Embed Size (px)
Citation preview
JSP 950 UNCONTROLLED ONCE PRINTED Leaflet 3-3-1
1 Last Revised Jan 13
PREVENTING MALARIA IN MILITARY POPULATIONS Introduction 1. Malaria remains a disease of global importance. World wide, it is estimated that 41% of the population reside in malaria risk areas and between 1.1 and 2.7 million people die from the disease annually. The disease presents a significant threat to travellers, whether recreational or vocational and every year some 2000 people present with the disease in the UK of which some 10 -15 die. Malaria also continues to be a disease of military importance with the outbreak amongst UK troops in Sierra Leone in 2000 generating attack rates of 10% in certain groups. 2. Malaria protection guidelines in the UK have been produced and published by the Health Protection Agency Advisory Committee on Malaria Prevention1. These guidelines are based on a review of the best available evidence for malaria protection interventions and it is upon these that Surgeon General’s (SG’s) malaria prevention policy is built. Aim 3. The aim of this JSP leaflet is to state SG’s policy on preventing malaria in military populations. 4. This JSP leaflet replaces SGPL 10/04 dated 13 May 04, which is cancelled. Policy Development 5. Malaria is a complex disease and a flexible policy is essential in order to provide the best possible protection. There are local variations in transmission rates, even in areas of high endemicity and the different species of Anopheles have different biting habits which impact on disease transmissibility. The 5 parasites that cause malaria (Plasmodium falciparum, P vivax, P ovale, P malariae and P knowlesi) cause disease of different severity and have different levels of resistance to prophylactic drugs throughout the world. There are, however, generic principles that can be applied to the prevention of malaria. 6. Protection follows 4 principles; awareness through education, bite prevention and chemoprophylaxis. The fourth principle, which is specific to the military, is the role of the chain of command in the integration of malaria protection measures into plans and risk assessments. Chain Of Command 7. Whilst the Defence Medical Services acknowledge their ownership of the specialist information that forms the basis of this policy, they have no executive control over its implementation. That responsibility lies with commanders. It may be inevitable that, in order to achieve the mission, a course of action is chosen that precludes complete compliance with the protection measures outlined in this policy letter. 8. The CoC is to identify where compliance cannot be achieved for operational reasons and is to acknowledge the risk that needs to be managed. Under these circumstances it is the responsibility of medical personnel to support the commander fully by developing appropriate contingencies to minimise the effects of any future malarial outbreak. In the context of force
1 Chiodini P, Hill D, Lalloo D, Lea G, Walker E, Whitty C and Bannister B. Guidelines for Malaria Prevention in Travellers from the United Kingdom, 2007. London, Health Protection Agency, January 2007.
JSP 950 UNCONTROLLED ONCE PRINTED Leaflet 3-3-1
2 Last Revised Jan 13
protection, the chain of command is ultimately responsible for the implementation of malarial protection measures but individual compliance is paramount if the policy is to be effective. Awareness and Education 9. Although there has been no evaluation of the effectiveness of awareness education, common sense would suggest that awareness of the risks and knowledge and understanding of the available protective measures should improve compliance. Personnel are to be briefed regularly on the risks of malaria. In particular, they are to be briefed on protective measures before deployment on operations or exercises and the message is to be reinforced whilst deployed. Immediately before leaving the risk zone, they are to be briefed on the need to continue prophylaxis after return, and on the importance of reporting any febrile illness. These briefings are not to be omitted. 10. Areas that are to be covered during force protection briefings are: a. The seriousness of malaria - it can and does kill people. b. The fact that malaria can be acquired after just one infected mosquito bite. c. How malaria may be prevented.
d. The fact that compliance with malaria protection policy can offer significant protection against the disease, although not 100% protection.
e. The fact that malaria may have an incubation period ranging from as short as 2 weeks to many months.
f. The common presenting symptoms of malaria - in particular that any feverish illness presenting after potential exposure is to be considered to be malaria until proven otherwise.
g. The fact that the disease is generally less severe if the infection is diagnosed quickly.
h. In relation to specialist occupational groups, any additional issues that are specific to those occupations are also be covered and medical practitioners experienced in the provision of specialist advice for these occupational groups (for example aviation medicine and diving medicine practitioners) are to give the briefings.
