Embed Size (px)
Citation preview
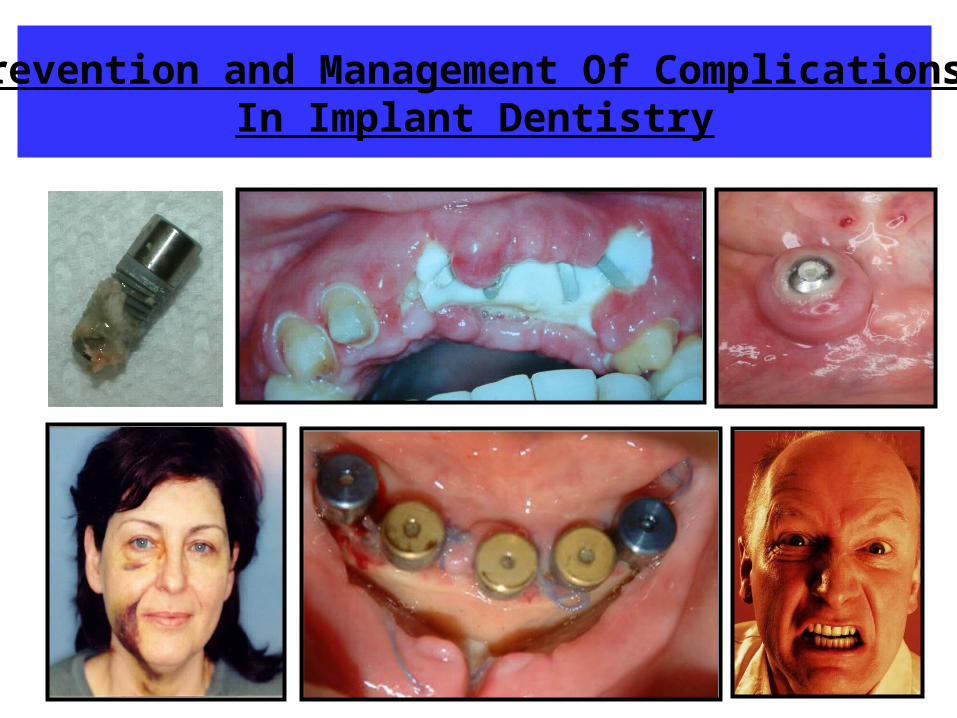
Prevention and Management Of Complications In Implant Dentistry
Evidence Based Medicine / Dentistry
EBM is the conscientious, explicit and judicious use of best evidence in making decisions about care of individual patients.
Cochrane CenterOxford, England
3 Components of Evidence Based Dentistry
1) Scientific Literature
2) Professional Experience and advise
3) Patient’s treatment desire and goal
“Train The Brain”
Dr. Mark H.E. Lin
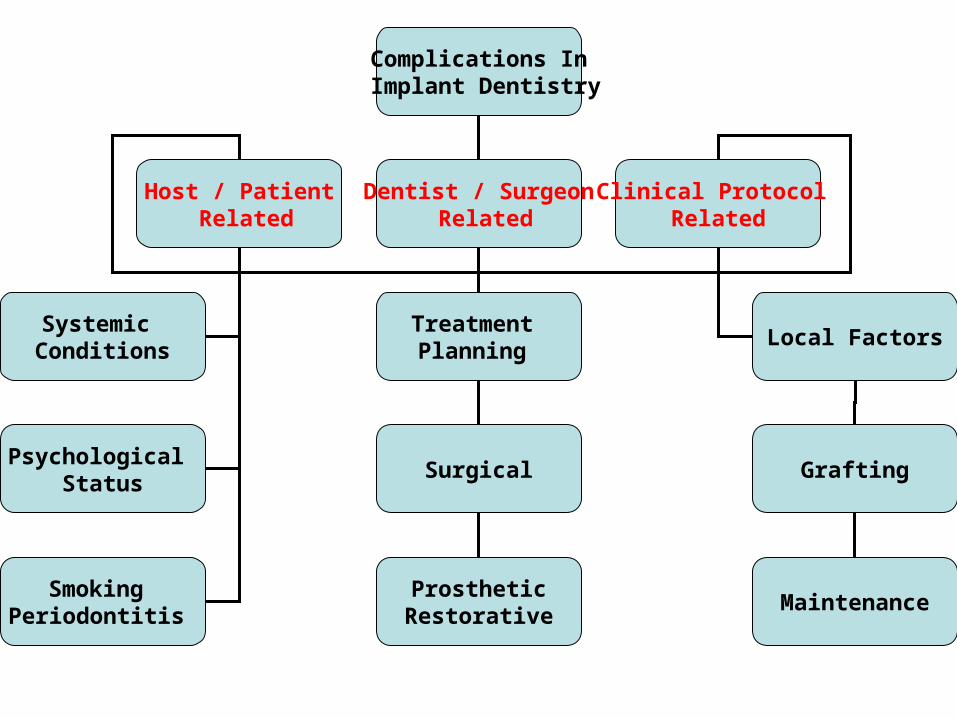
Complications In Implant Dentistry
Host / Patient Related
Dentist / Surgeon Related
Clinical Protocol Related
Systemic Conditions
Psychological Status
Smoking Periodontitis
Treatment Planning
Surgical
Local Factors
Grafting
ProstheticRestorative
Maintenance
Medical Status
Absolute Contraindications to Surgery
Relative Contraindications / Risk Factors to Surgery
Host / Patient Related:
Susceptibility to Infections and healing response in question
Medical Status: Absolute Contraindications
For Surgery (Dental alveolar, implant, hard or soft tissue grafting)
– Debilitating diseases:• Active cancer• chemotherapy• radiation therapy• transmittable infections- hepatitis, HIV
– Impaired healing capacity diseases: • Uncontrolled diabetes• Uncontrolled hypertension • immune compromised disease• history of osteomylitis in operative site
Host / Patient Related:
Medical Status:
Absolute Contraindications – Recent myocardial infarction (M.I.), cerebrovascular
accident, uncontrolled clotting / bleeding disorders– Pregnancy– Chronic or severe alcoholism– Drug abuse– Psychiatric disorders– I.V. bisphosphonate use or long term oral
bisphosphonate– Uncontrolled periodontal disease– ASA IV or V patients
Host / Patient Related:
Medical Status: Relative Contraindications / Risk Factors
For Surgery (Dental alveolar, implant, grafting)
– Debilitating diseases: Inactive cancer– Impaired diseases: Controlled diabetes, controlled
hypertension– Myocardial infarction (M.I.) history of >1 year – Oral bisphosphonate– Smoking habits– Periodontal disease
Host / Patient Related:
American Society of Anesthesiologists (ASA) Classifications
ASA I: a normal, healthy patient, without systemic disease.
ASA II: a patient with mild to moderate systemic disease.
ASA III: a patient with severe systemic disease, which limits or alters activity but is not incapacitating.
ASA IV: a patient with severe systemic disease, which is incapacitating and is a constant threat to life.
ASA V: a moribund patient not expected to live more than 24 hours without an operation.
Elective Implant surgeries are NOT indicated for ASA IV or V
patients
For a patient at risk, strict adherence to the standard
protocol does not always yield the expected results.
Infection
Invasion and multiplication of microorganisms in body tissues, which may be clinically inapparent or result in local cellular injury due to competitive metabolism, toxins, intracellular replication, or antigen-antibody response.
Dorland’s Illustrated Medical Dictionary 27th, Edition
Factors Associated with Increased risk of infection for dental implant procedures
Systemic Factors
1. Diabetes2. Long term corticosteroid use3. Immunocompromised systemic disorders4. Smoking5. Malnutrition, obesity6. Elderly population7. ASA III or IV classifications
Factors Associated with Increased risk of infection for dental implant procedures
Local Factors
1. Use of type or procedures of graft material
2. Generalized periodontal disease
3. Tissue inflammation
4. Odontogenic infections
5. ill-fitting provisional prosthesis
6. Incision line opening
7. Inadequate oral hygiene
Factors Associated with Increased risk of infection for dental implant procedures
Surgical Factors
1. Poor aseptic technique
2. Compromised skill and experience of the surgeon
3. Increased duration of surgical time
4. Wound contamination during surgery
5. Foreign body introduction (graft material, implants, debris, etc….)
Infection Prophylaxis
1) Aseptic Surgical techniques applied during all clinical grafting procedures.
2) Pre-operative Rx: Amoxicillin 500mg x 4 tablets (2 g), 1 hour prior to
surgery (Scientific Evidence)Post-operative 1 tablet t.i.d. for 1 week following surgery (Optional)
Infection Prophylaxis
3) Chemical Plaque control: Preoperative rinsing with .12%
Chlorhexidine digluconate for 1 minute.
Postoperative rinsing for 2-3 weeks with good oral hygiene.
4) Monitor and close follow up:Patient to return to clinic at 1-2 weeks to evaluate healing status.
Infection Prophylaxis
5) Confirm lack of localized infection from adjacent tooth (endodontic origin) or soft tissues (periodontitis) spreading into grafting site.
Diabetes
1. Higher prevalence in Adult African Americans, native and Hispanic Americans
2. Risk factors: Genetics, obesity, advancing age and inactive lifestyles.
3. Characterized by:1. Peripheral resistance to insulin
2. Increased production of glucose by the liver
3. Altered pancreatic insulin secretion.
Oral Manifestations for a Diabetic Patient
1. Poor wound healing (soft tissues, osseointegration)
2. Higher susceptibility to oral infections
3. Xerostomia
4. Higher incidence of dental caries
5. Pronounced hyperplasia of attached gingival
6. Increased accumulation of plaque and food debris
7. Neuropathy (burning mouth, tingling, numbness)
8. Greater incidence and severity of periodontal disease
9. Candidiasis and lichenoid reactions
Signs of Hypoglycemia:
1. Sweating
2. Palpitations
3. Tachycardia
4. Nausea
5. Hunger
6. Tremulousness
7. The symptoms may progress to coma and convulsions without intervention.
Management of type I diabetic patients: (To prevent Insulin shock)
1. Patient instructed to take their usual dosage of insulin medications
2. To eat a normal meal prior to appointment
3. Schedule the appointment early in the morning
4. Patient to communicate with dentist if they feel symptoms of an insulin reaction
5. A source of sugar available in office (orange juice, candy, sugar packs)
6. May consider Antibiotic prophylaxis coverage to prevent infections which is related to the fasting blood glucose levels.
Dental Managements
1. Minimize stress
2. Decrease risks of infection (Post operative antibiotics: Amoxicillin 500 mg, t.i.d. or Clindamycin 300 mg, t.i.d. for 7-10 days)
3. Avoid untoward metabolic imbalances during dental therapy
4. Instructions for diet and medications to avoid hypoglycemia.
Management of Hypoglycemia
1.Sugar source readily available (sugar packets, candy, orange juice)
2.Dextrosol 3mg tablets of glucose
3.Glucagon 1 mg IM
4.50% Glucose solution 50 ml IV
Bisphosphonates Induced Osteonecrosis of the Jaws (ONJ)
Defined as a non healing bone in the mandible or maxilla present for 8 weeks in a person that is on Bisphosphonates and
hasn’t received radiation to the jaws.
Risk of osteonecrosis of the jaws
• Exposed bone is dead with usually no pain.
• Pain may occur due to secondary infection
• The jaw bones are susceptible because the jaw bone remodels 10 times that of long bones in the body.
Bisphosphonates
• Used for treatment of osteoporosis, metastatic bone cancer and Paget’s disease.
• Oral form: Fosamax, Boniva, Actinol
• IV form: Aredia, Zonita
Mechanism of Bisphosphonates
• Mechanism of action by suppressing and reducing bone resorption by osteoclasts.
• Bisphosphonates inhibit osteoclasts by killing them when they take up the drug during resorption.
• Bisphosphonates binds to the hydoxyapatite in the bone
Bisphosphonates
• IV medications are worse then oral types.• Risk increase after being on oral medications
for > 3 years.• IV takes 6 months to build to toxic level• Oral takes 3 years to build to toxic level
• 140 IV reported cases versus 40 Oral cases
• Incidence: IV: .8%-12%• Incidence: Oral: .01%-1%
Signs of ONJ
• Sclerosis and thickening of the lamina dura
• Widening of the periodontal ligament (PDL)
• Mobile teeth with pain
• Exposed bone with necrosis of bone and soft tissues
• Non healing bone post surgical wound
Treatment of ONJ• We don’t know what is the best treatment protocol.
Dr. Robert Marx seems to be the expert on this topic.• Peridex rinse over surgical wound
• Antibiotics: a) Pen VKb) Levoquin (limit to 21 days due
to liver toxicity)
• Reduce risk of secondary infections and osteomylitis of the jaws.
• 50 % of cases will spontaneously heal.• 50 % of cases will require additional surgeries.
Prevention of ONJ
• Non invasive dental procedures are safe.
• Invasive dental procedures safe before 3 years.
• After 3 years- a drug holiday with consent of prescribing physician to a CTX of >= 150 pg/ml.
Serum C terminal telopeptide test (CTX)
• After 3 years of Bisphosphonate use, need a CTX to determine safety level.
• CTX <= 100 pg/ml: HIGH risk• CTX = 101-150 pg/ml: Moderate risk• CTX >= 150 pg/ml: Low risk
• CTX improves significantly with discontinued oral Bisphosphonates use.
• CTX is a marker for bone turnover and healing.• Measures osteoclast function as a C terminal fragment
is cleaved during bone resorption.

Suggested Treatment Regimen
• 1) Obtain references for CTX level
• 2) Drug holiday of 4-6 months with approval from prescribing physician.
• 3) Treat with Peridex (.12%) and antibiotics.
• 4) Monitor CTX until value is >150 pg/ml
• 5) Decide to refer or monitor for treatment options:
A) Spontaneous resolution
B) Treat surgically

Psychological Status
1. Psychological and mental stability for patient to accept and tolerate required procedures
2. Normal healing response and sequelae of bone and soft tissue grafting procedures
3. The 3 “C’s” prior to treatment:a) Communicationb) Compliancec) Consent
Host / Patient Related:
Normal healing response and sequelae of bone and soft tissue grafting procedures are:
• Hemorrhage / bleeding
• Ecchymosis / bruising
• Pain / discomfort
• Swelling
Host / Patient Related:
Hemorrhage / bleeding Management
1) Management of intra operative bleeding source (soft tissue / bone) prior to suturing.
2) Proper soft tissue suturing techniques to ensure primary closure without tension of soft tissues.
3) Proper use of sterile gauze pads with moistened sterilesaline solution with FIRM pressure over wound for 20 minutes.
4) Oral and written instructions for care to prevent vasoactive substance (caffeine or alcohol), minimize exercise, post operative care to minimize disturbance to wound clotting, oral hygiene instruction care.
Ecchymosis (Bruising)
• Due to extravasation and subsequent breakdown of blood in the subcutaneous tissues.
• Deposition of blood from the surgery in the interstitial tissues spaces and will be resorbed over a time period of 1-3 weeks.
• Occurs more in fair skinned patients and elderly patients with fragile capillaries.
Ecchymosis Management
1) Inform patient that it will be a normal sequelae of any surgical procedure.
2) Inform patient that degree of bruising is NOT an indicator of success / failure, traumatic / atraumatic nature of procedure or operator.
3) Application of ice bag or cold packs immediately after surgery for 2 days.
Pain / discomfort Management
1) Long term Local anesthetics:a) Bupivacaine (Marcaine / Vivacaine): 0.5% w
1:200,000 epinephrine used for block anesthesia. Duration time of 6-8 hours.
b) Articaine (Ultracaine Forte / Astracaine): 4% w 1: 200,000 epinephrine. Duration time of 4 hours.
2) Analgesics:a) NSAIDS: Ibuprofen 400mg (600-800mg if anticipate
swelling), 1 hour prior to surgery, then 1 tablet every 6-8 hours continuous for 2-3 days.
b) Narcotics: Tylenol #3, 1-2 tablets every 4-6 hours as required for pain relief.
Swelling Management 1) Application of ice bag or cold packs immediately after surgery
for 2 days.
2) I.V. administration of glucocorticoid steroids (prednisolone 250mg or dexamethasone 8 mg) prior to start of surgery.
3) I.M. administration of Dexamethasone / Decadron (Celestone Soluspan Injectable)6mg/per site adjacent to surgical
wound.
4) P.O. prescription of Dexamethasone (Decadron) 4 mg with regimen as follows:
– Preoperative 4mg x 2 tablets = 8 mg, 1hour prior to surgery– Postoperative 4mg x 1 tablet = 4 mg, 1st day after surgery– Postoperative 4mg x .5 tablet = 2 mg, 2nd day after surgery– Postoperative 4mg x .5 tablet = 2 mg, 3rd day after surgery
Complication
A secondary disease or condition aggravating an already existing one.
Dorland’s Illustrated Medical Dictionary 27th, Edition
Complication
Defined as a secondary condition that developed during or after implant surgery or prosthesis placement. The occurrence of a complication does not necessarily indicate that substandard dental care was provided and also does not necessarily mean that clinical failure has occurred.
Sequelae
Any lesion, condition, consequence or affection following a clinical procedure injury or caused by an attack of previous disease.
Dorland’s Illustrated Medical Dictionary 27th, Edition
a) Communication
Share or exchange information, news, or ideas
Oxford Dictionary 10th Edition
Allocate appropriate amount of TIME to educate and communicate prior to consent to treatment. Utilize patient education video, documents and software to aid in communication process.
b) Compliance
Disposed to agree with others or obey rules, especially to an excessive degree. Meeting or in accordance with rules or standards.
Oxford Dictionary 10th Edition
A quality of yielding to pressure or force without disruption, or an expression of the measure of the ability to do so.
Dorland’s Illustrated Medical Dictionary 27th, Edition
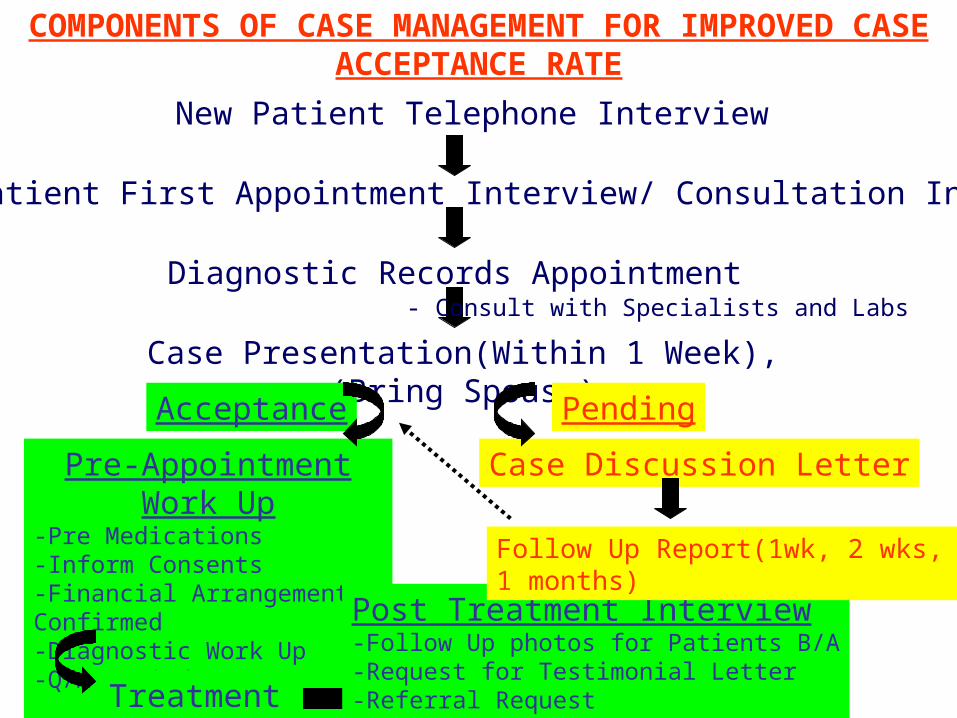
COMPONENTS OF CASE MANAGEMENT FOR IMPROVED CASE ACCEPTANCE RATE
New Patient Telephone Interview
New Patient First Appointment Interview/ Consultation Interview
Diagnostic Records Appointment
Case Presentation(Within 1 Week), (Bring Spouse)
Acceptance Pending
Case Discussion LetterPre-Appointment Work Up
-Pre Medications-Inform Consents-Financial Arrangements Confirmed-Diagnostic Work Up-Q/A Period
Treatment
Post Treatment Interview-Follow Up photos for Patients B/A-Request for Testimonial Letter-Referral Request
Follow Up Report(1wk, 2 wks, 1 months)
- Consult with Specialists and Labs
c) Consent Process
1. Communication and patient education
2. Process of informed consents and financial arrangements confirmed
3. Relationship and rapport development with patients
4. Continuous monitoring support, empathy and sincere compassionate care
Consequences of Smoking on wound healing
1. Arteriolar vasoconstriction reduces vascularization and microcirculations of tissues.
2. May lead to increase incidence of flap necrosis and dehiscence to early graft exposures.
3. Tobacco's toxic byproducts have been implicated as risk factors for impaired healing.
Studies on Smoking and Implants
Study # 1: 5% lost on non-smokers versus 11% on smokers. Smokers with higher implant failure rates in all regions except for the posterior mandible.
Study # 2: 3% lost on non-smokers versus 7% on smokers by number of implants. 9% lost on non-smokers versus 22% on smokers by number of patients. Regardless of method of analysis, a SIGNIGICANT difference was noted between smokers and non-smokers.
Studies on Smoking and Implants
Study # 3: Smoking cessation protocol of 1 week before surgery and 8 weeks after surgery.
-6% implant lost on non-smokers.
-38% implant lost on smokers WITHOUT smoking cessation program.
-12% implant lost on smokers WITH smoking cessation program.
Cessation protocol demonstrated improving implant success on treatment of smokers.
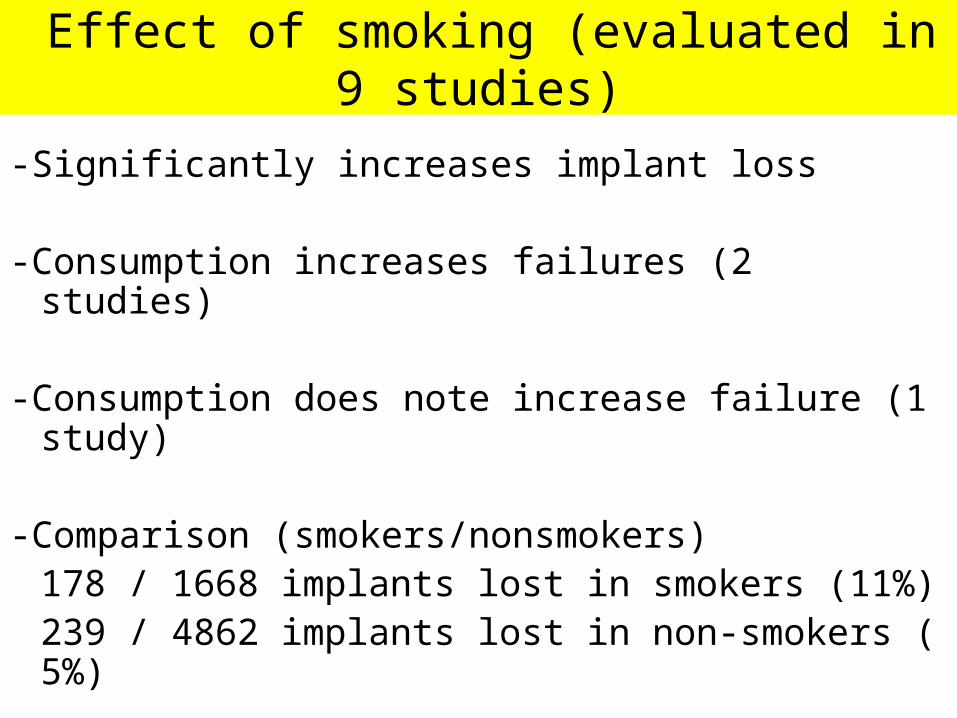
Effect of smoking (evaluated in 9 studies)
-Significantly increases implant loss
-Consumption increases failures (2 studies)
-Consumption does note increase failure (1 study)
-Comparison (smokers/nonsmokers)178 / 1668 implants lost in smokers (11%)
239 / 4862 implants lost in non-smokers ( 5%)
Management protocol for smokers
1) Don’t treat!
2) Smoking cessation programs
3) Treat with consent form

Tobacco and Nicotine Warning Consent forms
Nicotine and Tobacco Warning
The nicotine in tobacco constricts the blood vessels of your body. This effect is immediate and lasts up to one month. Furthermore, nicotine will reduce the amount of oxygen delivered to the body. This constriction of blood vessels and reduced oxygen delivered will affect the circulation of the tissues handled. Implant surgery and bone grafting may require extensive manipulation of soft tissues. The use of nicotine can compromise the healing and cosmetic outcome of these surgeries. YOU MUST STOP SMOKING one month prior to surgery. You must not smoke for at least three weeks following surgery. A nicotine patch may be used to help stop smoking. However, no nicotine patch or nicotine gum may be used one month prior to surgery and for three weeks after surgery. ________________________ _______________________ Parent Signature Date ________________________ _______________________ Witness Signature Date
Periodontal disease and Dental Implants
1. Implant survival in patients with a history of treated Periodontitis ranged from 59-100%
2. 17/18 studies reported high implant survival rates of >= 90% with turned or moderately rough implant surfaces
3. Need for continue regular supportive periodontal therapy
4. Statistically significantly greater risk of peri-implantitis, odds ratio of 3.1 to 4.7
Iatrogenic
Any adverse condition in a patient occurring as the result of treatment by a physician / dentist or surgeon, especially to infections acquired by the patient during the course of treatment.
Dorland’s Illustrated Medical Dictionary 27th, Edition
Implant Treatment Planning
Implantology is a “Prosthetically / Restorative” driven discipline with a “Surgical” component.
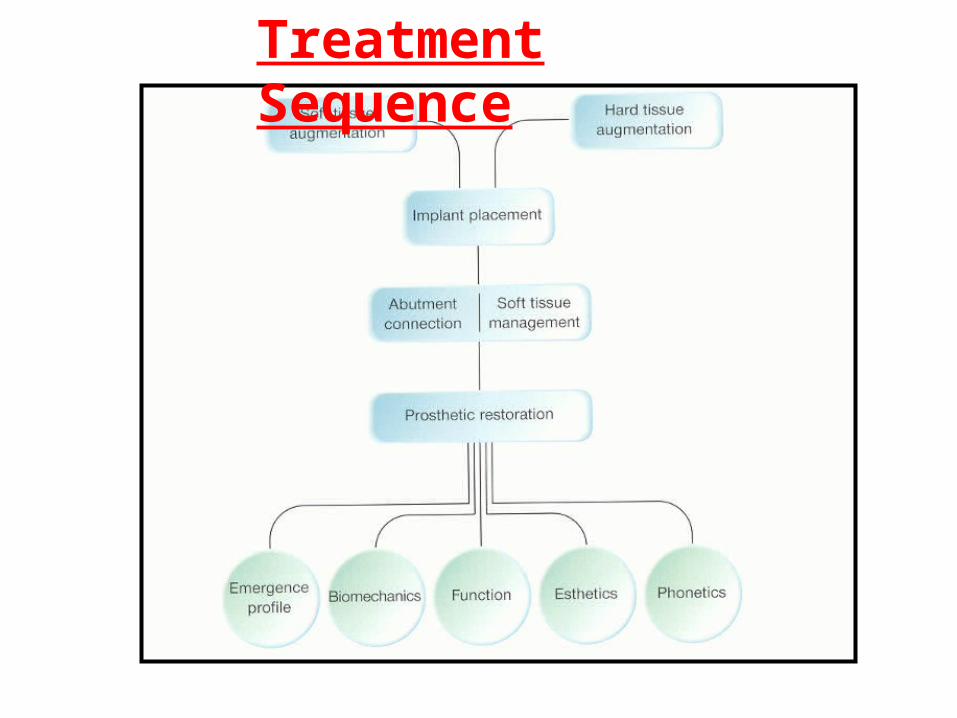
Treatment Sequence
Esthetic Implant Dentistry, Patrick Palacci, DDS
Improper Implant Treatment Planning
1) Improper surgical implant placements without desired prosthetic goals treatment planned
2) Improper use of number and location of dental implants for final prosthesis
3) Lack of understanding of Biomechanical rationale requirements for functional loads
Pretend the following:
-you had all the time -you had all the money-you had all the bone
-you had all the compliance
What is the most ideal treatment plan desired for
your patient?
Treatment planning philosophy- one of the most important factor to success
• Don’t compromise your ideal treatment plan with the following:
• -patient’s financial constraints.
• -unreasonable time demands for completion.
• -insurance limitations or moral compromises.
• -patient’s guidance on treatment decisions.
• (i.e. less implants, omit required grafting, use of material, etc….)
“The Lost Syndrome”1) Lost trust from the patient!
2) Lost patience from the patient who will require more surgeries and procedures!
3) Lost time and require to start again from a clinical condition in a MORE compromised state!
4) Lost clinical chair time to redo the case!
5) Lost lots of money to redo the case!
6) Lost of peace of mind! (Lawsuit or Regulatory College Complaint?)
Treatment planning philosophy- one of the most important factor to
success
My rule on Treatment Planning
Only treatment plan and execute implant treatment as you would for your own family members.
Improper use of number and location of dental implants for final prosthesis
Lack of understanding of Biomechanical rationale
requirements for functional loads
Biomechanical rationale
Definitions• Bone Remodeling- turnover or
internal restructuring of previously existing bone.
• It is a coupled tissue level phenomenon.• Activation- of osseous precursor cells.• Active Resorption.• Reversal or Quiescence.• Formation.
• Remodeling cycle called “Sigma”- in humans is 17 Weeks.
Definitions• Strain- the change in length divided by
the original length and the units of strain are given in percent.
• Too much bone strain at the implant interface causes bone loss.
• The strain to bone may be caused by the stress applied to the prosthesis.
