Embed Size (px)
Citation preview

Prevention of mother to child transmission of viral
hepatitis
Dr. Lawrence Mbuagbaw MD, MPH, PhD, FRSPH
2nd International HIV/Viral Hepatitis Co-infection Meeting
Friday July 17th, 2015

Outline
1. Background2. When can transmission occur?3. At what levels can we stop
transmission?4. Current recommendations5. Take home messages

BackgroundPrevalence of HIV in females and children1
• An estimated 35 million people were living with HIV worldwide in 2013.– 3.2 million were children under 15 years of age.– 17.6 million were women and girls.
• The annual number of newly infected children in 2013 was 240 000.– Over 90% of these children live in sub-Saharan
Africa
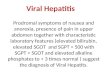
BackgroundIncidences of HIV, HBV, HCV co-infections2
*Shown are estimated numbers (in millions) of patients singly or doubly infected.

BackgroundHIV & HBV co-infection
• In areas of low endemicity of HIV/HBV co-infection3:– Prevalence of co-infection is 5-7% among HIV-infected
individuals– Mode of transmission is mainly in adulthood via sexual or
percutaneous transmission
• In areas of high endemicity of HIV/HBV co-infection4:– Prevalence of co-infection is 10-20%– Mode of transmission is mainly perinatal or in early
childhood.

BackgroundPrevalence of hepatitis B infection, adults
(19-49 years), 20055
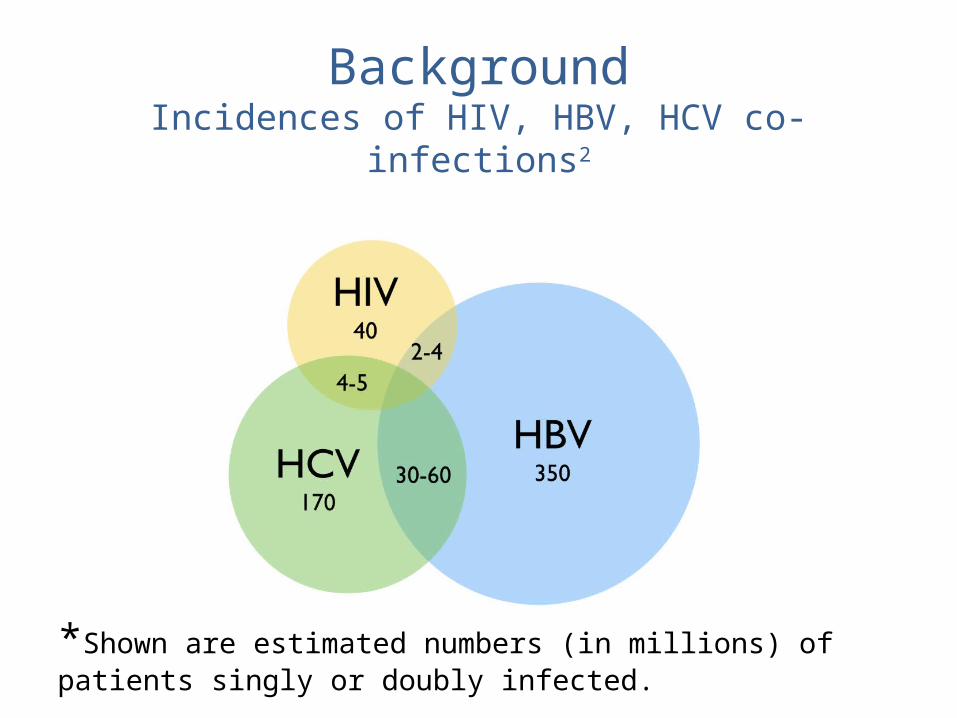
BackgroundPrevalence of hepatitis B infection, children (4-9 years),
20055