Bite Avoidance 11. Bite avoidance measures include the wearing of appropriate clothing in malarial areas, using bed-nets, door and window screens and insecticide sprays. These will, incidentally, reduce the risk of all diseases spread by biting insects. Clothes and bed nets provide better protection if treated with insecticide. 12. Bed nets. Wherever practicable, and whether they are indoors or out of doors, personnel in malaria-endemic areas are to sleep under bed nets (‘mosquito nets’). Insecticide treated bed nets are particularly effective. However, bed nets are only effective if used properly:
a. The bed net is to be checked regularly for holes, and any holes found are to be repaired immediately.
JSP 950 UNCONTROLLED ONCE PRINTED Leaflet 3-3-1
3 Last Revised Jan 13
b. Before retiring at night, the bed net is to be tucked carefully under the camp bed, mattress, sleeping mat or sleeping bag.
c. The inside of the net is to be checked for trapped insects before retiring. Knockdown insecticide should be applied.
d. Personnel are to try to ensure that no part of their body is in contact with the net during the night, as insects will bite through the mesh.
13. Mosquito Screens. In fixed locations, every attempt is to be made to provide mosquito-screened accommodation and as far as operationally practicable, personnel should avoid being outside such accommodation at peak biting times. 14. Clothing. Service personnel are to be reminded that minimising the levels of exposed skin will offer some protection against biting insects including mosquitoes. Long sleeves and long trousers/skirts are to be worn in biting areas at peak biting times. Socks and boots/shoes (not sandals) are to be worn. Greater protection is achieved if clothing is treated with insecticide. 15. Treatment of Bed Nets and Clothing. It is to be normal practice that the routine treatment of bed nets and clothing with Peripel® (a commercial preparation of a pyrethroid insecticide (permethrin) that is effective against mosquitoes) is carried out prior to deployment. The treatment procedure is described in detail in JSP 371, Annex A to Chapter 22. Re-impregnation with Peripel® is to take place every 6 weeks for combat clothing; every 6 months for bed nets. 16. Topical Insect Repellent. The topical application of choice in the military is N, N-diethyl-3-methylbenzamide (DEET). The repellent issued by the UK Armed Forces (Ultrathon®) is a slow-release, polymer-based cream formulation which contains DEET. DEET can damage plastics (e.g. spectacle frames, computer keys) and leather (e.g. watch straps), and care is needed with these items. Personnel should be aware of the following:
a. The Service-approved DEET preparation is effective for up to 12 hours in normal climates, but needs to be re-applied more frequently in hot or humid conditions.
b. DEET is to be applied to all areas of exposed skin, including the face, neck, ears, scalp, wrists, hands and ankles. The aim is to use just enough DEET to lightly cover the skin.
c. Contact of DEET with the eyes, mouth and genitals should be avoided since this may cause local irritation. Palms and fingers should be wiped thoroughly after applying DEET, to prevent the accidental transfer of repellent to eyes, mouth or genitals.
Vector Control 17. The reduction of the vector population at all stages of its life cycle, where operationally possible, remains an essential part of malaria prevention. Instructions and advice are detailed in JSP 371. Only those insecticides and larvicides approved in JSP 371 are to be used. They are only to be issued and used by appropriately trained and authorised personnel. 18. Mosquitoes breed in standing water. All potential breeding sites (e.g. blocked gutters, old tins, discarded tyres, tree stump holes and broken bottles etc.) are to be drained or treated with larvicide on a regular basis.
