Embed Size (px)
Citation preview

Preventable complications-How to avoid bad outcomes.
Bob WestMercy Hospital Electrophysiology

Disclosure of Relationships
Bob West, B.S., RCVT, CEPS
Still employed!!

Disclosure of RelationshipsParticipated in TTOP trial ………………Ablation Frontiers adverse device complications.Participated in STOP AF trial …………..Arctic Front balloon CryoCathBriefly participated in ENABLE study …………….Cardiofocus Laser balloon study stoppedParticipating in Voltage mapping collection for a novel approach to guided therapy

History of Arrhythmia Ablation
1969: Surgical division of WPW pathways 1982: Catheter ablation using DC shock 1987: Catheter ablation using
radiofrequency energy (RF) ‐ cure of SVT 1992: Catheter RF ablation of atrial flutter 1995: Catheter RF ablation of atrial fibrillation=26 years of RF catheter ablation experience

RF, standard and irrigatedRadiofrequency energy---resistance heats tissue
4mm,5mm,8mm 10mm deeper and wider lesions

Cryo, standard and balloonnitrous oxide freezes tissue

Laser, balloonCardiofocus diode laser

High resolution fluoroscopy

EP 120 channel physiology recorder with programmable stimulator

PVI goal is to electrically isolate the pulmonary veins

Safe and reliable transeptal accessa steerable introducer gives added flexibility for achieving good lesions

INTRA CARDIAC ECHO imaging for Ablation Pre ablation anatomic orientation

Ablation Goals(what is all this stuff for?)
Maximize Success
Reduce Complications

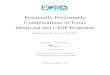
Death as a complication of catheter ablation of atrial fibrillation (AF) occurs in 1 of every 1000 patients
Thirty-one centers reported 32 deaths in 32,569 patients
tamponade (in 8 patients) stroke (5 patients) atrioesophageal fistula (5 patients) massive pneumonia (2 patients).
J Am Coll Cardiol 2009;53:1798-1803,1804-1806

J Am Coll Cardiol 2009;53:1798-1803,1804-1806
32 deaths out of 32,569 patients
tamponade25%
stroke16%
other37%
pneumonia6%
A E fistula16%
avoidable complications

Other 12 deaths includes……..
MI to TEE perforation…………….(Myocardial infarction, intractable torsades de pointes, septicemia, sudden respiratory arrest, extrapericardial pulmonary vein (PV) perforation, occlusion of both lateral PVs, hemothorax, and anaphylaxis caused 1 death each
Asphyxia from tracheal compression secondary to subclavian hematoma, intracranial bleeding, acute respiratory distress syndrome, and esophageal perforation from intraoperative transesophageal echocardiographic probe caused 1 late death each)

Monitor the vital signs---old school!

We routinely monitor femoral artery pressure throughout the PVI procedure
"It is of the utmost importance that tamponade (i.e., the most frequent cause of death in our survey) be recognized promptly, before it is too late."
Dr. Riccardo Cappato from the Policlinico San Donato, Milan, Italy

Have the vital signs changed?Stable hemodynamics Early recognition

Abnormal central Ao pressure
Pulsus paradoxus Tamponade COPD Pulmonary
embolism


Quick action and calm heads
Have equipment for tap available now
Critical to act soon!

Can recent additions to technology improve outcomes?

3-D MappingEnsite Velocity
Current improvement include CT or MRI fusion
Better understanding of anatomic variable
Map arrhythmia real-time and in review
Pinpoint critical path to determine ablation strategy

Ensite with fusion on CT

2009 INVESTIGATION PROCEDURES

RELEASED IN JANUARY 2011 STOP AF trial Cryo balloon Pulmonary vein isolation

Round balloon in an oval/egg shape hole!Some part of the ring will be missed!!

To touch up missed area Freezor Max or RF lesions are used or the Balloon repositioned and repeated

PVI goal is to electrically isolate the pulmonary veins
Pre cryo Post cryo

Esophagus damage after Esophagus damage after PV Isolation with the CryoballoonPV Isolation with the Cryoballoon Catheter
Presented at the Heart Rhythm Society 2008 Scientific Sessions, San Francisco, CA May 14-17.

