Embed Size (px)
Citation preview

Prevention of Pressure Ulcersin the Surgical PatientPATINA S. WALTON-GEER, RN-BC, MSN, CWCN, CFCN2.5
© AORN, Inc, 2009538 • AORN JOURNAL • MARCH 2009, VOL 89, NO 3
The development of pressure ul-cers (PUs) is of enormous con-cern in all health care settings. A
PU is any lesion (ie, localized area oftissue necrosis) caused by unrelievedpressure or pressure in combinationwith friction or shear that results indamage to the skin or underlying tis-sue.1,2 An ulcer often develops whensoft tissue is compressed between abony prominence and an external sur-face for a prolonged period.2-4
Pressure ulcers can occur any timebody tissue is compromised causing skinbreakdown. Monitoring and maintainingskin integrity is an essential componentof defining a patient’s health status andevaluating the quality of nursing care.5 Itis incumbent upon all health care provi -ders to work not only to decrease the in-cidence of PUs, but also to effectively
treat them when they occur. The Institutefor Healthcare Improvement has initiatedinterventions to help hospitals reducePUs through the use of evidence-basedpractices to improve patient care.6
According to Graves et al, any patientaffected by PU development will requirea longer hospital stay.7 Brown’s researchindicates that there is a link betweenhospital-acquired PUs and mortality.8
Reddy et al estimate that approximately60,000 patients will die each year fromhospital-acquired pressure ulcers andthat the cost of treating these wounds isapproximately $11 billion per year.9
The Centers for Medicare and Medi-caid Services will no longer reimbursehealth care facilities if a health care-associated PU develops or is not docu-mented as present on the patient’s ad-mission to the facility.10 Placing financialresponsibility for PU development onthe health care facility should intensifythe focus on reducing PU incidence.
It is important to look at all areaswithin health care to decrease the possi-bilities of PU development wheneverpossible. There are many times duringwhich patients are put at increased riskfor developing PUs, including duringsurgery. Literature reviews reveal thatPUs are discussed predominantly in re-gard to long-term care, intensive care,
Pressure ulcers (PUs) are a serious health careproblem, and it is crucial to assess how patientsacquire pressure ulcers after admission to ahealth care facility. In the OR, factors related to po-sitioning, anesthesia, and the duration of surgery,in addition to patient-related factors, all can affectPU development.
This article reviews current practices, includingAORN recommended practices, regarding pres-sure ulcer prevention efforts for surgical patients.
All surgical patients should be considered at-riskfor pressure ulcer development; therefore, perioper-ative departments should develop and implementstrategic plans for pressure ulcer prevention.
Key words: pressure ulcer, health care-acquired con-ditions, surgical patients, wound prevention. AORNJ 89 (March 2009) 538-548. © AORN, Inc, 2009.
ABSTRACT
indicates that continuing education contacthours are available for this activity. Earn the con-tact hours by reading this article and taking theexamination on pages 549–550 and then com-pleting the answer sheet and learner evaluationon pages 551–552. The contact hours for this ar-ticle expire March 31, 2012.
You also may access this article online athttp://www.aornjournal.org.
p538-552_03_09:Layout 1 2/11/2009 3:35 PM Page 538

Walton-Geer MARCH 2009, VOL 89, NO 3
AORN JOURNAL • 539
and rehabilitation settings however, with littlefocus on acute care settings including the surgi-cal environment.7,11-14 Even though a largeamount of information is available to educatehealth care providers and help them imple-ment policies, procedures, protocols, and nurs-ing care plans to decrease the number of healthcare-associated ulcers, the incidence of PUscontinues to climb.3,7,12 This article reviews thecauses of and risk factors for PUs and intraop-erative methods for pressure redistribution andprevention of ulcers that could occur duringsurgical procedures.
ETIOLOGY OF PRESSURE ULCERSAn intraoperatively acquired PU may resem-
ble, and is often documented as, a burn. Ac-cording to AORN’s “Recommended practicesfor positioning the patient in the perioperativesetting,” an intraoperatively acquired PU usual-ly develops outward on the muscle of a bonyprominence and has a purplish discoloration.15
Depending on the patient’s skin color, a purpleor maroon localized area of discolored intactskin or blood-filled blister occurs as a result ofdamage to underlying soft tissue.2,4,16 Accordingto the National Pressure Ulcer Advisory Panel(NPUAP) and the Wound, Ostomy, and Conti-nence Nurses Society (WOCN), PUs develop
based on three causes: pressure, extrinsic fac-tors, and intrinsic factors.2,4
PRESSURE. Pressure can be defined by its inten-sity and its duration. Pressure ulcers are causedby compression of soft tissue between a bonyprominence and an external surface such as abed or chair. When the external pressure exceedsnormal capillary filling pressure of approximate-ly 32 mmHg, local blood flow is occluded, caus-ing tissue ischemia and subsequent necrosis ofskin and subcutaneous tissues. Muscle is moresensitive to pressure than skin; underlying tis-sue may become necrotic by the time a lesionpresents on the skin surface.3,17
Tissue breakdown occurs in stages (Table 1).Tissue damage may become apparent withinseveral hours after surgery or may not appearfor up to three days. Therefore, a PU that resultsfrom surgery may not be noticed until the pa-tient’s recovery period.3,18 An inverse relation-ship may exist between the duration and inten-sity of pressure. Low-intensity pressure over along period can initiate the tissue breakdownprocess, as can high-intensity pressure for ashort period of time.3,17
Tissue tolerance is the condition or integrityof the skin and supporting structures that in-fluences the skin’s ability to tolerate pressure.3
Pressure risk factors for skin damage include
TABLE 1Stages of Tissue Breakdown1,2
Type of injury Length of pressure ResolutionHyperemia Occurs when pressure is applied for Resolves within 1 hour
less than 30 minutes
Ischemia Occurs after 2 to 6 hours of unrelieved May require up to 36 hourspressure to resolve
Necrosis Develops after 6 hours of unrelieved May require a vascular surgeonpressure with microvasculature and/or wound care team consultcollapse and thrombosis
Ulceration Occurs within 2 weeks of necrosis May require a vascular surgeon and/or wound care team consult
1. Pressure ulcers. Landon Center on Aging. http://www2.kumc.edu/coa/Education/AMED900/PressureUlc.htm. Accessed December 28, 2008.2. Pieper B. Mechanical forces: pressure, shear, and friction. In: Bryant R, Nix D, eds. Acute & ChronicWounds: Current Management Concepts. 3rd ed. St Louis, MO: Mosby Elsevier; 2007:205-234.
