Embed Size (px)
Citation preview

Prevalence of T Wave Alternans in Healthy SubjectsSTEFAN WEBER, HARALD TILLMANNS,∗ and BERND WALDECKER∗
From Deutsches Herzzentrum Munchen and 1. Medizinische Klinik, Klinikum rechts der Isar, TechnischeUniversitat Munchen, Munich and the *Medizinische Klinik I, Justus-Liebig University Giessen, Germany
WEBER, S., ET AL.: Prevalence of T Wave Alternans in Healthy Subjects. Beat-to-beat variations in theamplitude of the T wave (T wave alternans [TWA]) have been associated with malignant ventriculararrhythmias in patients with structural heart disease. TWA has also been observed sporadically in healthypersons during strenuous exercise. Therefore, it was the aim of this study to investigate the prevalenceof TWA in healthy subjects at rest and during exercise. TWA was assessed in 48 healthy volunteers witha mean age of 30 ± 8 years (21–53 years) using the CH2000 system for measurement of microvolt levelTWA. TWA was not observed in any individual at rest. Short transient intervals of TWA were observedduring exercise in five (10.4%) subjects. Sustained TWA was observed in two (4.2%) individuals. In one ofthese two individuals sustained TWA was recorded at heart rates >110 beats/min. In the other TWA wasobserved at an onset heart rate of <110 beats/min, and therefore, was considered alternans positive. Theprevalence of exercise related sustained TWA in healthy, young individuals is low (2.1%). Short transientintervals of TWA were observed in about 10% of healthy volunteers. These transient episodes of TWAhad no clinical impact with respect to a higher vulnerability to ventricular arrhythmias. (PACE 2003;26[Pt. I]:49–52)
T wave alternans, ventricular tachycardia, noninvasive risk stratification
IntroductionPatients with structural heart disease are
prone to develop life-threatening ventricular ar-rhythmias. A number of risk factors like impairedleft ventricular function, reduced heart rate vari-ability, late potentials, spontaneous or inducibleventricular tachycardia, and others have been as-sociated with such arrhythmias. However, none ofthese parameters nor a combination of them pro-vide satisfactory sensitivity, specificity, and posi-tive and negative predictive values to accuratelyidentify (or exclude) later arrhythmia occurrence.
A new stratifying technique is the assessmentof T wave alternations (T wave alternans [TWA])from the electrocardiogram (ECG). TWA means al-ternate beat-to-beat changes of ventricular repolar-ization. Although TWA in its macroscopic formwas first reported by Hering in 1909,1 it has beenregarded for many years as an ECG abnormalitywith no further clinical implications. With the de-velopment and introduction of a sensitive spectralmethod by Adam et al.2 and Smith et al.3 for rou-tine assessment of microvolt level TWA, “micro-scopic alternans” can be detected. TWA is a raterelated phenomenon that can be provoked by exer-cise induced sinus tachycardia.4 Such subtle TWAhas been related to the occurrence of malignantventricular arrhythmias in patients with struc-tural heart disease.2,3,5 Other investigators have
Address for reprints: Stefan Weber, M.D., Deutsches Herzzen-trum Munchen, Lazarettstrasse 36, D – 80636 Munich,Germany. Fax: +49-89-12184593; e-mail: [email protected]
Received August 8, 2001; revised January 21, 2002; acceptedFebruary 14, 2002.
found TWA to be a powerful indicator for recur-rent ventricular tachyarrhythmias in patients withimplanted defibrillators.6 The prevalence of sus-tained TWA in asymptomatic patients after acutemyocardial infarction (AMI) is reported in 15–25%of patients.7,8
TWAs have sporadically been detected in ap-parently healthy persons. However, the prevalenceof rate related TWA in healthy individuals isnot known. Therefore, this study investigates theprevalence of TWA in 48 healthy subjects at restand during exercise.
MethodsAll 48 persons (19 women) were healthy vol-
unteers (30 ± 8 years, 21–53 years) in whom func-tional and structural heart disease was excludedby the clinical history, physical examination, ECGat rest and during exercise, and echocardiographyincluding Doppler imaging (Table I). None of thevolunteers was on a permanent medication.
Assessment of TWA
Rate related TWA was assessed during restand exercise test (bicycle ergometry) using theCH2000 system (Cambridge Heart Inc., Bedford,MA, USA). Specifically designed, low impedancesilver-silverchloride electrodes (HiRes electrodes,Cambridge Heart Inc.) were applied using thestandard leads aVR, aVL, aVF, and V1–V6 andthe Frank orthogonal XYZ leads. These silver-silverchloride electrodes consist of four separatesegments, a center segment and three ring seg-ments. Each electrode can be used to record upto four individual ECG signals. By the use ofan enhancement algorithm the signals can be
PACE, Vol. 26 January 2003, Part I 49

WEBER, ET AL.
Table I.
