Embed Size (px)
Citation preview

Primary Clinical Care Manual
10th edition 2019
Primary Clinical Care M
anual10th edition 2019

10
777777
Appendices
Med
icat
ion
his
tory
an
d r
eco
nci
liat
ion
778778 | Primary Clinical Care Manual 10th edition |778
Medication history and reconciliation
Medication reconciliation1,2
Background• Medication reconciliation:
– is a formal process of obtaining and verifying a complete and accurate list of each patient's current medicines
– matches the medicines the patient should be prescribed against those they are actually prescribed. Any discrepancies are discussed with the MO/NP3
– is a requirement to meet the national Medication Safety Standards1
– is a strategy that has been shown to improve medication safety and significantly decrease errors.
• Medication history errors:1
– are common – often occur when patients are being transferred e.g. evacuated to hospital, returning home – can cause harm in up to 30% of cases – have been shown to occur in 26-87% of medication records
General approaches• Medication reconciliation must be documented and where possible be recorded on a clinical form
such as a National Medication Management Plan.
• The Queensland Medication Action Plan is available at https://qheps.health.qld.gov.au/__data/assets/pdf_file/0030/335478/sw016.pdf or https://www.safetyandquality.gov.au/wp-content/uploads/2010/01/Medication-Management-Plan.pdf
• Where possible, use a pharmacist, including via telehealth services for remote support3
• Medication reconciliation is a 4 step process.3 See Four steps of medication reconciliation table on following page:
– obtain and document the best possible medication history (BPMH). See Best possible medication history (BPMH), page 780
– confirm the accuracy of the medication history – reconcile the history with prescribed medicines and follow up discrepancies – supply accurate medicines information when care is transferred
• Ideally medication reconciliation should be completed on all patients before any medicines are ordered, administered or supplied
• Target patients at greater risk of adverse medication events and those using high risk medications where resources are limited e.g. time.4 See Target patients at greater risk of adverse medication events on the following page

Med
ication
histo
ry and
recon
ciliation
779Section 10: Appendices | Medication history and reconciliation 779
•
Target patients at greater risk of adverse medication events5
• The elderly – > 65 years for non-indigenous people – > 45 years for Aboriginal and Torres Strait Islander people
• Children
• Those who are clinically deteriorating
• Those taking > 4 medicines or medicines with complex regimens
• Those with a history of medication allergy, adverse drug reaction or medication intolerances
• Those with a poor level of adherence to medication regimens
• Those with impaired kidney, liver or heart function
• Those who are morbidly obese
• Those diagnosed with cancer
• Those diagnosed with a mental health condition
High-risk medicines are known by the acronym APINCH and include:6
– Anti-infectives – Potassium and other electrolytes – Insulin – Narcotics and other sedatives – Chemotherapeutic agents – Heparin, enoxaparin, warfarin and other anticoagulants
Four steps of medication reconciliation1
1. Obtain best possible medication history 2. Confirm the accuracy of the history
• See Best possible medication history (BPMH), page 780
• Compile list of medicines from patient interview and other sources such as:
– referrals, discharge summary – medication charts – prescriptions
• Review medication list• Inspect patient’s medication
containers including blister packs• Contact MO/NP and other
prescribers and pharmacists• Interview carers and family members• Review health records
3. Reconcile the history with prescribed medicines 4. Supply accurate medicines information
• Compare the patient's medication history with the prescribed medicines
• Check that these MATCH • Document reasons for change to medicines• Where there are discrepancies, discuss
these with the MO/NP or other prescriber• Document reasons for change to medicines
• Provide a list of medicines and reasons for any changes to:
– the incoming clinician when care is being transferred
– the retrieval team when transported i.e. RFDS, RSQ
– a carer when patient is being discharged – the patient

