Embed Size (px)
Citation preview

SYSTEMATIC REVIEW
Prevalence of peg-shaped maxillary permanentlateral incisors: A meta-analysis
Fang Hua,a Hong He,b Peter Ngan,c and Wassim Bouzida
Wuhan, China, and Morgantown, WVa
aResidHospiWuhabProfeStomacProfeVirginAll auPotenReprinof Sto237#com.Subm0889-Copyrhttp:/
Introduction: The aim of this meta-analysis was to gain more insight into the prevalence of peg-shapedmaxillary permanent lateral incisors and their associations with race, population type, sex, and sidedness.Methods: Electronic searches and supplementary hand searches initially yielded 3337 records. After applyinginclusion and exclusion criteria, 30 articles about 36 studies were included. The overall pooled prevalenceestimate was calculated with a random-effects model. An estimated risk ratio was used for sex comparison.Results: The overall prevalence of peg-shaped maxillary permanent lateral incisors was 1.8%. Nopublication bias was found. The occurrence rates were higher in Mongoloid (3.1%) than in black (1.5%) andwhite (1.3%) patients, and in orthodontic patients (2.7%) than in the general population (1.6%) and dentalpatients (1.9%). Women were 1.35 times more likely than men to have peg-shaped maxillary permanentlateral incisors. The prevalence rates of unilateral (0.8%) and bilateral peg-shaped maxillary permanentlateral incisors were approximately the same. However, among the unilateral lateral incisors, the left side(0.4%) was twice as common as the right side (0.2%). In addition, contralateral lateral incisor hypodontia wasseen in 55.5% of the subjects with unilateral lateral incisors. Conclusions: The prevalence of peg-shapedmaxillary permanent lateral incisors varies by race, population type, and sex. The prevalence rates werehigher among Mongoloid people, orthodontic patients, and women. Although the prevalence of unilateral andbilateral lateral incisors was the same, the left side was twice as common as the right side. Subjects withunilateral peg-shaped maxillary permanent lateral incisors might have a 55% chance of having lateral incisorhypodontia on the contralateral side. (Am J Orthod Dentofacial Orthop 2013;144:97-109)
Apeg-shaped tooth, defined by Grahn�en1 as theincisal mesiodistal width of the tooth crownshorter than the cervical width, is usually
a maxillary permanent lateral incisor (peg-lateral).Leading to esthetic, orthodontic, and periodontalproblems for affected persons, peg-laterals are a majorconcern of general dentists and dental specialists.2
Although the prevalence rates of peg-laterals havebeen reported in some survey studies, they varieddramatically from 0.6%3 to 9.9%.4
ent and postgraduate student, Department of Orthodontics, School andtal of Stomatology, Hubei-MOST KLOS & KLOBM, Wuhan University,n, China.ssor and chair, Department of Orthodontics, School and Hospital oftology, Hubei-MOST KLOS & KLOBM, Wuhan University, Wuhan, China.ssor and chair, Department of Orthodontics, School of Dentistry, Westia University, Morgantown, WVa.thors have completed and submitted the ICMJE Form for Disclosure oftial Conflicts of Interest and none were reported.t requests to: Hong He, Department of Orthodontics, School and Hospitalmatology, Hubei-MOST KLOS & KLOBM, Wuhan University, Luoyu Rd, Hongshan District, Wuhan, China 430079; e-mail, drhehong@hotmail.
itted, November 2012; revised and accepted, February 2013.5406/$36.00ight � 2013 by the American Association of Orthodontists./dx.doi.org/10.1016/j.ajodo.2013.02.025
For over 40 years, the literature has suggested thatthe occurrence of peg-laterals is associated with thesame genetic mechanism that causes agenesis of themaxillary lateral incisors, claiming that the defectivegene can express differently in distinct teeth.5,6 Granatand Chapelle7 advocated that in the evolution withina species a tooth is reduced in volume and becomesconic before disappearing. Furthermore, Brook8 pro-posed a multifactorial model based on an underlyingcontinuous distribution of tooth size, with thresholdsdetermining hypodontia and supernumerary teeth,and found a general trend that the more severe thehypodontia, the smaller the size of the tooth formed.9
In a previous meta-analysis, Polder et al10 founddifferences in the prevalence rates of dental agenesisbetween races, sexes, and continents of origin. Addition-ally, several studies in the last 15 years have focused ondental anomalies among orthodontic populations andhave shown different prevalence values compared withformer data derived from general populations.4,11,12
Thus, considering the generally accepted strongassociation between dental agenesis and peg-laterals,it became an interest to investigate the epidemiologicfeatures of peg-laterals.
97

Table I. Search strategy used in this study (as of October 14, 2011)
Electronic databases Search strategy Hits (n)PubMed (“tooth abnormalities”[MeSH] OR (“tooth”[All Fields] AND
“abnormalities”[All Fields]) OR “tooth abnormalities”[All Fields]) AND(“epidemiology”[Subheading] OR “epidemiology”[All Fields] OR“prevalence”[All Fields] OR “prevalence”[MeSH])
1624
EMBASE “tooth”/exp OR tooth AND (“abnormalities”/exp OR abnormalities) AND(“prevalence”/exp OR prevalence)
1291
Google Scholar intitle:tooth abnormalities AND prevalence anomalies OR tooth 400Cochrane Central Registerof Controlled Trials
(tooth abnormalities) AND prevalence 3
metaRegister of Controlled Trials (tooth abnormalities) AND prevalence 0OpenGrey (tooth abnormalities) AND prevalence 0
Table II. Study selection criteria of this meta-analysis
Criteria category Inclusion criteria Exclusion criteriaStudy design Cross-sectional or retrospective studies
reporting prevalence of peg-shapedmaxillary permanent lateral incisors
Studies regarding other tooth abnormalitiesStudies mixing peg-shaped teeth with microdontiaStudies regarding deciduous dentitionStudies with each tooth as a study unit
Studies using a diagnostic standard the sameas or similar to any reduction in mesiodistalcrown diameter in a gingivo-incisal direction
Studies concerning treatment, etiology, and theoryof peg-shaped teeth
Studies about an association between peg-shapedteeth and syndromes
Studies with each participant as a study unit Case reports/case seriesReviews/systematic reviews
Characteristics ofsubjects
Presented exact race and population type ofparticipants (general/patients)
Failed to mention race and population type of participants
98 Hua et al
According to Juki�c et al,13 the incidence and degreeof expression of dental anomalies can provide importantinformation for phylogenic and genetic studies and helpunderstand variations within and between populations.However, the occurrence rate of peg-laterals has notbeen analyzed in an integrated approach. The aims ofthis study were to shed insight into the prevalence ofpeg-laterals using a meta-analysis and to detect its po-tential relationship with races, sexes, population types,and continents of origin.