2 Joint Service Publication (JSP) 371: MOD Manual on Pest Management dated Jun 09.
JSP 950 UNCONTROLLED ONCE PRINTED Leaflet 3-3-1
4 Last Revised Jan 13
19. Tent canvas can hold insecticide effectively and wall spraying of tents is effective against mosquitoes that rest indoors (endophilic). Residual insecticide sprays are most effective if applied following vector assessment, which should be carried out where practicable to ensure that the correct insecticide delivery system is used. Environmental Health staff will provide advice. 20. Thermal fogging is normally used for wide area coverage. However, it is only effective if used frequently to overcome the dispersion of insecticide and applied to areas where vectors are found. It has no effective residual effect and therefore should be used when the vectors are most active. This is dependent on the species involved. 21. It is essential that unit commanders serving in malaria-endemic regions have access to appropriate Environmental Health advice through personnel trained in Combat Health Duties (CHD), Combat Health Advisers (CHA) or through Environmental Health Technicians or Officers. Detailed advice on mosquito control, including information on CHD and CHA courses, is to be found in JSP 371. Chemoprophylaxis 22. Chemoprophylaxis refers to the use of drugs to prevent malaria. In the UK Armed Forces, chemoprophylaxis policy is based on the guidelines at Footnote 1, which has evaluated a wide range of evidence in order to make its recommendations concerning the efficacy of chemoprophylactic drugs. 23. Responsibility – Issue of Instructions Concerning Chemoprophylaxis. The responsibility for issuing instructions regarding malaria chemoprophylaxis is as follows: a. Joint Service Exercises and Operations.
(1) The Permanent Joint Headquarters (PJHQ) is to issue an instruction on malaria chemoprophylaxis for all joint or potentially joint deployments to geographic regions where malaria presents a risk to health. PJHQ J4 Med Staff are to carry out an area-specific risk assessment, and to determine the most appropriate anti-malaria drug regimen. Specialist advice is available from the SO1 CDC at HQ SG.
(2) PJHQ’s instruction is then to be included in the Medical Warning Notice, and subsequently in the Medical Annex to Chief of Joint Operations (CJO) directive, issued to single Service commands and to the Joint Task Force Commander, who are responsible, thereafter, for implementing the chemoprophylaxis instruction.
b. Joint Service Exercises and Operations – RN Participation. Since RN ships tasked to participate in Joint Service exercises or operations will frequently be subject to pre-existing, single Service instructions to take chemoprophylaxis for a different geographical area, PJHQ J4 Med Staff are to consult the PH Consultant at NCHQ on the question of malaria chemoprophylaxis at an early stage of its medical planning.
c. Single Service Exercises. For single Service exercises and operations, it is a single Service Command responsibility to issue an instruction on malaria chemoprophylaxis. This is to be done only after a careful area-specific risk assessment has been carried out and discussed with single Service Public Health specialists. If required, further specialist advice is available from HQ SG SO1 CDC via the CoC through single Service medical directorates.
JSP 950 UNCONTROLLED ONCE PRINTED Leaflet 3-3-1
5 Last Revised Jan 13
d. Travel for Holiday Purposes. Recreational travel medicine is a separate discipline and is not covered by this policy. Advice on prescribing anti-malaria drugs for holiday purposes is to be obtained from the UK National Travel Health Network and Centre (NaTHNaC; telephone +44 (0)845 602 6712 or online at: http://www.nathnac.org/pro/index.htm). The Malaria Reference Laboratory also provides advice by fax on 020 7637 0248 using the form found at http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1244763931077.
e. Military Diplomacy. Personnel selected for military diplomatic posts are to use this policy to inform their initial preparations for deployment. They are to take into account any additional information provided to them by the Foreign and Commonwealth Office. Family members of personnel selected for military diplomatic posts are to consult with their own primary care physicians or with travel medicine clinics for current advice concerning malarial risks in the country in which they will be resident.