p538-552_03_09:Layout 1 2/11/2009 3:35 PM Page 539

MARCH 2009, VOL 89, NO 3 Walton-Geer
540 • AORN JOURNAL
immobility, sensory deficit, mental statuschanges, and “bottoming out.”2,19 Immobility isthe limitation of the patient’s ability to reposi-tion. Sensory defi cit is the patient’s limited abili-ty to sense the need to reposition. This could becaused by neuropathies, spinal cord lesions,stroke, coma, or chemical restraints. Mental andcognitive changes may prevent pressure sensi-tivity. Patients may not be able to move prompt-ly or may be too confused to follow commonmovement patterns. Bates-Jensen defines bot-toming out as when the pressure-relieving de-vice no longer prevents direct pressure on thesurface from which the patient needs to be pro-tected.19 This can be evaluated by sliding a handbetween the pressure-redistribution device andthe prominence exposed to the pressure.19
EXTRINSIC FACTORS. Extrinsic factors include shear,friction, and moisture. Shear is defined as theapplied force that can cause an opposite, parallelsliding motion in the planes of an object. Shearis affected by the amount of pressure that is ex-erted.3,16 This tends to occur in larger occludedareas of vascular supply. An example is pullingskin in one direction and the bone in another.Friction is defined as a superficial, mechanicalforce directed against the epidermis, resulting inincreased susceptibility to ulceration.3 For exam-ple, this can occur when a patient is draggedacross a sheet during repositioning or when apatient self-repositions. Another extrinsic factoroccurs when the layer of skin (eg, stratumcorneum) becomes overhydrated, causing weak-ness of the collagen or elasticity of the skin. Thisleads to maceration of the skin, resulting in tis-sue damage. All of these extrinsic factors cancause tissue damage, especially in older adultpatients, patients with spastic movements, andpatients who use braces or appliances that canrub against the skin.
INTRINSIC FACTORS. Many patients undergoingsurgery, especially older adults, have numer-ous risk factors that can result in PUs. Intrin-sic risk factors causing skin damage affect theability of the skin and supporting structuresto respond to pressure and shear forces. In-trinsic factors include advanced age, anaero-bic waste products, nutritional deficiencies,and steroid administration that affect collagensynthesis and degradation. Other factors that
affect tissue perfusion include• certain medications (eg, steroids, vasoactive
medications);3,20
• presence of comorbid diseases (eg, cancer,cardiovascular and peripheral vascular de-ficiencies, diabetes mellitus, neurological orrespiratory disease);3,20
• extracorporeal circulation;21
• impaired regulation in body temperature;3,20
• fractures;3
• low hemoglobin and hematocrit levels;3,20
• nutritional deficiencies;3,11
• obesity;22
• low serum protein (ie, prealbumin or totalalbumin plus globulin);3
• smoking;3,20 and• low systemic blood pressure.3,20
POSITIONINGPositioning is a crucial component of surgi-
cal care. Positioning for a surgical proceduredepends on the surgeon’s preference, theanesthesia care provider’s needs, the proce-dure being performed, the need for exposureof the surgical site, and the patient’s predis-posing conditions.5,15,23
Positioning is recognized as a balance be-tween the position a patient can physically assume and those that are physiologically toler-ated. A patient’s body must be positioned ade-quately on an OR bed and proper body align -ment must be maintained to lessen the potentialrisk of skin injuries. Factors to be taken into ac-count during the preoperative interview beforesedation and positioning occur include • preexisting conditions;24
• decreased ranges of motion;24
• previous surgical procedures;24
• presence of joint prostheses;24
• fractures;24 and• the patient’s age, height, and weight.23,24
A surgical patient should be positioned prop-erly during the intraoperative phase of surgeryto lessen possible injuries. Physiological injuriesthat are short-term (ie, resolving in 24 to 48hours) or long-term can occur during surgery.Some injuries are modifiable and others are not.25
The incidence of modifiable injuries can be de-creased by proper positioning during surgery tolessen the probability of adverse physiological
p538-552_03_09:Layout 1 2/11/2009 3:35 PM Page 540
Walton-Geer MARCH 2009, VOL 89, NO 3
AORN JOURNAL • 541
responses, while providing access to the surgicalsite, the patient’s airway, IV sites, and monitoringdevices.23,24 Maintaining optimal physiologicalconditions lessens the risk for complicationsboth intraoperatively and postoperatively.
When a patient has inadequate arterial bloodflow, improper positioning can cause complica-tions with blood pressure, decrease tissue perfu-sion and venous return, and cause thrombusformation. The patient’s skin is at increased riskof tissue damage when the patient’s bodyweight is not distributed evenly on the OR bedor if poor tissue perfusion is present.23,24
Safety is the primary concern when determin-ing a patient’s position for a procedure. Thenumber of personnel and devices must be ade-
quate to safely transfer or position the patientpreoperatively or intraoperatively. Transferringis accomplished with a lateral transfer device(eg, slide boards, air-assisted transfer devices)that reduces friction and shear. Perioperativeteam members should place proper paddingaround the patient’s body to help prevent skinbreakdown, especially on high-risk areas, de-pending on the position (Tables 2, 3, 4, 5, and 6).
Pressure-relieving devices should be used todecrease possible ischemic changes as a resultof pressure when a patient must remain in a po-sition for several hours. Rolled sheets and tow-els are not to be used beneath overlays. This de-creases the effectiveness of the overlay andcauses pressure. It is important to monitor the
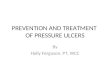
TABLE 2Common Surgical Positions—Supine1
Applicable VulnerableDescription procedures anatomy• Patient lies on back with face toward the
ceiling.• Ankles are uncrossed.• Arms are padded at sides in neutral position or
on padded arm boards at less than a 90-degreeangle with palms up.
• Head and upper body are in alignment withhips.
• Legs are parallel.• If patient is pregnant, a wedge should be
placed under patient’s right side to shift theuterus to the left and relieve compression onthe aorta and vena cava.
• Anterior chest (eg, open heart)
• Abdomen• Pelvis• Face, neck, and
mouth• Extremities
• Occiput• Scapulae• Arms• Elbows• Thoracic vertebrae• Lumbar area• Sacrum and coccyx• Heels
ScapulaeOcciput Arms and
elbows
Thoracicvertebrae
Lumbararea
Sacrum andcoccyx
Heels
1. Recommended practices for positioning the patientin the perioperative setting. In: Perioperative Stan-dards and Recommended Practices. Denver, CO:AORN, Inc; 2008:497-520.
