Embed Size (px)
Citation preview

Prevention of Medical Errors
Melanie A. Crandall, OD,MBA,FAAO
Associate Professor
Nova Southeastern University
All Medical Providers
State of Florida began requiring a “Prevention of Medical Errors” course in every biennium
Sentinel Errors: Those that should never happen
Root Cause Analysis
How we got here?
Effort To End Surgeries On Wrong Patient Or Body Part Falters
“Such errors are considered so egregious and avoidable that they are classified as "never events," because they should never happen.” Joint Commission 2011
Botched brain surgery prompts extensive review at SSM Health Care..2013
Hospital Medical Errors Kill 98,000 Americans Each Year
6TEAMSTEPPS 05.2Mod 1 05.2 Page 6Mod 1 06.2 Page 6
Institute of Medicine Report Impact of Error:
44,000–98,000 annual deaths occur as a result of errors
Medical errors are the leading cause, followed by surgical mistakes and complications
More Americans die from medical errors than from breast cancer, AIDS, or car accidents
7% of hospital patients experience a serious medication error
Cost associated with medical errors is $8–29 billion annually.
Federal Action:
By 5 years;
medical errors by 50%,
nosocomial* by 90%; and eliminate “never-events” (such as wrong-site surgery)
(*Infections acquired within 48hrs of hospital admissions)
Impact of Medical Errors
Medical errors cost $37.6 Billion annually $17 B relate to preventable errors (IOM
estimates) Hospital drug related injuries total $3.5 Billion annually
(excluding lost wages, productivity & additional medical care costs)
42% of Americans have been affected by a med error (National Patient Safety Foundation) 32% medication error had a permanent effect
1.5 million individuals/year harmed by medication errors (Rx, OTC, vitamins, minerals & herbals) (IOM estimates) 7,000 individuals die /year from medication errors
– 16% more than work-related injuries
Introduction
Why Do Errors Occur—Some Obstacles
• Workload fluctuations
• Interruptions
• Fatigue
• Multi-tasking
• Failure to follow up
• Poor handoffs
• Ineffective communication
• Not following protocol
• Excessive professional courtesy
• Halo effect
• Passenger syndrome
• Hidden agenda
• Complacency
• High-risk phase
• Strength of an idea
• Task (target) fixation
Introduction
The Components of a Patient Safety Program

Sentinel Event
Serious injury specifically includes loss of limb or function. The phrase, "or the risk thereof" includes any process variation for which a recurrence would carry a significant chance of a serious adverse outcome. Such events are called "sentinel" because they signal the need for immediate investigation and response.
Sentinel Event Alerts
Potassium chloride Wrong site surgery Suicide Restraint deaths Infant abductions Transfusion errors High Alert Medications Op/post-op complications Impact of SE Alert Fatal falls Infusion pumps Proactive risk reduction Home fires (O2 therapy) Kernicterus Look-alike, sound-alike
drugs Kreutzfeldt-Jakob disease Medical gas mix-ups
Needles & sharps injuries
Dangerous abbreviations
Ventilator-related events Delays in treatment Bed rail deaths &
injuries Nosocomial infections Surgical fires Perinatal deaths Anesthesia awareness PCA by proxy Intrathecal vincristine Medication reconciliation Wrong route / wrong tube Emergency electrical
power system failureswww.jointcommission.org
Optometry I Love You

Sentinel Event Alerts
Wrong site surgery
High Alert Medications
Op/post-op complications
Fatal falls (hmmm)
Look-alike, sound-alike drugs
Needles & sharps injuries
Dangerous abbreviations
Delays in treatment
www.jointcommission.org
Root Cause Analysis
Systems
People
Pressure
Failure Mode and Effects Analysis in Health Care: Proactive Risk Reduction, Third Edition
Root Cause Analysis
Issue- What happened?
Likely Cause-Why did it happen?
Possible Solution- What do you do to prevent it happening again?

Error Reduction and Prevention
Every “Event” should be analyzed and a plan put in place to prevent a recurrence.
Root Cause Analysis
1. Determination of human factors2. Determination of related processes
and systems3. Analysis of cause and effect
systems through a series of WHY questions
4. Identification of risks and their potential contributions
5. Determination of potential improvement in process and systems
Root Cause Analysismust include
Participation of leadership and those most closely involved in the process and systems
Be internally consistent
Include consideration of relevant literature