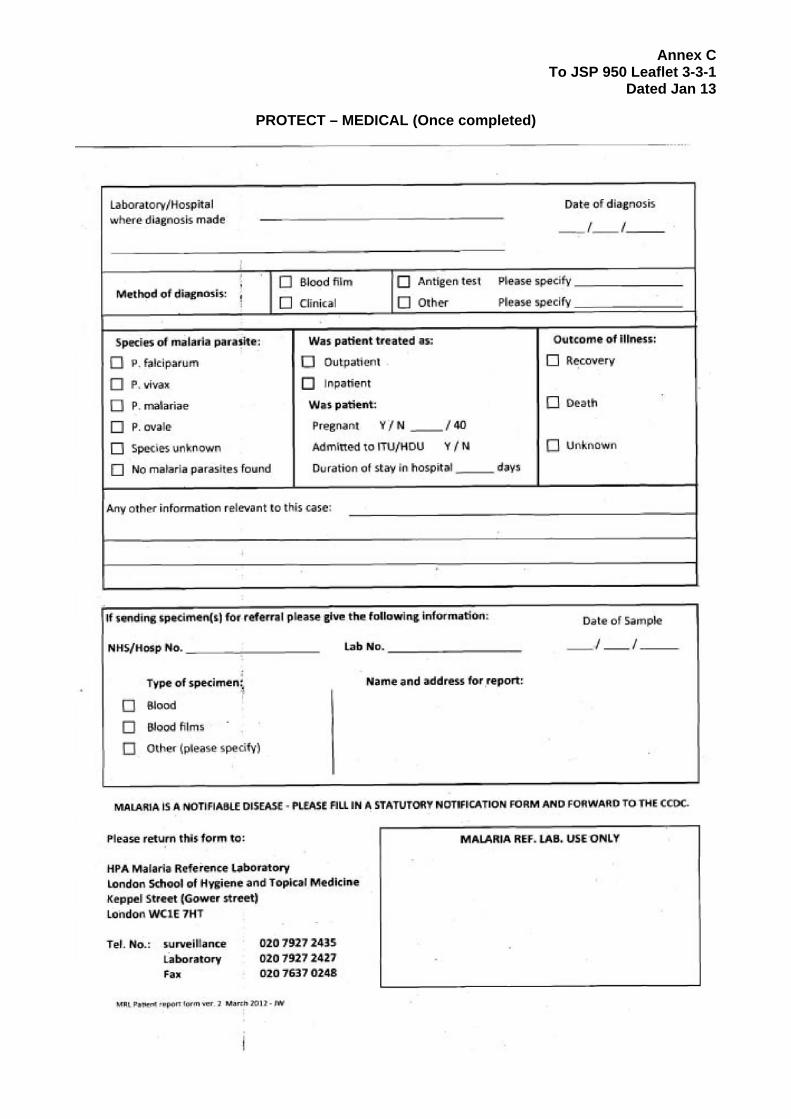
f. Official Visits to Malaria Risk Areas. Personnel travelling to malaria risk areas on official visits are to seek advice on malaria protection through the CoC.
g. Short Notice Deployments. Personnel deploying at short notice may have to forego the recommended therapeutic preparation time before departure. Should deployments occur at such speed it is essential that all personnel be given their chemoprophylactic drugs as soon as practicable and certainly before arrival in the malarial risk area. Personnel are to be briefed on the possible consequences of delayed commencement and deployed medical staffs are to ensure that the delay is reflected in their immediate contingencies for the investigation and management of febrile illness in the malarial risk area. Delayed commencement of anti-malarials is to be recorded in individual’s healthcare records.
24. Last Line of Defence. It is essential that all personnel realise that chemoprophylaxis is the last line of defence against malaria and not the first course of action. Just as bite prevention measures are not 100% effective, neither is chemoprophylaxis. Indeed, due to the ever-changing resistance pattern of the malaria parasite, drugs that have been effective in the recent past may not be effective in the near future. In addition, the following general principles are to be constantly reinforced to all personnel deployed to any malarial endemic area:
a. Prior to and during any deployments, they are to take their antimalaria drugs exactly as directed in the deployment medical instruction.
b. After departure from the malaria endemic area, they are to continue to take their anti-malaria drugs as indicated in the relevant section of the British National Formulary3 and re-enforced in the force redeployment instruction.
c. Should they at any time experience what they believe to be Adverse Drug Events (ADEs) from their antimalaria drugs, they are to seek medical advice as soon as possible, but are not to stop their anti-malaria drugs without first obtaining such advice.
25. Choice and Supply of Antimalaria Drug.
a. The spread of multi-drug resistant strains of malaria parasites in certain parts of the world necessitates a careful risk assessment before travel to any malarial risk area, taking into account the local malaria threat, the probability of exposure to infected mosquito bites, and the possibility of ADEs from chemoprophylaxis.
