Embed Size (px)
Citation preview

Preventing Pressure Ulcers
Repositioning and Microturns
Denise Nix MS RN CWOCN
MHA SAFE SKIN Consultant

Objectives
• Understand the significance of this topic for Minnesota Hospitals
• Define “optimal positioning” for the bedbound patient • Discuss MHA Recommendations for alternative positioning
(only in the absence of optimal positioning) • Describe the history and literature related to weight
shifting and microturning • Present examples of techniques for alternative positioning • Provide relevant references for further exploration of the
topic

Significance
Almost 60% of stage 3, 4, and unstageable pressure ulcers in MN hospitals develop on the sacral, coccygeal, buttocks region
Sacrum, Buttocks, Coccyx
Medical Devices
Other

AHE reports revealed:
o 52% - condition prohibited turning
o 22% - patient refused positioning
Hospitals reporting success:
o Nurse-MD communication about positioning issues
o Bed ahead programs
o Frequent tailbone offloads of some kind
o Frequent reevaluation, reeducation and turning trials
Significance

If a patient is not able to be adequately or
routinely repositioned:
owritten confirmation that patient
cannot be repositioned from the
physician with daily re-evaluation
o Immediate evaluation for the most
appropriate surface to redistribute
pressure
o at least hourly mini shifts off the
tailbone
MHA SAFE SKIN Recommendations

Optimal Positioning
Tissues of the body are not meant to be stationary
The average healthy person repositions him/herself every 6 to 11.6 minutes
Keane FX . The minimum physiological movement required for a man supported
on a soft surface. Paraplegia. 16, 383-9. 1978.

Optimal Positioning
• Hospital bedbound patients
• 30 degrees side lying turns
• Every 2 hours
Wound , Ostomy and Continence Nurses (WOCN) Society : Guideline for
prevention and management of pressure ulcers , Glenview , IL , 2010 , Author.

Optimal Positioning
• HOB 30 degrees or less
• Float heels
National Pressure Ulcer Advisory Panel (NPUAP) and European Pressure Ulcer Advisory Panel
(EPUAP) : Prevention and treatment of pressure ulcers: Washington DC , 2009

In the Absence of Optimal Positioning:
Courtesy Mayo Clinic

History Behind Weight Shifts
Panel on the Prediction and Prevention of Pressure Ulcers in Adults: Clinical Practice Guideline No. 3 Rockville, MD: Agency for Health Care Policy and Research; 1992. AHCPR Publication No 92-0047.
Wound , Ostomy and Continence Nurses (WOCN) Society : Guideline for prevention and management of pressure ulcers , Glenview , IL , 2010 , Author.
National Pressure Ulcer Advisory Panel (NPUAP) and European Pressure Ulcer Advisory Panel (EPUAP) : Prevention and treatment of pressure ulcers: Washington DC , 2009

Pressure Mapping

Pressure Mapping-Weight Shifts
Ischial Tuberosities (Sitting Bones) Sitting on Chair with Cushion
Ischial Tuberosities (Sitting Bones) Same Patient Leaning to Side

Lorraine

Pressure Mapping-MiniTurn
Supine Position Pressure Redistribution Mattress
HOB 30 Degrees
Same Patient –Miniturn Same Mattress
HOB 30 Degrees
15
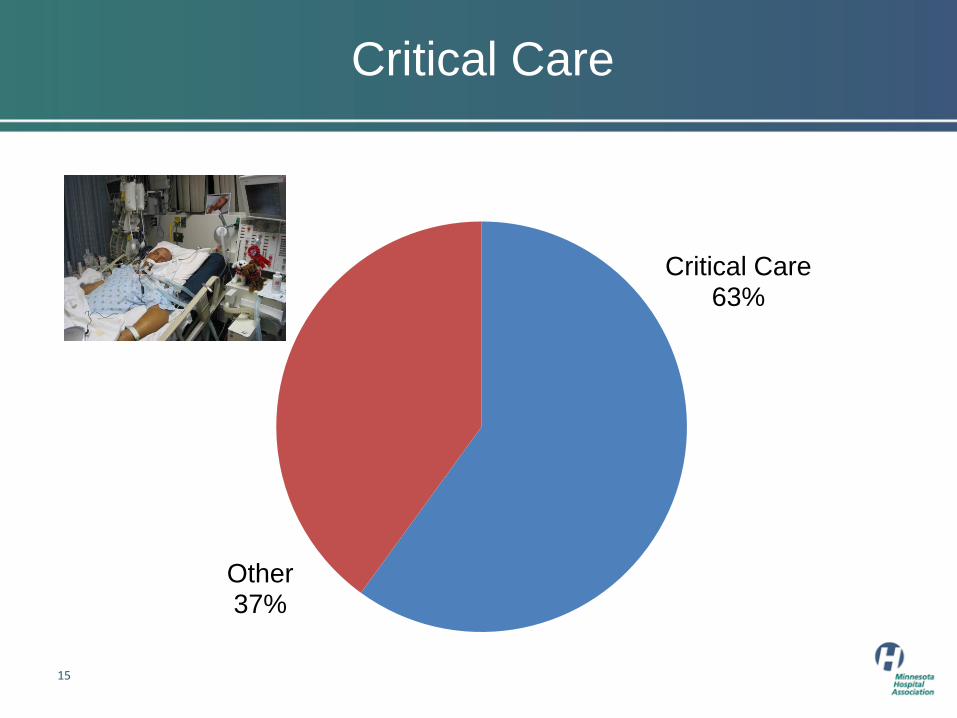
Critical Care
Critical Care 63%
Other 37%