Kurt Jones
p538-552_03_09:Layout 1 2/11/2009 3:36 PM Page 541
MARCH 2009, VOL 89, NO 3 Walton-Geer
quantity of pads, blankets, and warming blan-kets placed on top of or beneath a patient. Useof too many pads or blankets can cause the cap-illary pressure to rise over 32 mmHg, which in-creases the risk for poor tissue perfusion at thatarea of pressure, causing the patient to be at riskfor PU development.15
Patients should be repositioned during sur-gery if they are at high risk for skin break-down. For example, a patient in the lithotomyposition may have to be repositioned afterprolonged surgery. AORN’s “Recommendedpractices for positioning the patient in the pe-rioperative setting” suggests that a patientshould be repositioned every two hours toprevent continuous pressure on pressure
points and assist in decreasing the risk of ad-verse physiological responses.15
ANESTHESIATogether, positioning and anesthesia put the
patient in a compromised state. Anesthesia af-fects how the patient is positioned. It alsoblocks a patient’s sensitivity to pain and pres-sure, causing tissue damage vulnerability. Allagents used in anesthesia can depress the auto-nomic nervous system, causing some degree ofvasodilatation that is reflected in a lowering ofblood pressure that causes a decrease in tissueperfusion. The compounded effect of anesthesiaand the cold OR bed causes decreased perfu-sion.23,24 According to a study performed by
542 • AORN JOURNAL
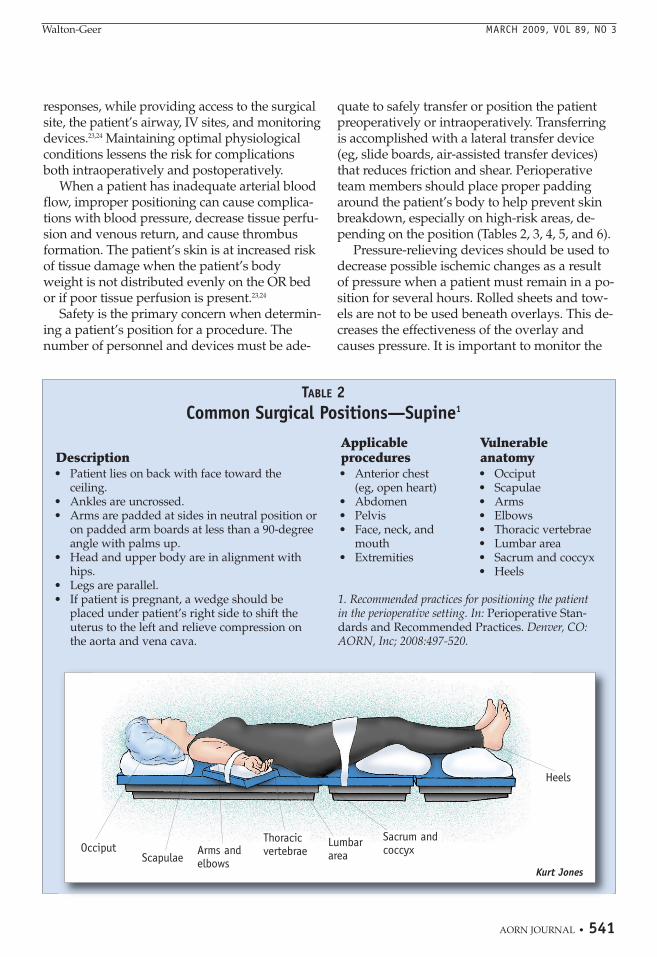
TABLE 3Common Surgical Positions—Prone1
Applicable VulnerableDescription procedures anatomy• Begins in the supine position.• After induction of anesthesia, patient is log-rolled
into the prone position (ie, face down).• Patient may be placed on a positioning device.• Head is placed on a padded headrest.• Head and cervical alignment is maintained.• Arms are at the patient’s sides or on padded arm
boards at less than a 90-degree angle.• Chest rolls may be used to accommodate chest
movement and lower abdominal pressure.• Protection is provided for patient’s forehead, eyes,
chin, breasts, genitalia, knees, and shins.• Toes are allowed to extend over the end of the bed or
are raised off the bed with padding under the shins.
• Back and spine• Posterior legs
• Forehead, eyes,ears, and chin
• Anterior shoulders• Breasts• Iliac crests• Genitalia• Knees• Shins• Dorsum of the feet• Toes
Forehead,eyes, ears,chin
Anterior shoulders
Breasts(women)
Genitalia(men)
Knees
Iliaccrests Shins
Toes
Dorsum ofthe feet
Kurt Jones
1. Recommended practices for positioning the patientin the perioperative setting. In: Perioperative Stan-dards and Recommended Practices. Denver, CO:AORN, Inc; 2008:497-520.
p538-552_03_09:Layout 1 2/11/2009 3:36 PM Page 542
Walton-Geer MARCH 2009, VOL 89, NO 3
AORN JOURNAL • 543
Lindgren et al,26 patients having epidural orspinal anesthesia were more likely to developpressure ulcers than patients having generalanesthesia. Other contributing factors in thestudy were low body mass, poor nutritional sta-tus, low albumin levels, and decreased bloodpressure. Changing the position of a patient un-dergoing anesthesia, regardless of what vasoac-tive medications are used, can decrease bloodpressure, putting skin integrity at risk.
SURGERY DURATIONMost tissue can only withstand excessive
pressure for brief periods. Prolonged exposureto pressure can initiate events resulting in tissueischemia, which may lead to tissue anoxia and
necrosis. In acute and chronic settings, it is sug-gested that patients who are immobile beturned at least every two hours.3,15,18 The dura-tion of the surgical procedure is a significant in-dicator in the risk of tissue damage. Reposition-ing a surgical patient, except for the heels, arms,and head, is rarely possible intraoperatively.14
O’Connell24 demonstrated that procedures last-ing longer than four hours triple the risk of tis-sue damage. Even the healthiest patient can beat risk for tissue damage if a surgical procedurelasts longer than four hours.