3 British National Formulary (BNF). BMJ Group and Pharmaceutical Press – Extant Version
JSP 950 UNCONTROLLED ONCE PRINTED Leaflet 3-3-1
6 Last Revised Jan 13
b. This policy does not seek to dictate specific drug regimens for specific locations or activities. Medical staffs are to be aware of the guidelines for use as found in the relevant section the British National Formulary4. These include identification and reporting of adverse events, dose regimes (including how long after exposure individuals are to continue taking the medication) and contraindications.
c. Anti-malarials are to be prescribed by individual prescription or by using a Patient Specific Direction (PSD). A Patient Group Direction (PGD) may be used to supply antimalarials, but the supply can only be made by a health professional legally allowed to supply medicines against a PGD, and who has been trained and deemed competent to work under the PGD.
d. If not supplied through individual consultation a medical officer, or suitably trained
deputy, is to present a malaria brief to all personnel prior to supply of anti-malarials. This brief should include correct dosage, frequency, and when to start and finish taking the anti-malarial.
26. Monitoring of Drug-related Adverse Effects. Medical officers are to report any adverse reactions to antimalaria drugs to the Committee on Safety of Medicines, using the ‘yellow card’ system. 27. Changing Chemoprophylaxis. Where high operational tempo exists, situations may arise where personnel leave one malaria risk area and redeploy immediately to another, where different risks require a change in chemoprophylaxis. A change from one regime to another is generally a simple matter but HQ SG SO1 CDC, through the chain of command, remains responsible for advising on the detail of chemoprophylactic regime changes. Compliance 28. Full compliance with all recommended antimalaria measures is essential to reduce the number of cases of malaria during military deployments. Commanders, specialist medical personnel and individuals all have a part to play in achieving complete compliance. 29. Individuals that wilfully fail to comply with stated policy put not only their own health at risk but also the combat strength of the deployed force. Whilst medical personnel will treat the disease, wilful non-compliance is a command, and therefore an administrative, issue rather than a medical one and failure to comply is to be treated in accordance with single Service administrative procedures. Special Occupational Groups – Aircrew and Divers 30. Aircrew and Divers. a. Aircrew. (1) Specialist direction concerning malaria protection in Aircrew is at Annex A. (2) All questions concerning the use of malarial chemoprophylaxis in aircrew are to be addressed to [email protected] . 4 British National Formulary (BNF). BMJ Group and Pharmaceutical Press – Extant Version
JSP 950 UNCONTROLLED ONCE PRINTED Leaflet 3-3-1
7 Last Revised Jan 13
b. Divers. (1) Specialist direction concerning malaria protection in Divers is at Annex B. (2) All questions concerning the use of malarial chemoprophylaxis in divers are to be
addressed to the Department of Underwater Medicine, INM Alverstoke. [email protected].
Other Considerations 31. Immunocompromised Individuals. Individuals suffering from medical conditions that might render them immunocompromised or otherwise alter their susceptibility to malaria, such as splenectomy, will require occupational health assessment of their fitness to deploy to malarial risk areas. 32. Pregnancy. Pregnancy is not an absolute contraindication for travel to malarial risk areas. However, it is not advisable for pregnant women to risk exposure to malaria as they are more susceptible to malaria and its consequences. The disease is generally more severe in pregnancy and may result in an adverse outcome to the pregnancy. Some chemoprophylactic medications can be harmful to the fetus. Accordingly, pregnant Servicewomen are not to deploy to malarial risk areas. 33. Blood Donation. Personnel who have served in a malaria endemic area should not donate blood until at least one year after return in line with National Blood Service (NBS) guidelines. 34. Aircraft Stopovers.
a. When the final destination of a RAF aircraft, or planned stopovers en route, are known to be within a malaria-endemic area, all passengers and crew are to be in possession of a personal supply of antimalaria medication. During check-in procedures, passengers will be asked to confirm that they are in possession of antimalaria medication. It is the responsibility of the dispatching unit to issue all personnel with the appropriate antimalarial chemoprophylaxis.
b. In the event that an aircraft is diverted to a malaria endemic area, the senior member of the crew is to seek advice from the medical officer at the aircraft’s home base. On arrival at the final destination, the senior member of the crew is to report the incident either to the medical officer at the destination, or where there is none, to the medical officer at the aircraft’s home base. On receipt of such an enquiry, medical officers are to report the incident and seek expert advice through the chain of command. Passengers are not to be allowed to disperse until suitable arrangements have been made to ensure that they receive appropriate chemoprophylaxis and medical advice.