Med
icat
ion
his
tory
an
d r
eco
nci
liat
ion
780780 | Primary Clinical Care Manual 10th edition |780
Best possible medication history (BPMH)7
Background• A medication history is a record of all prescribed and non-prescribed medicines that are taken at
the time of presentation.
• Obtaining a BPMH is one of the 4 steps in the medication reconciliation process, which aims to improve patient safety1
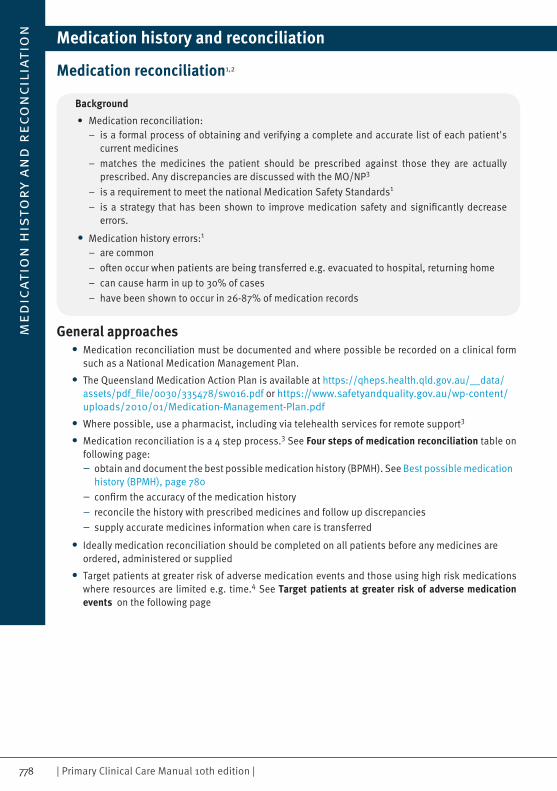
• Use the checklist below to prompt specific questions to obtain the best possible medication history8
• A BPMH is the responsibility of each clinician involved in the medication reconciliation process. It is a collaborative process
• A BPMH consists of: – an interview with the patients and/or family/carer wherever possible – patient details, date of history, name of staff member, sources of information – verification with more than one source e.g. previous medication charts, carer, MO/NP, GP – recording adverse reactions – document the history
• Types of medication to be noted include: – prescribed and prescription medicines – non-prescribed and non-prescription medicines – complementary or herbal medicines – traditional medication e.g. bush medicine – recreational drugs – prn medicines
• The following checklist can assist to complete a thorough BPMH
Med
ication
histo
ry and
recon
ciliation
781Section 10: Appendices | Medication history and reconciliation 781
Prescription medicines• Sleeping tablets• Inhalers, puffers with or without spacer, sprays, sublingual tablets• Oral contraceptives, hormone replacement therapyOver-the-counter medicines• Analgesics • Gastrointestinal medication for reflux, heartburn, constipation, diarrhoea• Nicotine replacement patches, gum, spray
Injected medicines including insulin pumps, analgaesia pumps
Topical medicines e.g. creams, ointments, lotions, patches
Inserted medicines e.g. nose/ear/eye drops, pessaries, suppositories, vaginal rings, medicated IUCD
Implantable medicines e.g. contraceptive rods, hormonal implants for cancer
Complementary medicines• Traditional medicines• Herbal medicines• Bush medicines• Vitamins• Natural therapies
Other people's medicine
Social and recreational drugs e.g. tobacco, alcohol, marijuana, illicit drugs
Intermittent medicines e.g. weekly or twice weekly
Recently changed medicines or regimens including:• Completed courses of medicine• Ceased medicines• Altered medicines
Any previous adverse medication reactions, include allergies, reactions and intolerances
Wearing any medical alert jewellery
Assess adherence by asking:• 'People often have difficulty taking their pills for one reason or another.
Have you had difficulty taking your pills?'• 'About how often would you say you miss taking your medicines?'