Captain “Sully” Sullenberger
“Like aviation, medicine is a highly technical and complex profession with most errors caused by individual error, poor communication, defective equipment or faulty systems.”
Flattened hierarchy, captains and crews are expected to work together as teams and share a sense of responsibility.
Hospital Based Medicine
5-R’s: Right Pt, Med, Dosage, Route, Time
Pre Surgical Stop Checklist
Infection Control(TV remotes?)
Good practitioners are recognizedbecause of their C-D-C
Good reputations develop because of their:
• Competence
• Diligence
• Communication skills

Communication
“Patients do not care how much you know until they know how much you care.”
When a patient decides they do not like you, the patient begins to look for what is wrong with your office:
The dust, cob webs , old equipment, grouchy staff , poor information
Things can go wrong…..
Consider Office Safety
Reduce slip and fall possibilities Maintain licensing , certification and
accreditation OSHA Staff training for emergency
procedures both rare and more common.
The Work Setting
Check for outdated or damaged equipment
Secure age & patient specific equipment

In Office Safety
Always Double Check
Medication Errors
Sound a Like drug names

Look a Like Packaging
“Branding” can also be confusing!
Where is the pink top!
Checklist
Consider using a checklist system at the conclusion of the exam to ensure you have completed communication, prescriptions and referrals if needed
The Checklist Manifesto: How to Get Things Right by Atul Gawande
Top 10 Screw-ups Pharmacists Make*
1. Dispensing the wrong drug
2. Dispensing the wrong dose
3. Not counseling patients
4. Ignoring interactions
5. Not standing up to doctors
6.Trusting all generic drugs
7. Relying on inadequate labels and leaflets
8. Not reporting errors
9. Switching drugs without patient approval
10. Not supervising techs carefully
*From #6 in references