Length of a surgical procedure is not al-ways the primary predictor of PU develop-ment. Other factors could complicate or influ-ence the course of the procedure, resulting in
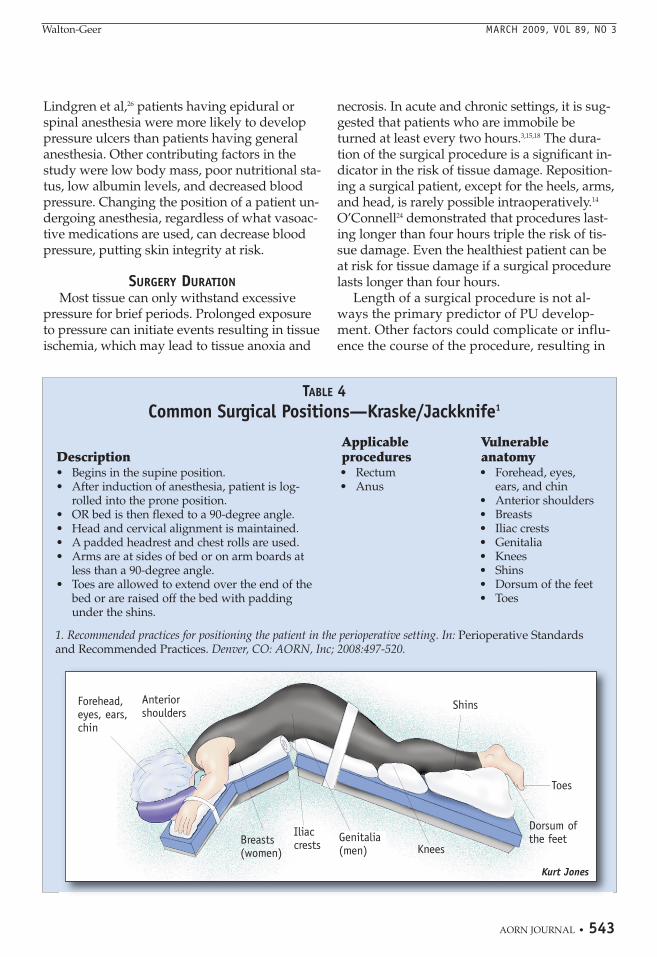
TABLE 4Common Surgical Positions—Kraske/Jackknife1
Applicable VulnerableDescription procedures anatomy• Begins in the supine position.• After induction of anesthesia, patient is log-
rolled into the prone position. • OR bed is then flexed to a 90-degree angle.• Head and cervical alignment is maintained.• A padded headrest and chest rolls are used.• Arms are at sides of bed or on arm boards at
less than a 90-degree angle.• Toes are allowed to extend over the end of the
bed or are raised off the bed with paddingunder the shins.
• Rectum• Anus
• Forehead, eyes,ears, and chin
• Anterior shoulders• Breasts• Iliac crests• Genitalia• Knees• Shins• Dorsum of the feet• Toes
Forehead,eyes, ears,chin
Anteriorshoulders
Breasts(women)
Iliaccrests
Genitalia(men) Knees
Shins
Dorsum ofthe feet
Toes
Kurt Jones
1. Recommended practices for positioning the patient in the perioperative setting. In: Perioperative Standardsand Recommended Practices. Denver, CO: AORN, Inc; 2008:497-520.
p538-552_03_09:Layout 1 2/11/2009 3:36 PM Page 543

MARCH 2009, VOL 89, NO 3 Walton-Geer
544 • AORN JOURNAL
longer time spent on the OR bed. Periopera-tive nurses and surgeons must address immo-bility if the patient will remain in one positionfor several hours.
VULNERABLE SURGICAL PATIENTSPatients who are 65 years of age or older
experience the highest incidence of PU devel-opment. The incidence of PUs in surgical pa-tients can be as high as 45%.2,3 In older adultpatients, there is a greater incidence of preop-erative variables (ie, extrinsic and intrinsic fac-tors) occurring that result in physiologicalchanges to the skin and ultimately, PU devel-opment.2,3 During the intraoperative phase ofsurgery, which includes the time on the OR
bed, hypotension and the type of procedureincrease the patient’s susceptibility to PU de-velopment.3,18 The skin of the older adult ismost likely to sustain tissue injury because itis less elastic with a thinner dermis and hasless collagen, muscle, and adipose tissue.These characteristics make older patients notjust susceptible to pressure problems with theskin, but also to increased bruising, skin tears,infection, impaired thermoregulation, andslow healing.24
SURGICAL PRESSURE REDISTRIBUTIONRather than focusing on pressure reduction
and pressure relief, support surfaces redistrib-ute pressure.16 These devices are designed to
TABLE 5Common Surgical Positions—Lithotomy1
Applicable VulnerableDescription procedures anatomy• Patient begins in the supine position then legs
are slowly and simultaneously raised andplaced in stirrups or leg holders that are at aneven height. Legs are not in contact with thestirrup posts.
• Patient’s buttocks are at the break in the proce-dure bed.
• Arms are on arm boards at less than a 90-degreeangle with thepalms up. Armsare tucked at sidesonly if this is sur-gically necessary.
• Heels are in thelowest possibleposition.
• After surgery, thepatient’s legsare lowered slowly and simultaneously.
• Obstetrics and gynecological procedures
• Genitourinary procedures
• Occiput• Shoulders• Scapulae• Hips• Sacrum/coccyx• Lateral aspect of
the legs• Heels
Shoulders andscapulae
Occiput
Sacrum andcoccyx
Lateralaspect ofthe legs
Heels
HipsKurt Jones
1. Recommended practicesfor positioning the patientin the perioperative set-ting. In: PerioperativeStandards and Recom-mended Practices.Denver, CO: AORN, Inc;2008:497-520.
p538-552_03_09:Layout 1 2/11/2009 3:36 PM Page 544
Walton-Geer MARCH 2009, VOL 89, NO 3
AORN JOURNAL • 545
prevent PUs or to promote reduction of inter-face tissue pressure.
Several types of pressure redistribution sup-port surfaces are available. One type is an over-lay, which is placed directly on the mattress oron the bed frame as a replacement for the stan-dard foam OR mattress. Foam, static air, gel, anddynamic air are common types of overlays, andall are latex free. Foam overlays are available ina variety of sizes, depths, densities, and con-struction. Static-air overlays allow air to ex-change through multiple chambers when a pa-tient lies on the overlay. This type of overlaymust be reinflated periodically.
Gel overlays (ie, visco-elastic polymer) pre-vent shearing, support weight, and prevent
bottoming out. If punctured, gel overlays arecapable of self-repair. One study found thatgel overlays helped to prevent both skinchanges and PU development in the olderadult population, including those with chron-ic health comorbidities or vascular diseaseand those experiencing extended surgicaltimes (ie, longer than two hours).27
Dynamic-air overlays have a mechanicalpump alternating inflation and deflation.These types of overlays include alternatingpressure mattresses, low-air-loss beds, and air-fluidized mattresses. Alternating-pressure mat-tresses produce alternating high and low pres-sures between the patient and the mattresswith diminishing periods of high pressure.