MATERIAL AND METHODS
This systematic review was written according to theMOOSE standards for the reporting of meta-analysesof observational studies in epidemiology.14
The following abstract databases were searchedfrom inception to October 2011: PubMed, Embase,Google Scholar, Cochrane Central Register ofControlled Trials, metaRegister of Controlled Trials,and OpenGrey. To identify underlying useful informa-tion in dental surveys, we adopted the search termcombinations of “tooth abnormalities” and “prevalence”(Table I). After electronic searches and the initialselection process, a supplementary hand search wasimplemented by checking the references of remaining
July 2013 � Vol 144 � Issue 1 American
key studies. No restrictions for language or publicationdate were used.
Studies reporting the occurrence rate of peg-lateralswere included. The diagnostic standard of peg-shapedteeth similar to that of Grahn�en1 was used: the incisalmesiodistal width of the tooth crown shorter than thecervical width. Prevalence was defined as the numberof people with peg-laterals divided by the number ofpeople studied. We excluded all studies that wereirrelevant to the prevalence of peg-laterals, studies ofother populations or subjects in the primary dentition,and studies that provided no adequate data after wecontacted the authors. The details on the predefinedinclusion and exclusion criteria are given in Table II.
All references identified were compiled into a refer-ence manager (NoteExpress 2; Aegean Software, Beijing,China). Two authors (F.H. and W.B.) performed thesearch independently using the inclusion and exclusioncriteria. Any disagreement was resolved by consultationwith a third author (H.H.) until mutual agreement wasreached. Full texts were retrieved mainly through the lit-erature delivery service of the library at Wuhan Universityin China or by directly contacting the correspondingauthors. For 7 studies with insufficient data, the authorswere contacted, and we received 2 responses.15,16
Journal of Orthodontics and Dentofacial Orthopedics

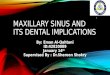
Fig 1. Flow diagram of the study selection process.
Hua et al 99
Two authors (F.H. and W.B.) independentlyreviewed the selected articles and tabulated the studycharacteristics with Excel for Windows software(Microsoft, Redmond, Wash). Any difference wasresolved by consultation with a professor (H.H.) untilmutual agreement was reached. The following datawere recorded: demographic information, studydesign, publication year, sidedness of peg-laterals,
American Journal of Orthodontics and Dentofacial Orthoped
number of people affected with peg-laterals(the numerator), and number of people studied(the denominator).
Two authors (F.H. and W.B.) independentlyperformed structured quality assessments according topublished methods.17,18 The quality system was thefollowing: (1) reasonable age range, (2) proper samplesize (neither too large nor too small),10 (3) either random
ics July 2013 � Vol 144 � Issue 1

Table III. Characteristics of included studies
StudyFirst author,
publication year Country/location Ethnicity Population Age (y)1 Onyeaso,36 2006 Nigeria/Ibadan Black SC 11-122 Sawyer,41 1984 Nigeria/Lagos Black SC 10-193 Rose,39 1906 Germany/– White Recruits –
4 Dolder,28 1936 Switzerland/– White SC 6-155 Rantenen,38 1955 Finland/– White SC –
6 Grahn�en,1 1956 Sweden/– White SC 11-147 Grahn�en,1 1956 Sweden/– White SC 17-438 Thilander,3 1973 Sweden/Umea White SC 7-139 Magnusson,33 1977 Iceland/Reykjav�ık White SC 8-1610 Backman,25 2001 Sweden/Umea White Children 711 Ling,32 1992 China/Hong Kong Mongoloid SC 1212 King,31 2010 China/Hong Kong Mongoloid SC 1213 Wu and Feng,16 2005 China/Beijing Mongoloid College students 17-2114 Ooshima,37 1996 Japan/Osaka Mongoloid HSS 15-1815 Chung,27 1972 USA/Hawaii White HSS 12-1816 Chung,27 1972 USA/Hawaii Mongoloid HSS 12-1817 Chung,27 1972 USA/Hawaii Mongoloid HSS 12-1818 Chung,27 1972 USA/Hawaii Mongoloid HSS 12-1819 Meskin,34 1963 USA/Minnesota White College students –
20 Nayak,35 2011 India/Jodhpur Indian SC 6-1521 Al-Hummayani,23 2005 Saudi Arabia/Jeddah White SC 11-1922 Salem,40 1989 Saudi Arabia/Gizan White SC 4-1223 Ucheonye,2 2010 Nigeria/Ibadan Black DP –
24 Shah,42 1978 Canada/Vancouver White DP –
25 Fujita,29 2009 Japan/Kitakyushu Mongoloid DP 5-1926 Stecker,43 2007 USA/Minnesota Mongoloid DP –
27 Gupta,30 2011 India/Indore Indian DP .1428 Albashaireh,22 2006 Jordan/– White DP 16-4529 Ucheonye,2 2010 Nigeria/Ibadan Black Ortho –
30 Thongudomporn,4 1998 Australia/Queensland White Ortho 10.2-26.431 Basdra,26 2001 Germany/Heidelberg White Ortho 7.2- 45.832 Basdra,11 2000 Germany/Heidelberg White Ortho 7-4433 Thilander,3 1973 Sweden/Umea White Ortho 7-1334 Kositbowornchai,15 2010 Thailand/KhonKaen Mongoloid Ortho 12-4035 Kazanci,12 2011 Turkey/Erzurum White Ortho 9-2536 Altug-Atac,24 2007 Turkey/Ankara White Ortho 8.5-14.75
SC, Schoolchildren; HSS, high school students; DP, dental patients; Ortho, orthodontic patients.*A number without a virgule (/) shows the overall nunber of affected subjects (the study provided no data by sex); y1, reasonable age range; 2, propersample size; 3, either random or consecutive sampling; 4, description of examination method; 5, exclusive focus on maxillary lateral incisors.
