PREVENTION OF POLYCYSTIC OVARIAN SYNDROME: SKY HIGH …
32
www.wjpps.com Vol 8, Issue 8, 2019. 515 Das et al. World Journal of Pharmacy and Pharmaceutical Sciences PREVENTION OF POLYCYSTIC OVARIAN SYNDROME: SKY HIGH OBJECT THROUGH NATURAL PRODUCTS Saptarshi Das 1 *, Sohini Sarkar 2 , Soumalya Sarkar 3 , Souvik Mukherjee 4 and Souranava Jana 5 * 1 Assistant Professor, Department of Pharmaceutical Analysis, Bharat Technology, Uluberia, Howrah, West Bengal, India. 2 Department of Pharmacy, Bengal College of Pharmaceutical Sciences and Research, Durgapur, West Bengal, India. 3 Drug Discovery Research Center, Translational Health Science and Technology Institute, Faridabad, Haryana, India. 4 UGC-SAP Research Lab, Department of Pharmacy, Guru Ghasidas Vishwavidyalaya (A Central University), Bilaspur C.G. India. 5 Department of Pharmacy, Guru Ghasidas Vishwavidyalaya (A Central University), Bilaspur C.G. India. ABSTRACT Polycystic ovarian syndrome (PCOS) is a diverse hormonal disorder that affects about one in 15 women worldwide. It is a most important disorder considered as elevated levels of male androgens, acne and hirsutism. It can even cause insulin resistance, anovulation and infertility on prolong incidence of cysts. However PCOS is a remediable disorder, it can be treated by use of natural remedies or allopathic medication. The natural remedies include treatment with phytoestrogen and non-estrogenic herbs such as Liquorice, Ginseng, Black cohosh, Dong qui, Hops and Kelp etc. These are effective and safe better than allopathic medicine. In this review, an attempt has been made to study the potential of natural products for treatment of Polycystic Ovarian Syndrome. KEYWORDS: PCOS, Hormone, Liquorice, Ginseng, Black cohosh, Dong qui, Hops and Kelp. WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES SJIF Impact Factor 7.421 Volume 8, Issue 8, 515-546 Review Article ISSN 2278 – 4357 *Corresponding Author Saptarshi Das Assistant Professor, Department of Pharmaceutical Analysis, Bharat Technology, Uluberia, Howrah, West Bengal, India. Article Received on 03 June 2019, Revised on 24 June 2019, Accepted on 15 July 2019 DOI: 10.20959/wjpps20198-14396
PREVENTION OF POLYCYSTIC OVARIAN SYNDROME: SKY HIGH …
515
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
PREVENTION OF POLYCYSTIC OVARIAN SYNDROME: SKY HIGH
OBJECT THROUGH NATURAL PRODUCTS
2 , Soumalya Sarkar
3 , Souvik Mukherjee
4 and Souranava
Howrah, West Bengal, India.
2 Department of Pharmacy, Bengal College of Pharmaceutical Sciences
and Research,
Durgapur, West Bengal, India.
3 Drug Discovery Research Center, Translational Health Science and
Technology Institute,
Faridabad, Haryana, India.
4 UGC-SAP Research Lab, Department of Pharmacy, Guru Ghasidas
Vishwavidyalaya
(A Central University), Bilaspur C.G. India.
5 Department of Pharmacy, Guru Ghasidas Vishwavidyalaya (A Central
University),
Bilaspur C.G. India.
Polycystic ovarian syndrome (PCOS) is a diverse hormonal
disorder
that affects about one in 15 women worldwide. It is a most
important
disorder considered as elevated levels of male androgens, acne
and
hirsutism. It can even cause insulin resistance, anovulation
and
infertility on prolong incidence of cysts. However PCOS is a
remediable disorder, it can be treated by use of natural remedies
or
allopathic medication. The natural remedies include treatment
with
phytoestrogen and non-estrogenic herbs such as Liquorice,
Ginseng,
Black cohosh, Dong qui, Hops and Kelp etc. These are effective
and
safe better than allopathic medicine. In this review, an attempt
has
been made to study the potential of natural products for treatment
of
Polycystic Ovarian Syndrome.
KEYWORDS: PCOS, Hormone, Liquorice, Ginseng, Black cohosh, Dong
qui, Hops and
Kelp.
SJIF Impact Factor 7.421
Volume 8, Issue 8, 515-546 Review Article ISSN 2278 – 4357
*Corresponding Author
Saptarshi Das
Assistant Professor,
Department of
Pharmaceutical Analysis,
Bharat Technology,
DOI: 10.20959/wjpps20198-14396
516
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
1. INTRODUCTION
Herbs can be described usually in trade as a plant, plant phase or
extract there of used for
flavor, or medicinal purposes. Traditional drugs are naturally
going on provisions with
minimal or no industrial dispensation that have been used to cure
various illnesses.
Traditional plant derived drug treatments are receiving broad
interest in world health. Plant
based drug has attached promotive, preventive, healing and
rehabilitative role. Herbal remedy
has grasped a rotating point. It is struggling to be diagnosed as a
science-a particular
discipline with its very own identity. [1]
It has grown to be necessary to exhibit that herbal
remedy can match other fields of medicinal drug in the integrity of
its scientific work and its
realistic use. Benefit of natural therapy compared to traditional
remedy is that natural therapy
is protected with lesser facet effects and presence of more than
one energetic compounds in
medicinal herbs altogether offers a potentiating effect. [2]
The ovary is the vital part of the
female reproductive organ which harvests the ovum. The word ovary
is native to the Latin
term ovarium meaning egg or nut. Ovaries produce and secretes
hormones which play a very
vital role in menstruation cycle, fertility throughout menopause.
The female gonads - ovaries
are white colored, situated along the lateral wall of the uterus
known as ovarian fossa. The
ovaries consist of three parts which are the capsule, outer cortex
and inner medulla. [3]
At the
age of puberty, the ovaries begin to secrete hormones in elevated
levels resulting in the
development of the secondary female characteristics and onset of
menstrual cycle. [4]
Therefore, the ability to produce ovum and reproduce is attained
with the onset of female
puberty. The principal function of the ovary is gamete production
called oogenesis which is
aided by its other functions of hormone secretion and ovarian
aging. In normal circumstances
the ovum is released from the follicle into the fallopian tube.
Unfortunately if the ovum is not
released, it may conduct to development of an ovarian cyst. Cluster
of cell aggregates
forming a pouch with a distinct membrane and division unlike
surrounding tissue is called as
cyst. Small cysts are common in healthy women. [5]
In certain cases, it has been found that
some women have more follicles than usual, which inhibits normal
follicular growth and
regular cycles. This is known as polycystic ovary syndrome (PCOS).
Polycystic ovarian
syndrome is a serious hormonal disorder. The word poly is derived
from Greek, means
many. [6]
Polycystic ovary syndrome (PCOS) is a multivariate disease of the
female
reproductive system, owing to a huge difficulty for clinicians and
researchers all around the
world. [7]
The PCOS morphology includes luteinized inner theca, non-maturating
and atretic
follicles, tiny follicular cyst, stromal abnormal hyperplasia,
thickening of ovarian cortex and
ovarian abnormal hyperplasia. These clinical indications infer
obstruction in oogenesis. [8]
The
517
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
etiology of PCOS hasn’t been completely resolved nevertheless it is
correlated with
hyperandrogenemia, hyperinsulinemia/insulin resistance, aberration
in luteinizing hormone to
follicle stimulating hormone ratio, metabolic and inflammatory
amiss, advance glycation end
products, unfold protein response and stress in endoplasmic
reticulum. [9-13]
Each female with
PCOS need to be treated as per their own requirements, symptoms or
other clinical
manifestations. Treatment strategies are made to increase the
quality of life and safeguard
continuing vitality and health. [14]
The pharmacological strategies to ameliorate PCOS often
include drugs such as metformin, orlistat, pioglitazone, vitamin D
and hormonal
contraceptives in combination with other therapeutic remedies.
[15-19]
A recent case control
study also found that the expression serum levels of microRNA-320
were lower in PCOS
patients as compared to the control and hence it could be a
noninvasive diagnostic biomarker
for PCOS. [20]
In this review it will be summarized possible herbal remedies for
polycystic
ovarian syndrome treatment. These are prevent ovarian cysts as well
as cure them. Herbal
products may take higher time to treat PCOS but daily usage may
cure the disorder from its
root. [21]
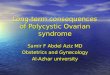
(a) Ovary (b) Ovarian Cyst (c) Polycystic Ovary
Fig.1: structure of (a) ovary (b) ovarian cyst (c) polycystic ovary
[22]
2. Symptoms of Pcos: Irregular ovulation is a general symptom of
PCOS. Several cysts
produce androgens. PCOS indicates the appearance of
‘hyper-androgenism’ symptoms such
as weight gain, facial and body hair, abdominal and subcutaneous
fat, enlargement of the
clitoris, hair loss, deep voice, oily skin, acne etc. Insulin
resistance is an important symptom
of PCOS. It results in hyper-insulinemia. Elevated insulin level is
blamable for the alteration
of fat around the abdomen or central adiposity. Other than above
symptoms hypertension,
cardiovascular issues, dyslipidemia, etc. are important symptoms of
PCOS. [23-25]
The PCOS
518
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
suffering patients often possess sugar cravings, fatigue, frequent
urination, delayed healing,
blurred vision, mood swing, tingling sensation, anxiety and
depression. Other symptom of
this disease is Sleep disorder in which breathing repeatedly stops
and starts. PCOS can put a
female at the risk for uterine cancer, as the prevailing elevated
level of estradiol and the lack
of progesterone due to ovarian malfunction enhance the chance of
endometrial
hyperplasia. [26]
Mucus lacking endocervix, and smooth vagina is an important
characteristic
of PCOS. Due to the endocrine system imbalance in PCOS, skin
develops light brown or
black patches, a condition known as ‘acanthosis nigricans’.