Stress = _____
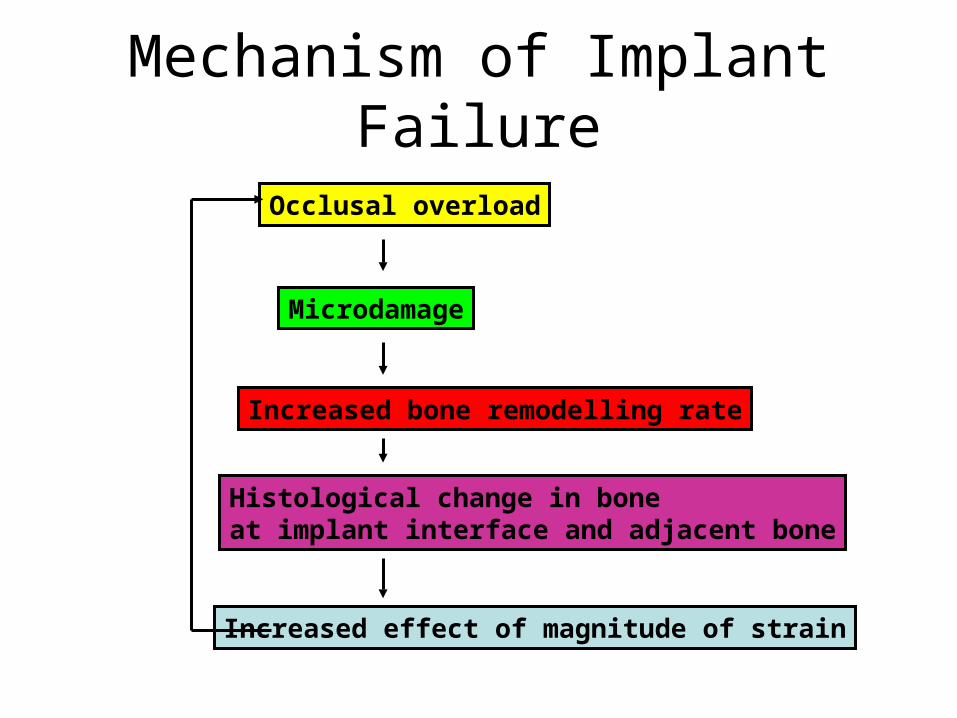
Mechanism of Implant Failure
Occlusal overload
Microdamage
Increased bone remodelling rate
Histological change in boneat implant interface and adjacent bone
Increased effect of magnitude of strain
Stress Factors• Excess stresses to an implant / bone interface will cause
overload and implant failure.
Complications from Stress:• -implant integration failure with fibrous tissue formation
around implant, mobility instead of rigid fixation.• -Early crestal bone loss.• -Occlusal overload bone loss• -Screw loosening (prosthesis or abutment)• -Implant fracture (body or component)• -Prosthesis fracture (occlusal material or framework)
5) Clinical Force factors
• 1) Bite Forces (light vs. normal vs. heavy)• 2) Parafunction• 3) Crown implant height ratio• 4) Masticatory Dynamics• 5) Opposing Arch• 6) Direction of load• 7) Nature of Opposing Arch• 8) Position of Abutment in the arch• 9) Occlusal scheme
1) Bite Forces (light vs. normal vs. heavy)
• Implant supported Fixed Prosthetics >
• Implant supported Removable Prosthetics >
• Natural dentition with Porcelain Prosthetics >
• Natural dentition >
• Partial Removable Prosthetics >
• Full Removable Prosthetics

2) Parafunction Repeated or sustained non-functional wear that is harmful to the stomatognathic system.
– A) Bruxism- vertical or horizontal nonfunctional grinding of teeth. A maximum bite force recorded at 990 psi (4-10 times normal)
– B) Clenching- a habit that generates a constant force exerted form 1 occlusal surface to the other without any lateral movement. Bruxing and clenching can exist in combination.
– C) Tongue Thrust and Size- unnatural force of the tongue against the teeth during swallowing.
Character Of Forces• A) Force Magnitude (heavy, medium, light)
• B) Force Duration
• C) Force Type (Compressive, tensile, shear)
• D) Force Direction
• E) Force Magnifiers (Horizontal and vertical cantilevers)
Surface Area for maximal Bone / implant interface
contacts
Options To Increase Surface Area
• 1) Increase Implant Numbers
• 2) Increase Implant Size and Length
• 3) Implant Design
• 4) Implant Surface conditioning
• 5) Bone Density
Surface Area for maximal Bone / implant interface contacts.
1) Maximize implant number.2) Maximize implant diameter.3) Maximize implant length.
(Without violation of the limits of bone volume or anatomical structures.)
4) Bone Density Classification
D1- Dense cortical ( > 1250 Hounsfield units)D2- Porous cortical and coarse Trabecular ( 850-1250 H. units)D3- Porous cortical (thin) and fine Trabecular (350-850 H. units)D4- Fine Trabecular (< 150 H. units)
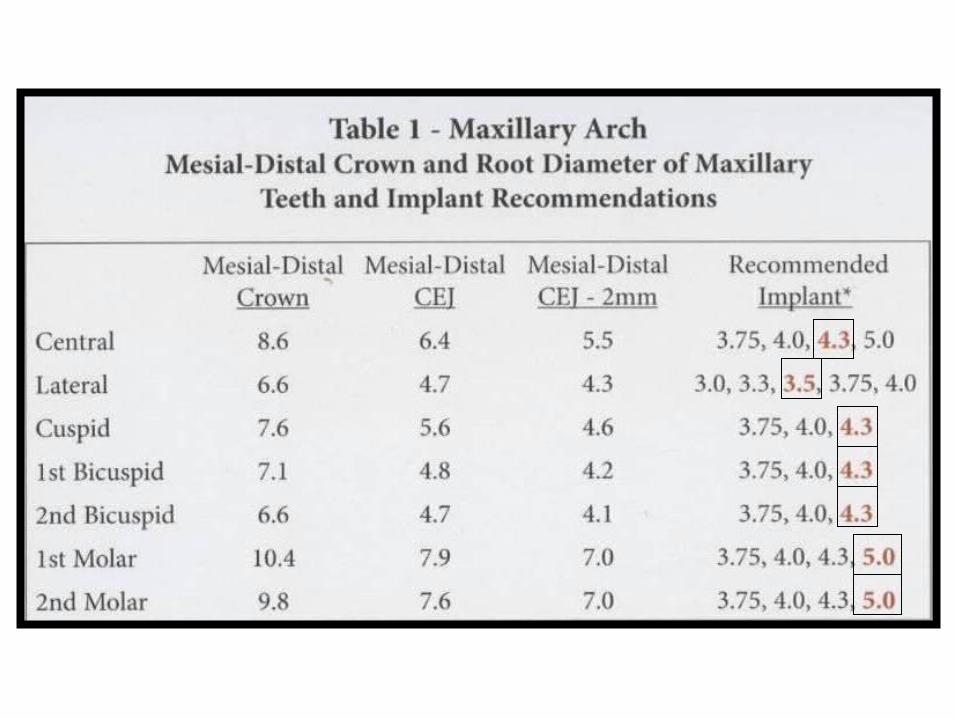
Goals of Diameter Of Implant1. Increase surface area
2. Compensate for unfavorable patient bite force factors
3. Minimize cantilevers for angled implants
4. Compensate for poor bone density
5. Enhance surface for shorter implants
6. Improve emergence profile
7. Decrease screw loosening
8. Minimize component fracture
9. Facilitate oral hygiene
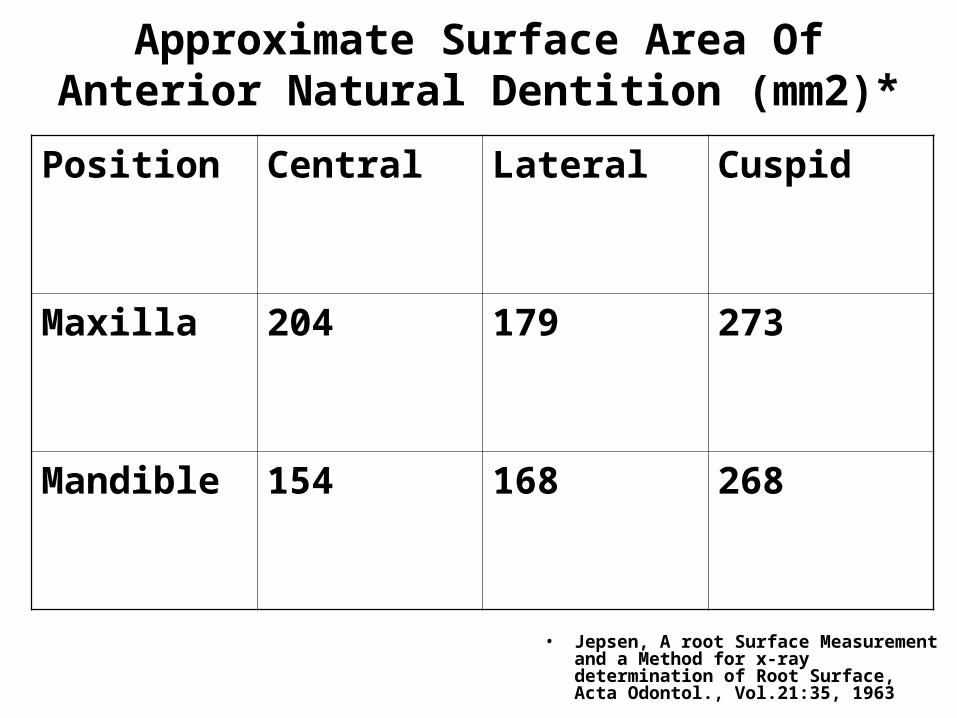
Approximate Surface Area Of Anterior Natural Dentition (mm2)*
• Jepsen, A root Surface Measurement and a Method for x-ray determination of Root Surface, Acta Odontol., Vol.21:35, 1963
Position Central Lateral Cuspid
Maxilla 204 179 273
Mandible 154 168 268
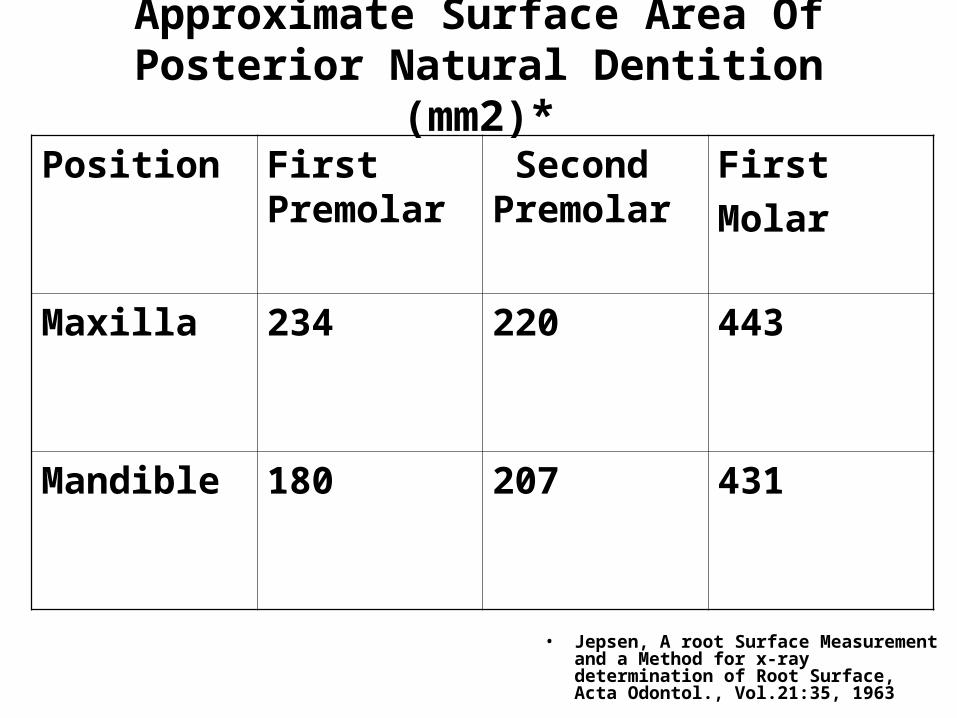
Approximate Surface Area Of Posterior Natural Dentition (mm2)*
• Jepsen, A root Surface Measurement and a Method for x-ray determination of Root Surface, Acta Odontol., Vol.21:35, 1963
Position First Premolar
Second Premolar
First
Molar
Maxilla 234 220 443
Mandible 180 207 431
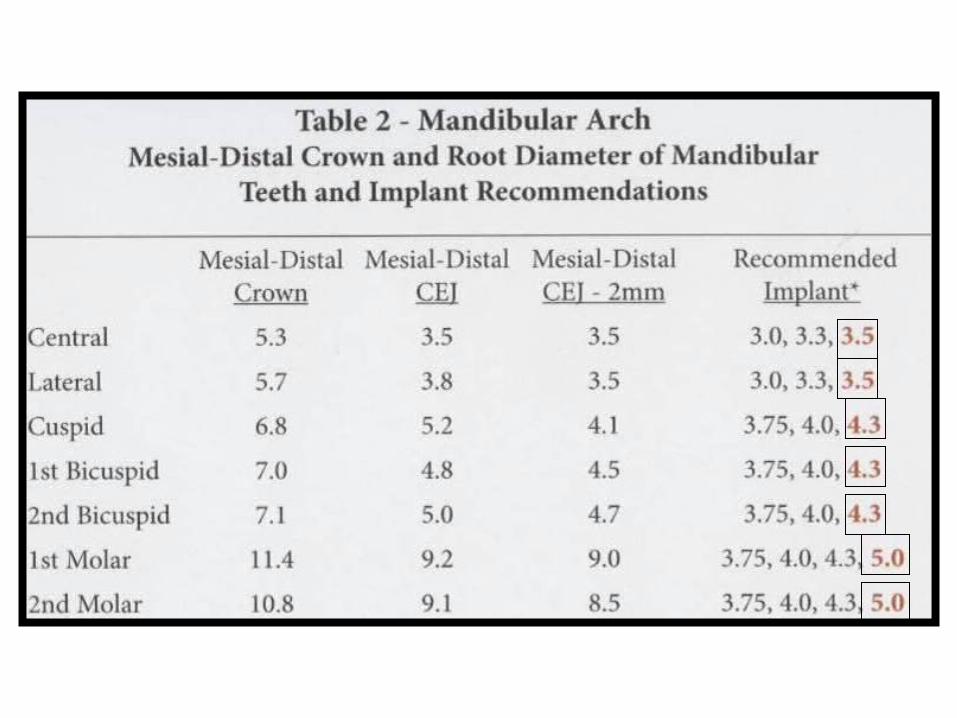
Goals of Length Of Implant1. Increase surface area
2. Compensate for unfavorable patient bite force factors
3. Gain initial ridged fixation of dental implant
4. Compensate for poor bone density
5. Not violate any vital anatomical anatomy (IAN, mental nerve, sinus, lingual concavities, nasal foramen, adjacent roots, etc….)
Failure Success
•Poor Bone Site Selection Short, Narrow, Porous
•Bone Site Selection High, Wide, Dense
•Implant Design Oversized implant
•Implant Choice/Design Bone around implant
•Poor Surgical Technique •Surgical Technique Proper implant placement Adequate healing time Sterile technique
•Poor Prosthetic Technique •Prosthetic Reconstruction Biomechanical design Occlusal relationships
•Poor Patient Cooperation •Patient Hygiene / Recall
Classification Of Oral Implant Failures
• 1) Biological:
• A) Early or Primary (before loading): Failure to establish osseointegration.
• B) Late or Secondary (after loading):Failure to maintain the achieved osseointegration.
Early or Primary (before loading): Failure
to establish osseointegration.
• 1) Inadequate quantity and quality of bone for initial fixation of dental implant.
• 2) Experience of surgical operator.
• 3) Over heating of bone during osteotomy preparations.
• 4) Pressure necrosis, especially in D1 bone.
• 5) Infection operatively after initial surgery.
• 6) Incision line opening leading to complications or infections.
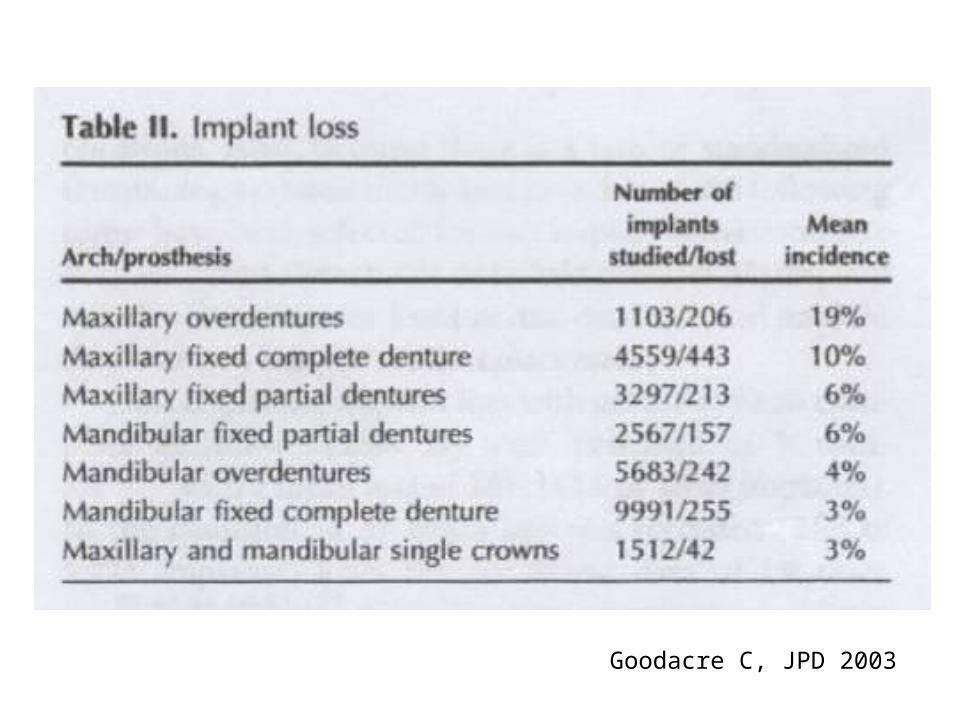
Goodacre C, JPD 2003
Classification Of Oral Implant Failures
• 2) Mechanical:
• Fracture of implants, connecting screws, bridge frameworks, coatings, porcelain, etc….
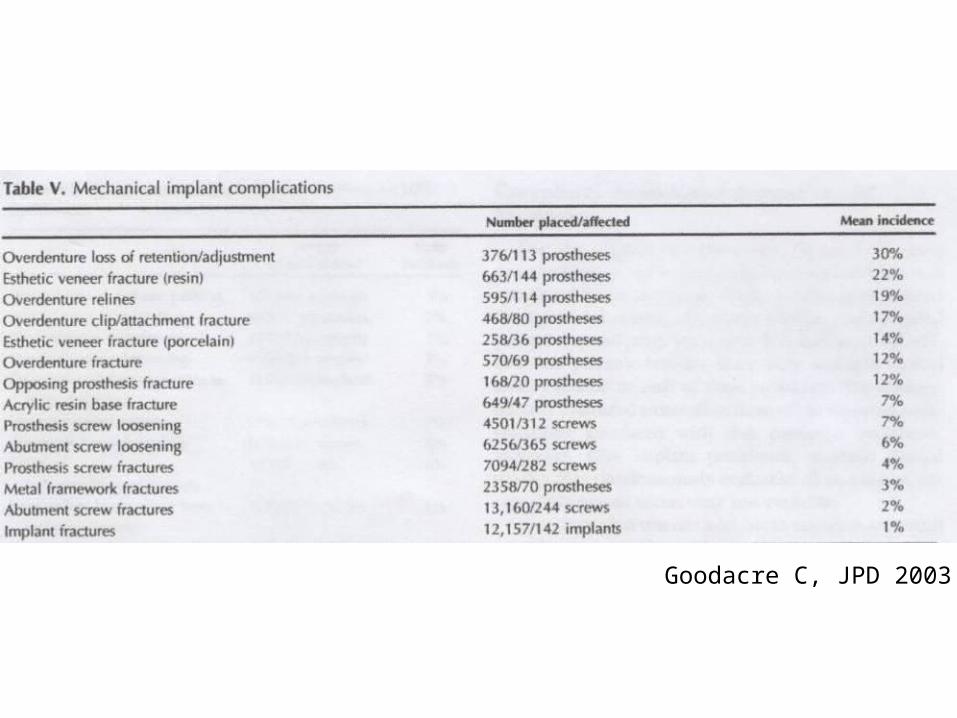
Goodacre C, JPD 2003
Iatrogenic
1) Treatment planning flaws and complications.
2) Violation of vital anatomical structures.
3) Inappropriate application of procedure to site requirement.
4) Compromised surgical skills.
5) Compromised prosthetic skills.
Types of Surgical Complications
A) Surgical complicationsB) Hemorrhage-related complicationsC) Neurosensory complicationsD) Mandibular fractureE) Adjacent Tooth devitalizationF) Life-Threatening hemorrhageG) Air EmboliH) Violation of Mandibular canalI) Aspiration of screwdriver, parts,
components

Surgical Parameter by REGIONS
Posterior Mandible
Surgical Parameter by REGIONSPosterior Mandible
D2 –D3 bone density• 1) Problem: Mandibular nerve location.
• Solution: Surgical landmark to be at least 2.0 mm above the mandibular canal to establish a surgical zone of safety.
• Pre-surgical diagnostic workup to measure allowed length of implant. Use of periapical and panoramic x-rays, tracings, CT scans to verify length.
• Surgical use of directional guide pins to verify proximity to mandibular nerve after initial pilot osteotomy.
• Remember: “The enemy of good is perfection.” If in doubt, use shorter implant lengths ( at least 10.0 mm)
Posterior Mandible
Factors to Consider in Zone
Potential Complications
Treatment Options
Damage to Inferior Alveolar Nerve (IAN)
Damage to Mental nerve
Paraesthesia Surgical landmark to be at least 2.0 mm above the mandibular canal to establish a surgical zone of safety
Use of Periapical and panoramic x-rays, tracings, CT scans to verify length.
Surgical use of directional guide pins to verify proximity to mandibular nerve after initial pilot Osteotomy.
Surgical Parameter by REGIONSPosterior Mandible
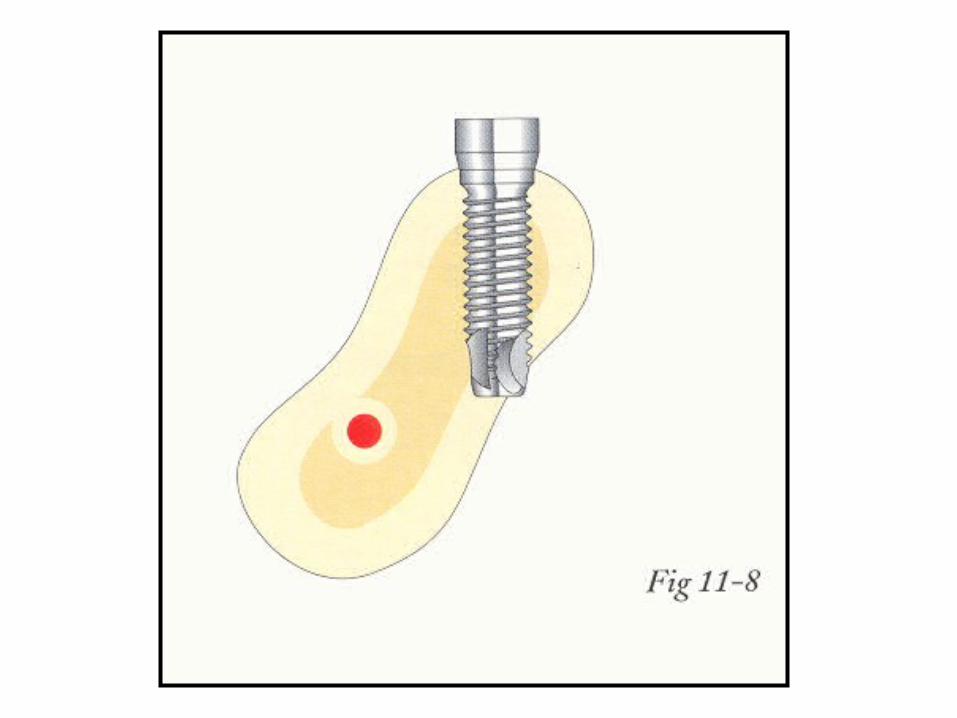
• 2) Problem: Lingual concavity and angulation flare of posterior mandible.
Solution: Use of CT scans to perform electronic surgery as part of treatment planning. Minimal reflection of lingual flap to visualize lingual wall of bone trajectory. Implant length to meet biomechanical requirement without anatomical violations.
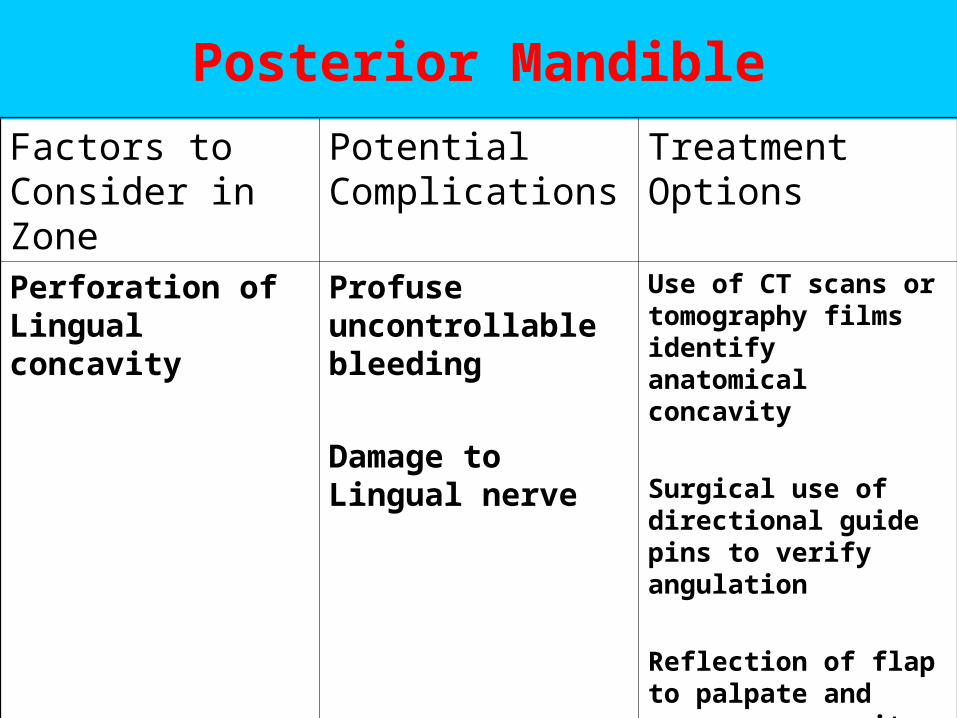
Posterior Mandible
Factors to Consider in Zone
Potential Complications
Treatment Options
Perforation of Lingual concavity
Profuse uncontrollable bleeding
Damage to Lingual nerve
Use of CT scans or tomography films identify anatomical concavity
Surgical use of directional guide pins to verify angulation
Reflection of flap to palpate and measure concavity undercut
Contraindications to posterior single –tooth implant
• 3) Inadequate bone volume –
• Width-consider grafting or alveloplasty or implant placement with guided bone regeneration.
• Length- Mesialdistal, intratooth space, need >7 for a 4.0mm implant with 1.5mm between implant and adjacent tooth.
• Height- no treatment, shorter implants, or particulate grafting of exposed threads.