100 Hua et al
or consecutive sampling, (4) description of examinationmethod, and (5) exclusive focus on maxillary lateralincisors. Quality was categorized as low (1-2 scores),medium (3-4 scores), or high (5 scores).
Statistical analysis
For data synthesis and heterogeneity assessment, thedata were imported into the STATA software (version12.0; StataCorp, College Station, Tex) to calculatepooled estimates and 95% confidence intervals (CIs) ofprevalence. Occurrence rates of comparable subgroupswere summarized when possible. For sex comparisons,the estimated risk ratio was obtained using ReviewManager 5 software (the Nordic Cochrane Centre,Copenhagen, Denmark).
July 2013 � Vol 144 � Issue 1 American
The Q statistic was used to identify the heterogeneityacross studies by checking their P values.19 The random-effects model was used when heterogeneity was found(P \0.1); otherwise, the fixed-effects model wasadopted. Considering the low power of Q to detectheterogeneity in small samples of studies, we alsoreported the I2 metrics.
Small study effects and publication bias wereevaluated by visually checking funnel plot asymmetryand quantified through the tests of Begg and Mazum-dar20 and Egger et al21 using the STATA software.
To investigate the robustness of the pooled estimate,we performed additional sensitivity analyses based onpotentially influential factors: study quality, samplesize, and age ranges of the subjects.
Journal of Orthodontics and Dentofacial Orthopedics

Subjects (n)(male/female)
Affected (n)(male/female)*
Affected (n) (left only/rightonly/bilateral) Overall prevalence (%) Quality criteria mety
171/190 1/4 – 1.4 1,3,41093/1110 14/20 – 1.5 1,2,3,4
12250/0 221/0 – 1.8 4,510000 87 – 0.9 42200 22 – 1.0 2,4,5531/475 17 – 1.7 1,2,4547/517 14 – 1.3 1,2,4
2664/2795 33 – 0.6 1,2,3,4521/595 6/15 –/–/11 1.9 1,2,3,4368/371 1/5 2/2/2 0.8 1,2,3,4292/161 1/2 – 0.7 1,3,4358/367 24 – 3.3 1,2,3,4
3017/3436 132/197 – 5.1 1,2,3,4391/354 13/14 –/–/12 3.6 1,2,3,4589 10 – 1.7 1,2,3,4828 16 – 1.9 1,2,3,46022 97 – 1.6 1,2,3,4833 26 – 3.1 1,2,3,4
5165/3124 43/30 25/13/35 0.9 1,2,3,4,5290/210 1/1 – 0.4 2,3,4
0/1500 0/20 – 1.3 1,2,3,4,52393 89 – 0.4 2,3,4405 4 0/3/1 1.0 2,4,57886 11/14 –/–/6 0.3 2,3,4625/723 3/6 3/2/4 0.7 1,2,3,4,5435 33 – 7.5 2,3,4
572/551 11/18 –/–/21 2.6 1,2,3,41045 24 – 2.3 1,2,4,5302/363 7/8 –/–/5 2.3 2,4,546/65 5/6 2/0/9 9.9 1,4
204/211 3/5 4/2/2 1.9 1,2,3,4106/161 5/15 4/3/13 7.5 1,2,3,4429/510 16 – 1.7 1,2,3,4124/446 31 –/–/24 5.4 1,2,3,4
1225/1940 23/45 23/11/34 2.1 1,2,3,41385/1658 22/24 –/–/26 1.5 1,2,4
Table III. Continued
Hua et al 101
RESULTS
Figure 1 shows the selection process. The searchesinitially yielded 3337 records (3318 from electronicsearches, 19 from hand searches). However, afterapplication of the inclusion and exclusion criteria, only30 articles from 17 countries comprising 87,172 subjectsremained (Table III).1-4,11,12,15,16,22-43 In studies thatincluded multiple samples of subjects, only those thatmet our inclusion criteria were used. Three surveysconcerned 2 different populations and were thus splitinto 6 substudies.1-3 Another study regarding 4 ethnicgroups was divided into 4 substudies.27 Therefore, thismeta-analysis included 36 study and substudy sampleson which the following research was based.
American Journal of Orthodontics and Dentofacial Orthoped
Characteristics and quality assessments of allincluded studies are shown in Table III. The articles inthis meta-analysis generally reported the number andsex of affected participants, the corresponding samplesize, and the sidedness of the peg-laterals. Three typesof population were involved in the included surveys:general populations (mainly schoolchildren and collegestudents), dental patients (outpatients who visiteddental clinics or hospitals), and orthodontic patients(those who received orthodontic treatment). When wecompared the potential impact of races, the studiescould be divided into 4 groups: black, white, Mongoloid,and Indian according to a published grouping method.10
In general, the overall quality of all included studieswas medium (Table III). Among the 36 studies and
ics July 2013 � Vol 144 � Issue 1

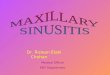
Fig 2. Summary of peg-lateral prevalence according to population type. Black diamonds representpeg-lateral prevalence in each study; horizontal lines indicate 95% CI; unfilled diamonds representpooled prevalence of each population or the overall meta-analysis; dashed vertical line indicates theoverall prevalence estimate.
