Embed Size (px)
Citation preview

Prevalence, prevention and addressing hypoglycaemia

Why address hypoglycemia in diabetes?
• Reducing HbA1c levels associated with prevention or delay in complications and death
• Hypoglycemia is a limiting factor in achieving glycaemic targets
• Hypoglycemia is associated with morbidity and rarely even be fatal
• Optimizing glycaemic control is of obvious importance:• $376 billion USD spent to treat diabetes and its
complications in 2010; hypoglycemia is cost-intensive
• 6.8% of global all-cause mortality attributed to diabetes in 2010 (4 million deaths)
Cryer et al 2003. Diabetes Care; 26,6: 1902-1912 IDF Diabetes Atlas 4th ed., 2009
Roglic and Unwin 2010. Diabetes Research and Clinical Practice; 87: 15-19

Symptoms of Hypoglycemia
• Neurogenic (ANS) Symptoms• (Caused by Falling Glucose
Level)• Shakiness• Trembling• Anxiety• Nervousness• Palpitations• Clamminess• Sweating• Dry mouth• Hunger• Pallor• Pupil dilation
• Neuroglycopenic Symptoms• (Caused by Brain Neuronal Glucose• Deprivation)• Abnormal mentation• Irritability• Confusion• Difficulty in thinking• Difficulty speaking• Paresthesias• Headaches• Stupor• Seizures• Coma• Death (if untreated)

Sequalae of hypoglycaemia
• Mild symptomatic hypoglycaemia • No direct serious clinical effects • May impair subsequent hypoglycaemia awareness
• Severe hypoglycaemia associated with• Stroke and transient ischaemic attacks• Memory loss/cognitive impairment• Myocardial infarction• Injury (direct/indirect)• Death

Hypoglycemia unawareness
• Patients with long-standing diabetes and onomic neuropathy, might not subjectively sense symptoms of hypoglycemia even in the presence of low glucose concentrations
• Glycemic targets of therapy should be adjusted upward in these patients because they are at particularly high risk for hypoglycemia

Hypoglycemia RiskFactors• Missed or delayed meal
• Eating less food at a meal than planned
• Vigorous exercise without carbohydrateCompensation
• Taking too much diabetes medicine (e.g., insulin, insulin secretagogues, and meglitinides)
• Drinking alcohol

SU should be discontinued
• There is evidence of feedback by exogenous insulin upon endogenous insulin secretion
• Combining insulin and SU in patients with significant residual endogenous insulin secretion might incur a high risk of hypoglycaemia

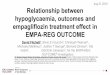
Hypoglycaemia: a barrier to insulin use?
Nakar et al. J Diab Compl 2007;21:220−6
Patients not treated with insulin
Physicians
Insulin makes one fat
Fear of hypoglycaemia
Pain from injection
Pain from blood tests
100
60
2010
504030
0
90
7080
*
**
****
Stu
dy p
art
icip
ants
in
agre
em
en
t (%
)
*p=<0.001, **p=0.01

Keys to addressing hypoglycaemia
• Patient education• Perception vs. reality: rates of hypoglycaemia are much lower in type 2
patients than type 1 patients, even on intensified insulin therapy
• Educate patients to properly self-monitor blood glucose (SMBG); actively monitoring BG to mitigate fear of hypoglycaemia
• Regimen selection and dosage• Physicians must tailor insulin therapy to the patient, while considering
glycaemic level and patient feedback
• Choice of insulin• Modern insulin analogues incur less hypoglycaemia at equivalent levels
of glycaemic control, thus offering the possibility of titrating more safely to target
Korytkowski M. Int J Obes Relat Metab Disord 2002;26:S18–S24
Danne T. MedscapeCME Diabetes & Endocrinology, 2009-09-21

Tips for Preventing Hypoglycemia• If blood glucose is < 70 mg/dl, give 15–20 g of quick-
acting carbohydrate (1–2 teaspoons of sugar or honey, 5–6 pieces of hard candy
• glucose gel or tablets as directed, or 1 cup of milk).• Test blood glucose 15 minutes after treatment. If it
is still < 70 mg/dl, re-treat with 15 g of additional carbohydrate.
• Keep glucagon injection kit available for patients who are unconscious or unable to take in oral carbohydrate

Treatment hints
• Intravenous glucose (25 g) should be given if the patient is unable or unwilling to take carbohydrates orally.
• If intravenous therapy is not practical, subcutaneous or intramuscular Glucagon can be used.
• This treatment raise plasma glucose concentrations only transientlytransiently, and patients should therefore be urged to eat as soon as is practical to replete glycogen stores.

Changing the dose: some general rules
Combating hypoglycaemia
• Reduce insulin dose by at least 20% and review after 1 week
• Preventing hypoglycaemiaPreventing hypoglycaemia takes priority over correcting hyperglycaemiacorrecting hyperglycaemia
http://www.rcn.org.uk/__data/assets/pdf_file/0009/78606/002254.pdf

HYPOGLYCAEMIA & MODERN INSULIN
Do modern insulins offer any advantages over traditional insulins?

NovoMix® 30 effectively reduces HbA1c in T2 patients; low hypo rates
OnceMix, Strojek et al 2009. Curr Med Res Opin; 25; 2887-941-2-3 Garber A et al. Diab Obesity Metab 2006; 8(1):58-66
EUROMIX, Kann et al. Exp Clin Endocrinol Diabetes 2006; 114:527-532REFORM Lund S et al. BMJ 2009;339: 2-11
INITIATE Raskin P et al. Diabetes Care 2005; 28:260-5ACTION Raskin et al. Diabetes Obes Metab. 2009 Jan; 11(1):27-32PREFER Liebl et al. Diabetes Obes Metab. 2009 Jan; 11(1):45-52

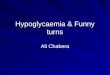
Aspart (NovoRapid®) maintains glycaemic control†: 3-year data...
Home et al. Diabetes Res Clin Pract 2006;71:131–9
8.5
8.0
7.5
0
HbA
1c
(%)
Months0 6 12 18 2
430 36
*
p=0.035 at 30 months
n=753
Insulin aspart (IAsp)Human insulin (HI)
† Study conducted in patients with T1 diabetes

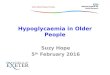
…and incurs a low risk of hypoglycaemia
Hypoglycaemia rate (event/patient-month)
RR (IAsp/HI) [95% CI], p-value
IAsp HI
Major 0.08 0.08 1.00 [0.72–1.39] NS
Minor 2.46 2.03 1.24 [1.09–1.39] p=0.02
Despite significant differences in glycaemic control, the risk of major hypoglycaemia did not
differ between the two treatments†
Home et al. Diabetes Res Clin Pract 2006;71:131–9
†Study conducted in patients with T1 diabetes;IAsp = NovoRapid®

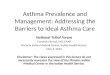
Aspart significantly reduced major nocturnal hypoglycaemia vs. HI†
0
0.5
1
1.5
2
2.5
3
Totalevents
Nocturnalevents
Diurnalevents
Hypogly
caem
ia e
vent
rate
(even
ts/p
ati
ent/
year)
Heller et al. Diabet Med 2004;21:769–75
IAsp
HI
n=155
72%* risk reduction with insulin aspart
† Study conducted in patients with T1 diabetes* P = 0.001

Modern analogues incur fewer hypos at equivalent levels of glycaemic control
• Hypoglycaemia is a major perceived barrier to insulin use for patients and physicians
• Modern insulin analogues incur less hypoglycaemia at equivalent levels of glycaemic control, thus offering the possibility of titrating more safely to target
• These findings have been reported both in clinical trials, and in observational studies