Volunteers’ Characteristics
N 48Women 19 (40%)Men 29 (60%)Age (years) 30 ± 8 (21–53)LV end-diastolic diameter 50 ± 5 mm (40–59)LV ejection fraction 67 ± 6% (50–80)
LV = left ventricular.
combined to produce a lower noise ECG. This com-posite ECG signal has the same beat morphologywithin a tolerance of 1% in comparison to the ECGsignal recorded from the center segment of theHi-Res electrode alone, but a lower noise level.9The signals were recorded during rest and in-creasing exercise, amplified, filtered with a band-width of 0.05–250 Hz, and digitized at 1,000 Hzwith a 16-bit resolution. After measurements dur-ing normal sinus rhythm at rest, the heart ratewas increased using exercise test. Exercise test-ing started with a workload of 30 W that increasedin steps of 30 W every 3 minutes until an indi-vidual target heart rate of 0.7 × (220 beats/min- age) was reached. By the use of a continuousauditory and visual feedback the pedaling ratewas maintained at one-third (33%) of the heartrate to have a good differentiation between arti-facts caused by the ergometry movements (musclenoise) and the TWA signal (Fig. 1). At the end of theTWA test, off-line analysis of the recorded data wasperformed using the spectral analysis algorithm(version D8).2,3,5,9
A sequence of 128 beats was analyzed to cal-culate a power spectrum. Noise or ectopic beatswere replaced by an average of adjacent beats up
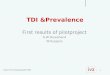
Figure 1. The figure shows a power spectrum obtainedin one of TWA positive volunteers. Using the spectralanalysis method, data are transferred from the time-domain to a frequency-domain. This makes it possibleto differentiate between artifacts and alternans signals.
to a maximum of 10%. The background noise hasto be lower than 1.0 µV at rest and lower than1.8 µV during bicycle ergometry. The alternans ra-tio (k), which provides a measure of the statisticalsignificance of the alternans voltage (Valt) had to be≥3. An alternans test was classified positive whenthere was sustained alternans in any of leads X, Y,Z, VM, or two adjacent precordial leads with analternans voltage (Valt) > 1.9 µV during exerciseor an alternans voltage >1.0 µV at rest with anratio (k) ≥ 3. The criteria for sustained alternansincluded that TWA had to be constantly presentabove individual’s specific heart rate. The onsetof TWA had to be at a heart rate ≤110 beats/min.A test was classified negative if alternans was notobserved during a sustained interval of exercisewith good quality ECG (ectopic beats <10%, noise<1.8 µV).
Follow-Up
All volunteers where followed in 6-month in-tervals for the first year and than in 12-month in-tervals. The follow-up was performed in the out-patient ambulance. Physical examination and ECGwere performed at any time of visits in all individ-uals. In individuals in whom any form of TWA wasdetected, a Holter recording analysis of late poten-tials and heart rate variability was performed af-ter the TWA testing. If these measurements werewithin normal limits these individuals were fol-lowed in the same way as individuals withoutTWA. In individuals with sustained TWA at eachof the follow-up visits, a Holter recording, anal-ysis of late potentials, heart rate variability, andechocardiography was performed.
ResultsAll 48 individuals reached their specific target
heart rate during exercise (i.e., a maximum heartrate of 115 beats/min for ≥1 minute. The noiselevel during rest and exercise was 0.64 ± 0.17 µV(range 0.3–0.9 µV) and 1.15 ± 0.24 µV (range 0.7–1.6 µV), respectively (Table II). TWA was not
Table II.
Parameters of TWA Measurement and Exercise Testing
Noise level at rest 0.64 ± 0.17 µVNoise level during exercise 1.15 ± 0.24 µVHeart rate at rest 80 ± 12 beats/minMax. heart rate during exercise 133 ± 5 beats/minMaximum workload 119 ± 37 WExercise duration 8.2 ± 2.6 minutes
TWA = T wave alternans.
50 January 2003, Part I PACE, Vol. 26

ALTERNANS IN HEALTHY SUBJECTS
Figure 2. Panel A shows an example of a negative alternans test (no alternans detected). Panel B shows an alternanstest with an onset of TWA < 110 beats/min (volunteer A). Panel C shows an alternans test with an onset of TWA >
110 beats/min (volunteer B). The alternans voltage is shown in each lead by the gray shaded area. The black bar underthe curve indicates that all parameters that may obscure alternans or produce a false-positive alternans test such asnoise, ectopic beats, fast heart rate changes or respiration, are within normal limits.