However, PCOS symptoms can
be deliberated as a spectrum. Hirsutism is mild or lacking in PCOS
suffering patients but
hirsutism more affect patients with origin of Middle Eastern and
Mediterranean. [27]
3. PATHOGENESIS OF PCOS
(a) Elevated level of androgens: Increased level of androgen
hormone is considered as the
main cause of PCOS. Under normal state, the ovaries and adrenal
glands are both contributed
about the production of testosterone. [28]
Half of testosterone is generally produced from direct
testosterone secretion, whereas another half is produced by
peripheral conversion of
circulating androstenedione. Androgen production is not produced
direct negative feedback
in females, recent research works are also described that elevated
level of androgen is also
produced the negative feedback with female sex hormone. [29]
Both the ovaries and adrenal
glands are secreted androgens in response to their tropic hormones
LH and ACTH
respectively. Ovarian theca cells synthesize C19 androgens are
synthesized by the influenced
of luteinizing hormone, and androgen. Then it is converted to
estradiol by aromatase enzyme
in granulosa cells. Increased androgen secretion is a principal
characteristic of polycystic
ovarian syndrome. [30-32]
present during pregnant state in affected women. [33]
www.wjpps.com Vol 8, Issue 8, 2019.
519
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
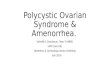
Fig. 2: Elevated level of androgen production during PCOS
[34]
(b) Ovulatory dysfunction: During ovarian follicular development,
primordial follicles are
recruited into a group of growing follicles, from which one antral
follicle is selected to
ovulate. These actions require coordinated three interaction viz
reproductive, metabolic and
intraovarian interactions. In PCOS, ovarian hyperandrogenism,
hyperinsulinemia from
insulin resistance and altered intra-ovarian paracrine signaling
can disrupt follicle growth. [35]
The consequent follicular arrest in PCOS is accompanied by
menstrual irregularity, an
ovulatory subfertility and the accumulation of small antral
follicles within the periphery of
the ovary, giving it a polycystic morphology. [36]
(c) Insulin resistance: a common feature of PCOS that arises in
part from adipose tissue
dysfunction, results in compensatory hyperinsulinemia, which
maintains normal glucose
levels but adversely effects ovarian androgen production.
[37-38]
Abnormal folliculogenesis and
the development of PCOS; these abnormalities may arise from
environmental insults as well
as genetic predisposition Hyperinsulinemia also amplifies
luteinizing hormone (LH)-
stimulated and insulin-like growth factor 1 (IGF-1)-stimulated
androgen production, elevates
serum free testosterone levels through decreased hepatic sex
hormone-binding globulin
production, and enhances serum IGF-1 bioactivity through suppressed
IGF-binding protein
production. [39]
follicle-stimulating hormone (FSH)-induced granulosa cell
differentiation, which arrests
www.wjpps.com Vol 8, Issue 8, 2019.
520
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
granulosa cell proliferation and subsequent follicle growth.
Finally, overproduction of anti-
Mullerian hormone (AMH) by the granulosa cells of ovarian follicles
in PCOS. [40]
(d) Obesity and adipose tissue dysfunction: In PCOS
Adiposity-dependent insulin
resistance is inextricably linked with PCOS. The molecular
mechanisms underlying insulin
resistance of PCOS remain elusive; however, primary defects in
insulin-mediated glucose
transport, GLUT4 production and insulin or adrenergic regulated
lipolysis in adipocytes,
despite normal insulin binding. These defects in insulin action
seem to represent perturbed
intracellular insulin signaling or action by paracrine, autocrine
and endocrine factors, with
abnormal insulin receptor auto phosphorylation or altered
phosphorylation of insulin-receptor
substrate, glycogen synthase kinase 3 or serine/threonine-protein
kinase AKT identified in
fibroblasts, adipocytes and myocytes of some women with PCOS.
[41]
In addition, insulin
resistance in PCOS might partially represent dysfunctional
adipogenesis from an impaired
capacity of regional adipose tissue stores to properly expand with
increased dietary caloric
intake. Adipose tissue secretes approximately 100 factors that
regulate metabolic function,
appetite, neural activity, digestion and inflammation; this tissue
is also heavily infiltrated by
macrophages, and crosstalk occurs between adipocytes, macrophages
and pluripotent cells
that induces complex paracrine interactions. [42]
(e) Gonadotropin abnormalities: LH hypersecretion rises serum
immunoactive and
bioactive LH levels in about 70% of women with PCOS, and increased
LH pulse amplitude
and frequency induces a twofold to threefold elevation in
circulating LH versus FSH levels.
58–60 Increased LH pulse frequency in PCOS, from increased
hypothalamic gonadotropin
releasing-hormone (GnRH) pulsatile release, occurs owing to reduced
steroid hormone
negative feedback on LH secretion because of androgen excess.
[43]
However, PCOS exhibit
reduced hypothalamic feedback inhibition from androgen excess is
not for all adolescent girls
with PCOS that may be because the availability of this defect
requires a genetic component
or depends on the duration of androgen excess. [44]
(f) Epigenetic changes: In fetal life are implicated in the
developmental origins of PCOS.
(g) Premature adrenarche: Some populations of girls with PCOS.
Moreover 30% of per
pubertal daughters of Chilean mothers with PCOS developed
exaggerated adrenarche
accompanied by higher serum. Obesity further influences the
adolescent PCOS phenotype by
unmasking or amplifying symptoms of hyperinsulinemia and
hyperandrogenism in
susceptible individuals.
Weight gain worsens metabolic and reproductive abnormalities of
PCOS, as evidenced by
www.wjpps.com Vol 8, Issue 8, 2019.
521
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
increased total and abdominal obesity as well as insulin
resistance, menstrual irregularity and
hyperandrogenism in women with the most severe PCOS. Endocrine
disrupting chemical that
is detectable in most individuals. [45]
Rodent studies show that BPA enhances ovarian
androgen production in vitro and induces insulin resistance in
vivo. BPA accumulates to an
increased level in women with PCOS owing to the decreased hepatic
clearance that arises
from androgen excess which has raised worry that BPA accumulation
in susceptible women
might exaggerate the severity of the PCOS phenotype. [46]
(i)Long-term morbidity Subfertility Anovulation: It is the
predominant cause of
subfertility in PCOS. In addition, a subgroup of women with PCOS
also exhibit impaired
oocyte developmental competence, or the ability of the oocyte to
complete meiosis and
undergo fertilization, embryogenesis and development to birth.
Obstetrical morbidity Women
with PCOS exhibit gestational androgen excess and hyperinsulinemia,
both of which may
adversely affect pregnancy outcome. [47]
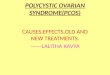
Fig. 3: Summery of pathogenesis of PCOS.
3. CURRENT SYNTHETIC DRUG FOR PCOS: The possible drug targets and
disease
genes are usually identified from the biological background of
PCOS. Previous researchers
were demonstrated differential pathways instead of differential
expressed genes, for
www.wjpps.com Vol 8, Issue 8, 2019.
522
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
analyzing the pathogenesis of PCOS and the way of drug response.
[48-50]
21 PCOS potential
drug targets were verified by various literatures to be associated
with the pathogenesis and
treatment of PCOS, which could reflect the status of disease and
drug response and 42 drugs
targeting to 13 PCOS potential drug targets were confirmed to be
investigated experimentally
or clinically for treating PCOS . One is insulin sensitization
agent such as Pioglitazone,
Rosiglitazone; the other is correcting the lipid metabolism
disorders agent such as
Repaginate, Telmisartan. [51]
4. HERBAL REMEDIES FOR PCOS
1. Liquorice: Liquorice is also known as yasti consists of dried,
unpeeled, roots and stolons
of Glycyrrhiza glabra, belonging to the family Leguminosae.
Traditionally liquorice has
medicinal imprtance as an expectorant and demulcent, anti-ulcer,
anti-spasmodic, anti-
bacterial, anti-fungal, anti- inflammatory and foam stabilizing
agent. [52]
Fig. 5: Liquorice.
523
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
Glycyrrhizic acid is the major biological active compounds in
liquorice. Liquiritigenin,
isoliquiritigenin, isoliquiritin, liquiritin, glabidin, and
glabrene are some of the
phytoestrogens present in liquorice. Somjen et al., described that,
glabridin, and glabrene
flavonoid which are obtained from liquorice root both established
estrogen-like activities that
the effects on vascular tissues in both in vitro and in vivo
[53]
Fig. 6: Structure of Glabridin and Glabrene.