102 Hua et al
substudies, 3 were low quality, 3 were high quality, andthe rest were medium quality.
The authors of 7 studies failed to report the ages ofthe subjects.2,34,38,39,42,43 Three other studies gave noclear evidence of using radiographs as an aid fordiagnosis and included children whose ages were lessthan 8 years.28,35,40 Since the average ages forpermanent lateral incisors to develop complete crownsand emerge are usually 5.5 and 8.25 years,respectively, the inclusion of these studies might havecaused a selection bias in this analysis.44
In 3 studies, the sample sizes were relatively small(under 500 for the general population study, under200 for the patient study); this might have compromisedtheir representativeness of the underlying
July 2013 � Vol 144 � Issue 1 American
population.4,32,36 On the other hand, the sample sizesof 2 studies were too large (beyond 10,000), causingthe danger of overlooking affected subjects andtherefore underestimating the prevalence rates.28,39
The inclusion of studies with improper sample sizescan lead to information bias.
The pooled overall prevalence of peg-laterals in thisanalysis was 1.8% (95% CI, 1.5-2.1) (Fig 2).
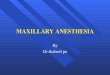
The pooled estimates according to race andpopulationtype are presented in Table IV, which also shows theheterogeneity and significance information of eachsubgroup. The occurrence rate of peg-laterals amongMongoloid subjects (3.1%; 95% CI, 1.9-4.3) was signifi-cantly higher than that of black (1.5%; 95% CI, 1.1-1.9)and white (1.3%; 95% CI, 1.0-1.6) subjects (Fig 3).
Journal of Orthodontics and Dentofacial Orthopedics

Table IV. Prevalence of peg-shaped maxillary lateral incisors in different races and populations
Race PopulationCases/total
(number of studies) Pooled estimate (%) 95% CI
Heterogeneity Significance
I2 P value Z P valueBlack* G 39/2564 (2) 1.5 1.0-2.0 0.0% 0.881 6.22 0.000
DP 4/405 (1) 1.0 0.0-2.0 – –
Ortho 15/665 (1) 2.3 1.2-3.4 – –
Subtotal 58/3634 (4) 1.5 1.1-1.9 0.0% 0.401 7.45 0.000White G 613/46605 (12) 1.1 0.8-1.4 88.2% 0.000 7.51 0.000
DP 49/8931 (2) – – – 1.25 0.212Ortho 169/7940 (6) 2.3 1.4-3.2 79.1% 0.000 5.29 0.000Subtotal 831/63476 (20) 1.3 1.0-1.6 92.5% 0.000 8.61 0.000
Mongoloid G 522/16059 (5) 2.7 1.4-4.1 95.9% 0.000 3.94 0.000DP 42/1810 (2) – – – 1.17 0.241Ortho 31/570 (1) 5.4 3.5-7.3 – –
Subtotal 595/18439 (8) 3.1 1.9-4.3 96.0% 0.000 5.23 0.000Indian G 2/500 (1) 0.4 �0.2-1.0 – –
DP 29/1123 (1) 2.6 1.7-3.5 – –
Subtotal 31/1623 (2) – – – 1.33 0.182Overall G 1176/65728 (22) 1.6 1.2-2.0 94.4% 0.000 8.32 0.000
DP 124/12269 (6) 1.9 0.9-2.8 93.4% 0.000 3.83 0.000Ortho 215/9175 (8) 2.7 1.9-3.5 81.7% 0.000 6.28 0.000Total 1515/87172 (36) 1.8 1.5-2.1 94.5% 0.000 11.03 0.000
G, General population; DP, dental patients; Ortho, orthodontic patients.*Effect size pooled with fixed-effects model.
Hua et al 103
The prevalence values in the general population,dental patients, and orthodontic patients were pooledat 1.6% (95% CI, 1.2-2.0), 1.9% (95% CI, 0.9-2.8), and2.7% (95% CI, 1.9-3.5), respectively. Because ofinsufficient data, pooled prevalence values for the Indianrace and dental patients of white and Mongoloidethnicities were not obtainable (z-value, P .0.05).
For investigations on the impact of continent oforigin, difference between sexes, and prevalence byside, not all studies could be used due to insufficientinformation. In studying the impact of continent oforigin among general populations of the same race, theprevalence for Mongoloid people in Asia (3.2%; 95%CI, 0.8-5.5) was found to be a little higher than thatfor Mongoloid people in North America (2.0%; 95% CI,1.3-2.8), and the prevalence for white people in Europe(1.2%; 95% CI, 0.8-1.6) was also slightly higher thanthat for North American white people (0.9%; 95% CI,0.7-1.1) (Table V).
Comparison of peg-lateral prevalence valuesbetween the sexes in the general population is presentedin Figure 4. The prevalence values for female subjectswere significantly higher than for male subjects(risk ratio, 1.35; 95% CI, 1.13-1.61).
The prevalence of unilateral peg-laterals (0.8%; 95%CI, 0.6-1.0) was found to be the same as for bilateralpeg-laterals (0.8%; 95% CI, 0.5-1.1). Among the unilat-eral peg-laterals, left-side ones (0.4%; 95% CI, 0.2-0.6)were twice as common as right-side ones (0.2%; 95%
American Journal of Orthodontics and Dentofacial Orthoped
CI, 0.1-0.3). In addition, contralateral lateral incisor hypo-dontia was present in 55.5% (95% CI, 29.2-81.9) of thesubjects affected with unilateral peg-laterals (Table VI).
Although asymmetry was found in the funnel plot(Fig 5), the tests of Begg and Mazumdar20 (P 5 0.929)and Egger et al21 (P 5 0.106) showed no evidence ofpublication bias.
