for distant metastases in head and neck squamous cell carcinoma. Arch Otolaryngol Head Neck Surg. 2006; 132: 762-766.
7. Haughey BH, Gates GA, Arfken CL, Harvey J. Meta-analysis of second malignant tumors in head and neck cancer: the case for an endoscopic screening protocol. Ann Otol Rhinol Laryngol. 1992; 101: 105-112.
8. Panosetti E, Luboinski B, Mamelle G, Richard JM. Multiple synchronous and metachronous cancers of the upper aerodigestive tract: a nine-year study. Laryngoscope. 1989; 99: 1267-1273.
9. Warren S, Gates O. Multiple primary malignant tumours: a survey of the literature and a statistical study. Am J Cancer. 1932; 16: 1358-414.
10. Joseph AW, Ogawa T, Bishop JA, Lyford-Pike S, Chang X, Phelps TH, et al. Molecular etiology of second primary tumors in contralateral tonsils of human papillomavirus-associated index tonsillar carcinomas. Oral Oncol. 2013; 49: 244-248.
11. Huang SH, Perez-Ordonez B, Liu FF, Waldron J, Ringash J, Irish J, et al. Atypical clinical behavior of p16-confirmed HPV-related oropharyngeal squamous cell carcinoma treated with radical radiotherapy. Int J Radiat Oncol Biol Phys. 2012; 82: 276-283.
12. Billroth T. DIe allgemeine chirurgische pathologie und therapie, in einundfunfzig vorlesungen: Ein handbuch fur studirende und aerzte. Berlin, Germany; 1889.
13. Slaughter DP, Southwick HW, Smejkal W. Field cancerization in oral stratified squamous epithelium; clinical implications of multicentric origin. Cancer. 1953; 6: 963-968.
14. León X, Martínez V, López M, García J, Quer M. Risk of third and fourth tumors in patients with head and neck cancer. Head Neck. 2010; 32: 1467-1472.
15. Jones AS, Morar P, Phillips DE, Field JK, Husband D, Helliwell TR. Second primary tumors in patients with head and neck squamous cell carcinoma. Cancer. 1995; 75: 1343-1353.
16. Hashibe M, Brennan P, Chuang SC, Boccia S, Castellsague X, Chen C, et al. Interaction between tobacco and alcohol use and the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Cancer Epidemiol Biomarkers Prev. 2009;18: 541-550.
17. Moertel CG, Dockerty MB, Baggenstoss AH. Multiple primary malignant neoplasms. II. Tumors of different tissues or organs. Cancer. 1961; 14: 231-237.
18. Moertel CG, Dockerty MB, Baggenstoss AH. Multiple primary malignant neoplasms. I. Introduction and presentation of data. Cancer. 1961; 14: 221-230.
19. de Vries N, Van der Waal I, Snow GB. Multiple primary tumours in oral cancer. Int J Oral Maxillofac Surg. 1986; 15: 85-87.
20. Haerle SK, Strobel K, Hany TF, Sidler D, Stoeckli SJ. (18)F-FDG-PET/CT versus panendoscopy for the detection of synchronous second primary tumors in patients with head and neck squamous cell carcinoma. Head Neck. 2010; 32: 319-325.
21. Rennemo E, Zatterstrom U, Boysen M. Impact of second primary tumors on survival in head and neck cancer: an analysis of 2,063 cases. Laryngoscope. 2008; 118: 1350-1356.
22. Priante AV, Castilho EC, Kowalski LP. Second primary tumors in patients with head and neck cancer. Curr Oncol Rep. 2011; 13: 132-137.
23. Di Martino E, Sellhaus B, Hausmann R, Minkenberg R, Lohmann M, Esthofen MW. Survival in second primary malignancies of patients with head and neck cancer. J Laryngol Otol. 2002; 116: 831-838.
24. Lin K, Patel SG, Chu PY, Matsuo JM, Singh B, Wong RJ, et al. Second primary malignancy of the aerodigestive tract in patients treated for cancer of the oral cavity and larynx. Head Neck. 2005; 27: 1042-1048.

Central
Kulasegarah et al. (2016)Email:
Ann Otolaryngol Rhinol 3(6): 1110 (2016) 7/7
Kulasegarah J, O’Regan E, Kennedy S, Toner M, Timon C (2016) Prevalence of Multiple Primary Squamous Cell Carcinoma of the Upper Aerodigestive Tract in an Irish Tertiary Referral Center. Ann Otolaryngol Rhinol 3(6): 1110.
Cite this article
25. León X, Del Prado Venegas M, Orús C, López M, García J, Quer M. Influence of the persistence of tobacco and alcohol use in the appearance of second neoplasm in patients with a head and neck cancer. A case-control study. Cancer Causes Control. 2009; 20: 645-652.
26. Schwartz LH, Ozsahin M, Zhang GN, Touboul E, De Vataire F, Andolenko P, et al. Synchronous and metachronous head and neck carcinomas. Cancer. 1994; 74: 1933-1938.
27. Garces YI, Schroeder DR, Nirelli LM, Croghan GA, Croghan IT, Foote RL, et al. Second primary tumors following tobacco dependence treatments among head and neck cancer patients. Am J Clin Oncol. 2007; 30: 531-539.
28. Wynder EL, Dodo H, Bloch DA, Gantt RC, Moore OS. Epidemiologic investigation of multiple primary cancer of the upper alimentary and respiratory tracts. I. A retrospective study. Cancer. 1969; 24: 730-739.