Embed Size (px)
Citation preview

Case Report
Primary Ascaridial Perforation of the SmallIntestine: Sonographic Diagnosis
Ashish Chawla, MBBS, Vasudha Patwardhan, DMRD, Mohit Maheshwari, MBBS, Ashish Wasnik, MBBS
Department of Radiology, King Edward VII Memorial Hospital, Parel, Mumbai 400012, India
Received 7 June 2002; accepted 17 October 2002
ABSTRACT: Ascaris lumbricoides is the most com-mon helminth affecting humans. Ascariasis can resultin serious complications, including intestinal obstruc-tion and perforation. Early diagnosis and treatment ofsuch complications reduces the risk of mortality. Wepresent a case of sonographically diagnosed as-caridial perforation in a 5-year-old girl. On sonogra-phy, each ascarid appeared as 2 pairs of parallel lines,representing the worm’s outer margins, flanking acentral sonolucent line, representing its digestivetract. Sonography revealed ascarides in the peritonealcavity and in some loops of the small bowel. Emer-gent laparotomy was performed to remove ascaridesfrom the peritoneal cavity and terminal ileum, and thepatient recovered well and was asymptomatic at a3-month follow-up. Knowledge of the sonographicfeatures described herein may aid in the evaluationof patients, especially children, in tropical countrieswho have clinical symptoms of ascariasis. © 2003Wiley Periodicals, Inc. J Clin Ultrasound 31:211–213,2003; Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/jcu.10152
Keywords: ascariasis; ascaris; intestinal perforation;peritonitis; ultrasonography
Ascaris lumbricoides is the most common hel-minth affecting humans and is especially
common in tropical countries. Infestation can oc-cur through accidental ingestion of embryonatedeggs in polluted drinking water, food, or soil. Af-ter ingestion, the eggs reach the duodenum,where intestinal juices soften the shells and freethe larvae,1 which, in turn, penetrate the intesti-nal wall to reach the bloodstream. The larvae mi-grate to the lungs and traverse the alveolar wall.After being coughed up, the larvae are swallowed
and thus return to the small intestine. In the il-eum, they mature and produce eggs, which leavethe body by the fecal route. Adult ascarides candamage the walls of the small intestine. Ascaria-sis can cause such complications as small-bowelobstruction, intussusception, volvulus, and perfo-ration. In the absence of predisposing intestinaldisease, primary ascaridial perforation of thesmall bowel resulting in peritonitis is rare.2,3 Thepresence of worms in the intestine can be diag-nosed sonographically.4 We present a case inwhich intestinal perforation due to ascariasis wasdiagnosed using sonography after plain radiogra-phy showed no signs of this complication.
CASE REPORT
A 5-year-old girl who had been experiencing ab-dominal pain, abdominal distension, and vomit-ing for the previous 5 days visited our hospital.Oral passage of roundworms had occurred 6 daysearlier. The abdominal pain had worsened in theprevious 6–8 hours, and the patient had had 1episode of diarrhea before visiting the hospital.
Clinical examination revealed that the patienthad tachycardia. Palpation of her abdomen re-vealed tenderness and rigidity with guarding.Bowel sounds were absent. A hemogram indi-cated anemia, with a hemoglobin level of 9 g/dl.The differential white blood cell count was nor-mal, and the Widal test for typhoid fever wasnegative.
Plain abdominal radiography with the patientstanding showed multiple air-fluid levels, sug-gesting small-bowel obstruction. No signs of in-testinal perforation were observed.
Sonography performed using an HDI 3000scanner (Philips-ATL, Bothell, WA) equipped
Correspondence to: A. Chawla
© 2003 Wiley Periodicals, Inc.