Hemodynamic Instability
“Hemodynamic Instability” may be used inappropriately to describe critically ill patients
Repositioning may be withheld due to fear of affecting systemic perfusion, ICP or oxygenation.
It is passed on from shift to shift without verification nor inclination of when to resume or trial positioning
Winkelman C, Peereboom K. Staff-perceived barriers and facilitators. Crit Care Nurse. 2010;30:13–16
Choi J, Tasota FJ, Hoffman LA. Mobility interventions to improve outcomes in patients undergoing prolonged mechanical ventilation: a review of literature. Biol Res Nurs. 2008;10(1):21–33
ICP Monitoring
Most neurosurgery patients with intracranial pressure monitoring can be turned safely beginning in the
immediate postoperative period
Jones B. The effects of patient repositioning on intracranial pressure. Aust J Adv Nurs.
1994;12(2):32–39.
O'Connor ED, Walsham J. Should we mobilise [sic] critically ill patients? A review. Crit Care Resusc. 2009;11(4):290–300.

Gravitational Equilibrium
Process
Failure to turn for prolonged periods
Hemodynamically calibrates to a supine position
Creates maladaption to position changes
Orthostatic response with rapid movement
Management
SLOW movement followed by 5- to 10-minute recovery periods
CLRT (turning beds) does not count as patient turning for pressure ulcer prevention
Vollman K. Introduction to progressive mobility. Crit Care Nurse. 2010;30:3–5

SVO2 and Heart Rate
Monitored changes in SvO2 and heart rate following lateral turns in ICU patients
Changes found to be transient
Most patients returned to baseline within 5 minutes
Winslow EH, Clark AP, White KM, Tyler DO. Effects of a lateral turn on mixed venous oxygen saturation and heart rate in critically ill adults. Heart Lung. 1990; 19:557–561

Respiratory Instability
Sometimes repositioning is the actual treatment for the respiratory instability:
• Atelectasis
• Shunting in the context of a collapsed lung
• Differences in lung compliance.
Brindle CT Turning and Repositioning the Critically Ill Patient With Hemodynamic Instability: A Literature Review and Consensus Recommendations J Wound Ostomy Continence Nurs. 2013;40(3):254-267

Turning Trials
Insufficient evidence to determine which patients are severe enough to preclude turning trials
Turning, repositioning, and mobilizing the intensive care patient requires multidisciplinary collaboration
Chulay M, Brown J, Summer W. Effect of postoperative immobilization after coronary artery bypass surgery. Crit Care Med. 1982;10(3):176–179.
Brindle CT Turning and Repositioning the Critically Ill Patient With Hemodynamic Instability: A Literature Review and Consensus Recommendations J Wound Ostomy Continence Nurs. 2013;40(3):254-267

Author Examples -Too Unstable To Turn (Use Weight Shifts, Passive ROM, Mini-turns Instead)
Discuss With MD and Reassess Each Shift:
Active uncontrolled bleeding (ex: Open chest graft failure)
Massive Transfusion protocols
No fluid/blood going in= no blood pressure (does NOT include minor fluid boluses for correction)
Sudden desaturation from patient’s baseline that doesn’t RECOVER
Sudden change in MAP that does not RECOVER (and can’t be corrected with vasopressive agents)
King LT Airway
Brindle CT Turning and Repositioning the Critically Ill Patient With Hemodynamic Instability: A Literature Review and Consensus Recommendations J Wound Ostomy Continence Nurs. 2013;40(3):254-267

Techniques
SLOWLY move to 10 degrees-allow recovery period- move to 20 degrees-allow recovery period etc
Using a turn/lift sheet to tilt off tailbone
Lift head or extremity off bed surface for 1-2 minutes at a time
Utilize the lost art of passive range of motion
Communicate, Trouble Shoot, Communicate!!
Brindle CT Turning and Repositioning the Critically Ill Patient With Hemodynamic Instability: A Literature Review and Consensus Recommendations J Wound Ostomy Continence Nurs. 2013;40(3):254-267

