Embed Size (px)
Citation preview

PREVENT COMPLICATIONS IN MAJOR SURGERY
Dept of Anesthesia and ICM
(Prof. G. Della Rocca)
Azienda Ospedaliero-Universitaria
University of Udine. Udine, Italy

Crit Care Med 1982;10(6):398-403
CLINICAL TRIAL OF SURVIVORS’ CARDIORESPIRATORY PATTERNS AS THERAPEUTIC GOALS IN CRITICALLY ILL POSTOP PTS
Shoemaker WC, Appel Pl, Waxmax K

Crit Care Med 1982;10(6):398-403
CLINICAL TRIAL OF SURVIVORS’ CARDIORESPIRATORY PATTERNS AS THERAPEUTIC GOALS IN CRITICALLY ILL POSTOP PTS
Shoemaker WC, Appel Pl, Waxmax K

Critical Care 2006, 10:R81

Exclusion criteria: endoscopyday-case surgcardio-thoracneurosurgorgan txobstetricsburns
From Jan 1999 to Oct 2004 (70 months)
94 Hosp in UK
All surgical procedures (HRG)
n = 4 117 727
Critical Care 2006, 10:R81

Critical Care 2006, 10:R81

Critical Care 2006, 10:R81

Critical Care 2006, 10:R81

Critical Care 2006, 10:R81

Critical Care 2006, 10:R81

• Renal: fluids!!! (fenoldopam?)
• Infections: sepsis



Critical Care 2005; 9:R687-693
RCT, HR surgical patients (n=122 pts)
DO2I 600 mL min-1 m-2 vs conventional management
Cardiac Output (LidCO System)
60 days
SVI/DO2I

Critical Care 2005; 9:R687-693

Critical Care 2005; 9:R687-693

Critical Care 2005; 9:R687-693

Critical Care 2005; 9:R687-693

Anesthesiology 2002; 97:820-826
Goal-directed Intraoperative Fluid Administration Reduces Lenght of Hospital Stay after Major Surgery.
TJ Gan, A Soppitt, M Maroof, H El-Moalem, KM Robertson, E Moretti, P Dawne, PS Glass
FTc

Anesthesiology 2002 ; 97: 820-6
Goal-directed Intraoperative Fluid Administration Reduces Lenght of Hospital Stay after Major Surgery.
TJ Gan, A Soppitt, M Maroof, H El-Moalem, KM Robertson, E Moretti, P Dawne, PS Glass

Anesthesiology 2002 – Gan et al.
Anesthesiology 2002 ; 97: 820-6
Goal-directed Intraoperative Fluid Administration Reduces Lenght of Hospital Stay after Major Surgery.
TJ Gan, A Soppitt, M Maroof, H El-Moalem, KM Robertson, E Moretti, P Dawne, PS Glass

Wakeling HG et al BJA 2005; 95(5): 634-42
SV vs CVP:
decreased LOS and complications

Preop eval Surgery ICU discharge Hospital discharge
High Risk patientsdefinition
OPTIMIZATION∆ outcome
High risk population“Supposed” normal goals ≠ “supranormal” goals
PERIOP HEMODYNAMIC OPTIMIZATION

DO2 = CO x CaO2
PERIOP HEMODYNAMIC OPTIMIZATION
(CVP, SV,ABF-FTc, SvO2, Lac, dynamic indexes)
(AP, HR, diuresis)
(DO2 >600 mL/min/m2)


Anesth Analg 2005;100:1093-106

Anesth Analg 2005;100:1093-106
How should fluid be administered

“SUPPOSED” NORMAL GOALS


Cardiac surgeryCardiac surgery

Orthopedic surgeryOrthopedic surgery

Major abdominal surgeryMajor abdominal surgery

Br J Anesth 2007;99:500-8
n = 32 prospective study
Liberal fluid regimen:
transiet pulmonary improvement but postop Hypoxiemia
tendency to deacrease in morbidity