BackgroundPrevalence of HIV infection, adult (15-49
years), 20136
BackgroundWhat is particular about a pregnant woman?
1. Potential teratogenicity of antivirals
2. Physiological changes associated with pregnancy have an impact on how the body processes HBV medication
3. Impact of chronic hepatitis B on pregnancy outcomes
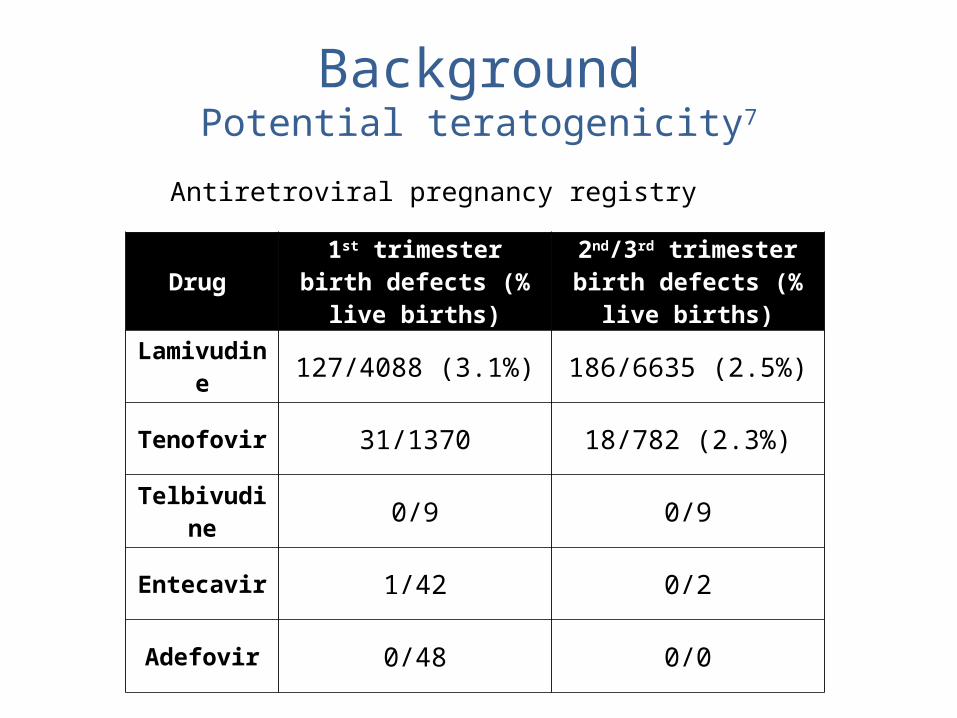
BackgroundPotential teratogenicity7
Drug
1st trimester birth defects (% live
births)
2nd/3rd trimester birth defects (%
live births)
Lamivudine 127/4088 (3.1%) 186/6635 (2.5%)
Tenofovir 31/1370 18/782 (2.3%)
Telbivudine 0/9 0/9
Entecavir 1/42 0/2
Adefovir 0/48 0/0
Antiretroviral pregnancy registry

BackgroundPhysiological changes caused by pregnancy8,9,10
• Pregnancy has been shown to alter pharmacokinetics of drugs metabolized by cytochrome P450 3A4.
• Aweeka et al. showed increases in the urinary ratio of 6-β hydroxycortisol to cortisol (a marker of CYP3A4 induction) during pregnancy compared with postpartum8.
• Consequently, the dosage of corresponding antiretroviral medication may need to be altered during pregnancy.

BackgroundImpact of CHB on maternal and fetal-neonatal outcomes11,12
• Lao et al. reported a significantly higher prevalence of gestational diabetes mellitus in mothers with HBsAg positivity when compared to those without chronic hepatitis B.
• Maternal HBsAg positivity is also associated wth increased antepartum hemorrhage, and threatened preterm labor.

BackgroundRisk factors for perinatal transmission
• HBV DNA Level13: Zou et al. demonstrated a linear correlation between immunoprophylaxis failure rates and maternal HBV DNA levels in 1043 mother-infant pairs
• HBV replicative status14: 85-90% transmission rates in infants born to HBeAg-positive mothers and 32% in infants born to HBeAg-negative mothers
When can maternal-infant HBV transmission occur?
Infection rate among infants born to HBeAg-positive mothers who do not receive any form of prophylaxis is as high as 90%15, 16.
1. During Pregnancy:A. AntepartumB. Intrapartum: majority of total
transmission16. Postulated mechanisms are:• Exposure of the baby’s
mucocutaneous surface to maternal blood and cervical secretions.

When can maternal-infant HBV transmission occur?17
2. After Delivery Breast Feeding: does NOT increase risk of MTCT of HBV– Hill et al. compared the rate of HBV
transmission from chronic HBV carrying mothers in 101 breast-fed infants with 268 formula-fed infants. Infants received HBIG and full course of hepatitis B vaccine series.
– MTCT of HBV was 0% when breast-fed vs. 3% when formula-fed.