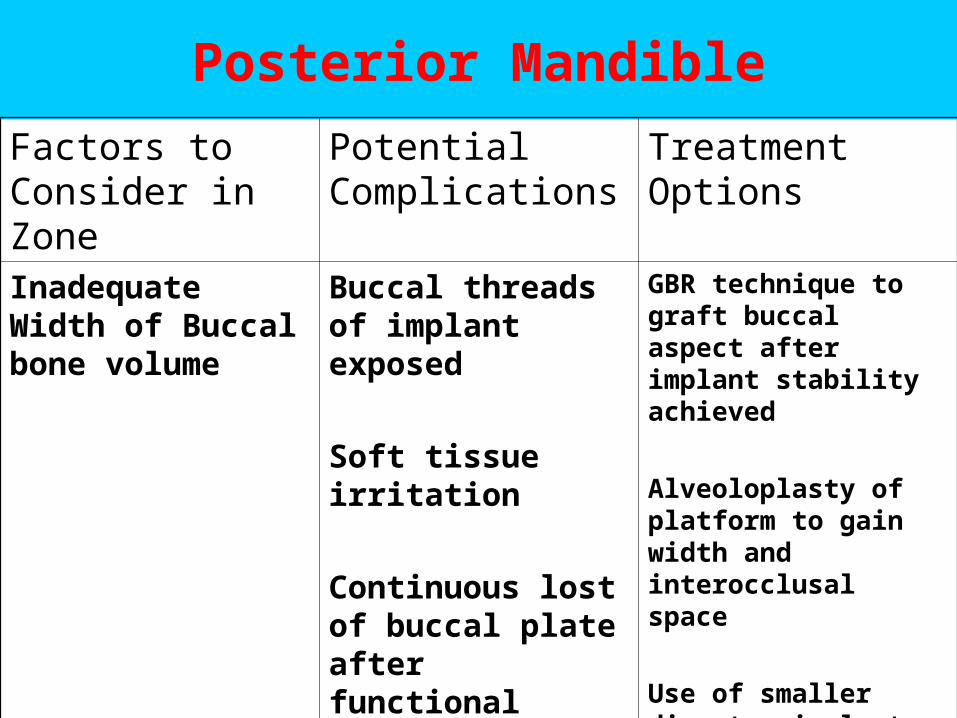
Posterior Mandible
Factors to Consider in Zone
Potential Complications
Treatment Options
Inadequate Width of Buccal bone volume
Buccal threads of implant exposed
Soft tissue irritation
Continuous lost of buccal plate after functional loading
GBR technique to graft buccal aspect after implant stability achieved
Alveoloplasty of platform to gain width and interocclusal space
Use of smaller diameter implant to accept compromise (>4.0 mm)
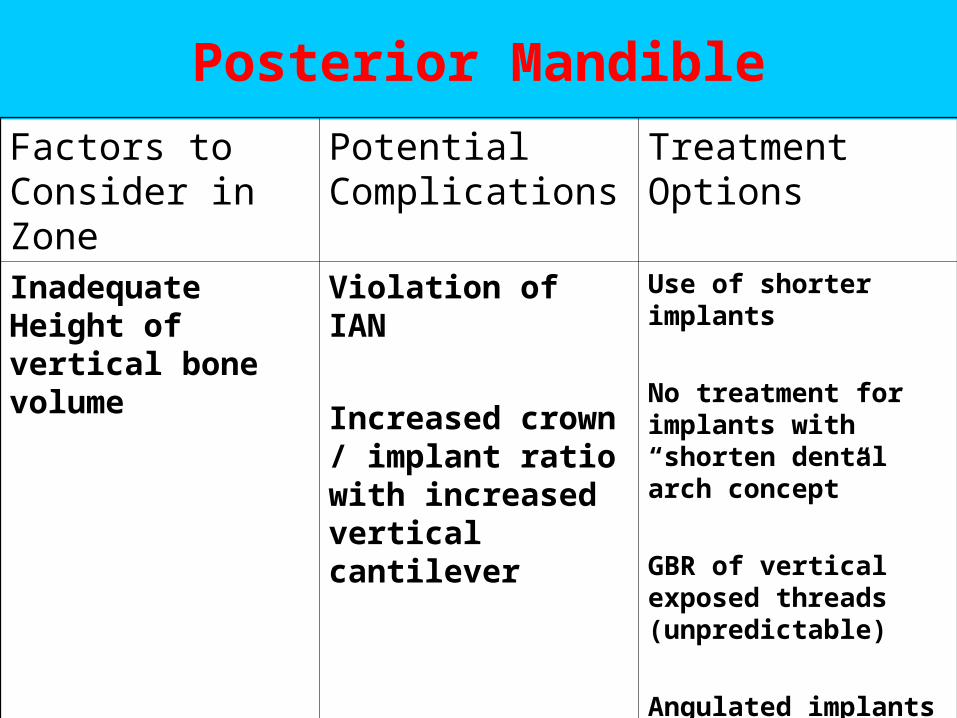
Posterior Mandible
Factors to Consider in Zone
Potential Complications
Treatment Options
Inadequate Height of vertical bone volume
Violation of IAN
Increased crown / implant ratio with increased vertical cantilever
Use of shorter implants
No treatment for implants with “shorten dental arch concept”
GBR of vertical exposed threads (unpredictable)
Angulated implants
Nerve Repositioning
Surgical Parameter by REGIONS
Anterior Maxilla
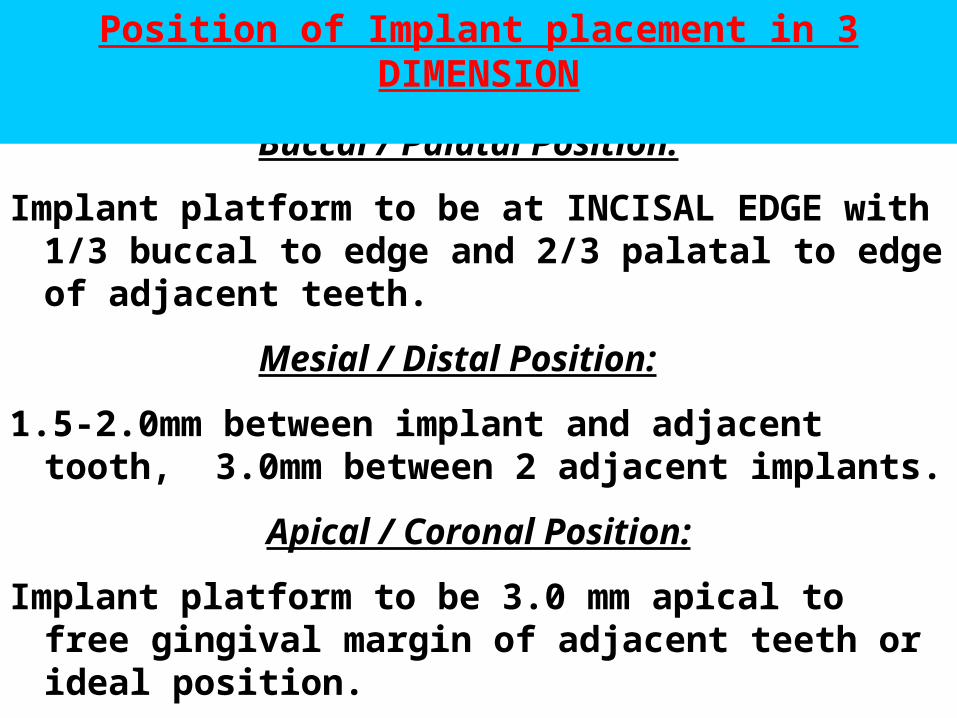
Buccal / Palatal Position:
Implant platform to be at INCISAL EDGE with 1/3 buccal to edge and 2/3 palatal to edge of adjacent teeth.
Mesial / Distal Position:
1.5-2.0mm between implant and adjacent tooth, 3.0mm between 2 adjacent implants.
Apical / Coronal Position:
Implant platform to be 3.0 mm apical to free gingival margin of adjacent teeth or ideal position.
Position of Implant placement in 3 DIMENSION
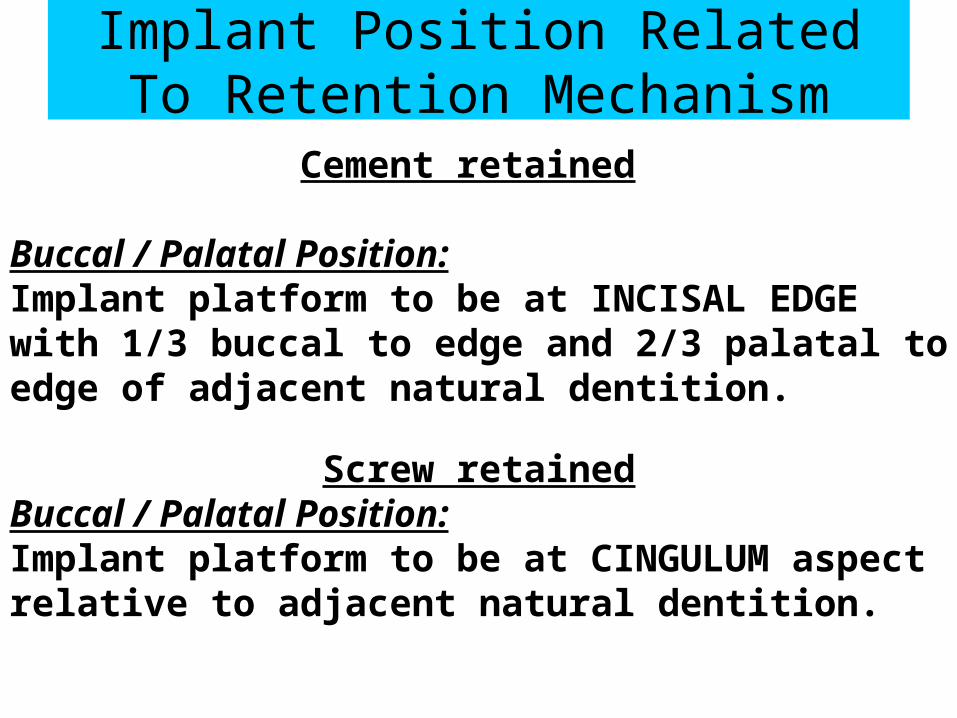
Implant Position Related To Retention Mechanism
Cement retained
Buccal / Palatal Position:Implant platform to be at INCISAL EDGE with 1/3 buccal to edge and 2/3 palatal to edge of adjacent natural dentition.
Screw retainedBuccal / Palatal Position: Implant platform to be at CINGULUM aspect relative to adjacent natural dentition.
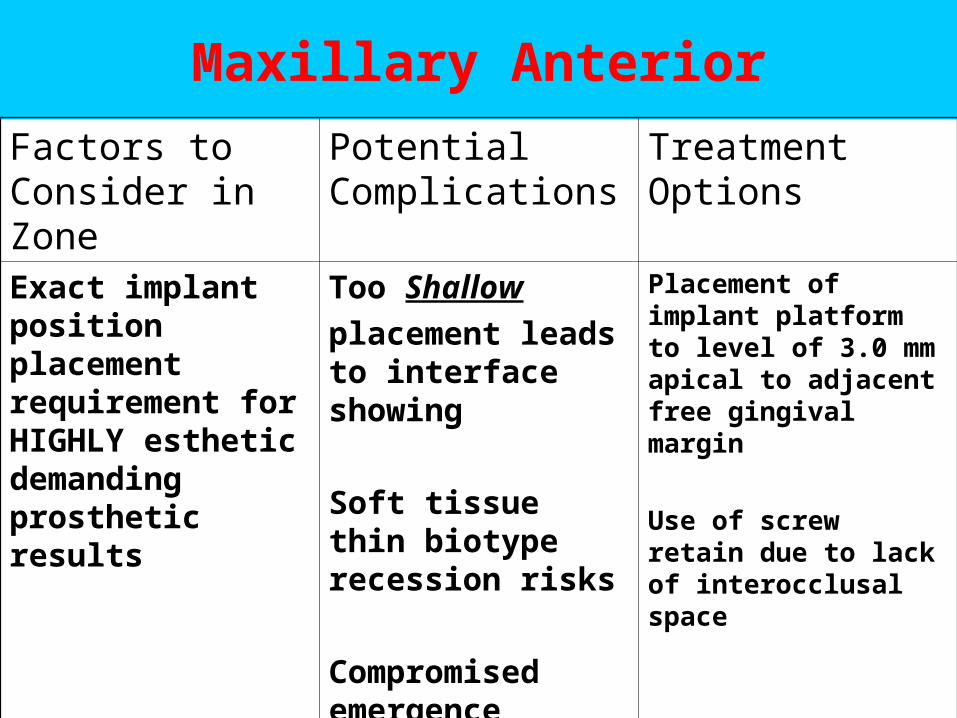
Maxillary Anterior
Factors to Consider in Zone
Potential Complications
Treatment Options
Exact implant position placement requirement for HIGHLY esthetic demanding prosthetic results
Too Shallow
placement leads to interface showing
Soft tissue thin biotype recession risks
Compromised emergence profile
Placement of implant platform to level of 3.0 mm apical to adjacent free gingival margin
Use of screw retain due to lack of interocclusal space
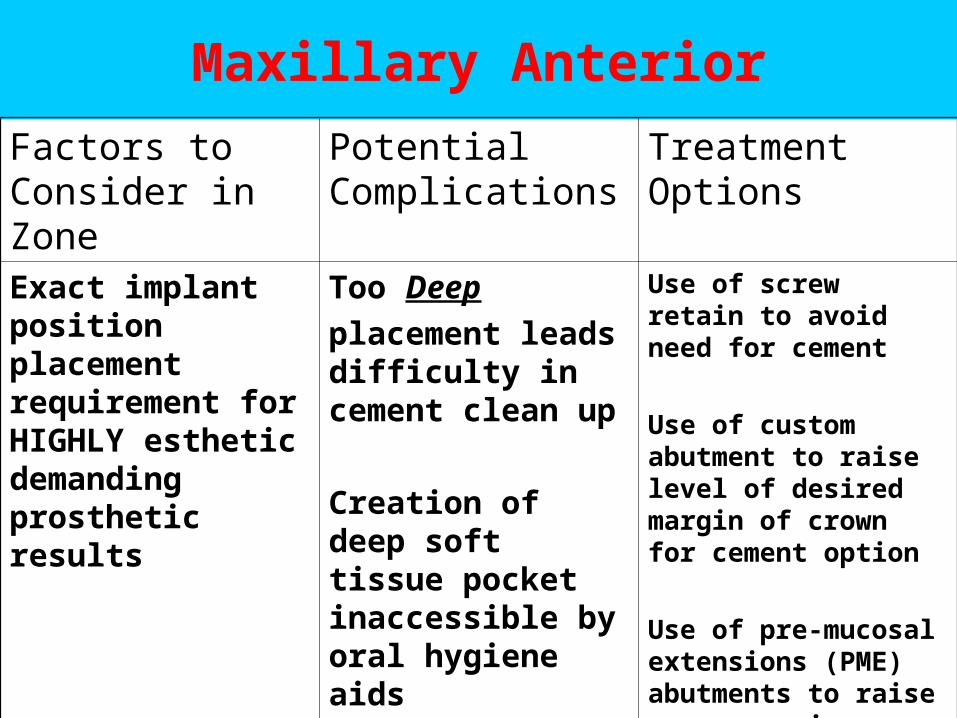
Maxillary Anterior
Factors to Consider in Zone
Potential Complications
Treatment Options
Exact implant position placement requirement for HIGHLY esthetic demanding prosthetic results
Too Deep
placement leads difficulty in cement clean up
Creation of deep soft tissue pocket inaccessible by oral hygiene aids
Use of screw retain to avoid need for cement
Use of custom abutment to raise level of desired margin of crown for cement option
Use of pre-mucosal extensions (PME) abutments to raise crown margin
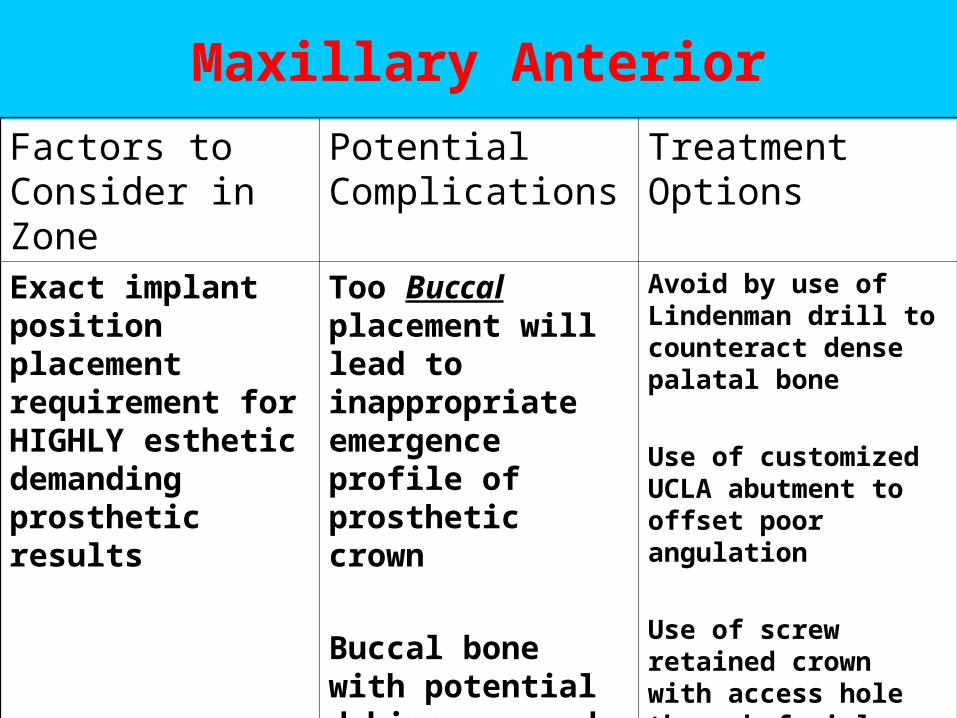
Maxillary Anterior
Factors to Consider in Zone
Potential Complications
Treatment Options
Exact implant position placement requirement for HIGHLY esthetic demanding prosthetic results
Too Buccal placement will lead to inappropriate emergence profile of prosthetic crown
Buccal bone with potential dehiscence and soft tissue recessions
Avoid by use of Lindenman drill to counteract dense palatal bone
Use of customized UCLA abutment to offset poor angulation
Use of screw retained crown with access hole through facial aspect
Remove implant
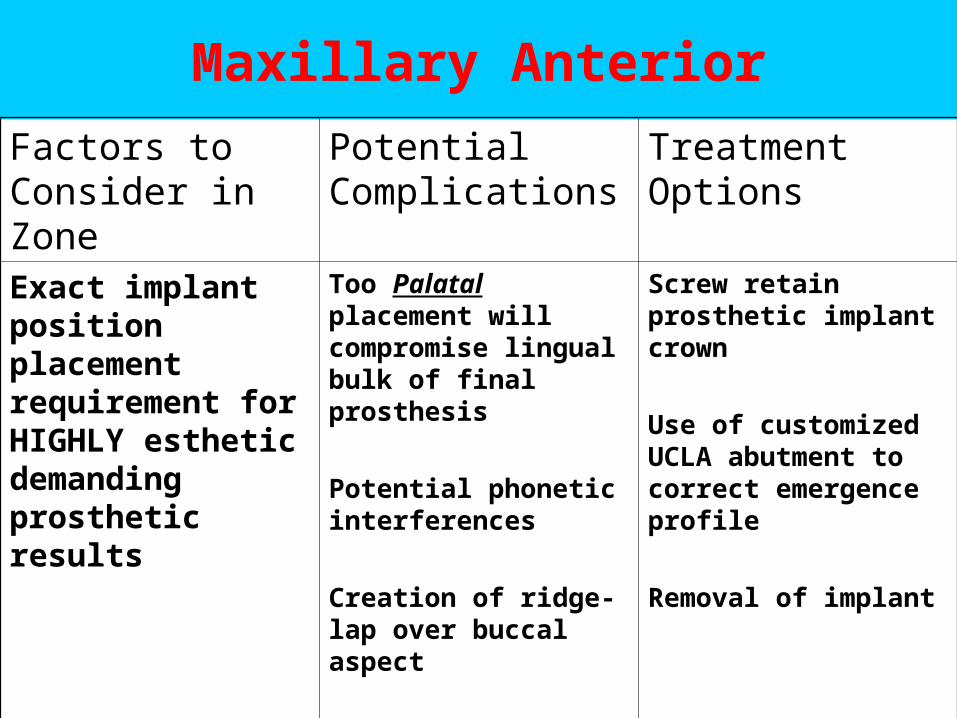
Maxillary Anterior
Factors to Consider in Zone
Potential Complications
Treatment Options
Exact implant position placement requirement for HIGHLY esthetic demanding prosthetic results
Too Palatal placement will compromise lingual bulk of final prosthesis
Potential phonetic interferences
Creation of ridge-lap over buccal aspect
Potential violation of incisive foramen/canal
Screw retain prosthetic implant crown
Use of customized UCLA abutment to correct emergence profile
Removal of implant
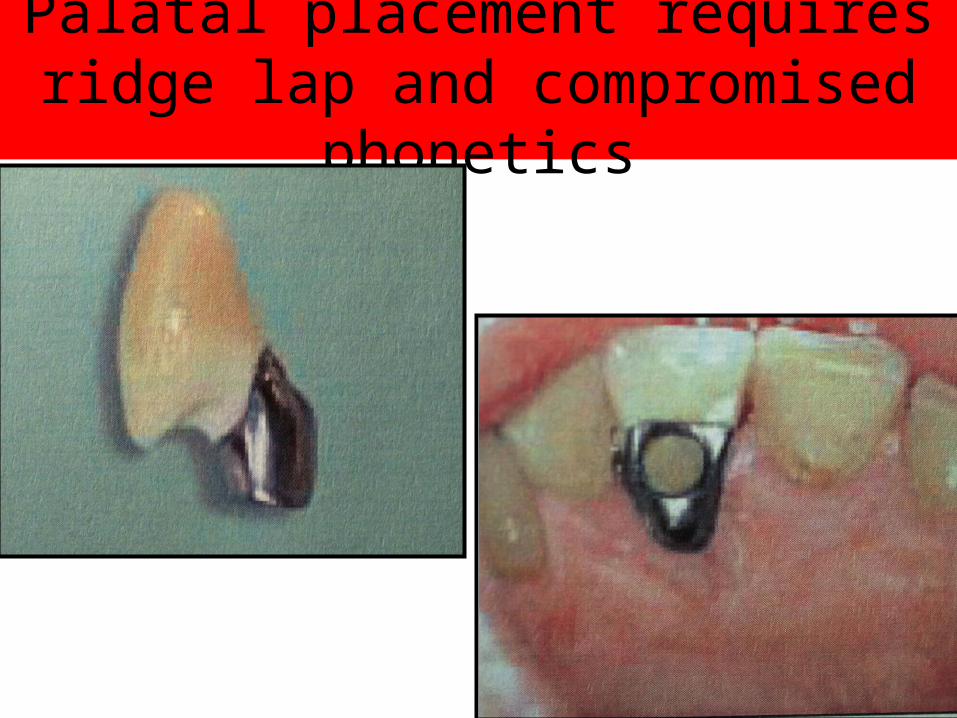
Palatal placement requires ridge lap and compromised phonetics
Surgical Parameter by REGIONS
Anterior Mandible
Surgical Parameter by REGIONSAnterior Mandible
• D1-D2 bone density• 1) Problem: Overheating during
osteotomy preparations.
– Solution: Prepare osteotomy with constant pumping motion
and use higher torque speed. Use new
drills with copious COOLED irrigations and
incremental drill sequence.
Surgical Parameter by REGIONSAnterior Mandible
• 2) Problem: Pressure necrosis of devital zone of bone around implants. (Early signs of RL around implants during healing with symptoms of pain to patient.)
• Solution: Must bone tap with hand ratchet each osteotomy site prior to surgical implant placement. Reverse torque final implant position by 1/4 - 1/2 turn to relieve internal stresses
and pressure.
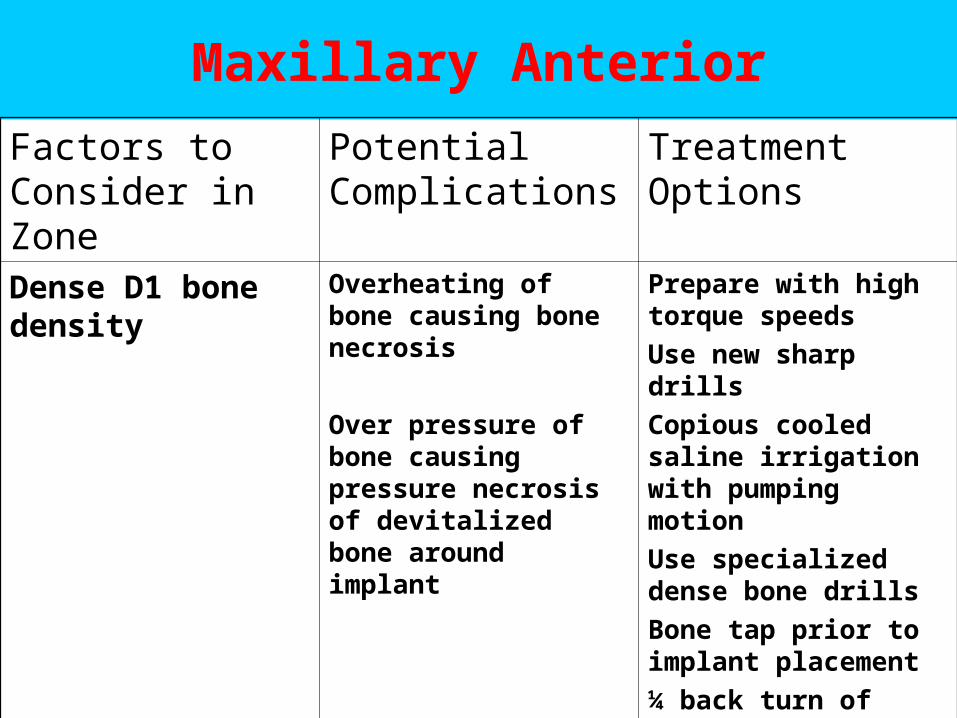
Maxillary Anterior
Factors to Consider in Zone
Potential Complications
Treatment Options
Dense D1 bone density
Overheating of bone causing bone necrosis
Over pressure of bone causing pressure necrosis of devitalized bone around implant
Prepare with high torque speeds
Use new sharp drills
Copious cooled saline irrigation with pumping motion
Use specialized dense bone drills
Bone tap prior to implant placement
¼ back turn of final implant position to release stress
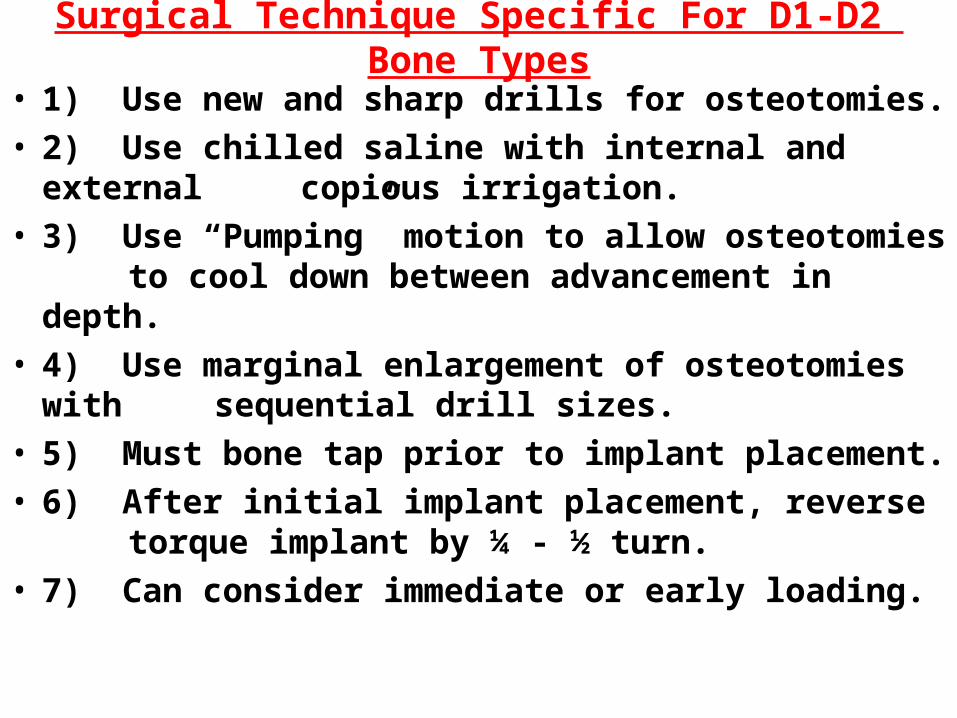
Surgical Technique Specific For D1-D2 Bone Types
• 1) Use new and sharp drills for osteotomies.• 2) Use chilled saline with internal and external
copious irrigation.• 3) Use “Pumping” motion to allow osteotomies to
cool down between advancement in depth.• 4) Use marginal enlargement of osteotomies with
sequential drill sizes.• 5) Must bone tap prior to implant placement.• 6) After initial implant placement, reverse torque
implant by ¼ - ½ turn.• 7) Can consider immediate or early loading.
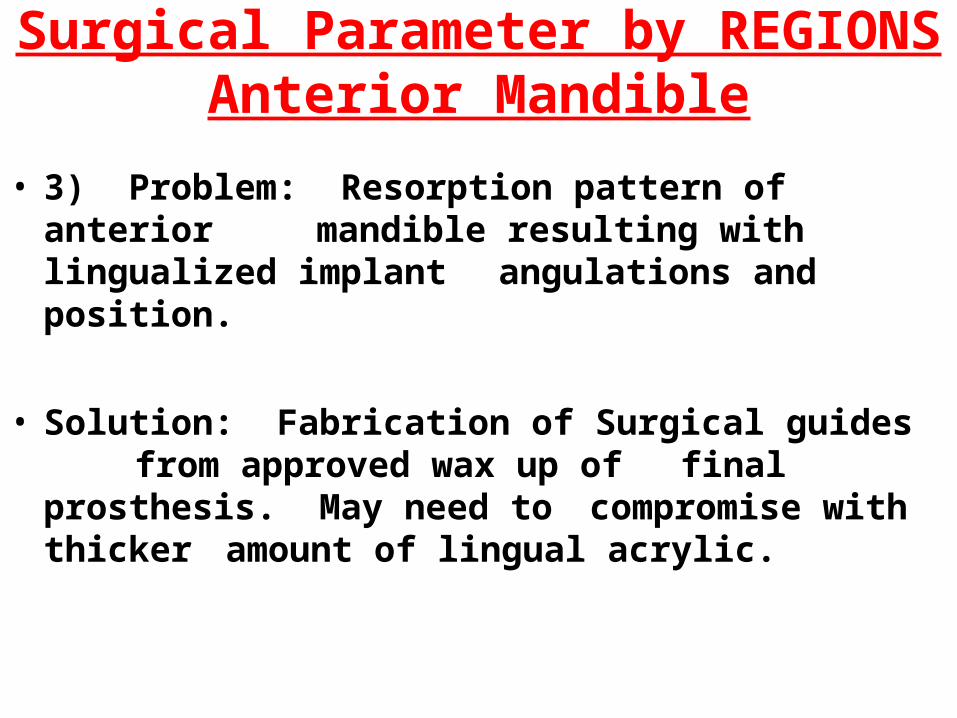
Surgical Parameter by REGIONSAnterior Mandible
• 3) Problem: Resorption pattern of anterior mandible resulting with lingualized implant angulations and position.
• Solution: Fabrication of Surgical guides from approved wax up of final prosthesis. May need to compromise with thicker amount of lingual acrylic.
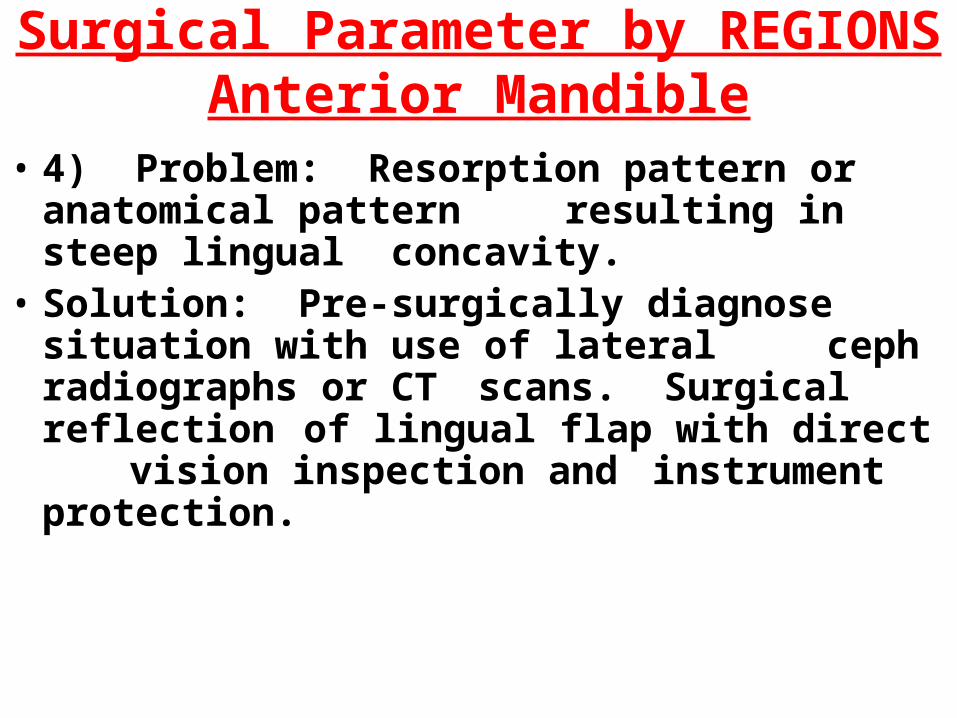
Surgical Parameter by REGIONSAnterior Mandible
• 4) Problem: Resorption pattern or anatomical pattern resulting in steep lingual concavity.