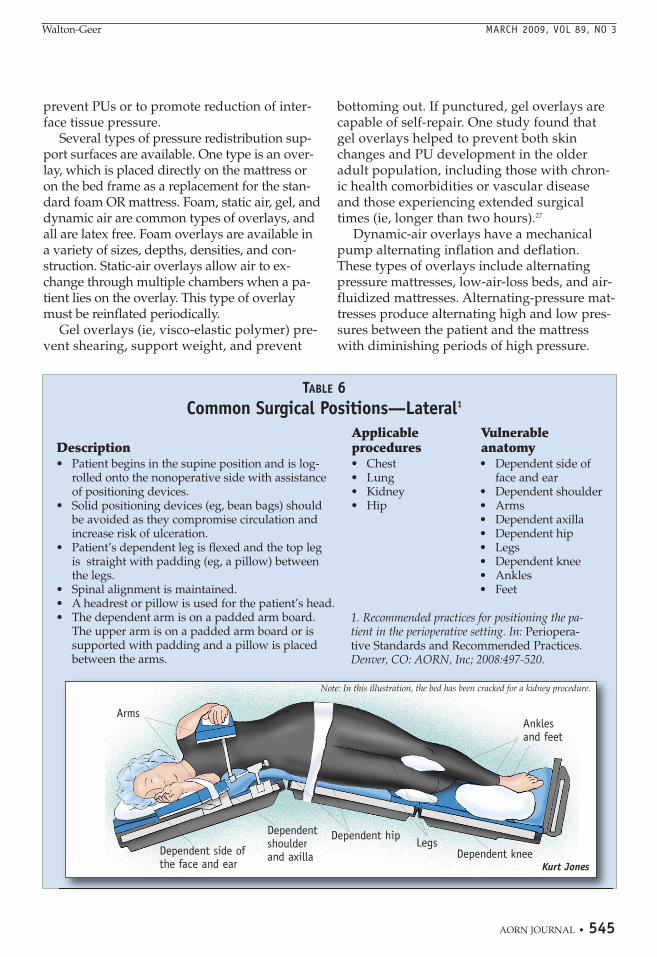
TABLE 6Common Surgical Positions—Lateral1
Applicable VulnerableDescription procedures anatomy
• Chest• Lung• Kidney• Hip
• Dependent side offace and ear
• Dependent shoulder• Arms• Dependent axilla• Dependent hip• Legs• Dependent knee• Ankles• Feet
• Patient begins in the supine position and is log-rolled onto the nonoperative side with assistanceof positioning devices.
• Solid positioning devices (eg, bean bags) shouldbe avoided as they compromise circulation and increase risk of ulceration.
• Patient’s dependent leg is flexed and the top leg is straight with padding (eg, a pillow) betweenthe legs.
• Spinal alignment is maintained.• A headrest or pillow is used for the patient’s head.• The dependent arm is on a padded arm board.
The upper arm is on a padded arm board or issupported with padding and a pillow is placedbetween the arms.
Anklesand feet
Dependent kneeLegs
Arms
Dependent side ofthe face and ear
Dependentshoulderand axilla
Dependent hip
Note: In this illustration, the bed has been cracked for a kidney procedure.
Kurt Jones
1. Recommended practices for positioning the pa-tient in the perioperative setting. In: Periopera-tive Standards and Recommended Practices.Denver, CO: AORN, Inc; 2008:497-520.
p538-552_03_09:Layout 1 2/11/2009 3:36 PM Page 545

MARCH 2009, VOL 89, NO 3 Walton-Geer
546 • AORN JOURNAL
Low-air-loss mattresses are air sacs throughwhich warm air passes. Air-fluidized mattressescontain small silicone-coated beads; warm airunder pressure sets the beads in motion to stim-ulate circulation and evenly distribute weight.7
Dynamic-air overlays are not often used intra-operatively because of the possibility of bodymovement, electrical problems, and asepsis.15
Mackey28 reviewed three OR trials that indi-cated that the use of air and gel pressure over-lays on the OR bed might be beneficial in reduc-ing the incidence of PU for high-risk surgical pa-tients.28 Reddy et al9 reviewed 59 randomizedcontrolled trials that addressed impairment ofmobility, skin integrity, and nutrition in relationto PU development. Strategies to address mobil-ity impairment included the use of a supportsurface, mattress overlays on the OR bed, andspecialized foam and specialized sheepskinoverlays. Reddy’s review reaffirmed that mat-tress overlays on the OR bed may decrease theincidence of postoperative PUs along with ade-quate nutrition, moistening the skin, and reposi-tioning.9 More current and unbiased research isneeded to address the effectiveness and defi-ciencies of surgical pressure redistribution sup-port surfaces.
SURGICAL CONSIDERATIONSAND RECOMMENDATIONS
All surgical patients should be consideredat risk for PU development because of the un-controllable length of surgery and the effectsof anesthesia on the patient’s hemodynamicstate along with the use of vasoactive medica-tions during surgery. Classifying all surgicalpatients as “at risk” for PU development is anappropriate preoperative intervention to suc-cessfully help reduce the incidence of possiblePU development. The preoperative assess-ment should include details of the patient’sskin status along with a risk assessment not-ing whether the patient is a high-risk candi-date for PU development based on the pro-posed procedure and intrinsic and extrinsicfactors. Perioperative nurses should developnursing guidelines and protocols and individ-ualized nursing care plans based on the pa-tient’s condition, the type and length of thesurgical procedure, the required surgical posi-
tioning devices, and risk factors (Table 7).SKIN ASSESSMENT. The perioperative nurse
should perform a thorough skin assessment ofeach surgical patient. This establishes a preop-erative baseline to compare with the patient’spostoperative status. The preoperative nurseshould check thoroughly for any skin compli-cations (eg, rash, maceration, infection, break-down, dermatitis, incontinence, lymphedema)and look for signs of venous insufficiency21
(eg, aching, cramps, pain, tiredness, paresthe-sia in the legs that worsens with standing orwalking and is relieved by rest and elevation).A Braden or Norton Scale can be used to vali-date the patient’s skin integrity and provide acomparison of preoperative and postoperativeskin status. These scales can determine preop-eratively whether the patient is at high risk forPU development, depending on the parame-ters being assessed. These assessments canprovide evidence that would suggest the needto take more proactive steps before surgery tohelp prevent possible tissue damage and PUdevelopment.
Pressure ulcer development does not neces-sarily start in the OR. Many factors that cancontribute to tissue fragility begin before sur-gery. It would be appropriate, therefore, tothoroughly assess the patient’s skin when per-forming the preoperative physical examina-tion (eg, nutrition, hydration) and laboratorytests (eg, hemoglobin, total albumin, prealbu-min), all of which are important in evaluatingskin integrity. For example, if a patient hasbeen immobile or unable to react to ischemicpain before surgery, the patient is at increasedrisk for skin breakdown. Perioperative nursesshould emphasize evaluating skin integritybefore surgery. More research needs to be per-formed to help support the preoperative andpostoperative use and effectiveness of a skinassessment for surgical patients.