At what levels can we stop antepartum transmission?
• Current immunoprophylaxis is less efficacious in mothers with high serum levels of HBV DNA > 6 log10 copies/mL13.
• Antiviral treatment in third trimester may reduce risk of HBV MTCT18, 19, 20
– In a randomized, placebo-controlled study, lamivudine was administered to highly viremic mothers (HBV DNA >1000 mEq/mL) starting at 32 weeks gestation until 4 weeks postpartum. Rate of MTCT was 18% in lamivudine group vs. 39% in control group at 52 weeks.

At what levels can we stop intrapartum transmission?
• Currently, both HBIG and hepatitis B vaccine is given to the infant immediately after birth.
• Early RCT by Beasley et al. showed that HBIG administration can reduce rate of HBV transmission from more than 90% from HBeAg-positive mothers down to about 26% 21
• When combined with the hepatitis B vaccine, the rates of transmission fell to 3% from 7% 22
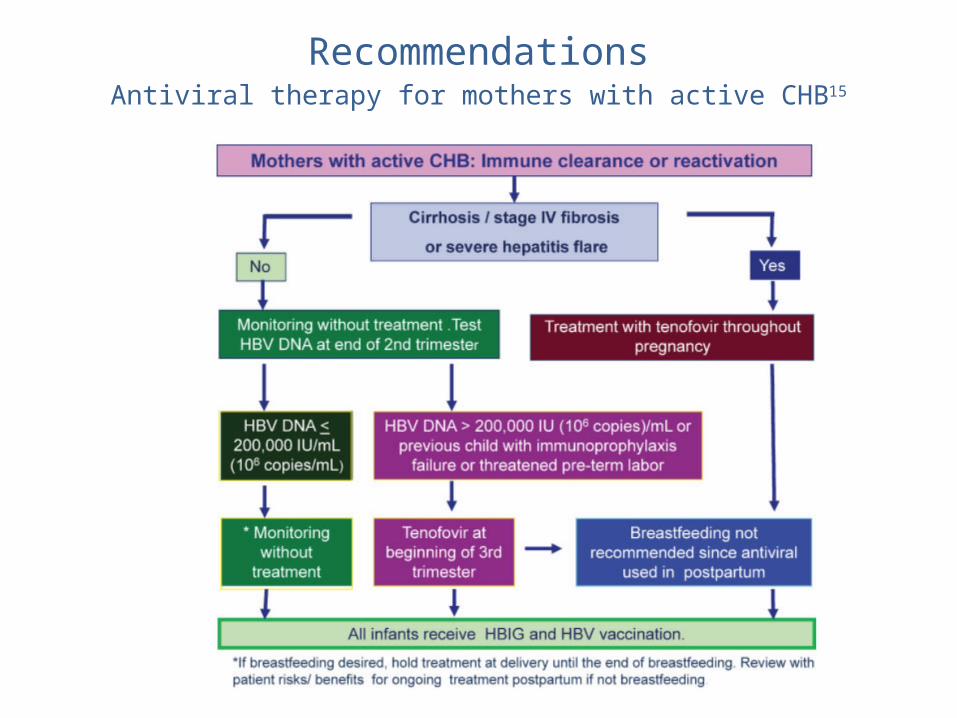
RecommendationsAntiviral therapy for mothers with active CHB15

RecommendationsAntiviral therapy for mothers without active
CHB15
Issues with current recommendations
• Gap in literature with regards to the benefits of antiviral therapy for mothers with HBV DNA levels <200,000 IU/mL.
• More data are needed regarding the long-term safety of fetal exposure to antiviral therapy.– The lack of access to HBV DNA level
testing may prohibit women from receiving needed treatment.

The way forward
• Further research• Do what we know works– Screening– Immunisation– Chemoprophylaxis
• Share our experiences working with co-infected women
Take home messages1. Screen all HIV-infected pregnant women for Hep B&C2. All –ve should receive Hep B vaccine3. All co-infected pregnant women should receive cART
(tenofovir, lam, emtricitabine)
4. Frequent monitoring of liver function tests & Hep B DNA
5. Children born to women with HBV infection should receive HBIG and HBV vaccination series
6. Mode of delivery is based on standard OB/HIV considerations
7. Mgt is complex and requires specialist consultation

THANKS FOR LISTENING