observed in any individual at rest. Some form ofexercise related TWA occurred in 7 (14.6%) of 48subjects. Five (10.4%) of 48 subjects had short tran-sient intervals of TWA with a duration of 2.3 ±1 minutes (range 1.5–3.5 minutes), which werenot constantly observed above the patient’s spe-cific onset heart rate and did not meet the criteriafor sustained TWA. None of this group had abnor-mal findings in Holter recordings performed afterTWA analysis. The analysis of late potentials andheart rate variability were within normal limits inall five individuals. So further follow-up was per-formed in the same way as in individuals with-out TWA. In 2 (4.2%) of 48 subjects there wassustained TWA detectable with onset heart rates108 beats/min (volunteer A) and 118 beats/min(volunteer B), respectively (Fig. 2). According tothe criteria described in Methods (Valt > 1.9 µV,ratio [k] ≥ 3, onset heart rate ≤ 110 beats/min) onlyone of these individuals fulfilled criteria for a pos-itive TWA test. Thus, 1 (2.1%) person of the 48 hadpositive TWA. Both individuals with sustainedTWA had no arrhythmias during Holter monitor-ing and no late potentials on the signal-averagedECG. However, in both individuals the analysis ofheart rate variability showed slightly reduced val-
ues of the rmssd parameter (rmssd 10 and 16 ms,respectively), whereas the SDNN parameter waswithin normal limits in both individuals. These re-sults were constantly found at repeated visits dur-ing 36-month (volunteer A) and 32-month (volun-teer B) of follow-up. During a mean follow-up of30 ± 8 months (range 12–40 months), none of the48 volunteers developed arrhythmia morbidity.
DiscussionThe aim of the study was to determine the
prevalence of the TWA in healthy individuals andit is the first study to systematically assess theprevalence of TWA in healthy and arrhythmia-free subjects. The study found a low prevalenceof TWA (1/48 [2.1%]) using the strict criteriadescribed in Methods. Forty-seven healthy andarrhythmia-free subjects had no sustained TWA atheart rates <110 beats/min at rest or during exer-cise induced sinus tachycardia.
One individual developed sustained TWA ata heart rate of 118 beats/min which was beyondthe cut-off point of 110 beats/min, and therefore,was not classified positive. No other subject de-veloped sustained TWA at even higher heart rates.Therefore, an arbitrary cut-off rate of 110 beats/min
PACE, Vol. 26 January 2003, Part I 51

WEBER, ET AL.
above which TWA is regarded as “physiologic”needs to be reconsidered. Interestingly, both sub-jects in whom sustained alternans could be de-tected had a reduced rmssd value in the analysis ofheart rate variability, whereas the SDNN value waswithin normal limits. This finding was present inall follow-up visits. Whether there is any link be-tween the rmssd parameter and TWA needs furtherinvestigation. No symptoms of arrhythmias werereported by these individuals with positive TWAand no arrhythmias were found in any of the Holterrecordings during follow-up. Both individuals hadno familial history with respect to ventriculararrhythmias.
Sporadic, unsustained TWA was observed in5 of 48 individuals. These short transient intervalsof TWA have never been observed in any study tobe predictive to a higher vulnerability to ventricu-lar arrhythmias. However, the authors could spec-ulate that the short transient episodes of TWA may
be related to changes in the autononmic nervoussystem during exercise testing.
Study LimitationsThe study has two limitations. First, with re-
spect to the low prevalence of TWA in healthy vol-unteers the number of individuals tested is rela-tively small.
Second, all individuals studied were young(range 21–53 years) and had no structural heartdisease and no history of arrhythmias. So it is dif-ficult to extrapolate data to individuals of moreadvanced age.
ConclusionThe prevalence of exercise induced TWA in
healthy, young persons is low (2.1%). The valueof a positive test in healthy subjects needs furtherinvestigation to establish a link between TWA andventricular tachyarrhythmias.
References1. Hering E. Experimentelle Studie an Saugetieren uber das Elektrokar-
diogramm. Zeitschrift f.exp. Pathologie u.Therapie 1909; 7:363–378.
2. Adam R, Akselrod S, Cohen RJ. Estimation of ventricular vulner-ability to fibrillation through T-wave time series analysis. ComputCardiol 1981.
3. Smith M, Clancy EA, Valeri CR, et al. Electrical alternans and cardiacelectrical instability. Circulation 1988; 77:110–121.
4. Kavesh G, Shorofsky Sarang SE, et al. Effect of heart rate on T wavealternans. J Cardiovasc Electrophysiol 1998; 9:703–708.
5. RosenbaumS, Jackson LE, Smith JM, et al. Electrical alternansand vulnerability to ventricular arrhythmias. N Engl J Med 1994;330:235–241.
6. Hohnloser H, Klingenheben T, Zabel M, et al. T wave alternans as a
predictor of recurrent VT in ICD Recipients: Prospective comparisonwith conventional risk factors. J Cardiovasc Electrophysiol 1998;9:1258–1268.
7. Schwab JO, Weber S, Schmitt H, et al. Incidence of T wave alter-nation after acute myocardial infarction and correlation with otherprognostic parameters: Results of a prospective study. PACE 2001;24:957–961.
8. Tapanainen JM, Still AM, Airaksinen KE, et al. Prognostic signif-icance of risk stratifiers of mortality, including T wave alternans,after acute myocardial infarction: Results of a prospective follow-up study. J Cardiovasc Electrophysiol 2001; 12:645–652.
9. Albrecht P, Arnold J, Krishnamachari S, et al. Exercise recordingsfor the detection of T wave alternans. Promises and pitfalls. J Elec-trocardiol 1996; 29(Suppl.):46–51.
52 January 2003, Part I PACE, Vol. 26