• Solution: Pre-surgically diagnose situation with use of lateral ceph radiographs or CT scans. Surgical reflection of lingual flap with direct vision inspection and instrument protection.
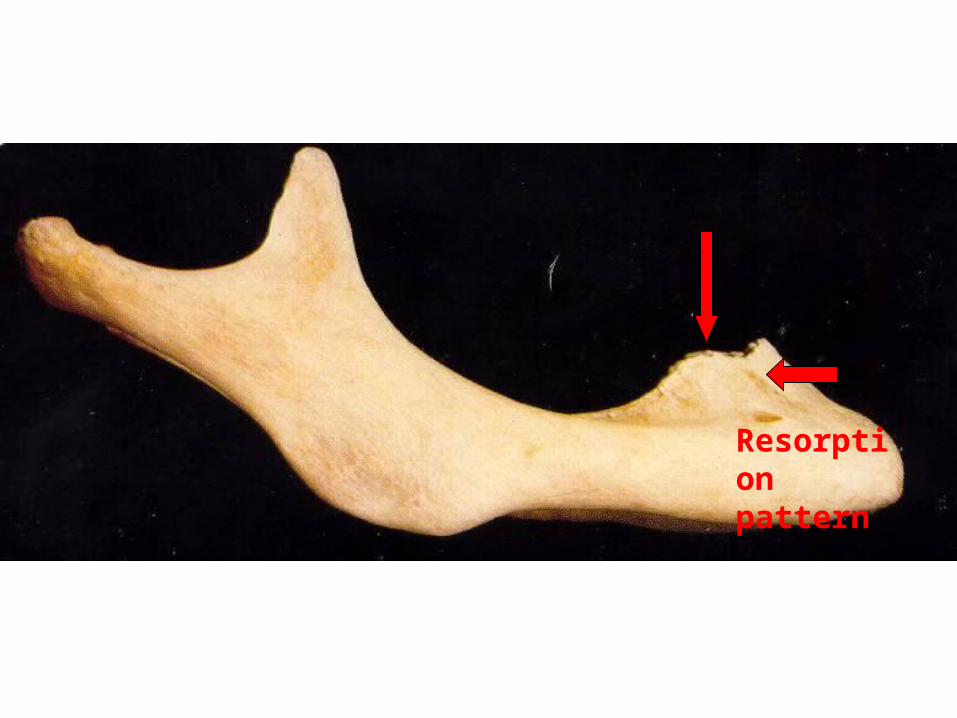
Resorption pattern
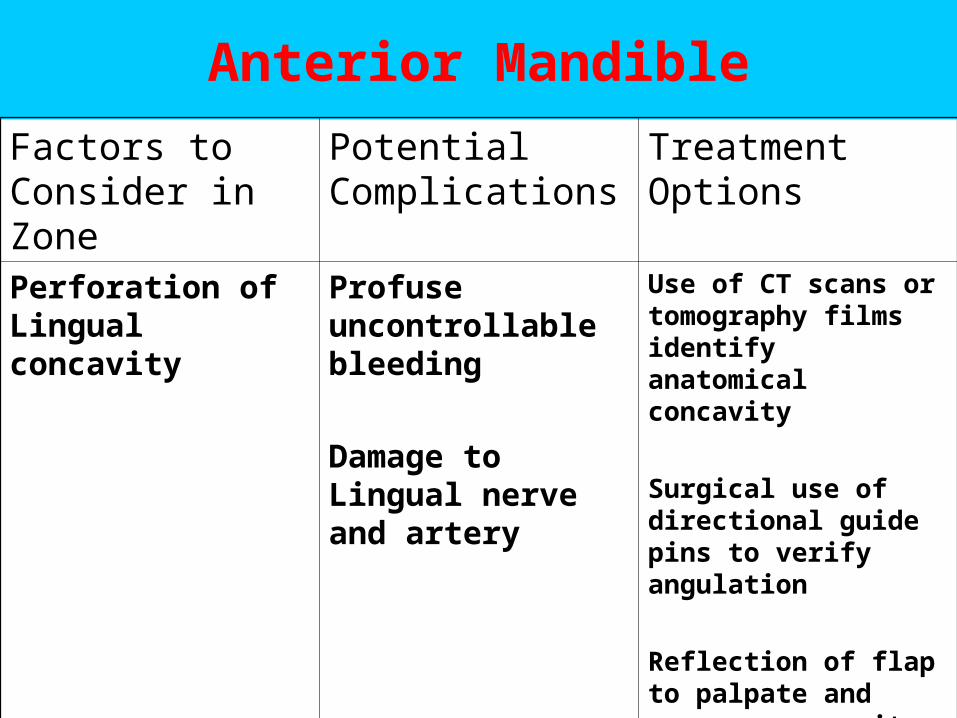
Anterior Mandible
Factors to Consider in Zone
Potential Complications
Treatment Options
Perforation of Lingual concavity
Profuse uncontrollable bleeding
Damage to Lingual nerve and artery
Use of CT scans or tomography films identify anatomical concavity
Surgical use of directional guide pins to verify angulation
Reflection of flap to palpate and measure concavity undercut
Surgical Parameter by REGIONSAnterior Mandible
• 5) Problem: Location of Mental foramen with or without anterior loop.
Solution: Locate the mental nerve by anatomical location relative to the face. Vertical line through pupils of the patient’s eyes passes through infraorbital and mental foramen. Finger width lateral to ala of the nose also is on this vertical landmark.
Surgical dissection to identify and locate the mental nerve with safety zones marked.
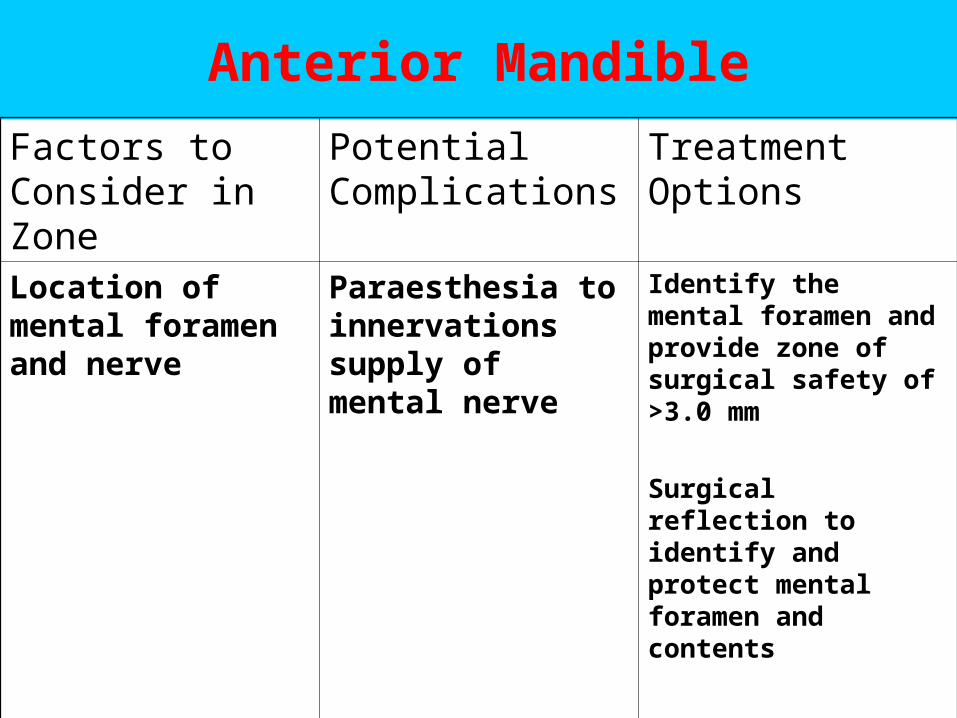
Anterior Mandible
Factors to Consider in Zone
Potential Complications
Treatment Options
Location of mental foramen and nerve
Paraesthesia to innervations supply of mental nerve
Identify the mental foramen and provide zone of surgical safety of >3.0 mm
Surgical reflection to identify and protect mental foramen and contents
Surgical Parameter by REGIONS
Posterior Maxilla
Surgical Parameter by REGIONSPosterior Maxilla
D3-D4 bone density:
1) Problem: Violation of Maxillary Sinus
Solution: Determine need for sinus augmentations prior to implant placement.
Need minimal of 5.0 mm of autogenous recipient bone for simultaneous implant placement with sinus graft.
Posterior Maxilla
Factors to Consider in Zone
Potential Complications
Treatment Options
Compromised height due to violation of maxillary sinus
Radiographs, CT scans to determine treatment plan to manage lack of height
Sinus augmentations
Angulated implants
Short implants
No Treatment and utilize “shorten dental arch concept”
Surgical Parameter by REGIONSPosterior Maxilla
• 2) Problem: Bone density with least implant contact (50%).
Solution: Use a bone condensing (osteotomes) rather than bone removing
(osteotomies) technique for implant site preparations.
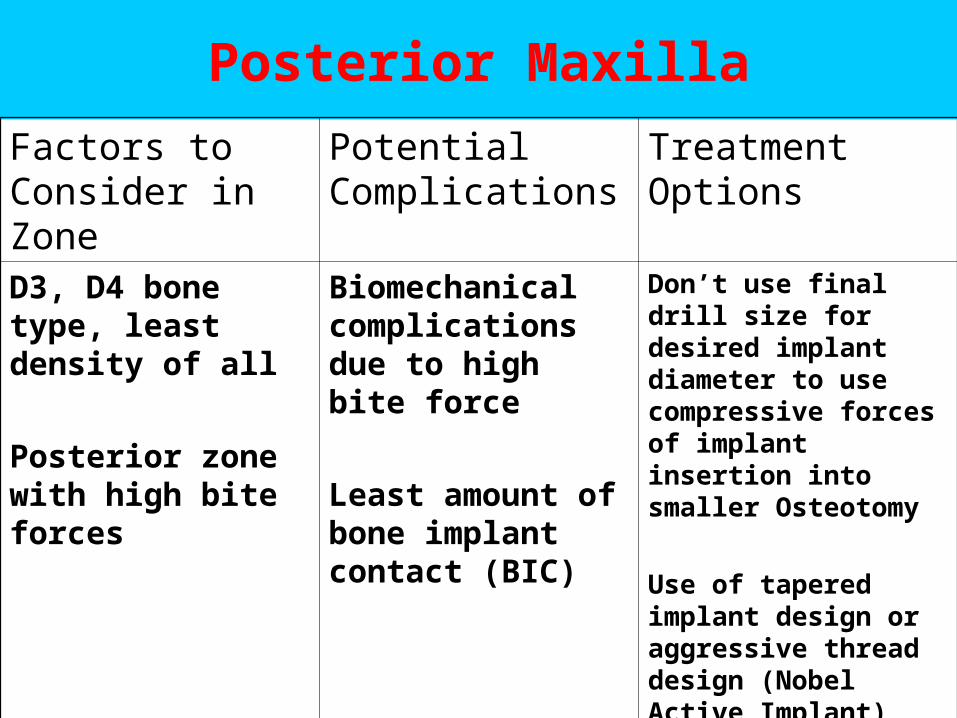
Posterior Maxilla
Factors to Consider in Zone
Potential Complications
Treatment Options
D3, D4 bone type, least density of all
Posterior zone with high bite forces
Biomechanical complications due to high bite force
Least amount of bone implant contact (BIC)
Don’t use final drill size for desired implant diameter to use compressive forces of implant insertion into smaller Osteotomy
Use of tapered implant design or aggressive thread design (Nobel Active Implant)
Extend healing periods
Implant Prosthetic Implant Prosthetic concepts concepts
Implant Prosthetic Concepts
1) Minimize ( < 3 units )Minimize ( < 3 units ) number of pontics.
2) No Cantilevers (especially distal)
3) No Connection to natural teeth.
4) Splinting of implant crowns.
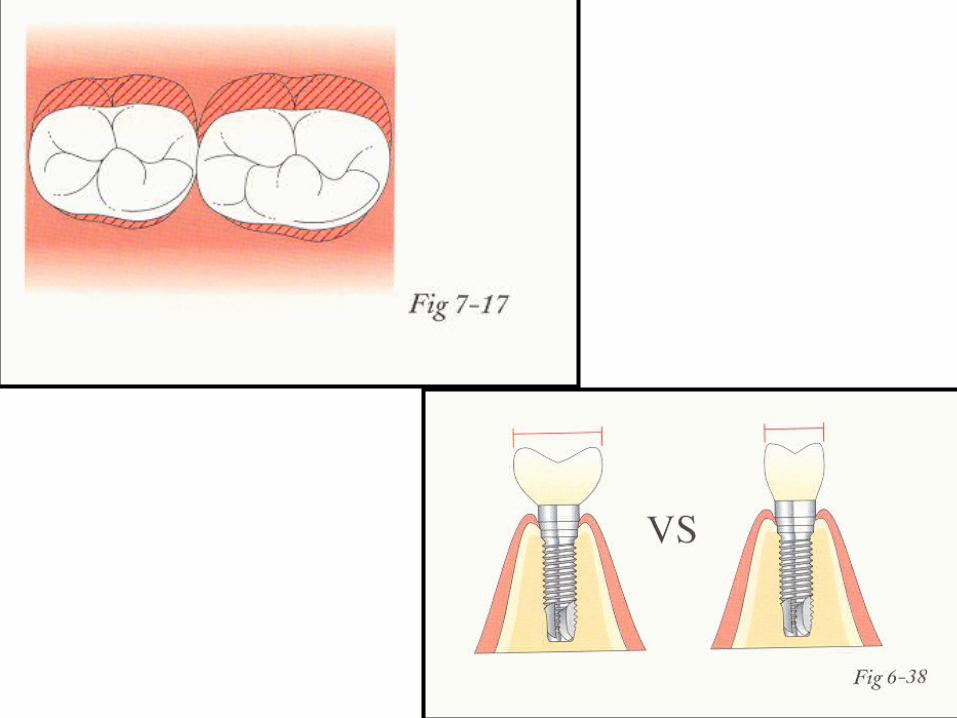
5) Minimize facial / lingual occlusal table.
6) Implant protected occlusal scheme.
7) Progressive bone loading concept on softer bone.
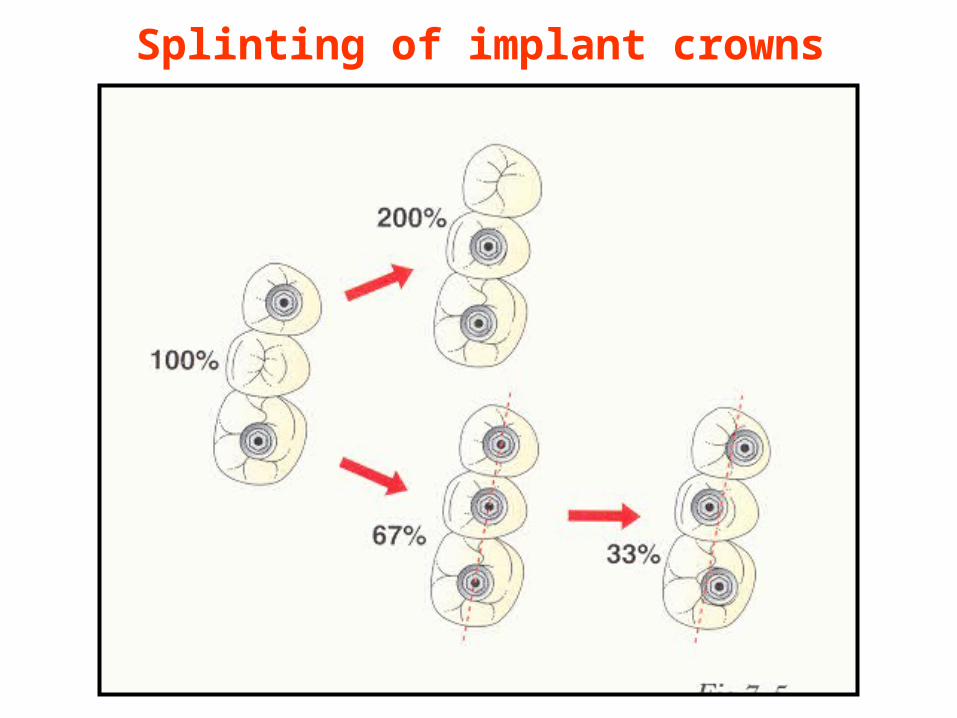
Splinting of implant crowns
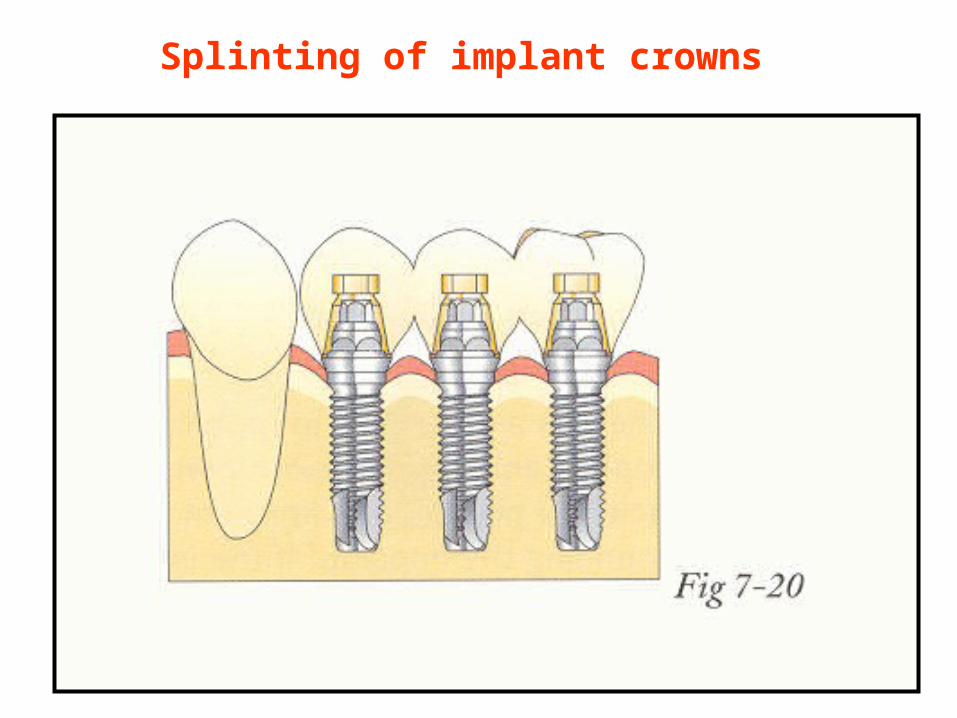
Splinting of implant crowns
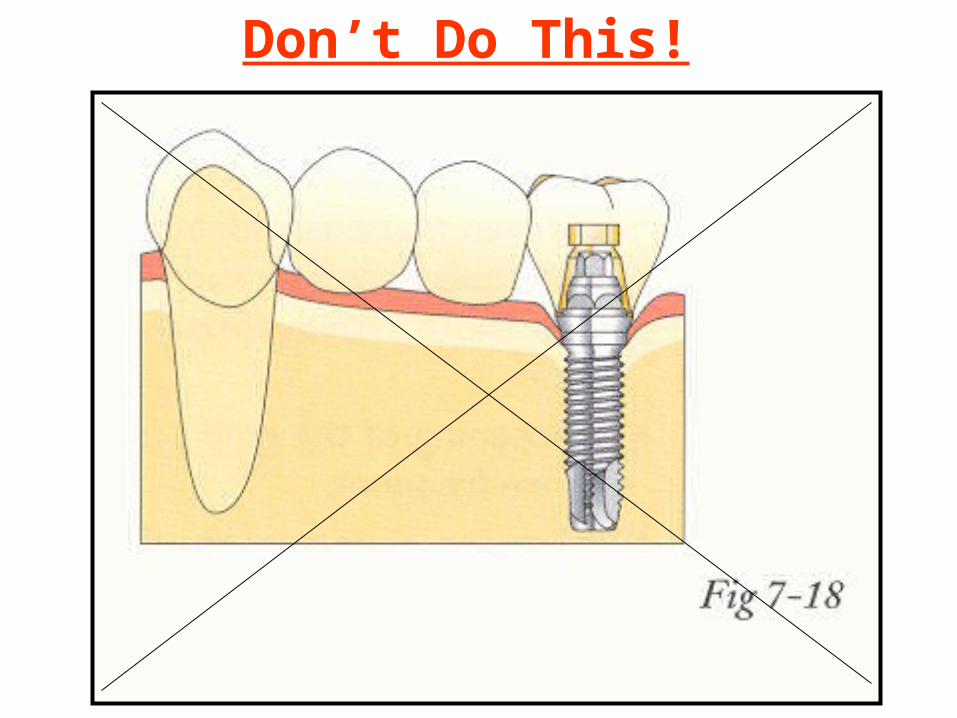
Don’t Do This!
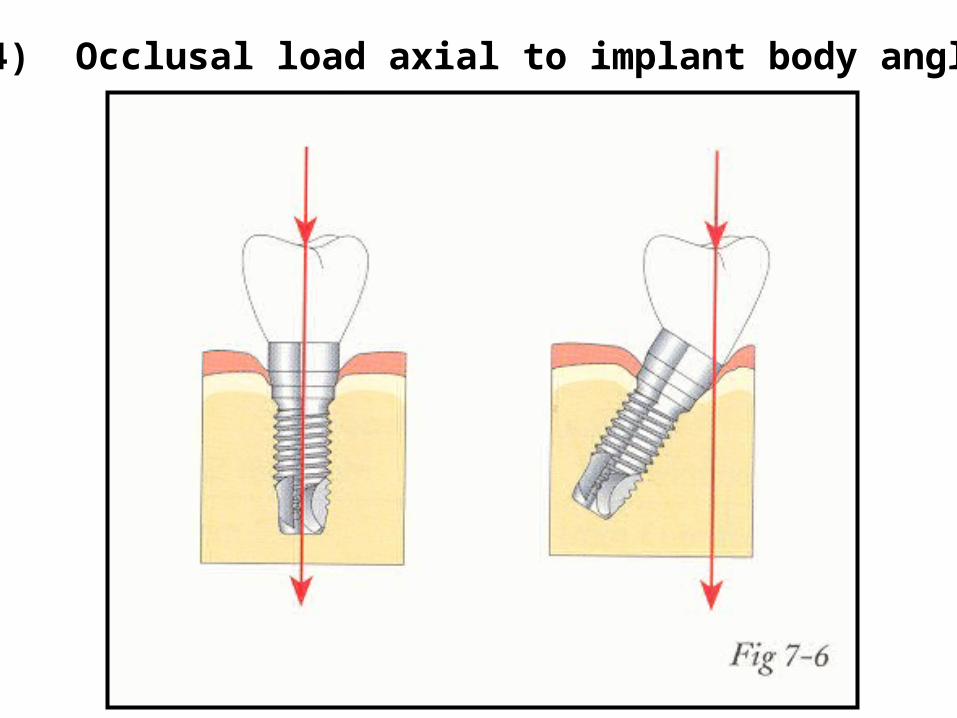
4) Occlusal load axial to implant body angle
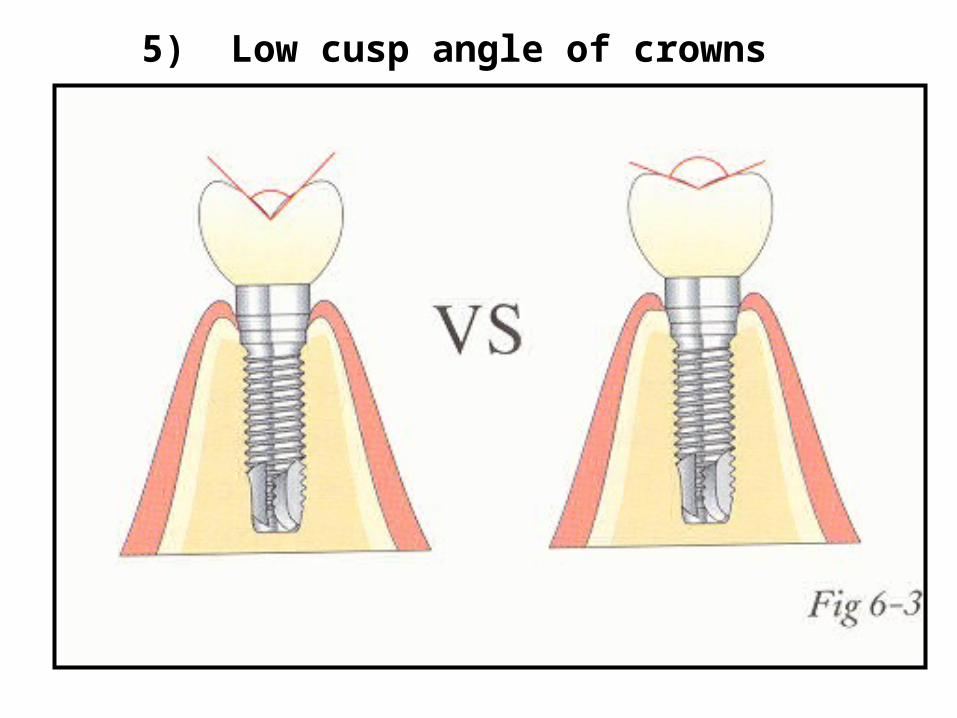
5) Low cusp angle of crowns
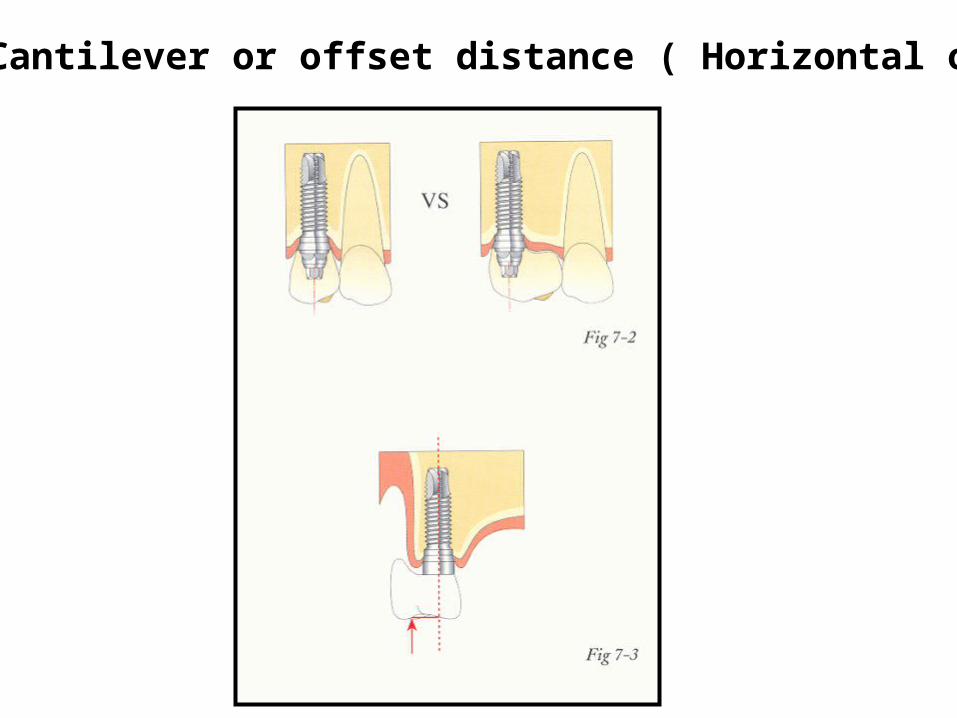
7) Cantilever or offset distance ( Horizontal offset)
Indications For Open Tray Impression Technique
1) Require adequate access for prosthetic open tray impression copings. (Anterior regions of mouth.)
2) Multiple units to register accurate relationship by indexing of impression copings.
3) Allow impressions with Divergent angulated dental implants.
4) Usually require custom impression trays or altered disposable trays.
5) Must verify seating with radiograph
6) Consider indexing with resin pattern
Indications for Closed Tray Impression Technique
1) Require minimal access for prosthetic closed tray impression copings. (Posterior regions mouth.)
2) Single or quadrant units.
3) Allow impressions with Parallel alignment of dental implants.
4) Usually require stock impression trays or disposable trays.
5) Must verify seating with radiograph.
6) Plug screw hole to avoid positive impression registration
Implant Protected Occlusion• 1) No premature occlusal contacts or interferences.
Timing of occlusal contacts protected by natural dentition.
• 2) Influence of surface area• 3) Mutually protected articulation (No lateral excursion)• 4) Occlusal load axial to implant body angle • 5) Low cusp angle of crowns• 6) Crown Height (vertical offset)• 7) Cantilever or offset distance ( Horizontal offset)• 8) Implant crown contour (narrow B /L dimensions)• 9) Selection of occlusal materials• 10) Verify implant supported prosthesis have lightened
occlusion where shim stock (12 um) pulls through in C.O. or M.I.P.