VOL. 31, NO. 4, MAY 2003 211
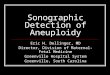
with a 5–12-MHz linear-array transducer re-vealed multiple long echogenic tubular structuresmoving freely in the peritoneal cavity (Figure 1).Each tubular structure consisted of 2 pairs of par-allel outer lines, representing the outer marginsof an ascarid, flanking a central sonolucent linerepresenting the ascarid’s digestive tract (Figures1 and 2). Minimal free fluid and a few ascarideswere present outside the bowel lumen near theleft iliac fossa. The patient also showed markedtenderness on compression with the transducer inthis region. Some of the small-bowel loops alsoappeared to contain ascarides (Figure 3). No signsof pneumoperitoneum were seen.
On the basis of these sonographic findings,emergent laparotomy was performed. Peritonitiswas present, and many ascarides were removedfrom the peritoneal cavity and terminal ileum(Figure 3). Multiple perforations were present inthe antimesenteric wall of a discolored, necroticloop of the terminal ileum. Ascarides extrudedfrom these perforations, which had necrotic mar-gins.
The patient’s postoperative course was un-eventful, and prophylactic antibiotics were ad-ministered. She was asymptomatic at the time ofher 3-month follow-up visit.
DISCUSSION
Obstruction and perforation of the small bowelare serious complications of ascariasis and oftenoccur with migration of ascarides into the perito-neal cavity, resulting in peritonitis. The exact in-cidence of primary ascaridial perforation of thesmall bowel is not known. The proposed mecha-nism of this complication is direct pressure andirritation of the bowel wall by impacted ascaridialmasses, leading to ulceration, necrosis, and per-foration. Lytic secretions from ascarides alsoprobably play a role.5
When sonographically imaged longitudinally,an ascarid appears as a linear echogenic struc-ture: 2 pairs of parallel echogenic lines, represent-ing the body margins, flank a broader central so-nolucent line, representing the digestive tract.When sectioned and viewed transversely, the as-carid resembles a bull’s-eye target, with an echo-genic body margin encircling an inner dot-like so-nolucent digestive tract. These sonographicfeatures have been variously designated as the“strip,” “four-lines,” “inner-tube,” “double-tube,”“bull’s-eye,” “target,” or “zig-zag” sign and de-scribed as a “worm mass” or “spaghetti-like” ap-pearance.6 Live ascarides exhibit nondirectionalslow writhing movements, making them easy to
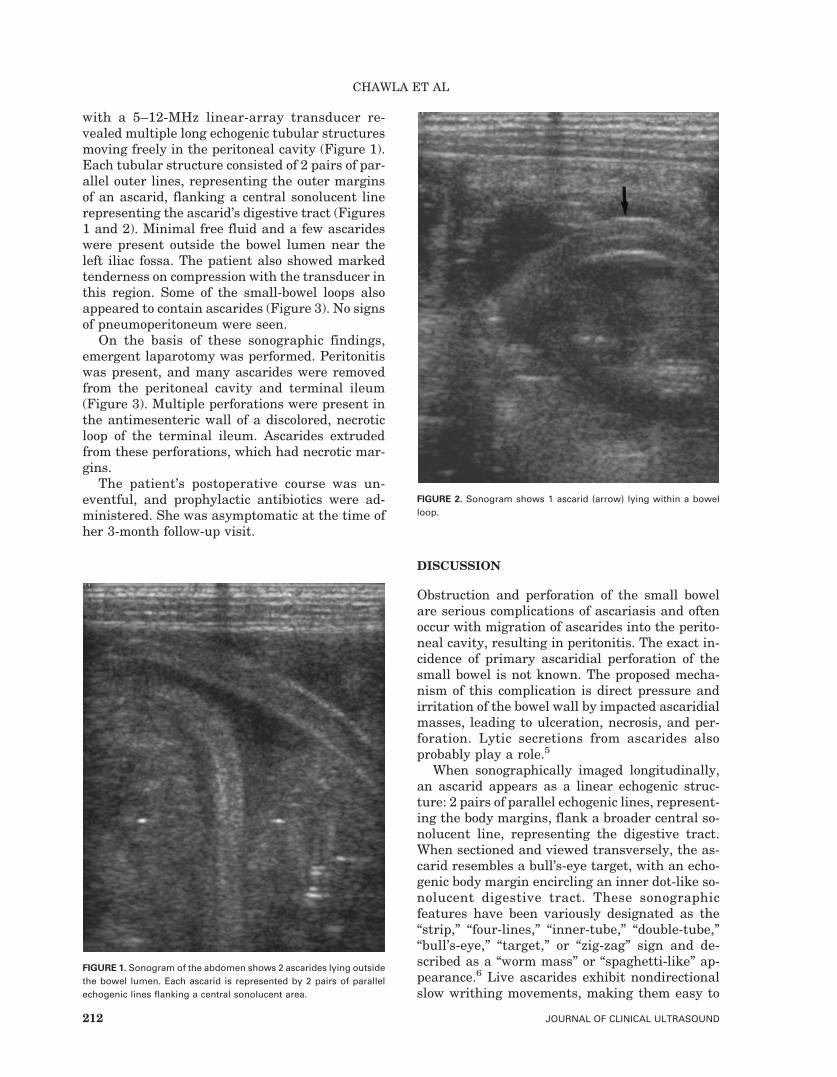
FIGURE 1. Sonogram of the abdomen shows 2 ascarides lying outsidethe bowel lumen. Each ascarid is represented by 2 pairs of parallelechogenic lines flanking a central sonolucent area.