No
tifi
cati
oN
of
a pa
tieN
t d
eath
782782 | Primary Clinical Care Manual 10th edition |782
Notification of a patient death
Information• The following refers to the management of a patient death in the state of Queensland• Other jurisdictions are advised to follow local policy and procedures
• Some resources for other States are listed in the Resources section below
1. Obvious death• Complete a Life Extinct Form
– can be completed by an MO/NP, Registered Nurse, Paramedic or Police Officer (in certain obvious death cases only) for the purpose of management and transportation of the deceased body and to facilitate the management of the deceased in the community prior to the death certificate being issued for the deceased
– 'Obvious death' is defined on the Life Extinct Form, available in all Queensland facilities or on the Queensland Health intranet at: https://qheps.health.qld.gov.au/__data/assets/pdf_file/0035/577673/life_extinct.pdf
2. Reportable death• A decision must be made if the death is a reportable death in accordance with the Coroners Act 2003
(Qld). The criteria for a reportable death1 are: – death of an unknown person – death in suspicious circumstances – death in care (applies to people cared for under disability, mental health, justice, child guardianship or child protection legislation)
– violent or otherwise unnatural death – death in custody of police, courts, corrective services or juvenile justice – death as a result of police operations – health procedure related death where death was not reasonably expected to be the outcome – death where Form 9: Cause of Death Certificate not issued and unlikely to be issued
• Where the death is considered a reportable death or if unsure and there is a need to seek coroner's advice, the MO will complete a Form 1a: Medical practitioner report of death to a coroner and fax/scan/email to the coroner available from: https://www.courts.qld.gov.au/__data/assets/pdf_file/0008/87803/cor-f-1a.pdf
• When the death is considered reportable as a violent or otherwise unnatural death (other than those from mechanical falls) the death must be reported to the police who will then report the death to the coroner
• An MO is not to complete a Form 9:Cause of Death Certificate for a reportable death, unless authorised to do so by the coroner
• Information for health professionals about Coronial processes is available at: https://www.courts.qld.gov.au/__data/assets/pdf_file/0006/92868/m-osc-fs-information-for-health-professionals.pdf
• Medical equipment, tubes and medical devices attached or inserted should remain in situ until police investigations have concluded, unless otherwise directed by the police

No
tificatioN
of a patieN
t death
783Section 10: Appendices | Notification of a patient death 783
3. Non-reportable death• Where the death is not a reportable death a Form 9: Cause of Death Certificate can be completed by
an MO only. Refer to guidance issued by the Office of the State Coroner Issuing cause of death certificates for apparent natural causes deaths available at: https://www.courts.qld.gov.au/__data/assets/pdf_file/0014/210218/osc-fs-issuing-cause-of-death-certificates-apparent-natural-causes-deaths.pdf
• Where the death is a perinatal death (baby at least 20 weeks gestation or 400 grams weight and died within 28 days after birth) a Form 9a Perinatal Supplement to Form 9: Cause of Death Certificate must also be completed
• Since November 2016, all expected stillbirths > 24 weeks gestation are a reportable event in the Hospital and Health Boards Regulation 2012 – s29(1). Unexpected stillbirths should be reported using the RiskMan incident reporting tool. Refer to the Queensland Health Guide to reporting a stillbirth in RiskMan http://qheps.health.qld.gov.au/psu/clinicalincident/docs/fs-stillbirth-report.pdf
• Form 9 and Form 9a are triplicate forms available in all facilities
4. Specific instances• Where a deceased person requires transport, funeral directors may require an Authority to Transport;
check Hospital and Health Service forms
• Other Forms may apply to specific types of deaths: – child death - Report Of Suspected Child In Need Of Protection form, available from: https://secure.communities.qld.gov.au/cbir/PrescribedEntityChildSafetyReport. See Child protection, page 760
– mental health patient - contact Hospital and Health Service Director of Mental Health – maternal patient death - contact Hospital and Health Service Director of Obstetrics – perioperative patient death - Queensland Audit of Surgical Mortality contact the Hospital and Health Service Director of Medical Services
• All inpatient deaths in Queensland Health facilities and non-inpatient deaths where the patient was treated by a Queensland Health facility within the last 30 days are subject to a local death review process. Contact the Hospital and Health Service Director of Medical Services for more information and applicable forms
Perinatal death Form 9 and Form 9a
Complete Form 1a and notify coroner
Death other than perinatal Form 9
Life extinct formConsider HHS Death Review Process
Reportable death to coroneror unsure
Not reportable
Deceased person