35. Diagnosis and Treatment in the Home Base. Medical staffs are to be alert for symptoms in those personnel returning from malaria-endemic areas and are to consider the diagnosis of malaria in all febrile patients with a history of recent travel to malaria-endemic areas. Early referral for diagnosis and treatment is essential to prevent serious illness and death. 36. Early Diagnosis and Treatment On Deployment.
a. Personnel who present with a history of feverish or flu-like illness in a malaria endemic area are to be considered to have malaria until otherwise proven.
JSP 950 UNCONTROLLED ONCE PRINTED Leaflet 3-3-1
8 Last Revised Jan 13
b. Equipment to enable near-to-patient blood testing for malaria is to be deployed in support of all deployments to malaria-endemic areas. DCA CDC or DCA Path, in conjunction with DE&S M&GS, will give direction on the most appropriate test. Stocks of test kits may be demanded from DE&S M&GS. In the context of current practice the two test kits that are issued are the "ICT pF" (NSN - 6550-99-244-9080) and "Optimal" (NSN - 6550-99-191-1311).
c. In the event of near to patient diagnostic tests being unavailable, the theatre medical instruction5 is to detail the location of the nearest appropriate laboratory services for microscopic investigation. In addition, the theatre medical instruction will direct on the holding policy for those with feverish or flu-like illnesses and the procedure for referral or evacuation for further diagnostic tests and treatment if required.
d. If a diagnosis is made in theatre, medical staffs are to initiate treatment without delay in accordance with advice and direction issued in the theatre medical instruction or in accordance with SME advice from a Consultant in Infectious Disease/Microbiology obtained through reach-back support. Stocks of therapeutic drugs are to be included in medical stores from the beginning of the deployment.
e. Once a diagnosis has been made, the patient is to be evacuated to the home base, or a designated regional destination for further treatment and observation. The priority for evacuation is to be based on clinical need. Advice and direction can be obtained from AEROMED staffs; contact details for whom can be found in the theatre medical instruction.
37. Malaria Warning Card (F Med 568). All at-risk personnel are to be issued with a Malaria Warning Card (F Med 568) before leaving a malaria-endemic area. This card warns the individual that the diagnosis of malaria is to be considered if any illness develops. The card is to be shown to medical staff when seeking treatment for febrile illness for up to 2 years after possible exposure to malaria. 38. Notification of Malaria Cases. Medical officers are reminded that they are to report all suspected and confirmed cases of malaria in accordance with current Service instructions, using the F Med 85 and the HPA malaria report form. The HPA malaria report form is at Annex C. Once completed, the HPA malaria report form is to be sent to HQ SG SO1 CDC who will be responsible for onward transmission to the Malaria Reference Laboratory. Implementation 39. Further advice concerning this policy can be obtained from HQ SG SO1 CDC. The general point of contact is HQ SG Strat Med Pol SO2 Med Pol. Unless cancelled or otherwise revised, this leaflet will routinely be reviewed after three years. HQ Surgeon General will make policy leaflets publicly available in accordance with the Freedom of Information Act. This policy leaflet is releasable to the Internet. An Equality Analysis has been undertaken in the production of this policy and no impact is anticipated in terms of the Equality Act 2010. Annexes: A. Malarial Chemoprophylaxis and Aircrew. B. Malarial Chemoprophylaxis and Divers. C. HPA Malaria Report Form.