Liquiritigenin a selective estrogen receptor compound might be one
of the biologically active
compound responsible for weight loss. It has been stated that the
combined treatment with
Liquorice and spironolactone in hirsute women is effective in PCOS,
in order to reduce the
volume depletion induced by spironolactone and possibly boost its
anti-androgenic activity. It
helps in proper production of hormones as well as their release
through endocrine system.
This herb balances estrogen levels, maintains healthy levels of
insulin and promotes liver
health. In addition, it boosts the immune system and reduces
inflammation and stress there by
relieving. The effect of Liquorice was explored on the pathway of
androgen metabolism in
the luteal phase of the cycle in nine healthy women of 22–26 years
old, They were
administered 3.5 g of a commercial preparation of licorice
(containing 7.6% W/W of
glycyrrhizic acid) daily for two cycles. They were not on any other
treatment. Plasma renin
activity, gonadal androgens and serum adrenal, aldosterone and
cortisol were measured by
radioimmunoassay (RIA). Total serum testosterone decreased
gradually within two months. It
returned to pretreatment levels after discontinuation. Licorice can
reduce serum testosterone
probably due to the block of 17hydroxysteroid dehydrogenase and
17–20 lyase. Licorice
could be considered an adjuvant therapy of hirsutism and polycystic
ovary syndrome. [54-59]
www.wjpps.com Vol 8, Issue 8, 2019.
524
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
(2) Spearmint Tea: It consists of dried leaves and flowering tops
of the plant known as
Mentha spicate, belonging to the family Labiatae. It is used as a
carminative and flavoring
agent.
In PCOS condition, obesity, insulin resistance and hyperglycemia
all correlate with a high
level of oxidative stress, inducing a hyper and ogenemic
environment in the ovary. [60]
Although locally produced androgens serve as substrate for estrogen
production in
folliculogenesis, an excessive level of androgens overrides
follicular development, resulting
in follicular atresia, disturbed follicular development and
anovulation. Elevated visceral
adiposity and hyperinsulinemia are observed in PCOS women,
resulting in increased
androgen production of the ovaries and adrenal gland. Reducing body
weight of an ovulatory
obese women decreases insulin resistance, testosterone
concentration and restores ovulation.
According to our results, spearmint oil decreases body weight in
the PCOS condition, and
since it has anti-androgenic potential, its administration leads to
decrease of androgen
production. Studies show that spearmint leaves decrease cholesterol
and, in type II diabetes,
decrease oxidative stress. Additionally, phenolic compounds of
spearmint leaf extract
significantly enhance the antioxidant defense system and reduce
body weight and levels of
glucose and cholesterol in diabetic male rats. Furthermore,
administration of spearmint
decreased the number of atretic follicles and ovarian cysts in
PCOS-induced rats, a
circumstance which is also associated with the antioxidant and
anti-androgenic effects of
spearmint oil. Moreover, the attenuated level of corpus lutea in
PCOS-induced rats increased
in PCOS rats that received spearmint oil, which reflects the higher
rate of ovulation in these
groups. Therefore, spearmint oil by reduction of weight and
testosterone and having
antioxidant potential can restore follicular maturation and induce
ovulation, which,
www.wjpps.com Vol 8, Issue 8, 2019.
525
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
respectively, was observed in the lower number of atretic follicles
and higher number of
Graafian follicles and corpus lutea in the PCOS-induced rats that
received spearmint oil. The
study was carried out in Turkey in a two centre as 30 day
randomized controlled trial. Forty
two volunteers were randomized to take spearmint tea twice a day
for a 1 month period and
compared with a placebo herbal tea. At 0, 15 and 30 days of the
study serum androgen
hormone levels and gonadotropin were checked; the degree of
hirsutism was clinically rated.
41 out of 42 patients completed the study. Free and total
testosterone levels and degree of
hirsutism were reduced over the 30 day period in the spearmint tea
group. LH and FSH were
increased. It was demonstrated and confirmed that spearmint has
anti-androgen properties. [61-
63]
www.wjpps.com Vol 8, Issue 8, 2019.
526
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
(3) Ginseng saponin: It strengthens the HPA axis and hence restores
hormonal balance. It
also boosts immune system and manages stress. It maintaines healthy
glucose levels in
women, which is crucial to fight PCOS. Female Sprague-Dawley rats
(190-210 g) were
induced polycystic ovary with injection of Estradiol Valerate (EV)
intramascular and
separated into three groups: EV control (n=10), EV plus Ginseng
Total Saponins (n=10), and
oil control (n=10). Parameter observed in this study include
Ovarian morphology and Nerve
Growth Factor (NGF) protein expression. Increased expression of
Nerve Growth Factor was
noted in the ovaries and the brain of rats with Poly Cystic Ovary.
Ginseng Total Saponins
administration diminished NGF expression in the ovaries. [60]
(4) Flaxseed: In this study the effect of flaxseed supplementation
(30 g/day) on hormonal
levels in a 31-year old woman with PCOS was observed. During a four
month period, the
patient administered orally 83% of the flaxseed dose. Height,
weight measurement and
fasting blood samples monitoring at baseline and 4-month follow-up
directed significant
decrease in Body Mass Index (BMI), total serum testosterone,
insulin and free serum
testosterone levels. The patient also reported a decrease in
hirsutism at the completion of the
study period. The clinically significant decrease in androgen
levels with a concomitant
reduction in hirsutism reported in this case study. [62]
(5) Aloe-vera: A. barbadensis Mill. Is one of the oldest known
medicinal plants gifted by
nature and is often called miracle plant or natural healer. It
belongs to liliaceae family which
includes about 250 species; however only two species, viz. A.
barbadensis Mill. and A.
arborescens Mill. Are considered as the most important ones. The
innermost part of A. Vera
leaf is a clear, soft moist and slippery tissue which contains
vital ingredients, viz.
polysaccharides, vitamins, minerals, amino acid, saponins,
anthraquinones etc. Most of the
health benefits associated with this plant have been attributed to
polysaccharides contained in
the mucilageous gel of leaves. In the present study, the efficacy
of Aloe vera gel formulation
in a PCOS rat model was checked. [63]
Five month old Charles Foster female rats were orally
fed with letrozole, a non-steroidal aromatase inhibitor, to induce
PCOS. The rats were then
treated orally with the Aloe vera gel formulation (1 ml dose daily
for 45 days). This restored
their estrus cyclicity, glucose sensitivity, and steroidogenic
activity. Co-treatment of the
inductive agent (letrozole) with the Aloe vera gel prevented the
development of the PCO
phenotype [64]
. Aloe vera gel formulation exerts a protective effect in against
the PCOS
phenotype by restoring the ovarian steroid status, and altering key
steroidogenic activity. This
can be attributed to phyto-components present in the extract.
[63]
www.wjpps.com Vol 8, Issue 8, 2019.
527
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
(6) Cinnamon: Cinnamon, which is a spice used to flavor foods, has
been possess anti-PCOS
and anti-diabetic properties. In a high-fructose diet induce
insulin resistance rat model,
cinnamon extract not only increase systemic insulin sensitivity and
dyslipidemia by
improving insulin signaling, but also effectively elevate
circulating levels of adipokines
partially mediated via regulation of the expression of multiple
genes involved in insulin
sensitivity and lipogenesis. [69]
Several in vitro and in vivo studies have shown cinnamon can
reduce insulin resistance by increasing activation of the IRS/PI-3
kinase insulin signaling
pathway. The extracts from cinnamon stimulate auto phosphorylation
of the insulin receptor
and inhibit protein tyrosine phosphatase I. Through these two
mechanisms cinnamon extract
make adipocytes to increase the glucose uptake and glycogen
synthesis. Oral cinnamon
extract reduced fasting glucose, triglycerides, low-density
lipoprotein (LDL), and total
cholesterol in patients with type 2 diabetes mellitus as well as
improved insulin sensitivity in
women with PCOS. Based on these findings, we put forward our
hypothesis that cinnamon
has an overall impact on PCOS treatment. Previous studies proved
dehydroepiandrosterone
(DHEA) induced PCOS model represents similar characteristic seen in
human patients, such
as hyperandrogenism, abnormal maturation of ovarian follicles and
anovulation. In this
experiment, we tried to gain a deeper understanding of the effect
and mechanism of
cinnamon on PCOS using a DHEA induced PCOS like mice model.
Cinnamon extract has
been shown to reduce insulin resistance in in vitro and in vivo
studies by increasing
phosphatidylinositol 3-kinase activity in the insulin signaling
pathway and thus potentiating
insulin action. Fifteen women with polycystic ovary syndrome (PCOS)
were randomized to
daily oral cinnamon and placebo for 8 weeks. Comparisons of
post-treatment to baseline
insulin sensitivity indices using fasting and 2-hour oral glucose
tolerance tests showed
significant reductions in insulin resistance in the cinnamon group
but not in the placebo
group. [70]
528
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
Fig. 9: Mechanism of Cinnamaldehyde in PCOS treatment.