Clomiphene v. Clonazepam
Clomid: Clomiphene CLOMID is indicated for
the treatment of ovulatory dysfunction in women desiring pregnancy. Impediments Recommended Dosage:
Treatment of the selected patient should begin with a low dose, 50 mg daily (1 tablet) for 5 days.
Klonopin: ClonazepamPRESCRIBED FOR:
Clonazepam is used for the short-term relief of symptoms of anxiety.
DOSING: The dose of clonazepam is tailored to the patient's needs. For seizuresin adults the initial dose is 1.5 mg daily in 3 divided doses. Dosage may be increased by 0.5 to 1 mg daily every 3 days until seizures are controlled or side effects preclude further increases in dose. The maximum dose is 20 mg daily. The initial dose for panic disorders is 0.25 mg twice daily. The dose may be increased to the target dose of 1 mg daily after 3 days.
Oops
Right Aid Pharmacy in New Hampshire filled Rx for
Clomid 50mg for 5 days with
Klonopin 50mg , this double the maximum daily dose and this drug is never started full strength.
Infectious Keratitis-unknown cause
Sample of Moxeza
Rx of Tobramycin
Pt instructed to use alternately every hour
Patient was seen as an emergency
Seen and treated on Wednesday and asked to return Friday
Patient said Pharmacist would not fill Rx because “She did not need it.”
She had been well instructed to call if not better the next day…. Next time I will include specific language on Rx.
Florida’s Prescription Law
A written prescription for drugs MUST be legibly printed or typed and contain the following information: Name of prescribing practitioner Name and strength of medication Quantity of the drug in both textual and numeric formats
(e.g. #45 forty-five) Directions for use Dated with the month written in textual letters (e.g. July
10, 2014, not 7/10/14)
Florida’s Prescription Law
Always use a leading zero before a number less than one (e.g. 0.5 mg) and never use a terminal zero (e.g. 5.0 gm).
Write out the actual amount prescribed in addition to giving the Arabic number or Roman numeral to discourage alterations.
Do not make any changes or cross-outs.
Top 10 Screw-up's Doctors Make*
1. Not listening to patients
2. Misdiagnosing
3. Providing too little information
4. Not dealing with side effects
5. Under-treating or ignoring evidence
6. Over reacting or being seduced by numbers
7. Overlooking drug interactions
8.Failure to revise the plan
9. Overlooking lab results
10. Not addressing life style issues
*From #6 in references
#1 Not Listening
Studies show Doctors interrupt patients within 12-20 seconds of the beginning of an office visit.
“Thought in Action” Doctors already coming up with diagnoses during hello and exam. This is the use of heuristics.
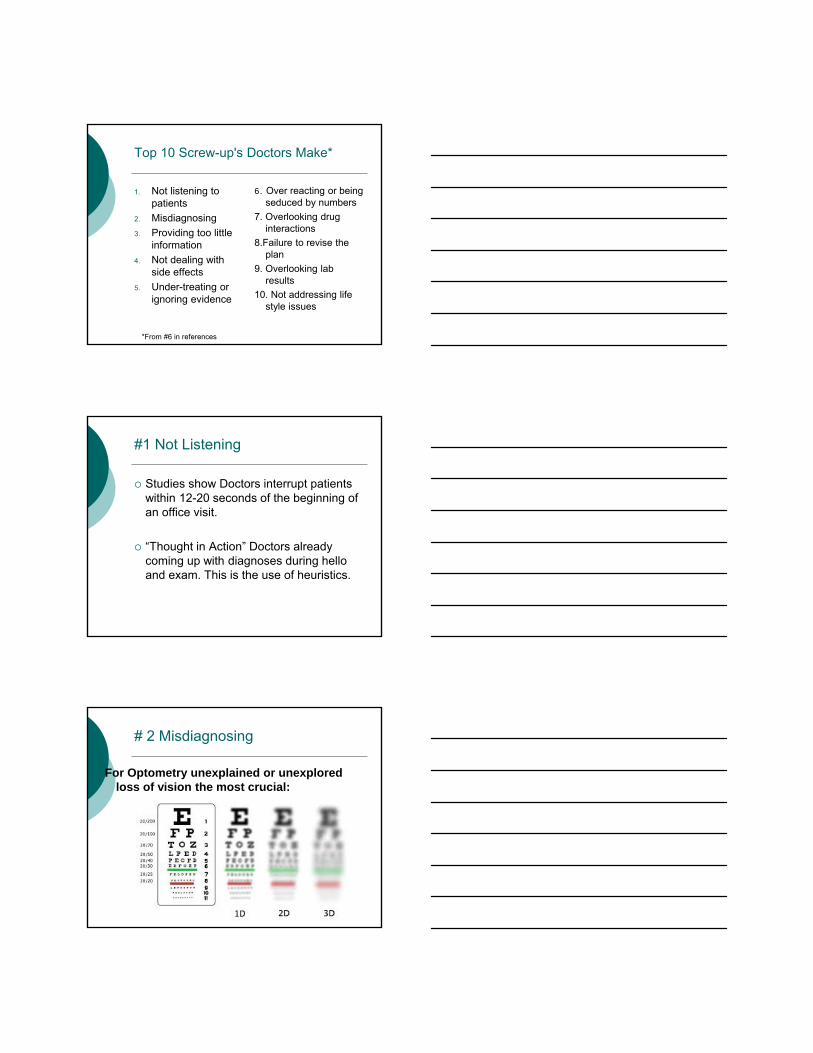
# 2 Misdiagnosing
For Optometry unexplained or unexplored loss of vision the most crucial:
Top 10 Screw-up's Doctors Make
1. Not listening to patients
2. Misdiagnosing
3. Providing too little information
4. Not dealing with side effects
5. Under-treating or ignoring evidence
6. Over reacting or being seduced by numbers
7. Overlooking drug interactions
8.Failure to revise the plan
9. Overlooking lab results
10. Not addressing life style issues
Prevention of Medical Errors
Proper data collection: we are guided by Medicare and Vision care plans
Documenting Findings:
Evaluating Findings , considering all of them,
Clearly communicating to our patients
Clinical Decision Making
“Most Clinical Decisions involve many factors, great uncertainty and difficult value decisions” (1)

Clinical Decision Making
Applying our science, learning our art.
Making judgments and taking action in the face of uncertainty.
Heuristics
A heuristic is a method to help solve a problem, commonly informal. It is particularly used for a method that often rapidly leads to a solution
Heuristic
Heuristic (hyu-ˈris-tik) is an adjective for methods that help in problem solving, in turn leading to learning and discovery. These methods in most cases employ experimentation and trial and error techniques. A heuristic method is particularly used to rapidly come to a solution that is reasonably close to the best possible answer, or 'optimal solution'. Heuristics are "rules of thumb", educated guesses, intuitive judgments or simply common sense. Heuristics (hyu-ˈris-tiks) as a noun is another name for heuristic methods. (from Wikipedia)

Heuristics
Help us solve complex problems in a short amount of time
There are known cognitive errors that can occur
We need to be aware of the pitfalls and try to avoid them
The Three A’s
Anchoring
Attribution
Availability
Anchoring
Anchoring or focalism is a cognitive bias that describes the common human tendency to rely too heavily, or "anchor," on one trait or piece of information when making decisions.
Anchoring
A shortcut in thinking where one fails to consider multiple possibilities but quickly and firmly latches on to a single one
Attribution Error
When patients fit a negative stereo type
Availability
The availability heuristic is a phenomenon (which can result in a cognitive bias) in which people base their prediction of the frequency of an event or the proportion within a population based on how easily an example can be brought to mind.
Simply stated, where an anecdote ("I know a American guy who...") is used to "prove" an entire proposition or to support a bias, the availability heuristic is in play. (from Wikipedia)