CONSIDERATIONS FOR SUPPORT SURFACES. Pressure re-distribution devices should be used for all sur-gical patients. The use of pressure redistribu-tion support surfaces has been proven to be ef-fective in decreasing PU formation, especiallyamong high-risk populations.9,14,27,28 For surgery,research supports the use of a static-air mat-tress in the OR. Gel overlays have been shown
p538-552_03_09:Layout 1 2/11/2009 3:36 PM Page 546
Walton-Geer MARCH 2009, VOL 89, NO 3
AORN JOURNAL • 547
to provide a reduction in pressure but not aseffectively as air mattresses. More researchneeds to be done to help identify preventativetechniques, supplies, and equipment.
Nurse managers should assess the supportsurfaces used throughout the hospital, includ-ing in the emergency department (ED). Manypatients are transported to the ED in ambu-lances on hard surfaces. Patients then are trans-ferred onto stretcher mattresses that do not pro-vide the pressure redistribution needed to helpprevent PU development. Often, patients in theED are left on that surface waiting for admis-sion for many hours. Patients may already haveadversely affected tissue because of this exten-sive and long-term pressure.
More research is needed to address the pre-vention of PUs in surgical patients. The re-
search then should be translated into better ed-ucation to improve the competency of periop-erative team members and to help developand implement policies and procedures, whereneeded, to decrease the vulnerability for PUdevelopment. More evidence-based research inthis area will encourage practice changes thatwill in turn help decrease PU development,improve patient comfort, decrease patientmortality, and lower health care costs.
Acknowledgment: The author acknowledgesMichelle M. Byrne, PhD, RN, CNOR, associateprofessor of nursing and coordinator of the MSNursing Education Program, North Georgia College and State University, Dahlonega, GA, for her support and mentorship during the devel-opment of this manuscript.
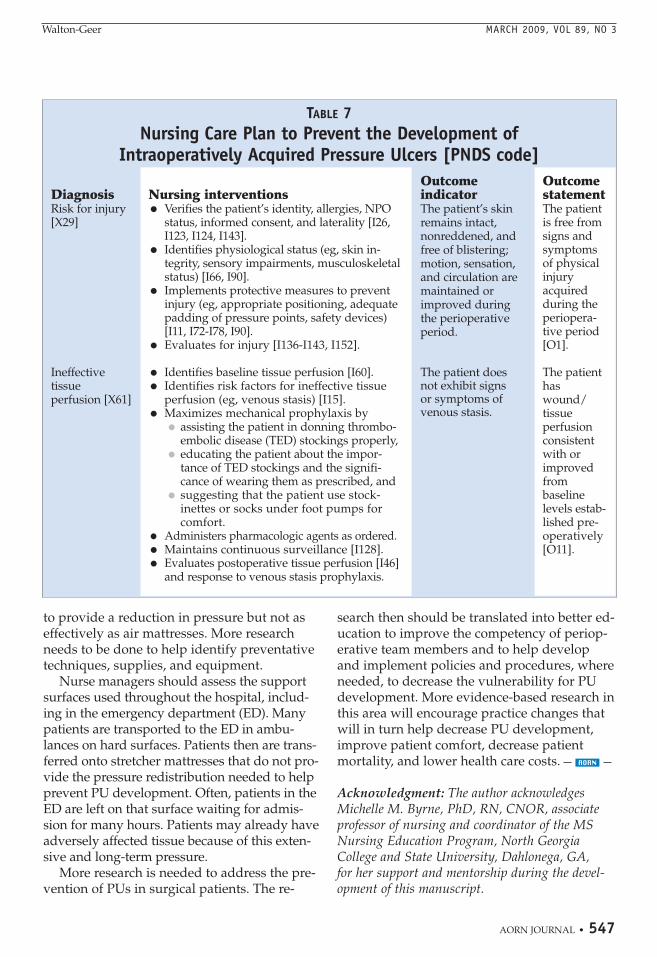
TABLE 7Nursing Care Plan to Prevent the Development of
Intraoperatively Acquired Pressure Ulcers [PNDS code]
Nursing interventions• Verifies the patient’s identity, allergies, NPO
status, informed consent, and laterality [I26,I123, I124, I143].
• Identifies physiological status (eg, skin in-tegrity, sensory impairments, musculo skeletalstatus) [I66, I90].
• Implements protective measures to preventinjury (eg, appropriate positioning, adequatepadding of pressure points, safety devices)[I11, I72-I78, I90].
• Evaluates for injury [I136-I143, I152].
• Identifies baseline tissue perfusion [I60].• Identifies risk factors for ineffective tissue
perfusion (eg, venous stasis) [I15].• Maximizes mechanical prophylaxis by
• assisting the patient in donning thrombo -embolic disease (TED) stockings properly,
• educating the patient about the impor-tance of TED stockings and the signifi-cance of wearing them as prescribed, and
• suggesting that the patient use stock-inettes or socks under foot pumps forcomfort.
• Administers pharmacologic agents as ordered.• Maintains continuous surveillance [I128].• Evaluates postoperative tissue perfusion [I46]
and response to venous stasis prophylaxis.
OutcomestatementThe patientis free fromsigns andsymptomsof physicalinjury acquiredduring theperiopera-tive period[O1].
The patienthaswound/tissue perfusionconsistentwith or improvedfrom baseline levels estab-lished pre-operatively[O11].
DiagnosisRisk for injury[X29]
Ineffective tissue perfusion [X61]
Outcome indicatorThe patient’s skinremains intact, nonreddened, andfree of blistering;motion, sensation,and circulation aremaintained or improved duringthe perioperativeperiod.
The patient does not exhibit signs or symptoms of venous stasis.