(7) Chaste berry: Otherwise, it is also known as vitex. It is the
most singled out herb for
restoring normal menstrual cycle in women with PCOS. It regularizes
menstrual cycle by
balancing hormonal feedback loop and promoting ovulation. It also
regulates the pituitary
gland that has a normalizing effect on the menstrual cycle. It
initiates release of LH for
preparing ovulation. It also helps in the release of FSH that
stimulates the ovulation. In this
study, 93 women who had tried to conceive for 6-36 months were
given a supplement
containing chaste tree, L-arginine, vitamins and minerals. Their
progesterone level, menstrual
cycle length, pregnancy rate and side effects were documented.
After 3 months, the
supplementation group demonstrated increased mid-luteal
progesterone and normalized
menstrual cycles compared to no significant changes in the placebo
group. 14 out of the 53
women who received the supplement became pregnant as compared to 4
of the 40 women
who received placebo. 3 other women in the supplement group
conceived after 6 months. The
recommended dose is 1-4 ml of 1:2 dried plant tincture of 500-1000
mg of dried berries
daily. [71]
529
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
(8) White peony: The particular herb reduces chances of uterine
stagnation by promoting
circulation to female reproductive organ. It discards chances of
ovarian cysts. It also relieves
from pain during menstruation, especially when taken along with
licorice root. It also lowers
testerone level. In the present study, we investigated the in vivo
effects of unkei-to (Japanese
herbal medicine) and its compounds on the Steroidogenesis and
cytokine secretion in human
granulosa cells. Unkei-to stimulate the oozes of 17-betaestradiol
and progesterone from
highly luteinized granulosa cells obtained from in vitro
fertilization patients. Effect observed
due to its various ingredients herb like Paeoniae radix, Paeonia
lactiflora, Cinnamomi cortex
and Cinnamomum cassia. The various beneficial actions of unkei-to
on the ovary may result
from a combination of different ingredient herbs with different
stimulatory effects on both
steroidogenesis and the ovulatory process within the ovary, as well
as stimulatory effect on
the hypothalamus-pituitary axis. [62]
(9) Milk thistle: In this study, the effect of silymarin which is
known to have insulin
sensitivity effects on the levels of glucose, insulin,
testosterone, leutinizing hormone (LH)
and progesterone was tested. Ovulation rate and Homeostasis Model
Assessment of insulin
Resistance (HOMA) ratio were determined. A 3-months of treatment
were conducted in 60
PCOS patients in three well-matched groups. The first one (n=20),
received silymarin
(750mg/day). The second group received metformin (1500mg/day) while
the third group
treated by combination of metformin (1500mg/day) and silymarin
(750mg/day). All these
groups had taken the drugs in divided doses. The results showed
significant increment in
progesterone levels after completion of treatment. In conclusion
the addition of silymarin to
metformin in treatment of PCOS patients has improving effect on
disturbed hormones and
ovulation rate. [63]
(10) Kasip Fatimah: In this study, effect of a Malaysian herb Kasip
Fatimah had been
checked on 9 week old PCOS rats. PCOS was induced in female rats
before puberty by
treating continuously with dihydrotestosterone. The PCOS rats were
randomly subdivided
into two groups; PCOS herb treated and PCOS control. PCOS herb
treated rats received a
daily oral dose of (50mg/kg body weight), dissolved in 1 ml of
deionised water, for 4-5
weeks. PCOS controls received 1 ml of deionised water on the same
schedule. Result showed
reducing body weight gain in ovariectomized rats. Herb treatment
increases uterine weight,
indicating estrogenic effects and improves insulin sensitivity and
lipid profile in PCOS rats
without affecting body composition. [64]
(11) Chamomile: Thirty virgin adult cycling Wistar rats, weighting
200 - 220 g were divided
into two groups and housed every six mice into cage under standard
conditions (21 ± 2°C,
www.wjpps.com Vol 8, Issue 8, 2019.
530
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
12-hour light/ 12-hour dark cycles) for at least one week before
and throughout the study.
Estrous cyclicity of 30 virgin adult cycling rats was monitored by
vaginal smears obtained
between 0800 and 1200 hours. After about 4 days, each rat received
an i.m. injection of
Estradiol Valerate), 2 mg in 0.2 ml of corn oil, to induce PCO.
Corn oil was injected to the
rats in the control group. All the rats in the experimental group
were evaluated for follicular
cysts 60 days after the injection. Rats with PCOS were treated by
multiple doses (25, 50, 75
mg/kg) of intraperitoneal injections of Chamomile alcoholic-extract
for ten days. The
histological and hormonal results showed that Chamomile can
decrease the signs of PCOS in
the ovarian tissue and help LH secretion in rats. [65]
(12) Astragalus: In this study, 32 women with PCOS were
administered with combined
application of astragalus polysaccharides and diane-35 for 3
months. Sex hormones, insulin
sensitivity and blood lipid were evaluated before and after the
therapy. After the treatment,
fasting serum insulin levels, LH/FSH ratio was found be reduced and
insulin sensitivity index
increased significantly. Astragalus polysaccharides plus diane-35
can be effective in
improving insulin resistance, high androgen hormone status and
lipid metabolism in patients
with PCOS and it may be alternative for PCOS. [66]
(13) Curcuma longa (Turmeric): Curcumin is a water-insoluble, low
molecular weight,
polyphenolic curcuminoid derivative found in rhizomes of Indian
spice, Curcuma longa of
the family Zingiberaceae (turmeric). Turmeric is extensively used
as a food additive and
coloring agent in Asian cuisine and also in Indian herbal medicine.
Curcumin has been
reported to possess a wide variety of biological effects like
anti-inflammatory, antioxidant
hypoglycemic antihyperlipidemic activities and estrogenic effects.
A study was conducted in
30 female Albino Wistar rats, using Letrozole-aromatase inhibitor,
to induce Polycystic
Ovarian Syndrome. Its effect was comparable to that of Clomiphene
citrate, most widely used
treatment for ovulation induction in PCOS condition. Serum levels
of Progesterone and
Estradiol were decreased in PCOS induced group. Curcumin restored
the hormone and lipid
profile, antioxidant and glycemic status as well as ovarian
morphology in Letrozole induced
PCOS animals. Decreased progesterone levels are also indicative of
anovulation and
curcumin successfully restore the ovulation. The study suggests
that the effects may be
attributed to its multiple pharmacological activities like
estrogenic, antihyperlipidemic,
antioxidant and hypoglycemic effects which could be useful in
managing PCOS condition
and prevent ovarian cell dysfunction, ovulation and thereby
improving fertility. The studies
show that the effect of curcumin is similar to that of Clomiphene
citrate. [67]
www.wjpps.com Vol 8, Issue 8, 2019.
531
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
(14) Trigonella foenum-graecum (Fenugreek): Another recent study
investigated the
efficacy of a novel, fenugreek (Trigonella foenum-graecum of the
family Fabaceae) seed
extract in PCOS. Fenugreek is enriched in furostanolic saponins
(Furocyst), the trial was
conducted in female subjects suffering from PCOS over a period of
90 consecutive days.
Plasma glucose levels (fasting glucose), serum triglyceride and HDL
levels, total leukocyte
count and hemoglobin levels were also monitored at the beginning
and end of 90 days
treatment. 94% of patients responded positively to the treatment
and significant improvement
in menstrual cycle was also observed following Furocyst treatment
resulted in significant
reduction in both ovary volume and ovarian cyst. Also significant
increases in LH and FSH
were observed following Furocyst treatment. 12% of study population
got pregnant.
Approximately 46% of study population showed reduction in cyst
size, while 36% of subjects
showed complete dissolution of cyst. No significant adverse effects
were observed. [68]
(15) Cocus nucifera (Coconut): Soumya et al., reported the effect
of Cocus nucifera
(Arecaceae) flowers in reducing the major multiple symptoms of
letrozole-induced PCOD in
female rats. Antioxidant status (superoxide dismutase (SOD) and
glutathione reductase
(GSH)) of the uterus homogenate, lipid profile (total cholesterol
(TC), high density
lipoprotein (HDL), low density lipoprotein (LDL), and
triglycerideslevels moreover
increased uterine weight, indicating estrogenic effects of the
labsinia extract. Treatment with
labisia extract increased insulin sensitivity in PCOS rats without
influencing body weight. [69]
(16) Thuja occidentalis (White Cedar): Thuja occidentalis
(Cupressaceae) has been used in
folk medicine for the treatment of rheumatism, amenorrhea,
cystitis, and uterine carcinomas,
and as an abortifacient and contraceptive. Thujone found in the
essential oil was reported to
be responsible for the curative properties of T.occidentalis. A
recent study investigated the
activity potential of the essential oil and its major compound
thujone obtained from the leaves
of T. occidentalis using an in vivo letrozole-induced PCOS model.
The phytochemical
analysis identified the main constituents of the oil is terpene
ketones, α and β-thujone,
fenchone, and sabinene, as well as the diterpenes beyerene and
rimuene. The levels of serum
gonadotropins, steroids, blood lipid, leptin, and glucose and the
values of antioxidant
parameters were monitored in the study. The estradiol and
progesterone levels significantly
increased, while the LH and testosterone levels decreased in the T.
occidentalis- and α-
thujone-administered groups when compared to the control group. The
potential activity of T.
occidentalis in the treatment of PCOS may be related to its
hormone-regulating effect. The
study also reported that administration of T. occidentalis
essential oil and its active
component, α-thujone, did not cause osteoporosis development the
rats was measured by
www.wjpps.com Vol 8, Issue 8, 2019.