No
tifi
cati
oN
of
a pa
tieN
t d
eath
784784 | Primary Clinical Care Manual 10th edition |784
5. Resources
Queensland• The Queensland Coroner is available for advice and assistance Monday to Friday 0830-1630 hours 07 3239 6193, or On Call after hours 07 3247 3372
• Coronial management resources: https://www.courts.qld.gov.au/courts/coroners-court/about-coroners-court/resources-and-legislation#state
Victoria• Coroners court available at: www.coronerscourt.vic.gov.au
• Coroner Clinical Liaison Service available at: www.health.vic.gov.au/cls/index.htm

GlasG
ow
com
a scale / aVPU
785Section 10: Appendices | Glasgow coma scale/AVPU 785
Glasgow Coma Scale/AVPU
A Alert
V Responds to verbal statement
P Responds to painful stimuli
U No response (unresponsive)
Glasgow coma scale (GCS) - adult/child/infant1,2
(GCS) AdultChild > 5 years
Child2-5 years
Eyes open
4. Opens eyes spontaneously3. Opens eyes on command or to speech2. Opens eyes with pain (pinching)1. No eye opening/no response
Best verbal response
5. Fully orientated4. Confused, disorientated: not sure of
their name or where they are or what happened
3. Inappropriate meaningless words2. Incomprehensible
noises - grunts, moans 1. No sounds
5. Orientated/interacts/follows objects/smiles/alert/coos/babbles words to usual ability
4. Confused, cries but is consolable3. Inappropriate words/moaning/
persistent cries and/or screams2. Grunts, moans, inconsolable,
irritable, restless1. No sounds
Best motor response
6. Obeys commands5. Localises to pain 4. Withdraws to pain 3. Flexor response to pain (bends arm or leg)2. Extensor response to pain (straightens arm or leg)1. No response
• Maximum scale: 15 (fully alert, conscious) Minimum scale: 3 (unconscious)• Always act on:
− Scale < 15− Drop of 2 or more from last assessment. If GCS ≤ 8 prepare to intubate
GCS not testable if any of the following apply:− had medicines including anaesthetics, sedatives, neuromuscular
blockades and similar, intoxication with alcohol or drugs− a direct eye injury or periorbital swelling− cranial nerve injuries− a hearing impairment− been intubated or has a tracheostomy− immobilised limbs or spinal cord injuries− dysphasia− a language or cultural barrier− dementia or some psychiatric disorders
In these situations, it is appropriate to record the individual scales for each measurable response (motor, verbal or eyes)

Safe
uSe
of
para
ceta
mo
l
786786 | Primary Clinical Care Manual 10th edition |786
Safe use of paracetamolBackground1
• Paracetamol (also known as acetaminophen) is a common and widely used non-opioid analgesic
• Paracetamol has a well established safety profile when used appropriately
• In acute overdose, paracetamol can lead to severe and sometimes fatal hepatotoxicity
• Dose should be titrated according to weight and risk factors. In obese children the dosage should be based on ideal body weight2 i.e. 50th centile on an appropriate weight-for-age percentile chart available from https://www.rch.org.au/childgrowth/Growth_Charts/#
• For neonates and infants < 3 months seek specialist advice
Recommended dose paracetamol (oral) - Prescribing guide3
Risk Factor (see next Table) Dose Duration
Children 3 months to 1 year1,2
• No risk factors (see risk factors on next page)
• 15 mg/kg/dose every 4-6 hours up to a maximum of 60 mg/kg in 24 hours
• Do not exceed 1 g per dose• Do not exceed 4 g in 24 hours
• Review at 48 hours • If treatment to continue
beyond 48 hours, consider reducing dose
• 1 or more risk factors
• 15 mg/kg/dose every 4-6 hours up to a maximum of 45 mg/kg in 24 hours
• Do not exceed 1 g per dose• Do not exceed 3 g in 24 hours
• Review at 48 hours • If treatment to continue
beyond 48 hours, consider monitoring LFT and INR
Adult and child ≥ 12 years1
• No risk factors• 0.5-1 g every 4-6 hours, up to
a maximum of 4 g in 24 hours• Review at 48 hours
• 1 or more risk factors and actual weight ≥ 50 kg
• 0.5-1 g every 4-6 hours, up to a maximum of 3 g in 24 hours
• Review at 48 hours• If treatment to continue
beyond 48 hours, consider monitoring LFT and INR
• 1 or more risk factors and actual weight < 50 kg
• 15 mg/kg/dose every 4-6 hours up to a maximum of 4 doses in 24 hours
• Severe hepatic impairment and actual weight ≥ 50 kg
• 0.5-1 g every 4-6 hours, up to a maximum of 2 g in 24 hours
• Severe hepatic impairment and actual weight < 50 kg
• 15 mg/kg/dose every 4-6 hours up to a maximum of 3 doses in 24 hours