FIGURE 2. Sonogram shows 1 ascarid (arrow) lying within a bowelloop.
CHAWLA ET AL
212 JOURNAL OF CLINICAL ULTRASOUND

identify on sonography. Dead ascarides undergocalcification and appear as parallel stripes of cal-cification.
In our patient, sonography provided direct vi-sualization of live ascarides moving freely withinthe extraluminal fluid near the left iliac fossa.The sonographic findings were strongly sugges-tive of bowel perforation, with live ascarides ex-truding from the bowel lumen into the peritonealcavity.
Plain abdominal radiography did not showpneumoperitoneum or intestinal perforation,whereas sonography suggested small-bowel per-foration. Surgical exploration confirmed this di-agnosis and revealed massive ascaridial infesta-tion, perforations of the distal ileum, and thepresence of worms moving freely within the peri-toneal cavity.
Our report shows that sonography is valuablenot only in identifying ascaridial infestation butalso in detecting intestinal perforation, which fa-cilitated timely, targeted surgical intervention inour patient. In tropical countries, where ascaria-
sis is a possible cause of intestinal obstructionand primary intestinal perforation, especially inpediatric patients, knowledge of the sonographicfeatures described herein may be useful in theevaluation and diagnosis of patients with clinicalsymptoms of ascariasis.
REFERENCES
1. Ihekwaba FN. Ascaris lumbricoides and perforationof the ileum: a critical review. Br J Surg 1979;66:132.
2. Dickson JAS, Cole GJ. Perforation of terminal il-eum: a view of 38 cases. Br J Surg 1964;51:893.
3. DeSa AE. Surgical ascariasis. Indian J Surg 1966;28:182.
4. Margulis AR, Burhenne HJ. Alimentary tract radi-ology. 4th ed. St. Louis: Mosby; 1989. p 1518.
5. Hangloo VK, Koul I, Safaya R, et al. Primary as-caridial perforations of small intestine and Meckel’sdiverticulum. Indian J Gastroenterol 1990;9:287.
6. Hui JY, Woo PC, Kan PS, et al. Ultrasonographicfeatures of pseudotumorous form of ascariasis. EurJ Radiol 2001;39:188.
FIGURE 3. Intraoperative photograph shows an ascarid (arrow) extruding from a small-bowel loop.
ASCARIDIAL PERFORATION OF THE SMALL INTESTINE
VOL. 31, NO. 4, MAY 2003 213








![Fish Bone Causing Perforation of the Intestine and Meckel ...downloads.hindawi.com/journals/cris/2020/8887603.pdf · ureteric colic [11, 13, 14]. But very often, these patients can](https://img.pdfslide.net/doc/110x75/609465cb1f78b227b336f964/fish-bone-causing-perforation-of-the-intestine-and-meckel-ureteric-colic-11.jpg)