5 For those deployed afloat, RN pre-deployment briefings will advise on specifics for relevant theatre(s) of operations.
Annex A To JSP 950 Leaflet 3-3-1
Dated Jan 13
A -1
Malarial Chemoprophylaxis and Aircrew 1. The chemoprophylaxis of malaria can never be absolute and personal protection against being bitten, along with vector control, are also important. These non-therapeutic measures are addressed in other parts of this policy and are as important for aircrew, as they are for all other personnel. For the purpose of this policy, aircrew are defined as those personnel who have a role in the command, control and operation of the aircraft, both on the ground and in the air, and who remain within the aircraft during flight. 2. There are a number of drugs that can be used for the chemoprophylaxis of malaria in aircrew. These drugs are listed below. The particular drug chosen from this list should be appropriate for the area to be visited and should be selected using the guidelines detailed at Paragraphs 21-26 of the main text. 3. Drugs that may be used by aircrew for malaria chemoprophylaxis are as follows: a. Chloroquine. b. Proguanil. c. Malarone® - (Proguanil 100mg and Atovaquone 250mg). d. Doxycycline. 4. Malarone® is approved for use in aircrew on the basis of two studies6,7. Continuous prophylaxis with an alternative agent may be preferable to repeated courses of Malarone®, until more experience with the use of the drug in aircrew is obtained. 5. Aircrew likely to require Malarone®, are to have a one-off trial period of the drug during a non-flying phase. This is to be for approximately 5 days, although in cases of urgent operational necessity this could be reduced to 2 days. This period is to determine the presence of any idiosyncratic reactions to the drug. Malarone® is to be started 1-2 days before arrival in an endemic area and need only be taken for one week after returning from the endemic area. The use of Malarone® is to be compatible with extant theatre policy. Its use would not be appropriate if it was being used as a treatment agent in that theatre. 6. Aircrew are not to take mefloquine (Larium®) as there is a small, but significant, risk of side-effects, which could degrade concentration and co-ordination. There is also a risk of cardiac conduction defects with this drug. Aircrew in non-flying roles may take mefloquine, but will be classed as, ‘unfit flying duties,’ for 3 months after taking the last dose of the drug. Aircrew who inadvertently take mefloquine, are to be grounded, and made, ‘unfit flying,’ for a period of 3 months after the last dose of mefloquine. 7. If Doxycycline is used for malaria prophylaxis in aircrew, it is not to be given to aircrew that may become pregnant. To be effective it is to be started one week before travel to the endemic area and is to be continued for 4 weeks after return from the endemic area. Due to its short half-life it is to be taken daily, and at the same time every day.
6 Paul MA, McCarthy AE, Gibson N et al. The Impact of Malarone and Primaquine on Psychomotor Performance. Aviation, Space and Environmental Medicine 2003;74:738-45. 7 Turner C, Stone BM, Mills SL. In preparation for Aviation, Space and Environmental Medicine.

Annex A To JSP 950 Leaflet 3-3-1
Dated Jan 13
A -2
8. Chloroquine and Proguanil can be used by aircrew and are to be started one week before travel and continued for 4 weeks after return from the endemic area. 9. Further advice is contained in AP 1269A Lft 5-19 Drugs and Aircrew.
Annex B To JSP 950 Leaflet 3-3-1
Dated Jan 13
B-1
Malarial Chemoprophylaxis and Divers 1. In geographic regions where malaria presents a risk to health, general measures of protection against malaria such as awareness and education, bite avoidance and vector control should be identified and implemented prior to diving operations, as detailed in the main body of this JSP leaflet. 2. The use of chemoprophylaxis in divers may impact on their fitness to dive and this should be considered in conjunction with the area-specific risk assessment to determine the most appropriate anti-malarial drug regimen. 3. Drugs considered acceptable for use by divers for malaria chemoprophylaxis are as follows: a. Chloroquine. b. Proguanil. c. Malarone® - (Proguanil 100mg and Atovaquone 250mg). d. Doxycycline. 4. Per the BR 1750A, Handbook of Naval Medical Standards, Chapter 12, Standards for Diving and Hyperbaric Exposure, when starting new medications, a period of observation is required to identify any adverse drug events (ADEs) prior to diving. In general, a period of 2 weeks is considered optimal when starting any new medications. However, adjustments may be made for urgent operational demands. Therefore, depending on the operational necessity, this period of observation can be reduced to a little as 2 days for Malarone® if absolutely required. 5. Divers who suffer any adverse drug effects whilst taking anti-malarial drugs should be considered ‘Temporarily Medically Unfit (TMU) for Diving’ and seek medical care and advice as soon as possible. If an ADE (non-life threatening) occurs whilst in, or following departure from, the malaria-endemic area, they are to cease diving but continue taking their anti-malarial drugs as prescribed until obtaining medical advice. 6. Use of the anti-malarial drug Mefloquine (Lariam) is not compatible with diving duty due to its significant side effect profile, in particular, the risk of seizures. Any diver who has used Mefloquine for any medical indication is Temporarily Medical Unfit (TMU) for Diving for 12 weeks after their last dose. Therefore, any use of Mefloquine by military divers (to include military sports divers) must be closely regulated to avoid any unintended adverse impact on a service-member’s availability for military duties.