Because of the significant heterogeneity amongthe studies, a sensitivity analysis was conducted,and it turned out to be robust. Three studies were as-sessed to be low quality in the quality assessment. Weexcluded them, and the pooled prevalence estimatewas 1.8% (95% CI, 1.5-2.2), nearly the same as theestimate when these 3 studies were included. To in-vestigate the potential impact of improper samplesize, we excluded 5 studies whose sample sizes wereeither too large or too small, and the pooled estimate(1.9%; 95% CI, 1.5-2.2) was not different from thepooled overall prevalence in this meta-analysis. Like-wise, after we excluded 10 studies with improper ageranges, the pooled estimate became 2.0% (95% CI,1.6-2.5), and still no significant difference wasfound.
DISCUSSION
This meta-analysis provides insight into the epidemi-ologic characteristics of peg-laterals; this informationmight be helpful in not only discovering the geneticand environmental causes for peg-lateral occurrence,
ics July 2013 � Vol 144 � Issue 1

Fig 3. Peg-lateral prevalence according to race and population type. Vertical lines indicate 95% CI.
Table V. Prevalence of peg-shaped maxillary lateral incisors of the same race in general populations but differentcontinent of origin
Race ContinentCases/total
(number of studies) Pooled estimate (%) 95% CI (%)
Heterogeneity Significance
I2 P value Z P valueWhite Europe 421/33834 (8) 1.2 0.8-1.6 89.7% 0.000 6.04 0.000
North America* 83/8878 (2) 0.9 0.7-1.1 54.0% 0.000 9.13 0.000West Asia 109/3893 (2) – – – 1.81 0.070
Mongoloid Asia 383/8376 (4) 3.2 0.8-5.5 96.5% 0.000 2.63 0.009North America 139/7683 (3) 2.0 1.3-2.8 66.5% 0.050 5.12 0.000
*Effect size pooled with fixed-effects model.
104 Hua et al
but also establishing a basic awareness among dentists,especially for those who work in a multiethniccommunity. With the large numbers of subjects, thismeta-analysis might provide conclusive answers toquestions that used to be controversial. Based on theliterature, the overall prevalence rate of peg-lateralswas pooled at 1.8% in our study, indicating that nearly1 in every 55 people is affected worldwide. However,this overall rate should be viewed with caution, since itwas a product of the current publications and reflectsthe main common features of these studies. Compared
July 2013 � Vol 144 � Issue 1 American
with other systematic reviews concerning dentalanomalies, the overall occurrence rate of peg-lateralsin this study was higher than tooth transposition18 andlower than dental agenesis.10
The reported prevalence rates of peg-laterals in thegeneral population ranged from 0.6% in Sweden3 to5.1% in China16; most researchers suggested that thisvariation could be a real difference among ethnicgroups. Stecker et al43 reported that the prevalence ratesof peg-laterals in the Minneapolis and St Paul metropol-itan area of Minnesota were 7.5% and 1.6% for Asians
Journal of Orthodontics and Dentofacial Orthopedics

Fig 4. Forest plot for sex comparison in prevalence of peg-laterals. M-H, Mantel-Haenszel method.
Hua et al 105
and other races, respectively. However, in anothermultiethnic study conducted in Hawaii, the prevalencerate of peg-laterals was significantly higher in thedescendants of Filipinos (3.1%), whereas the prevalencerates in descendants of whites (1.7%), Chinese (1.6%),and Japanese (1.9%) were similar.27 In this meta-analysis, the pooled prevalence rate of peg-laterals inMongoloid people (3.1%) was significantly higher thanthe rates for black (1.5%) and white (1.3%) people.Furthermore, comparing studies from North Americaonly, Mongoloids (2.0%) were significantly moreaffected than white people (0.9%). These rates agreewith the findings of Stecker et al, indicating a potentiallyreal difference betweenMongoloid and the other 2 races.A published method of grouping subjects according torace was referred to in this meta-analysis.10 Pooledprevalence rates for Indian people and some other raceswere unavailable because of few studies; further studiesconcerning the prevalence of peg-laterals in these racesare needed.
Other than genetic factors, some environmentalfactors were also held to be responsible for missing
American Journal of Orthodontics and Dentofacial Orthoped
teeth and reduced tooth sizes.8,45 In a meta-analysisconcerning dental agenesis, the prevalence rate amongthe white population appeared to be lower in NorthAmerica than in Europe and Australia, suggesting thatcontinent of origin could be an underlying environmen-tal determinant.19 Similarly, in our study, the pooledprevalence of peg-laterals for the general populationof white people was higher in Europe (1.2%) than inNorth America (0.9%), and the prevalence amongMongoloids was also higher in Asia (3.2%) than in NorthAmerica (2.0%). These differences, without statisticalsignificance, might suggest some differences in environ-mental factors between North America and the other2 continents. Polder et al10 found that black and whitepeople in North America had similar prevalencerates of dental agenesis. Although the prevalence ofpeg-laterals for black people in North America couldnot be obtained from this analysis, the close pooledoverall prevalence of white (1.3%) and black (1.5%)people might support the findings by Polder et al.Further studies are needed for information about the ex-act environmental factors underlying this phenomenon.
ics July 2013 � Vol 144 � Issue 1

Table VI. Prevalence of peg-shaped maxillary lateral incisor according to sidedness
SideCase/total
(number of studies) Pooled estimate (%) 95% CI (%)
Heterogeneity Significance
I2 P value Z P valueUnilateralLeft only 63/14766 (8) 0.4 0.2-0.6 55.0% 0.038 3.95 0.000Right only* 36/14766 (8) 0.2 0.1-0.3 11.9% 0.339 5.55 0.000Total 188/29914 (15) 0.8 0.6-1.0 82.3% 0.000 6.52 0.000CAMLIy 22/60 (5) 55.5 29.2-81.9 99.8% 0.000 4.14 0.000
Bilateral 205/29914 (15) 0.8 0.5-1.1 89.8% 0.000 5.71 0.000
CAMLI, Contralateral absent maxillary lateral incisor.*Effect size pooled with fixed effects model; yprevalence of a contralateral absent maxillary lateral incisor among unilateral peg-lateral subjects.
Fig 5. Funnel plot for the pooled overall prevalence of peg-laterals.