To date no esophageal fistula has been seen in cryo procedures. NOT true anymore!!!!
Conclusions: This case clearly demonstrates that Cryoballoon ablation can cause esophageal ulceration. Perhaps the absence of atrial-esophageal fistula formation with cryoablation may be related to the post-ablation healing process, rather than an inherent inability of cryoenergy to cause esophageal damage.
Ablation technology by definition causes cellular damage

Fistula causing air embolus to brain

TTOP Linear Ablation Ablation Frontiers

Linear lesions to the roof and Septum Ablation Frontiers

technology to improve outcome

Variation in anatomy
Location, size, branching and number of pulmonary veins
Size and location of atrial appendage Proximity of esophagus to PV antrum Phrenic nerve proximity to ablation site Coronary artery proximity to ablation
site

Location, size, branching and number of pulmonary veins
PA CT of Left atrium Red LA Green distal PV’s White esophagus

Size and location of atrial appendage

Proximity of esophagus to PV antrum

Pulmonary vein ostia are not round

If you know there is a risk
Take every effort to avoid a bad outcome

Phrenic nerve proximity to ablation site
(A)pre ablation (B)phrenic palsy (C)recovery

Sanchez-Quintana found the anterior wall of the RSPV is <2mm from the right phrenic nerve in 32% of their autopsy series

Phrenic nerves are independent

Coronary artery proximity to isthmus ablation site common atrial flutter 68 yo man

Is deeper and wider better? 13 yo maleSTEMI during Posterior wall accessory pathway ablationEarly recognition of a complication is critical ……… emergent coronary stent interrupted this boys MI
Distal RCA occlusion

Is something important near the ablation site?.......... Two reported coronary occlusions in Epstein’s WPW
Incidence of coronary artery injury immediately after catheter ablation for supraventricular tachcardias in infants and children.
Heart Rhythm, Volume 6,Issue 4, Pages 461-467

15 year old male Epstein's anomaly with WPW pacing RV- right side posterior Accessory Pathway is common

RCA 4mm from right atrial endocardial surface

Cryo lesion paint to RCA posterior to Kent bundle
No acute or residual symptoms
Lower Incident of Thrombus Formation With Cryoenergy Versus Radiofrequency Catheter AblationKhairy et al. ,Circulation 2003;107

RF lesion into Venticle

Steam pops?
What causes bubbling and popping? Local heating causes water
content to vaporize High temperature inside tissue causes water vaporization and explosion, which is popping
At high power Inadequate cooling capacity
of irrigation flow High temperature inside tissue, which is not cooled directly by irrigation flow, can cause
popping as well SJM Solution
Controlling the amount of power according to preset temp

Typical rupture of intramyocardial structure due to overheating. Evaporation of tissue liquid led to the formation of gas bubbles that escaped by tearing the endocardium. Visible is a crater discolored by carbonization

What is the future?
built in Safety and a quick arrival at the goal Beautifully engineered

Beautiful simplicity
"Things should be made as simple as possible, but not simpler." — Albert Einstein (1879–1955)

Low voltage bridges occur in both atriums and their veins
LSVC LSVC
RAA

Importance of low voltage bridges
“Ideally, a method to identify abnormal atrial substrate would offer the best chance to understand the underlying atrial disease, as well as, offer the best chance to intervene with ablation.”
Steven J. Bailin, MD Iowa Heart Center

10 patients undergoing AF ablation
Cryo lesions

The ability to map atrial substrate makes apparent the fundamental structures necessary to maintain and propagate AF

In all 10 patients, AF was terminated to sinus rhythm

The voltage gradients as well as high voltage areas were dramatically altered
Voltage pre ablation Voltage post ablation

Published in Europace 19 April 2011 13, 1188–1194Direct visualization of the slow
pathway using voltage gradient mapping: a novel approach for successful ablation of atrioventricular nodal
reentry tachycardia Steven J. Bailin , Matt A. Korthas, Neal
J.Weers, and Craig J. Hoffman

It looks like this is a good tool!AVNRT PW anatomy Voltage guided cryo

Physiologic changes effect conduction








![Front cover [Converted]...the shocking fact that over half a million women die needlessly due to complications related to pregnancy and childbirth. One of the most easily preventable](https://img.pdfslide.net/doc/110x75/60c2af334c9eec448e54fc42/front-cover-converted-the-shocking-fact-that-over-half-a-million-women-die.jpg)