Embed Size (px)
Citation preview

Prevention and Cessation Education in US Medical Schools
Harvard Tobacco Control
Working Group
March 17, 2004
NCI R25-CA9-1958-02

At the end of this five-year grant, we anticipate that tobacco education modules will be successfully incorporated into a number of US medical schools and graduating students at these schools will be able to skillfully perform tobacco prevention and cessation counseling for children, adolescents, and adults.
PACE (August 1, 2002 – July 31st, 2007)

PACE Study Sites and Number of Enrolled Students
Dartmouth Medical School – (286)
University of Kentucky – (368)
University of Rochester – (391)
University of South Florida – (397)
University of Massachusetts Medical School – (419)
Case Western Reserve University – (566)

PACE Study Sites and Number of Enrolled Students (cont.)
University of Iowa – (591)
UCLA – (598)
Boston University – (623)
University of Alabama at Birmingham (UAB) – (643)
Loma Linda University – (653)
Harvard University – (712)

Rationale for selection of sites: As our long-term objective is inclusion of tobacco control curriculum in multiple US medical schools, we have selected a representative sample of these schools. We used the following criteria for choosing sites:
a.) Public and private schools;b.) The major geographic sites in the United States;c.) Inner city and rural areas;d.) Schools with varying amounts of tobacco education (range of no current content to multiple modules);e.) Internet access to students for survey completion.

Evolution of Current NCI R-25 Award
a.) Missed opportunities-"specific curriculum devoted to smoking cessation and prevention must become a mandatory component of undergraduate education in every US school"-JAMA 1994
b.) Work of UMass teamc.) Linda Ferry article-JAMA 1999d.) BU R25-Preventive Medicine 2002e.) Collaborations with American Association of
Cancer Education

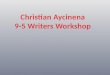
Percent of Current Smokers Ever Receiving Advice to Quit from Physicians and Dentists
26%
51%56% 56%
19%
60%
21%
63%
25%
0%10%20%
30%40%
50%60%
70%80%90%
100%
1974 1986 1991 1993 1996 1999
PhysicianDentist
Source: NHIS 1974, 1986, 1991; CPS 1993, 1996, 1999.

Physicians’ Counseling Behavior*
74%67%
35%
8%0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Ask
> 8
0%of
pat
ient
sab
out
smok
ing
stat
us
Adv
ise
>80
% o
fsm
okin
gpa
tient
s to
quit
Ass
ist >
80%
of
smok
ing
patie
nts
Arra
nge
follo
w-u
pfo
r > 8
0%of
sm
okin
gpa
tient
s
*A representative sample of 246 community-based Rhode Island primary care physicians
Source: Goldstein MG, DePue JD, Monroe AD, et al. A population-based survey of physician smoking cessation counseling practices. Preventive Medicine. 1998;27:720-729.

Percent of Pediatricians Reporting Giving Advice to Parents of Patients, CA (1997-8)
62%
5%
13%
73%
18%
56%
0%
20%
40%
60%
80%
100%A
ski
ng a
bout
sm
oki
ng s
tatu
s
Recom
mendin
gsettin
g a
quit
date
Pre
scribin
gN
RT
Schedulin
g a
follo
w-u
p v
isit
or
tele
phone c
all
Ask
pare
nts
ifth
ey
sm
oke
insid
e their
house
Aski
ng p
are
nts
about sm
oki
ng
in fro
nt of th
eir
child
outs
ide
the h
om
e
CESSATION ADVICE ETS ADVICE
Source: Perez-Stable EJ, Juarez-Reyes M, Kaplan CP, Fuentes-Afflick E, Gildengorin V, Millstein SG. Counseling smoking parents of young children: comparison of pediatricians and family physicians. Arch Pediatr Adolesc Med. 2001;155:25-31.