532
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
real-time quantitative PCR and immunohistochemistry. The positive
effect of the extract in
alleviates the PCOS related hyperandrogenism has been linked to the
ovarian expression of
FSHR and AQP-9. The phytochemicals of flavonoid glycosides might be
responsible for the
observed effects. [70]
(17) Atractylodes macrocephala (Atractylode): Atractylodes
macrocephala Koidz
(Compositae) is a tonic herb widely prescribed in most Asian
countries, and it has been
clinically used as the dominant herb in most of the Chinese
medicinal formula of treating
PCOS. The effect of Atractylodes macrocephala polar extracts in
alleviating
hyperandrogenism in PCOS rats was studied. Hyperandrogenic rat
model of PCOS induced
by testosterone propionate is used for the study The plasma levels
of total testosterone, sex
hormone binding globulin, androstenedione, luteinizing hormone
(LH), follicle stimulating
hormone (FSH), antimullerian hormone were measured by enzyme linked
polar extracts. The
extract lowers plasma testosterone and androstenedione levels in
PCOS. It also significantly
reduced LH and increased FSH levels. No adverse effects were found
on liver function. [71]
(18) Corylus avellana (Hazel nut): Corylus avellana L., Betulaceae,
is growing wild in
Europa, Western Asia and Northern Africa as large shrubs or small
trees about 3.5–4.5 m
high. One of the most important features of C.avellana is to have
the highest ratio of
unsaturated/saturated fattyacids. Demirel et al., reported the
activity of the hazelnut oil in the
treatment of polycystic ovarian syndrome in rats. Serum
follicle-stimulating hormone,
luteinizing hormone, estradiol, progesterone, testosterone, serum
lipid parameters, leptin and
glucose levels were evaluated. The phytosterol content of the oil
was determined by HPLC.
According to the phytochemical analysis, the main component of the
oil was detected as α-
tocopherol, tocopherol, squalene, β-sitosterol, campesterol and
stigmasterol. Serum
gonadotropin levels were determined using radioimmunoassay. After
the hazel nut oil
administration treatment group and the reference group exhibited
regular estrous cycles. It
has a favorable effect in controlling follicular cysts. High FSH
and LH levels levels were
found to be normal. The ethanolic extract of C. avellana seed
displayed remarkable
antioxidant activity in total antioxidant and radical scavenging
tests. C. avellana seed
regulating the gonadotropins, steroids and serum lipid parameters
and possess antioxidant
activity. The author suggested that phytosterols determined,
probably promoted the treatment
of PCOS by their antioxidant effect. The improvement in the blood
glucose and serum insulin
levels could be associated with the improvement in the serum FSH
and LH hormones. [72]
(19) Tribulus terrestris (Puncture vine): Tribulus terrestris,
(Zygophyllaceae) commonly
known as Puncture vine or Devil’s eyelashes plays an important role
in traditional medicine.
www.wjpps.com Vol 8, Issue 8, 2019.
533
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
This particular herb enhances the timing of menstrual cycle and
blocks menstrual
irregulation. In addition, it acts as a tonic for the reproductive
system of women and
nourishes the ovaries. This herb reduces ovarian cysts as well as
stimulates ovulation. In an
investigation done in rats with polycystic ovaries induced with
estradiol valerate, found that
Tribulus terrestris extract is effective in improvement of
ovulation in rats. The extract
treatment normalized estrous cyclicity and steroidal hormonal
levels and regularized ovarian
follicular growth. Many herbalists find tribulus is an effective,
overall female fertility tonic
and ovarian stimulant, making it an excellent choice for women with
polycystic ovary. [73]
(20) Gymnema sylvestre (Gymnema): Gymnema sylvestre
(Asclepiadaceae) is an herb which
is used in traditionally in Ayurvedic system of medicine. It has
various pharmacological
effects like anti-diabetic, hypoglycemic, and lipid lowering
effects. The active constituent of
gymnema is saponins, especially gymnemic acids. It is particularly
known for its amazing
potential of blocking sugar. It delays sugar absorption by blocking
the paths that sugar
traverses through during digestion process. It is regenerated the
pancreatic cells to enhance
insulin production in the absence of which normal ovulation is
badly affected. In addition,
gymnemic acid is reduced the lipid level and helped in weight loss.
Gymnema has potential
hypoglycemic activity in experimental models of diabetes. It
regulates the blood glucose
level. Conventional therapy focusing on metformin therapy for PCOS.
Therefore gymnema
can be used for the underlying factor of insulin resistance.
Gymnema is well indicated for
PCOS, due to its insulin modulating activity and the added benefits
of reducing the elevated
triglycerides associated with PCOS. [74]
www.wjpps.com Vol 8, Issue 8, 2019.
534
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
Fig. 10: Mechanism of Gymnemic acid in the prevention of
PCOS.
(21) Punica granatum (Pomegranate): Pomegranate (Punica granatum of
the family
Punicaceae) is one of the known fruit and has numerous medicinal
propertiesThe fruit
contains vitamins such as B2, C, B1, folic acid, pantothenic acid,
sugars, and organic acids.
The seed is reported to contain saturated and unsaturated fatty
acids. The effect of
pomegranate extract in the management of PCOS was performed in
adult rats using control
and PCOS group. The concentration of serum estrogen, free
testosterone and andrestandoin
hormone levels in experimental group was monitored. The study
suggests the beneficial
effect of pomegranate extract on hormonal imbalances of
polycysticovarian syndrome. The
phytosterols and phenolic compounds found in the extract have
positive effect in improving
the complications of PCOS. The study recommends that the
consumption of the extract
reduces complications associated with PCOS. [75]
www.wjpps.com Vol 8, Issue 8, 2019.
535
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
(22) Cimicifuga racemosa (Black cohash): Cimicifuga racemosa
(Ranunculaceae) is a well-
known medicinal plant for its estrogenic effects. This herb
comprises of hormonally active
compound that suppress LH secretion, which causes PCOS in
women.
Fig. 11: Black cohash.
A randomized controlled study was conducted in 50 women with PCOS.
Ovulation induction,
hormonal profile concentration and outcome of pregnancy rate were
studied. The Cimicifuga
racemosa extract treatment significantly reduces the LH level and
LH/FSH ratio. The reduced
LH level decreases the excessive androgen level associated with
PCOS, ultimately resulted in
better ovulation and implantation rates. Reduced LH increases the
sensitivity of ovarian
tissue to circulate FSH, which improves the follicular growth,
ovulation and implantation.
The study revealed that phytoestrogens present in cimicifuga
racemosa extract increases the
endometrial thicknesses, which improve the implantation rate and
pregnancy outcome. [76]
(23) Mimosa pudica (shy plant): Mimosa pudica Linn belongs to
family Mimosaceae is
used in folk medicine and traditional systems of medicine in
various disorders of female
reproductive system.
536
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
The effect of Mimosa pudica extract was evaluated by Letrozole
induced PCOS rat model.
The biomarkers of ovarian function, plasma testosterone, estrogen
and progesterone were
analyzed to determine the fluctuations in sex steroid levels in
PCOS induced rats. When
compared with control, the PCOS induced rats showed characteristic
ovary with high
incidence of ovarian cysts with a diminished granulosa layer,
significant number of atretic
follicles and absence of corpora lutea. Mimosa pudica significantly
reduced histopathological
changes in ovary and endocrinological and biochemical changes
induced by
hyperandrogenism. Thus Mimosa pudica was found to have a good
potential to be a very
good alternative therapy in the treatment of PCOS. [77]
(24) Symplocos racemosa (Lodh Tree): Symplocos racemosa Roxb. From
the family
Symplocaceae, is a widely used Ayurvedic remedy mainly for
gynecological disorders.
Fig. 13: Symplocos racemosa.
It is also known as Lodhra and is used in Indian System of Medicine
as single drug or in
multicomponent preparations. The anti-androgenic properties S.
racemosa in the treatment of
PCOS was investigated in letrozole induced rat model. Syplocus
racemosa treatment
excibited significant recovery of testosterone, estrogen,
progesterone levels and ovarian
tissues. Moreover it showed anti-androgenic effect and prevents
ovarian cell dysfunction in
PCOS and improved the fertility. [79]
(25) Withania sominifera and Tribulus Terrestnis ; WS and TT are
hot in the first and third
degree respectively suggesting that the drugs possess such a degree
of hotness which suits
induction of response in amenorrhea and infertility. On treatment,
the histopathological
changes reached up to the normal level, which clearly indicates
that the test combination
stimulates the ovarian function as cortex shows primary and
secondary follicles with
aggregation of granulosa cells. The result clearly demonstrated
that the test combination due
www.wjpps.com Vol 8, Issue 8, 2019.