p538-552_03_09:Layout 1 2/11/2009 3:36 PM Page 547

MARCH 2009, VOL 89, NO 3 Walton-Geer
REFERENCES1. Ayello EA, Baranoski S, Lyder CH, Cuddigan J.Pressure ulcers. In: Baranoski S, Ayello EA, eds.Wound Care Essentials: Practice Principles. 2nd ed.Philadelphia, PA: Lippincott Williams & Wilkins;2007:254-286.2. Pressure ulcer stages revised by NPUAP. Nation-al Pressure Ulcer Advisory Panel. http://www.npuap.org/pr2.htm. Accessed December 27, 2008.3. Pieper B. Mechanical forces: pressure, shear, and friction. In: Bryant R, Nix D, eds. Acute &Chronic Wounds: Current Management Concepts. 3rd ed. St Louis, MO: Mosby; 2007:205-234.4. Position statement: Pressure ulcer staging. WoundOstomy and Continence Nurses Society. http://www.wocn.org/pdfs/WOCN_Library/Position_Statements/PressureUlcerStaging.pdf. Accessed Decem-ber 27, 2008.5. Montalvo I. The National Database of NursingQuality IndicatorsTM (NDNQI®). The Online Journalof Issues in Nursing. 2007;12(3). http://www.nursingworld.org/MainMenuCategories/ANAMarketplace/ANAPeriodicals/OJIN/TableofContents/Volume122007/No3Sept07/NursingQualityIndicators.aspx. Accessed January 30, 2009.6. Relieve the pressure and reduce harm. Institute forHealthcare Improvement. http://www.ihi.org/IHI/Topics/PatientSafety/SafetyGeneral/ImprovementStories/FSRelievethePressureandReduceHarm.htm.Accessed January 28, 2009.7. Graves N, Birrell F, Whitby M. Effect of pressureulcers on length of hospital stay. Infect Control HospEpidemiol. 2005;26(3):293-297.8. Brown G. Long-term outcomes of full-thicknesspressure ulcers: healing and mortality. OstomyWound Manage. 2003;49(10):42-50.9. Reddy M, Gill SS, Rochon PA. Preventing pressureulcers: a systematic review. JAMA. 2006;296(8):974-984.10. Hospital-acquired conditions (present on ad-mission indicator). The Centers for Medicare andMedicaid Services. http://www.cms.hhs.gov/HospitalAcqCond. Accessed January 28, 2009. 11. Baumgarten M, Margolis D, Localio AR, et al.Extrinsic risk factors for pressure ulcers early in thehospital stay: a nested case-control study. J GerontolA Biol Sci Med Sci. 2008;63(4):408-413.12. Ayello EA, Lyder CH. Protecting patients fromharm: preventing pressure ulcers in hospital pa-tients. Nursing. 2007;37(10):36-40.13. Padula CA, Osborne E, Williams J. Preventionand early detection of pressure ulcers in hospital-ized patients. J Wound Ostomy Continence Nurs.2008;35(1):65-75.14. Dybec RB. Intraoperative positioning and care ofthe obese patient. Plast Surg Nurs. 2004;24(3):118-122.15. Recommended practices for positioning the pa-tient in the perioperative setting. In: PerioperativeStandards and Recommended Practices. Denver, CO:AORN, Inc; 2008:497-520.
16. Nix DP. Support surfaces. In: Bryant R, Nix D,eds. Acute & Chronic Wounds: Current ManagementConcepts. 3rd ed. St Louis, MO: Mosby; 2007:235-248.17. Lee BY, Ostrander LE. Noninvasive evaluation ofthe cutaneous circulation. In: Lee BY, ed. The WoundManagement Manual. New York, NY: McGraw-Hill;2005:131-140.18. Price MC, Whitney JD, King CA, Doughty D.Development of a risk assessment tool for intraop-erative pressure ulcers. J Wound Ostomy ContinenceNurs. 2005;32(1):19-30.19. Bates-Jensen BM. Pressure ulcers: pathophysi-ology and prevention. In: Sussman C, Bates-JensenBM, eds. Wound Care: A Collaborative Practice Manu-al for Health Professionals. 3rd ed. Philadelphia, PA:Lippincott Williams & Wilkins; 2007:336-373.20. Posthauer M. Introduction to wound diagnosis.In: Sussman C, Bates-Jensen BM, eds. Wound Care:A Collaborative Practice Manual for Health Profession-als. 3rd ed. Philadelphia, PA: Lippincott Williams &Wilkins; 2007:52-71.21. Sewchuk D, Padula C, Osborne E. Preventionand early detection of pressure ulcers in patients un-dergoing cardiac surgery. AORN J. 2006;84(1):75-96.22. Nixon J, Cranny G, Iglesias E, et al. Randomisedcontrolled trial of alternating pressure mattresses com-pared with alternating pressure overlays for the pre-vention of pressure ulcers: PRESSURE (pressure reliev-ing support surfaces) trial. BMJ. 2006;332(7555):1413.23. Phillips NF. Positioning, prepping, and drapingthe patient. In: Phillips NF, ed. Berry and Kohn’s Operat-ing Room Technique. St Louis, MO: Mosby; 2004:470-511.24. O’Connell MP. Positioning impact on the surgi-cal patient. Nurs Clin North Am. 2006;41(2):173-192.25. Intraoperative nursing management. In:Smeltzer SC, Bare BG, Hinkle JL, Cheever KH, eds.Brunner & Suddarth’s Textbook of Medical-SurgicalNursing. 11th ed. Philadelphia, PA: LippincottWilliams & Wilkins; 2006:417-435.26. Lindgren M, Unosson M, Krantz AM, Ek AC.Pressure ulcer risk factors in patients undergoingsurgery. J Adv Nurs. 2005;50(6):605-612. 27. Hoshowsky VM, Schramm CA. Intraoperativepressure sore prevention: an analysis of beddingmaterials. Res Nurs Health. 1994;17(5):333-339.28. Mackey D. Support surfaces: beds, mattresses,overlays—oh my! Nurs Clin North Am. 2005;40(2):251-265.
548 • AORN JOURNAL
Patina S. Walton-Geer, RN-BC, MSN,CWCN, CFCN, is a wound and foot carenurse clinician at AnMed Health OutpatientWound and Foot Care Clinic, Anderson, SC.Ms Walton-Geer has no declared affiliation thatcould be perceived as a potential conflict of interest in publishing this article.
p538-552_03_09:Layout 1 2/11/2009 3:36 PM Page 548
1. Local blood flow is occluded when theexternal pressure exceeds normal capil-lary filling pressure of approximately a. 32 mmHg.b. 64 mmHg.c. 86 mmHg.d. 92 mmHg.
2. Underlying tissue may become necroticby the time a lesion presents on the skinsurface because a. muscle rests directly on bone.b. muscles have less vascular supply than
skin.c. muscle is more sensitive to pressure
than skin.d. muscles have more vascular supply than
skin.
3. Necrosis occurs when unrelieved pressureis applied for a. less than 30 minutes.b. two to four hours.c. four hours or more.d. six hours or more.
4. Extrinsic risk factors for tissue damage include
1. comorbid diseases.
2. friction.3. overhydration of tissue.4. shear.
a. 1 and 3b. 2 and 4c. 2, 3, and 4d. 1, 2, 3, and 4
5. When a patient has inadequate arterialblood flow, improper positioning can
1. cause blood pressure complications.2. decrease tissue perfusion.3. decrease venous return.4. result in thrombus formation.
a. 1 and 2b. 3 and 4c. 1, 3, and 4d. 1, 2, 3, and 4
6. According to AORN’s “Recommendedpractices for positioning the patient in theperioperative setting,” the OR team shouldreposition the patient every __________ toprevent continuous pressure on pressurepoints.a. 30 minutesb. hourc. two hoursd. three hours
ExaminationPrevention of Pressure Ulcers
in the Surgical Patient
PURPOSE/GOALTo educate perioperative nurses about prevention of intraoperatively acquired pressure ulcers(PUs).