Annex C To JSP 950 Leaflet 3-3-1
Dated Jan 13
PROTECT – MEDICAL (Once completed)
PROTECT – MEDICAL (Once completed)
C-1
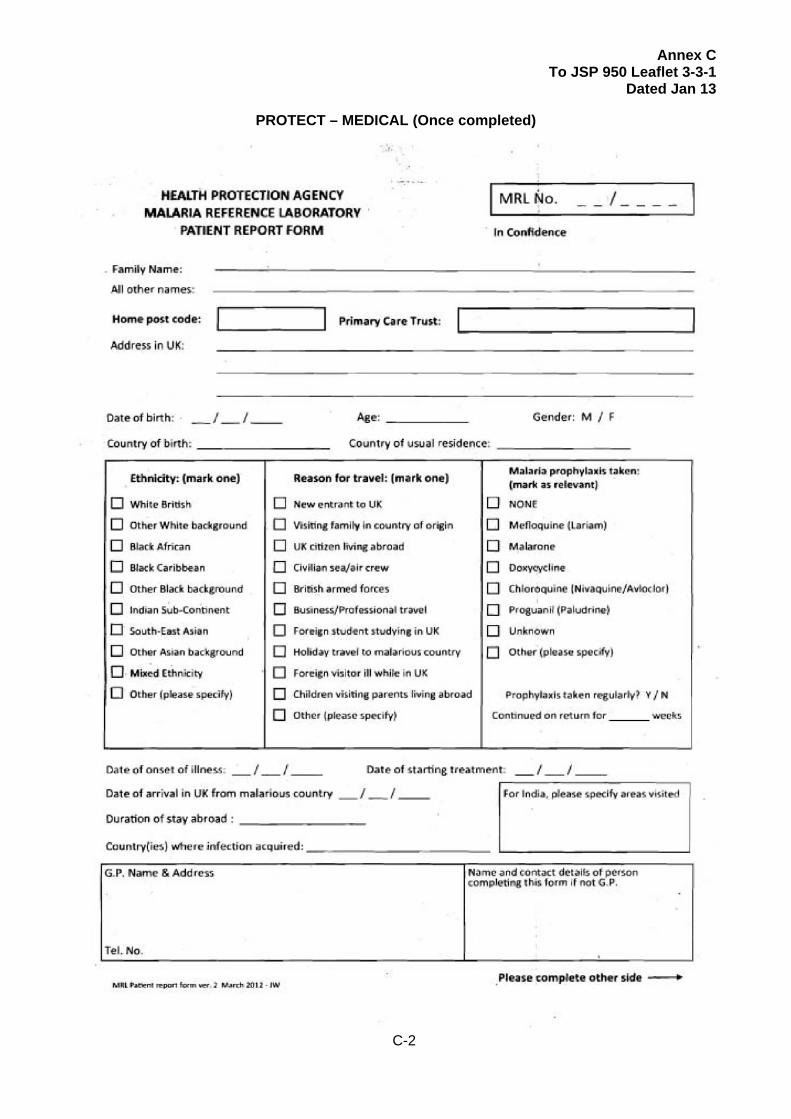
MALARIA IS A NOTIFIABLE DISEASE - THIS FORM IS TO BE COMPLETED AND FORWARDED TO HQ SG SO1 CDC AT: HQ SG DMS WHITTINGTON WHITTINGTON BARRACKS LICHFIELD STAFFORDSHIRE WS14 9PY This form is also available at the link HPA Malaria Referral Form
Annex C To JSP 950 Leaflet 3-3-1
Dated Jan 13
PROTECT – MEDICAL (Once completed)
C-2
PROTECT – MEDICAL (Once completed)
Annex C To JSP 950 Leaflet 3-3-1
Dated Jan 13
PROTECT – MEDICAL (Once completed)
PROTECT – MEDICAL (Once completed)
C-3





