537
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
to their hot temperament dissolves the cyst. Therefore, it can be
concluded that the test
combination normalizes the ovarian functions by alteration of
temperament of ovaries. TT
has already been reported for its effect in formation of corpus
luteum when administered to
immature rats for 21 days. Moreover TT has also been studied in a
very low dose (5 mg/kg
and 10 mg/kg) in alternative treatment of ovarian cysts induced by
estradiol valerate in
rat, which further justified the efficacy of the test
drugs.Amenorrhea is the prevalent feature
of the disease. The test combination has been described to possess
emmenaogogue properties
useful in improving the amenorrhea. Test drugs also have lenitive
and resolvent properties,
with these inherited properties may liquefy the viscous matter and
resolve the matter forming
cysts, thus correcting and normalizing the ovarian functions.
Therefore, the mechanism
proposed by the Unani physicians appears to be comprehensive and
very much in
commensuration of the modern approaches of treatment. On account of
the results and
discussion it can be concluded that the hydroalcoholic extract of
combination WS and TT
exhibited significant recovery of FSH, LH, estradiole, and
testosterone levels in serum. The
hydroalcoholic extract demonstrated significant antiandrogenic
effects by reducing increased
testosterone level and preventing ovarian dysfunction in rats. This
property of the test drugs
may be due to the presence of phytoestrogens in hydroalcoholic
extract of the test
combination. Further studies are required to explain the exact
mechanism of action of the test
drug combinations. [80]
5. DISCUSSION: We conducted this review to present confirmations on
the etiology of
PCOS and introduce plants that have been recently investigated for
their effects on this
disease in studies with human subjects and animal models. Most
studies investigated the
serum levels of sex hormones, hyperandrogenism, insulin resistance,
ovarian weight and
histopathology, ovulation, and the symptoms of PCOS before and
after the treatment. By
inducing polycystic ovary syndrome and then, treatment with
different extracts the blood
testosterone and LH levels were reduced and the blood progesterone
and FSH levels
increased. Also, histopathological changes indicated that there
were many types of
follicles in different stages of growth in the treatment groups,
including primary follicles,
antral, peri- antral, graafian, corpus luteum, and large oocytes.
Most of these studies
reported that the studied herbal extracts were effective in
treating PCOS and improved
the levels of sex hormones, insulin resistance, hyperandrogenism,
ovulation, and PCOS
symptoms. In these studies, testosterone propionate, estradiol
valerate, and letrozole
were used to induce PCOS. In estradiol valerate-induced PCOS,
widely used in studies,
www.wjpps.com Vol 8, Issue 8, 2019.
538
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
LH and testosterone increase and FSH decreases. Besides that,
letrozole, an aromatase
inhibitor, has been used to induce PCOS. Aromatase is a small
member of the
cytochrome p450 family that converts androstenedione to estro- gen
and testosterone to
estradiol. Hormone changes in such mod- els are associated with
increased levels of
testosterone and LH, and decreased levels of estrogen,
progesterone, and FSH that are in
agreement with PCOS-induced changes in different species. In women
with PCOS,
secretion rate and metabolism of androgens and estrogens are
impaired and androgens
levels increase. As a result, insulin resistance causes increase in
LH/FSH, and such
hormone changes at theca cell surface and granulosa cause increase
in the synthesis of
androgens and decrease in the synthesis of estradiol. Finally, the
maturation of follicles is
stopped and therefore ovulation is impaired. Currently, because
there is no definite and
ideal treatment for hormonal disorders and asso- ciated clinical
manifestations, and also
chemical drugs have several side effects, thereby alternative
treatment, especially
phytother- apy, can be considered instead of commercially available
drugs. Because
medicinal plants contain active compounds as well as has no major
adverse effects,
therefore, they have attracted much attention within recent years.
For example licorice,
raspberry, and soybean are some of these plants and contains large
amounts of certain
phytoestrogens such as biochanin A, daidzein, genistein, and
formononetin. The anti-
androgenic property of this plant causes decrease in androgens
levels in patients with
PCOS. A study demonstrated that raspberry fruit extract caused
decrease in testosterone
through inhibiting NF-kB pathway, and improved ovarian tissue
symptoms including the
number of developing follicles, granulosa layer thickness, and the
number of corpus
luteum through antioxidant and anti-inflammatory proper- ties.
Jelodar et al. reported
that the consumption of V. agnus- castus fruit extract could cause
increase in aromatase
activity, and decrease in testosterone through aromatizing
testosterone. Isoflavones-rich
diet can be the biochemical basis of preventive effects against
cancer. Other studies
indicated that genistein could inhibit 3b-HSD and 17b-HSD in the
testicular microsomes
of both human and mouse. It has been reported that isoflavonoids
due to having phenolic
ring preferably inhibit the activities of 3b- HSD and 17b-HSD. In
addition to inhibiting
steroid-synthesizing enzymes, genistein can be involved in LH
receptor’s binding to G-
protein, and affect adenylatecyclase activity if LH receptor does
not bind to the G-protein
and block steroidogenesis-stimulated production of LH. Oxidative
stress is considered a
pathological characteristic of PCOS, and in women with PCOS, total
antioxidant status
declines. Evidence indicates that the levels of ROS in ovarian
tissue increase in PCOS,
www.wjpps.com Vol 8, Issue 8, 2019.
539
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
causing imbalance between oxidant and antioxidant systems. Soybean
isoflavonoids
exert antioxidant effect because of containing aromatic ring and
genistein. P. dactylifera
pollen contains antioxidant compounds such as differ- ent vitamins
and minerals, e.g.
zinc and selenium, that cause regu- lation of the body’s
antioxidant balance in people
with PCOS . Many of the studied plants including Soybean,
Raspberry, A. vera, L. pumila,
C. nucifera, G. max, and G. glabra have anti-androgenic property
and certain plants such
as: P dactylifera, G. max, C. sinensis, M. piperita and T. vulgaris
have antioxidant
property that are effec- tive in treating PCOS through improving
the serum levels of sex
hormones and decreasing oxidative stress. In the light of the evi-
dence, different types of
phytoestrogens and antioxidant com- pounds found in medicinal
plants can improve
PCOS symptoms and therefore be effectively used to treat this
syndrome.
REFERENCES
1. Kelly, C. C., Lyall, H., Petrie, J. R., Gould, G. W., Connell,
J. M., & Sattar, N. Low grade
chronic inflammation in women with polycystic ovarian syndrome. The
Journal of
Clinical Endocrinology & Metabolism, 2001; 86(6):
2453-2455.
2. Gjönnaess, H. Polycystic ovarian syndrome treated by ovarian
electrocautery through the
laparoscope. Fertility and Sterility, 1984; 41(1): 20-25.
3. Franks, S. Polycystic ovary syndrome. New England Journal of
Medicine, 1995; 333(13):
853-861.
4. Azziz, R. Diagnosis of polycystic ovarian syndrome: the
Rotterdam criteria are
premature. The Journal of Clinical Endocrinology & Metabolism,
2006; 91(3): 781-785.
5. Dunaif, A., & Book, C. B. Insulin resistance in the
polycystic ovary syndrome.
In Clinical Research in Diabetes and Obesity. Humana Press, Totowa,
NJ., 1997; 249-
274.
6. Ehrmann, D. A. Polycystic ovary syndrome. New England Journal of
Medicine, 2005;
352(12): 1223-1236.
7. Glueck, C. J., Papanna, R., Wang, P., Goldenberg, N., &
Sieve-Smith, L. Incidence and
treatment of metabolic syndrome in newly referred women with
confirmed polycystic
ovarian syndrome. Metabolism, 2003; 52(7): 908-915.
8. Ciaraldi, T. P., el-Roeiy, A. L. B. E. R. T., Madar, Z. E. C. H.
A. R. I. A., Reichart, D. O.
N. N. A., Olefsky, J. M., & Yen, S. S. Cellular mechanisms of
insulin resistance in
polycystic ovarian syndrome. The Journal of Clinical Endocrinology
&
Metabolism, 1992; 75(2): 577-583.
540
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
9. Rosenfield, R. L., Barnes, R. B., Jose’F, C., & Lucky, A. W.
Dysregulation of
cytochrome P450c17α as the cause of polycystic ovarian syndrome.
Fertility and
sterility, 1990; 53(5): 785-791.
10. Sheehan, M. T. Polycystic ovarian syndrome: diagnosis and
management. Clinical
Medicine & Research, 2004; 2(1): 13-27.
11. Kitzinger, C., & Willmott, J. ‘The thief of womanhood’:
women's experience of
polycystic ovarian syndrome. Social science & medicine, 2002;
54(3): 349-361.
12. Lewy, V. D., Danadian, K., Witchel, S. F., & Arslanian, S.
Early metabolic abnormalities
in adolescent girls with polycystic ovarian syndrome. The Journal
of pediatrics, 2001;
138(1): 38-44.
13. Norman, R. J., Dewailly, D., Legro, R. S., & Hickey, T. E.
Polycystic ovary
syndrome. The Lancet, 2007; 370(9588): 685-697.
14. Mikola, M., Hiilesmaa, V., Halttunen, M., Suhonen, L., &
Tiitinen, A. Obstetric outcome
in women with polycystic ovarian syndrome. Human reproduction,
2001; 16(2): 226-229.
15. Mikola, M., Hiilesmaa, V., Halttunen, M., Suhonen, L., &
Tiitinen, A. Obstetric outcome
in women with polycystic ovarian syndrome. Human reproduction,
2001; 16(2): 226-229.