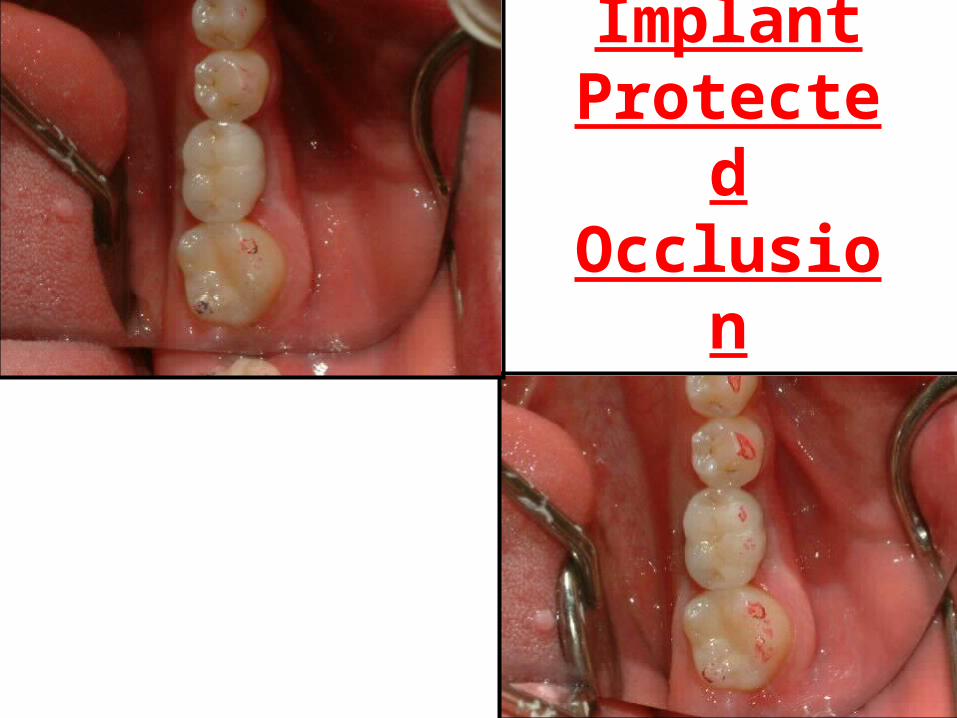
Implant Protected Occlusion
The Maintenance Requirement1) Post insertion 1 week later- verification of soft
tissue health and implant protected occlusion
2) Post insertion follow up every 4 months for the first year after loading of prosthesis- verification of crestal bone changes with radiograph, soft tissue health and implant protected occlusion
3) Post insertion follow up every 6 months for the second year and beyond.
3) Prosthetic Parameters:3) Prosthetic Parameters:
Biomechanical rationaleBiomechanical rationaleImplant Prosthetic conceptsImplant Prosthetic conceptsImplant provisionalization optionsImplant provisionalization optionsOpen versus Closed tray impressionOpen versus Closed tray impressionScrew versus cement retentionScrew versus cement retentionImplant protected occlusionImplant protected occlusionManagement protocol for parafunctional Management protocol for parafunctional habitshabitsManagement Options For Compromised
Interocclusal distance
Management protocols Management protocols specific for patients with specific for patients with
parafunctional habitsparafunctional habits
Force Factors
1) Magnitude (light, normal, heavy)
2) Duration (day time, night time)
3) Frequency (number / unit time)
4) Direction (vector of forces)
5) Type (compression, tensile, shear)
6) Magnifiers (height, cantilevers, parafunctional habits)
6) Combination
Strategies To Manage Parafunction Forces1) Educate patient of parafunctional habits.2) Placing increased number of implants.3) Placing larger diameter implants.4) Placing implants in positions to reduce bending overload
or positions to promote axial loading.5) Avoid use of cantilevers or pontics.6) Use bruxism night guard appliances.7) Increasing time intervals during prosthetic restoration
stages for progressive loading protocol.8) Paying diligent attention to occlusal contact design for
“Implant Protected Occlusion” and axial loading.9) Alter occlusal material of prosthetic teeth to be acrylic
resin for removable prosthesis and metal occlusal for fixed prosthesis.
Incidence Rate Of Mechanical Complications
1) OD loss of retention or adjustments 30%
2) Resin acrylic veneer facture of FPD 22%
3) OD relines required 19%
4) OD clip / attachment fractures 17%
5) Prosthesis screw loosening 7%
6) Abutment screw loosening 6%
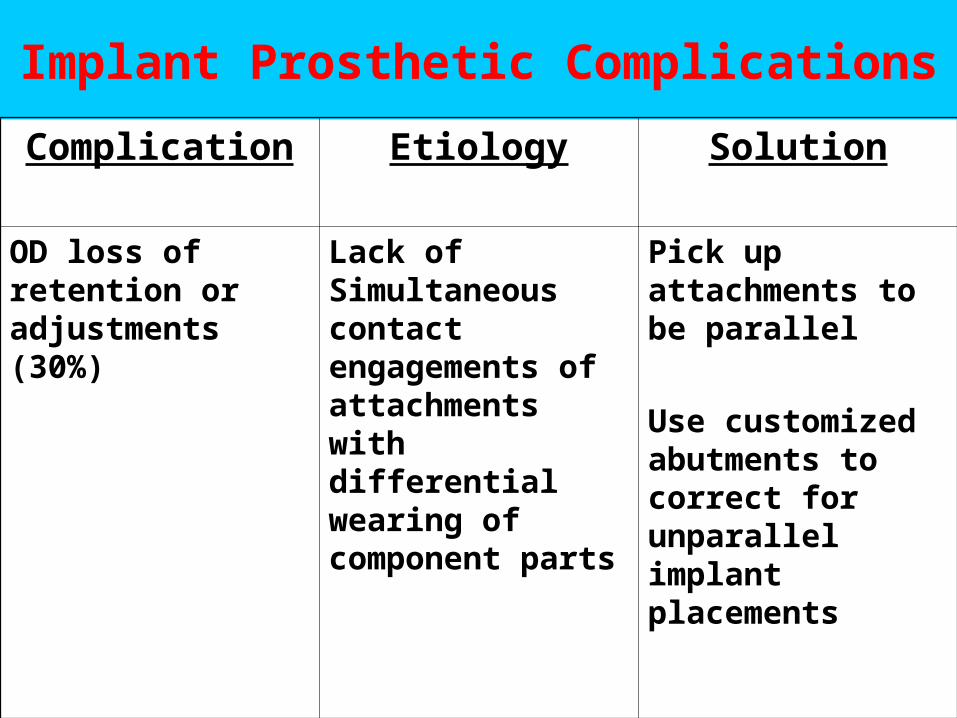
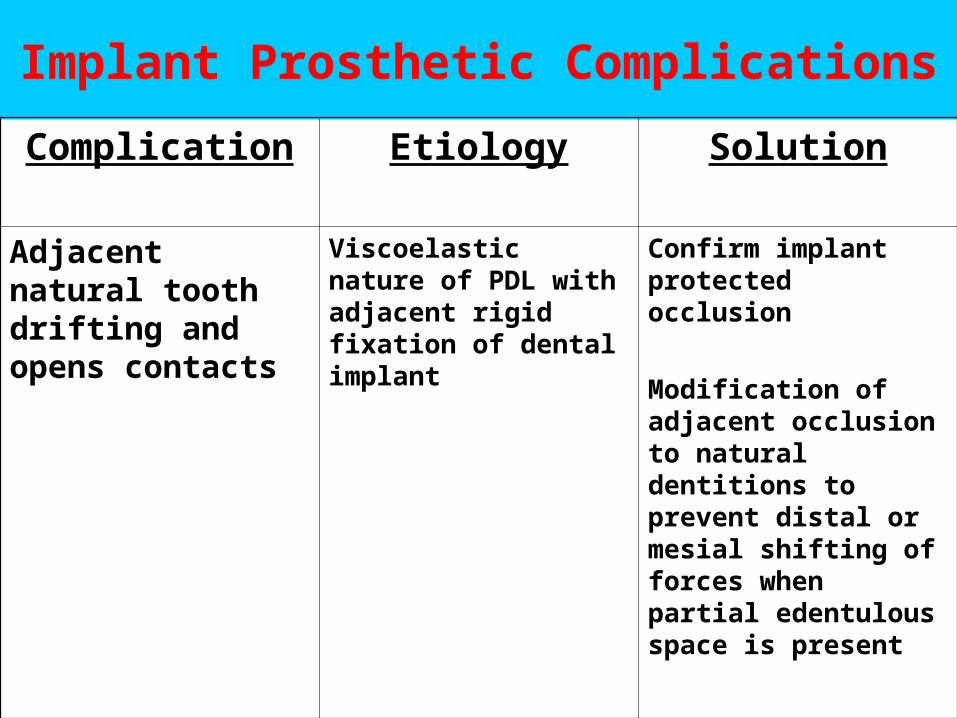
Implant Prosthetic Complications
Complication Etiology Solution
OD loss of retention or adjustments (30%)
Lack of Simultaneous contact engagements of attachments with differential wearing of component parts
Pick up attachments to be parallel
Use customized abutments to correct for unparallel implant placements
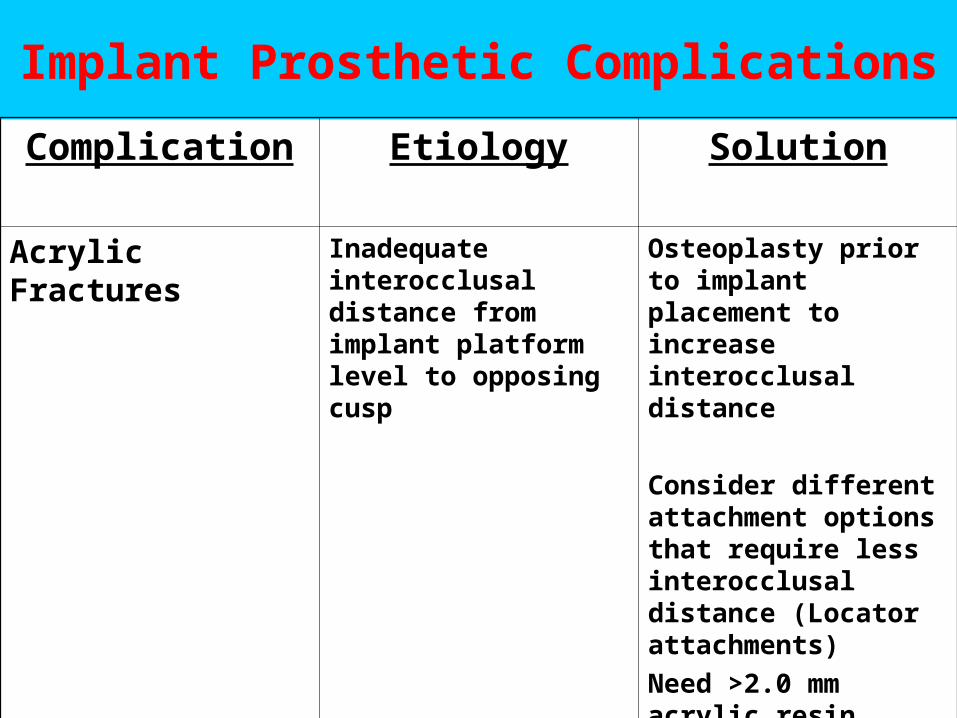
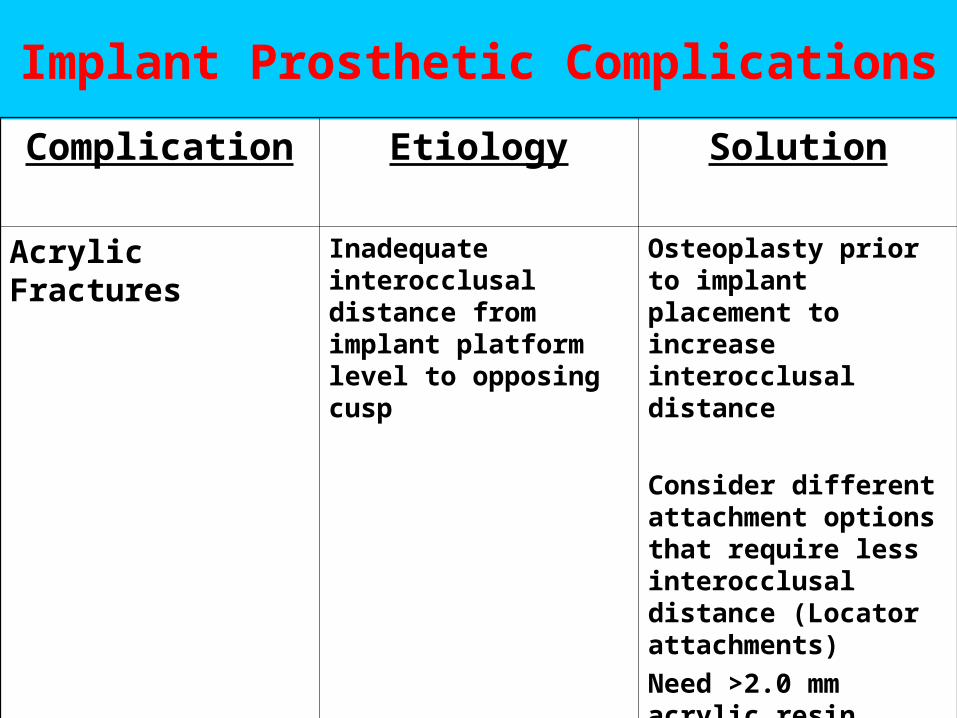
Implant Prosthetic Complications
Complication Etiology Solution
Acrylic Fractures Inadequate interocclusal distance from implant platform level to opposing cusp
Osteoplasty prior to implant placement to increase interocclusal distance
Consider different attachment options that require less interocclusal distance (Locator attachments)
Need >2.0 mm acrylic resin thickness over attachments for strength
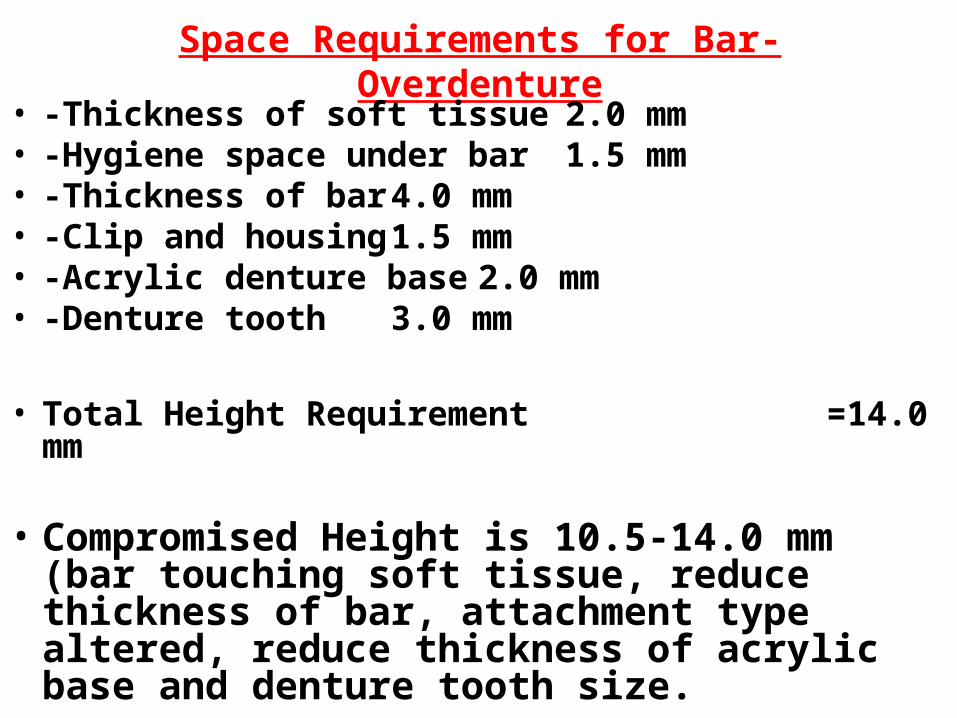
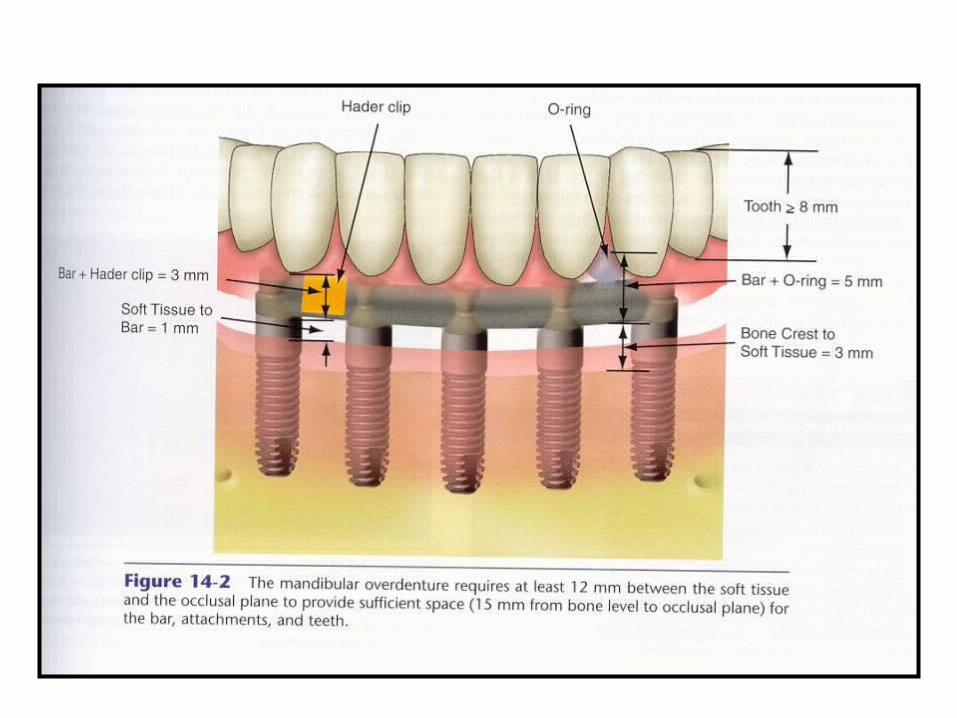
Space Requirements for Bar-Overdenture• -Thickness of soft tissue 2.0 mm• -Hygiene space under bar 1.5 mm• -Thickness of bar 4.0 mm• -Clip and housing 1.5 mm• -Acrylic denture base 2.0 mm• -Denture tooth 3.0 mm
• Total Height Requirement =14.0 mm
• Compromised Height is 10.5-14.0 mm (bar touching soft tissue, reduce thickness of bar, attachment type altered, reduce thickness of acrylic base and denture tooth size.
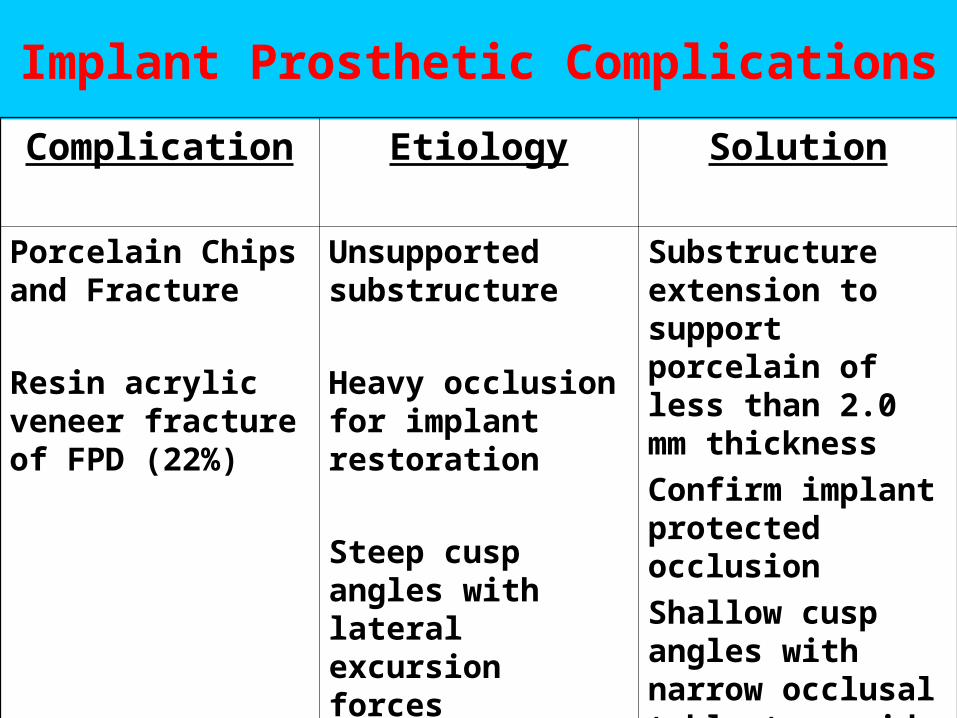
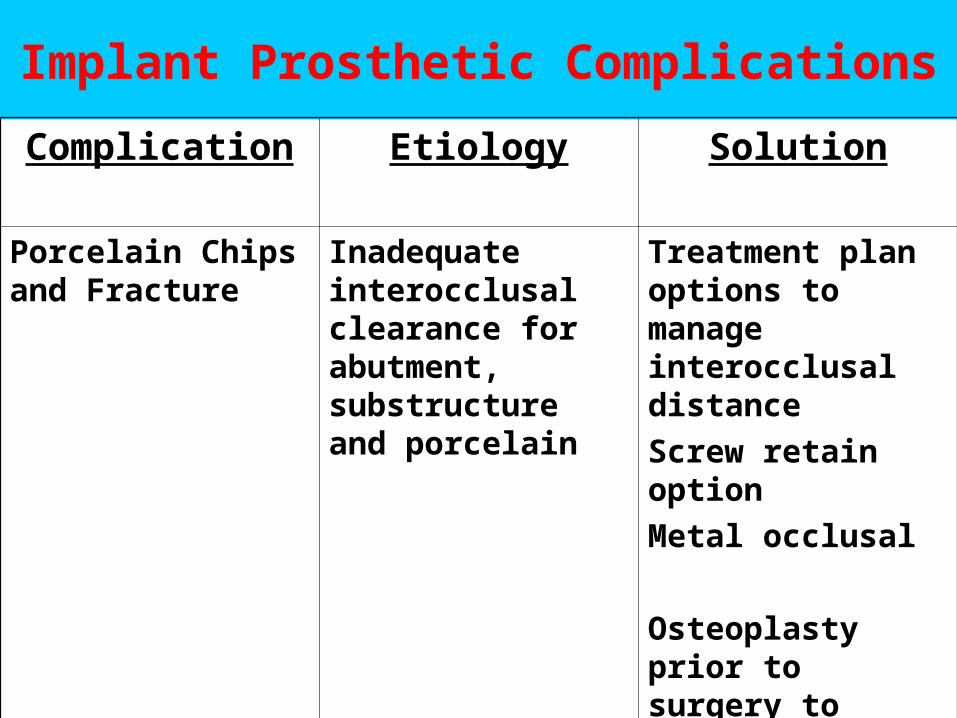
Implant Prosthetic Complications
Complication Etiology Solution
Porcelain Chips and Fracture
Resin acrylic veneer fracture of FPD (22%)
Unsupported substructure
Heavy occlusion for implant restoration
Steep cusp angles with lateral excursion forces
Substructure extension to support porcelain of less than 2.0 mm thickness
Confirm implant protected occlusion
Shallow cusp angles with narrow occlusal table to avoid lateral forces
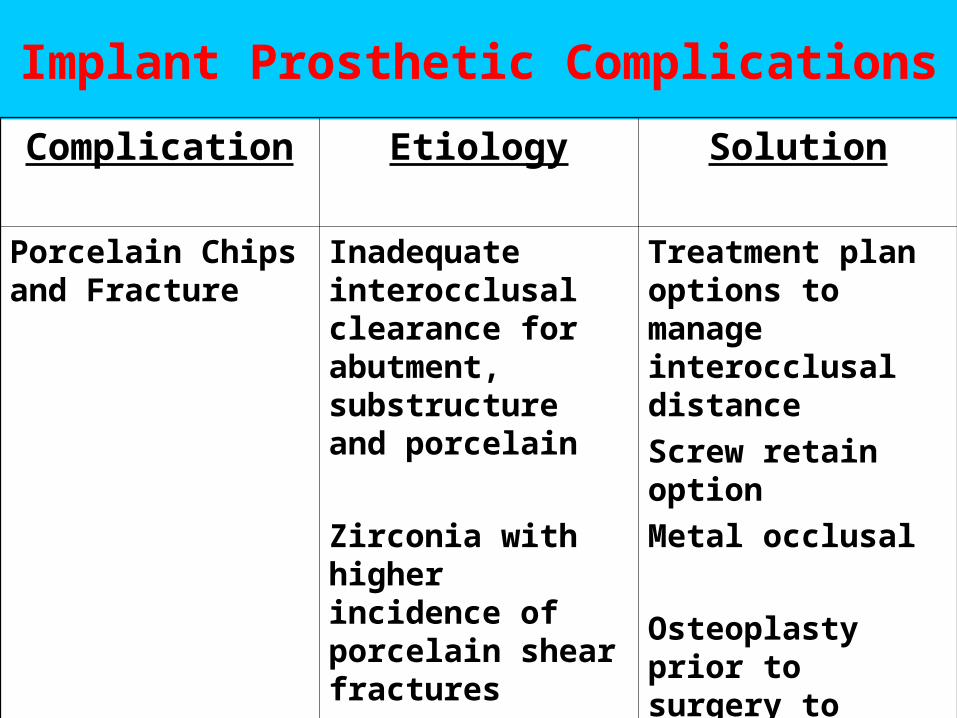
Implant Prosthetic Complications
Complication Etiology Solution
Porcelain Chips and Fracture
Inadequate interocclusal clearance for abutment, substructure and porcelain
Zirconia with higher incidence of porcelain shear fractures
Treatment plan options to manage interocclusal distance
Screw retain option
Metal occlusal
Osteoplasty prior to surgery to submerge implant platform level
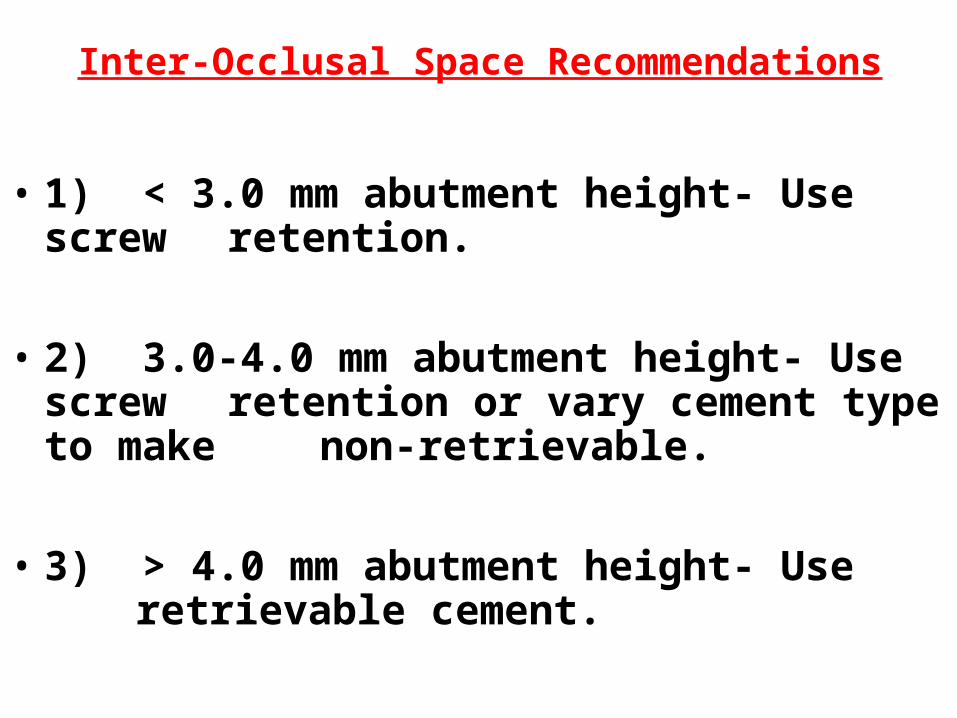
Inter-Occlusal Space Recommendations
• 1) < 3.0 mm abutment height- Use screw retention.
• 2) 3.0-4.0 mm abutment height- Use screw retention or vary cement type to make non-retrievable.
• 3) > 4.0 mm abutment height- Use retrievable cement.