BEHAVIORAL OBJECTIVESAfter reading and studying the article on preventing PUs in surgical patients, nurses will be able to
1. discuss the etiology of PU development,
2. describe factors that contribute to the development of intraoperatively acquired PUs,
3. identify surgical patient populations that may have an increased risk of developing PUs, and
4. describe methods available to help prevent PUs in surgical patients.
QUESTIONS
2.5
MARCH 2009, VOL 89, NO 3 • AORN JOURNAL • 549© AORN, Inc, 2009
p538-552_03_09:Layout 1 2/11/2009 3:36 PM Page 549
ExaminationMARCH 2009, VOL 89, NO 3
7. All agents used in anesthesia can1. cause a decrease in tissue perfusion. 2. cause some degree of vasodilatation.3. depress the autonomic nervous
system.4. lower blood pressure to some degree.
a. 1 and 3b. 2 and 4c. 1, 2, and 3d. 1, 2, 3, and 4
8. Anatomical sites that are vulnerable topressure ulcer development when a pa-tient is in the jackknife position include
1. dorsum of the feet.2. eyes, ears, and forehead.3. genitalia and breasts.4. knees.5. occiput.6. sacrum.
a. 1 and 5
b. 1, 2, 3, and 4c. 2, 3, 4, 5, and 6d. 1, 2, 3, 4, 5, and 6
9. The highest incidence of PU developmentoccurs in patients who are a. younger than 10 years of age.b. 50 years of age or older.c. 65 years of age or older.
10. Gel overlays (ie, visco-elastic polymer)1. allow gel to exchange through multiple
chambers.2. are capable of self-repair.3. prevent bottoming out.4. prevent shearing.5. support the patient’s weight.
a. 2 and 3b. 1, 4, and 5c. 2, 3, 4, and 5d. 1, 2, 3, 4, and 5
550 • AORN JOURNAL
The behavioral objectives and exam -ination for this program were preparedby Rebecca Holm, RN, MSN, CNOR,clinical editor, with consultation fromSusan Bakewell, RN, MS, BC, direc-tor, Center for Perioperative Educa-tion. Ms Holm and Ms Bakewell haveno declared affiliations that could beperceived as potential conflicts of inter-est in publishing this article.
This program meets criteria for CNOR and CRNFA recertification, as wellas other continuing education requirements.
AORN is accred ited as a provider of continuing nursing education by theAmerican Nurses Creden tialing Center’s Commission on Accredit ation.
AORN recognizes this activity as continuing education for registered nurses. This recognition does not imply that AORN or the American Nurses Credentialing Center approves or endorses products mentioned in the activity.
AORN is provider-approved by the California Board of Registered Nurs-ing, Provider Number CEP 13019. Check with your state board of nurs-ing for acceptance of this activity for relicensure.
p538-552_03_09:Layout 1 2/11/2009 3:36 PM Page 550
© AORN, Inc, 2009
Event #09100Session #1115
Please fill out the application and answer formon this page and the evaluation form on the back
of this page. Tear the page out of the Journal or makephoto copies and mail with appropriate fee to:
AORN Customer Servicec/o AORN Journal Continuing Education
2170 S Parker Rd, Suite 300Denver, CO 80231-5711
or fax with credit card information to (303) 750-3212.
Additionally, please verify by signature that you have reviewed the objectives and read the
article, or you will not receive credit.
Signature ______________________________________
1. Record your AORN member identification number inthe appropriate section below. (See your membercard.)
2. Completely darken the spaces that indicate your an-swers to examination questions 1 through 10. Use blueor black ink only.
3. Our accrediting body requires that we verify the timeyou needed to complete this 2.5 continuing educationcontact hour (150-minute) program. ______
4. Enclose fee if information is mailed.
AORN (ID) #_________________________________________
Name_______________________________________________
Address_____________________________________________
City ___________________________________________________ State __________ Zip __________
Phone number _______________________________________
RN license #____________________________________________ State __________
Fee enclosed ___________________________________________
or bill the credit card indicated ■■ MC ■■ Visa ■■ American Express ■■ Discover
Card # __________________________________ Expiration date _____________________
Signature _______________________________________________________________ (for credit card authorization)
Fee: Members $12.50Nonmembers $25
Program offered March 2009
The deadline for this program is March 31, 2012
Answer Sheet 2.5
A score of 70% correct on the examination is required for credit.
Participants receive feedback on incorrect answers.
Each applicant who successfully completes this program will receive a certificate of completion.
Prevention of Pressure Ulcers in the Surgical Patient
MARCH 2009, VOL 89, NO 3 • AORN JOURNAL • 551
p538-552_03_09:Layout 1 2/11/2009 3:36 PM Page 551
552 • AORN JOURNAL • MARCH 2009, VOL 89, NO 3 © AORN, Inc, 2009
This evaluation is used to determine theextent to which this continuing education
program met your learning needs. Rate theseitems on a scale of 1 to 5.
PURPOSE/GOALTo educate perioperative nurses about preven-tion of intraoperatively acquired pressure ul-cers (PUs).
OBJECTIVESTo what extent were the following objectives ofthis continuing education program achieved?1. Discuss the etiology of PU development.2. Describe factors that contribute to the de-
velopment of intraoperatively acquiredPUs.
3. Identify surgical patient populations thatmay have an increased risk of developingPUs.
4. Describe methods available to help pre-vent PUs in surgical patients.
CONTENTTo what extent5. did this article increase your know ledge
of the subject matter?6. was the content clear and organized?7. did this article facilitate learning?8. were your individual objectives met?9. did the objectives relate to the overall
purpose/goal?
TEST QUESTIONS/ANSWERSTo what extent10. were they reflective of the content?11. were they easy to understand?12. did they address important points?
LEARNER INPUT13. Will you be able to use the information
from this article in your work setting?a. yesb. no
14. I learned of this article viaa. the AORN Journal I receive as an AORN
member.
b. an AORN Journal I obtained elsewhere.c. the AORN Journal web site.
15. What factor most affects whether you takean AORN Journal continuing educationexamination?a. need for continuing education contact
hoursb. pricec. subject matter relevant to current posi-
tiond. number of continuing education contact
hours offered
What other topics would you like to see ad-dressed in a future continuing education arti-cle? Would you be interested or do you knowsomeone who would be interested in writingan article on this topic?Topic(s): ____________________________________________________________________________Author names and addresses: ___________________________________________________________________________________________________
Learner EvaluationPrevention of Pressure Ulcers
in the Surgical Patient
2.5
p538-552_03_09:Layout 1 2/11/2009 3:36 PM Page 552