National Cancer Institute panel (1992)
a.) Specific curriculum devoted to smoking cessation
and prevention must become a mandatory
component of undergraduate medical education;
b.) An assessment of tobacco curricula at medical
schools is necessary;
c.) Certain core materials can serve as key
components of different tobacco curricula;

National Cancer Institute panel (1992) (cont.)
d.) The effectiveness of a smoking cessation and prevention
curriculum must be evaluated
e.) Questions on this topic should be included as part of the
USMLE steps 1,2,3;
f.) The AMA and the Association of American Medical Colleges
(AAMC) and other organizations are important vehicles for
promoting discussion and action;

A National Action Plan for Tobacco Cessation (2004)
‘clinicians feel inadequately prepared to intervene with patients who smoke and appraisals of medical school curricula reveal little training in tobacco intervention strategies’
Subcommittee recommended that ‘USDHH provide grants to medical and other health professional schools to develop, implement, and evaluate curriculum for treatment of tobacco dependence’ ‘Licensure and certification exams assess knowledge of tobacco dependence’ ‘Ensure that competency in tobacco dependence interventions is a core graduation requirement for all new physicians’
(AJPH February 2004)

Year Course Topic # Hours
1 Essentials of Public Health Cancer prevention and detection 2
1 Essentials of Public Health Case-control studies on tobacco and lung cancer 1
1 Introduction to Clinical Medicine Introduction to substance abuse – Tobacco cessation 1
2 Biology of Disease-Cardiology Discussion of tobacco effects
0.5
2 Biology of Disease-Pulmonary Diseases Discussion of tobacco effects
0.5
2 Introduction to Clinical Medicine Cancer skills laboratory 2
3 Pediatric Orientation Role of pediatrician in smoking prevention 1
3 Introduction to Ambulatory Medicine Cancer communication skills laboratory 2
4 Home Medical Service Cancer detection in the elderly 1
Tobacco Curriculum Boston University Medical School (BUSM) 2003

Self-Rated Skills Among BUSM IV by Chronological Year
33.13.23.33.43.53.63.73.83.9
44.14.24.34.44.5
1996 1997 1998 1999
Mean scores with responses ranging from 1(very unskilled) to 5 (very skilled)
SmokingpreventioncounselingSmokingcessationcounselingSun protectioncounseling
Skin cancerexamination
Clinical breastexamination
Obtaining smearsfor Pap test

0%10%
20%30%
40%50%60%
70%80%
90%100%
Sm
ok
ing
As
se
ss
me
nt
Inju
ryP
rev
en
tio
n
Sm
ok
ing
As
se
ss
me
nt
Inju
ryP
rev
en
tio
n
Sm
ok
ing
As
se
ss
me
nt
Inju
ryP
rev
en
tio
n
Sm
ok
ing
As
se
ss
me
nt
Inju
ryP
rev
en
tio
n
Preceptor madeexpectations clear
Observe preceptor talkwith family
Preceptor observe youtalking with family
Preceptor gave youfeedback
Yes
No
Proportion of BUSM III (2001-02) completing assessments as a function of
preceptor reinforcement

Smoking Prevention Activities Conducted by BUSM III
(average response per six weeks)
0
10
20
30
40
50
60
70
Discourageparents from
smoking in thehouse
Initiatediscussions withchildren about
smoking
Discuss nicotinereplacement
therapy (NRT)with parents
Ask parent if theytalked with childabout smoking
Offer tips forparents to
counsel childrenabout smoking

PACE Design (2003-2007)
NA = Needs Assessment
SS = Student Surveys (2nd + 4th year students)
* Course development consists of the creation of three separate modules
^ Module Intervention I is the stage in which each school initiates the one course that the PI took part in developing
+ Complete module intervention is the stage when each of the 12 schools initiates all modules that were developed
# The national dissemination stage is when the modules are made available to all medical schools in the United States
2003 2004 2005 2006 2007
Education Course
Development *
Module Intervention
I^
Complete Module
Intervention +
National dissemination
#
Evaluation NA SS Course Evaluation
SS/NA

PACE Timetable
Aim 1/Year 1- Assess current curriculum and organize and convene a national
conference
Aim 2/Year 2- Develop new curriculum, plans for integration, and conduct
faculty training
Aim 3/Year 3- Conduct trial implementation of new curriculum
Aim 3/Year 4- Share ‘best content’ across all 12 schools
Aim 4/Years 1-4 Conduct a comprehensive process and
impact evaluation
Aim 5/Year 5- Disseminate Resource Guides/Tool Kits to other
medical schools