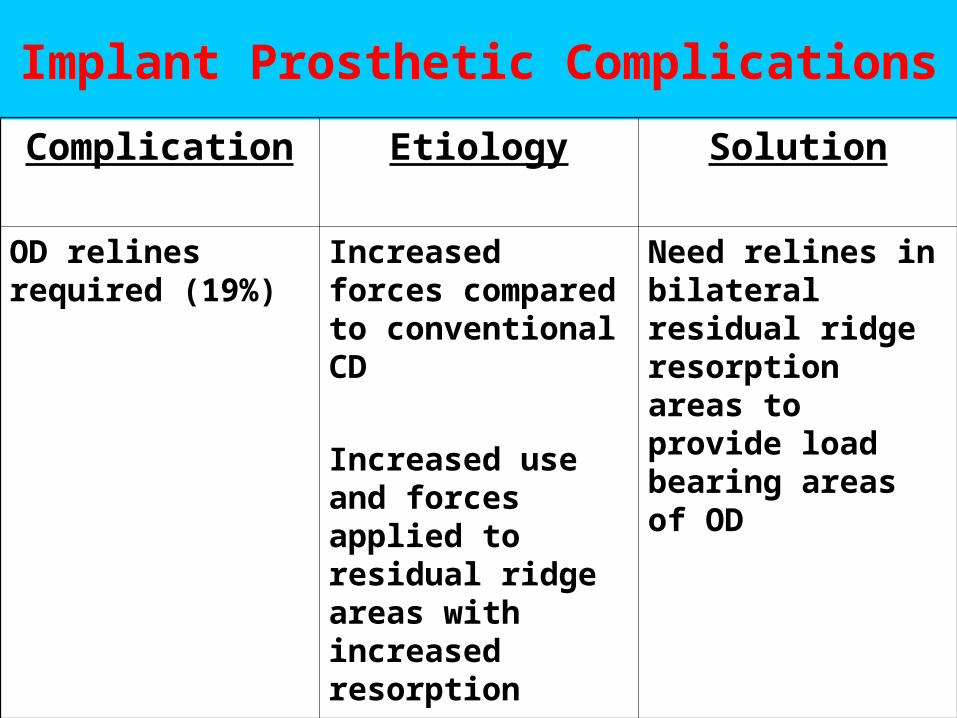
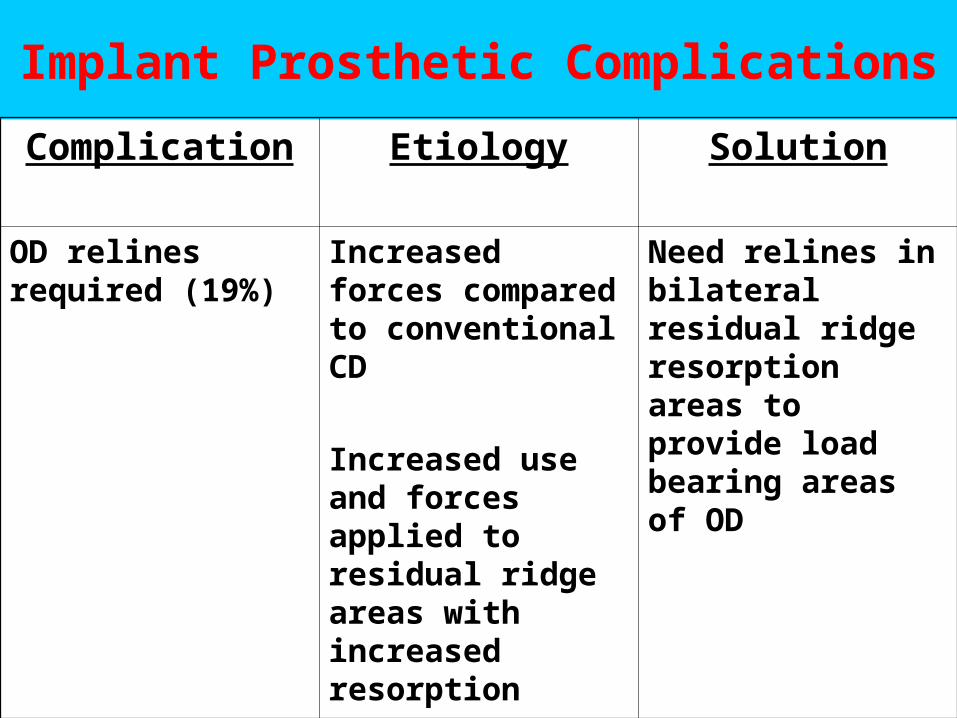
Implant Prosthetic Complications
Complication Etiology Solution
OD relines required (19%)
Increased forces compared to conventional CD
Increased use and forces applied to residual ridge areas with increased resorption
Need relines in bilateral residual ridge resorption areas to provide load bearing areas of OD

Incidence Rate Of Mechanical Complications
1) OD loss of retention or adjustments 30%
2) Resin acrylic veneer facture of FPD 22%
3) OD relines required 19%
4) OD clip / attachment fractures 17%
5) Prosthesis screw loosening 7%
6) Abutment screw loosening 6%

Implant Prosthetic Complications
Complication Etiology Solution
Attachment breakage or fractures
(17%)
Improper loading, angulated and/or imbalance of engagements of attachments
Differential wear of attachment parts
Soft tissue support adequate for loading bearing areas of OD
Inadequate interocclusal distance
Pick up attachments after correction of imbalance and obtain parallel alignment of attachments and achieve simultaneous contacts of components
Treatment plan properly
Change attachment types that require less interocclusal distance
Broken AttachmentsBroken Attachments
Plastic bar clipPlastic bar clip– damaged or brokendamaged or broken
• cut along long axis with sharp knife and cut along long axis with sharp knife and remove.remove.
– MissingMissing• replace by inserting a new clip into denture replace by inserting a new clip into denture
base receptaclebase receptacle• if unavailable, contact Command Implant if unavailable, contact Command Implant
CoordinatorCoordinator
Broken AttachmentsBroken Attachments
Metal bar clipMetal bar clip– damaged or broken (replacement clip available)damaged or broken (replacement clip available)
• remove the clip and perforate the denture base remove the clip and perforate the denture base carefully for intraoral pick up replacement.carefully for intraoral pick up replacement.
• Block out under the bar with wax, seat the denture Block out under the bar with wax, seat the denture and position a new clip through access in denture and position a new clip through access in denture base.base.
• Use autopolymerizing acrylic resin with “bead brush” Use autopolymerizing acrylic resin with “bead brush” technique to fill in access and connect clip to denture technique to fill in access and connect clip to denture base. Polish , disinfect and deliver.base. Polish , disinfect and deliver.
• Always confirm seating of denture after repair and Always confirm seating of denture after repair and evaluate occlusion.evaluate occlusion.
Broken AttachmentsBroken Attachments
• Metal bar clipMetal bar clip– Damaged or broken (replacement clip not available)Damaged or broken (replacement clip not available)
• remove all remnants of the clip from the denture base.remove all remnants of the clip from the denture base.
• block out under the bar with waxblock out under the bar with wax
• reline the clip area of the denture with a resilient chair side reline reline the clip area of the denture with a resilient chair side reline material (viscogel).material (viscogel).
– Intact clip with no retentionIntact clip with no retention• carefully bend the leaves of the clip toward the bar with a thin carefully bend the leaves of the clip toward the bar with a thin
instrument.instrument.
• Reseat the denture to confirm increased retention.Reseat the denture to confirm increased retention.
• Recheck occlusion.Recheck occlusion.
Broken AttachmentsBroken Attachments
• Stud attachmentsStud attachments– treatment is similar to clipstreatment is similar to clips
• tease out “O” ring with an explorer and replace as needed.tease out “O” ring with an explorer and replace as needed.
• Fractured housing can be treated like a clip replacement.Fractured housing can be treated like a clip replacement.
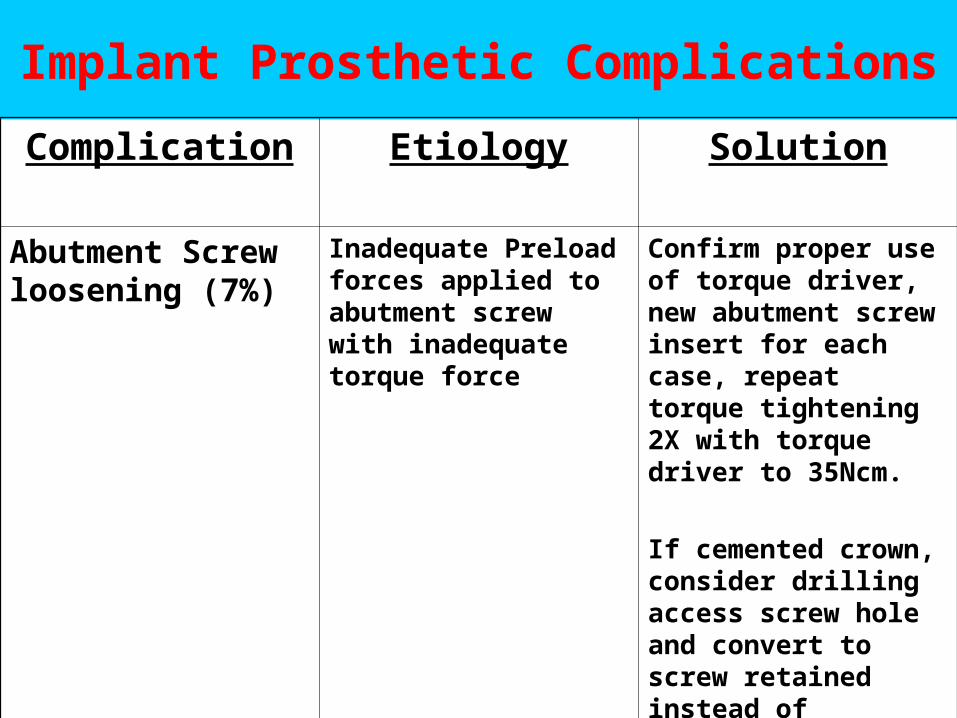
Implant Prosthetic Complications
Complication Etiology Solution
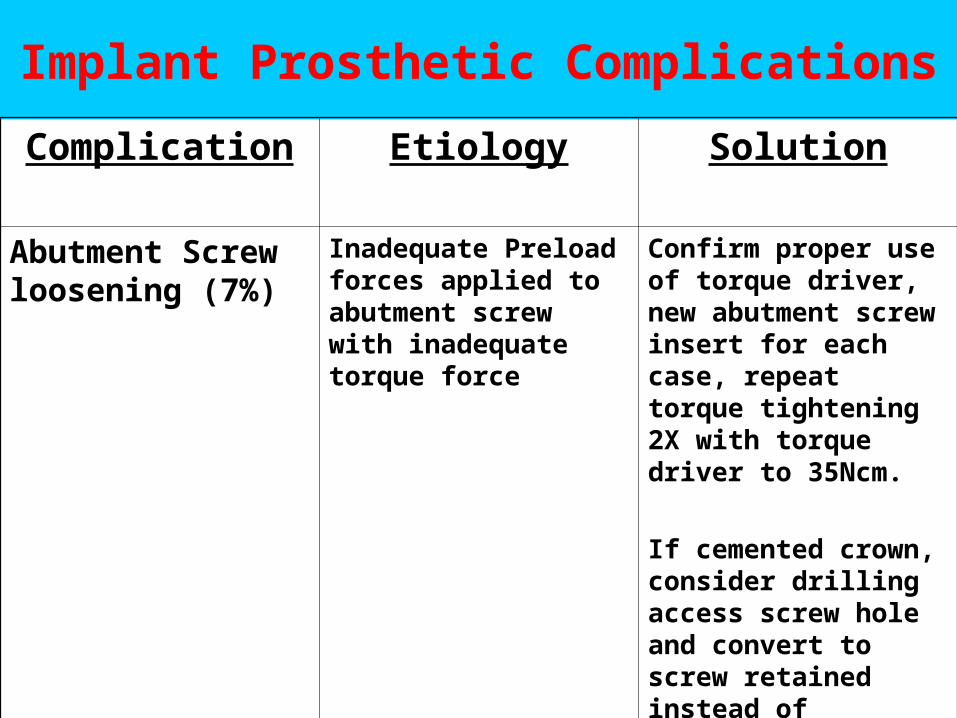
Abutment Screw loosening (7%)
Inadequate Preload forces applied to abutment screw with inadequate torque force
Confirm proper use of torque driver, new abutment screw insert for each case, repeat torque tightening 2X with torque driver to 35Ncm.
If cemented crown, consider drilling access screw hole and convert to screw retained instead of fabrication of new crown
Problems with Screw Loosening
1) Improper use of torque driver leading to inadequate “preload” force application
2) Stripped screw driver or screw head
3) Use of lab screws versus definitive screws
4) Material and surface used for fabrication of screws
5) Design of screws
6) Occlusal overload
7) Combination of any or all of the above
Implant Prosthetic Complications
Complication Etiology Solution
Adjacent natural tooth drifting and opens contacts
Viscoelastic nature of PDL with adjacent rigid fixation of dental implant
Confirm implant protected occlusion
Modification of adjacent occlusion to natural dentitions to prevent distal or mesial shifting of forces when partial edentulous space is present
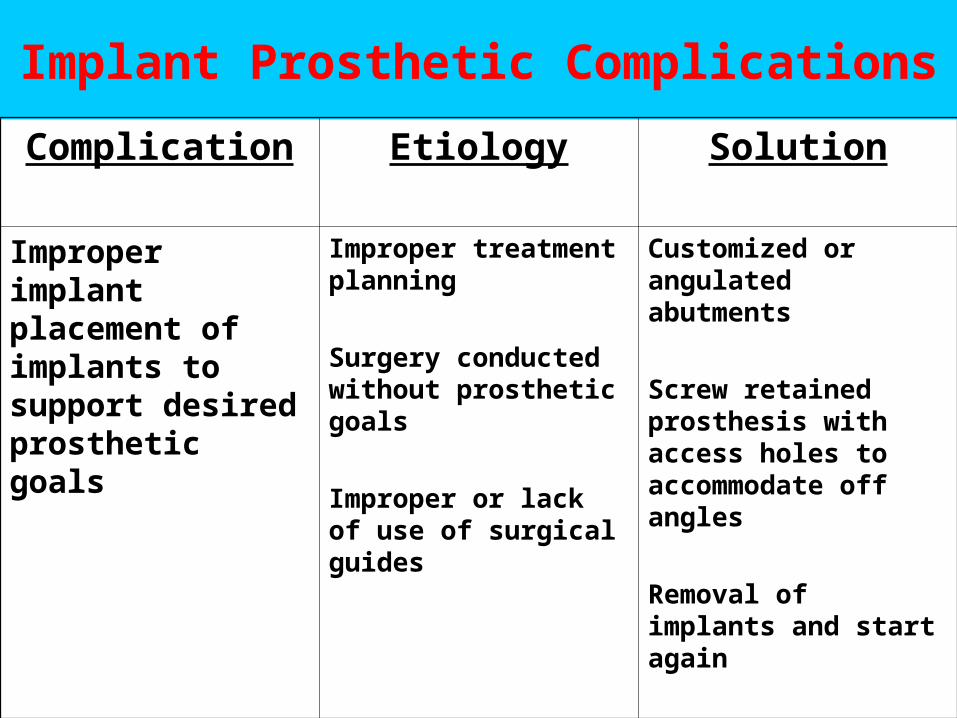
Implant Prosthetic Complications
Complication Etiology Solution
Improper implant placement of implants to support desired prosthetic goals
Improper treatment planning
Surgery conducted without prosthetic goals
Improper or lack of use of surgical guides
Customized or angulated abutments
Screw retained prosthesis with access holes to accommodate off angles
Removal of implants and start again
Treatment Options when presented with minimal Interocclusal Distance
1) Increase vertical dimension of occlusion for restorative convenience.
2) Extract teeth involved that violated the interocclusal distance and replace accordingly.
3) Orthodontic intrusion of opposing teeth involved.
4) Coronoplasty, crown preparations, prophylactic endodontic therapy, periodontal crown lengthening options to restore teeth involved.
Treatment Options when presented with minimal Interocclusal Distance
5) Prior to surgical placement of implants, perform alveoloplasty of residual ridge to increase interocclusal distance.
6) Prosthetic design: screw retain as opposed to cement retain to implant level.
7) Restorative material: metal occlusal as opposed to porcelain fused to metal.
Lack of Inter Occlusal Clearance: Treatment Options
• 1) Coronal adjustment of opposing arch or prophylactic endodontic therapy, crown lengthening and crowns to opposing arch.
• 2) Alveloplasty prior to implant placement with deeper surgical implant placement.
• 3) Prosthetically compensate with screw retained and metal occlusal to decrease required restorative clearance.
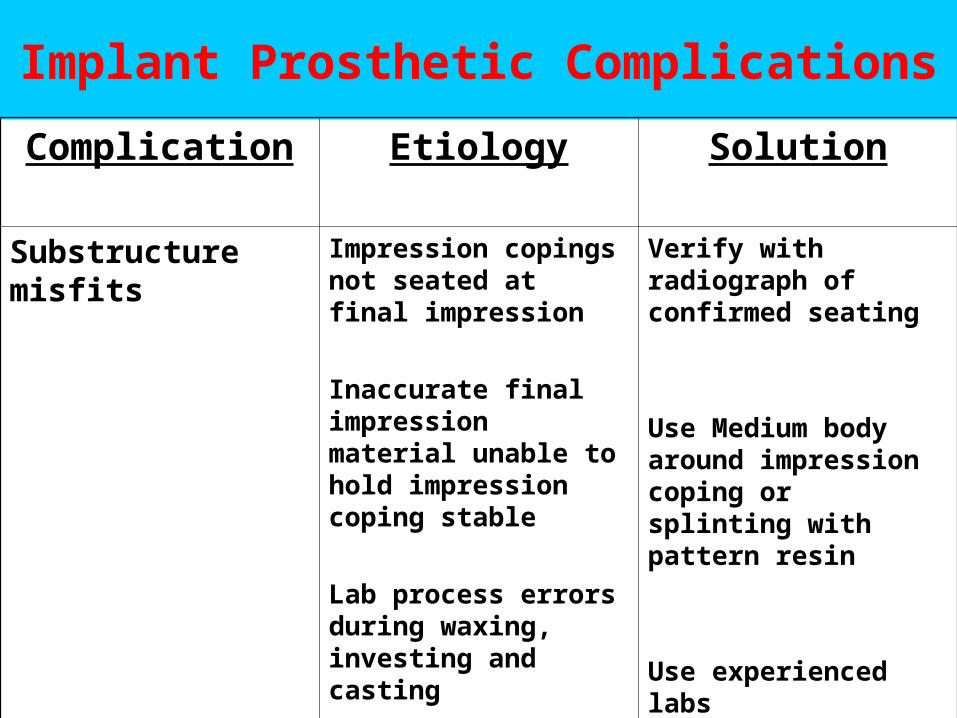
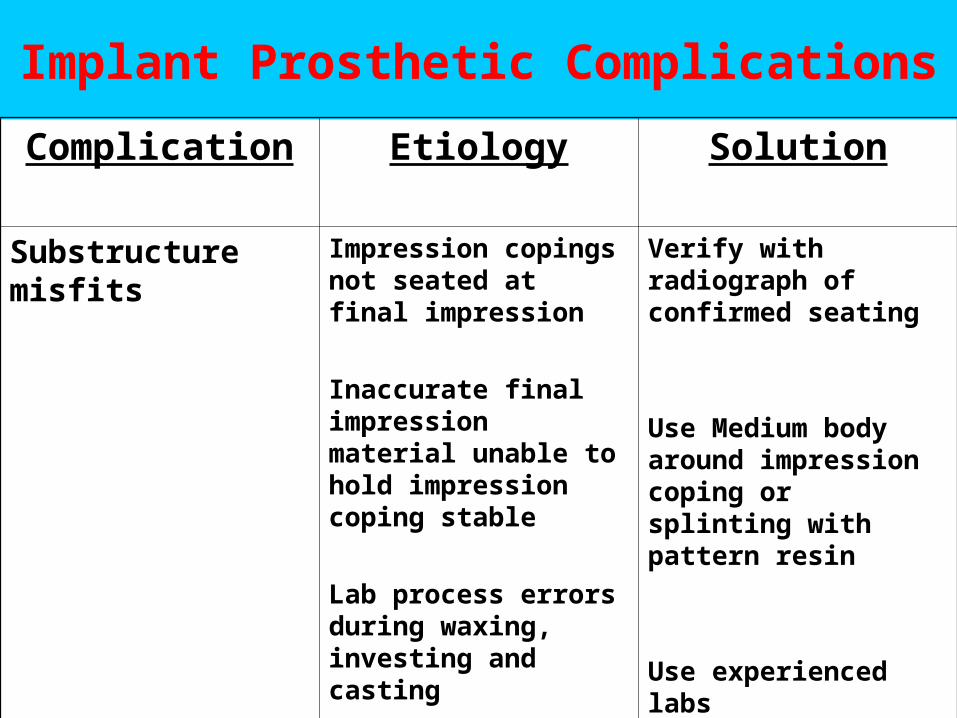
Implant Prosthetic Complications
Complication Etiology Solution
Substructure misfits
Impression copings not seated at final impression
Inaccurate final impression material unable to hold impression coping stable
Lab process errors during waxing, investing and casting
Verify with radiograph of confirmed seating
Use Medium body around impression coping or splinting with pattern resin
Use experienced labs

Iatrogenic / Prosthetic
Need for Provisional Restorations:– Positional stability– Occlusal function– Easily cleaned and maintenance of oral
hygiene– Nonimpinging soft tissues– Strength and retention– Esthetics
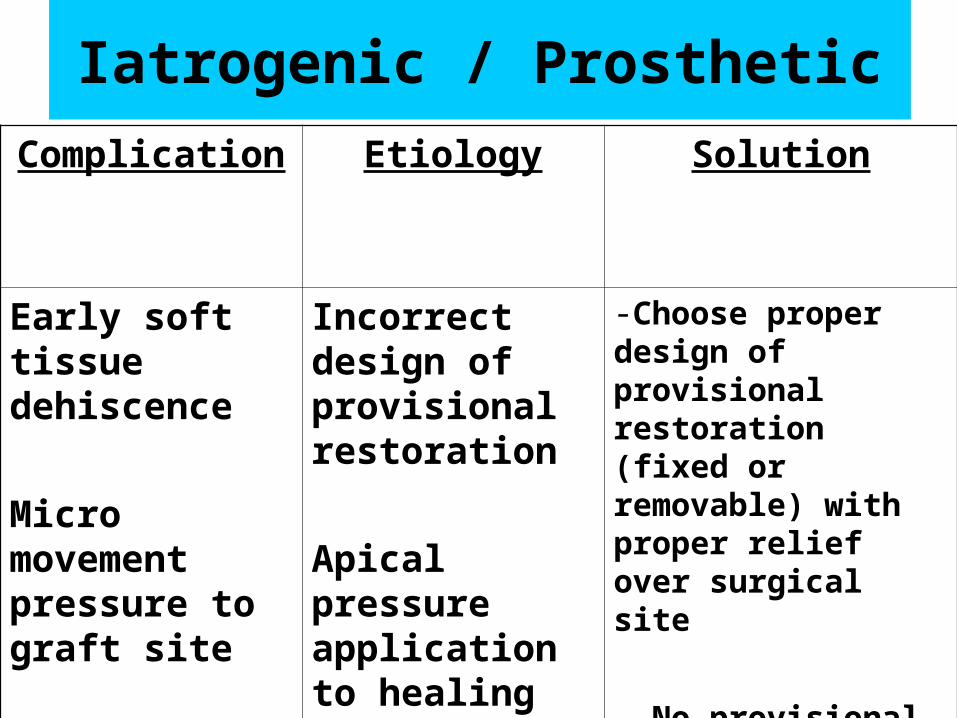
Iatrogenic / Prosthetic
Complication Etiology Solution
Early soft tissue dehiscence
Micro movement pressure to graft site
Incorrect design of provisional restoration
Apical pressure application to healing site
-Choose proper design of provisional restoration (fixed or removable) with proper relief over surgical site
- No provisional restoration
Removable Provisional1) Acrylic RPD (flipper)
a) Need proper design for occlusal stops.
b) Adequate relief under pontic site or above grafted site upon occlusal pressure.
c) Permanent soft tissue reline material as occlusal force buffer.
Removable Provisional
2) Essix appliance (Acrylic removable overlay prosthesis)
a) Need proper design for occlusal stops.
b) Adequate relief under pontic site or above grafted site upon occlusal pressure.
c) Permanent soft tissue reline material as occlusal force buffer.
Removable Provisional
3) Hawley orthodontic retainer appliance:
a) Need proper design of occlusal stops.
b) Adequate relief under pontic site or above grafted site upon occlusal pressure.
c) Permanent soft tissue reline material as occlusal force buffer.
Consequences of Peri-Implantitis
• 1) May lead to eventual implant loss.
• 2) Soft tissue exudates, abscess or infection localized to peri-implant locations.
• 3) Guarded prognosis and continuous soft tissue maintenance requirement for peri- implant soft tissues.
• 4) Possible source of irritation and discomfort to patient.
Possible Etiologies of Peri-Implantitis
• 1) Location of Microgap
• 2) Implant Thread Design
• 3) Surgical Trauma
• 4) Quality of bone
• 5) Occlusal Forces
• 6) Bacterial contamination
• 7) Biologic width consideration
• 8) Cement trap contamination
• 9) Combination of any / or all of above
Peri-Implantitis-Definitions• Defined as an inflammatory process
affecting the tissues around an osseointegrated implant in function, resulting in loss of supporting bone.
(Albrektsson & Isidor 1994)
• Plaque-induced progressive marginal bone loss observed on radiographs with clinical signs of infection of the peri-implant soft tissues.
(Cochrane Database of Systematic Reviews 2006)

Peri-implant Mucositis-Definitions
• Defined as reversible inflammatory changes of the peri-implant soft tissues without any bone loss.
(Albrektsson & Isidor 1994)
Prevalence Rates
• Peri-implant Mucositis: 8-44%
• Peri-Implantitis: 1-19%
Cement retainedCement retained1) Ideal aesthetics.2) Questionable retrievability.3) Retention require conventional fixed
prosthodontic principles of CHS of >7.0 mm.4) Ideal Implant placement to support prosthesis
with use of straight or angulated abutments.5) Ideal Occlusion or support over axially loaded
ceramics.6) Less requirements for passivity or lab costs.7) Removal of cement subgingival may be
compromised.8) Depth of implant level placement should allow
ease of cement clean up.
Cement Problems
• Subgingival cement left after cementation acting as a foreign body reaction causing pathologic bony and soft tissue reactions.
Dr. Mark Lin’s Cementation Technique
1) Paint and coat OUTSIDE crown margins with Vaseline. Confirm lab provided 2 layers of die spacers on implant abutment or scanning of abutments.
2) Light coat of cement of choice into implant crown restoration.
3) Pump restoration “Up and Down” motion to release hydraulic pressure build in to allow thinning of cement layer.
4) Removal after setting with curettes and floss.5) Soft tissue release may be required to confirm
total removal of excess cement.6) Verification of seating of abutment and crown to
implant platform level and cement removal.
Screw retainedScrew retained• 1) Compromised aesthetics.• 2) Reliable retrievability. (Multiple or full mouth
reconstructions.)• 3) Retention achieved with minimal CHS of < 7.0 mm
using screw retention preload principles.• 4) Accommodate compromised Implant placement to
support prosthesis with use of custom or angulated abutments.
• 5) Compromised Occlusion or support over axially loaded compromised integrity ceramics.
• 6) More requirements for passivity or lab costs.• 7) No cement clean up considerations.• 8) Deep implant level placements.• 9) Transitional provisionals with multiple units.
Problems with Screw Loosening
1) Improper use of torque driver leading to inadequate “preload” force application
2) Stripped screw driver or screw head
3) Use of lab screws versus definitive screws
4) Material and surface used for fabrication of screws
5) Design of screws
6) Occlusal overload
7) Combination of any or all of the above
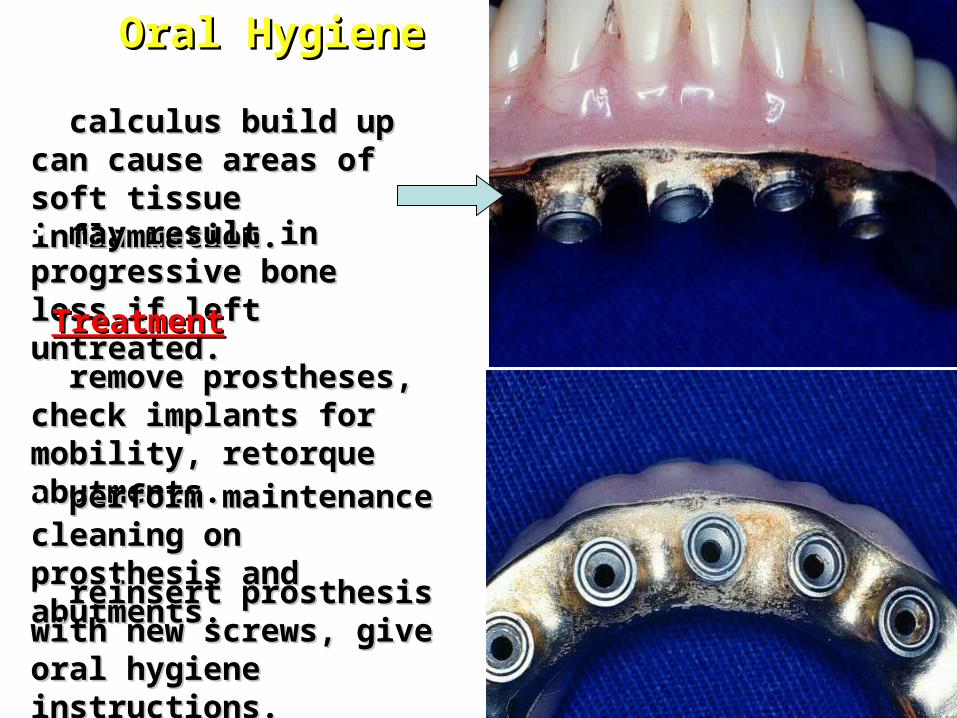
Oral HygieneOral Hygiene
• calculus build up can cause calculus build up can cause areas of soft tissue areas of soft tissue inflammation.inflammation.• may result in progressive may result in progressive bone loss if left untreated.bone loss if left untreated.
TreatmentTreatment
• remove prostheses, check remove prostheses, check implants for mobility, implants for mobility, retorque abutments.retorque abutments.• perform maintenance perform maintenance cleaning on prosthesis and cleaning on prosthesis and abutments.abutments.• reinsert prosthesis with new reinsert prosthesis with new screws, give oral hygiene screws, give oral hygiene instructions.instructions.
Maintenance and RecallMaintenance and Recall• AnnuallyAnnually
– periapical radiographs should be taken to monitor the crestal bone levels. (crestal bone periapical radiographs should be taken to monitor the crestal bone levels. (crestal bone can be at the level of the first thread in one year with 0.1mm continued loss to can be at the level of the first thread in one year with 0.1mm continued loss to approximately 1. 5 mm total bone loss)approximately 1. 5 mm total bone loss)
– remove and reinsert screw retained implant prostheses every 2 years unless indicated remove and reinsert screw retained implant prostheses every 2 years unless indicated otherwise.otherwise.
• Replace prosthesis with new retaining screws if removed.Replace prosthesis with new retaining screws if removed.
– Cemented restorations are usually permanent (nonretrievable).Cemented restorations are usually permanent (nonretrievable).– Recall focusRecall focus
• OcclusionOcclusion - verify there are no excursive contacts. Should not hold shimstock. Better to be out - verify there are no excursive contacts. Should not hold shimstock. Better to be out of occlusionof occlusion
• Oral hygieneOral hygiene - same requirements as for natural teeth. - same requirements as for natural teeth.• Soft tissue healthSoft tissue health - periodontal probing for evidence of disease. - periodontal probing for evidence of disease.• Screw joint torqueScrew joint torque - check for loosened screws (most common problem). - check for loosened screws (most common problem).• Integrity of attachmentsIntegrity of attachments - applies to overdenture / overpartials. - applies to overdenture / overpartials.• Stability of implantsStability of implants - must - must be stable (non mobile) to be successful be stable (non mobile) to be successful
Maintenance and RecallMaintenance and Recall• Screw retained prosthesisScrew retained prosthesis
– Remove prosthetic retention screwsRemove prosthetic retention screws• Screw access holes are usually sealed with a layer of cotton pellet, silicone plug Screw access holes are usually sealed with a layer of cotton pellet, silicone plug
or gutta percha the acrylic or composite resin.or gutta percha the acrylic or composite resin.• Expose the screw by drilling carefully through the resin.Expose the screw by drilling carefully through the resin.• Remove the screw (slot or hex) with the appropriate screw driver.Remove the screw (slot or hex) with the appropriate screw driver.• Throat drapes are highly recommended.Throat drapes are highly recommended.