16. Franks, S. Diagnosis of polycystic ovarian syndrome: in defense
of the Rotterdam
criteria. The Journal of Clinical Endocrinology & Metabolism,
2006; 91(3): 786-789.
17. Dunaif, A., Segal, K. R., Futterweit, W., & Dobrjansky, A.
Profound peripheral insulin
resistance, independent of obesity, in polycystic ovary syndrome.
Diabetes, 1989; 38(9):
1165-1174.
18. Sir-Petermann, T., Maliqueo, M., Angel, B., Lara, H. E.,
Perez-Bravo, F., & Recabarren,
S. E. Maternal serum androgens in pregnant women with polycystic
ovarian syndrome:
possible implications in prenatal androgenization. Human
reproduction, 2002; 17(10):
2573-2579.
19. Norman, R. J., Masters, L., Milner, C. R., Wang, J. X., &
Davies, M. J. Relative risk of
conversion from normoglycaemia to impaired glucose tolerance or
non-insulin dependent
diabetes mellitus in polycystic ovarian syndrome. Human
reproduction, 2001; 16(9):
1995-1998.
20. Lunde, O., Magnus, P., Sandvik, L., & Høglo, S. Familial
clustering in the polycystic
ovarian syndrome. Gynecologic and obstetric investigation, 1989;
28(1): 23-30.
21. Zangeneh, F. Z., Minaee, B., Amirzargar, A., Ahangarpour, A.,
& Mousavizadeh, K.
Effects of chamomile extract on biochemical and clinical parameters
in a rat model of
polycystic ovary syndrome. Journal of reproduction &
infertility, 2010; 11(3): 169.
www.wjpps.com Vol 8, Issue 8, 2019.
541
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
22. Maharjan, R., Nagar, P. S., & Nampoothiri, L. Effect of
Aloe barbadensis Mill.
formulation on Letrozole induced polycystic ovarian syndrome rat
model. Journal of
Ayurveda and integrative medicine, 2010; 1(4): 273.
23. Ansari, R. M. Potential use of durian fruit (Durio zibenthinus
Linn) as an adjunct to treat
infertility in polycystic ovarian syndrome. Journal of integrative
medicine, 2016; 14(1):
22-28.
24. Jungbauer, A., & Medjakovic, S. Phytoestrogens and the
metabolic syndrome. The
Journal of steroid biochemistry and molecular biology, 2014; 139:
277-289.
25. Jalilian, N., Modarresi, M., Rezaie, M., Ghaderi, L., &
Bozorgmanesh, M.
Phytotherapeutic management of polycystic ovary syndrome: role of
aerial parts of wood
betony (Stachys lavandulifolia). Phytotherapy Research, 2013;
27(11): 1708-1713.
26. Jalilian, N., Modarresi, M., Rezaie, M., Ghaderi, L., &
Bozorgmanesh, M.
Phytotherapeutic management of polycystic ovary syndrome: role of
aerial parts of wood
betony (Stachys lavandulifolia). Phytotherapy Research, 2013;
27(11): 1708-1713.
27. Mahood, R. A. H. Effects of Pimpinella anisum oil extract on
some biochemical
parameters in mice experimentally induced for human polycystic
ovary syndrome. Jornal
of Biotechnology Research Center, 2012; 6(2): 67-73.
28. Jahan, S., Munir, F., Razak, S., Mehboob, A., Ain, Q. U.,
Ullah, H., & Almajwal, A.
Ameliorative effects of rutin against metabolic, biochemical and
hormonal disturbances
in polycystic ovary syndrome in rats. Journal of ovarian research,
2016; 9(1): 86.
29. Wu, C. H., Chen, M. J., Shieh, T. M., Wang, K. L., Wu, Y. T.,
Hsia, S. M., & Chiang, W.
Potential benefits of adlay on hyperandrogenism in human chorionic
gonadotropin-treated
theca cells and a rodent model of polycystic ovary syndrome.
journal of functional
foods, 2014; 11: 393-406.
30. Arentz, S., Abbott, J. A., Smith, C. A., & Bensoussan, A.
Herbal medicine for the
management of polycystic ovary syndrome (PCOS) and associated
oligo/amenorrhoea
and hyperandrogenism; a review of the laboratory evidence for
effects with corroborative
clinical findings. BMC complementary and alternative medicine,
2014; 14(1): 511.
31. Shah, K. N., & Patel, S. S. Phosphatidylinositide 3-kinase
inhibition: A new potential
target for the treatment of polycystic ovarian syndrome.
Pharmaceutical biology, 2016;
54(6): 975-983.
32. Borzoei, A., Rafraf, M., Niromanesh, S., Farzadi, L., Narimani,
F., & Doostan, F. Effects
of cinnamon supplementation on antioxidant status and serum lipids
in women with
www.wjpps.com Vol 8, Issue 8, 2019.
542
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
polycystic ovary syndrome. Journal of traditional and complementary
medicine, 2018;
8(1): 128-133.
33. Orostica, L., Astorga, I., Plaza-Parrochia, F., Vera, C.,
Garcia, V., Carvajal, R., & Vega,
M. Proinflammatory environment and role of TNF-α in endometrial
function of obese
women having polycystic ovarian syndrome. International Journal of
Obesity, 2016;
40(11): 1715.
34. Jahan, S., Abid, A., Khalid, S., Afsar, T., Shaheen, G.,
Almajwal, A., & Razak, S.
Therapeutic potentials of Quercetin in management of polycystic
ovarian syndrome using
Letrozole induced rat model: a histological and a biochemical
study. Journal of ovarian
research, 2018; 11(1): 26.
35. Jahan, S., Abid, A., Khalid, S., Afsar, T., Shaheen, G.,
Almajwal, A., & Razak, S.
Therapeutic potentials of Quercetin in management of polycystic
ovarian syndrome using
Letrozole induced rat model: a histological and a biochemical
study. Journal of ovarian
research, 2018; 11(1): 26.
36. Rezvan, N., Moini, A., Janani, L., Mohammad, K., Saedisomeolia,
A., Nourbakhsh, M.,
& Hosseinzadeh-Attar, M. J. Effects of quercetin on
adiponectin-mediated insulin
sensitivity in polycystic ovary syndrome: a randomized
placebo-controlled double-blind
clinical trial. Hormone and Metabolic Research, 2017; 49(02):
115-121.
37. Wang, Z., Zhai, D., Zhang, D., Bai, L., Yao, R., Yu, J., &
Yu, C. Quercetin decreases
insulin resistance in a polycystic ovary syndrome rat model by
improving inflammatory
microenvironment. Reproductive Sciences, 2017; 24(5):
682-690.
38. Oyelami, O. A., Yusuf, K. O., & Oyelami, A. O. The use of
kigelia africana in the
management of polycystic ovary syndrome (PCOS). Chinese Medicine,
2012; 3(01): 1.
39. Chan, C. C., Koo, M. W., Ng, E. H., Tang, O. S., Yeung, W. S.,
& Ho, P. C. Effects of
Chinese green tea on weight, and hormonal and biochemical profiles
in obese patients
with polycystic ovary syndrome—a randomized placebo-controlled
trial. Journal of the
Society for Gynecologic Investigation, 2006; 13(1): 63-68.
40. Chan, C. C., Koo, M. W., Ng, E. H., Tang, O. S., Yeung, W. S.,
& Ho, P. C. Effects of
Chinese green tea on weight, and hormonal and biochemical profiles
in obese patients
with polycystic ovary syndrome—a randomized placebo-controlled
trial. Journal of the
Society for Gynecologic Investigation, 2006; 13(1): 63-68.
41. Oh, J. S., Ahn, M. J., Han, C. J., Kim, H., Kwon, O., Chung, H.
W., & Chang, N.
Relationship between flavonoids intake and metabolic syndrome in
Korean women with
polycystic ovary syndrome. Journal of Nutrition and Health, 2014;
47(3): 176-185.
www.wjpps.com Vol 8, Issue 8, 2019.
543
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
42. Knight, D. C., & Eden, J. A. A review of the clinical
effects of phytoestrogens. Obstetrics
& Gynecology, 1996; 87(5): 897-904.
43. Reyes-Muñoz, E., Sathyapalan, T., Rossetti, P., Shah, M., Long,
M., Buscema, M., &
Vitale, S. G. Polycystic ovary syndrome: implication for drug
metabolism on assisted
reproductive techniques—a literature review. Advances in therapy,
2018; 35(11): 1805-
1815.
44. Peluso, I., Raguzzini, A., & Serafini, M. Effect of
flavonoids on circulating levels of
TNFα and IL6 in humans: A systematic review and metaanalysis.
Molecular nutrition
& food research, 2013; 57(5): 784-801.
45. Morris, J. B. Morphological and reproductive characterization
in hyacinth bean, Lablab
purpureus (L.) Sweet germplasm with clinically proven nutraceutical
and pharmaceutical
traits for use as a medicinal food. Journal of dietary supplements,
2009; 6(3): 263-279.
46. Saiyed, A., Jahan, N., Makbul, S. A. A., Ansari, M., Bano, H.,
& Habib, S. H. Effect of
combination of Withania somnifera Dunal and Tribulus terrestris
Linn on letrozole
induced polycystic ovarian syndrome in rats. Integrative medicine
research, 2016; 5(4):
293-300.