Assessment of Current Curriculum
What is currently being taught?- Can get to minutes but not quality of teaching
Defining what needs to be taught? - Educational visioning
Offering means to address the deficit
- Course development, evaluation of sites of inclusion

Courses and Tobacco Content (12 schools)
Courses with Tobacco
41 (range=0-7)
mode=2,5 mean=3
39 (range=1-10)
mode=3 mean=3
26 (range=1-7)
mode=2 mean=3
Courses
112 (range =6-11)
mode=9 mean=9
92 (range =4-17)
mode=6,7 mean=8
92 (range =4-10)
mode=5 mean=6
YEAR 1
YEAR 2
YEAR 3

Number of Tobacco Hours by School (n=12)
0
1
2
3
4
5
6
# of Schools
< 5 hours 6-9 hours 10-15 hours 27 hours
Hours

Clerkships
Heavy Hitters:
Family MedicineInternal Medicine
Soft Spots:PediatricsOB GYN

Lack of Faculty Training for Tobacco Prevention and Cessation (“NO” Responses)
Among 12 US Medical Schools
0
2
4
6
8
10
12
Tobacco CME's Prevention/CessationGuidelnes
Prevention CourseWorkshop
Mentor/MasterTeaching
InstructionalDevelopment Seminar
PharmacologicTherapy

Uncovered Impediments to Reform
Time overload-stealth approach
- Advantage-cuts across so many disciplines
Lack of any organized tobacco infrastructure Far more didactics than skills

Aim 2-Development of New Curriculum Modules, Plans for Integration, and Faculty Training (Year 2)
a) Formulate graduating competencies for tobacco control education and related goals and objectives;
b) Construct a formally evaluated series of educational modules for teaching in all medical school years, both in preclinical and clinical years.
c) Develop strategies to integrate the educational modules into existing courses specific for each school;

Why integrate tobacco control curriculum?
Tobacco control should be part of basic skills of ALL medical students “ what every student should know”
Core courses are venues for basic skills

Year 2 Tasks Resulting from Initial PACE Meeting
Major Domains Tasks
Adult cessation
Pediatric Prevention
Public Health Approaches
Preceptor education
Clerkship orientations and in-services
Integrate tobacco into community
health programs
Other – OB/GYN

Study Design/Timeline
Pediatrics Orientation
(4 Schools)
Preceptor Orientation
(4 Schools)
Community Electives
(4 Schools)
2004-5
Pilot Year
2005-6
PACE School Dissemination
BU CWRU Dartmouth Harvard Loma Linda UAB
U.KentuckyUCLA U.Iowa UMass U.Rochester USF
2006-7
U.S. Medical Schools
Dissemination
All U.S. Medical Schools

Graduating competencies are
organized according to:
a.) Adult cessation and prevention competencies;
b.) Pediatric prevention and cessation competencies;
c.) Public health advocacy/population science competencies;
d.) Support systems in clinic/medical setting competencies; and
e.) Professional development/global competencies

All presentations will be tailored and available as:
Seminar presentationsAudioCDWritten copies of print-outsWith teacher manualsHand-outs for students to give to patients

The Difference Between a Curriculum and a Pile of Stuff
Transferability: Contains tools and resources so others can use it
Ease of Use: Materials are well organized and complete Format: Materials conform to a common format. Synergy: Modules fit together coherently Coverage: Adequate coverage of a competency area

PRECEPTORSHIP MODULE
Students must practice what they have learned in the classroom
Students model what they see in clinical settings
Preceptors have an important role as teachers and mentors
Will be encouraged to promote feedback

Community Tobacco Electives
Teaching and training: First year and fourth
year students
Tobacco Advocacy: working with national organizations on policy and legislation
On-line training in tobacco prevention and
cessation

Exploratory:
OB GYNNational Board of Medical Examiners Step IIbUS Student OrganizationsInternational medical students