– Check for implant mobility and retorque abutments to 20 Ncm. (hand tighten Check for implant mobility and retorque abutments to 20 Ncm. (hand tighten as much as possible with finger abutment driver if no torque control device as much as possible with finger abutment driver if no torque control device is available)is available)
– Clean and polish abutments (Do not remove)Clean and polish abutments (Do not remove)– Reseat restoration using new gold retaining screws.Reseat restoration using new gold retaining screws.
• Tighten screws as if doing nuts on the lugs of an automobile - place all screws Tighten screws as if doing nuts on the lugs of an automobile - place all screws back with minimal torque. Then work back and forth across the arch until all are back with minimal torque. Then work back and forth across the arch until all are tightened to 10 Ncm. (hand torque with appropriate hand screw driver if no tightened to 10 Ncm. (hand torque with appropriate hand screw driver if no torque controller is available)torque controller is available)
Maintenance and RecallMaintenance and Recall• Screw retained prosthesis (cont.)Screw retained prosthesis (cont.)
– Temporary reinsertionTemporary reinsertion• fill access holes with small cotton pellet and polyvinylsiloxane fill access holes with small cotton pellet and polyvinylsiloxane
impression material or putty.impression material or putty.
– Long-term reinsertionLong-term reinsertion• fill access hole with small cotton pellet over the head of the screw, fill access hole with small cotton pellet over the head of the screw,
followed by warm gutta percha and only 1-2 mm of acrylic or followed by warm gutta percha and only 1-2 mm of acrylic or composite resin.composite resin.
• Cemented restorationsCemented restorations– Single unitSingle unit
• usually nonretrievable and not removed for maintenance.usually nonretrievable and not removed for maintenance.
– Multiple unit (usually not indicated)Multiple unit (usually not indicated)• carefully tap off with crown remover, check for mobile implants and carefully tap off with crown remover, check for mobile implants and
retorque abutment screws.retorque abutment screws.• Replace restoration with provisional luting media, and recheck Replace restoration with provisional luting media, and recheck
occlusion.occlusion.
Hygiene AidsHygiene Aids
• Super - flossSuper - floss
• End tufted brushesEnd tufted brushes
• Proxy brushesProxy brushes
• Tarter control dentrificesTarter control dentrifices
• Mechanical instrumentsMechanical instruments
• PeridexPeridex
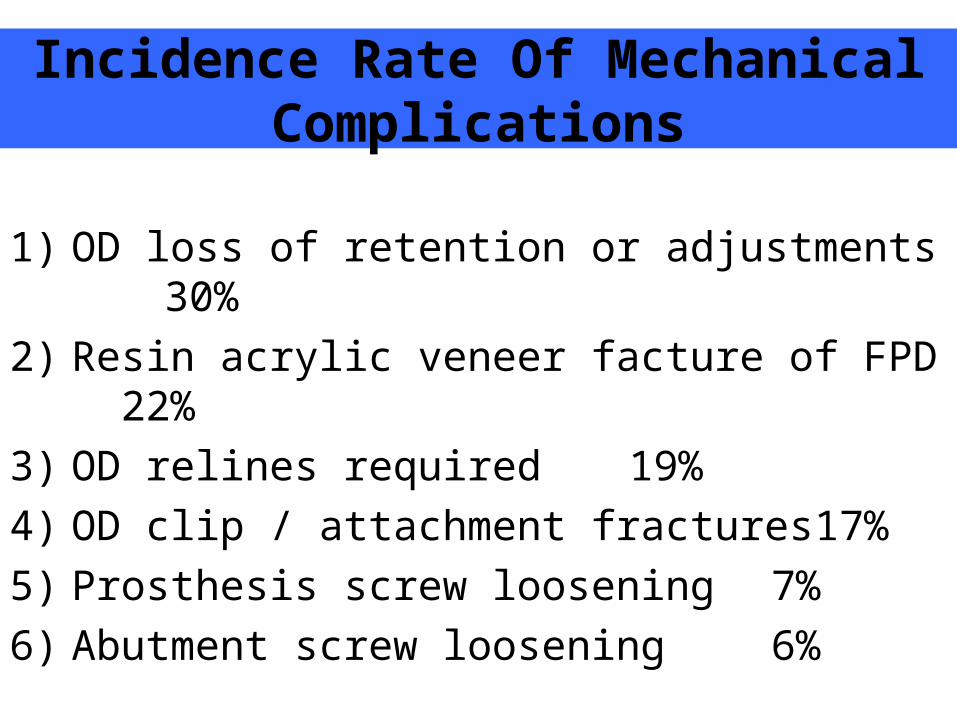
Incidence Rate Of Mechanical Complications
1) OD loss of retention or adjustments 30%
2) Resin acrylic veneer facture of FPD 22%
3) OD relines required 19%
4) OD clip / attachment fractures 17%
5) Prosthesis screw loosening 7%
6) Abutment screw loosening 6%
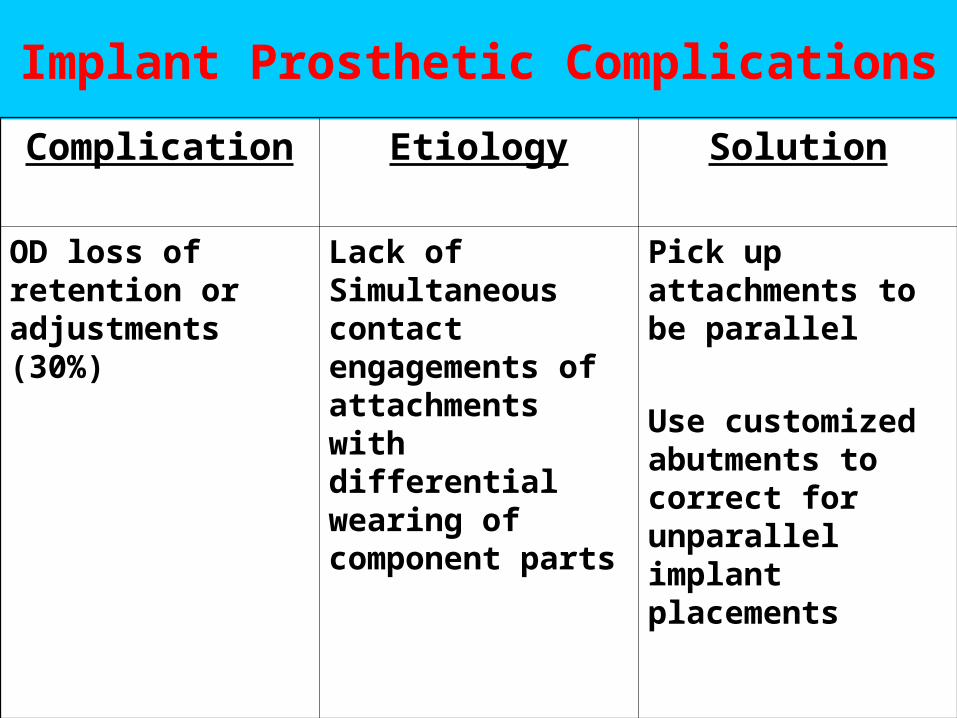
Implant Prosthetic Complications
Complication Etiology Solution
OD loss of retention or adjustments (30%)
Lack of Simultaneous contact engagements of attachments with differential wearing of component parts
Pick up attachments to be parallel
Use customized abutments to correct for unparallel implant placements
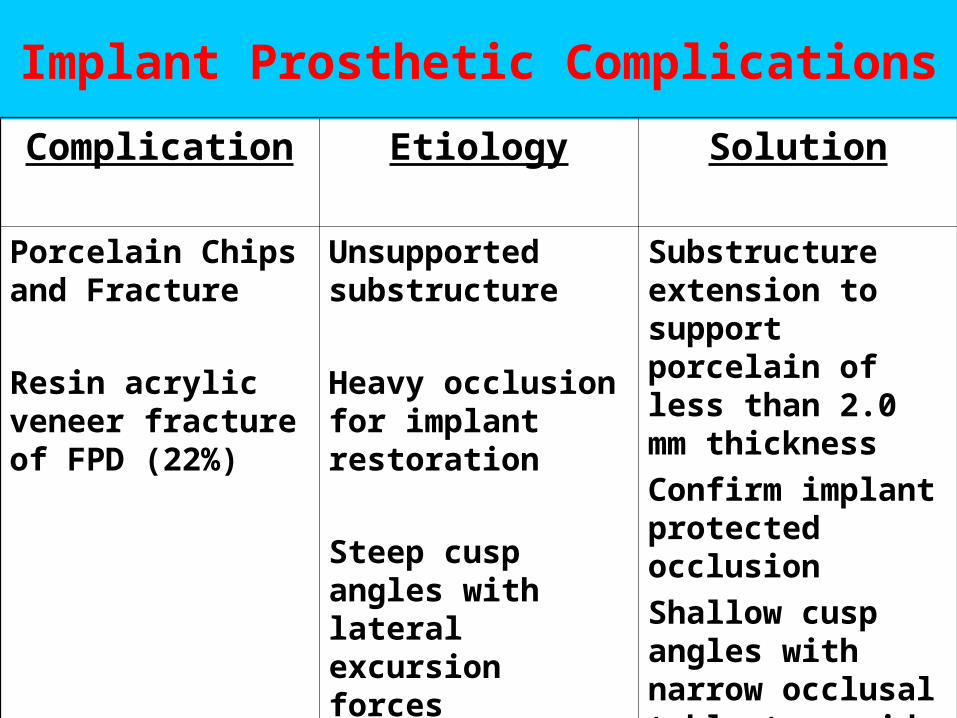
Implant Prosthetic Complications
Complication Etiology Solution
Porcelain Chips and Fracture
Resin acrylic veneer fracture of FPD (22%)
Unsupported substructure
Heavy occlusion for implant restoration
Steep cusp angles with lateral excursion forces
Substructure extension to support porcelain of less than 2.0 mm thickness
Confirm implant protected occlusion
Shallow cusp angles with narrow occlusal table to avoid lateral forces
Implant Prosthetic Complications
Complication Etiology Solution
Porcelain Chips and Fracture
Inadequate interocclusal clearance for abutment, substructure and porcelain
Treatment plan options to manage interocclusal distance
Screw retain option
Metal occlusal
Osteoplasty prior to surgery to submerge implant platform level
Implant Prosthetic Complications
Complication Etiology Solution
OD relines required (19%)
Increased forces compared to conventional CD
Increased use and forces applied to residual ridge areas with increased resorption
Need relines in bilateral residual ridge resorption areas to provide load bearing areas of OD
Implant Prosthetic Complications
Complication Etiology Solution
Abutment Screw loosening (7%)
Inadequate Preload forces applied to abutment screw with inadequate torque force
Confirm proper use of torque driver, new abutment screw insert for each case, repeat torque tightening 2X with torque driver to 35Ncm.
If cemented crown, consider drilling access screw hole and convert to screw retained instead of fabrication of new crown
Problems with Screw Loosening
1) Improper use of torque driver leading to inadequate “preload” force application
2) Stripped screw driver or screw head
3) Use of lab screws versus definitive screws
4) Material and surface used for fabrication of screws
5) Design of screws
6) Occlusal overload
7) Combination of any or all of the above
Implant Prosthetic Complications
Complication Etiology Solution
Adjacent natural tooth drifting and opens contacts
Viscoelastic nature of PDL with adjacent rigid fixation of dental implant
Confirm implant protected occlusion
Modification of adjacent occlusion to natural dentitions to prevent distal or mesial shifting of forces when partial edentulous space is present
Implant Prosthetic Complications
Complication Etiology Solution
Improper implant placement of implants to support desired prosthetic goals
Improper treatment planning
Surgery conducted without prosthetic goals
Improper or lack of use of surgical guides
Customized or angulated abutments
Screw retained prosthesis with access holes to accommodate off angles
Removal of implants and start again
Implant Prosthetic Complications
Complication Etiology Solution
Substructure misfits
Impression copings not seated at final impression
Inaccurate final impression material unable to hold impression coping stable
Lab process errors during waxing, investing and casting
Verify with radiograph of confirmed seating
Use Medium body around impression coping or splinting with pattern resin
Use experienced labs
Implant Prosthetic Complications
Complication Etiology Solution
Acrylic Fractures Inadequate interocclusal distance from implant platform level to opposing cusp
Osteoplasty prior to implant placement to increase interocclusal distance
Consider different attachment options that require less interocclusal distance (Locator attachments)
Need >2.0 mm acrylic resin thickness over attachments for strength
Problems in the fieldProblems in the field
• Fractured/loosened screwsFractured/loosened screws
• Fixture lossFixture loss
• Poor oral hygienePoor oral hygiene
• Soft tissue reactionsSoft tissue reactions
• Broken attachmentsBroken attachments
• Fractured componentsFractured components
Problems in the fieldProblems in the field
• Fractured/loosened screwsFractured/loosened screws
• Fixture lossFixture loss
• Poor oral hygienePoor oral hygiene
• Soft tissue reactionsSoft tissue reactions
• Broken attachmentsBroken attachments
• Fractured componentsFractured components
Fractured or loosened screwsFractured or loosened screws• Usually results in localized inflammation, loose restorations and Usually results in localized inflammation, loose restorations and
discomfort.discomfort.– First suspicion when patient complains of discomfort or loose implant.First suspicion when patient complains of discomfort or loose implant.
• Prosthetic gold retaining screws have either a slot or hex head.Prosthetic gold retaining screws have either a slot or hex head.• Abutment screws require a hex abutment driver, large slot, hex or Abutment screws require a hex abutment driver, large slot, hex or
square driver.square driver.– Standard and conical (estheticone) abutments have a raised hex and require Standard and conical (estheticone) abutments have a raised hex and require
a wrench that fits over this hex.a wrench that fits over this hex.– All other abutment screws have the slot, hex or square depression inside the All other abutment screws have the slot, hex or square depression inside the
screw head.screw head.
• Loose single tooth abutments are Loose single tooth abutments are true emergenciestrue emergencies. Continued . Continued rotation can risk rounding the corners of the hex on the implant, rotation can risk rounding the corners of the hex on the implant, causing a loss in anti-rotation.causing a loss in anti-rotation.
Fixture lossFixture loss((Must differentiate between “failing” and Must differentiate between “failing” and
“failed”)“failed”) • Failing ImplantFailing Implant– Clinical signs:Clinical signs:
• progressive bone lossprogressive bone loss
• soft tissue pocketing and crestal bone losssoft tissue pocketing and crestal bone loss
• bleeding on probing with possible purulencebleeding on probing with possible purulence
• tenderness to percussion or torque forcestenderness to percussion or torque forces
– Causes:Causes:• overheating of boneoverheating of bone at the time of surgery or lack of initial at the time of surgery or lack of initial
stability.stability.
• Nonpassive superstructuresNonpassive superstructures
• inadequate screw joint closureinadequate screw joint closure
• functional overloadfunctional overload
• periodontal infection (peri-implantitis)periodontal infection (peri-implantitis)
Fixture lossFixture loss• Failing ImplantFailing Implant
– Treatment:Treatment:• Interim: remove prosthesis and abutmentsInterim: remove prosthesis and abutments
– irrigate with Peridexirrigate with Peridex– ultrasonic and disinfect all componentsultrasonic and disinfect all components– reinsert assuring proper screw torquereinsert assuring proper screw torque– recheck passive fit of framework and occlusionrecheck passive fit of framework and occlusion
• Failed ImplantFailed Implant– Clinical signs:Clinical signs:
• MobilityMobility– verify fixture mobility by removing any abutments and superstructures first.verify fixture mobility by removing any abutments and superstructures first.
• A “Dull” percussion sound has been associated with a failed implantA “Dull” percussion sound has been associated with a failed implant• Peri-implant radiolucency can be a radiographic findingPeri-implant radiolucency can be a radiographic finding
– often this is not evident on an X-rayoften this is not evident on an X-ray
Fixture lossFixture loss
• Failed ImplantFailed Implant– CausesCauses
• surgical compromise (overheating bone and initial lack of surgical compromise (overheating bone and initial lack of stability).stability).
• Nonpassive superstructures.Nonpassive superstructures.
• Inadequate screw joint closureInadequate screw joint closure
• Too rapid initial loadingToo rapid initial loading
• Functional overloadFunctional overload
• Periodontal infection (“peri-implantitis”)Periodontal infection (“peri-implantitis”)
– TreatmentTreatment• removal of the implantremoval of the implant
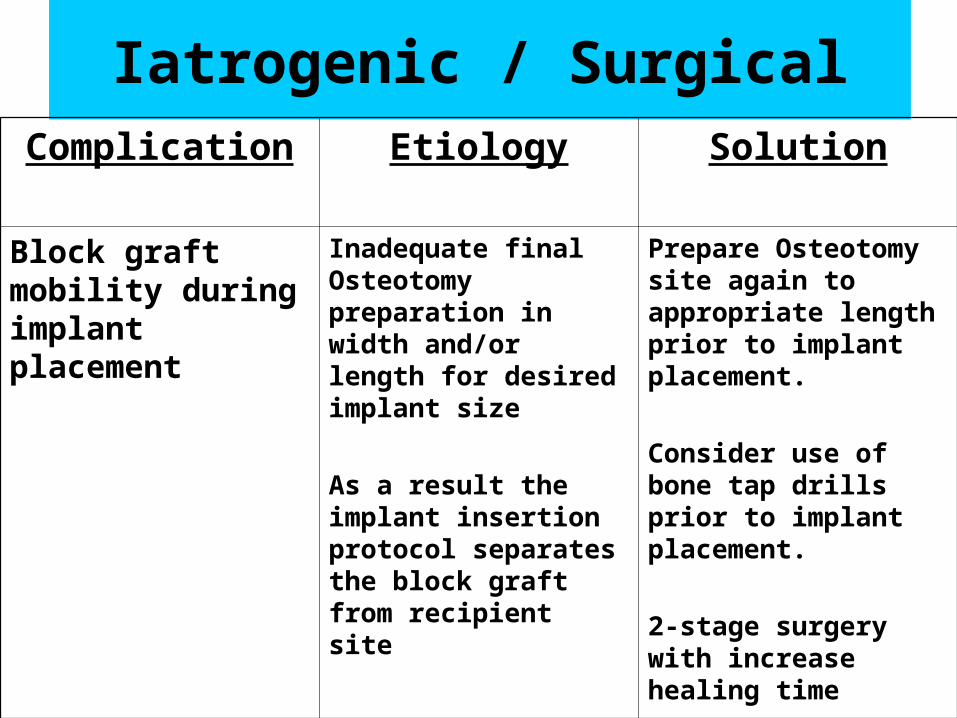
Iatrogenic / SurgicalComplication Etiology Solution
Block graft mobility during implant placement
Inadequate final Osteotomy preparation in width and/or length for desired implant size
As a result the implant insertion protocol separates the block graft from recipient site
Prepare Osteotomy site again to appropriate length prior to implant placement.
Consider use of bone tap drills prior to implant placement.
2-stage surgery with increase healing time

Clinical Protocol Related Block Grafts (Symphysis)
• Easier surgical access
• Larger donor graft size
• Potentially thicker volume of donor graft
• Mostly cortical with cancellous parts
• More demanding for wound closure
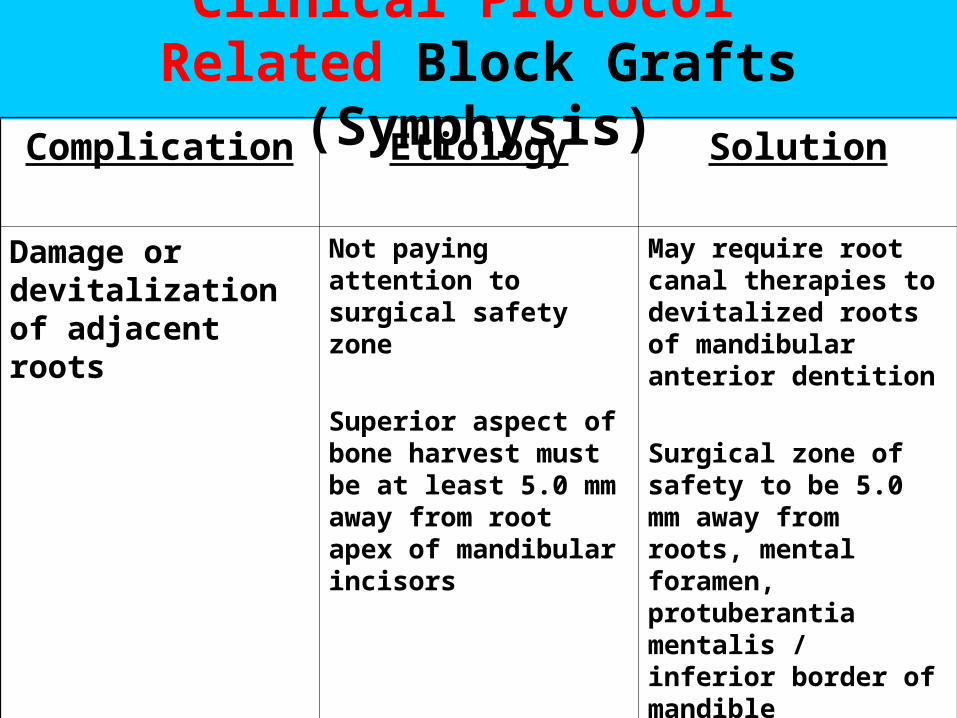
Clinical Protocol Related Block Grafts (Symphysis)Complication Etiology Solution
Damage or devitalization of adjacent roots
Not paying attention to surgical safety zone
Superior aspect of bone harvest must be at least 5.0 mm away from root apex of mandibular incisors
May require root canal therapies to devitalized roots of mandibular anterior dentition
Surgical zone of safety to be 5.0 mm away from roots, mental foramen, protuberantia mentalis / inferior border of mandible
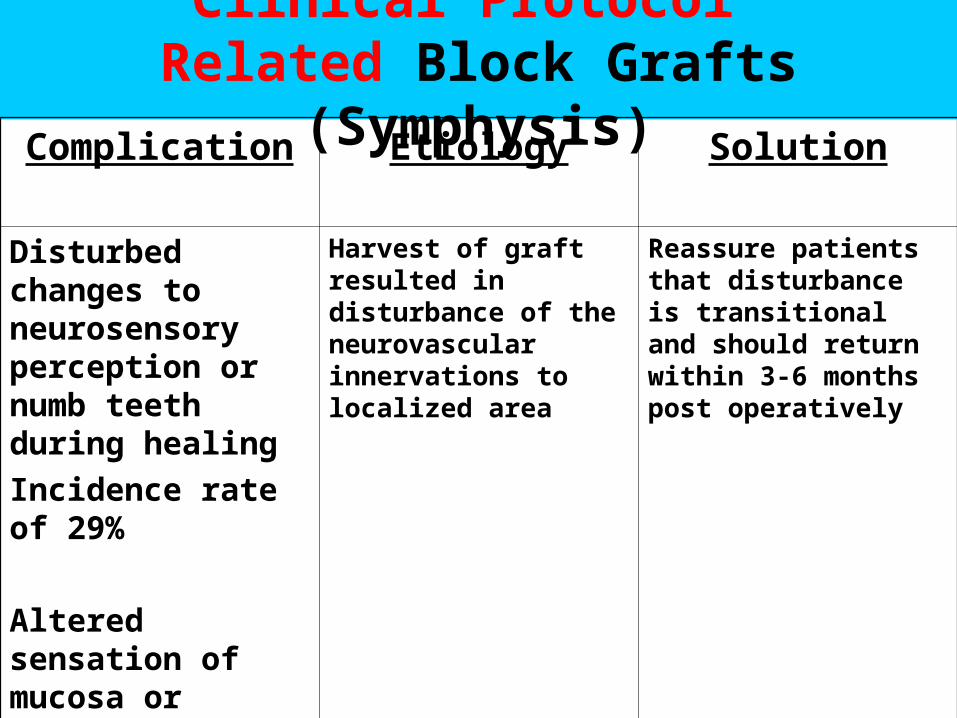
Clinical Protocol Related Block Grafts (Symphysis)Complication Etiology Solution
Disturbed changes to neurosensory perception or numb teeth during healing
Incidence rate of 29%
Altered sensation of mucosa or facial aspect of the lip or chin area
Harvest of graft resulted in disturbance of the neurovascular innervations to localized area
Reassure patients that disturbance is transitional and should return within 3-6 months post operatively
Clinical Protocol Related Block Grafts (Ramus)
• Difficult surgical access, especially inferior cut
• Smaller donor graft size
• Potentially thinner volume of donor graft
• Mostly cortical with few cancellous parts
• Easy wound closure
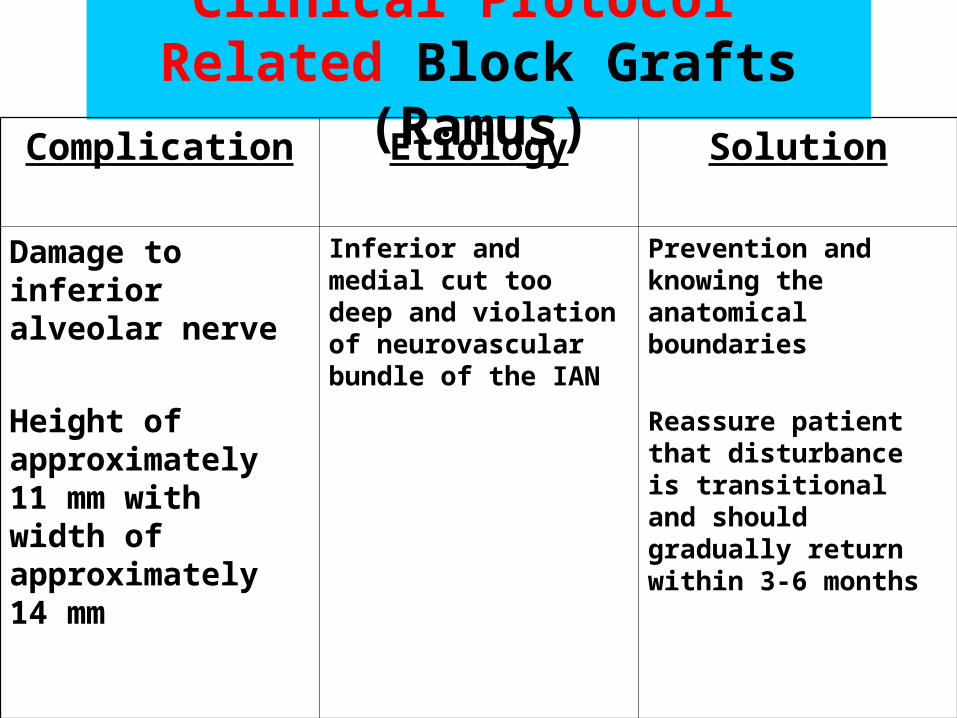
Clinical Protocol Related Block Grafts (Ramus)
Complication Etiology Solution
Damage to inferior alveolar nerve
Height of approximately 11 mm with width of approximately 14 mm
Inferior and medial cut too deep and violation of neurovascular bundle of the IAN
Prevention and knowing the anatomical boundaries
Reassure patient that disturbance is transitional and should gradually return within 3-6 months
Clinical Protocol Related Block Grafts (Ramus)
Complication Etiology Solution
Inadequate donor size harvest, too thin or too small
Difficulty of surgical access
Impaired visual access to inferior cut
Poor patient selection for Ramus harvest
Soft tissue incision and reflection to access desired size of graft required
Use of additional site to complete desired size of graft
Iatrogenic / SurgicalComplication Etiology Solution
Block graft mobility during implant placement
Insufficient healing time
Lack of initial block stability
Dead space too large or granulation tissue interposed between donor and recipient site
Micro movement of graft during healing from prosthesis loading
If graft appears vital: remove it, revive the recipient site, reposition graft and reaffix with micro screws.
Wait at least 6 months of healing with no loading.
If graft appears Non vital:
Remove it, clean recipient site, consider another grafting procedure.
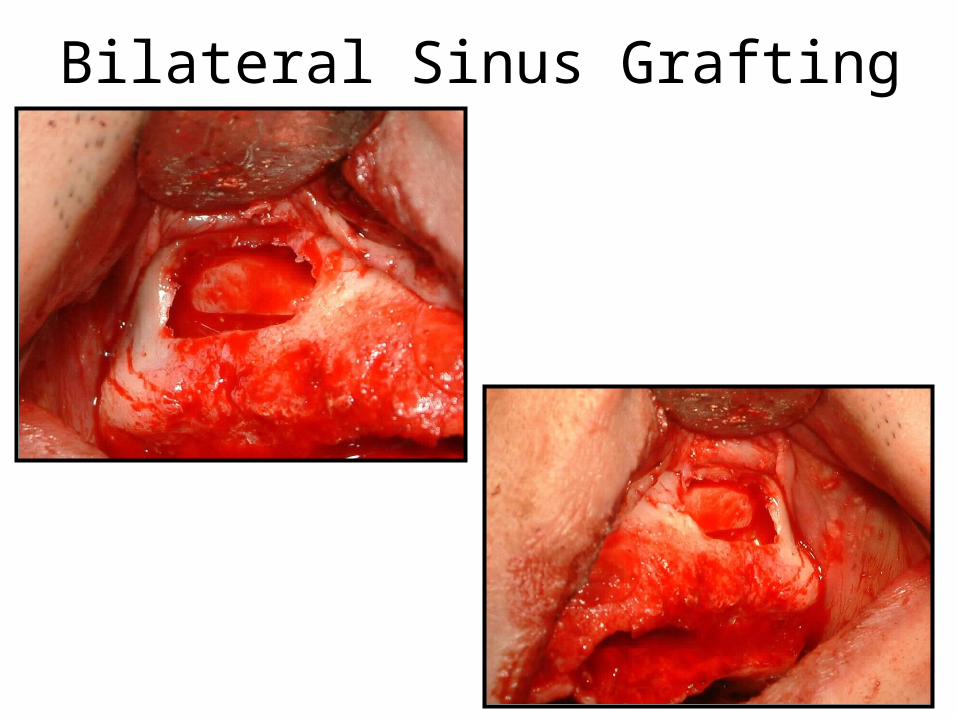
Bilateral Sinus Grafting
Iatrogenic / SurgicalComplication Etiology Solution
Small Perforation
(>5 mm) of the sinus Schneiderian membrane
incidence rate of
10-35%
Membrane is too thin specific to the patient
Membrane separation too rapid or wrong instrumentation
Presence of mucoid cyst
Presence of bony septae
Continue to separate around the small perforation to collapse and fold itself, then place a resorbable collagen membrane patch to close the breach integrity of membrane.