47. Sankhwar, P., & Jaiswar, S. P. Resident Perception of
Obstetrical Hospitalists as
Parturient Care Providers and Educators. Gynecol Reprod Health,
2018; 2(4): 1-7.
48. EbrahimiMamaghani, M., SaghafiAsl, M., Pirouzpanah, S., &
AsghariJafarabadi, M.
Effects of raw red onion consumption on metabolic features in
overweight or obese
women with polycystic ovary syndrome: A randomized controlled
clinical trial. Journal
of Obstetrics and Gynaecology Research, 2014; 40(4):
1067-1076.
49. Shayan, A., Masoumi, S. Z., Shobeiri, F., Tohidi, S., &
Khalili, A. Comparing the effects
of agnugol and metformin on oligomenorrhea in patients with
polycystic ovary syndrome:
A randomized clinical trial. Journal of clinical and diagnostic
research: JCDR, 2016;
10(12): QC13.
50. Armanini, D., Fiore, C., Mattarello, M. J., Bielenberg, J.,
& Palermo, M. History of the
endocrine effects of licorice. Experimental and clinical
endocrinology & diabetes, 2002;
110(06): 257-261.
51. Rajan, R. K., & Balaji, B. Soy isoflavones exert beneficial
effects on letrozole-induced rat
polycystic ovary syndrome (PCOS) model through
anti-androgenic
mechanism. Pharmaceutical biology, 2017; 55(1): 242-251.
52. Saleem, F., & Rizvi, S. W. New therapeutic approaches in
obesity and metabolic
syndrome associated with polycystic ovary syndrome. Cureus, 2017;
9(11).
www.wjpps.com Vol 8, Issue 8, 2019.
544
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
53. Melissa, P. S. W., Navaratnam, V., & Yin, C. Y.
Phytoestrogenic property of Labisia
pumila for use as an estrogen replacement therapy agent. African
Journal of
Biotechnology, 2012; 11(50): 11053-11056.
54. Armanini, D., Castello, R., Scaroni, C., Bonanni, G., Faccini,
G., Pellati, D., & Moghetti,
P. Treatment of polycystic ovary syndrome with spironolactone plus
licorice. European
Journal of Obstetrics & Gynecology and Reproductive Biology,
2007; 131(1): 61-67.
55. Armanini, D., Mattarello, M. J., Fiore, C., Bonanni, G.,
Scaroni, C., Sartorato, P., &
Palermo, M. Licorice reduces serum testosterone in healthy women.
Steroids, 2004;
69(11-12): 763-766.
56. Armanini, D., Mattarello, M. J., Fiore, C., Bonanni, G.,
Scaroni, C., Sartorato, P., &
Palermo, M. Licorice reduces serum testosterone in healthy women.
Steroids, 2004;
69(11-12): 763-766.
57. Armanini, D., Fiore, C., Mattarello, M. J., Bielenberg, J.,
& Palermo, M. History of the
endocrine effects of licorice. Experimental and clinical
endocrinology & diabetes, 2002;
110(06): 257-261.
58. Armanini, D., Fiore, C., Mattarello, M. J., Bielenberg, J.,
& Palermo, M. History of the
endocrine effects of licorice. Experimental and clinical
endocrinology & diabetes, 2002;
110(06): 257-261.
59. Goswami, P. K., Khale, A., & Ogale, S. Natural remedies for
polycystic ovarian
syndrome (PCOS): a review. International journal of pharmaceutical
and
phytopharmacological research, 2012; 1(6): 396-402.
60. Jungbauer, A., & Medjakovic, S. Phytoestrogens and the
metabolic syndrome. The
Journal of steroid biochemistry and molecular biology, 2014; 139:
277-289.
61. Stewart, P. M., Edwards, C. R. W., Shackleton, C. H. L., &
Beastall, G. H. 5 α-reductase
activity in polycystic ovary syndrome. The Lancet, 1990; 335(8687):
431-433.
62. Rodin, A., Thakkar, H., Taylor, N., & Clayton, R.
Hyperandrogenism in Polycystic Ovary
Syndrome--Evidence of Dysregulation of 11β-Hydroxysteroid
Dehydrogenase. New
England Journal of Medicine, 1994; 330(7): 460-465.
63. Liang, R. N., Liu, J., & Lu, J. Treatment of refractory
polycystic ovary syndrome by
bushen huoxue method combined with ultrasound-guided follicle
aspiration. Zhongguo
Zhong xi yi jie he za zhi Zhongguo Zhongxiyi jiehe zazhi= Chinese
journal of integrated
traditional and Western medicine, 2008; 28(4): 314-317.
64. Hart, R. Polycystic ovarian syndrome–prognosis and treatment
outcomes. Current
Opinion in Obstetrics and Gynecology, 2007; 19(6): 529-535.
www.wjpps.com Vol 8, Issue 8, 2019.
545
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
65. Dastagir, G., & Rizvi, M. A. Glycyrrhiza glabra
L.(Liquorice). Pakistan journal of
pharmaceutical sciences, 2016; 29(5).
66. Grant, P. Spearmint herbal tea has significant antiandrogen
effects in polycystic ovarian
syndrome. A randomized controlled trial. Phytotherapy Research: An
International
Journal Devoted to Pharmacological and Toxicological Evaluation of
Natural Product
Derivatives, 2010; 24(2): 186-188.
67. Akdoan, M., Tamer, M. N., Cüre, E., Cüre, M. C., Körolu, B. K.,
& Deliba, N. Effect
of spearmint (Mentha spicata Labiatae) teas on androgen levels in
women with
hirsutism. Phytotherapy Research: An International Journal Devoted
to Pharmacological
and Toxicological Evaluation of Natural Product Derivatives, 2007;
21(5): 444-447.
68. Toso, C., RubbiaBrandt, L., Negro, F., Morel, P., & Mentha,
G. Hepatocellular adenoma
and polycystic ovary syndrome. Liver international, 2003; 23(1):
35-37.
69. Arentz, S., Abbott, J. A., Smith, C. A., & Bensoussan, A.
Herbal medicine for the
management of polycystic ovary syndrome (PCOS) and associated
oligo/amenorrhoea
and hyperandrogenism; a review of the laboratory evidence for
effects with corroborative
clinical findings. BMC complementary and alternative medicine,
2014; 14(1): 511.
70. Mokaberinejad, R., Zafarghandi, N., Bioos, S., Dabaghian, F.
H., Naseri, M.,
Kamalinejad, M., & Hamiditabar, M. Mentha longifolia syrup in
secondary amenorrhea: a
double-blind, placebo-controlled, randomized trials. DARU Journal
of Pharmaceutical
Sciences, 2012; 20(1): 97.
71. Jadhav, M., Menon, S., & Shailajan, S. In vivo evaluation
of Mimosa pudica linn. In the
management of polycystic ovary using rat model, 2013.
72. Thakor, A. P., & Patel, A. J. Normalizing of estrous cycle
in polycystic ovary syndrome
(PCOS) induced rats with Tephrosia purpurea (Linn.) Pers. Journal
of Applied and
Natural Science, 2014; 6(1): 197-201.
73. Reddy, P. S., Begum, N., Mutha, S., & Bakshi, V. Beneficial
effect of Curcumin in
Letrozole induced polycystic ovary syndrome. Asian Pacific Journal
of
Reproduction, 2016; 5(2): 116-122.
74. Saiyed, A., Jahan, N., Makbul, S. A. A., Ansari, M., Bano, H.,
& Habib, S. H. Effect of
combination of Withania somnifera Dunal and Tribulus terrestris
Linn on letrozole
induced polycystic ovarian syndrome in rats. Integrative medicine
research, 2016; 5(4):
293-300.
546
Das et al. World Journal of Pharmacy and Pharmaceutical
Sciences
75. Kashmira, J. G., Mayuri, A. L., & Varsha, M. S. A
comprehensive review on ‘Mimosa
pudica’: A potential herbal panacea. Journal of Biologically Active
Products from
Nature, 2011; 1(5-6): 285-292.
76. Patel, M., & Prajapati, D. Concept of Polycystic Ovarian
Syndrome: Perspectives of
Ayurveda and Modern Science. International Journal of Pharmacognosy
and
Phytochemical Research, 2017; 9(10): 1363-1372.
77. Sawant, A., Patil, S., & Shah, S. Review on PCOD/PCOS &
its treatment in different
medicinal systems–allopathy, ayurveda, homeopathy. Sci Jurno, 2017;
1(1): 1-16.
78. Anbu, A. S., & Venkatachalam, P. Biological macromolecule
cross linked TPP–chitosan
complex: a novel nanohybrid for improved ovulatory activity against
PCOS treatment in
female rats. RSC Advances, 2016; 6(97): 94301-94313.
79. Seethalakshmi, G., Muthukumar, N. J., Kanakavalli, K.,
Parthiban, P., & Banumathi, V.
Toxicity study on Sanga Thiravagam for polycystic ovarian syndrome.
Int. J. Curr. Res.
Med. Sci., 2018; 4(1): 21-27.
80. Hywood, A. Phytotherapy for polycystic ovarian syndrome.
Australian Journal of Herbal
Medicine, 2012; 24(3): 81.