Many More….
The representativeness heuristic is a heuristic wherein people assume commonality between objects of similar appearance, or between an object and a group it appears to fit into. While often very useful in everyday life, it can also result in neglect of relevant base ratesand other errors. (from Wikipedia)
Representativeness Error
Your thinking is guided by a prototype, so you fail to consider possibilities that contradict the prototype
Conformation Bias
Confirming what you expect to see and ignoring signs and symptoms that don’t fit
Driven by the expectation that your initial diagnosis was correct, you only consider findings that prove you right.

Affective Error
“We lull ourselves into thinking what we wish for will occur when we get the first inkling, however fragmentary, that our wish may come true.”
This is driven by a wish for a certain outcome
Combinations…..
Anchoring and adjustment is a psychological heuristic that influences the way people intuitively assess probabilities. According to this heuristic, people start with an implicitly suggested reference point (the "anchor") and make adjustments to it to reach their estimate.
(from Wikipedia)
What is wrong with this picture?
How to Avoid Errors (1)
Always generate a short list of alternatives (differentials)What else can it be?
Is there anything that doesn’t fit?
Is it possible there is another problem?
Is there anything in the history, exam or lab test that seems to be at odds with the working diagnosis?
Clinical Maxims, Some Rules of Clinical Reasoning
They guide the development of clinical judgment
They replicate the thought practice engaged in by clinical doctors
Aphorisms and maxims guide the acts of practical reasoning essential to patient care: history taking, exam, diagnostic reasoning and therapeutic choice
Clinical Maxims, Some Rules of Clinical Reasoning (4)
They are not definitive or absolute
Every maxim is qualified or contradicted by another
Judiciously balanced application of generalized scientific or clinical knowledge to an individual patient

History- Taking
“The diagnosis is usually made from the history.”
“The patient denies alcohol use.”
Professionalized doubt about the reliability of history
Examination
Fit clinical observations into known patterns.
Take account of every detail and weigh them carefully.
Tests
“The best medicine is to do as much nothing as possible.”
(Suttons Law)
“Full Court Press”
Diagnosis
“Look for a single diagnosis that can explain all the findings.”(Occam’s razor)
“It’s parsimonious, but it may not be right”(Hickam’s dictum)“The patient can have as many diseases as he damn well pleases”
Treatment
“Relieve the symptoms.”
“Make the diagnosis.”
Diagnosis
“When you hear hoof beats, don’t think zebras.”
And yet the injunction not to consider “zebras” reminds us that they are out there and we need to know them.
Rare diseases are rare…..
The Goal of Clinical Medicine
The therapeutic imperative, or: “Always do everything for every patient forever”
or
“Don’t just do something, stand there.”, above all do no harm
The use of Experience in Clinical Knowing
“The research shows…..”
“In my experience….”
The Nature of Clinical Knowing
“Medicine is a science.”
“Medicine is an art.”
Avoid Malpractice
Put Patients needs first
Do not make findings fit diagnosis
Insist that everything make sense
Do not disregard patient complaints
Check drug facts and PRINT medical prescriptions
Document everything….and do it legibly
Introduction
Why Do Errors Occur—Some Obstacles
• Workload fluctuations
• Interruptions
• Fatigue
• Multi-tasking
• Failure to follow up
• Poor handoffs
• Ineffective communication
• Not following protocol
• Excessive professional courtesy
• Halo effect
• Passenger syndrome
• Hidden agenda
• Complacency
• High-risk phase
• Strength of an idea
• Task (target) fixation
In Quality Optometric Care
Do not feel you have to do everything in one visit.
Do not hesitate to have patient to come back to do additional test or follow up.
Document Thinking

References
1. How Doctors Think by Jerome Groopman
2. Judgment under uncertainty: Heuristics and biases by Kahneman et al
3. Critical Thinking in Clinical Practice, Improving the Quality of Judgments and Decisions By Gambrell
4. How Doctors Think, Clinical Judgment and the Practice of Medicine by Montgomery
References- Error Reduction
5. The Checklist Manifesto: How to Get Things Right by Atul Gawande
6. Top Screwups Doctors Make and How to Avoid Them. Graedon and Graedon, Three Rivers Press, 2011
7. The Harm We Do: A Doctor Breaks Rank About Being Sick In America by Brawley, Otis Webb, MD
More Reading
Waking Up Blind by Tom Harbin, MD





