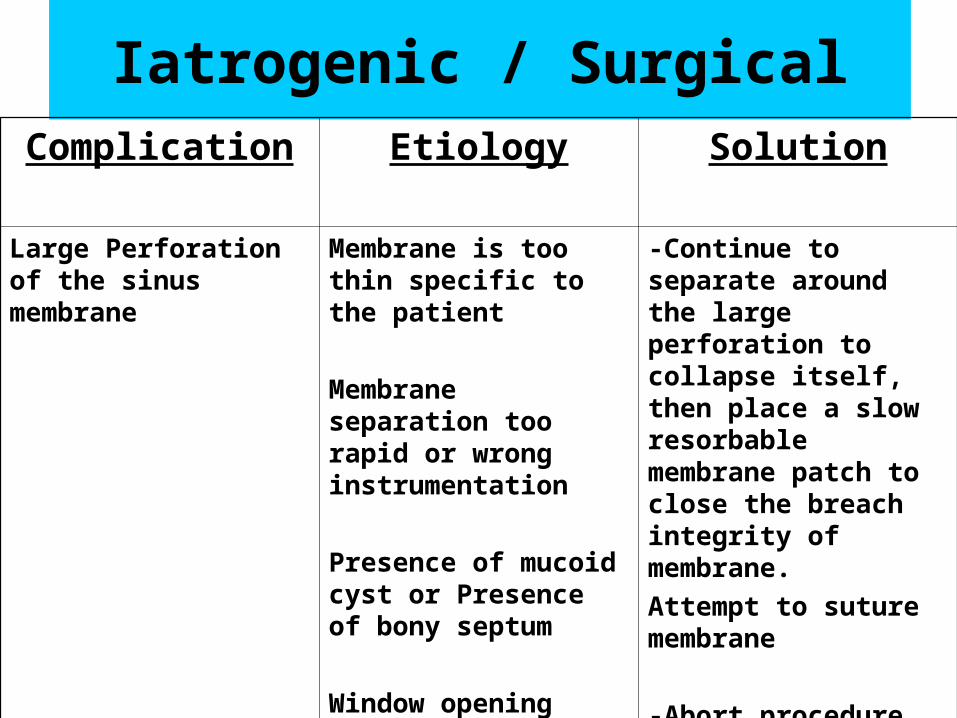
Iatrogenic / SurgicalComplication Etiology Solution
Large Perforation of the sinus membrane
Membrane is too thin specific to the patient
Membrane separation too rapid or wrong instrumentation
Presence of mucoid cyst or Presence of bony septum
Window opening with carbide instead of diamond burs
-Continue to separate around the large perforation to collapse itself, then place a slow resorbable membrane patch to close the breach integrity of membrane.
Attempt to suture membrane
-Abort procedure and reattempt entry after 6-12 months of healing.
During the Procedure• Window Separation• Haemorrhage• Pus• Serous Fluid• Difficulties in Sinus Lining Elevation
Difficulties in Window Separation
• Cut not through Bone
• Lower Cut below Floor of Sinus
• Cut too far Anterior
• Presence of Buttress
• Laceration of Lining
Difficulties in Lining Elevation
• Buttresses
• Undulations over Roots
• Peduncles over Roots
• Visibility and Access
• Sinus Lining Tears
Cause of Lining Perforation
• During Periosteal Elevation• During Window Preparation• Inadequate Instruments• Buttresses

• Layering
• Suturing
• Abort
Lining Perforation Management
When Tear Occurs
continue Elevation away from Tear
Suturing Tears• Do NOT attempt to Suture Thin Fragile Linings
• Larger Tears will occur
Immediately Post-operative
• Bruising • Haemorrhage• Swelling• Pain• Suture Line Opening• Infection
Delayed Post-Operative
• Pain
• Infection and Swelling
• Acute Sinusitis
• Chronic Sinusitis
• Oral-Antral Fistula
During Implant Placement
• Pus
• Sterile Serous Fluid
• Non-conversion of Graft
• Sinus Lining Perforation
Late Complications• Infection
• Loss of Graft
• Bone Loss around Implants
• Loss of Implants
Causes of Complications
• Pre-existing Infection
• Lining Perforation
• Surgical Field Contamination
• Graft Non-conversion
• Patient Non-compliance

Patient Non-compliance
• Smoking
• Drugs
• Alcohol
• Poor Oral Hygiene
• Self Abuse
Surgical Field Contamination
• Poor Surgical Technique
• Contaminated Graft Material
• Contaminated Implants
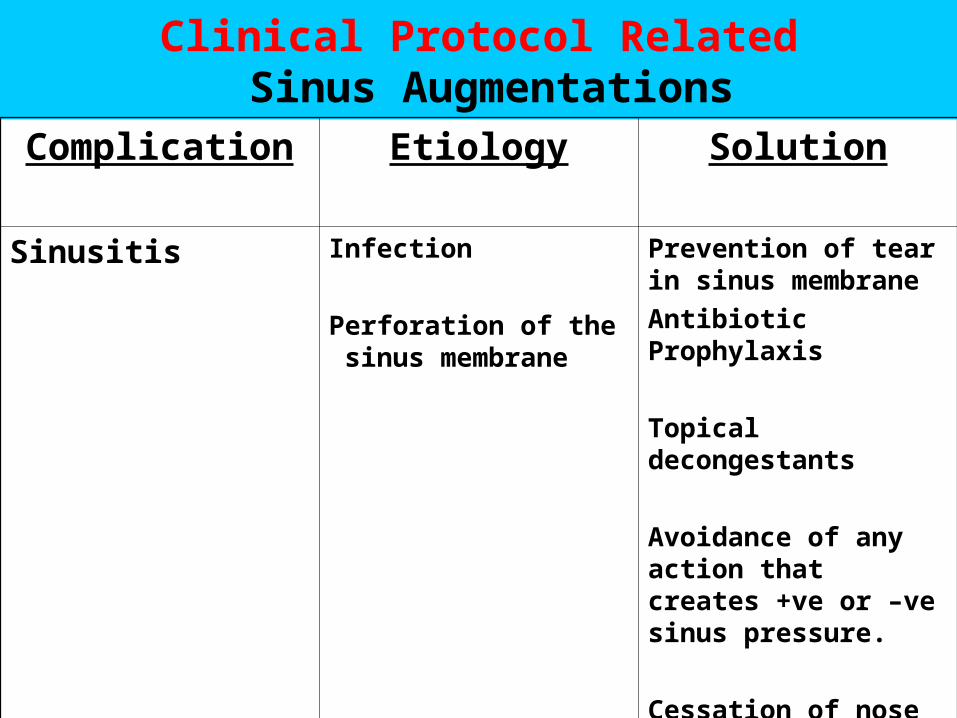
Clinical Protocol Related Sinus Augmentations
Complication Etiology Solution
Sinusitis Infection
Perforation of the sinus membrane
Prevention of tear in sinus membrane
Antibiotic Prophylaxis
Topical decongestants
Avoidance of any action that creates +ve or –ve sinus pressure.
Cessation of nose blowing and sneezing with open mouth
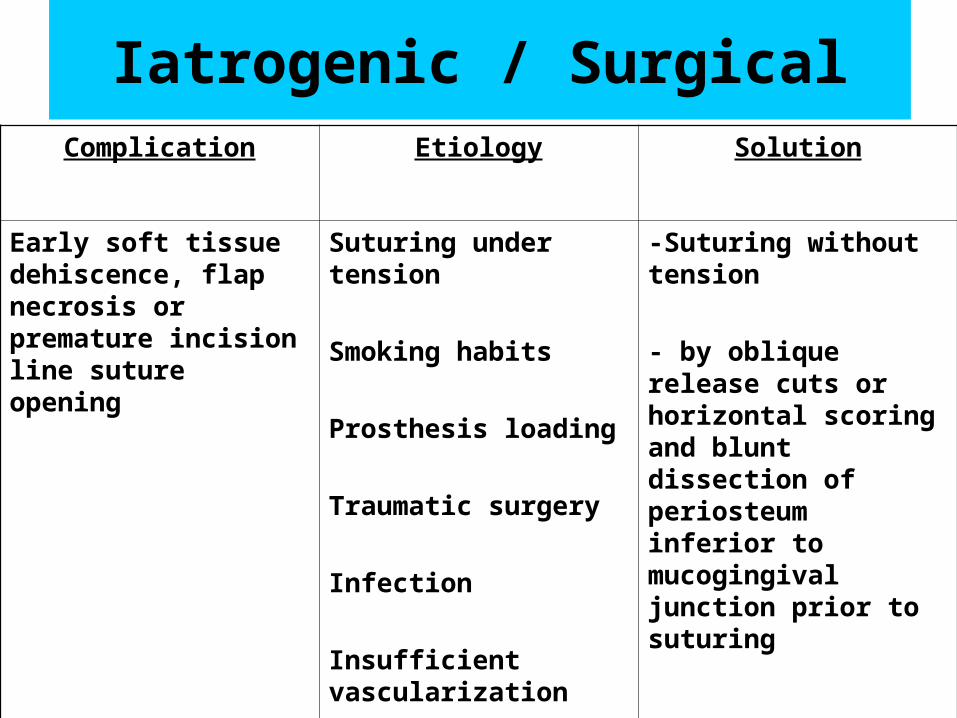
Iatrogenic / SurgicalComplication Etiology Solution
Early soft tissue dehiscence, flap necrosis or premature incision line suture opening
Suturing under tension
Smoking habits
Prosthesis loading
Traumatic surgery
Infection
Insufficient vascularization
-Suturing without tension
- by oblique release cuts or horizontal scoring and blunt dissection of periosteum inferior to mucogingival junction prior to suturing
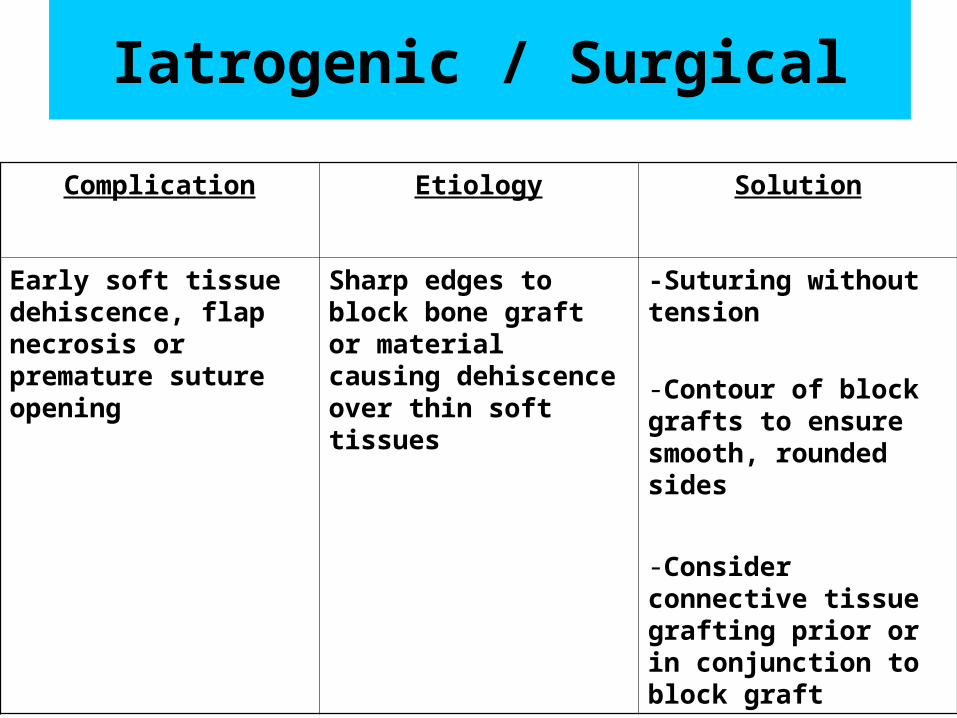
Iatrogenic / Surgical
Complication Etiology Solution
Early soft tissue dehiscence, flap necrosis or premature suture opening
Sharp edges to block bone graft or material causing dehiscence over thin soft tissues
-Suturing without tension
-Contour of block grafts to ensure smooth, rounded sides
-Consider connective tissue grafting prior or in conjunction to block graft
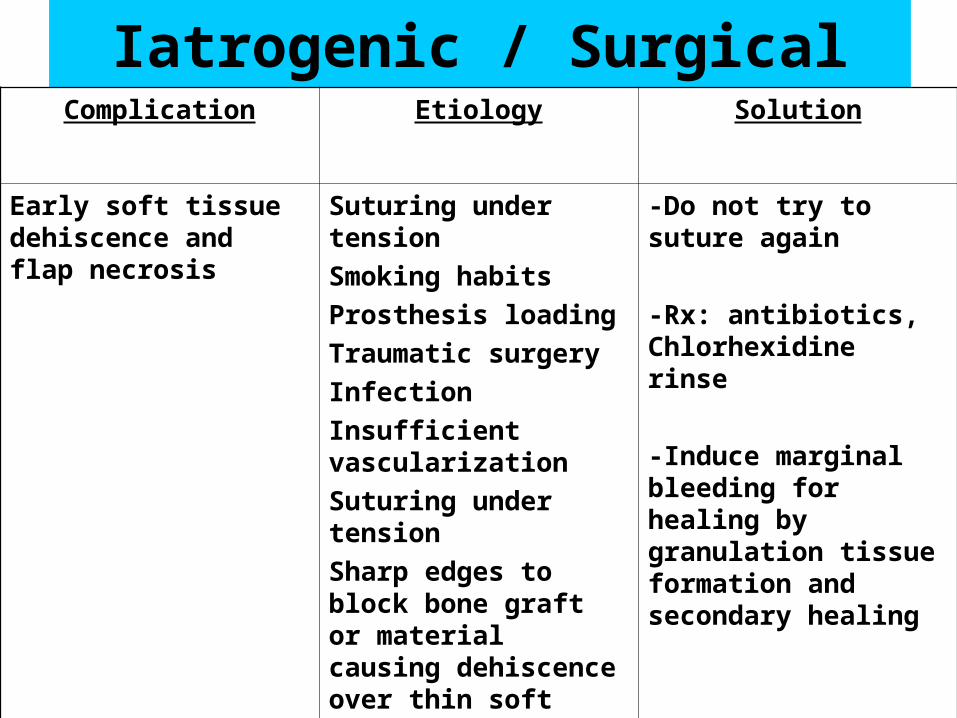
Iatrogenic / SurgicalComplication Etiology Solution
Early soft tissue dehiscence and flap necrosis
Suturing under tension
Smoking habits
Prosthesis loading
Traumatic surgery
Infection
Insufficient vascularization
Suturing under tension
Sharp edges to block bone graft or material causing dehiscence over thin soft tissues
-Do not try to suture again
-Rx: antibiotics, Chlorhexidine rinse
-Induce marginal bleeding for healing by granulation tissue formation and secondary healing
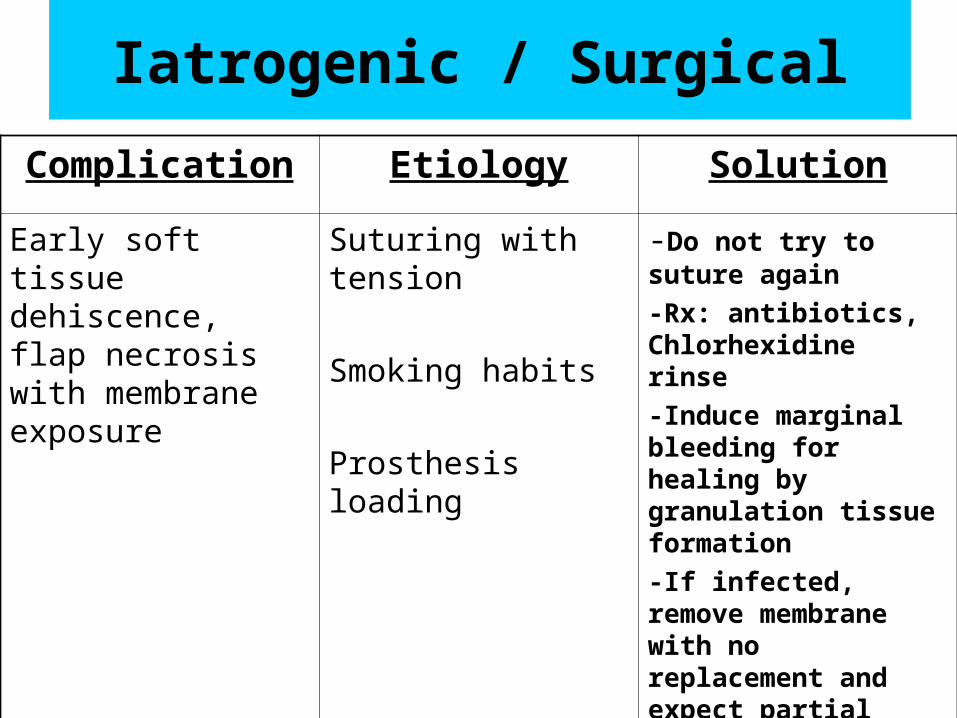
Iatrogenic / Surgical
Complication Etiology Solution
Early soft tissue dehiscence, flap necrosis with membrane exposure
Suturing with tension
Smoking habits
Prosthesis loading
-Do not try to suture again
-Rx: antibiotics, Chlorhexidine rinse
-Induce marginal bleeding for healing by granulation tissue formation
-If infected, remove membrane with no replacement and expect partial loss of graft
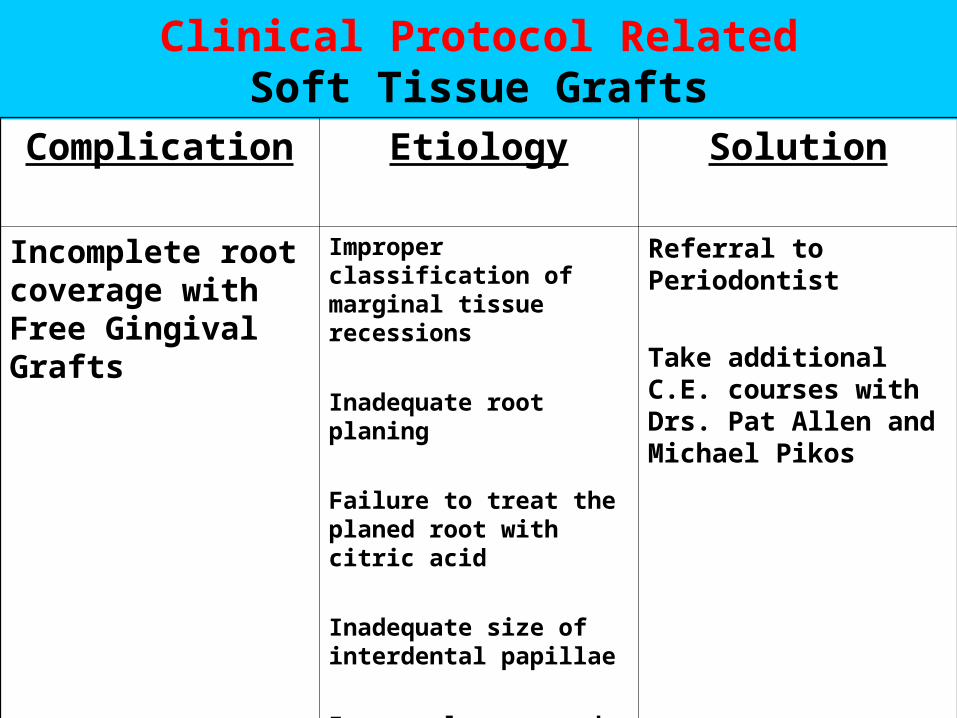
Clinical Protocol RelatedSoft Tissue Grafts
Complication Etiology Solution
Incomplete root coverage with Free Gingival Grafts
Improper classification of marginal tissue recessions
Inadequate root planing
Failure to treat the planed root with citric acid
Inadequate size of interdental papillae
Improperly prepared
donor tissue
Referral to Periodontist
Take additional C.E. courses with Drs. Pat Allen and Michael Pikos
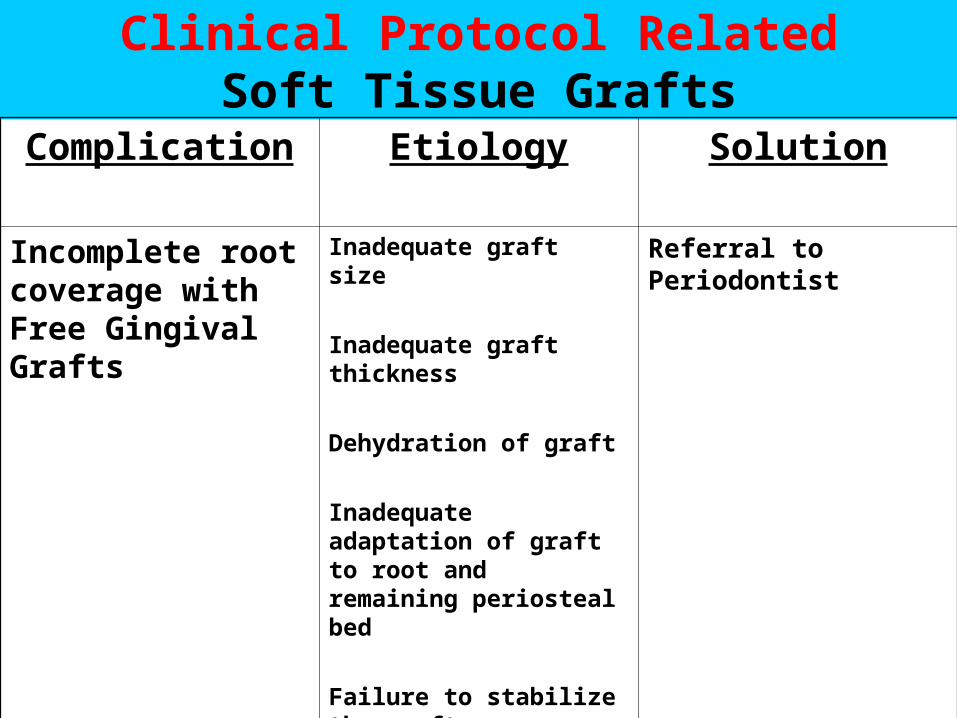
Clinical Protocol RelatedSoft Tissue Grafts
Complication Etiology Solution
Incomplete root coverage with Free Gingival Grafts
Inadequate graft size
Inadequate graft thickness
Dehydration of graft
Inadequate adaptation of graft to root and remaining periosteal bed
Failure to stabilize the graft
Referral to Periodontist
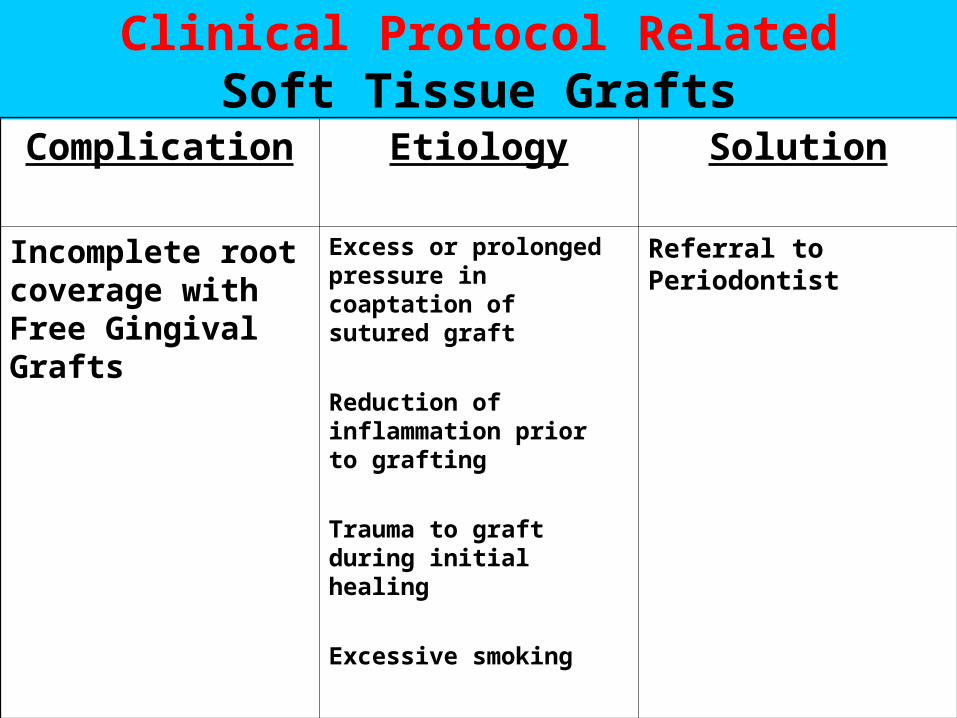
Clinical Protocol RelatedSoft Tissue Grafts
Complication Etiology Solution
Incomplete root coverage with Free Gingival Grafts
Excess or prolonged pressure in coaptation of sutured graft
Reduction of inflammation prior to grafting
Trauma to graft during initial healing
Excessive smoking
Referral to Periodontist
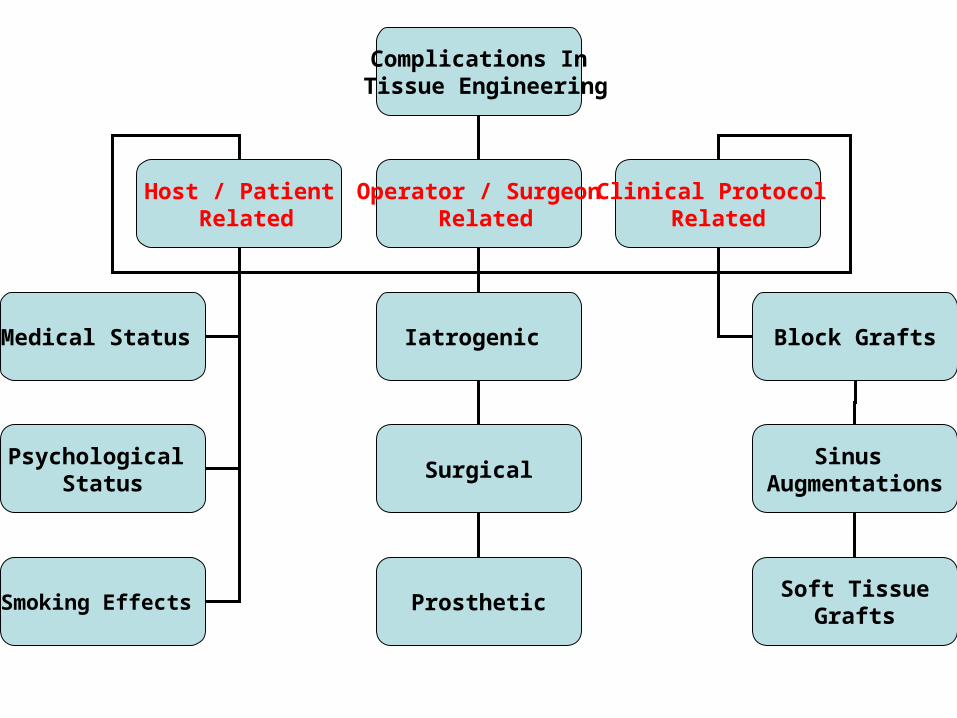
Complications In Tissue Engineering
Host / Patient Related
Operator / Surgeon Related
Clinical Protocol Related
Medical Status
Psychological Status
Smoking Effects
Iatrogenic
Surgical
Block Grafts
Sinus Augmentations
ProstheticSoft Tissue
Grafts
Advantages of Immediate Loading
• Immediate patient rehabilitation with instant gratification by patients
• Support and contours marginal soft tissues in esthetic zones
• Stimulation of bone regeneration with progressive loading protocol
• Decreased clinical interventions and appointments• Decreased treatment time / increase profit margin
Disadvantages of Immediate Loading
• Increased cost due to provisional fabrications
• Potential higher failure rate if inappropriately applied
• Rely on patient cooperation and compliance for success
• Need back up plan for provisional options
Indications to Immediate loading
• Primary surgical implant stability of >35 Ncm
• Lower anterior zones with splinting
• Patient driven for esthetic zones
• Aid in soft tissue contouring during healing phase
• Compliance of soft diet by patient during healing
Contraindications to Immediate loading
• Inadequate surgical initial stability of < 35 Ncm
• Need for bone grafting to implant recipient site
• Smokers
• Periodontal disease
• Poor prosthetic occlusal control of biomechanics
• Poor patient compliance and cooperation
Indications for Flapless Surgery
1) Confirmed 3 dimensional anatomical bony recipient site for desired implant diameter, length and angulations.
2) Abundant keratinized attached soft tissue adjacent the buccal aspect of implant recipient site.
3) Adjustment to depth of drilling length with soft tissue thickness accounted during osteotomies.
Advantages for Flapless Surgery
1) Less discomfort and morbidity for patients
2) Minimal to no swelling or bruising after surgical procedure
3) No suturing or removal of sutures post surgical appointment

Disadvantages for Flapless Surgery
1) Blinded procedure without flap release
2) Cannot visualize, identify and protect important anatomical landmarks
3) Risk of bone fenestration and dehiscence not identified
4) Risk of perforations of bone and incorrect implant alignment
5) Experienced surgeons to attempt
Complication Management
1) Plan
2) Prepare
3) Prevent
Dr. Mark Lin’s Contact Information
• E-Mail address:
• Office Number:416-221-8828
• Personal Cellular number:416-991-8828