106 Hua et al
Although it is generally maintained that orthodonticpatients have a greater tendency for dental anomaliesincluding peg-laterals, only a few authors have surveyedpopulations of different types and made direct compar-isons.4,11 Ucheonye and Tokunbo2 found that theprevalence of peg-laterals among orthodontic patients(2.3%) was a little higher than in dental outpatients(1.0%) in Nigeria. A meta-analysis concerning toothtransposition showed an insignificant differencebetween prevalence rates in pupils (0.2%), dentalpatients (0.3%), and orthodontic patients (0.6%).18 Inthis study, interestingly, a similar result was obtained,with the order of peg-lateral occurrence beingorthodontic patients (2.7%), dental patients (1.9%),
July 2013 � Vol 144 � Issue 1 American
and general population (1.6%), with no significantdifference found. Confirming the findings of theforegoing 2 studies, this result might reflect a realrelative relationship between these 3 population typesin their susceptibility to peg-laterals and even otherdental anomalies. However, this susceptibility could bea product of several factors such as the gene pool, andthe physical and psychological treatment need of eachpopulation.
Due to contrasting results in the literature, thedifference in the occurrence rates of peg-lateralsbetween sexes has been a controversy for decades.This meta-analysis, based on enough samples and anintegrated approach, provided a conclusion that women
Journal of Orthodontics and Dentofacial Orthopedics

Hua et al 107
are 1.35 (risk ratio, 95% CI, 1.13-1.61) times more likelythan men to have peg-laterals. This finding is consistentwith that of Polder et al,10 who reported that theprevalence of dental agenesis among women was1.37 (risk ratio, 95% CI, 1.28-1.45) times higher thanthat for men. The significant differences found betweenthe sexes in these 2 studies could become new evidencethat peg-shaped teeth and dental agenesis share thesame mechanism. However, since previous studies havesuggested that peg-shaped teeth are inherited in anautosomal dominant manner, the higher prevalence inwomen found in this meta-analysis might or mightnot explain it genetically. Further studies are needed inthis area.5,6,46
The reports on the prevalence of the sidedness ofpeg-shaped teeth also vary in the literature. Althoughin most studies bilateral peg-shaped teeth were morecommon,34,42 unilateral peg-laterals were morecommon in several surveys.4,30 Hrdlicka47 found a slighttendency for left-sided peg-laterals; Meskin andGorlin34 found a 2-to-1 ratio favoring left-sided peg-shaped teeth and hypodontia. In our meta-analysis,the pooled prevalence rates for unilateral and bilateralpeg-laterals were approximately the same (0.8%), whichis similar to the results of 2 large-sample surveys.12,33
Furthermore, among unilateral peg-shaped teeth,left-sided ones (0.4%) were just 2 times more prevalentthan right-sided ones (0.2%); this coincided with theratio of Meskin and Gorlin. The equal expressions ofbilateral and unilateral peg-laterals, as well as theleft-side tendency, are not fully understood yet.However, the 2-to-1 ratio favoring the left side inpatients with cleft lip and palate might suggest an un-derlying genetic mechanism similar to peg-laterals.48,49
Interpretation of these phenomena needs furtherresearch.
For over 40 years, the literature has been suggestingthat maxillary peg-laterals are caused by the samegenetic mechanism as for agenesis of the maxillarylateral incisors, claiming that microdontia and peg-shaped maxillary lateral incisors should be considereda milder form of the hypodontia phenotype.5,6
However, the prevalence rate of maxillary lateralincisor hypodontia among subjects with unilateralpeg-laterals was rarely reported in the literature. In ourmeta-analysis, the prevalence was estimated at 55.5%(95% CI, 29.2-81.9), which is significantly higher thanthe prevalence of maxillary lateral incisor agenesisin the general population (95% CI, 1.55%-1.78%),indicating that for a person with a unilateral peg-lateral his or her contralateral lateral incisor hasapproximately a 50% chance to be congenitallymissing.10 The current data serve as novel proof in
American Journal of Orthodontics and Dentofacial Orthoped
support of the aforementioned genetic theory regardinghypodontia and peg-shaped teeth. Orthodontists mightwant to pay attention to contralateral lateral incisorhypodontia in treatment planning for patients withunilateral peg-laterals for esthetic reasons.50,51
Although other anomalies have also been reported inthe literature to be associated with peg-laterals, suchas palatally displaced canines52 and tooth transposi-tions,53 their relationship with peg-laterals is beyondthe scope of this meta-analysis.
The limitations of this meta-analysis includedconsiderable heterogeneity and medium quality of theincluded studies, as well as few studies for somesubgroup calculations. Although similar high heteroge-neity among studies is common in systematicreviews concerning the prevalence of certain diseases(I2 5 92.5%-100), every effort to minimize potentialbiases was made in this study.17,18,54,55
Since the prevalence rates of peg-laterals are usuallymentioned in surveys focusing on multiple dentalabnormalities, we used broad search terms for theelectronic searches in several databases and registers. Asupplementary hand search by checking the referencesof the remaining key studies was performed after theinitial article review process. No restrictions for languageor publication date were used. In addition, detailedinclusion and exclusion criteria were developed beforethis study to make sure to include only appropriatearticles. The overall study selection and extractionprocess was accomplished by 2 researchers (F.H. andW.B.) independently, with any difference resolved byconsultation with a third author (H.H.) to reach mutualagreement. When abstracts or full-text articles providedinsufficient information, we contacted the correspond-ing authors. After these efforts, both the tests of Beggand Mazumdar20 (P 5 0.929) and of Egger et al21
(P 5 0.106) showed no evidence of publication bias inthis meta-analysis.