ben
zathin
e and
procain
e ben
zylpenicillin
adm
inistratio
n
787Section 10: Appendices | Benzathine and procaine benzylpenicillin administration 787
Factors that may increase the risk of paracetamol toxicity1
Adult Child• Prolonged fasting or dehydration• Chronic under-nutrition• Chronic, excessive alcohol use• Chronic use of anticonvulsants• Severe hepatic impairment• Elderly, frail patients
• Febrile illness• Younger age• Prolonged fasting, vomiting or dehydration• Chronic under-nutrition• Hepatic impairment• Prior paracetamol intake e.g. in over-the-
counter cough/cold preparations• Use of adult rather than paediatric formulations• Use of paediatric formulations designed for an
older age group e.g. siblings or availability of multiple strengths of paediatric formulations
Administration tips for benzathine benzylpenicillin (Bicillin LA®) and procaine benzylpenicillin (procaine penicillin)
1. Administration tips• Apply EMLA® cream to the injection site 30-60 minutes prior to giving needle
• Allow medicine to warm up to room temperature by rolling the syringe between hands for 1-2 minutes
• Consider other pain management measures such as applying ice to injection site 10 minutes prior to injection, use of a 'Buzzy®' device, and distraction techniques for children1,2,3
• Administer analgesia as clinically indicated. See Acute pain management, page 35
• Give by deep IM injection only into the upper, outer quadrant of the buttock, mid lateral aspect of the thigh or into the ventrogluteal area
• Avoid major nerves and blood vessels. Do not give into the deltoid
• Apply firm pressure with thumb to the exact injection site for 30 seconds prior to the injection
• Use 21 G needle and deliver injection very slowly i.e. over 2 minutes
• Note: The addition of 0.5-1.0 mL of 1% lidocaine (lignocaine) is used elsewhere but is not recommended with preloaded syringes available in Australia
2. Giving a ventrogluteal (gluteus medius muscle) injection4
• Approach the patient with the drawn-up medicine in a syringe and explain the procedure
• Position the patient on their side (position of choice) and bend their knee on the leg chosen for the injection. This helps to locate the greater trochanter
• If lying prone, ask them to ‘toe in’ to internally rotate the femur. If lying supine, ask them to flex their knee. It is not recommended to give a ventrogluteal injection from a standing position
• Place the heel of your opposite hand on the grater trochanter, that is, your left hand on their right leg and vice versa
• Locate and place your index finger on the anterior superior iliac crest. Your thumb should be pointed towards the front of the leg
• Spread your middle finger to form a ‘V’ - the injection site is in the middle of the ‘V’, which should be level with the knuckles of your index and middle fingers
• Remember to remove your fingers before you inject, to prevent a needle stick injury

ben
zath
ine
and
pro
cain
e b
enzy
lpen
icil
lin
ad
min
istr
atio
n
788788 | Primary Clinical Care Manual 10th edition |788
• If you have small hands and find that with the ball of your hand on the greater trochanter your index finger does not reach the iliac crest, then slide your hand up the leg until it does
Anterior superior iliac spine (ASIS) - (index finger)
Ventrogluteal (gluteus medius) injection site
Greater trochanter (palm)
Posterior iliac crest (middle finger)
Posterior iliac crest (middle finger)
Finding the ventrogluteal site5,6