Br J Anesth 2007;99:500-8

Br J Anesth 2007;99:500-8

Br J Anesth 2007;99:500-8

Vasc Endovasc Surg 2008;June 25
Retrospective Study
n = 41 divided in 2 groups: < 3L vs >3L intraop
- Restricted regimen: <LOS (MV?) ICU and Hospital
- No difference in morbidity

Vasc Endovasc Surg 2008;June 25

Eur J Vasc Endovasc Surg 2007;34:522-7
Conclusion: more fluids more complications!
n = 100: retrospective study

Eur J Vasc Endovasc Surg 2007;34:522-7

Intraoperative fluid management duringorthotopic liver transplantation
RA Schroeder, BH Collins, E Tuttle-Newhall, K Robertson, J Plotkin, LB Johnson, PC Kuo
J Cardiothorac Vasc Anesth 2004;18(4): 438-441
2 liver transplant centers experience
low CVP method vs normal CVP method
clinical safety of a low CVP fluid management strategy in
patients undergoing Ltx

J Cardiothorac Vasc Anesth 2004;18(4): 438-441
“despite sussess in lowering blood transfusion requirements in liver
resection patients, a low CVP should be avoided in patients
undergoing liver transplantation”
Intraoperative fluid management duringorthotopic liver transplantation
RA Schroeder, BH Collins, E Tuttle-Newhall, K Robertson, J Plotkin, LB Johnson, PC Kuo

J Cardiothor Vasc Anesth 2008; 22(2):311-4



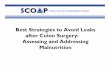
Lobo SM et al Crit Care 2006; 10:R72 (doi:10.1186/cc4913)
“We aimed to investigate the effects of DO2I
optimization,
with and without dobutamine,
on the incidence of perioperative complication
in HR surgical patients”

Lobo SM et al Crit Care 2006; 10:R72 (doi:10.1186/cc4913)
dobutaminevolume

Lobo SM et al Crit Care 2006; 10:R72 (doi:10.1186/cc4913)
dobutamine
volume

Lobo SM et al Crit Care 2006; 10:R72 (doi:10.1186/cc4913)

Lobo SM et al Crit Care 2006; 10:R72 (doi:10.1186/cc4913)
PAC-guided hemodynamic optimization using
dobutamine determines better outcomes,
whereas fluids alone increase the incidence of
postoperative complications in patients with
high risk of perioperative death.
Conclusion
IS SUPRANORMAL DO2 NECESSARY?

Use it only when you need and not only because of protocols….





NIV AND PERIOPERATIVE OPTIMIZATION

Incluison criteria:
ASA I-II
Major abdominal surgery
PaO2/FiO2 < 300 1 hr after extubation
Exclusion criteria:
Cardiac, Respiratory and Obese patients
Recent Major surgery, CT, immunosuppression
Acidosis, hipercapnia (CO2>50 mmHg)
SpO2<80 %
Hypoalbuminemia, renal insufficiency, anemia, ARDS

1 hr after extubation:
CTRL group → 6 h Venti Mask FiO2 0.5
PROT group → 6h CPAP 7.5 cmH2O FiO2 0.5 (Helmet)
After 6 h
1 h Venti Mask FiO2 0.3 and then:
If PaO2/FiO2 < 300→ back to the assigned group
> 300→stop treatment



Preop eval Surgery ICU discharge Hospital discharge
High Risk patientsdefinition
OPTIMIZATION∆ outcome
High risk population“Supposed” normal goals ≠ “supranormal” goals
Postoperative NIV.
PERIOP HEMODYNAMIC OPTIMIZATION

Is ICU postoperative care necessary forHR patients?
Yes but to optimize and not to “monitor” …..


HEMODYNAMIC OPTIMIZATION
Volume/dobutamine/ITBVI (intraop or eary ICU)
(No recent MI-ischemia or ↑ ß-blocker therapy)
Lung protection: EVLWI (early predictor of mortality/latewarning system)
Fast track anesthesia + NIV (if PaO2/FiO2<300)

Renalprotection
Lungprotection


When? Early!