According to Papadopoulos et al18 and Polder et al,10
the possible sources of bias in a meta-analysis for theprevalence of dental anomalies are (1) size of the initialsample, (2) sample origin, (3) focus on a specific type ofanomaly, (4) age at diagnosis, and (5) method of patientevaluation. Further introducing another criterion froma recent study, we established the foregoing qualityassessment system in this meta-analysis.17 The defini-tion of too-small or too-large sample sizes in this studyalso refers to the above-mentioned studies.10,18
However, potential biases with regard to sample originwere not evaluated in the quality assessment but weretreated with subgroup analysis: grouping samplesaccording to races, population types, and continents oforigin. Finally, a subsequent sensitivity analysis, aimed
ics July 2013 � Vol 144 � Issue 1

108 Hua et al
at these specific sources of biases and the low-qualitystudies, turned out to be robust.
CONCLUSIONS
1. Worldwide, nearly 1 in every 55 persons (1.8%) isaffected with peg-laterals.
2. The prevalence of peg-laterals in Mongoloid people(3.1%) is significantly higher than in black (1.5%)and white (1.3%) people.
3. Women are 1.35 times more likely than men to havepeg-laterals.
4. Although unilateral and bilateral peg laterals seemequally common, some left-side predispositionexists among those with unilateral peg-laterals.
REFERENCES
1. Grahn�en H. Hypodontia in the permanent dentition: a clinical andgenetical investigation. Odont Rev 1956;7:1-100.
2. Ucheonye IJ, Tokunbo AA. Prevalence of peg-shaped laterals insouth western Nigeria: a comparison of field and clinic findings.Internet J Dent Sc. Available at: http://archive.ispub.com/journal/the-internet-journal-of-dental-science/volume-8-number-2/prevalence-of-peg-shaped-laterals-in-south-western-nigeria-a-comparison-of-field-and-clinic-findings.html#sthash.LXJoRgXh.dpbst. Ac-cessed October 25, 2011.
3. Thilander B, Myrberg N. The prevalence of malocclusion inSwedish schoolchildren. Scand J Dent Res 1973;81:12-21.
4. Thongudomporn U, Freer TJ. Prevalence of dental anomalies inorthodontic patients. Aust Dent J 1998;43:395-8.
5. Witkop CJ. Agenesis of succedaneous teeth: an expression of thehomozygous state of the gene for the pegged or missing maxillarylateral incisor trait. Am J Med Genet 1987;26:431-6.
6. Alvesalo L, Portin P. The inheritance pattern of missing,peg-shaped, and strongly mesio-distally reduced upper lateralincisors. Acta Odontol Scand 1969;27:563-75.
7. Granat J, Chapelle P. Dental agenesis, hypergenesis and evolution.Paris: Actual Odontostomatol; 1988:31-48.
8. Brook AH. A unifying aetiological explanation for anomalies ofhuman tooth number and size. Arch Oral Biol 1984;29:373-8.
9. Brook AH, Elcock C, Al-Sharood MH, McKeown HF, Khalaf K,Smith RN. Further studies of a model for the etiology of anomaliesof tooth number and size in humans. Connect Tissue Res 2002;43:289-95.
10. Polder BJ, Van'THofMA,Vander LindenFP, Kuijpers-JagtmanAM.A meta-analysis of the prevalence of dental agenesis of permanentteeth. Community Dent Oral Epidemiol 2004;32:217-26.
11. Basdra EK, Kiokpasoglou M, Stellzig A. The Class II Division2 craniofacial type is associated with numerous congenital toothanomalies. Eur J Orthod 2000;22:529-35.
12. Kazanci F, Celikoglu M, Miloglu O, Ceylan I, Kamak H. Frequencyand distribution of developmental anomalies in the permanentteeth of a Turkish orthodontic patient population. J Dent Sci2011;6:82-9.
13. Juki�c J, Skrinjari�c I, Glavina D, Ulovec Z. The prevalence of oral anddental anomalies in children with developmental disturbances.Acta Stomatol Croat 2002;36:79-83.
14. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D,et al. Meta-analysis of observational studies in epidemiology:
July 2013 � Vol 144 � Issue 1 American
a proposal for reporting. Meta-analysis of observational studiesin epidemiology (MOOSE) group. JAMA 2000;283:2008-12.
15. Kositbowornchai S, Keinprasit C, Poomat N. Prevalence anddistribution of dental anomalies in pretreatment orthodonticThai patients. Khon Kaen Univ Dent J 2010;13:92-100.
16. Wu H, Feng HL. A survey of number and morphology anomalies inpermanent teeth of 6453 youths between 17 to 21 years old.Zhonghua Kou Qiang Yi Xue Za Zhi 2005;40:489-90.
17. Cheng JW, Cheng SW, Ma XY, Cai JP, Li Y, Wei RL. The prevalenceof primary glaucoma in mainland China: a systematic review andmeta-analysis. J Glaucoma 2011;22:301-6.
18. Papadopoulos MA, Chatzoudi M, Kaklamanos EG. Prevalence oftooth transposition. A meta-analysis. Angle Orthod 2010;80:275-85.
19. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuringinconsistency in meta-analyses. BMJ 2003;327:557-60.
20. Begg CB, Mazumdar M. Operating characteristics of a rankcorrelation test for publication bias. Biometrics 1994;50:1088-101.
21. Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysisdetected by a simple, graphical test. BMJ 1997;315:629-34.
22. Albashaireh ZS, Khader YS. The prevalence and pattern ofhypodontia of the permanent teeth and crown size and shapedeformity affecting upper lateral incisors in a sample of Jordaniandental patients. Community Dent Health 2006;23:239-43.
23. Al-Hummayani F. Agenesis and malformation of maxillary lateralincisors in Saudi Arabian female students. Egypt Dent J 2005;51:1-6.
24. Altug-Atac AT, Erdem D. Prevalence and distribution of dentalanomalies in orthodontic patients. Am J Orthod DentofacialOrthop 2007;131:510-4.
25. Backman B, Wahlin YB. Variations in number and morphology ofpermanent teeth in 7-year-old Swedish children. Int J PaediatrDent 2001;11:11-7.