References (Micro/Minor/Mini) Shifts or Turns
Brindle CT Outliers to the Braden Scale Identifying high ICU patients and the results of prophylactic
dressing use WCET Journal Volume 30 Number 1 – January/March 2010.
Brindle CT Turning and Repositioning theCritically Ill Patient WithHemodynamic Instability: A Literature Review and Consensus Recommendations J Wound Ostomy Continence Nurs. 2013;40(3):254-267.
Bryant, R. Nix D. Developing and Maintaining a Pressure Ulcer Program. In Bryant, R. Nix, D. Coeditors: Acute and Chronic Wounds: Current Management Concepts, 4th Edition. St. Louis, Mosby, January, 2012.
Institute for Clinical Systems Improvement (ICSI): Health Care Protocol :Pressure Ulcer Prevention and Treatment Protocol 3rd Edition January, 2012 Available at www.icsi,org
Keane FX (1978) The minimum physiological movement required for a man supported on a soft surface. Paraplegia. 16, 383-9.
Knox, D.M., Anderson, T.M., & Anderson, P.S. (1994). Effects of different turn intervals on skin of healthy older adults. Advances in Wound Care, 7(1), 48–52, 54–56.
Oertwich PA, Kindschuh AM, Bergstrom N. The effects of small shifts in body weight on blood flow and interface pressure. Res Nurs Health. 1995 Dec;18(6):481-8.
Paralyzed Veterans of America (PVA). (2000). Pressure Ulcer Prevention and Treatment Following Spinal Cord Injury:. A Clinical Practice Guideline for Health-Care Professionals. Washington, D.C.: Author
Pressure Redistribution: Seating, positioning, and support surfaces. Matching Support to Patient Needs. IN Baranoski S. Wound care essentials:practice principles. Second Edition 2008.
Wound , Ostomy and Continence Nurses (WOCN) Society : Guideline for prevention and management of pressure ulcers , Glenview , IL , 2010 , Author.
Young T. The 30 degree tilt position vs the 90 degree lateral and supine positions in reducing the incidence of non-blanching erythema in a hospital inpatient population: a randomized controlled trial. J Tissue Viability. 2004 Jul;14(3):88, 90, 92-6.

References Positioning & Hemodynamic Unstablity
Winkelman C , Peereboom K . Staff-perceived barriers and facilitators. Crit Care Nurse. 2010 ; 30 : 13-16 .
De Jonghe B , Lacherade JC , Shashar T , Outin H . Intensive care unit–acquired weakness: risk factors and prevention . Crit Care Med. 2009 ; 37 ( 10 ): s309-s315 .
Bailey P , Thomsen GE , Spuhler VJ , et al. Early activity is feasible and safe in respiratory failure patients . Crit Care Med . 2007 ; 35 ( 1 ): 139-145 .
Morris PE , Goad A , Thompson C , et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure . Crit Care Med . 2008 ; 36 ( 8 ): 2238 2243 .
Choi J , Tasota FJ , Hoffman LA . Mobility interventions to improve outcomes in patients undergoing prolonged mechanical ventilation: a review of literature . Biol Res Nurs. 2008 ; 10 ( 1 ): 21-33 .
Winslow EH , Clark AP , White KM , Tyler DO . Effects of a lateral turn on mixed venous oxygen saturation and heart rate in critically ill adults . Heart Lung. 1990 ; 19 : 557-561 .
Vollman K . Introduction to progressive mobility . Crit Care Nurse . 2010 ; 30 : 3-5 .
Coupe M , Fortrat JO , Larina I , Gauquelin-Koch G , Gharib C , Custaud MA . Cardiovascular deconditioning: from autonomic nervous system to microvascular functions . Respir Physiol Neurobiol. 2009 ; 169s : s10-s12 .
Offner PJ , Haepel JB , Moore EE , Bliff WL , Franciose RJ , Burch JM . Complications of prone ventilation in patients with multisystem trauma with fulminant acute respiratory distress syndrome . J Trauma . 2000 ; 48 ( 2 ): 224-228 .
References: Pressure Mapping, “Capillary Closing”, and Interface Tissue Measurement
Le KM et al : An in-depth look at pressure sores using monolithic silicon pressure sensors,
Plast Reconstr Surg 74 ( 6 ): 745 , 1984 .
Nix D, Mackey Diane. Support Surfaces. In Bryant, R. Nix, D. Coeditors: Acute and Chronic Wounds: Current Management Concepts, 4th Edition. St. Louis, Mosby, January, 2012.
Reger SI et al : Correlation of transducer systems for monitoring tissue interface pressures , J Clin Eng 13 ( 5 ): 365 - 371 , 1988 .
Stinson M, Porter A, Eakin P. Measuring interface pressure: a laboratory-based investigation into the effects of repositioning and sitting. Am J Occup Ther. 2002;56(2):185-190.
Stinson MD, Porter-Armstrong A, Eakin P. Seat interface pressure: a pilot study of the relationship to gender, body mass index, and seating position. Arch Phys Med Rehabil. 2003;84(3):405-409.
Stinson MD, Porter-Armstrong AP, Eakin PA. Pressure mapping systems: reliability of pressure map interpretation. Clin Rehabil. 2003;17(5):504-511.
Wound, Ostomy and Continence Nurses (WOCN) Society : Guideline for prevention and management of pressure ulcers , Glenview, IL , 2003 , Author .

Thank You!!
Denise Nix