De-escalatio
n tech
niq
ues
789Section 10: Appendices | De-escalation techniques 789
De-escalation techniques1,2
• De-escalation is the use of techniques, including verbal and non-verbal communication skills, aimed at short-term defusing of anger, avoiding aggression and reducing the use of restrictive interventions. The aim is to avoid confrontation, to offer the patient choices in a difficult situation and to assist in reaching a calmer state3
• Never attempt to manage a distressed or agitated patient without adequate support and resources
• If a patient presents a risk to public safety or their own safety which cannot be managed by resources within the facility, call Police
• In smaller health facilities and in remote areas, referral should occur at a much earlier stage
• Follow your facility’s Emergency Preparedness Plan, including activating a Code Black emergency if appropriate
1. General principles• Establish a working relationship with patients who may be angry or uncooperative
• Use 'active listening' techniques, and a verbal 'loop' seeking to find a way to respond that agrees with the patient
• Explain to the patient what the clinician wants the patient to do e.g. accept medication, sit down with the clinician
• Empower patients to actively participate in their care, including young patients and children
• Work in partnership with patients and their families or carers
• Monitor changes in mood or composure that may lead to aggression
• Manage patients who may become, or who are, angry, aggressive or uncooperative in areas away from other patients or visitors, but ensure staff are not alone
• Use a wide range of verbal and non-verbal skills and interactions to avoid or manage 'flashpoints'
• Consent to administration of sedating medication can be used as part of the de-escalation process
• Use patients’ behaviour care plans (if they have one) to discuss their wishes if they become agitated
• Continually show respect and empathy for patient
• Be aware of or suspect abuse as a contributory factor in violence and aggression in children. See Child protection, page 760
• Consider de-escalation techniques that have worked in the past for this patient
2. Techniques• Make sure more than one staff member is present. If there is a trusted staff member of the patient
available this may help in de-escalation
• If patient persists in directing anger or suspicion at the staff member, change to another staff member to continue de-escalation
• One staff member should take the primary role in communicating with an agitated or angry patient
• Introduce yourself, your role and the purpose of the discussion
• Do not routinely administer sedating medicines upon presentation
• Lead the discussion and engage the patient. Even though other staff are nearby, it is imperative that only one staff member verbally engage the patient
• Be empathic, non-judgemental and respectful. Emphasise your desire to help
De-
esca
lati
on
tec
hn
iqu
es
790790 | Primary Clinical Care Manual 10th edition |790
• Avoid potentially provocative statements such as 'calm down' or 'if you don’t settle down x will happen', 'you’d better stop that right now … or else' as this is likely to be perceived as a threat by the patient and aggressive behaviour may escalate
• Listen to the patient’s concerns, ask what they want and what they are worried about
• Try to identify patient’s needs that have not been met and help them explore their fears
• Focus on the here and now, identify what is achievable, rather than declining all requests, small concessions can build trust and rapport
• Use short, clear statements, avoid medical jargon. The patient may not have the capacity to process information
• Use a slow, clear and steady voice and do not raise your voice. If the patient raises their voice, pause and wait for an opening to allow the patient to vent some of their frustrations
• Courtesies such as a cup of (lukewarm) tea, sandwiches, access to a telephone (0r a staff member making a phone call on their behalf) and attending to physical needs can be very helpful
• Where relevant, the patient should be given the option of taking oral medication
• Avoid entering discussion about leaving the facility, focus conversation on staying within the room/area. If patient wants a cigarette consider nicotine replacement e.g. gum/lozenges, patches or nicotine inhaler
• For patients with a disability, ensure that the communication aligns with the patient's communication plans
3. Additional techniques with children and adolescents• Use calming techniques and distraction with children - if appropriate ask parents/guardians which
de-escalation techniques they use
• Offer opportunity for a child or young person to move away from situations where violence or aggression is occurring i.e. to a quiet room or area
• Using a non judgemental attitude towards the behaviour of the child or adolescent is critical to engagement
• Where relevant, the child or adolescent should be given the option of taking oral medication (most children/adolescents can be supported to take this option)
• Reassure and help parents/guardians with their own anxiety
• If the presence of parents/guardians/friends is increasing the level of agitation then separating them within the facility may be useful. Individuals who appear to calm the patient can be asked to stay if it is safe to do so