26. Basdra EK, Kiokpasoglou MN, Komposch G. Congenital toothanomalies and malocclusions: a genetic link? Eur J Orthod2001;23:145-51.
27. Chung CS, Niswander JD, Runck DW, Bilben SE, Kau MC. Geneticand epidemiologic studies of oral characteristics in Hawaii'sschool children: dental anomalies. Am J Phys Anthropol 1972;36:427-33.
28. Zahn-unterzahl Dolder E. Schweiz Mschr Zahnheilk 1936;46:663-701.
29. Fujita Y, Hidaka A, Nishida I, Morikawa K, Hashiguchi D, Maki K.Developmental anomalies of permanent lateral incisors in youngpatients. J Clin Pediatr Dent 2009;33:211-5.
30. Gupta SK, Saxena P, Jain S, Jain D. Prevalence and distribution ofselected developmental dental anomalies in an Indian population.J Oral Sci 2011;53:231-8.
31. King NM, Tsai JSJ, Wong HM. Morphological and numericalcharacteristics of the southern Chinese dentitions. Part I:anomalies in the permanent dentition. Open Anthropol J 2010;3:54-64.
32. Ling J. A morphometric study of the dentition of 12-year-oldChinese children in Hong Kong [PhD thesis]. Hong Kong: Univer-sity of Hong Kong; 1992.
33. Magnusson TE. Prevalence of hypodontia and malformations ofpermanent teeth in Iceland. Community Dent Oral Epidemiol1977;5:173-8.
34. Meskin LH, Gorlin RJ. Agenesis and peg-shaped permanentmaxillary lateral incisors. J Dent Res 1963;42:1476-9.
35. Nayak P, Nayak S. Prevalence and distribution of dental anomaliesin 500 Indian school children. Bangladesh JMed Sci 2011;10:41-4.
Journal of Orthodontics and Dentofacial Orthopedics

Hua et al 109
36. Onyeaso CO, Oneyeaso AO. Occlusal/dental anomalies found ina random sample of Nigerian schoolchildren. Oral Health PrevDent 2006;4:181-6.
37. Ooshima T, Ishida R, Mishima K, Sobue S. The prevalence ofdevelopmental anomalies of teeth and their association with toothsize in the primary and permanent dentitions of 1650 Japanesechildren. Int J Paediatr Dent 1996;6:87-94.
38. Rantenen A. Yl€aleuan toisen inkisiivin reduktio ilmi€oist€a. FinskaL€ak S€allsk Handl 1955;51:155.
39. Rose C. €Uber die ruckbildung der seitlichen schneidez€ahne desoberkiefers und der weisheitz€ahne im menschlichen gebisse. DtschMschr Zahnheilk 1906;24:255-8.
40. Salem G. Prevalence of selected dental anomalies in Saudi childrenfrom Gizan region. Community Dent Oral Epidemiol 1989;17:162-3.
41. Sawyer DR, Taiwo EO, Mosadomi A. Oral anomalies in Nigerianchildren. Community Dent Oral Epidemiol 1984;12:269-73.
42. Shah RM, Boyd MA, Vakil TF. Studies of permanent toothanomalies in 7,886 Canadian individuals. II: congenitally missing,supernumerary and peg teeth. Dent J 1978;44:265-8, 276.
43. Stecker SS, Beiraghi S, Hodges JS, Peterson VS, Myers SL.Prevalence of dental anomalies in a Southeast Asian populationin the Minneapolis/Saint Paul metropolitan area. NorthwestDent 2007;86:25-8.
44. Proffit WR. Early stages of development. Contemporary orthodon-tics. St Louis: Mosby; 2006. p. 94.
45. Vastardis H. The genetics of human tooth agenesis: newdiscoveries for understanding dental anomalies. Am J OrthodDentofacial Orthop 2000;117:650-6.
46. Finn SB. Anomalies of tooth numbers including peg-shaping. BirthDefects Orig Artic Ser 1971;7:185-93.
American Journal of Orthodontics and Dentofacial Orthoped
47. Hrdlicka A. Further studies of tooth morphology. Am J PhysAnthropol 1921;4:141-76.
48. Gundlach KK, Maus C. Epidemiological studies on the frequency ofclefts in Europe and world-wide. J Craniomaxillofac Surg 2006;34(Supp 2):1-2.
49. Zhou QJ, Shi B, Shi ZD, Zheng Q, Wang Y. Survey of the patientswith cleft lip and palate in China who were funded for surgeryby the Smile Train Program from 2000 to 2002. Chin Med J(Engl) 2006;119:1695-700.
50. Shaw WC. The influence of children's dentofacial appearance ontheir social attractiveness as judged by peers and lay adults. AmJ Orthod 1981;79:399-415.
51. Zachrisson BU, RosaM, Toreskog S. Congenitally missingmaxillarylateral incisors: canine substitution. Point. Am J OrthodDentofacial Orthop 2011;139:434, 436, 438.
52. Peck S, Peck L, Kataja M. Prevalence of tooth agenesis andpeg-shaped maxillary lateral incisor associated with palatallydisplaced canine (PDC) anomaly. Am J Orthod Dentofacial Orthop1996;110:441-3.
53. Papadopoulos MA, Chatzoudi M, Karagiannis V. Assessment ofcharacteristic features and dental anomalies accompanying toothtransposition: a meta-analysis. Am J Orthod Dentofacial Orthop2009;136:301-9.
54. Hwang CK, Han PV, Zabetian A, Ali MK, Narayan KM.Rural diabetes prevalence quintuples over twenty-five years inlow- and middle-income countries: a systematic review andmeta-analysis. Diabetes Res Clin Pract 2012;96:271-85.
55. van der Linde D, Konings EE, Slager MA, Witsenburg M,Helbing WA, Takkenberg JJ, et al. Birth prevalence of congenitalheart disease worldwide: a systematic review and meta-analysis.J Am Coll Cardiol 2011;58:2241-7.
ics July 2013 � Vol 144 � Issue 1